LMA Airways Manual
23
LMA TM AIRWAY INSTRUCTION MANUAL INSTRUCTION MANUAL Revised 2005 Revised 2005 www.lmana.com San Diego, CA 92122 (800) 788-7999 P/N: 3000327-1-04/05 ©April 2005 The Laryngeal Mask Company Limited. All rights reserved Manufactured by: Distributed by:
-
Upload
sally-sarena-hasbolah -
Category
Documents
-
view
217 -
download
6
Transcript of LMA Airways Manual
LMATM AIRWAY INSTRUCTION MANUAL
INST
RU
CT
ION
MA
NU
AL
Revised 2005
Revised 2005
www.lmana.comSan Diego, CA 92122
(800) 788-7999P/N: 3000327-1-04/05
©April 2005 The Laryngeal Mask Company Limited. All rights reserved
Manufactured by:
Distributed by:
LM
AT
M
Air
way
(Yea
r of
U.S
.In
trod
uctio
n)P
rim
ary
Use
PP
VSp
onta
neou
sbr
eath
ing
Reu
sabl
e(Y
/N)
Adu
ltSi
zes
Ped
iatr
icSi
zes
Eas
e of
Intu
bati
onU
se w
ith
MR
I
LM
A C
lass
icT
M
(199
2)R
outi
ne G
A c
ases
Up
to20
cm
H2O
++
+Y
4, 5
, 61,
11/
2, 2
,2 1
/2, 3
++
++
LM
A P
roSe
alT
M
(200
0)
Cas
es n
eedi
ng h
ighe
r se
alpr
essu
res,
esp
ecia
lly w
ith
PP
V
Cas
es w
here
acc
ess
to
GI
trac
t is
desi
red
Up
to30
cm
H2O
++
Y4,
511
/2, 2
, 2 1
/2, 3
++
LM
A F
lexi
bleT
M
(199
6)
Hea
d &
nec
k ca
ses,
espe
cial
ly e
yes,
ears
, nos
e &
thro
atU
p to
20 c
m H
2O+
Y4,
5, 6
2, 2
1/2,
3–
+
Sing
le U
seL
MA
Fle
xibl
eTM
(200
4)
Hea
d &
nec
k ca
ses,
espe
cial
ly e
yes,
ears
, nos
e &
thro
atU
p to
20 c
m H
2O+
N4,
52,
21/
2, 3
–+
LM
A U
niqu
eTM
(199
7)
Rou
tine
GA
cas
es
Stoc
k cr
ash
cart
s fo
r re
scue
air
way
Up
to20
cm
H2O
++
+N
4, 5
2, 2
1/2,
3+
++
+
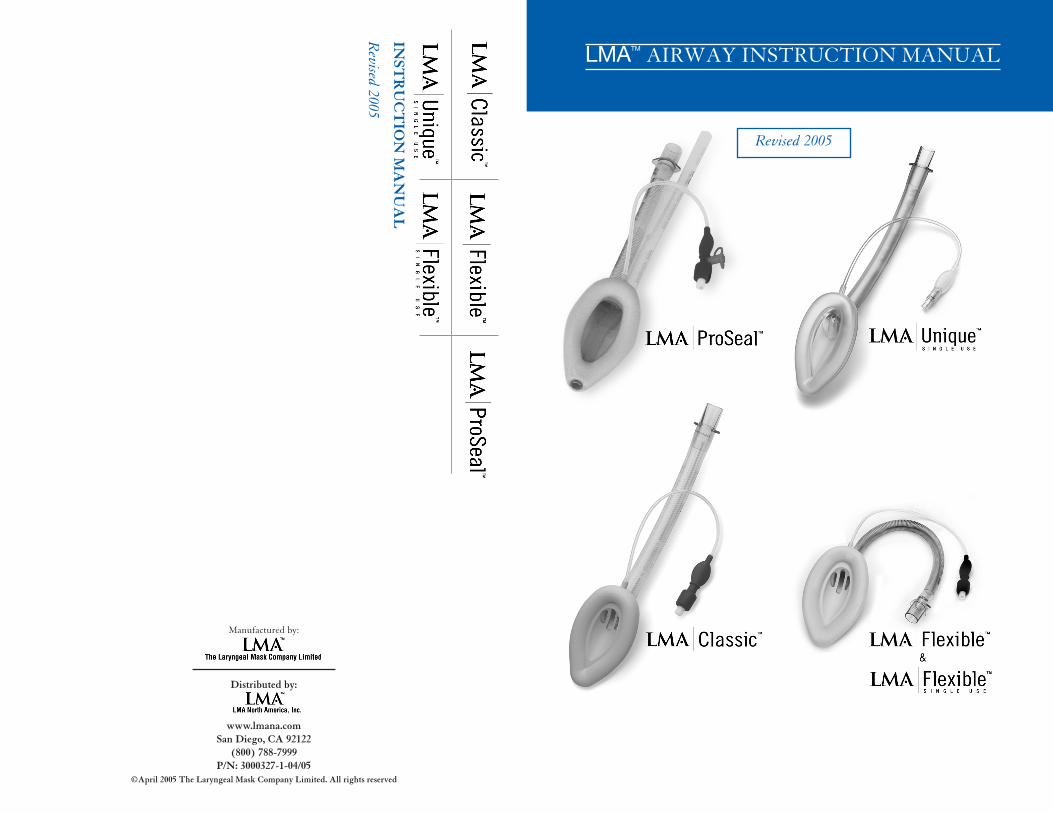
( -) =
Not
com
pati
ble
+=
Com
pati
ble
++
= R
ecom
men
ded
++
+=
Opt
imal
GA
= G
ener
al a
nest
hesi
a*
Det
aile
d in
stru
ctio
ns in
a s
epar
ate
man
ual
LMA
TM
Air
way
Sum
mar
y
LM
A F
astr
achT
M *
(199
8)F
acili
tate
intu
bati
onU
p to
20 c
m H
2O+
+Y
4, 5
3+
++
–
TM
TABLE OF CONTENTS1 DEVICE DESCRIPTION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1
2 INDICATIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4
3 CONTRAINDICATIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4
4 WARNINGS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5
5 PRECAUTIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .7
6 ADVERSE EFFECTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .8
7 PREPARATION FOR USE . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .97.1 Cleaning Reusable LMATM
Airways . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .97.1.1 Cleaning the LMA ClassicTM
and reusable LMA FlexibleTM . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .9 7.1.2 Additional Instructions for Cleaning the LMA ProSealTM . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .10 7.2 Sterilization of LMATM
Airways . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .10 7.2.1 Sterilization of the LMA ClassicTM
, reusable LMA FlexibleTM
and LMA ProSealTM
without manual vent 10 7.2.2 Sterilization of the LMA ProSealTM
with manual vent . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .11 7.3 Autoclave Settings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .11 7.4 Special Considerations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .12 7.5 Performance Tests . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .12
8 INSERTION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .158.1 Pre-insertion preparation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .15 8.2 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .16 8.3 Insertion methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .16 8.4 Insertion problems . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .22 8.5 Inflation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .22 8.6 Connecting to the anesthetic system . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .22 8.7 Fixation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .23 8.8 Diagnosis of correct and incorrect LMA ProSealTM
position . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .23
9 ANESTHESIA MAINTENANCE AND RECOVERY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .25 9.1 Spontaneous ventilation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .25 9.2 Positive pressure ventilation (PPV) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .25 9.3 Potential problems after insertion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .26 9.4 Emergence from anesthesia and removal . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .28
10 SPECIALIZED USES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .29 10.1 Pediatric use . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .29 10.2 Gastric drainage with the LMATM
airway . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .29 10.2.1 LMA ClassicTM
, LMA UniqueTM
, LMA FlexibleTM and single use LMA FlexibleTM . . . . . . . . . . . . .29 10.2.2 LMA ProSealTM . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .29 10.3 Use of the LMA FlexibleTM / and single use LMA FlexibleTM . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .30 10.3.1 Ventilation with LMA FlexibleTM / and single use LMA FlexibleTM . . . . . . . . . . . . . . . . . . . . . . . . . .30 10.3.2 Use of throat pack with LMA FlexibleTM / and single use LMA FlexibleTM . . . . . . . . . . . . . . . . . . . . .31 10.4 Use with magnetic resonance imaging (MRI) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .31 10.5 Use with endoscopy and fiberoptic intubation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .31 10.6 Blind tracheal intubation through the LMATM
airway . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .32
11 REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .33
12 APPENDIX . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .34
Manufacturer’s Warranty
The Laryngeal Mask Company Limited warrants the LMATM airway products against faulty materials ormanufacturing defects. The reusable LMATM airways are warranted for forty (40) uses or a period of one (1) yearfrom date of invoice, whichever comes first, provided that the product is used in accordance with theprocedures set forth in the instruction manual. A completed LMATM airway record card or log sheet recordinguses and the LMATM airway must accompany any return for evaluation of a manufacturing defect. Single-useproducts are warranted against faulty materials or manufacturing defects at time of delivery to customer.Warranty applicable only if purchased from an authorized distributor. THE LARYNGEAL MASK COMPANYLIMITED DISCLAIMS ALL OTHER WARRANTIES, WHETHER EXPRESS OR IMPLIED, INCLUDING, WITHOUTLIMITATION, THE WARRANTIES OF MERCHANTABILITY OR FITNESS FOR A PARTICULAR PURPOSE.
CAUTION: Federal law restricts this device to sale by or on the order of a practitioner licensed by state law to usesuch device.
No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form orby means electrical, mechanical, photocopying, recording or otherwise, without the prior permission ofthe publisher. LMATM, LMA ProSealTM, LMA ClassicTM, LMA UniqueTM, LMA FlexibleTM, single use LMAFlexibleTMand LMA FastrachTM are trademarks of The Laryngeal Mask Company Limited.
© April 2005 The Laryngeal Mask Company Limited. All rights reserved.

DEVICE DESCRIPTION
The LMATM airway is a supraglottic airway management device.1 Since its commercial introduction in 1988, the LMATM airway has been used in over 200 million patients for routine and emergency procedures.
The LMATM system of products includes 6 airway devices and various accessories, all ofwhich are latex-free. A summary table describing the airway devices is provided on theinside front cover of the manual. This manual covers 5 of the airway devices: the LMAProSealTM, the LMA UniqueTM, the LMA ClassicTM, the LMA FlexibleTM and the single use LMAFlexibleTM. An additional LMATM airway designed to facilitate endotracheal intubation, the LMAFastrachTM, is covered in another instruction manual.
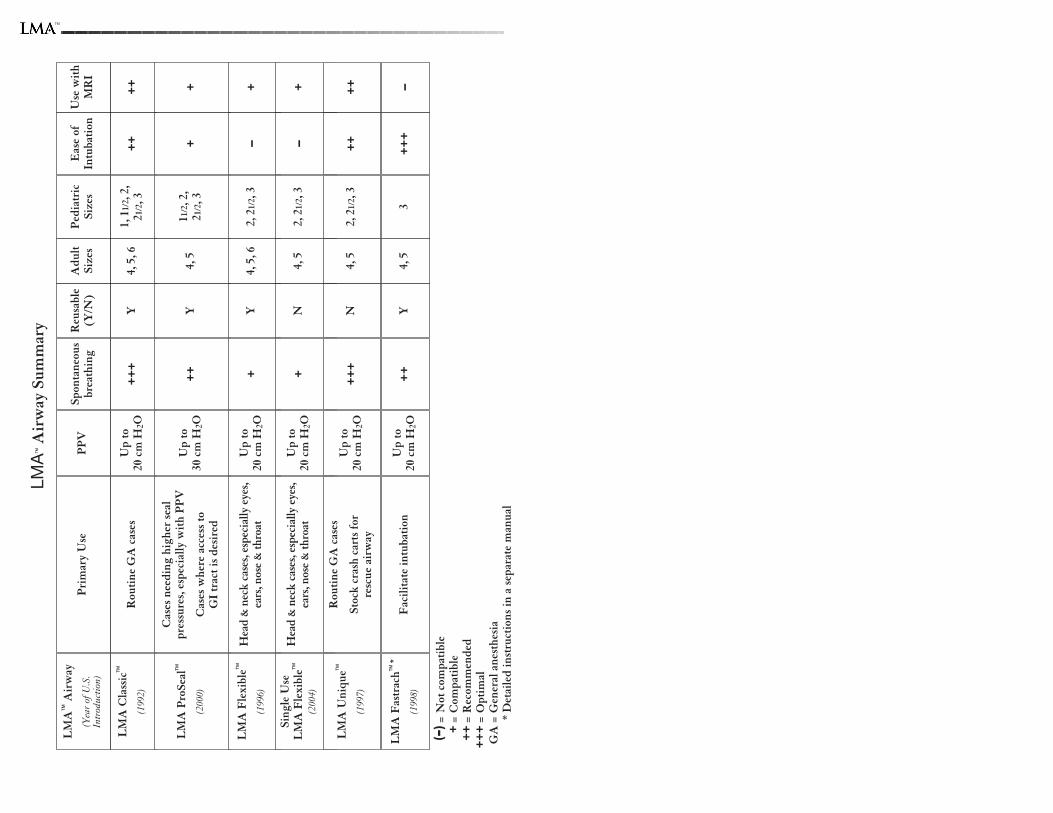
All LMATM airway devices have three main components: airway tube, mask, and inflation line(Figure 1). The airway tube has a standard 15 mm connector. The mask is designed to conform to the contours of the hypopharynx with its lumen facing the laryngeal opening.
Fig. 1: The components of the LMATM airway.
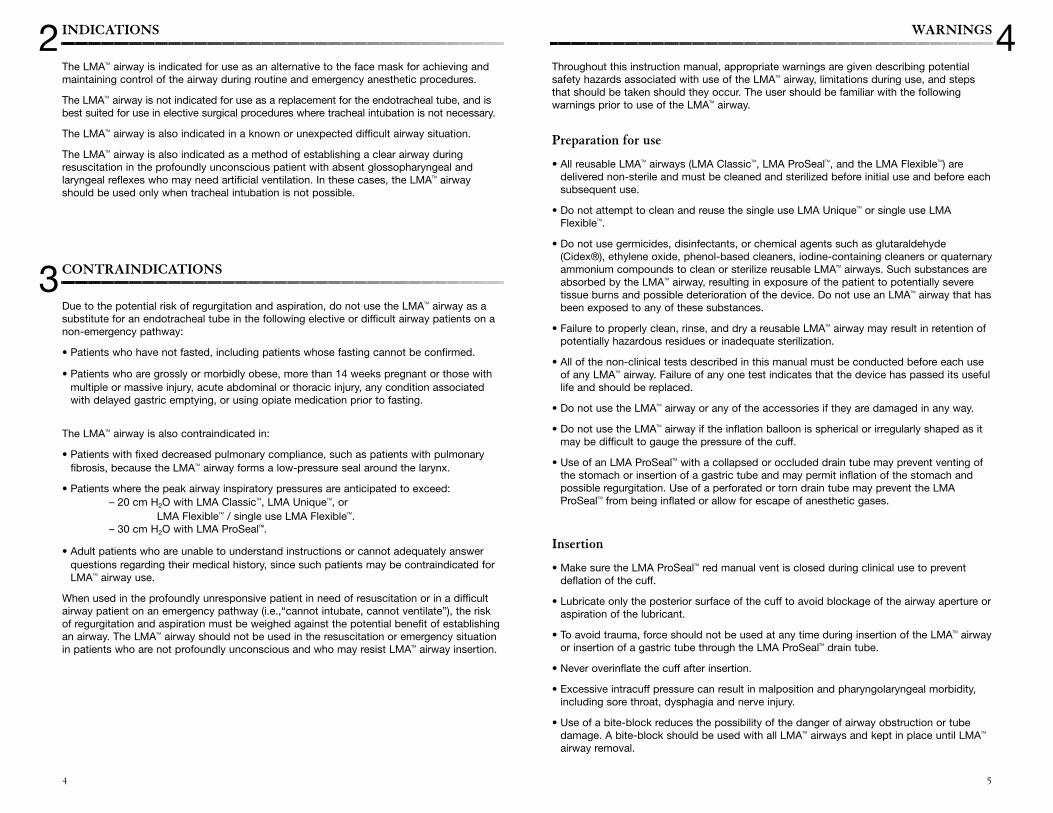
Fig. 2: Dorsal view of the LMATM cuff showing position inrelation to pharyngeal anatomy.
The LMATM airway is designed to be a minimally-stimulating device. When fully insertedusing the recommended insertion technique, the distal tip of the LMATM cuff presses againstthe upper esophageal sphincter. Its sides face into the pyriform fossae and the upper border rests against the base of the tongue (Figure 2).
