
Activation of cytosolic phospholipase A2 by transforming growth ...

James Madison University James Madison University
JMU Scholarly Commons JMU Scholarly Commons
Masters Theses, 2020-current The Graduate School
5-7-2020
Lipoprotein associated phospholipase A2 in individuals with Lipoprotein associated phospholipase A2 in individuals with
obstructive sleep apnea obstructive sleep apnea
Kendall G. Clark James Madison University
Follow this and additional works at: https://commons.lib.jmu.edu/masters202029
Part of the Cardiovascular Diseases Commons
Recommended Citation Recommended Citation Clark, Kendall G., "Lipoprotein associated phospholipase A2 in individuals with obstructive sleep apnea" (2020). Masters Theses, 2020-current. 41. https://commons.lib.jmu.edu/masters202029/41
This Thesis is brought to you for free and open access by the The Graduate School at JMU Scholarly Commons. It has been accepted for inclusion in Masters Theses, 2020-current by an authorized administrator of JMU Scholarly Commons. For more information, please contact [email protected].
Lipoprotein Associated Phospholipase A2 (Lp-PLA2) in Individuals with Obstructive
Sleep Apnea (OSA)
Kendall Clark
A thesis submitted to the Graduate Faculty of
JAMES MADISON UNIVERSITY
In
Partial Fulfillment of the Requirements
for the degree of
Master of Science
Department of Kinesiology
May 2020
FACULTY COMMITTEE:
Committee Chair: Trent A. Hargens, Ph. D.
Committee Members/ Readers:
Stephanie P. Kurti, Ph. D.
Christopher J. Womack, Ph. D.
ii
Acknowledgments
I would first like to thank my committee chair, Dr. Trent Hargens. This project
would not have happened without your help and encouragement. I am grateful for the
opportunity to work closely with you throughout this process. Your feedback and
instruction have made me a better writer and researcher.
I would also like to thank my other committee members, Dr. Stephanie Kurti and
Dr. Christopher Womack. Dr. Kurti, thank you for your guidance in the lab and providing
me with the best undergraduate assistants. Dr. Womack, thank you for your time and
expertise in the blood analysis process.
Additionally, I would like to thank my undergraduate assistants, Amanda Placide
and Sydney Sharp, for dedicating their time to countless hours in the lab helping me
calibrate equipment and run subjects through the protocol. These two were essential in
the data collection process.
I would not have made it through this process without my fellow classmates and
colleagues. Thank you to everyone who gave their assistance in the lab on a whim and
provided encouragement along the way. I am thankful to have gotten to spend my
graduate time at JMU with each of you and you all will always be a part of why JMU is
so special to me.
Lastly, I would like to thank all of the subjects that participated in this study. I
appreciate you dedicating your time to the lab and am very grateful to have had the
opportunity to work with each of you.

iii
Table of Contents
Acknowledgments .............................................................................................................. ii
Table of Contents…………………………………………………………………………iii
List of Tables …………………………………………………………………………….iv
List of Figures ......................................................................................................................v
Abstract .............................................................................................................................. vi
I. Introduction ......................................................................................................................1
II. Methodology .................................................................................................................13
III. Manuscript ...................................................................................................................17
IV. Appendices ..................................................................................................................39
V. References .....................................................................................................................55
iv
List of Tables
Table 1. Subject Characteristics Between OSA & Non-OSA………………………….. 36
Table 2. Physical Activity Between OSA & Non-OSA ……………………………….. 36
Table 3. Subject Characteristics Between High & Low Lp-PLA2………….………….. 37
Table 4. Physical Activity Between High & Low Lp-PLA2………………..………….. 37

v
List of Figures
Figure 1. Lp-PLA2 Between OSA & Non-OSA ……………………….……………… 38
Figure 2. Lp-PLA2 & Sedentary Minutes……………………….…………………...….38
vi
Abstract
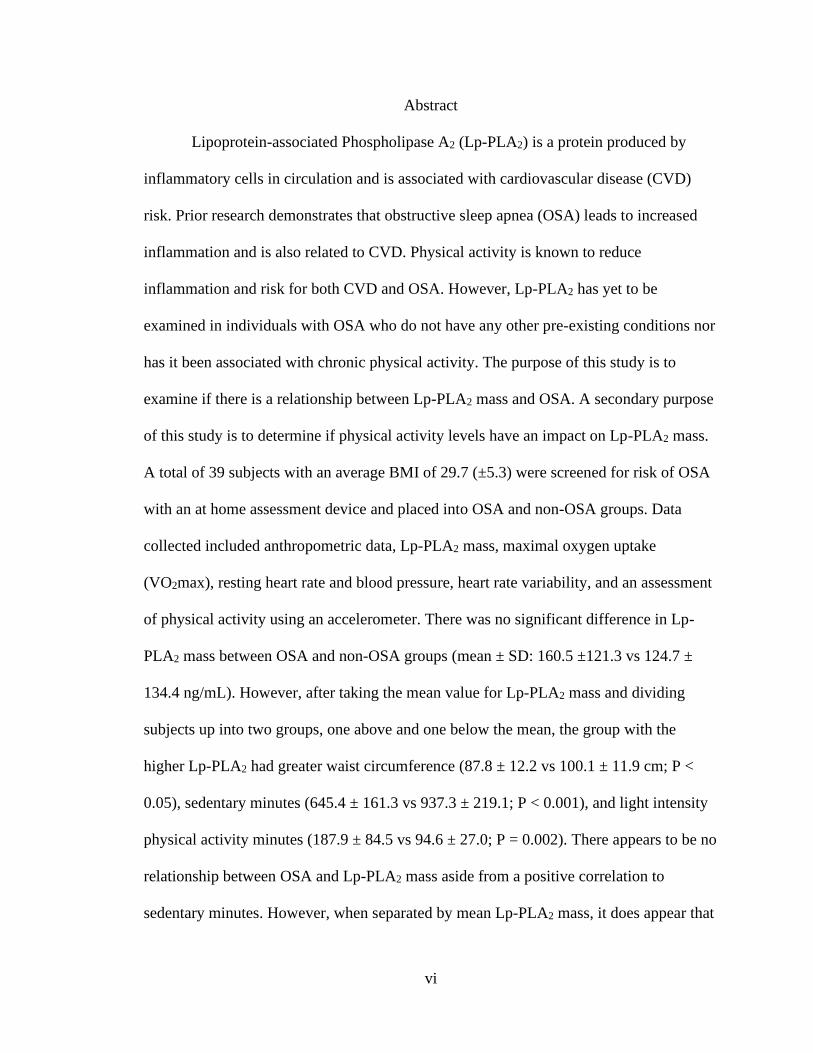
Lipoprotein-associated Phospholipase A2 (Lp-PLA2) is a protein produced by
inflammatory cells in circulation and is associated with cardiovascular disease (CVD)
risk. Prior research demonstrates that obstructive sleep apnea (OSA) leads to increased
inflammation and is also related to CVD. Physical activity is known to reduce
inflammation and risk for both CVD and OSA. However, Lp-PLA2 has yet to be
examined in individuals with OSA who do not have any other pre-existing conditions nor
has it been associated with chronic physical activity. The purpose of this study is to
examine if there is a relationship between Lp-PLA2 mass and OSA. A secondary purpose
of this study is to determine if physical activity levels have an impact on Lp-PLA2 mass.
A total of 39 subjects with an average BMI of 29.7 (±5.3) were screened for risk of OSA
with an at home assessment device and placed into OSA and non-OSA groups. Data
collected included anthropometric data, Lp-PLA2 mass, maximal oxygen uptake
(VO2max), resting heart rate and blood pressure, heart rate variability, and an assessment
of physical activity using an accelerometer. There was no significant difference in Lp-
PLA2 mass between OSA and non-OSA groups (mean ± SD: 160.5 ±121.3 vs 124.7 ±
134.4 ng/mL). However, after taking the mean value for Lp-PLA2 mass and dividing
subjects up into two groups, one above and one below the mean, the group with the
higher Lp-PLA2 had greater waist circumference (87.8 ± 12.2 vs 100.1 ± 11.9 cm; P <
0.05), sedentary minutes (645.4 ± 161.3 vs 937.3 ± 219.1; P < 0.001), and light intensity
physical activity minutes (187.9 ± 84.5 vs 94.6 ± 27.0; P = 0.002). There appears to be no
relationship between OSA and Lp-PLA2 mass aside from a positive correlation to
sedentary minutes. However, when separated by mean Lp-PLA2 mass, it does appear that

vii
Lp-PLA2 is associated with waist circumference, sedentary time, and time in light
activity. This suggests that there could be a relationship between physical activity
behavior and Lp-PLA2, as a result of differing adiposity profile.