1
1
MASK
AIRWAY TUBE
AIRWAY CONNECTOR
INFLATION LINE
INFLATION INDICATOR BALLOON
VALVEAPERTURE BAR
CUFF
SOFT PALATE
POSTERIORTHIRD OFTONGUE
LARYNGEALINLET
INTERARYTENOIDNOTCH
THYROID GLAND
ESOPHAGUS
MUCOUSMEMBRANECOVERINGCRICOIDCARTILAGE
UVULA
PYRIFORMFOSSA
ARYEPIGLOTTICFOLD
EPIGLOTTIS
UPPERESOPHAGEALSPHINCTER
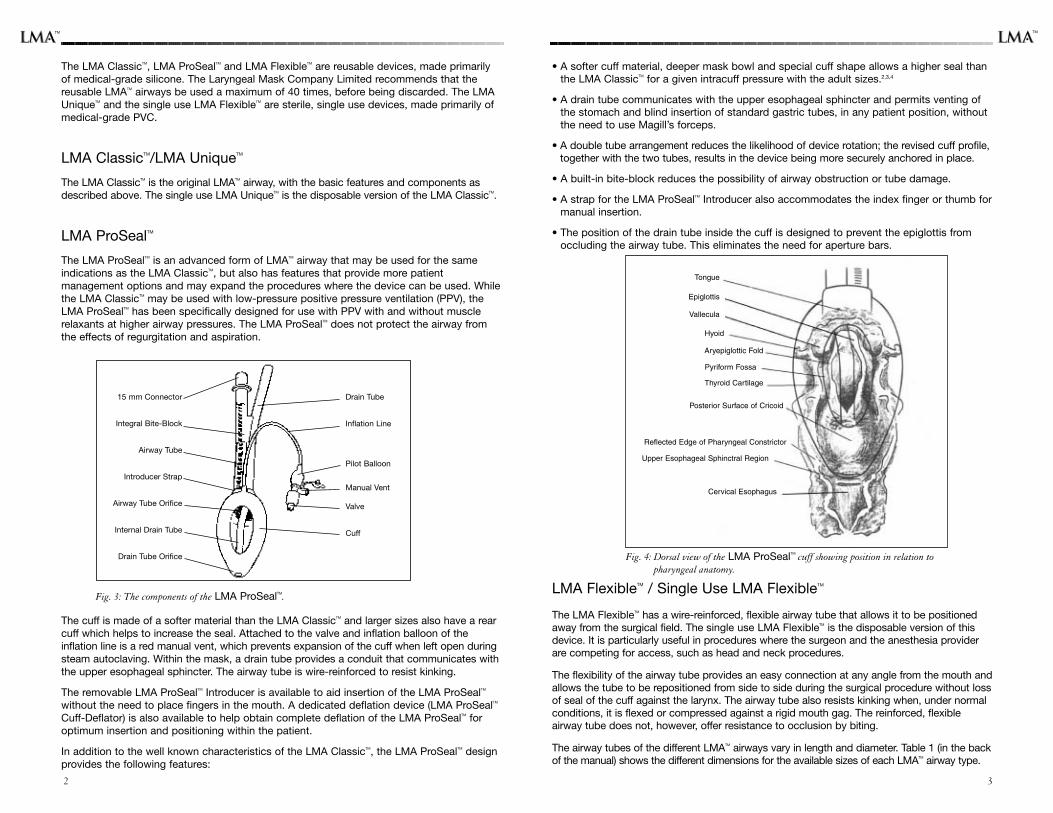
• A softer cuff material, deeper mask bowl and special cuff shape allows a higher seal thanthe LMA ClassicTM for a given intracuff pressure with the adult sizes.2,3,4
• A drain tube communicates with the upper esophageal sphincter and permits venting ofthe stomach and blind insertion of standard gastric tubes, in any patient position, withoutthe need to use Magill’s forceps.
• A double tube arrangement reduces the likelihood of device rotation; the revised cuff profile,together with the two tubes, results in the device being more securely anchored in place.
• A built-in bite-block reduces the possibility of airway obstruction or tube damage.
• A strap for the LMA ProSealTM Introducer also accommodates the index finger or thumb formanual insertion.
• The position of the drain tube inside the cuff is designed to prevent the epiglottis fromoccluding the airway tube. This eliminates the need for aperture bars.
Fig. 4: Dorsal view of the LMA ProSealTM cuff showing position in relation to pharyngeal anatomy.
LMA FlexibleTM / Single Use LMA FlexibleTM
The LMA FlexibleTM has a wire-reinforced, flexible airway tube that allows it to be positionedaway from the surgical field. The single use LMA FlexibleTM is the disposable version of thisdevice. It is particularly useful in procedures where the surgeon and the anesthesia providerare competing for access, such as head and neck procedures.
The flexibility of the airway tube provides an easy connection at any angle from the mouth andallows the tube to be repositioned from side to side during the surgical procedure without lossof seal of the cuff against the larynx. The airway tube also resists kinking when, under normalconditions, it is flexed or compressed against a rigid mouth gag. The reinforced, flexibleairway tube does not, however, offer resistance to occlusion by biting.
The airway tubes of the different LMATM airways vary in length and diameter. Table 1 (in the backof the manual) shows the different dimensions for the available sizes of each LMATM airway type.
Tongue
Epiglottis
Vallecula
Hyoid
Aryepiglottic Fold
Pyriform Fossa
Thyroid Cartilage
Posterior Surface of Cricoid
Reflected Edge of Pharyngeal Constrictor
Upper Esophageal Sphinctral Region
Cervical Esophagus
The LMA ClassicTM, LMA ProSealTM and LMA FlexibleTM are reusable devices, made primarilyof medical-grade silicone. The Laryngeal Mask Company Limited recommends that thereusable LMATM airways be used a maximum of 40 times, before being discarded. The LMAUniqueTM and the single use LMA FlexibleTM are sterile, single use devices, made primarily ofmedical-grade PVC.
LMA ClassicTM/LMA UniqueTM
The LMA ClassicTM is the original LMATM airway, with the basic features and components asdescribed above. The single use LMA UniqueTM is the disposable version of the LMA ClassicTM.
LMA ProSealTM
The LMA ProSealTM is an advanced form of LMATM airway that may be used for the sameindications as the LMA ClassicTM, but also has features that provide more patientmanagement options and may expand the procedures where the device can be used. Whilethe LMA ClassicTM may be used with low-pressure positive pressure ventilation (PPV), theLMA ProSealTM has been specifically designed for use with PPV with and without musclerelaxants at higher airway pressures. The LMA ProSealTM does not protect the airway fromthe effects of regurgitation and aspiration.
Fig. 3: The components of the LMA ProSealTM.
The cuff is made of a softer material than the LMA ClassicTM and larger sizes also have a rearcuff which helps to increase the seal. Attached to the valve and inflation balloon of theinflation line is a red manual vent, which prevents expansion of the cuff when left open duringsteam autoclaving. Within the mask, a drain tube provides a conduit that communicates withthe upper esophageal sphincter. The airway tube is wire-reinforced to resist kinking.
The removable LMA ProSealTM Introducer is available to aid insertion of the LMA ProSealTM
without the need to place fingers in the mouth. A dedicated deflation device (LMA ProSealTM
Cuff-Deflator) is also available to help obtain complete deflation of the LMA ProSealTM foroptimum insertion and positioning within the patient.
In addition to the well known characteristics of the LMA ClassicTM, the LMA ProSealTM designprovides the following features:
32
15 mm Connector
Integral Bite-Block
Airway Tube
Introducer Strap
Airway Tube Orifice
Internal Drain Tube
Drain Tube Orifice
Drain Tube
Inflation Line
Pilot Balloon
Manual Vent
Valve
Cuff
TMTM
WARNINGS
Throughout this instruction manual, appropriate warnings are given describing potentialsafety hazards associated with use of the LMATM airway, limitations during use, and stepsthat should be taken should they occur. The user should be familiar with the followingwarnings prior to use of the LMATM airway.
Preparation for use
• All reusable LMATM airways (LMA ClassicTM, LMA ProSealTM, and the LMA FlexibleTM) aredelivered non-sterile and must be cleaned and sterilized before initial use and before eachsubsequent use.
• Do not attempt to clean and reuse the single use LMA UniqueTM or single use LMAFlexibleTM.
• Do not use germicides, disinfectants, or chemical agents such as glutaraldehyde(Cidex®), ethylene oxide, phenol-based cleaners, iodine-containing cleaners or quaternaryammonium compounds to clean or sterilize reusable LMATM airways. Such substances areabsorbed by the LMATM airway, resulting in exposure of the patient to potentially severetissue burns and possible deterioration of the device. Do not use an LMATM airway that hasbeen exposed to any of these substances.
• Failure to properly clean, rinse, and dry a reusable LMATM airway may result in retention ofpotentially hazardous residues or inadequate sterilization.
• All of the non-clinical tests described in this manual must be conducted before each useof any LMATM airway. Failure of any one test indicates that the device has passed its usefullife and should be replaced.
• Do not use the LMATM airway or any of the accessories if they are damaged in any way.
• Do not use the LMATM airway if the inflation balloon is spherical or irregularly shaped as itmay be difficult to gauge the pressure of the cuff.
• Use of an LMA ProSealTM with a collapsed or occluded drain tube may prevent venting ofthe stomach or insertion of a gastric tube and may permit inflation of the stomach andpossible regurgitation. Use of a perforated or torn drain tube may prevent the LMAProSealTM from being inflated or allow for escape of anesthetic gases.
Insertion
• Make sure the LMA ProSealTM red manual vent is closed during clinical use to preventdeflation of the cuff.
• Lubricate only the posterior surface of the cuff to avoid blockage of the airway aperture oraspiration of the lubricant.
• To avoid trauma, force should not be used at any time during insertion of the LMATM airwayor insertion of a gastric tube through the LMA ProSealTM drain tube.
• Never overinflate the cuff after insertion.
• Excessive intracuff pressure can result in malposition and pharyngolaryngeal morbidity,including sore throat, dysphagia and nerve injury.
• Use of a bite-block reduces the possibility of the danger of airway obstruction or tubedamage. A bite-block should be used with all LMATM airways and kept in place until LMATM
airway removal.
4INDICATIONS
The LMATM airway is indicated for use as an alternative to the face mask for achieving andmaintaining control of the airway during routine and emergency anesthetic procedures.
The LMATM airway is not indicated for use as a replacement for the endotracheal tube, and isbest suited for use in elective surgical procedures where tracheal intubation is not necessary.
The LMATM airway is also indicated in a known or unexpected difficult airway situation.
The LMATM airway is also indicated as a method of establishing a clear airway duringresuscitation in the profoundly unconscious patient with absent glossopharyngeal andlaryngeal reflexes who may need artificial ventilation. In these cases, the LMATM airwayshould be used only when tracheal intubation is not possible.
CONTRAINDICATIONS
Due to the potential risk of regurgitation and aspiration, do not use the LMATM airway as asubstitute for an endotracheal tube in the following elective or difficult airway patients on anon-emergency pathway:
• Patients who have not fasted, including patients whose fasting cannot be confirmed.
• Patients who are grossly or morbidly obese, more than 14 weeks pregnant or those withmultiple or massive injury, acute abdominal or thoracic injury, any condition associatedwith delayed gastric emptying, or using opiate medication prior to fasting.
The LMATM airway is also contraindicated in:
• Patients with fixed decreased pulmonary compliance, such as patients with pulmonaryfibrosis, because the LMATM airway forms a low-pressure seal around the larynx.
• Patients where the peak airway inspiratory pressures are anticipated to exceed:– 20 cm H2O with LMA ClassicTM, LMA UniqueTM, or
LMA FlexibleTM / single use LMA FlexibleTM.– 30 cm H2O with LMA ProSealTM.
• Adult patients who are unable to understand instructions or cannot adequately answerquestions regarding their medical history, since such patients may be contraindicated forLMATM airway use.
When used in the profoundly unresponsive patient in need of resuscitation or in a difficultairway patient on an emergency pathway (i.e.,“cannot intubate, cannot ventilate”), the riskof regurgitation and aspiration must be weighed against the potential benefit of establishingan airway. The LMATM airway should not be used in the resuscitation or emergency situationin patients who are not profoundly unconscious and who may resist LMATM airway insertion.
2
3
54
PRECAUTIONS
This manual contains numerous precautionary statements regarding the special care to beexercised for the safe and effective use of the LMATM airway. The user and others involved inthe preparation for use of the device should be familiar with and adhere to these instructions.
Preparation for use
• Careful handling is essential. The LMATM airways are made of medical-grade silicone ormedical-grade PVC which can be torn or perforated. Avoid contact with sharp or pointedobjects at all times.
• For reusable LMATM aiways, do not expose the valve (the white plastic piece protruding fromthe blue inflation balloon) to any cleaning solution as it may cause premature valve failure.
• Make sure the LMA ProSealTM manual vent is closed during cleaning to prevent exposureof the valve to any cleaning solution.
• Any air or moisture left in the cuff of the LMA ClassicTM, reusable LMA FlexibleTM or LMAProSealTM without manual vent will expand at the high temperatures and low pressures ofthe autoclave, causing irreparable damage (herniation and/or rupture) to the cuff and/orinflation balloon.
• Make sure the LMA ProSealTM manual vent is open during sterilization to prevent herniationof the cuff.
• The integrity of the reusable LMATM airway materials may be adversely affected byexceeding sterilization temperatures of 275°F or 135°C.
• Gloves should be worn during preparation and insertion to minimize contamination of the device.
Usage
• MRI artifacts for the LMATM airways have been characterized using a 1.5 Tesla MR systemand various pulse sequences. Based on this information, MR image quality may becompromised if the area of interest is in the same area or relatively close to the position ofthe LMA ProSealTM, LMA FlexibleTM or single use LMA FlexibleTM. The valve componentlocated at the end of the inflation line should also be directed away from the area ofinterest to avoid artifacts.
• The need for instrumentation should be carefully considered and evaluated prior toinsertion of an LMA FlexibleTM / single use LMA FlexibleTM. If the need for instruments thatcannot be passed through the device is anticipated, the use of another LMATM airway or analternate method of airway management should be considered.
5
7
• An incorrectly placed mask may result in an unreliable or obstructed airway or failure ofthe LMA ProSealTM drain tube to channel fluids or gases from the stomach and mayincrease the likelihood of gastric insufflation if used with PPV. Always check for properplacement after insertion.
Usage
• The LMATM airway does not protect the patient from the effects of regurgitation andaspiration.
• Should the LMATM airway be used in a fasted patient who is at risk of retained gastriccontents, prophylactic measures to empty the stomach contents and appropriate antacidtherapy should be employed. Examples of conditions where fasted patients may be at riskof retained gastric contents include, but are not limited to: hiatal hernia and moderateobesity.
• In patients with severe oropharyngeal trauma, the device should only be used when allother attempts to establish an airway have failed.
• If airway problems persist or ventilation is inadequate, the LMATM airway should beremoved and an airway established by some other means.
• The presence of a gastric tube does not rule out the possibility of regurgitation and mayeven make regurgitation more likely because the gastric tube may make the loweresophageal sphincter incompetent.
• Do not attempt to pass a gastric tube through the LMA ProSealTM drain tube in the presence of known or suspected esophageal pathology.
• To prevent injury to the upper esophageal sphincter, do not apply suction directly to theend of the LMA ProSealTM drain tube.
• The effects of performing magnetic resonance imaging (MRI) procedures using LMATM
airways and MR systems with static magnetic fields greater than 1.5 Tesla and otherconditions have not been tested.
• The LMA ProSealTM, LMA FlexibleTM, and single use LMA FlexibleTM airways exhibit magneticfield interactions with respect to translational force and torque during exposure to ashielded 1.5 Tesla MR system (maximum spatial gradient, 450 gauss/cm). However, whenthese devices are properly positioned and adhesive tape or other similar dressing is used toretain placement, there is no additional risk to the patient with regard to movement ordislodgment using a shielded MR system with static magnetic field of 1.5 Tesla or less.Thus,when used with MRI, care should be taken to monitor the patient carefully to assurethat correct positioning of the LMATM airway tube is maintained.
6
TM
PREPARATION FOR USE
With proper cleaning, sterilization, and handling, the reusable LMATM airways can be used amaximum of 40 times. Proper cleaning and sterilization of the LMATM airways are essential toensure continued safe usage up to 40 times.
WARNING: All reusable LMATM airways (LMA ClassicTM, LMA ProSealTM, and the (reusable) LMAFlexibleTM) are delivered non-sterile and must be cleaned and sterilized before initial useand before each subsequent use. The packaging cannot withstand the high temperaturesof autoclaving and should be discarded before sterilization.
CAUTION: Careful handling is essential. The LMATM airways are made of medical-grade silicone ormedical-grade PVC which can be torn or perforated. Avoid contact with sharp or pointedobjects at all times.
WARNING: Do not attempt to clean and reuse a single use LMA UniqueTM or single useLMA FlexibleTM.
The LMATM airway accessories, i.e., the LMATM Cuff-Deflator, LMA ProSealTM Introducer andLMA ProSealTM Cuff-Deflator, should be cleaned and sterilized in the same manner as theLMATM airways.
7.1 Cleaning reusable LMATM airways
Thoroughly wash the device in warm water using a dilute (8-10% v/v) sodiumbicarbonate/water solution until all visible foreign matter is removed. A 10% sodiumbicarbonate solution can be prepared by mixing 1 cup of baking soda with 10 cups ofwater.
Mild detergents or enzymatic cleaning agents may be used in accordance with themanufacturer’s instructions. The cleaners must not contain skin or mucous membraneirritants. A specific cleaner found to be compatible with LMATM airway use is Endozime®(Ruhof, Valley Stream, NY).
WARNING: Do not use germicides, disinfectants, or chemical agents such as glutaraldehyde(Cidex®), ethylene oxide, phenol-based cleaners, iodine-containing cleaners orquaternary ammonium compounds to clean or sterilize the LMATM airway. Suchsubstances are absorbed by the materials, resulting in exposure of the patient topotentially severe tissue burns and possible deterioration of the device. Do not use an LMATM airway that has been exposed to any of these substances.
CAUTION: For reusable LMATM airways, do not expose the valve (the white plastic piece protrudingfrom the blue inflation balloon) to any cleaning solution as it may cause prematurevalve failure.
If moisture is noticed in the valve, tap against a towel to remove excess moisture.
7.1.1 Cleaning the LMA ClassicTM and (reusable) LMA FlexibleTM
Clean the airway tube using a small soft bristle brush approximately 1/2 inch in diameter.Gently insert the brush through the LMA ClassicTM or (reusable) LMA FlexibleTM aperture barsinto the airway tube, taking care not to damage the bars.
Thoroughly rinse the cuff and tube in warm running tap water to remove cleaning residues.Carefully inspect to ensure that all visible foreign matter has been removed.
Repeat the above as necessary.
9
ADVERSE EFFECTS
Both minor adverse effects (e.g., sore throat) and major adverse effects (e.g., aspiration)following use of LMATM airways have been reported in the published literature.5 Review ofpublished literature shows the incidence of aspiration with the LMATM airway is low(0.012%), with the main causes being inappropriate patient selection and inadequate depthof anesthesia.5
The incidence of sore throat following LMATM airway use is approximately 13%, and isusually mild and short-lived5; however, severe or prolonged sore throat, sometimesaccompanied by dysphagia and tissue burns, has been reported in patients in whom animproperly cleaned or sterilized reusable mask has been used.
Infrequent neurovascular events reported with LMATM airway use include cases ofhypoglossal nerve injury, tongue numbness secondary to lingual nerve injury, tonguecyanosis, tongue macroglossia, recurrent laryngeal nerve injury, and vocal cord paralysis.These complications are most likely the result of malposition or excessive intracuffpressure, causing compression of nerves and/or blood vessels. Cuff malposition orexcessive cuff pressure can be exacerbated by incorrect mask size, prolonged surgery, anduse of nitrous oxide.
Adverse events reported with LMATM airway use include airway obstruction, arytenoiddislocation, aspiration, bleeding, breath holding, bronchospasm, coughing, dental/denturedamage, dry mouth/throat, dysarthria, dysphagia, dysphonia, dysrhythmia, ear pain,gagging, gastric dilatation/insufflation/rupture, glottic closure, head and neck edema,hearing impairment, hiccup, hoarseness, hypersalivation, hypoglossal nerve paralysis,hypoxia, laryngeal hematoma, laryngeal spasm, lingual nerve paralysis, mouth ulcer,myocardial ischemia, nausea, parotid gland swelling, pharyngeal dysesthesia, pharyngealulcer, pulmonary edema, recurrent laryngeal nerve injury, regurgitation, retching, sore jaw,sore mouth, sore throat, stridor, submandibular gland swelling, temporomandibular jointdislocation, tissue trauma (epiglottis, larynx, lip, mouth, posterior pharyngeal wall, softpalate, uvula, tonsils), tongue cyanosis, tongue macroglossia, vocal cord paralysis, andvomiting.
6 7
8
however, for the cuff to re-inflate slowly over a period of several hours as the silicone rubbermaterial is gas permeable.
CAUTION: Any air or moisture left in the cuff of LMA ClassicTM, LMA FlexibleTM or LMA ProSealTM
without manual vent will expand at the high temperatures and low pressures of theautoclave, causing irreparable damage (herniation and/or rupture) to the cuff and/orinflation balloon.
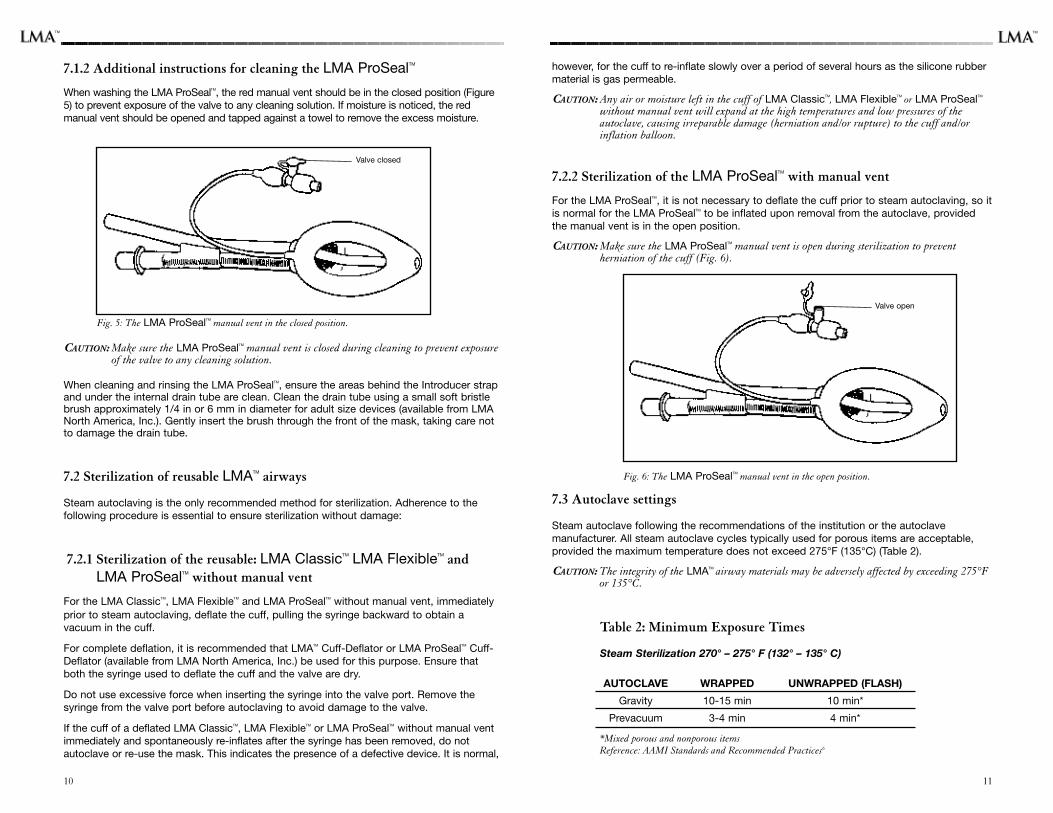
7.2.2 Sterilization of the LMA ProSealTM with manual vent
For the LMA ProSealTM, it is not necessary to deflate the cuff prior to steam autoclaving, so itis normal for the LMA ProSealTM to be inflated upon removal from the autoclave, providedthe manual vent is in the open position.
CAUTION: Make sure the LMA ProSealTM manual vent is open during sterilization to preventherniation of the cuff (Fig. 6).
Fig. 6: The LMA ProSealTM manual vent in the open position.
7.3 Autoclave settings
Steam autoclave following the recommendations of the institution or the autoclavemanufacturer. All steam autoclave cycles typically used for porous items are acceptable,provided the maximum temperature does not exceed 275°F (135°C) (Table 2).
CAUTION: The integrity of the LMATM airway materials may be adversely affected by exceeding 275°For 135°C.
Table 2: Minimum Exposure Times
Steam Sterilization 270° – 275° F (132° – 135° C)
AUTOCLAVE WRAPPED UNWRAPPED (FLASH)
Gravity 10-15 min 10 min*
Prevacuum 3-4 min 4 min*
*Mixed porous and nonporous itemsReference: AAMI Standards and Recommended Practices6
7.1.2 Additional instructions for cleaning the LMA ProSealTM
When washing the LMA ProSealTM, the red manual vent should be in the closed position (Figure5) to prevent exposure of the valve to any cleaning solution. If moisture is noticed, the redmanual vent should be opened and tapped against a towel to remove the excess moisture.
Fig. 5: The LMA ProSealTM manual vent in the closed position.
CAUTION: Make sure the LMA ProSealTM manual vent is closed during cleaning to prevent exposureof the valve to any cleaning solution.
When cleaning and rinsing the LMA ProSealTM, ensure the areas behind the Introducer strapand under the internal drain tube are clean. Clean the drain tube using a small soft bristlebrush approximately 1/4 in or 6 mm in diameter for adult size devices (available from LMANorth America, Inc.). Gently insert the brush through the front of the mask, taking care notto damage the drain tube.
7.2 Sterilization of reusable LMATM airways
Steam autoclaving is the only recommended method for sterilization. Adherence to thefollowing procedure is essential to ensure sterilization without damage:
7.2.1 Sterilization of the reusable: LMA ClassicTM LMA FlexibleTM andLMA ProSealTM without manual vent
For the LMA ClassicTM, LMA FlexibleTM and LMA ProSealTM without manual vent, immediatelyprior to steam autoclaving, deflate the cuff, pulling the syringe backward to obtain avacuum in the cuff.
For complete deflation, it is recommended that LMATM Cuff-Deflator or LMA ProSealTM Cuff-Deflator (available from LMA North America, Inc.) be used for this purpose. Ensure thatboth the syringe used to deflate the cuff and the valve are dry.
Do not use excessive force when inserting the syringe into the valve port. Remove thesyringe from the valve port before autoclaving to avoid damage to the valve.
If the cuff of a deflated LMA ClassicTM, LMA FlexibleTM or LMA ProSealTM without manual ventimmediately and spontaneously re-inflates after the syringe has been removed, do notautoclave or re-use the mask. This indicates the presence of a defective device. It is normal,
1110
Valve closed
Valve open
TMTM
WARNING: Do not use the LMATM airway if it is damaged or if visible particles cannot be removedfrom inside the airway tube as they may be inhaled by the patient after insertion.
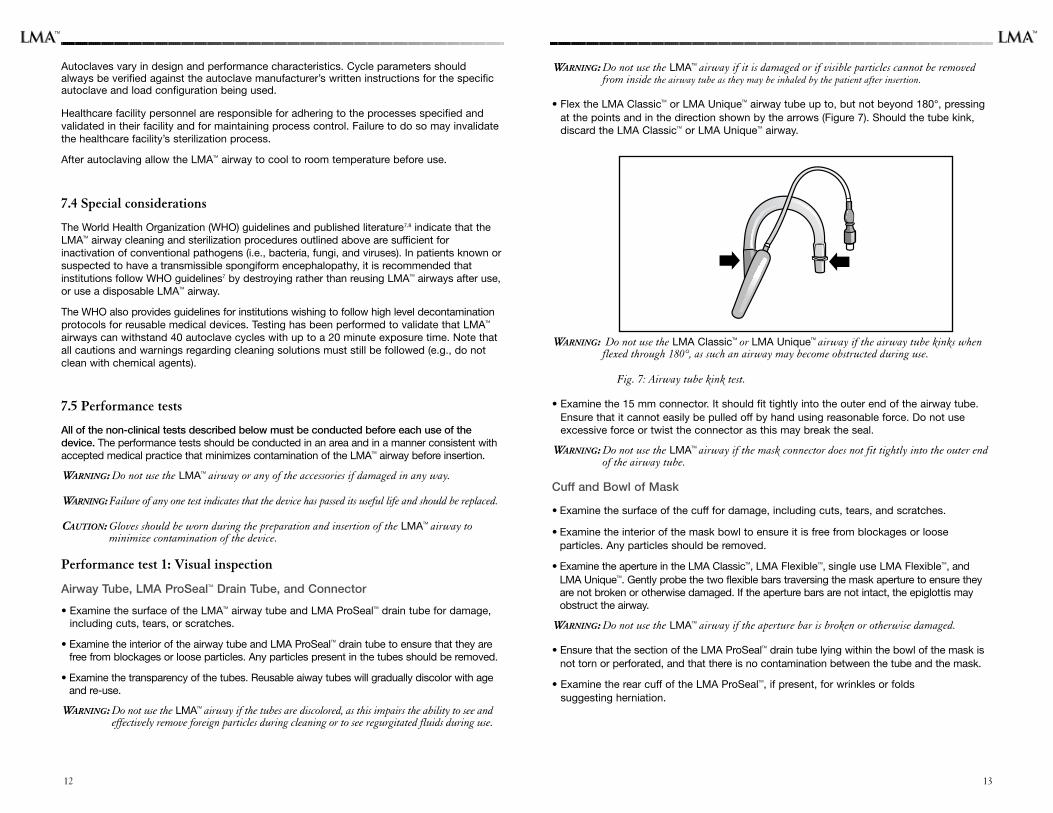
• Flex the LMA ClassicTM or LMA UniqueTM airway tube up to, but not beyond 180°, pressingat the points and in the direction shown by the arrows (Figure 7). Should the tube kink,discard the LMA ClassicTM or LMA UniqueTM airway.
WARNING: Do not use the LMA ClassicTM or LMA UniqueTM airway if the airway tube kinks whenflexed through 180°, as such an airway may become obstructed during use.
Fig. 7: Airway tube kink test.
• Examine the 15 mm connector. It should fit tightly into the outer end of the airway tube.Ensure that it cannot easily be pulled off by hand using reasonable force. Do not useexcessive force or twist the connector as this may break the seal.
WARNING: Do not use the LMATM airway if the mask connector does not fit tightly into the outer endof the airway tube.
Cuff and Bowl of Mask
• Examine the surface of the cuff for damage, including cuts, tears, and scratches.
• Examine the interior of the mask bowl to ensure it is free from blockages or looseparticles. Any particles should be removed.
• Examine the aperture in the LMA ClassicTM, LMA FlexibleTM, single use LMA FlexibleTM, andLMA UniqueTM. Gently probe the two flexible bars traversing the mask aperture to ensure theyare not broken or otherwise damaged. If the aperture bars are not intact, the epiglottis mayobstruct the airway.
WARNING: Do not use the LMATM airway if the aperture bar is broken or otherwise damaged.
• Ensure that the section of the LMA ProSealTM drain tube lying within the bowl of the mask isnot torn or perforated, and that there is no contamination between the tube and the mask.
• Examine the rear cuff of the LMA ProSealTM, if present, for wrinkles or folds suggesting herniation.
Autoclaves vary in design and performance characteristics. Cycle parameters shouldalways be verified against the autoclave manufacturer’s written instructions for the specificautoclave and load configuration being used.
Healthcare facility personnel are responsible for adhering to the processes specified andvalidated in their facility and for maintaining process control. Failure to do so may invalidatethe healthcare facility’s sterilization process.
After autoclaving allow the LMATM airway to cool to room temperature before use.
7.4 Special considerations
The World Health Organization (WHO) guidelines and published literature7,8 indicate that theLMATM airway cleaning and sterilization procedures outlined above are sufficient forinactivation of conventional pathogens (i.e., bacteria, fungi, and viruses). In patients known orsuspected to have a transmissible spongiform encephalopathy, it is recommended thatinstitutions follow WHO guidelines7 by destroying rather than reusing LMATM airways after use,or use a disposable LMATM airway.
The WHO also provides guidelines for institutions wishing to follow high level decontaminationprotocols for reusable medical devices. Testing has been performed to validate that LMATM
airways can withstand 40 autoclave cycles with up to a 20 minute exposure time. Note thatall cautions and warnings regarding cleaning solutions must still be followed (e.g., do notclean with chemical agents).
7.5 Performance tests
All of the non-clinical tests described below must be conducted before each use of thedevice. The performance tests should be conducted in an area and in a manner consistent withaccepted medical practice that minimizes contamination of the LMATM airway before insertion.
WARNING: Do not use the LMATM airway or any of the accessories if damaged in any way.
WARNING: Failure of any one test indicates that the device has passed its useful life and should be replaced.
CAUTION: Gloves should be worn during the preparation and insertion of the LMATM airway tominimize contamination of the device.
Performance test 1: Visual inspection
Airway Tube, LMA ProSealTM Drain Tube, and Connector
• Examine the surface of the LMATM airway tube and LMA ProSealTM drain tube for damage,including cuts, tears, or scratches.
• Examine the interior of the airway tube and LMA ProSealTM drain tube to ensure that they arefree from blockages or loose particles. Any particles present in the tubes should be removed.
• Examine the transparency of the tubes. Reusable aiway tubes will gradually discolor with ageand re-use.
WARNING: Do not use the LMATM airway if the tubes are discolored, as this impairs the ability to see andeffectively remove foreign particles during cleaning or to see regurgitated fluids during use.