Chapter 1
Introduction
Lipoprotein-associated Phospholipase A2
Lipoprotein-associated Phospholipase A2 (Lp-PLA2) is a protein produced by
inflammatory cells in circulation and is associated with cardiovascular disease (CVD)
risk in individuals with metabolic disorders (Lavi, 2007). After being produced by
macrophages in atherosclerotic plaque, Lp-PLA2 is then secreted into the circulatory
system with about 80% of it bound to low-density lipoproteins (LDL) and the other 20%
bound to high-density lipoproteins (HDL) (Stafforini, 2015). Within the endothelium,
LDL becomes oxidized and yields products that are hydrolysed by Lp-PLA2, generating
oxidized phospholipids, such as lysophosphatidylcholine (lysoPC) and non-esterified
fatty acids (NEFAs) (Benitez, 2004). These products are important in mediating the
inflammatory process by upregulating expression of adhesion molecules (Shi, 2007),
activating leukocytes (Shi, 2007), and recruiting macrophages and monocytes to the
atherosclerotic plaque (Quinn, 1988). This cycle accelerates plaque formation because the
increase in inflammation produces even more Lp-PLA2, essentially upregulating itself
(Shi, 2007). One study suggests that Lp-PLA2 may be made locally by the macrophages
as Lp-PLA2 mRNA transcripts have been found in macrophages (Hakkinen, 1999).
Lp-PLA2 in normal population
Lp-PLA2 measurements can be separated into enzyme mass and activity. Both
mass and activity are significantly correlated with each other as well as with very low
density lipoprotein (VLDL), LDL, and HDL (Caslake, 2000). Both Lp-PLA2 mass and
activity stay relatively consistent in an individual, not being affected by acute
2
inflammation or infection compared to other markers of inflammation, such as high
sensitivity C-reactive protein (hsCRP) (Corson, 2008; Brilakis, 2008; Persson, 2007-epi).
This enables better clinical decisions from a single measurement and provides confidence
in trends in this inflammatory marker over a period of time (Corson, 2008). One review
found a strong positive correlation (r=0.87) between Lp-PLA2 mass and activity in
plasma samples taken from 22 subjects (Dada, 2002). In a large epidemiologic study,
there was a strong correlation between Lp-PLA2 mass and activity, with more variance
occurring between the two at higher levels (Persson, 2007-epi). The highest correlations
were seen in Lp-PLA2 activity and cholesterol, LDL, and LDL/HDL ratio, with an
inverse relationship to HDL. A weaker correlation was seen between these variables and
Lp-PLA2 mass (Persson, 2007-epi). In this same study, higher Lp-PLA2 levels were
found in smokers compared to non-smokers, individuals with a history of CVD compared
to those without, obese individuals compared to non-obese, and diabetics comparend to
non-diabetics (Persson, 2007-epi); although it should be noted that these differences were
not statistically significant. In addition, men tend to have higher levels of Lp-PLA2 mass
and activity than women (Brilakis, 2008; Persson, 2007-epi). Lp-PLA2 activity was also
lower in African Americans and Hispanics compared to Caucasians with the lowest levels
found in African American women and the highest in Caucasian males (Brilakis, 2008).
Lp-PLA2 & CVD risk
Many of the common risk factors for atherosclerosis and CVD, such as
hypertension, high LDL, smoking, and obesity, are not exhibited in up to 50% of cardiac
patients, indicating that there are other potential risk factors that need to be studied
further (Sytkowski, 1990; Dada, 2002). Compared to healthy individuals, activity and

3
mass of Lp-PLA2 is significantly increased in people with CVD (Cai, 2013). Evidence
shows that Lp-PLA2 plays a crucial role in the pathophysiology of atherosclerosis and is
indicative of future cardiovascular disease (Acevedo, 2015). Measuring Lp-PLA2 levels
is useful to evaluate the presence of atherosclerosis, especially in high risk individuals
that may have metabolic syndrome (Acevedo, 2015). Originally, >235 ng/mL of Lp-
PLA2 mass was defined as the cutoff for increased risk based off of the 50th percentile of
a healthy population (Lanman, 2006). After reviewing many Lp-PLA2 studies, one
consensus panel determined that a clinical cut point of Lp-PLA2 mass >200 ng/mL would
indicate a patient being at higher risk for cardiovascular disease (Davidson, 2008).
Vascular events alter both Lp-PLA2 mass and activity, which may be due to the
alterations in HDL/LDL levels (Delgado, 2012). While Lp-PLA2 mass and activity are
both linked to lipid levels, Lp-PLA2 mass also has a strong link with cholesterol and
triglyceride levels (Delgado, 2012). One study found that Lp-PLA2 mass was higher in
individuals with coronary artery disease (CAD) and subjects post-myocardial infarction
compared to a control group (Caslake, 2000). Interestingly, the Lp-PLA2 mass levels
were higher in individuals with CAD even though LDL was not significantly different
from the control group. This indicates that plasma Lp-PLA2 mass was a strong predictor
of risk, independent of common risk factors (LDL, HDL, smoking, and BP) in the CAD
group (Caslake, 2000). It was speculated that as LDL is cleared from plasma, Lp-PLA2
would be cleared at the same rate. However, Lp-PLA2 has also been found bound to a
small dense LDL subtype that has a prolonged half-life, which could explain the elevated
Lp-PLA2 mass in these subjects regardless of LDL (Guerra, 1997).
4
Lp-PLA2 activity and mass has been associated as an independent and significant
indicator of metabolic syndrome and inflammation, possibly increasing the risk of CVD
(Persson, 2007; Acevedo, 2015). Regardless of metabolic syndrome, higher Lp-PLA2
levels have been found to increase risk of CVD (Persson, 2007). However, high Lp-PLA2
levels in combination with metabolic syndrome has the highest risk for CVD (Persson,
2007). In addition, Lp-PLA2 appears to be influenced by weight, metabolic state and
unfavorable circulating lipid profiles (increased oxidized LDL and triglycerides)
(Jackisch, 2018). These responses are exacerbated in individuals with type 2 diabetes,
which also increases risk for CVD (Jackisch, 2018).
The expression of Lp-PLA2 was observed in coronary arteries from 25 subjects
who died from sudden cardiac death. Plaque samples with increased Lp-PLA2 were
associated with thin, fibrous caps or ruptured plaques compared to more stable lesions
that had less Lp-PLA2 (Kolodgie, 2006). An increased Lp-PLA2 mass and activity and
lysoPC levels in carotid artery plaques of patients with symptomatic cerebrovascular
disease has also been associated with markers of tissue oxidative stress, inflammation,
and instability. (Mannheim, 2008) This suggests that there may be a relationship between
Lp-PLA2 and plaque instability (Kolodgie, 2006; Mannheim, 2008).
A large portion of patients who suddenly die from CVD present no symptoms
prior to their event (Go, 2014). The Framingham Risk Score (FRS) has been used to help
detect CVD risk but still many patients are misclassified (NCEP, 2002). In a previous
study, many of those who were classified as low risk by the FRS were still classified as
high risk by Lp-PLA2 mass (>200 ng/mL) (Hargens, 2014). This suggests that Lp-PLA2
mass may be indicative of CVD independently of other risk factors.
5
A meta-analysis of 25 clinical trials found elevated Lp-PLA2 caused an almost
two-fold increase in risk for future and recurring CVD events (Corson, 2008). Thus, it
was determined that Lp-PLA2 is a relevant risk factor to identify individuals at a high risk
for CVD and those who could benefit from intensive lipid-lowering interventions
(Corson, 2008). Another meta-analysis of 32 clinical studies found increased relative
risks in individuals with elevated Lp-PLA2 levels for CHD, ischemic stroke, vascular
mortality, and non-vascular mortality (Thompson, 2010). There have also been observed
elevations in Lp-PLA2 in individuals with proven coronary artery disease, independently
of LDL, HDL, smoking, and systolic blood pressure (Caslake, 2000). This adds to the
evidence that Lp-PLA2 levels may be a valuable addition to traditional risk factors in
assessing CVD risk as been suggested by a consensus panel (Davidson, 2008).
Obstructive Sleep Apnea (OSA)
Obstructive Sleep Apnea (OSA) can be described as recurrent episodes of full or
partial collapse of the airways during sleep, leading to decreased ventilation, frequent
arousals, sleep fragmentation, and oxyhemoglobin desaturation (Somers, 2008). An
apnea event can be described as a complete restriction of airflow for greater than 10
seconds while a hypopnea event is defined as a reduction in airflow to less than 50% of
normal airflow (Somers, 2008). Diagnosis and determination of severity of sleep apnea is
defined by the apnea-hypopnea index (AHI), which is the number of apnea or hypopnea
events per hour (mild OSA: ≥ 5 AHI; moderate OSA: ≥ 15 AHI; severe OSA ≥ 30 AHI)
(Young, 2002). Recent prevalence estimates of moderate to severe sleep apnea are 10%
among 30–49-year-old men; 17% among 50–70-year-old men; 3% among 30–49-year-
old women; and 9% among 50–70 year-old women (Peppard, 2013). These estimates
6
represent a significant increase of 14% to 55% over the last two decades depending on
the subgroup (Peppard, 2013). The Wisconsin Sleep Cohort measured AHI over a period
of eight years and found the greatest increase in AHI across individuals who were
habitual snorers, had a body mass index (BMI) ≥ 30, and those who were 45-60 years of
age (Young, 2002). In addition, it is predicted that about 80% of individuals with
moderate to severe OSA are undiagnosed (Lee, 2008) and even those who are diagnosed
often choose not to accept treatment (Weaver, 2008). When left untreated, OSA can lead
to daytime sleepiness, cognitive dysfunction, and decrease in quality of life (Punjabi,
2008).
Sleep Apnea and CVD
Interrupted sleep, hypoxemia, and daytime sleepiness due to OSA induces an
increase in oxidative stress, inflammation, and endothelial apoptosis, which contributes to
endothelial dysfunction, eventually leading to atherosclerosis or CVD if left untreated
(Somers, 2008; Atkeson, 2009; Savransky, 2007). Individuals with OSA have been
shown to have an increased sympathetic activation, leading to an increased resting heart
rate (Narkiewicz, 1998). These individuals have also been seen to have decreased heart
rate variability and increased blood pressure variability (Narkiewicz, 1998). In addition,
OSA has been associated with insulin resistance, independent of BMI (Punjabi, 2004).
Lastly, the forced inspiration during sudden arousals at night creates dramatic pressure
change, causing a negative intrathoracic pressure environment and increased stress on the
heart (Somers, 2008). About 50% of patients who have OSA also have hypertension
(Silverberg, 1998). Even after controlling for age, sex, BMI, and hypertension
7
medications, the Wisconsin Sleep Cohort study found a dose response relationship
between blood pressure and OSA (Peppard, 2000).
One study found that, in middle aged males with OSA, those who were not treated
for their condition had a significantly higher CVD incidence (56.8%) compared to those
who were treated for their OSA (6.7%) (Peker, 2002). They concluded that individuals
with OSA have an increased risk for CVD, independent of age, BMI, blood pressure, and
smoking habits. However, those who are treated for their OSA greatly reduced their risk
of developing CVD (Peker, 2002).
Due to the metabolic damage caused by apnea events, OSA has also been linked
to type 2 diabetes. One study found that sleep disordered breathing was independently
related to glucose intolerance and insulin resistance and that the severity of the sleep
disordered breathing was also associated with the degree of insulin resistance (Punjabi,
2004). These hypoxic events have been linked to an increase in proinflammatory
cytokines, specifically interleukin 6 (IL-6) and tumor necrosis factor alpha (TNF-ɑ),
which has been linked to insulin resistance and increased risk for type 2 diabetes
(Huiguo, 2000; Punjabi, 2004). Individuals with sleep disordered breathing have also
shown to have increased sympathetic neural activity (Peled, 1998), which can increase
glycogen breakdown and gluconeogenesis and disrupt glucose homeostasis (Punjabi,
2004). In addition, sleep-disordered patients have increased levels of cortisol (Bratel,
1999), which has been shown to increase glucose levels and insulin concentration (Plat,
1999).
Weight and Sleep Apnea
8
Obesity has consistently been associated with OSA and has even been said to be
one of the most important risk factors for sleep disordered breathing (Young, 2002,
Wolk, 2003). About 40% of obese indivuals have significant sleep apnea and about 70%
of indiviuals with OSA are obese (Vgontzas, 1994). One study found that a 10% increase
in weight increased the odds of developing sleep apnea 6-fold (Peppard, 2000). In
addition, a 10% decrease in weight was associated with a 26% decrease in AHI (Peppard,
2000). Research suggests that obesity leads to the narrowing and altering of function of
the airways (Horner, 1989; Schwartz, 1991). Obese individuals have large fat deposits
surrounding the collapsible part of the pharynx, and this is exacerbated in individuals
with OSA compared to weight-matched controls without OSA (Horner, 1989). Weight
loss has been associated with a decrease in airway collapsibility in individuals who have
sleep apnea (Schwartz, 1991). Male patients who have OSA have about 50% higher
leptin levels than weight-matched individuals without OSA (Phillips, 2000). Thus, it is
likely that leptin resistance is especially increased in individuals with OSA, potentially
leading to even greater weight gain and progression of OSA (Wolk, 2003). In healthy
individuals who experience weight gain, the possibility of developing OSA is increased.
In overweight individuals with OSA, further weight gains accelerate the progression of
OSA (Young, 2002; Peppard, 2000). The greater the increase in body weight or waist
circumference, the greater the progression of OSA and vice versa (Young, 2002;
Peppard, 2000). In addition, individuals who currently have OSA and gain weight
experience an increase in OSA severity independent of other factors such as age, body
composition, and smoking habits (Peppard, 2000).
Exercise & Sleep Apnea
9
Similar to baseline weight, habitual physical activity levels predict development
of OSA. Awad et al. observed that active individuals exhibited a decreased incidence of
OSA in an 8-year follow up compared to sedentary individuals. Furthermore, decreasing
exercise over time was associated with an increase in AHI (Awad, 2012). Individuals
with OSA tend to be more sedentary regardless of levels of obesity or daytime sleepiness
(Hargens, 2019). In addition to just being active, exercise training volume exhibits a
dose-response relationship for likelihood of OSA (Peppard, 2004).
Exercise is also beneficial in the reduction of obesity, blood pressure, and CVD,
which are all associated with OSA (Young, 2002). In addition to these benefits, AHI
levels may be reduced by up to 50% following chronic exercise training in those who
have sleep apnea (Norman, 2000; Sengul, 2011). This may be due to general
improvements in strength and fatigue resistance of the airways (Vincent, 2002). In
sedentary, obese individuals with untreated moderate to severe sleep apnea, significant
improvements in AHI were observed following an exercise training program, even
without a significant reduction in body weight (Kline, 2011). There were also
improvements in both objective and subjective sleep quality, suggesting that exercise
training may be beneficial (Kline, 2011). Similarly, another study found that exercise
training led to improvements in AHI, sleep efficiency, and daytime sleepiness,
independent of changes in BMI (Iftikhar, 2014). A similar study in OSA patients found
that regular exercise training improved BMI, along with aerobic capacity and quality of
life (Norman, 2000). A meta-analysis of exercise intervention studies also observed a
reduction in AHI regardless of types, durations, or frequencies of exercise or continuous
positive airway pressure (CPAP) use (Aiello, 2016).
10
Chronic exercise is associated with an increase in slow wave sleep (SWS), total
sleep time; and decreases in rapid eye movement (REM) sleep, sleep onset latency
(SOL), and wake after sleep onset (WASO) (Kubitz, 1996). In previously sedentary
individuals, a two month exercise intervention increased vagal activity and decreased
sympathetic activity during sleep (Pichot, 2002). The exact physiological mechanisms of
how exercise improves OSA are unknown and more research is needed to determine how
exercise improves OSA independent of weight loss.
Exercise intensity is also associated with prevalence and severity of OSA.
Vigorous physical activity for >3 hours has been associated with a larger decrease in the
prevalence of OSA than the same duration of exercise performed at a moderate intensity
(Quan, 2007). These outcomes were more pronounced in males and obese individuals
(Quan, 2007). These findings were similar to another study who also observed increased
planned exercise associated with less severe OSA (Peppard, 2004). Both studies
determined that benefits were seen with about 3-6 hours of exercise per week or at least 3
hours of vigorous intensity, independent of weight loss and daytime sleepiness (Quan,
2007; Peppard, 2004).
OSA & Lp-PLA2
In recent years research has evaluated the relationship between OSA and Lp-
PLA2 concentration. In one study looking at CVD risk among individuals with OSA,
COPD, or overlap syndrome (having both OSA and COPD), they found that Lp-PLA2
mass was elevated in all 3 groups, with the highest concentration in the overlap syndrome
group, followed by the OSA group (Badr, 2014). In a similar study, Lp-PLA2 mass was
elevated in individuals with OSA and in individuals with metabolic syndrome, but those
11
who had OSA and metabolic syndrome had the highest concentration of Lp-PLA2
(Moise, 2018). Another study separated the OSA subjects into mild, moderate, and severe
categories and found that Lp-PLA2 mass increased with OSA severity and also increased
with the presence of CVD in addition to OSA (Xu, 2020). Lastly, a study that solely
studied OSA and its correlation to Lp-PLA2 mass, separated 50 male patients diagnosed
with OSA into quartiles based on their number of arousals. They found that those in the
highest quartile had the highest Lp-PLA2 (Bekci, 2011).