1312
TM TM
INSERTION8.1 Pre-insertion preparation
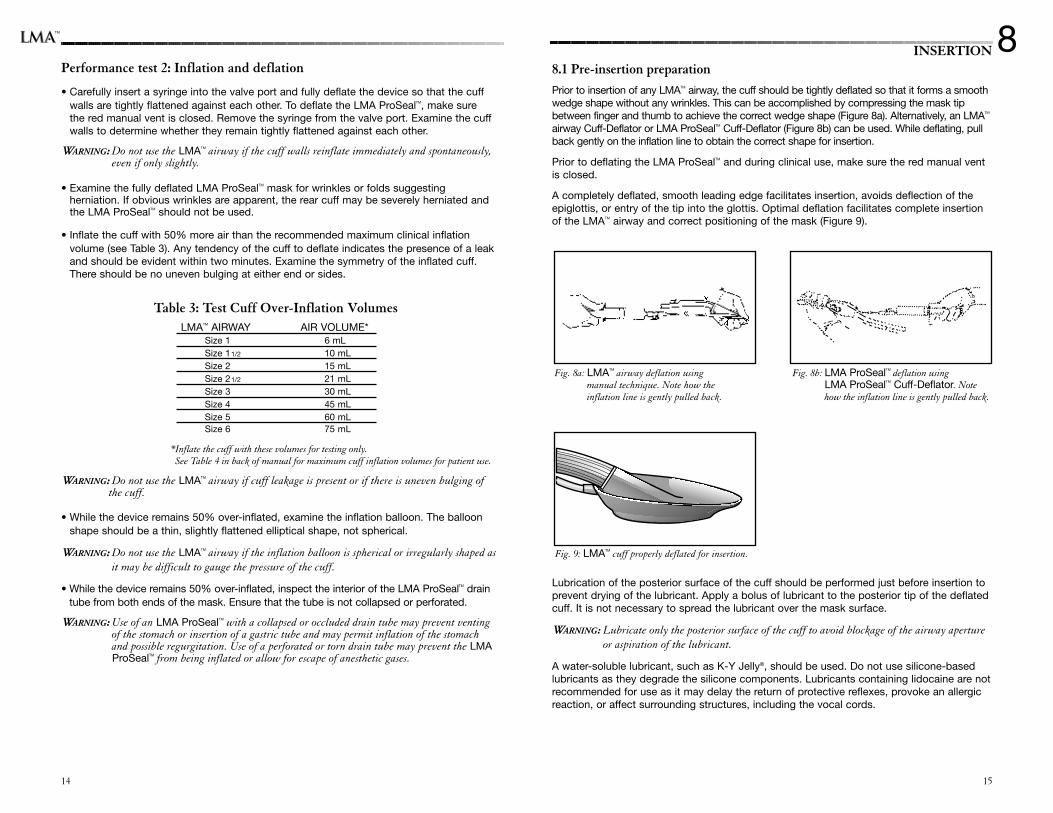
Prior to insertion of any LMATM airway, the cuff should be tightly deflated so that it forms a smoothwedge shape without any wrinkles. This can be accomplished by compressing the mask tipbetween finger and thumb to achieve the correct wedge shape (Figure 8a). Alternatively, an LMATM
airway Cuff-Deflator or LMA ProSealTM Cuff-Deflator (Figure 8b) can be used. While deflating, pullback gently on the inflation line to obtain the correct shape for insertion.
Prior to deflating the LMA ProSealTM and during clinical use, make sure the red manual ventis closed.
A completely deflated, smooth leading edge facilitates insertion, avoids deflection of theepiglottis, or entry of the tip into the glottis. Optimal deflation facilitates complete insertionof the LMATM airway and correct positioning of the mask (Figure 9).
Lubrication of the posterior surface of the cuff should be performed just before insertion toprevent drying of the lubricant. Apply a bolus of lubricant to the posterior tip of the deflatedcuff. It is not necessary to spread the lubricant over the mask surface.
WARNING: Lubricate only the posterior surface of the cuff to avoid blockage of the airway apertureor aspiration of the lubricant.
A water-soluble lubricant, such as K-Y Jelly®, should be used. Do not use silicone-basedlubricants as they degrade the silicone components. Lubricants containing lidocaine are notrecommended for use as it may delay the return of protective reflexes, provoke an allergicreaction, or affect surrounding structures, including the vocal cords.
15
Performance test 2: Inflation and deflation
• Carefully insert a syringe into the valve port and fully deflate the device so that the cuffwalls are tightly flattened against each other. To deflate the LMA ProSealTM, make sure the red manual vent is closed. Remove the syringe from the valve port. Examine the cuffwalls to determine whether they remain tightly flattened against each other.
WARNING: Do not use the LMATM airway if the cuff walls reinflate immediately and spontaneously,even if only slightly.
• Examine the fully deflated LMA ProSealTM mask for wrinkles or folds suggestingherniation. If obvious wrinkles are apparent, the rear cuff may be severely herniated andthe LMA ProSealTM should not be used.
• Inflate the cuff with 50% more air than the recommended maximum clinical inflation volume (see Table 3). Any tendency of the cuff to deflate indicates the presence of a leakand should be evident within two minutes. Examine the symmetry of the inflated cuff.There should be no uneven bulging at either end or sides.
Table 3: Test Cuff Over-Inflation VolumesLMATM AIRWAY AIR VOLUME*
Size 1 6 mLSize 11/2 10 mLSize 2 15 mLSize 21/2 21 mLSize 3 30 mLSize 4 45 mLSize 5 60 mLSize 6 75 mL
*Inflate the cuff with these volumes for testing only.See Table 4 in back of manual for maximum cuff inflation volumes for patient use.
WARNING: Do not use the LMATM airway if cuff leakage is present or if there is uneven bulging of the cuff.
• While the device remains 50% over-inflated, examine the inflation balloon. The balloonshape should be a thin, slightly flattened elliptical shape, not spherical.
WARNING: Do not use the LMATM airway if the inflation balloon is spherical or irregularly shaped asit may be difficult to gauge the pressure of the cuff.
• While the device remains 50% over-inflated, inspect the interior of the LMA ProSealTM draintube from both ends of the mask. Ensure that the tube is not collapsed or perforated.
WARNING: Use of an LMA ProSealTM with a collapsed or occluded drain tube may prevent ventingof the stomach or insertion of a gastric tube and may permit inflation of the stomachand possible regurgitation. Use of a perforated or torn drain tube may prevent the LMAProSealTM from being inflated or allow for escape of anesthetic gases.
8
14
Fig. 9: LMATM cuff properly deflated for insertion.
Fig. 8a: LMATM airway deflation using manual technique. Note how the inflation line is gently pulled back.
Fig. 8b: LMA ProSealTM deflation using LMA ProSealTM Cuff-Deflator. Notehow the inflation line is gently pulled back.
TM
17
8.2 Introduction
Before using any LMATM airway, the user should be familiar with the instructions contained in thismanual. If the device is inserted incorrectly, an unreliable or obstructed airway may be obtained.In addition, an incorrectly placed mask may result in failure of the LMA ProSealTM drain tube tochannel fluids or gases from the stomach and may increase the likelihood of gastric insufflation ifused with PPV. Always check for proper placement after insertion (see Sections 8.4, 8.5 and 8.8).
WARNING: An incorrectly placed mask may result in an unreliable or obstructed airway or failure of theLMA ProSealTM drain tube to channel fluids or gases from the stomach and may increase thelikelihood of gastric insufflation if used with PPV. Always check for proper placement after insertion.
Before insertion it is important to note the following points:• Check that the size of the device is appropriate for the patient (see Table 4 in back of
manual).The ranges are approximate and clinical judgment should be used in selecting anappropriate size.
• The cuff must always be fully deflated by firmly pulling back on the deflating syringe andgently pulling on the inflation line.
• Check the shape of the cuff and its lubrication, as described previously.
• Have a spare sterile LMATM airway ready and prepared for immediate use. Where possible, analternative size of LMATM airway should also be available.
• Pre-oxygenate and implement standard monitoring procedures.
• Achieve an adequate level of anesthesia before attempting insertion. Resistance or swallowingindicates inadequate anesthesia. Retching indicates inadequate anesthesia and/orinappropriate technique. Inexperienced users should choose a deeper level of anesthesia.
• The ideal head position is extension of the head with flexion of the neck in the positionnormally used for tracheal intubation (“the sniffing position”).This can be achieved by pushingthe head from behind with the non-dominant hand during the movement of insertion. A pillowcan also be used to keep the neck flexed.
• Excessive force must be avoided at all times.
• When using the LMA ProSealTM Introducer, it may be possible to reduce or eliminate head andneck manipulation.
• Make sure the LMA ProSealTM red manual vent is closed during clinical use.
WARNING: Make sure the LMA ProSealTM red manual vent is closed during clinical use to preventdeflation of the cuff.
8.3 Insertion methods
The LMA ClassicTM, LMA ProSealTM, LMA FlexibleTM, single use LMA FlexibleTM, and LMA UniqueTM
may be inserted using the standard index finger or the thumb technique, depending on accessto the patient.
The LMA ProSealTM may also be inserted using the LMA ProSealTM Introducer. The dedicatedIntroducer may provide a more useful method of insertion than the thumb/finger techniques,when using LMA ProSealTM sizes 1-2 1/2.
All three techniques follow the same principles. To position the LMATM airway correctly, the cufftip must avoid entering the valleculae or the glottic opening and must not become caught upagainst the epiglottis or the arytenoids. The cuff must be deflated in the correct wedge shape(Figure 9) and should be kept pressed against the patient’s posterior pharyngeal wall. To avoidcontact with anterior structures during insertion, the inserting finger must press the tubeupwards (cranially) throughout the insertion maneuver.
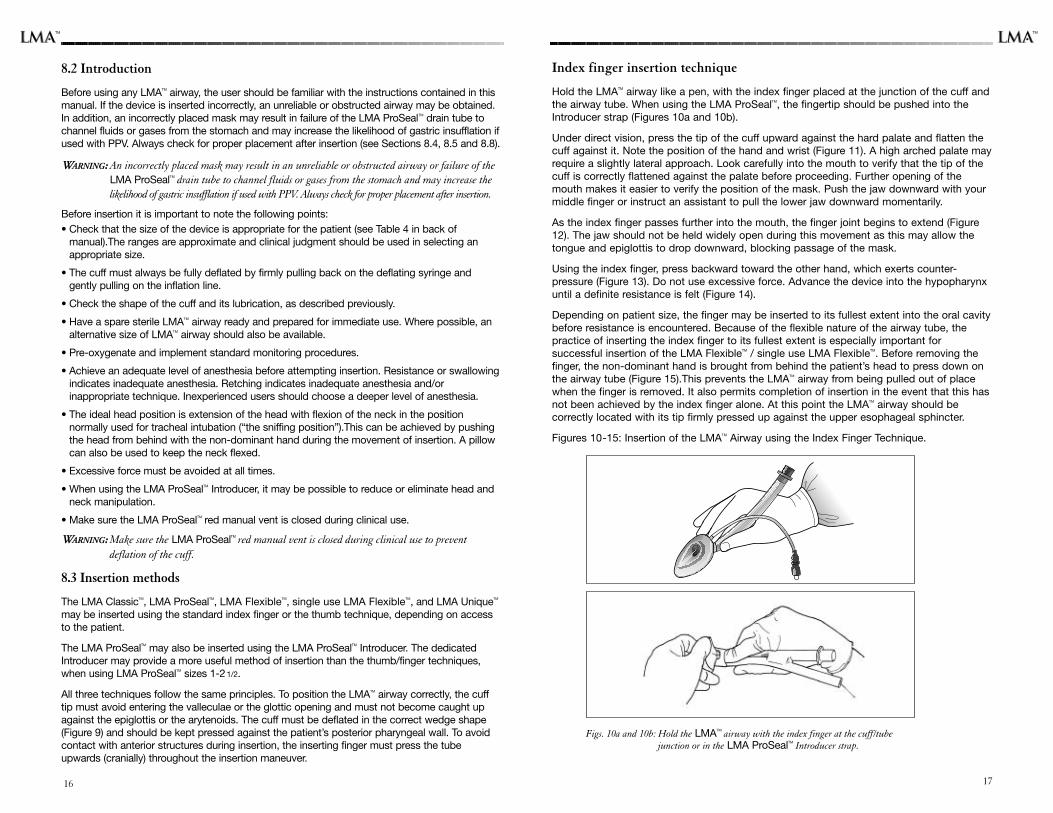
Index finger insertion technique
Hold the LMATM airway like a pen, with the index finger placed at the junction of the cuff andthe airway tube. When using the LMA ProSealTM, the fingertip should be pushed into theIntroducer strap (Figures 10a and 10b).
Under direct vision, press the tip of the cuff upward against the hard palate and flatten thecuff against it. Note the position of the hand and wrist (Figure 11). A high arched palate mayrequire a slightly lateral approach. Look carefully into the mouth to verify that the tip of thecuff is correctly flattened against the palate before proceeding. Further opening of themouth makes it easier to verify the position of the mask. Push the jaw downward with yourmiddle finger or instruct an assistant to pull the lower jaw downward momentarily.
As the index finger passes further into the mouth, the finger joint begins to extend (Figure12). The jaw should not be held widely open during this movement as this may allow thetongue and epiglottis to drop downward, blocking passage of the mask.
Using the index finger, press backward toward the other hand, which exerts counter-pressure (Figure 13). Do not use excessive force. Advance the device into the hypopharynxuntil a definite resistance is felt (Figure 14).
Depending on patient size, the finger may be inserted to its fullest extent into the oral cavitybefore resistance is encountered. Because of the flexible nature of the airway tube, thepractice of inserting the index finger to its fullest extent is especially important forsuccessful insertion of the LMA FlexibleTM / single use LMA FlexibleTM. Before removing thefinger, the non-dominant hand is brought from behind the patient’s head to press down onthe airway tube (Figure 15).This prevents the LMATM airway from being pulled out of placewhen the finger is removed. It also permits completion of insertion in the event that this hasnot been achieved by the index finger alone. At this point the LMATM airway should becorrectly located with its tip firmly pressed up against the upper esophageal sphincter.
Figures 10-15: Insertion of the LMATM Airway using the Index Finger Technique.
Figs. 10a and 10b: Hold the LMATM airway with the index finger at the cuff/tube junction or in the LMA ProSealTM Introducer strap.
16
TM TM
1918
Fig. 11: Press the mask up against the hardpalate. Note the flexed wrist
Fig. 12: Slide the mask inward, extendingthe index finger.
Fig. 13: Press the finger towards the other hand, which exerts counter-pressure.
Fig. 14: Advance the LMATM cuff into thehypopharynx until resistance is felt.
Fig. 15: Hold the outer end of the airwaytube while removing the indexfinger.
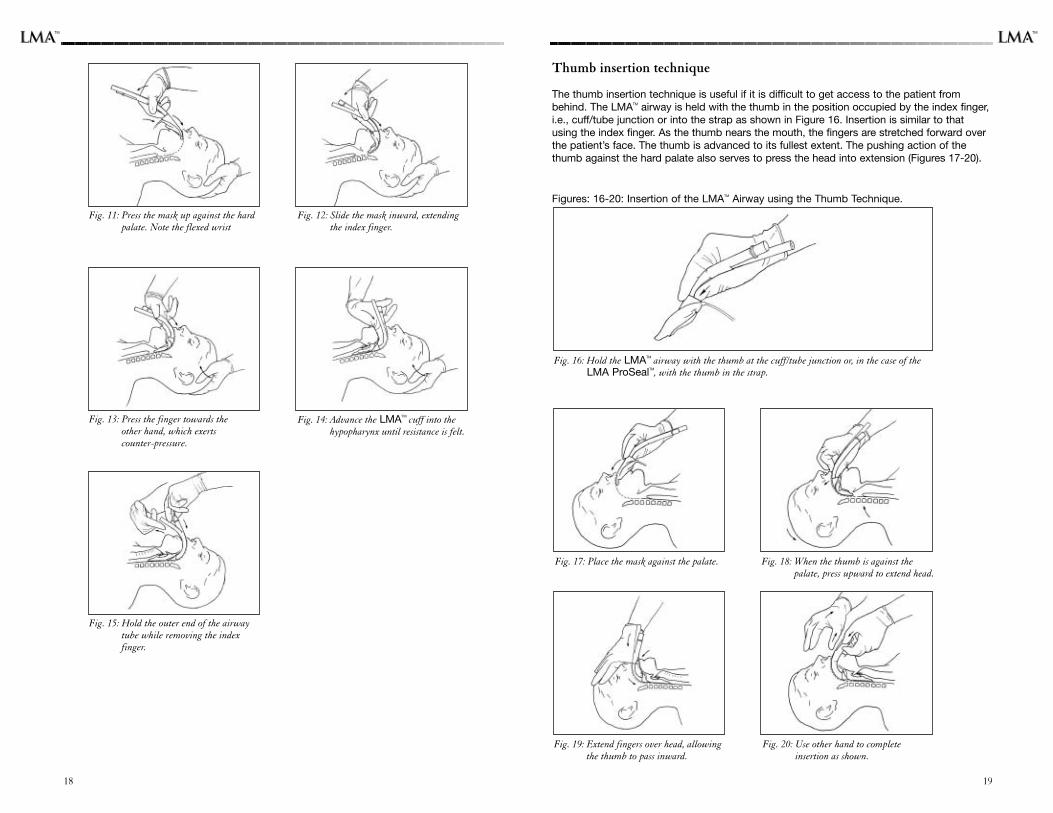
Thumb insertion technique
The thumb insertion technique is useful if it is difficult to get access to the patient frombehind. The LMATM airway is held with the thumb in the position occupied by the index finger,i.e., cuff/tube junction or into the strap as shown in Figure 16. Insertion is similar to thatusing the index finger. As the thumb nears the mouth, the fingers are stretched forward overthe patient’s face. The thumb is advanced to its fullest extent. The pushing action of thethumb against the hard palate also serves to press the head into extension (Figures 17-20).
Figures: 16-20: Insertion of the LMATM Airway using the Thumb Technique.
Fig. 16: Hold the LMATM airway with the thumb at the cuff/tube junction or, in the case of theLMA ProSealTM, with the thumb in the strap.
Fig. 17: Place the mask against the palate. Fig. 18: When the thumb is against thepalate, press upward to extend head.
Fig. 20: Use other hand to complete insertion as shown.
Fig. 19: Extend fingers over head, allowingthe thumb to pass inward.