Thus, it is apparent that there is a relationship between Lp-PLA2 and OSA. It is
also known that Lp-PLA2 concentration and presence of OSA are typically higher in
individuals who are at risk for CVD and in individuals who are overweight. In addition to
these risk factors, OSA has been shown to be both more prevalent and more severe in
those who lead a sedentary lifestyle.
Purpose
It has not been examined if chronic physical activity influences Lp-PLA2
concentration. Additionally, there needs to be more research in the relationship between
Lp-PLA2 and individuals with OSA who have no other pre-existing conditions.
Therefore, the primary purpose of this study is to determine whether there is an increase
in Lp-PLA2 concentration in individuals with OSA who have no other chronic conditions.
In addition, we will determine if there is a relationship between Lp-PLA2 concentration
and physical activity. We hypothesize that individuals with OSA will have higher Lp-
PLA2 concentrations. In addition, individuals Lp-PLA2 concentration will be associated
with chronic physical activity, with more active individuals exhibiting a lower
concentration of Lp-PLA2.
12
Limitations
One limitation in this study includes using an at home screening device to
diagnose OSA. However, despite this being an at-home screening tool, it has been
validated against hospital based polysomnography (Ng, 2009). We are assuming that the
equipment used in this study provides valid assessments of the variables we are observing
and that the participants understand our instructions and are knowledgeable in how to
properly assemble the at home screening device. The questionnaires utilized for this
study are also assuming that participants are disclosing accurate information about their
health history and physical activity. Additionally, we are limiting our subjects to
individuals who do not have other pre-existing chronic diseases. Lastly, placing an age
range on our subjects means that we will not be able to generalize our results to
individuals who are outside that age range.

13
Chapter 2
Methodology
Subjects
Participants were recruited through bulk email requests to all JMU faculty and
students. Thirty-nine subjects were recruited for the study (11 individuals with OSA and
28 control subjects). Inclusion criteria for both the experimental and control groups
included subjects that have been cleared to exercise by the Physical Activity
Questionnaire-Plus (PAR-Q+) and are between the ages of 18 and 57 years old.
Individuals in the experimental group had an AHI of at least 5. Individuals in the control
group had an AHI of <5. Exclusion criteria included participants who had a current
diagnosis of any cardiovascular, metabolic, or pulmonary disease as well as participants
who were pregnant (due to the low dose of radiation from DEXA).
Experimental methods
This study was part of a larger study that looked at airway responsiveness and
nitric oxide (NO) exhalation in individuals with OSA following a maximal exercise bout.
Subjects visited the laboratory a total of 2 times. During the first visit, after explaining
and signing a subject consent form, subjects completed a series of questionnaires,
including a PAR-Q+, International Physical Activity Questionnaire (IPAQ), Epworth
Sleepiness Scale (ESS), and Berlin Questionnaire. The IPAQ is validated in adults to
assess moderate to vigorous physical activity (MVPA) per week both in leisure time and
work related physical activity (Craig, 2003). The PAR-Q+ is a validated, self-guided
physical activity readiness questionnaire (Riebe, 2018). If the participant reported that
they do not regularly participate in planned exercise, they must also have no signs or
14
symptoms of cardiovascular disease, metabolic or renal disease. If they did have signs
and symptoms or were asymptomatic but have previously been diagnosed with the
aforementioned diseases, they were excluded from the study. Participants that engaged in
regular physical activity, were asymptomatic and had never been diagnosed with renal,
metabolic or cardiovascular diseases were cleared by the American College of Sports
Medicine (ACSM) guidelines to undergo the incremental exercise test to exhaustion to
determine peak oxygen uptake (VO2peak), even if they have sleep apnea. The Berlin
Questionnaire and ESS assessed the subjects snoring habits and daytime sleepiness
(Kang, 2013; Johns, 1992). Anthropometric variables were then obtained including,
height, weight, and waist/neck circumferences. Cardiorespiratory fitness was determined
using a graded cycle ergometer VO2max test. Subjects were then sent home with an
unattended, home sleep evaluation using a type III validated device (ApneaLink™ Plus,
RedMed Corp., San Diego, CA) to assess for the likely presence of OSA (Ng, 2009).
Research staff instructed the patient on the proper setup and use of the at-home screening
device. The device is composed of a pulse oximeter, which was worn on the end of an
index finger, and a nasal cannula, which was worn over the face, and into the nose to
measure airflow. This device is harmless and painless to wear. The results of this test will
objectively divide the subjects into OSA and non-OSA control groups. Subjects were also
sent home with an accelerometer (Actigraph GT3X+, Actigraph Corp., Pensacola, FL) to
assess their 7-day physical activity. Subjects were asked to wear the device on their waist
at all times, except while sleeping and showering. Accelerometers have been validated to
assess MVPA per week (Kelly, 2013). On their second visit, a fasted, resting venous
blood draw was taken. This was followed by a heart rate variability assessment that also
15
included a resting blood pressure measurement in the supine position. Lastly, a Dual-
energy X-ray absorptiometry (DEXA) analysis using the General Electrics (GE) Lunar
iDEXA was performed to assess body composition (body fat percentage and lean mass).
Fasting blood collection
10 ml of blood was drawn from an antecubital vein using clean venipuncture.
Blood samples were immediately centrifuged for 20 min at 1,500xg and 4°C to obtain
platelet-poor plasma. Plasma aliquots were frozen and stored at - 20°C until assayed.
These samples were used to assess Lp-PLA2 mass.
Blood Analysis
An Enzyme-Linked Immunosorbent Assay (ELISA) kit was used to determine
Lp-PLA2 mass. Plasma samples were pipetted into the wells and the target protein
becomes bound to the wells by an immobilized antibody after sitting for 2.5 hours. Cells
are then washed four times to remove any unbound antibodies. The wells are then washed
with another antibody, sandwiching the Lp-PLA2 molecules between the two antibodies
after sitting for 1 hour. Cells are then washed four times again to remove any unbound
antibodies. A HRP-streptavidin solution was then pipetted into the wells with the
absorbance of this enzyme being directly proportional to the Lp-PLA2 concentration in
the sample. After 45 minutes, the wells were washed for a third time. A TMB substrate is
then added to the wells and a color develops, proportional to the concentration of Lp-
PLA2. A Stop solution is then added and the color turns from blue to yellow with the
intensity of the color being measured at 450 nm. (Sigma-Aldrich ELISA Kit Information;
Dada, 2002)
Graded Exercise Test
16
A maximal ramped (15 Watts per minute ramp rate) exercise test was completed
on an electronically braked, cycle ergometer. Metabolic responses were measured
continuously using a metabolic cart (Parvo Medics TrueOne 2400, Parvo Medics, Salt
Lake City, UT). Heart rate was measured continuously using a Polar V800 watch and
Polar H10 heart rate chest strap (Polar Electro). Rating of perceived exertion was
measured every minute using the Borg 6-20. Dyspnea ratings were also recorded every
minute using a dyspnea scale from 1-10. Blood pressure was taken manually every 3
minutes during the test. Subjects were instructed to keep their revolutions per minute
(RPM) above 50 and the test was terminated either by the subject voluntarily or if 50
RPMs could not be maintained.
Statistical Analysis
All statistical analyses were performed using IBM SPSS Statistics (version 26.0).
Independent sample t tests were used to assess group differences in Lp-PLA2 mass.
Pearson correlations were calculated to determine relationships between Lp-PLA2, OSA,
physical activity and sedentary behavior. A value of P < 0.05 was considered statistically
significant a priori.

17
Chapter 3
Manuscript
Lipoprotein Associated Phospholipase A2 (Lp-PLA2) in Individuals with
Obstructive Sleep Apnea (OSA)
Authors: Kendall G. Clark, Stephanie P. Kurti, Christopher J. Womack, Trent A.
Hargens
Institution: James Madison University, Harrisonburg, Virginia, 22807
Contacts: Kendall G. Clark, [email protected]
Trent A. Hargens, [email protected]
Stephanie P. Kurti, [email protected]
Christopher J. Womack, [email protected]
Address of Correspondence
Trent A. Hargens, Ph.D.
Department of Kinesiology
James Madison University
Harrisonburg VA, 22807
Phone: (540) 568-6145
Email: [email protected]
18
Abstract
Introduction: Lipoprotein-associated Phospholipase A2 (Lp-PLA2) is a protein produced
by inflammatory cells in circulation and is associated with cardiovascular disease (CVD)
risk. Prior research demonstrates that obstructive sleep apnea (OSA) leads to increased
inflammation and is also related to CVD. Physical activity is known to reduce
inflammation and risk for both CVD and OSA. However, Lp-PLA2 has yet to be
examined in individuals with OSA who do not have any other pre-existing conditions nor
has it been associated with chronic physical activity. The purpose of this study was to
examine if there is a relationship between Lp-PLA2 mass and OSA. A secondary purpose
of this study was to determine if physical activity levels have an impact on Lp-PLA2
mass.