TMTM
2120
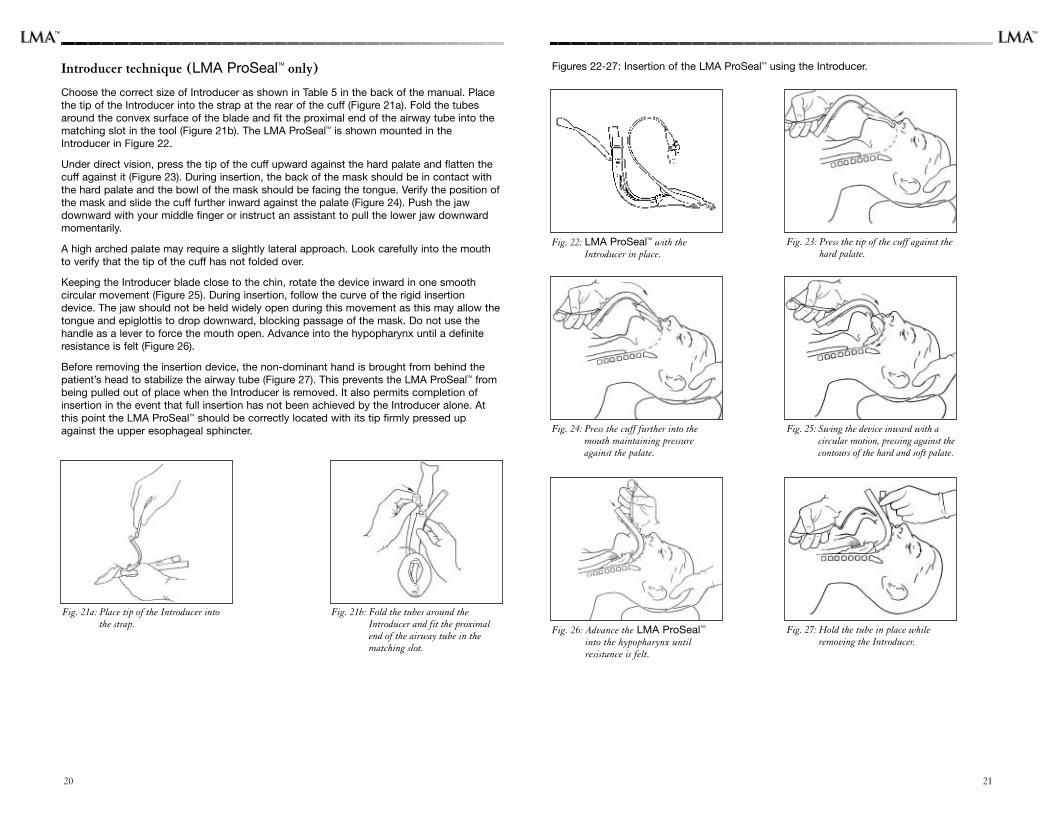
Introducer technique (LMA ProSealTM only)
Choose the correct size of Introducer as shown in Table 5 in the back of the manual. Placethe tip of the Introducer into the strap at the rear of the cuff (Figure 21a). Fold the tubesaround the convex surface of the blade and fit the proximal end of the airway tube into thematching slot in the tool (Figure 21b). The LMA ProSealTM is shown mounted in theIntroducer in Figure 22.
Under direct vision, press the tip of the cuff upward against the hard palate and flatten thecuff against it (Figure 23). During insertion, the back of the mask should be in contact withthe hard palate and the bowl of the mask should be facing the tongue. Verify the position ofthe mask and slide the cuff further inward against the palate (Figure 24). Push the jawdownward with your middle finger or instruct an assistant to pull the lower jaw downwardmomentarily.
A high arched palate may require a slightly lateral approach. Look carefully into the mouthto verify that the tip of the cuff has not folded over.
Keeping the Introducer blade close to the chin, rotate the device inward in one smoothcircular movement (Figure 25). During insertion, follow the curve of the rigid insertiondevice. The jaw should not be held widely open during this movement as this may allow thetongue and epiglottis to drop downward, blocking passage of the mask. Do not use thehandle as a lever to force the mouth open. Advance into the hypopharynx until a definiteresistance is felt (Figure 26).
Before removing the insertion device, the non-dominant hand is brought from behind thepatient’s head to stabilize the airway tube (Figure 27). This prevents the LMA ProSealTM frombeing pulled out of place when the Introducer is removed. It also permits completion ofinsertion in the event that full insertion has not been achieved by the Introducer alone. Atthis point the LMA ProSealTM should be correctly located with its tip firmly pressed upagainst the upper esophageal sphincter.
Fig. 21a: Place tip of the Introducer intothe strap.
Fig. 21b: Fold the tubes around theIntroducer and fit the proximalend of the airway tube in thematching slot.
Figures 22-27: Insertion of the LMA ProSealTM using the Introducer.
Fig. 23: Press the tip of the cuff against thehard palate.
Fig. 22: LMA ProSealTM with theIntroducer in place.
Fig. 25: Swing the device inward with acircular motion, pressing against thecontours of the hard and soft palate.
Fig. 24: Press the cuff further into themouth maintaining pressureagainst the palate.
Fig. 27: Hold the tube in place whileremoving the Introducer.
Fig. 26: Advance the LMA ProSealTM
into the hypopharynx until resistance is felt.
TM TM
8.4 Insertion problems
An inadequate depth of anesthesia may result in coughing and breathholding duringinsertion. If this occurs, anesthesia should be deepened immediately with inhalational orintravenous agents and manual ventilation instituted.
If the patient’s mouth cannot be opened sufficiently to insert the mask, first ensure that thepatient is adequately anesthetized. An assistant can be asked to pull the jaw downward. Thismaneuver makes it easier to see into the mouth and verify the position of the mask. However,do not maintain downward jaw traction once the mask has passed beyond the teeth.
The inserting finger must press the tube against the palate throughout the insertionmaneuver, otherwise the tip may fold on itself or impact on an irregularity or swelling in theposterior pharynx (e.g., hypertrophied tonsils). If the cuff fails to flatten or begins to curlover as it is advanced, it is necessary to withdraw the mask and reinsert it. In case oftonsillar obstruction, a diagonal shift of the mask is often successful.
If difficulty persists with the chosen technique, one of the other techniques described aboveshould be used.
WARNING: To avoid trauma, force should not be used at any time during insertion of an LMATM airway.
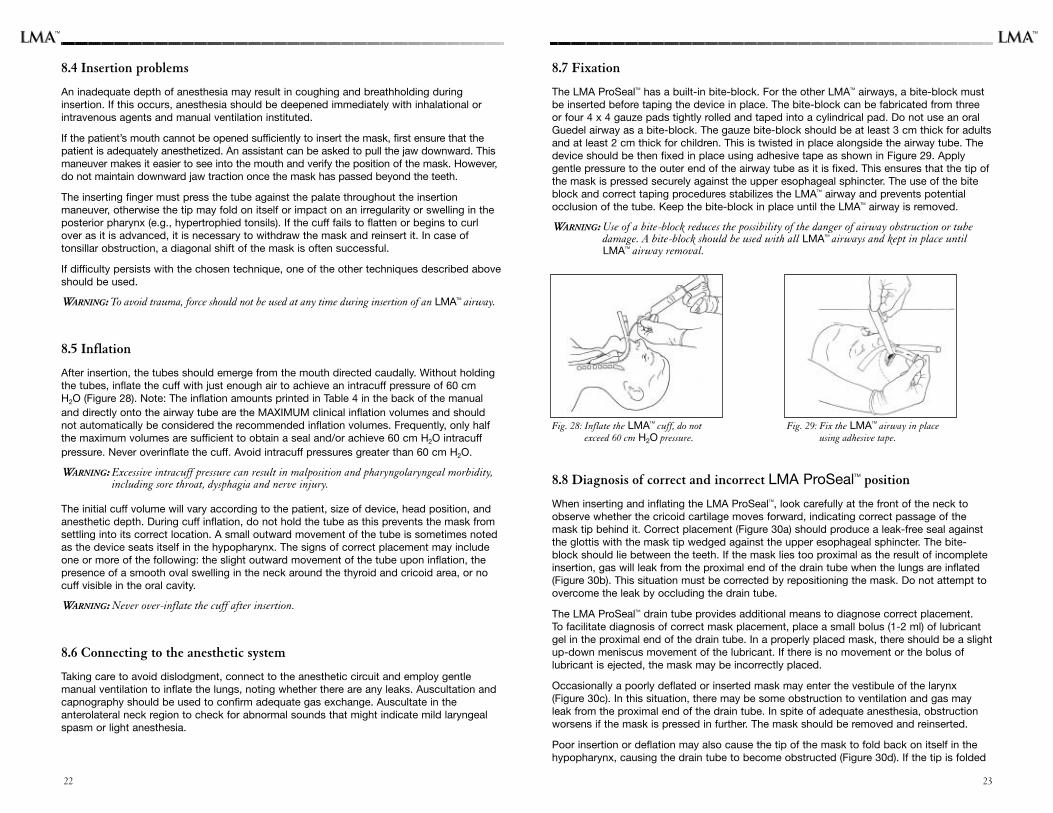
8.5 Inflation
After insertion, the tubes should emerge from the mouth directed caudally. Without holdingthe tubes, inflate the cuff with just enough air to achieve an intracuff pressure of 60 cm H2O (Figure 28). Note: The inflation amounts printed in Table 4 in the back of the manualand directly onto the airway tube are the MAXIMUM clinical inflation volumes and shouldnot automatically be considered the recommended inflation volumes. Frequently, only halfthe maximum volumes are sufficient to obtain a seal and/or achieve 60 cm H2O intracuffpressure. Never overinflate the cuff. Avoid intracuff pressures greater than 60 cm H2O.
WARNING: Excessive intracuff pressure can result in malposition and pharyngolaryngeal morbidity,including sore throat, dysphagia and nerve injury.
The initial cuff volume will vary according to the patient, size of device, head position, andanesthetic depth. During cuff inflation, do not hold the tube as this prevents the mask fromsettling into its correct location. A small outward movement of the tube is sometimes notedas the device seats itself in the hypopharynx. The signs of correct placement may includeone or more of the following: the slight outward movement of the tube upon inflation, thepresence of a smooth oval swelling in the neck around the thyroid and cricoid area, or nocuff visible in the oral cavity.
WARNING: Never over-inflate the cuff after insertion.
8.6 Connecting to the anesthetic system
Taking care to avoid dislodgment, connect to the anesthetic circuit and employ gentlemanual ventilation to inflate the lungs, noting whether there are any leaks. Auscultation andcapnography should be used to confirm adequate gas exchange. Auscultate in theanterolateral neck region to check for abnormal sounds that might indicate mild laryngealspasm or light anesthesia.
2322
8.7 Fixation
The LMA ProSealTM has a built-in bite-block. For the other LMATM airways, a bite-block mustbe inserted before taping the device in place. The bite-block can be fabricated from threeor four 4 x 4 gauze pads tightly rolled and taped into a cylindrical pad. Do not use an oralGuedel airway as a bite-block. The gauze bite-block should be at least 3 cm thick for adultsand at least 2 cm thick for children. This is twisted in place alongside the airway tube. Thedevice should be then fixed in place using adhesive tape as shown in Figure 29. Applygentle pressure to the outer end of the airway tube as it is fixed. This ensures that the tip ofthe mask is pressed securely against the upper esophageal sphincter. The use of the biteblock and correct taping procedures stabilizes the LMATM airway and prevents potentialocclusion of the tube. Keep the bite-block in place until the LMATM airway is removed.
WARNING: Use of a bite-block reduces the possibility of the danger of airway obstruction or tubedamage. A bite-block should be used with all LMATM airways and kept in place untilLMATM airway removal.
8.8 Diagnosis of correct and incorrect LMA ProSealTM position
When inserting and inflating the LMA ProSealTM, look carefully at the front of the neck toobserve whether the cricoid cartilage moves forward, indicating correct passage of themask tip behind it. Correct placement (Figure 30a) should produce a leak-free seal againstthe glottis with the mask tip wedged against the upper esophageal sphincter. The bite-block should lie between the teeth. If the mask lies too proximal as the result of incompleteinsertion, gas will leak from the proximal end of the drain tube when the lungs are inflated(Figure 30b). This situation must be corrected by repositioning the mask. Do not attempt toovercome the leak by occluding the drain tube.
The LMA ProSealTM drain tube provides additional means to diagnose correct placement. To facilitate diagnosis of correct mask placement, place a small bolus (1-2 ml) of lubricantgel in the proximal end of the drain tube. In a properly placed mask, there should be a slightup-down meniscus movement of the lubricant. If there is no movement or the bolus oflubricant is ejected, the mask may be incorrectly placed.
Occasionally a poorly deflated or inserted mask may enter the vestibule of the larynx(Figure 30c). In this situation, there may be some obstruction to ventilation and gas mayleak from the proximal end of the drain tube. In spite of adequate anesthesia, obstructionworsens if the mask is pressed in further. The mask should be removed and reinserted.
Poor insertion or deflation may also cause the tip of the mask to fold back on itself in thehypopharynx, causing the drain tube to become obstructed (Figure 30d). If the tip is folded
Fig. 29: Fix the LMATM airway in placeusing adhesive tape.
Fig. 28: Inflate the LMATM cuff, do notexceed 60 cm H2O pressure.
TMTM
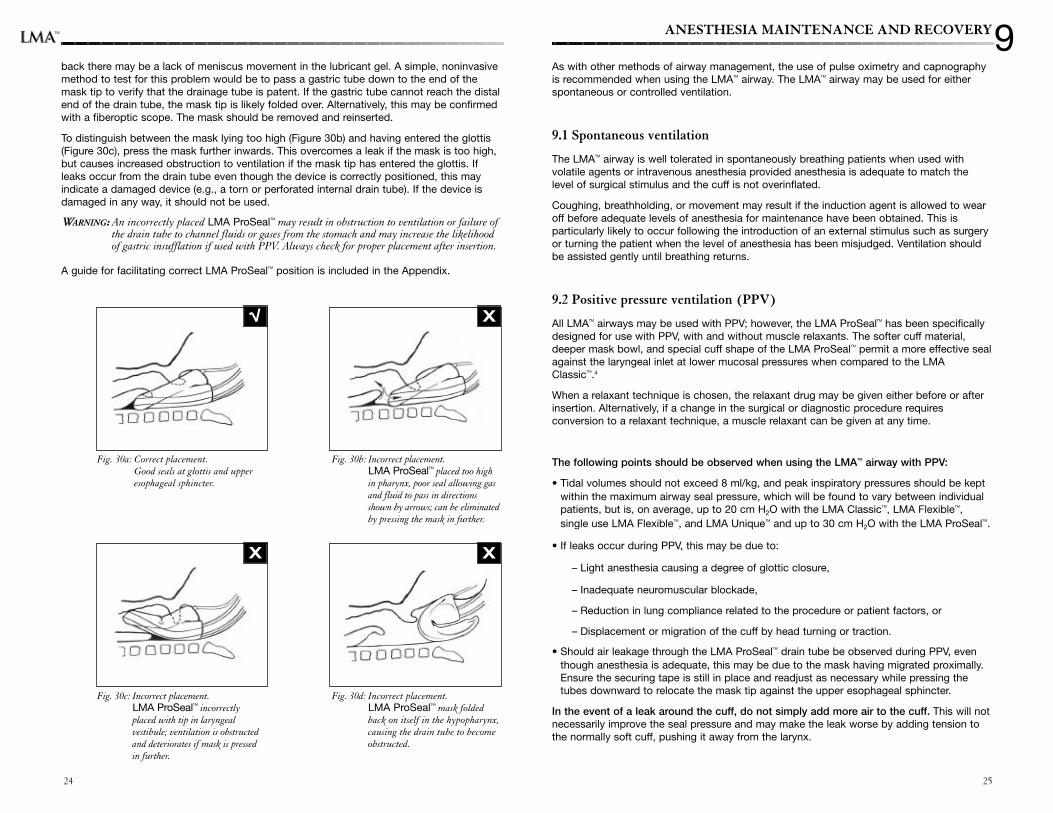
back there may be a lack of meniscus movement in the lubricant gel. A simple, noninvasivemethod to test for this problem would be to pass a gastric tube down to the end of themask tip to verify that the drainage tube is patent. If the gastric tube cannot reach the distalend of the drain tube, the mask tip is likely folded over. Alternatively, this may be confirmedwith a fiberoptic scope. The mask should be removed and reinserted.
To distinguish between the mask lying too high (Figure 30b) and having entered the glottis(Figure 30c), press the mask further inwards. This overcomes a leak if the mask is too high,but causes increased obstruction to ventilation if the mask tip has entered the glottis. Ifleaks occur from the drain tube even though the device is correctly positioned, this mayindicate a damaged device (e.g., a torn or perforated internal drain tube). If the device isdamaged in any way, it should not be used.
WARNING: An incorrectly placed LMA ProSealTM may result in obstruction to ventilation or failure ofthe drain tube to channel fluids or gases from the stomach and may increase the likelihoodof gastric insufflation if used with PPV. Always check for proper placement after insertion.
A guide for facilitating correct LMA ProSealTM position is included in the Appendix.
Fig. 30b: Incorrect placement. LMA ProSealTM placed too highin pharynx, poor seal allowing gasand fluid to pass in directionsshown by arrows; can be eliminatedby pressing the mask in further.
Fig. 30a: Correct placement. Good seals at glottis and upperesophageal sphincter.
Fig. 30c: Incorrect placement. LMA ProSealTM incorrectlyplaced with tip in laryngealvestibule; ventilation is obstructedand deteriorates if mask is pressedin further.
X
X X
Fig. 30d: Incorrect placement. LMA ProSealTM mask foldedback on itself in the hypopharynx,causing the drain tube to becomeobstructed.
2524
ANESTHESIA MAINTENANCE AND RECOVERY
As with other methods of airway management, the use of pulse oximetry and capnographyis recommended when using the LMATM airway. The LMATM airway may be used for eitherspontaneous or controlled ventilation.