Methods: A total of 39 subjects with an average BMI of 29.7 ±5.3 were screened for risk
of OSA with an at home assessment device and placed into OSA and non-OSA groups.
Data collected included anthropometric data, Lp-PLA2 mass, maximal oxygen uptake
(VO2max), resting heart rate and blood pressure, heart rate variability, and an assessment
of physical activity using an accelerometer.
Results: There was no significant difference in Lp-PLA2 mass between OSA and non-
OSA groups (160.5 ±121.3 vs 124.7 ± 134.4 ng/mL). However, after taking the mean
value for Lp-PLA2 mass and dividing subjects up into two groups, one above and one
below the mean, the group with the higher Lp-PLA2 had greater waist circumference
(87.8 ± 12.2 vs 100.1 ± 11.9 cm; P < 0.05), sedentary minutes (645.4 ± 161.3 vs 937.3 ±
219.1; P < 0.001), and light intensity physical activity minutes (187.9 ± 84.5 vs 94.6 ±
27.0; P = 0.002).

19
Conclusions: There appears to be no relationship between OSA and Lp-PLA2 mass aside
from a positive correlation to sedentary minutes. However, when separated by mean Lp-
PLA2 mass, it does appear that higher Lp-PLA2 is associated with waist circumference,
sedentary time, and time in light activity. This indicates that there could be a relationship
between physical activity behavior and Lp-PLA2, as a result of differing adiposity profile.
20
Introduction
Lipoprotein-associated Phospholipase A2 (Lp-PLA2) is a protein produced by
inflammatory cells in circulation and is associated with increased cardiovascular disease
(CVD) risk in individuals with metabolic disorders (Lavi, 2007). This biomarker is bound
primarily to low density lipoprotein (LDL) and causes an acceleration in plaque
formation, increasing inflammation and essentially upregulating itself (Stafforini, 2015;
Shi, 2007). Lp-PLA2 concentration can be separated into enzyme mass and activity,
which are both associated with very low density lipoprotein (VLDL), LDL, and high
density lipoprotein (HDL), with Lp-PLA2 mass also being correlated with triglyceride
and cholesterol levels (Caslake, 2000; Delgado, 2012). Lp-PLA2 concentration stays
relatively consistent, as it is not affected by acute inflammation compared to other
markers of inflammation, such as high sensitivity C-reactive protein (hsCRP) (Corson,
2008; Brilakis, 2008; Persson, 2007-epi). However, Lp-PLA2 concentration can be
influenced by chronic inflammation. Higher levels of the biomarker are found in men,
smokers and individuals with a history of CVD, obesity, diabetes, or metabolic syndrome
(Persson, 2007-epi; Persson, 2007; Brilakis, 2008; Jackisch, 2018) and has also been
associated with plaque instability (Kolodgie, 2006; Mannheim, 2008). Elevated Lp-PLA2
increases risk for developing CVD or experiencing recurring CVD events, even in those
determined to be low risk (Thompson, 2010, Corson, 2008, Hargens, 2014). This adds to
the evidence that Lp-PLA2 levels may be a valuable prognostic tool for CVD events in
addition to traditional risk factors.
With this research, it seems that Lp-PLA2 is associated with many risk factors and
conditions that often lead to or are caused by chronic inflammation. Obstructive Sleep
21
Apnea (OSA), which can be described as recurrent episodes of full (apnea) or partial
(hypopnea) collapse of the airways during sleep, results in systemic inflammation
(Somers, 2008; Atkeson, 2009; Savransky, 2007). Apneas and hypopneas leads to
decreased ventilation, frequent arousals, sleep fragmentation, and oxyhemoglobin
desaturation (Somers, 2008). Diagnosis and severity of sleep apnea is determined by the
apnea-hypopnea index (AHI), which is the number of apneas and hypopneas per hour of
sleep. Interrupted sleep due to OSA induces an increase in oxidative stress, inflammation,
and endothelial apoptosis, which contributes to endothelial dysfunction, eventually
leading to atherosclerosis or CVD if left untreated (Atkeson, 2009; Savransky, 2007).
The link between OSA, inflammation, and CVD suggests a possible role of Lp-PLA2.
This has been demonstrated in recent studies finding that Lp-PLA2 mass is higher in
individuals with OSA, and increased with OSA severity (Badr, 2014; Moise 2018; Xu,
2020, Bekci, 2011). However, many of these studies examined an older population with
OSA and other co-morbid conditions.
While OSA may increase inflammatory markers, including Lp-PLA2, habitual
physical activity is anti-inflammatory and has been associated with a decrease in
traditional risk factors (Kokkinos, 2012). In regard to OSA, individuals with the
condition tend to be more sedentary, regardless of BMI or daytime sleepiness (Hargens,
2019). However, active individuals exhibited a decreased incidence of OSA in an 8-year
follow up compared to sedentary individuals, while individuals who decreased exercise
over time exhibited a significant increase in AHI (Awad, 2012). Since physical activity
reduces indicators of inflammation, the impact that physical activity may have on Lp-
PLA2 has not been explored.
22
Therefore, the primary purpose of this study is to determine whether there is an
increase in Lp-PLA2 concentration in individuals with OSA who have no other chronic
conditions. In addition, we will determine if there is a relationship between Lp-PLA2
concentration and physical activity. It is hypothesized that individuals with OSA will
have higher Lp-PLA2 concentration. In addition, more active individuals will exhibit a
lower concentration of Lp-PLA2.
Methodology
Subjects
Participants were recruited through bulk email requests to all JMU faculty and
students. In addition to subjects recruited through these methods, previous data was
added to the sample pool (6 individuals with OSA and 10 control subjects) from an
unpublished study using identical methods. Thirty-nine subjects (18-57 years of age)
were used in the analysis for this study (11 individuals with OSA and 28 control
subjects). Inclusion criteria for both the experimental and control groups included
subjects that have been cleared to exercise by the Physical Activity Questionnaire-Plus
(PAR-Q+). Individuals in the experimental group had an AHI of at least 5. Individuals in
the control group had an AHI of <5. Exclusion criteria included participants with known
cardiovascular, metabolic, or pulmonary disease as well as participants who were
pregnant (due to the low dose of radiation from DEXA).
Experimental methods
This study was part of a larger study evaluating airway responsiveness and nitric
oxide (NO) exhalation in individuals with OSA following a maximal exercise bout.
Subjects visited the laboratory a total of 2 times. During the first visit, subjects completed
23
the informed consent and initial questionnaires, including a PAR-Q+, International
Physical Activity Questionnaire (IPAQ), Epworth Sleepiness Scale (ESS), and Berlin
Questionnaire. The IPAQ is validated in adults to assess moderate to vigorous physical
activity (MVPA) per week both in leisure time and work related physical activity (Craig,
2003). The PAR-Q+ is a validated, self-guided physical activity readiness questionnaire
(Riebe, 2018). The Berlin Questionnaire and ESS assessed the subjects snoring habits and
daytime sleepiness (Kang, 2013; Johns, 1992). Anthropometric variables were then
obtained including, height, weight, and waist/neck circumferences. Cardiorespiratory
fitness was determined using a graded cycle ergometer maximal oxygen uptake (VO2
max) test. Subjects were then sent home with an unattended, home sleep evaluation using
a type III validated device (ApneaLink™ Plus, RedMed Corp., San Diego, CA) to assess
for the likely presence of OSA (Ng, 2009). Research staff instructed the patient on the
proper setup and use of the at-home screening device. The device is composed of a pulse
oximeter, which was worn on the end of an index finger, and a nasal cannula, which was
worn over the face, and into the nose to measure airflow. The results of this test were
used to objectively divide the subjects into OSA and non-OSA control groups. Subjects
were also sent home with an accelerometer (Actigraph GT3X+, Actigraph Corp.,
Pensacola, FL) to assess their 7-day physical activity. Subjects were asked to wear the
device on their waist at all times, except while sleeping and showering. Accelerometers
have been validated to assess MVPA per week (Kelly, 2013). On their second visit, a
fasted, resting venous blood draw was taken. This was followed by a Dual-energy X-ray
absorptiometry (DEXA) analysis using the General Electrics (GE) Lunar iDEXA to
assess body composition (body fat percentage and lean mass).
24
Fasting blood collection
10 ml of blood was drawn from an antecubital vein using clean venipuncture.
Blood samples were immediately centrifuged for 20 min at 1,500xg and 4°C to obtain
platelet-poor plasma. Plasma aliquots were frozen and stored at - 20°C until assayed.
These samples were used to assess Lp-PLA2 mass.
Blood Analysis
An Enzyme-Linked Immunosorbent Assay (ELISA) kit was used to determine
Lp-PLA2 mass (Sigma-Aldrich). All samples were measured in duplicate at minimum.
Statistical Analysis
All statistical analyses were performed using IBM SPSS Statistics (version 26.0).
Independent sample t tests were used to assess group differences in Lp-PLA2 mass.
Pearson correlations were calculated to determine relationships between Lp-PLA2, AHI,
physical activity, and sedentary behavior variables. A value of P < 0.05 was considered
statistically significant a priori.
Results
By design, the OSA group had a significantly higher AHI than the non-OSA
group. Subject characteristics for the OSA and non-OSA groups are listed in Table 1. The
OSA group was older than the non-OSA group (P = 0.001). There were no group
differences in any body composition variable, however there was a trend for a greater
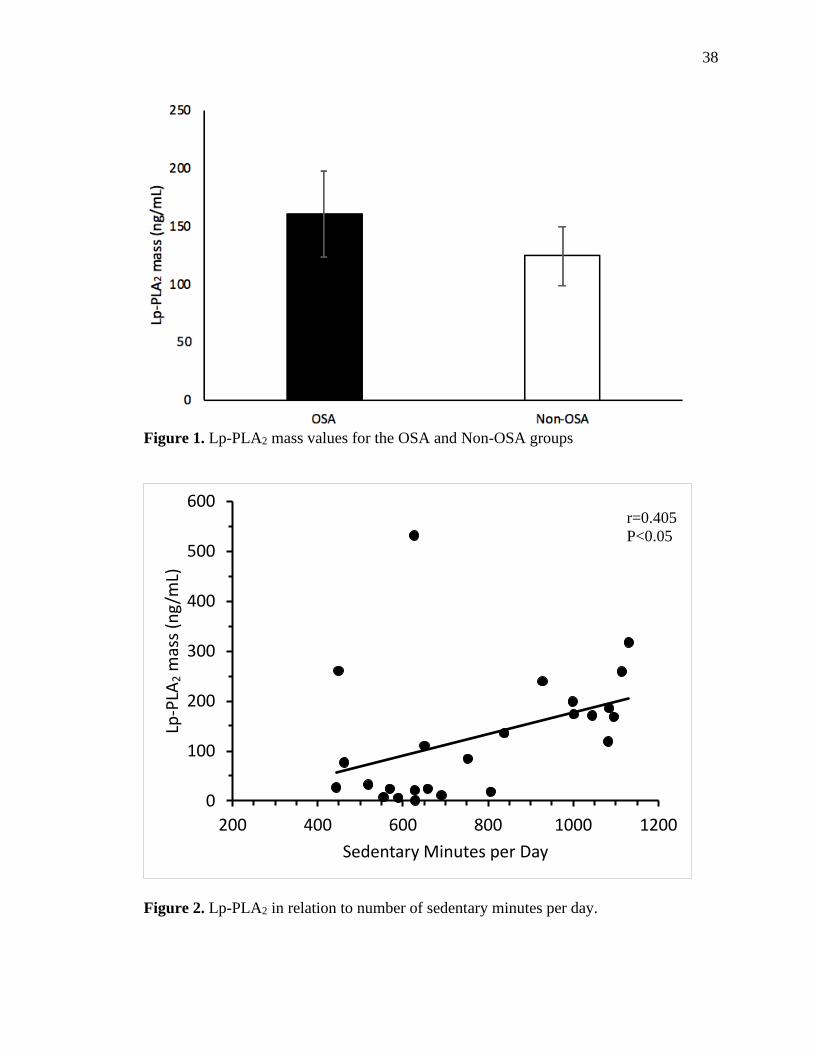
neck circumference in the OSA group (P = 0.05). There was no correlation between Lp-
PLA2 mass and age (r=0.104, P=0.536) or AHI (r=0.122, P=0.458). Independent sample
t-test revealed no difference in Lp-PLA2 mass between the OSA and non-OSA groups,
25
which did not change when age was used as a covariate in a one way analysis of variance
(P=0.45). (Figure 1)
Lp-PLA2 Mass & Physical Activity
There was a positive correlation between Lp-PLA2 mass and sedentary minutes
per day (r=0.405, P<0.05), based on an analysis of 25 subjects, as those with insufficient
accelerometer data were not included in this analysis. (Figure 2) Physical activity
between groups did not differ between the OSA and non-OSA groups, with the exception
of the OSA group having fewer moderate intensity minutes per day (P = 0.039).
However, when controlled for age this difference was no longer significant. (Table 2)
Due to the positive association seen between sedentary time and Lp-PLA2 in the
entire sample, we sought to explore the relationship between sedentary behavior and Lp-
PLA2 further. The sample of 25 subjects were split into two groups based on whether they
were above or below the mean value for Lp-PLA2 mass (134.7 ng/mL). The mean was
chosen due to the fact that our subjects were healthy and relatively young, which resulted
in overall lower Lp-PLA2 compared to other studies, and only four subjects with an Lp-
PLA2 mass over 200 ng/mL. The two groups did not differ in age, AHI, BMI, or % body
fat. Waist circumference was greater in the higher Lp-PLA2 group compared to the lower
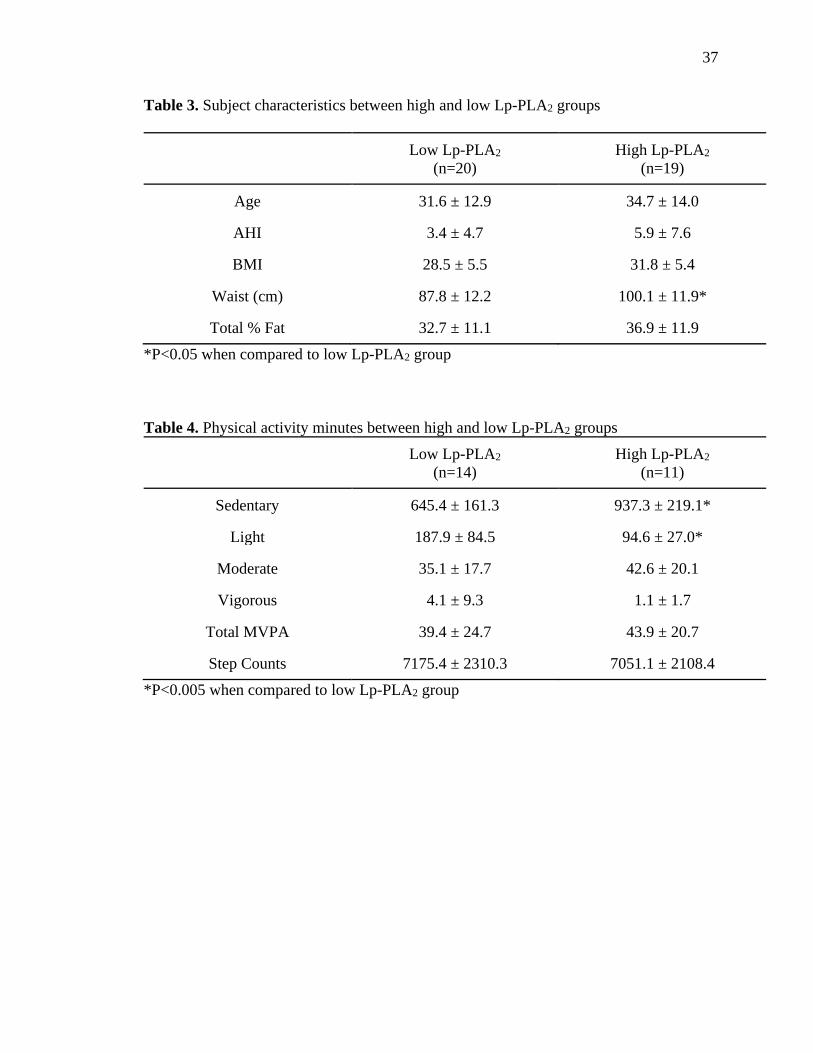
Lp-PLA2 group (P<0.05). (Table 3) Those in the higher Lp-PLA2 group had a greater
number of sedentary minutes per day (<0.001) and fewer light intensity PA minutes per
day compared to the lower Lp-PLA2 group (P=0.002). Total moderate to vigorous
intensity physical activity and average step count per day did not differ between groups.
(Table 4)
26
Discussion
Results from this study suggest that OSA may not impact Lp-PLA2 mass in a
younger, healthier cohort, as we found no difference in Lp-PLA2 in those at high
likelihood for OSA compared to those screened as negative for likely presence of OSA. It
is important to note that our OSA group had a mean OSA severity rated as “mild”, with
only four reaching a moderate severity and none reaching severe. Of these four moderate
OSA subjects, the mean Lp-PLA2 was 182 ng/mL and only three of them exceeded 200
ng/mL. This may have impacted our ability to observe a relationship between OSA
severity and Lp-PLA2. In addition, our sample was relatively young, with ages in the
OSA group ranging from 21-57. Thus, some subjects may have only been exposed to the
potential inflammatory effects of OSA for a short period of time.