9.1 Spontaneous ventilation
The LMATM airway is well tolerated in spontaneously breathing patients when used withvolatile agents or intravenous anesthesia provided anesthesia is adequate to match thelevel of surgical stimulus and the cuff is not overinflated.
Coughing, breathholding, or movement may result if the induction agent is allowed to wearoff before adequate levels of anesthesia for maintenance have been obtained. This isparticularly likely to occur following the introduction of an external stimulus such as surgeryor turning the patient when the level of anesthesia has been misjudged. Ventilation shouldbe assisted gently until breathing returns.
9.2 Positive pressure ventilation (PPV)
All LMATM airways may be used with PPV; however, the LMA ProSealTM has been specificallydesigned for use with PPV, with and without muscle relaxants. The softer cuff material,deeper mask bowl, and special cuff shape of the LMA ProSealTM permit a more effective sealagainst the laryngeal inlet at lower mucosal pressures when compared to the LMAClassicTM.4
When a relaxant technique is chosen, the relaxant drug may be given either before or afterinsertion. Alternatively, if a change in the surgical or diagnostic procedure requiresconversion to a relaxant technique, a muscle relaxant can be given at any time.
The following points should be observed when using the LMATM airway with PPV:
• Tidal volumes should not exceed 8 ml/kg, and peak inspiratory pressures should be keptwithin the maximum airway seal pressure, which will be found to vary between individualpatients, but is, on average, up to 20 cm H2O with the LMA ClassicTM, LMA FlexibleTM,single use LMA FlexibleTM, and LMA UniqueTM and up to 30 cm H2O with the LMA ProSealTM.
• If leaks occur during PPV, this may be due to:
– Light anesthesia causing a degree of glottic closure,
– Inadequate neuromuscular blockade,
– Reduction in lung compliance related to the procedure or patient factors, or
– Displacement or migration of the cuff by head turning or traction.
• Should air leakage through the LMA ProSealTM drain tube be observed during PPV, eventhough anesthesia is adequate, this may be due to the mask having migrated proximally.Ensure the securing tape is still in place and readjust as necessary while pressing thetubes downward to relocate the mask tip against the upper esophageal sphincter.
In the event of a leak around the cuff, do not simply add more air to the cuff. This will notnecessarily improve the seal pressure and may make the leak worse by adding tension tothe normally soft cuff, pushing it away from the larynx.
9TM
27
9.3 Potential problems after insertion
Inadequate level of anesthesia
The most common problem following insertion is failure to maintain an adequate level ofanesthesia. Administer an additional bolus of induction agent and/or increase theconcentration of volatile agent, while gently assisting ventilation.
Nitrous oxide diffusion
Nitrous oxide diffuses into the silicone cuff causing a rise in intracuff pressure. Studies haveshown that use of nitrous oxide can increase reusable LMATM airway cuff pressure by asmuch as 1 mm Hg per minute. The LMA UniqueTM and single use LMA FlexibleTM PVC cuffsare much more resistant to nitrous oxide diffusion.
Diffusion rate and resulting peak pressure may vary with the initial volume of air injectedinto the cuff, the type of gases used to inflate the cuff, the percentage of nitrous oxide inthe inhaled mixture, and the size of the device.
The incidence of post-operative sore throat may increase if intracuff pressure becomesexcessive. To reduce the risk of a sore throat or possible neurovascular injury, the cuffpressure should be periodically checked and gas intermittently withdrawn to maintain 60cm H2O intracuff pressure or the minimal “just seal” pressure.
This can be achieved in several different ways. First, a pressure monitor or pressure transducermay be used. Pressure manometers are commercially available from Posey, Mallinckrodt,Portex, and VBM-Medical. Secondly, simply feeling the inflation indicator balloon can beperformed. At intracuff pressure of 60 cm H2O, the inflation balloon should feel very compliant.If the inflation indicator balloon becomes stiff or olive-shaped, this indicates excessivepressure. Finally, gas can be withdrawn until there is a slight leak, and then 1-2 ml added.
WARNING: Excessive intracuff pressure can result in malposition and pharyngolaryngeal morbidity,including sore throat, dysphagia and nerve injury.
Poor airway seal/Air leak
Should signs of a poor airway seal or air leak occur at the beginning or during a case, oneor more of the following measures may be taken:
• Verify the depth of anesthesia is adequate and deepen if necessary.
• Check cuff pressures at start and periodically during a case, especially if using nitrous oxide.
• Ensure intracuff pressures are not >60 cm H2O; reduce intracuff pressure, if necessary,while maintaining an adequate seal.
• If the mask is seated too high in the pharynx, then press in further to confirm contact withthe upper esophageal sphincter.
• Ensure proper fixation by applying palatal pressure while taping in place.
• Always confirm cuff integrity prior to placement.
Malposition of the LMATM airway
In general, malposition of the LMATM airway can be assessed by capnography or by observationof changes in tidal volume, e.g., a reduced expired tidal volume. If malposition is suspected,check whether there is a smooth, oval neck swelling extending below the thyroid cartilage. Ifabsent, it may indicate anterior misplacement of the mask tip into the laryngeal inlet, particularlyif there is an unusually prolonged expiratory phase. If malposition is suspected, the LMATM
airway may be removed and reinserted once anesthetic depth is adequate for reinsertion.
Specific malpositions of the LMA ProSealTM were discussed in Section 8.8. In addition,migration/rotation of the LMA ProSealTM during use may occur due to overinflation of the cuff, aherniated cuff and/or accidental displacement. Check cuff pressure at the start and periodicallyduring a case, verify cuff integrity prior to use and ensure proper fixation. If the LMA ProSealTM
pops out of the mouth during insertion, the mask may be incorrectly positioned with the distaltip folded backward in the pharynx. Remove and reinsert or digitally sweep behind the tip.
Unexpected regurgitation
Even in fasted patients, regurgitation may occur for a variety of reasons (for example, ifanesthesia becomes inadequate), resulting in fluid emerging from the LMATM airway tube or the LMA ProSealTM drain tube. It has been shown in cadavers that fluids pass up the LMA ProSealTM
drain tube without laryngeal contamination when the mask has been correctly placed.9
If regurgitation occurs, provided that oxygen saturation remains at acceptable levels, theLMATM airway should not be removed. The patient should immediately be tilted head down.Momentarily disconnect the anesthetic circuit so that gastric contents are not forced into thelungs. Verify that anesthetic depth is adequate and deepen anesthesia intravenously, ifappropriate. Reposition the device to ensure the distal end is lying against the upperesophageal sphincter and secure it in place using the fixation method described earlier.
Suction should then be applied through the airway tube. Suction of the tracheobronchialtree using a fiberoptic bronchoscope through the airway tube may be employed if theairway reflexes are adequately obtunded.
If clinically indicated, commence preparation for immediate tracheal intubation of thepatient. If aspiration has occurred, the patient should receive a chest X-ray and be treated,as clinically appropriate, with antibiotics, physiotherapy, and tracheal suction.
A gastric tube may be inserted behind the LMATM airway or through the LMA ProSealTM draintube to complete drainage if the presence of further gastric contents is suspected.
Airway obstruction with the LMA ProSealTM
There have been reports of airway obstruction occurring with the LMA ProSealTM airway.10,11,12
Some of the reports were associated with noisy respiration and negative pressure, causingair to be drawn into the esophagus with inspiration. Other clinicians have reported anincreased incidence of stridor with the LMA ProSealTM airway. One proposed mechanism ofthe airway obstruction is pressure from the distal mask causing narrowing of the glottic inletand subsequent mechanical closure of the vocal cords. Another mechanism is folding of thecuff wall medially, causing a physical airway obstruction.
Should the patient show signs of airway obstruction, one or more of the following measuresmay be taken:
• Verify the depth of anesthesia is adequate and deepen if necessary.
• Ensure intracuff pressures are not >60 cm H2O; reduce intracuff pressure, if necessary,while maintaining an adequate seal.
• If the patient is spontaneously breathing, provide expiratory PEEP up to a clinically safelevel or use PPV.
• Try placing the patient’s head and neck in a sniffing position.
26
TMTM
2928
• Consider fiberoptic examination to evaluate cuff position and vocal cord function.
• If all else fails, remove and reinsert.
• If appropriate, consider insertion of a smaller sized LMA ProSealTM airway.
WARNING: If airway problems persist or ventilation is inadequate, the LMATM airway should beremoved and an airway established by some other means.
9.4 Emergence from anesthesia and removal
If applicable, reverse the neuromuscular block or allow the block to wear off beforeswitching off the anesthetic agents at the end of the surgical or diagnostic procedure. Withgentle assisted ventilation, the patient should be allowed to start breathing spontaneously.At this stage it is advisable to check the intracuff pressure.
The correctly placed LMATM airway is well tolerated until the return of protective reflexes,provided that intracuff pressures are kept around 60 cm H2O.This means that a clear airwaycan be maintained until the patient is able to swallow and cough effectively. Removalshould always be carried out in an area where suction equipment and the space for rapidtracheal intubation are present. The following procedure should be followed:
• Patient monitoring should continue throughout the recovery stage. Oxygen should becontinuously administered through the anesthetic circuit or via a T-piece. If suction isrequired around the oral cavity or down the airway tube, it should be carried out prior torecovery of reflexes.
• Leave the patient undisturbed until reflexes are restored, except to administer oxygen andperform monitoring procedures. It is not advisable to move the patient from the supine tothe lateral recumbent position unless there is urgent reason to do so, such asregurgitation or vomiting. If the patient needs to be awakened in the lateral position, thepatient must be turned in this position under adequate anesthesia.
• Avoid suctioning the airway tube with the LMATM airway in place. The inflated cuff protectsthe larynx from oral secretions and suctioning is not likely to be required. Suctioning andphysical stimulation may provoke laryngeal spasm if anesthesia is light.
• Watch for signs of swallowing. It is usually safe and convenient to remove adhesive tapewhen swallowing begins. However, the interval between the beginning of swallowing andthe ability to open the mouth varies from patient to patient according to the length andtype of anesthesia.
• Deflate the cuff and simultaneously remove the device only when the patient can open themouth on command. If the cuff is deflated before the return of effective swallowing andcough reflexes, secretions in the upper pharynx may enter the larynx, provoking coughingor laryngeal spasm. Verify airway patency and respiratory depth. Oral suctioning may nowbe performed, if required.
If the LMATM airway is to be removed in a Post-Anesthesia Care Unit (PACU), recovery roomstaff should receive training in all aspects of LMATM airway management. An anesthesiologistshould always be readily available if the device is to be removed away from the operating room.
10SPECIALIZED USES
10.1 Pediatric use
The smaller LMATM airway sizes have been shown to function effectively in children despitethe differences between the adult and the infant larynx. It is recommended that LMATM
airway use in neonates and small children be performed by anesthesiologists familiar withpediatric patients and already experienced in adult LMATM airway anesthesia.
Table 4 provides basic guidelines for sizing. In children at the transition weights, substitutionof one size for another may be necessary.
LMATM airway insertion in children is carried out in the same way as described for adultsfollowing either intravenous or gaseous induction, provided an adequate depth ofanesthesia is achieved. Insertion should be successful at the same plane of anesthesia thatwould be suitable for tracheal intubation. The incidence of airway problems in children withthe LMATM airway seems to follow the same trend as in adults. However, as with any form ofanesthesia and airway management in infants and children where ventilation is inadequate,desaturation is likely to occur faster due to their higher oxygen consumption.13
LMATM airway anesthesia in children and infants is associated with maintenance of higheroxygen saturation compared to a face mask and Guedel airway14 and the ability to coughand cry while waking up. The LMATM airway is suitable for many short pediatric ambulatorysurgical or diagnostic procedures and those where access to the head and neck wouldotherwise be limited by the use of a face mask.14
10.2 Gastric drainage with the LMATM airwayWARNING: Should the LMATM airway be used in a fasted patient who is at risk of retained gastric
contents, prophylactic measures to empty the stomach contents and appropriate antacidtherapy should be employed. Examples of conditions where fasted patients may be at risk ofretained gastric contents include, but are not limited to: hiatal hernia and moderate obesity.
10.2.1 LMA ClassicTM, LMA UniqueTM, LMA FlexibleTM and single use LMA FlexibleTM
Gastric drainage through a gastric tube is compatible with the LMATM airway and does notinterfere with its seal against the larynx. The gastric tube is best passed before LMATM
airway insertion, but it is possible to pass it during anesthesia, if necessary, by slightdeflation of the LMATM airway cuff. A Magill’s forceps may be used to push the tip downbehind the mask. The insertion of a gastric tube does not guarantee that the stomach canbe drained completely.
WARNING: The presence of a gastric tube does not rule out regurgitation and may even makeregurgitation more likely because the tube may make the lower esophagealsphincter incompetent.
10.2.2 LMA ProSealTM
In addition to its diagnostic function (see Section 8.8), the LMA ProSealTM drain tube facilitateschanneling of fluids and gases out of the patient and/or the insertion of standard gastric(nasogastric or orogastric) tubes into the stomach at any time during the anesthetic procedure(Figure 31). Refer to Table 5 in the back of the manual for maximum gastric tube sizes.
WARNING: Do not attempt to pass a gastric tube through the drain tube in the presence of known orsuspected esophageal damage.
TM
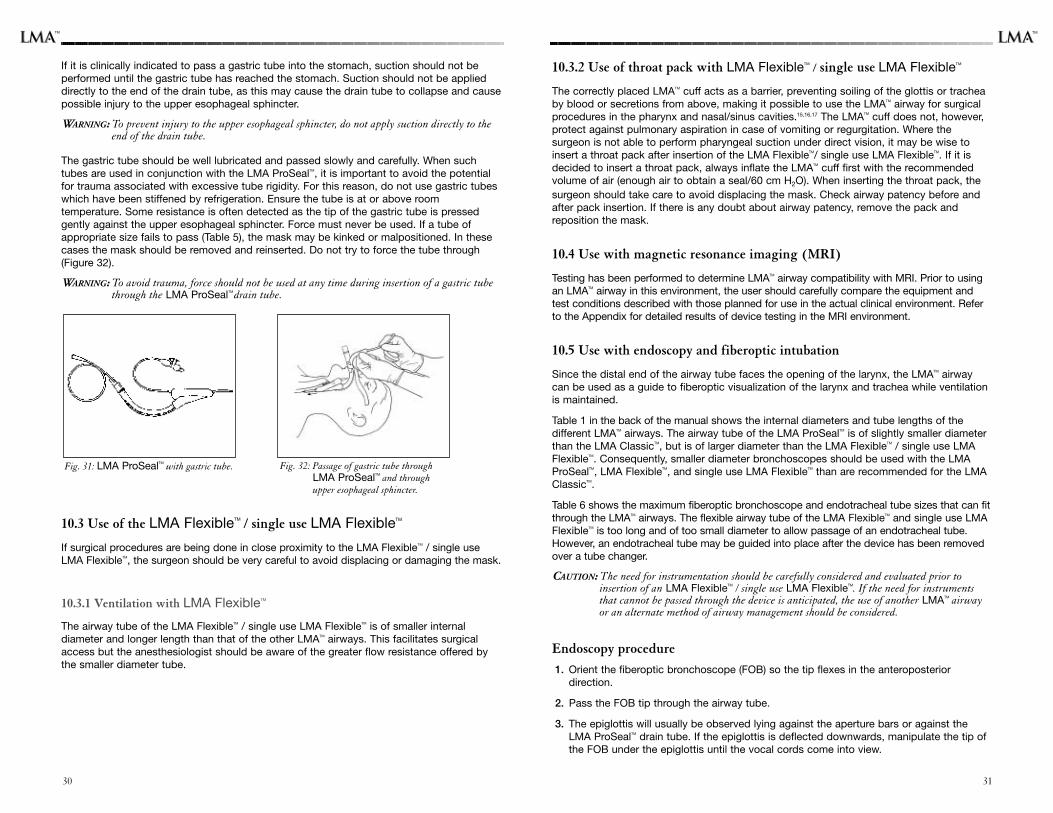
30
If it is clinically indicated to pass a gastric tube into the stomach, suction should not beperformed until the gastric tube has reached the stomach. Suction should not be applieddirectly to the end of the drain tube, as this may cause the drain tube to collapse and causepossible injury to the upper esophageal sphincter.
WARNING: To prevent injury to the upper esophageal sphincter, do not apply suction directly to theend of the drain tube.
The gastric tube should be well lubricated and passed slowly and carefully. When suchtubes are used in conjunction with the LMA ProSealTM, it is important to avoid the potentialfor trauma associated with excessive tube rigidity. For this reason, do not use gastric tubeswhich have been stiffened by refrigeration. Ensure the tube is at or above roomtemperature. Some resistance is often detected as the tip of the gastric tube is pressedgently against the upper esophageal sphincter. Force must never be used. If a tube ofappropriate size fails to pass (Table 5), the mask may be kinked or malpositioned. In thesecases the mask should be removed and reinserted. Do not try to force the tube through(Figure 32).
WARNING: To avoid trauma, force should not be used at any time during insertion of a gastric tubethrough the LMA ProSealTM drain tube.
10.3 Use of the LMA FlexibleTM / single use LMA FlexibleTM
If surgical procedures are being done in close proximity to the LMA FlexibleTM / single useLMA FlexibleTM, the surgeon should be very careful to avoid displacing or damaging the mask.