In previous clinical studies, Lp-PLA2 was typically evaluated in relation to OSA
and another chronic condition, such as CVD, COPD, and metabolic syndrome (Xu, 2020;
Badr, 2014; Moise, 2018). In each of these studies, Lp-PLA2 was found in the greatest
amount in the groups diagnosed with OSA in addition to another condition. In studies
that split OSA groups into severities, the most severe group had the greatest increase in
Lp-PLA2 (Xu, 2020; Bekci, 2011). These previous studies used subjects with moderate to
severe sleep apnea, which would also lead us to expect greater Lp-PLA2 concentrations
than the present study (Moise, 2018; Badr, 2014; Bekci, 2011) as Xu et al. (2020) have
observed that Lp-PLA2 mass is only increased in individuals with moderate and severe
sleep apnea. The present study sought to evaluate the effects of OSA independent of
other chronic conditions that increase inflammation, such as CVD. Thus, prior findings
may have been influenced by comorbid conditions and OSA per se may not have a large
27
impact on Lp-PLA2. Additionally, our OSA group was younger (44.1 ± 12.9 years) than
all of the aforementioned studies with our control group being even younger (28.6 ± 10.8
years), which could have contributed to the similar Lp-PLA2 between groups.
The interesting finding of the current study was the relationship between Lp-PLA2
and sedentary behavior, independent of OSA. We observed that in those with greater
sedentary behavior, Lp-PLA2 was higher, Additionally, those with higher Lp-PLA2 had
fewer minutes of light intensity PA and greater waist circumference. While both groups
would be classified as being “low active” based on step counts (Tudor-Locke, 2013), and
are meeting current physical activity recommendations in terms of MVPA (Riebe, 2018),
the group with higher Lp-PLA2 had a lower overall physical activity profile with less
light activity minutes and greater sedentary minutes. This decrease in overall activity
profile may contribute to the greater waist circumference observed, which may correlate
to the greater Lp-PLA2.
Habitual physical activity is anti-inflammatory and has been associated with a
decrease in traditional risk factors (Kokkinos, 2012). Data from the Harvard Alumni
Health Study suggests that while light intensity activities are not associated with reduced
mortality rates, moderate intensity is somewhat beneficial, and vigorous intensity
significantly reduces mortality rates (Lee, 2000). In contrast, one systematic review found
that while moderate to vigorous intensity activities provide more benefits per unit of time,
light intensity physical activity offers some reduction of cardiovascular risk and all-cause
mortality (Chastin, 2019). Sedentary time, independent of total activity levels, is also an
important risk factor for CVD and all-cause mortality with more than 2.5 times greater
risk in those who accumulate 10 hours/day compared to 6.5 hours/day (Dohrn, 2018).
28
Even intermittent breaks in sedentary time is beneficially correlated to waist
circumference and cardiometabolic biomarkers (Healy, 2011). In the present study, both
groups exceeded 10 hours/day of sedentary time on average, regardless of if groups were
separated based on presence of OSA (13.6 hours vs 12.6 hours) or concentration of Lp-
PLA2 (10.8 hours vs 15.6 hours).
With much of the research and data published, including the national guidelines,
focusing on the importance of MVPA, this somewhat novel information on sedentary
time and light intensity PA is an important contribution to this area of literature. With
many Americans struggling to even meet the guidelines it is important to research how
our sedentary time is impacting our mortality risk and what even the smallest bit of
activity can do to help.
Physical activity has also been a predictor of waist circumference with those who
engage in higher levels of physical activity typically having lower abdominal adiposity
(Ekelund, 2011). We found that, in addition to a lack of light PA and an excess of
sedentary time, the high Lp-PLA2 group also appeared to have a larger waist
circumference, regardless of BMI or body fat percent. Although BMI is typically used to
determine health risks, waist circumference may be a better determinant of predicting
obesity-related health risks, with most individual risk factors for CVD having a higher
correlation to waist circumference than BMI (Janssen, 2004; Zhu, 2002). In addition to
obesity and visceral adiposity, inflammatory cytokines such as tumor necrosis factor
alpha (TNF-ɑ), interleukin 6 (IL-6), and C-reactive protein (CRP) have been associated
with waist circumference, indicating that an increase in waist circumference can create an
increase in inflammation (Park, 2005). When comparing normal weight women to

29
overweight/obese women, the overweight/obese group had significant increases in waist
circumference and Lp-PLA2 in addition to other indicators of oxidative stress (Paik,
2015). A separate study observed an increase in waist circumference, inflammatory
biomarkers, including Lp-PLA2, and a decrease in physical activity among men and
women who developed CVD across a mean follow-up of 10 years compared to those who
did not (Rana, 2011). One study indicates that Lp-PLA2 is actively produced in adipose
tissue and is also expressed in greater amounts specifically in abdominal subcutaneous
tissue (Jackisch, 2018). Weight loss interventions resulting in a reduction of waist
circumference have also been associated with a reduction in Lp-PLA2 (Tzotzas, 2008).
Our findings indicate similar results that individuals with greater waist circumferences
exhibited greater Lp-PLA2 concentrations. This adds to the evidence that location of
adipose tissue may contribute greater risk for obesity related conditions.
One limitation of the present study is that there was a relatively small sample size
with only 39 individuals used for the analysis of Lp-PLA2 mass, only 11 of which were
classified as having sleep apnea. Additionally, those that we did identify as having sleep
apnea, only exhibited a mild form of it with the average AHI being 12.4 ± 7.3. However,
it is informative that Lp-PLA2 levels are not altered in individuals with mild OSA. Lastly,
our subjects were recruited from a college campus, which likely led to the discrepancy in
age between the OSA and non-OSA groups (44.1 ± 12.9 years vs 28.6 ± 10.8 years).
In conclusion, our results showed no difference in Lp-PLA2 mass between OSA
and non-OSA subjects. When split up based on mean Lp-PLA2 mass, there was a
significant difference in waist circumference, sedentary time, and time spent in light
intensity physical activity, with MVPA and step count remaining the same between

30
groups. This suggests that abdominal fat as well as activity and sedentary time outside of
MVPA may be important in determining Lp-PLA2 concentration.
31
Manuscript References
Atkeson A, Yeh SY, Malhotra A, Jelic S. (2009). Endothelial function in obstructive
sleep apnea. Progress in cardiovascular diseases. 2009;51(5):351-362.
Awad KM, Malhotra A, Barnet JH, Quan SF, Peppard PE. Exercise is associated with a
reduced incidence of sleep-disordered breathing. The American journal of
medicine. 2012;125(5):485-490.
Badr EA, Yousif M, Hazzaa SM. Lipoprotein-associated phospholipase A2 levels as a
predictor of cardiovascular risks in patients with COPD and obstructive sleep
apnea. Egyptian Journal of Chest Diseases and Tuberculosis, 2014;63(2):405-
410.
Bekci TT, Kayrak M, Kiyici A, et al. The association among lipoprotein-associated
phospholipase A2 levels, total antioxidant capacity and arousal in male patients
with OSA. International journal of medical sciences. 2011;8(5):369.
Brilakis ES, Khera A, McGuire DK, et al. Influence of race and sex on lipoprotein-
associated phospholipase A2 levels: observations from the Dallas Heart Study.
Atherosclerosis. 2008;199(1):110-5.
Caslake MJ, Packard CJ, Suckling KE, Holmes SD, Chamberlain P, Macphee CH.
Lipoprotein-associated phospholipase A2, platelet-activating factor
acetylhydrolase: a potential new risk factor for coronary artery disease.
Atherosclerosis. 2000;150(2):413–419.
Chastin SF, De Craemer M, De Cocker K, et al. How does light-intensity physical
activity associate with adult cardiometabolic health and mortality? Systematic
review with meta-analysis of experimental and observational studies. Br J Sports
Med. 2019;53(6):370-376.
Corson MA, Jones PH, Davidson MH. Review of the evidence for the clinical utility of
lipoprotein-associated phospholipase A2 as a cardiovascular risk marker. Am J
Cardiol. 2008;101(12):S41–S50.
Craig CL, Marshall AL, Sjöström M, et al. International physical activity questionnaire:
12-country reliability and validity. Medicine & science in sports & exercise.
2003;35(8):1381-1395.

32
Delgado P, Chacón P, Penalba A, et al. Temporal profile and prognostic value of Lp-
PLA2 mass and activity in the acute stroke setting. Atherosclerosis.
2012;220(2):532-536.