10.3.1 Ventilation with LMA FlexibleTM
The airway tube of the LMA FlexibleTM / single use LMA FlexibleTM is of smaller internaldiameter and longer length than that of the other LMATM airways. This facilitates surgicalaccess but the anesthesiologist should be aware of the greater flow resistance offered bythe smaller diameter tube.
Fig. 32: Passage of gastric tube throughLMA ProSealTM and throughupper esophageal sphincter.
Fig. 31: LMA ProSealTM with gastric tube.
10.3.2 Use of throat pack with LMA FlexibleTM
/ single use LMA FlexibleTM
The correctly placed LMATM cuff acts as a barrier, preventing soiling of the glottis or tracheaby blood or secretions from above, making it possible to use the LMATM airway for surgicalprocedures in the pharynx and nasal/sinus cavities.15,16,17 The LMATM cuff does not, however,protect against pulmonary aspiration in case of vomiting or regurgitation. Where thesurgeon is not able to perform pharyngeal suction under direct vision, it may be wise toinsert a throat pack after insertion of the LMA FlexibleTM/ single use LMA FlexibleTM. If it isdecided to insert a throat pack, always inflate the LMATM cuff first with the recommendedvolume of air (enough air to obtain a seal/60 cm H2O). When inserting the throat pack, thesurgeon should take care to avoid displacing the mask. Check airway patency before andafter pack insertion. If there is any doubt about airway patency, remove the pack andreposition the mask.
10.4 Use with magnetic resonance imaging (MRI)
Testing has been performed to determine LMATM airway compatibility with MRI. Prior to usingan LMATM airway in this environment, the user should carefully compare the equipment andtest conditions described with those planned for use in the actual clinical environment. Referto the Appendix for detailed results of device testing in the MRI environment.
10.5 Use with endoscopy and fiberoptic intubation
Since the distal end of the airway tube faces the opening of the larynx, the LMATM airwaycan be used as a guide to fiberoptic visualization of the larynx and trachea while ventilationis maintained.
Table 1 in the back of the manual shows the internal diameters and tube lengths of thedifferent LMATM airways. The airway tube of the LMA ProSealTM is of slightly smaller diameterthan the LMA ClassicTM, but is of larger diameter than the LMA FlexibleTM / single use LMAFlexibleTM. Consequently, smaller diameter bronchoscopes should be used with the LMAProSealTM, LMA FlexibleTM, and single use LMA FlexibleTM than are recommended for the LMAClassicTM.
Table 6 shows the maximum fiberoptic bronchoscope and endotracheal tube sizes that can fitthrough the LMATM airways. The flexible airway tube of the LMA FlexibleTM and single use LMAFlexibleTM is too long and of too small diameter to allow passage of an endotracheal tube.However, an endotracheal tube may be guided into place after the device has been removedover a tube changer.
CAUTION: The need for instrumentation should be carefully considered and evaluated prior toinsertion of an LMA FlexibleTM / single use LMA FlexibleTM. If the need for instrumentsthat cannot be passed through the device is anticipated, the use of another LMATM airwayor an alternate method of airway management should be considered.
Endoscopy procedure
1. Orient the fiberoptic bronchoscope (FOB) so the tip flexes in the anteroposterior direction.
2. Pass the FOB tip through the airway tube.
3. The epiglottis will usually be observed lying against the aperture bars or against theLMA ProSealTM drain tube. If the epiglottis is deflected downwards, manipulate the tip ofthe FOB under the epiglottis until the vocal cords come into view.
31
TMTM
3332
Fiberoptic Intubation
4. If intubation through the LMATM airway is planned, a well-lubricated, fully deflated endotracheal tube (ETT) can be threaded over the FOB.
Alternatively, an ETT with a resealing adaptor may be inserted through the LMATM airway untilthe tip just protrudes through the central aperture slot prior to insertion in the patient.
Table 6 in the back of the manual provides guidance for selecting the appropriate size ETTand FOB for use with each LMATM airway. The compatibility of the ETT and its adaptor shouldbe tested before insertion, since the outside diameter of endotracheal tubes may vary.
5. Administer oxygen throughout the intubation procedure and monitor the adequacy ofventilation by capnography and pulse oximetry.
6. Once the cords are visualized, pass the tip of the FOB into the trachea.
7. Thread the ETT downwards into the trachea over the FOB.
8. Inflate the ETT cuff and ventilate to check for correct position by auscultation and capnography.
9. Leave the LMATM airway in place with the cuff slightly deflated.
10. Remove the LMATM airway when protective reflexes have returned.
11. If a larger ETT is needed, remove the LMATM airway and ETT over a tube changer andguide a larger ETT into place.
Using a slightly longer endotracheal tube may be helpful in fiberoptic intubation through theLMATM airway in large patients. The microlaryngeal tracheal tube (Mallinckrodt, St. Louis,MO; Rüsch Inc., Duluth, GA) or nasal RAE® tube (Mallinckrodt) offer increased length,which allows the cuff of the ETT to be positioned below the vocal cords in large patients.
10.6 Blind tracheal intubation through the LMATM airway
In general, use of the LMA FastrachTM is recommended when blind intubation is anticipated.The success rate of direct blind intubation through the LMA ClassicTM airway is highly variable(20-100%)5 depending on clinician experience, technique, number of attempts, patientanatomy, and available equipment. There are currently no published data on blind intubationthrough the LMA ProSealTM. There is one published study of blind intubation by paramedicsthrough the LMA Unique™ in a mannequin. The successful blind intubation rate was 21%.18
The ET tube is inserted into the LMA ClassicTM or LMA Unique TM airway tube with a slightrotation to the left so the bevel will not catch on the right hand aperture bar. Flexion of thehead may help prevent the tube tip from catching on the walls of the larynx anteriorly.Listening down the tube or using capnography may help guide the ET tube into the trachea.If the ET tube passes into the esophagus, slight manipulation of the ET tube or the LMATM
airway may help align the glottic opening and the LMATM aperture more accurately.
REFERENCES
1. Brain AIJ. The laryngeal mask — a new concept in airway management. Br J Anaesth1983;55:801-804.
2. Brain AIJ, Verghese C, Strube PJ. The ‘LMA ProSeal’ — a laryngeal mask with anoesophageal vent. Br J Anaesth 2000;84:650-4.
3 Brimacombe J, Keller C. The ProSeal laryngeal mask airway. A randomized crossoverstudy with the standard laryngeal mask airway in paralyzed, anesthetized patients.Anesthesiology 2000;93:104-109.
4. Keller C, Brimacombe J. Mucosal pressure and oropharyngeal leak pressure with theProSeal versus the Classic laryngeal mask airway. Br J Anaesth 2000;85:262-6.
5. Brimacombe JR. Laryngeal mask anesthesia. Principles and practice. Saunders 2005.
6. ANSI/AAMI ST46-1993 and ST36-1992. In AAMI Standards and RecommendedPractices. Association for the Advancement of Medical Instrumentation: Arlington,Virginia, 1995.
7. WHO Infection Control Guidelines for Transmissible Spongiform Encephalopathies,Report of a WHO Consultation: Geneva, Switzerland, 23-26, March 1999.
8. Weber D, Rutala W. Managing the risk of nosocomial transmission of prion disease.Current Opinion in Infectious Diseases 2002;15:421-425.
9. Keller C, Brimacombe J, Kleinsasser A, Loeckinger A. Does the ProSeal laryngeal maskprevent aspiration of regurgitated fluid? Anesth Analg 2000;91:1017-20.
10. Stix MS, Rodriguez – Sallaberry FE, Cameron EM, Teaque D, O’Connor CJ. Esophagealaspiration of air through the drain tube of the ProSealTM laryngeal mask. Anesth Analg2001;93:1354-7.
11. Brain AIJ. Esophageal breathing and upper airway obstruction with the ProSealTM
laryngeal mask. Anesth Analg 2002;94:1669.
12. Brimacombe J, Richardson C, Keller C, Donald S. Mechanical closure of the vocal cordswith the laryngeal mask airway ProSealTM. Br J Anaesth 2002; 88:296-7.
13. Watcha MF, Garner FT, White PF, Lusk R. Laryngeal mask airway vs. face mask andGuedel airway during pediatric myringotomy. Archives of Otolaryngeal/Head and NeckSurgery 1994;120:877-880.
14. Mason DG, Bingham RM. The laryngeal mask airway in children. Anaesthesia1990;45:760-763.
15. John RE, Hill S, Hughes TJ. Airway protection by the laryngeal mask. A barrier to dyeplaced in the pharynx. Anaesthesia 1991;46:366-367.
16. Williams RJ, Bailey PM. Comparison of the reinforced laryngeal mask and trachealintubation for adenotonsillectomy. Br J Anaesth 1993;70:30-33.
17. Ahmed MZ, Vohra A. The reinforced laryngeal mask airway (RLMA) protects the airway inpatients undergoing nasal surgery – an observation study of 200 patients. Can J Anesth2002;49:863-866.
18. Barnes DR, Reed DB, Weinstein G, Brown LH. Blind tracheal intubation by paramedicsthrough the LMA-Unique. Prehospital Emergency Care 2003;7:470-473.
11TM
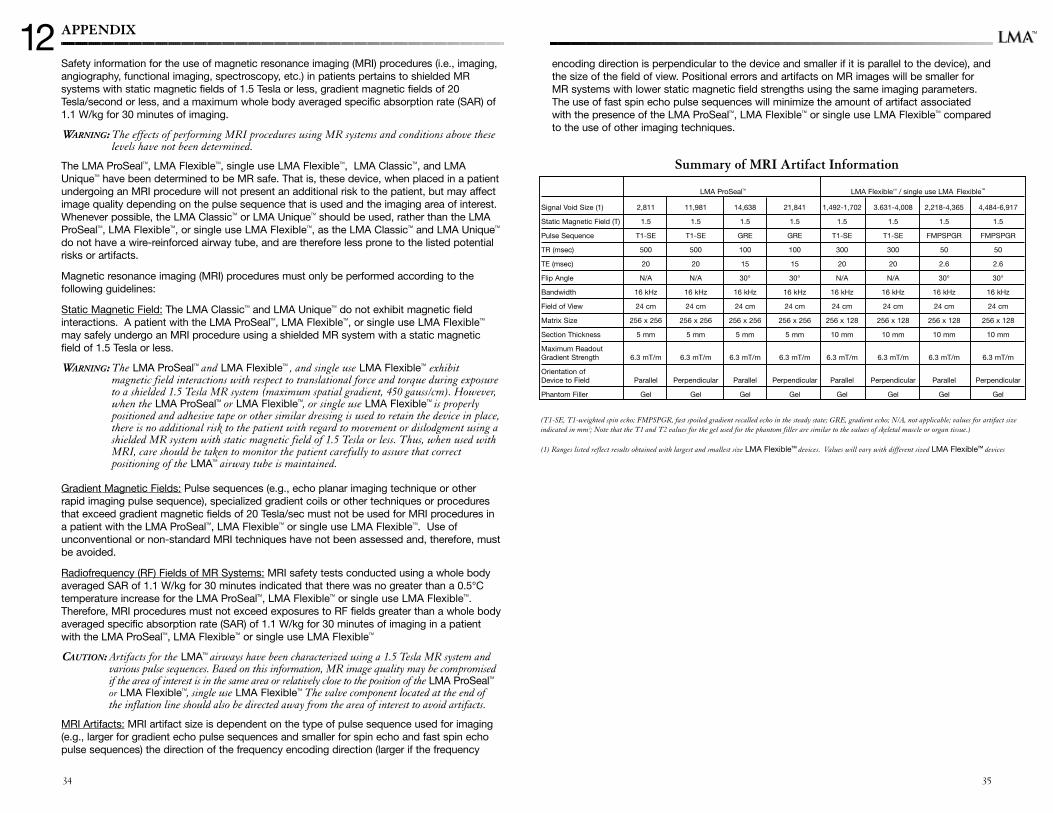
APPENDIX
Safety information for the use of magnetic resonance imaging (MRI) procedures (i.e., imaging,angiography, functional imaging, spectroscopy, etc.) in patients pertains to shielded MRsystems with static magnetic fields of 1.5 Tesla or less, gradient magnetic fields of 20Tesla/second or less, and a maximum whole body averaged specific absorption rate (SAR) of1.1 W/kg for 30 minutes of imaging.
WARNING: The effects of performing MRI procedures using MR systems and conditions above theselevels have not been determined.
The LMA ProSealTM, LMA FlexibleTM, single use LMA FlexibleTM, LMA ClassicTM, and LMAUniqueTM have been determined to be MR safe. That is, these device, when placed in a patientundergoing an MRI procedure will not present an additional risk to the patient, but may affectimage quality depending on the pulse sequence that is used and the imaging area of interest.Whenever possible, the LMA ClassicTM or LMA UniqueTM should be used, rather than the LMAProSealTM, LMA FlexibleTM, or single use LMA FlexibleTM, as the LMA ClassicTM and LMA UniqueTM
do not have a wire-reinforced airway tube, and are therefore less prone to the listed potentialrisks or artifacts.
Magnetic resonance imaging (MRI) procedures must only be performed according to thefollowing guidelines:
Static Magnetic Field: The LMA ClassicTM and LMA UniqueTM do not exhibit magnetic fieldinteractions. A patient with the LMA ProSealTM, LMA FlexibleTM, or single use LMA FlexibleTM
may safely undergo an MRI procedure using a shielded MR system with a static magneticfield of 1.5 Tesla or less.
WARNING: The LMA ProSealTM and LMA FlexibleTM , and single use LMA FlexibleTM exhibitmagnetic field interactions with respect to translational force and torque during exposureto a shielded 1.5 Tesla MR system (maximum spatial gradient, 450 gauss/cm). However,when the LMA ProSealTM or LMA FlexibleTM, or single use LMA FlexibleTM is properlypositioned and adhesive tape or other similar dressing is used to retain the device in place,there is no additional risk to the patient with regard to movement or dislodgment using ashielded MR system with static magnetic field of 1.5 Tesla or less. Thus, when used withMRI, care should be taken to monitor the patient carefully to assure that correctpositioning of the LMATM airway tube is maintained.
Gradient Magnetic Fields: Pulse sequences (e.g., echo planar imaging technique or otherrapid imaging pulse sequence), specialized gradient coils or other techniques or proceduresthat exceed gradient magnetic fields of 20 Tesla/sec must not be used for MRI procedures ina patient with the LMA ProSealTM, LMA FlexibleTM or single use LMA FlexibleTM. Use ofunconventional or non-standard MRI techniques have not been assessed and, therefore, mustbe avoided.
Radiofrequency (RF) Fields of MR Systems: MRI safety tests conducted using a whole bodyaveraged SAR of 1.1 W/kg for 30 minutes indicated that there was no greater than a 0.5°Ctemperature increase for the LMA ProSealTM, LMA FlexibleTM or single use LMA FlexibleTM.Therefore, MRI procedures must not exceed exposures to RF fields greater than a whole bodyaveraged specific absorption rate (SAR) of 1.1 W/kg for 30 minutes of imaging in a patientwith the LMA ProSealTM, LMA FlexibleTM or single use LMA FlexibleTM
CAUTION: Artifacts for the LMATM airways have been characterized using a 1.5 Tesla MR system andvarious pulse sequences. Based on this information, MR image quality may be compromisedif the area of interest is in the same area or relatively close to the position of the LMA ProSealTM
or LMA FlexibleTM, single use LMA FlexibleTM The valve component located at the end ofthe inflation line should also be directed away from the area of interest to avoid artifacts.
MRI Artifacts: MRI artifact size is dependent on the type of pulse sequence used for imaging(e.g., larger for gradient echo pulse sequences and smaller for spin echo and fast spin echopulse sequences) the direction of the frequency encoding direction (larger if the frequency
12
3534
encoding direction is perpendicular to the device and smaller if it is parallel to the device), andthe size of the field of view. Positional errors and artifacts on MR images will be smaller forMR systems with lower static magnetic field strengths using the same imaging parameters.The use of fast spin echo pulse sequences will minimize the amount of artifact associatedwith the presence of the LMA ProSealTM, LMA FlexibleTM or single use LMA FlexibleTM comparedto the use of other imaging techniques.
LMA ProSealTM LMA FlexibleTM / single use LMA FlexibleTM
Signal Void Size (1) 2,811 11,981 14,638 21,841 1,492-1,702 3.631-4,008 2,218-4,365 4,484-6,917
Static Magnetic Field (T) 1.5 1.5 1.5 1.5 1.5 1.5 1.5 1.5
Pulse Sequence T1-SE T1-SE GRE GRE T1-SE T1-SE FMPSPGR FMPSPGR
TR (msec) 500 500 100 100 300 300 50 50
TE (msec) 20 20 15 15 20 20 2.6 2.6
Flip Angle N/A N/A 30° 30° N/A N/A 30° 30°
Bandwidth 16 kHz 16 kHz 16 kHz 16 kHz 16 kHz 16 kHz 16 kHz 16 kHz
Field of View 24 cm 24 cm 24 cm 24 cm 24 cm 24 cm 24 cm 24 cm
Matrix Size 256 x 256 256 x 256 256 x 256 256 x 256 256 x 128 256 x 128 256 x 128 256 x 128
Section Thickness 5 mm 5 mm 5 mm 5 mm 10 mm 10 mm 10 mm 10 mm
Maximum ReadoutGradient Strength 6.3 mT/m 6.3 mT/m 6.3 mT/m 6.3 mT/m 6.3 mT/m 6.3 mT/m 6.3 mT/m 6.3 mT/m
Orientation ofDevice to Field Parallel Perpendicular Parallel Perpendicular Parallel Perpendicular Parallel Perpendicular
Phantom Filler Gel Gel Gel Gel Gel Gel Gel Gel
Summary of MRI Artifact Information
(T1-SE, T1-weighted spin echo; FMPSPGR, fast spoiled gradient recalled echo in the steady state; GRE, gradient echo; N/A, not applicable; values for artifact sizeindicated in mm2; Note that the T1 and T2 values for the gel used for the phantom filler are similar to the values of skeletal muscle or organ tissue.)
(1) Ranges listed reflect results obtained with largest and smallest size LMA FlexibleTM devices. Values will vary with different sized LMA FlexibleTM devices
TM
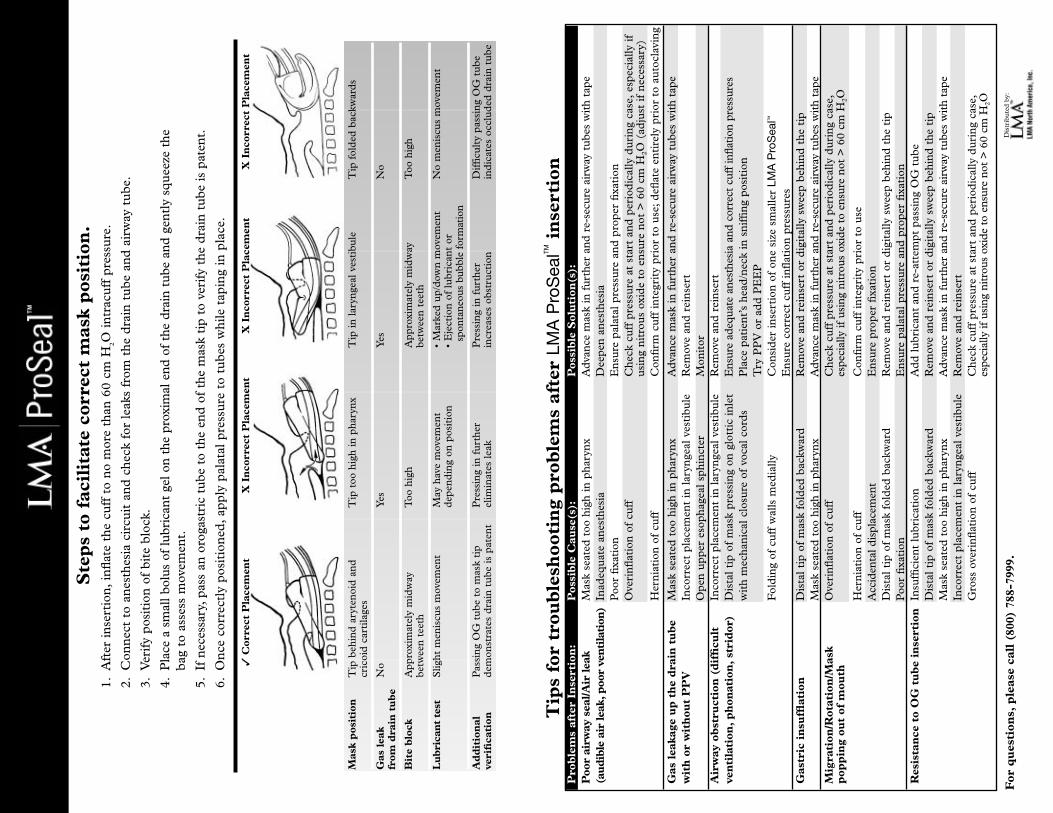
For
qu
esti
ons,
ple
ase
call
(80
0) 7
88-7
999.
Dis
trib
ute
d b
y:
Tip
s fo
r tr
oub
lesh
ooti
ng
pro
ble
ms
afte
r LM
A P
roS
ealTM
inse
rtio
nP
rob
lem
s af
ter
Inse
rtio
n:
Pos
sib
le C
ause
(s):
Pos
sib
le S
olu
tion
(s):
Poo
r ai
rway
sea
l/Air
lea
k M
ask
seat
ed t
oo h
igh
in p
hary
nx
Ad
van
ce m
ask
in f
urt
her
and
re-
secu
re a
irw
ay t
ube
s w
ith
tape
(au
dib
le a
ir le
ak,p
oor
ven
tila
tion
)In
adeq
uat
e an
esth
esia
Dee
pen
an
esth
esia
Poo
r fi
xati
onE
nsu
re p
alat
al p
ress
ure
an
d p
rope
r fi
xati
on
Ove
rin
flat
ion
of
cuff
Che
ck c
uff
pre
ssu
re a
t st
art
and
per
iod
ical
ly d
uri
ng
case
,esp
ecia
lly i
fu
sin
g n
itro
us
oxid
e to
en
sure
not
> 6
0 cm
H2O
(ad
just
if
nec
essa
ry)
Her
nia
tion
of
cuff
Con
firm
cu
ff i
nte
grit
y pr
ior
to u
se;d
eflat
e en
tire
ly p
rior
to
auto
clav
ing
Gas
lea
kage
up
th
e d
rain
tu
be
Mas
k se
ated
too
hig
h in
pha
ryn
xA
dva
nce
mas
k in
fu
rthe
r an
d r
e-se
cure
air
way
tu
bes
wit
h ta
pew
ith
or
wit
hou
t P
PV
Inco
rrec
t pl
acem
ent
in l
aryn
geal
ves
tibu
leR
emov
e an
d r
ein
sert
Ope
n u
pper
eso
phag
eal
sphi
nct
erM
onit
orA
irw
ay o
bst
ruct
ion
(d
iffi
cult
Inco
rrec
t pl
acem
ent
in l
aryn
geal
ves
tibu
leR
emov
e an
d r
ein
sert
ven
tila
tion
,p
hon
atio
n,
stri
dor
)D
ista
l ti
p of
mas
k pr
essi
ng
on g
lott
ic i
nle
tE
nsur
e ad
equa
te a
nest
hesi
a an
d co
rrec
t cu
ff in
flati
on p
ress
ures
wit
h m
echa
nic
al c
losu
re o
f vo
cal
cord
sP
lace
pat
ien
t’s
head
/nec
k in
sn
iffi
ng
posi
tion
Try
PP
V o
r ad
d P
EE
PF
old
ing
of c
uff
wal
ls m
edia
llyC
onsi
der
in
sert
ion
of
one
size
sm
alle
r LM
A P
roS
ealTM
En
sure
cor
rect
cu
ff i
nfl
atio
n p
ress
ure
sG
astr
ic i
nsu
fflat
ion
Dis
tal
tip
of m
ask
fold
ed b
ackw
ard
Rem
ove
and
rei
nse
rt o
r d
igit
ally
sw
eep
behi
nd
the
tip
Mas
k se
ated
too
hig
h in
pha
ryn
xA
dva
nce
mas
k in
fu
rthe
r an
d r
e-se
cure
air
way
tu
bes
wit
h ta
peM
igra
tion
/Rot
atio
n/M
ask
Ove
rin
flat
ion
of
cuff
Che
ck c
uff
pre
ssu
re a
t st
art
and
per
iod
ical
ly d
uri
ng
case
,p
opp
ing
out
of m
outh
espe
cial
ly if
usi
ng n
itro
us o
xide
to
ensu
re n
ot >
60
cm H
2O
Her
nia
tion
of
cuff
Con
firm
cu
ff i
nte
grit
y pr
ior
to u
seA
ccid
enta
l dis
plac
emen
t E
nsu
re p
rope
r fi
xati
onD
ista
l ti
p of
mas
k fo
lded
bac
kwar
dR
emov
e an
d r
ein
sert
or
dig
ital
ly s
wee
p be
hin
d t
he t
ipP
oor
fixa
tion
En
sure
pal
atal
pre
ssu
re a
nd
pro
per
fixa
tion
R
esis
tan
ce t
o O
G t
ub
e in
sert
ion
Insu
ffici
ent
lubr
icat
ion
Ad
d l
ubr
ican
t an
d r
e-at
tem
pt p
assi
ng
OG
tu
beD
ista
l ti
p of
mas
k fo
lded
bac
kwar
dR
emov
e an
d r
ein
sert
or
dig
ital
ly s
wee
p be
hin
d t
he t
ipM
ask
seat
ed t
oo h
igh
in p
hary
nx
Ad
van
ce m
ask
in f
urt
her
and
re-
secu
re a
irw
ay t
ube
s w
ith
tape
Inco
rrec
t pl
acem
ent
in l
aryn
geal
ves
tibu
leR
emov
e an
d r
ein
sert
Gro
ss o
veri
nfl
atio
n o
f cu
ffC
heck
cu
ff p
ress
ure
at
star
t an
d p
erio
dic
ally
du
rin
g ca
se,
espe
cial
ly if
usi
ng n
itro
us o
xide
to
ensu
re n
ot >
60
cm H
2O
Ste
ps
to f
acil
itat
e co
rrec
t m
ask
pos
itio
n.
1.A
fter
in
sert
ion
,in
flat
e th
e cu
ff t
o n
o m
ore
than
60
cm H
2O i
ntr
acu
ff p
ress
ure
.
2.C
onn
ect
to a
nes
thes
ia c
ircu
it a
nd
che
ck f
or l
eaks
fro
m t
he d
rain
tu
be a
nd
air
way
tu
be.
3.V
erif
y po
siti
on o
f bi
te b
lock
.
4.P
lace
a s
mal
l bol
us o
f lu
bric
ant
gel o
n th
e pr
oxim
al e
nd o
f th
e dr
ain
tube
and
gen
tly
squ
eeze
the
bag
to a
sses
s m
ovem
ent.
5.If
nec
essa
ry,p
ass
an o
roga
stri
c tu
be t
o th
e en
d o
f th
e m
ask
tip
to v
erif
y th
e d
rain
tu
be i
s pa
ten
t.
6.O
nce
cor
rect
ly p
osit
ion
ed,a
pply
pal
atal
pre
ssu
re t
o tu
bes
whi
le t
apin
g in
pla
ce.
Mas
k p
osit
ion
Tip
beh
ind
ary
ten
oid
an
dT
ip t
oo h
igh
in p
hary
nx
Tip
in
lar
ynge
al v
esti
bule
Tip
fol
ded
bac
kwar
ds
cric
oid
car
tila
ges
Gas
lea
kN
oY
esY
esN
ofr
om d
rain
tu
be
Bit
e b
lock
App
roxi
mat
ely
mid
way
T
oo h
igh
App
roxi
mat
ely
mid
way
Too
hig
hbe
twee
n t
eeth
betw
een
tee
th
Lu
bri
can
t te
stS
light
men
iscu
s m
ovem
ent
May
hav
e m
ovem
ent
• M
arke
d u
p/d
own
mov
emen
tN
o m
enis
cus
mov
emen
td
epen
din
g on
pos
itio
n•
Eje
ctio
n o
f lu
bric
ant
orsp
onta
neou
s bu
bble
for
mat
ion
Ad
dit
ion
alP
assi
ng
OG
tu
be t
o m
ask
tip
Pre
ssin
g in
fu
rthe
rP
ress
ing
in f
urt
her
Dif
ficu
lty
pass
ing
OG
tu
beve
rifi
cati
ond
emon
stra
tes
dra
in t
ube
is
pate
nt
elim
inat
es l
eak
incr
ease
s ob
stru
ctio
nin
dic
ates
occ
lud
ed d
rain
tu
be
✓C
orre
ct P
lace
men
tX
In
corr
ect
Pla
cem
ent
X I
nco
rrec
t P
lace
men
tX
In
corr
ect
Pla
cem
ent
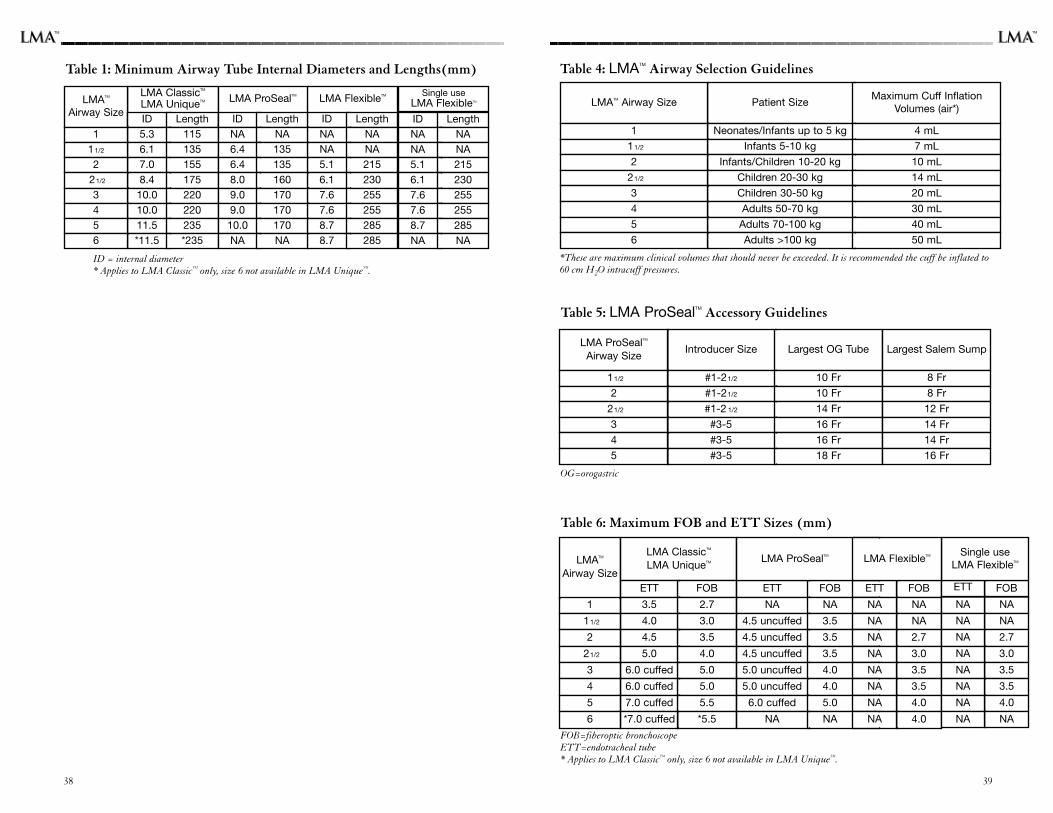
Table 6: Maximum FOB and ETT Sizes (mm)
FOB=fiberoptic bronchoscopeETT=endotracheal tube* Applies to LMA ClassicTM only, size 6 not available in LMA UniqueTM.
Table 1: Minimum Airway Tube Internal Diameters and Lengths(mm)
ID = internal diameter* Applies to LMA ClassicTM only, size 6 not available in LMA UniqueTM.
3938
LMATM
Airway Size
LMA ClassicTM
LMA UniqueTM
ETT FOB ETT FOB ETT FOB
3.5 2.7 NA NA NA NA
4.0 3.0 4.5 uncuffed 3.5 NA NA
4.5 3.5 4.5 uncuffed 3.5 NA 2.7
5.0 4.0 4.5 uncuffed 3.5 NA 3.0
6.0 cuffed 5.0 5.0 uncuffed 4.0 NA 3.5
1
11/2
2
21/2
3
6.0 cuffed 5.0 5.0 uncuffed 4.0 NA 3.5
7.0 cuffed 5.5 6.0 cuffed 5.0 NA 4.0
*7.0 cuffed *5.5 NA NA NA 4.0
4
5
6
LMA ProSealTM
Table 4: LMATM Airway Selection Guidelines
*These are maximum clinical volumes that should never be exceeded. It is recommended the cuff be inflated to60 cm H2O intracuff pressures.
LMATM Airway Size Patient SizeMaximum Cuff Inflation
Volumes (air*)
1 Neonates/Infants up to 5 kg 4 mL
11/2 Infants 5-10 kg 7 mL
2 Infants/Children 10-20 kg 10 mL
21/2 Children 20-30 kg 14 mL
3 Children 30-50 kg 20 mL
4 Adults 50-70 kg 30 mL
5 Adults 70-100 kg 40 mL
6 Adults >100 kg 50 mL
Table 5: LMA ProSealTM Accessory Guidelines
OG=orogastric
LMA ProSealTM
Airway SizeIntroducer Size Largest OG Tube
11/2 #1-21/2 10 Fr
2 #1-21/2 10 Fr
21/2 #1-2 1/2 14 Fr
3 #3-5 16 Fr
4 #3-5 16 Fr
5 #3-5 18 Fr
Largest Salem Sump
8 Fr
8 Fr
12 Fr
14 Fr
14 Fr
16 Fr
LMATM
Airway Size
111/2
221/2
3456
LMA ClassicTM
LMA UniqueTM LMA ProSealTM LMA FlexibleTM
ID Length ID Length ID Length5.3 115 NA NA NA NA6.1 135 6.4 135 NA NA7.0 155 6.4 135 5.1 2158.4 175 8.0 160 6.1 23010.0 220 9.0 170 7.6 25510.0 220 9.0 170 7.6 25511.5 235 10.0 170 8.7 285*11.5 *235 NA NA 8.7 285
ID LengthNA NANA NA5.1 2156.1 2307.6 2557.6 2558.7 285NA NA
Single useLMA FlexibleTM
ETT FOB
NA NA
NA NA
NA 2.7
NA 3.0
NA 3.5
NA 3.5
NA 4.0
NA NA
Single useLMA FlexibleTMLMA FlexibleTM
TMTM