Dohrn M, Sjöström M, Kwak L, Oja P, Hagströmer M. Accelerometer-measured
sedentary time and physical activity—a 15 year follow-up of mortality in a
Swedish population-based cohort. Journal of science and medicine in sport.
2018;21(7):702-707.
Ekelund U, Besson H, Luan JA, et al. Physical activity and gain in abdominal adiposity
and body weight: prospective cohort study in 288,498 men and women. The
American journal of clinical nutrition. 2011;93(4):826-835.
Hargens TA, Martin RA, Strosnider CL, Giersch GEW, Womack CJ. Obstructive sleep
apnea negatively impacts objectively measured physical activity. Sleep and
Breathing. 2019;23(2):447-454.
Hargens TA, Rhodes PG, VanReenen J, Kaminsky LA. Lipoprotein-associated
phospholipase A2 and carotid intima-media thickness in individuals classified as
low-risk according to Framingham. Cardiovascular diagnosis and therapy.
2014;4(6):487.
Healy GN, Matthews CE, Dunstan DW, Winkler EA, Owen N. Sedentary time and
cardio-metabolic biomarkers in US adults: NHANES 2003–06. European heart
journal. 2011;32(5):590-597.
Jackisch L, Kumsaiyai W, Moore JD, et al. Differential expression of Lp-PLA2 in
obesity and type 2 diabetes and the influence of lipids. Diabetologia.
2018;61(5):1155-1166.
Janssen I, Katzmarzyk PT, Ross R. Waist circumference and not body mass index
explains obesity-related health risk. The American journal of clinical nutrition.
2004;79(3):379-384.
Johns, M. W. Reliability and factor analysis of the Epworth Sleepiness Scale. Sleep.
1992;15(4):376-381.
Kang K, Park KS, Kim JE, Kim SW, Kim YT, Kim JS, Lee HW. Usefulness of the Berlin
Questionnaire to identify patients at high risk for obstructive sleep apnea: a
population-based door-to-door study. Sleep and Breathing. 2013;17(2):803-810.
33
Kelly LA, McMillan DG, Anderson A, Fippinger M, Fillerup G, Rider J. Validity of
actigraphs uniaxial and triaxial accelerometers for assessment of physical activity
in adults in laboratory conditions. BMC medical physics. 2013;13(1):5.
Kokkinos P. Physical activity, health benefits, and mortality risk. ISRN cardiology. 2012.
Kolodgie FD, Burke AP, Skorija KS et al. Lipoprotein-associated phospholipase A2
protein expression in the natural progression of human coronary atherosclerosis.
Arterioscler Thromb Vasc Biol. 2006;26(11):2523–9.
Lavi S, McConnell JP, Rihal CS, et al. Local production of lipoprotein-associated
phospholipase A2 and lysophosphatidylcholine in the coronary circulation:
association with early coronary atherosclerosis and endothelial dysfunction in
humans. Circulation. 2007;115(21):2715-21.
Lee IM, Paffenbarger Jr RS. Associations of light, moderate, and vigorous intensity
physical activity with longevity: the Harvard Alumni Health Study. American
journal of epidemiology. 2000;151(3):293-299.
Mannheim D, Herrmann J, Versari D, et al. Enhanced expression of Lp-PLA2 and
lysophosphatidylcholine in symptomatic carotid atherosclerotic plaques. Stroke.
2008;39(5):1448-1455.
Moise LG, Marta DS, Raşcu A, Moldoveanu E. Serum Lipoprotein-Associated
Phospholipase A2 in Males With Metabolic Syndrome and Obstructive Sleep
Apnea. Acta Endocrinologica (Bucharest). 2018;14(1):36.
Ng SSS, Chan TO, To KW, et al. Validation of a portable recording device (ApneaLink)
for identifying patients with suspected obstructive sleep apnoea syndrome.
Internal medicine journal. 2009;39(11):757-762.
Paik JK, Kim M, Kim M, et al. Circulating Lp-PLA 2 activity correlates with oxidative
stress and cytokines in overweight/obese postmenopausal women not using
hormone replacement therapy. Age. 2015;37(2):32.
Park HS, Park JY, Yu R. Relationship of obesity and visceral adiposity with serum
concentrations of CRP, TNF-α and IL-6. Diabetes research and clinical practice.
2005;69(1):29-35.
Persson M, Hedblad B, Nelson JJ, Berglund G. Elevated Lp-PLA2 levels add prognostic
information to the metabolic syndrome on incidence of cardiovascular events
34
among middle-aged nondiabetic subjects. Arteriosclerosis, Thrombosis, and
Vascular Biology. 2007;27(6):1411-1416.
Persson M, Nilsson JÅ, Nelson JJ, Hedblad B, Berglund G. The epidemiology of Lp-
PLA2: Distribution and correlation with cardiovascular risk factors in a
population-based cohort. Atherosclerosis. 2007;190(2):388-396.
Rana JS, Arsenault BJ, Després JP, et al. Inflammatory biomarkers, physical activity,
waist circumference, and risk of future coronary heart disease in healthy men and
women. European Heart Journal. 2011;32(3):336-344.
Riebe D, Ehrman JK, Liguori G, Magal M. ACSM's Guidelines for Exercise Testing and
Prescription. 10th ed. Philadelphia: Wolters Kluwer; 2018.
Savransky V, Nanayakkara A, Li J, et al. Chronic intermittent hypoxia induces
atherosclerosis. Am J Respir Crit Care Med. 2007;175(12):1290-1297.
Shi Y, Zhang P, Zhang L et al. Role of lipoprotein-associated phospholipase A2 in
leukocyte activation and inflammatory responses. Atherosclerosis.
2007;191(1):54–62.
Somers VK, White DP, Amin R, et al. Sleep apnea and cardiovascular disease: An
American heart association/American college of cardiology foundation scientific
statement from the American heart association council for high blood pressure
research professional education committee, council on clinical cardiology, stroke
council, and council on cardiovascular nursing in collaboration with the national
heart, lung, and blood institute national center on sleep disorders research
(national institutes of health). Journal of the American College of Cardiology,
2008;52(8):686-717.
Stafforini DM. Plasma PAF-AH (PLA2G7): Biochemical properties, association with
LDLs and HDLs, and regulation of expression. The Enzymes. 2015;38:71–93.
Thompson A, Gao P, Orfei L, et al. Lipoprotein-associated phospholipase A(2) and risk
of coronary disease, stroke, and mortality: Collaborative analysis of 32
prospective studies. Lancet. 2010;375(9725):1536-44.
Tudor-Locke C, Craig CL, Thyfault JP, Spence JC. A step-defined sedentary lifestyle
index:< 5000 steps/day. Applied physiology, nutrition, and metabolism.
2013;38(2):100-114.
35
Tzotzas T, Filippatos TD, Triantos A, Bruckert E, Tselepis AD, Kiortsis DN. (2008).
Effects of a low-calorie diet associated with weight loss on lipoprotein-associated
phospholipase A2 (Lp-PLA2) activity in healthy obese women. Nutrition,
Metabolism and Cardiovascular Diseases. 2008;18(7):477-482.
Xu C, Yu F, Mao S, et al. Lipoprotein-associated phospholipase A2 predicted
cardiovascular disease in obstructive sleep apnea syndrome. Respiratory
Medicine. 2020;163:105881.
Zhu S, Wang Z, Heshka S, Heo M, Faith MS, Heymsfield SB. Waist circumference and
obesity-associated risk factors among whites in the third National Health and
Nutrition Examination Survey: clinical action thresholds. The American journal of
clinical nutrition. 2002;76(4):743-743.

36
Table 1. Subject characteristics between OSA and Non-OSA groups
OSA (n=11) Non-OSA (n=28)
Age 44.1 ± 12.9* 28.6 ± 10.8
AHI 12.4 ± 7.3 1.5 ± 1.2
Weight (kg) 95.4 ± 15.6 84.6 ± 17.9
Height (cm) 175.3 ± 9.6 169.7 ± 10.5
BMI 31.0 ± 4.7 29.7 ± 6.0
Waist (cm) 99.6 ± 12.1 91.5 ± 13.4
Neck (cm) 39.1 ± 4.5 36.0 ± 4.1
HR rest 68.2 ± 8.0 69.0 ± 11.0
*P=0.001 when compared to Non-OSA group
Table 2. Physical activity minutes between OSA and Non-OSA groups
OSA (n=8) Non-OSA (n=17)
Sedentary 815.3 ± 260.5* 754.3 ± 230.2
Light 123.9 ± 59.7 157.6 ± 87.5
Moderate 29.4 ± 9.7 42.7 ± 20.7
Vigorous 1.1 ± 2.4 3.6 ± 8.5
Very Vigorous 0.4 ± 0.5 0.2 ± 0.5
Total MVPA 32.9 ± 15.5 42.4 ± 26.5
Step Count 6303.1 ± 1440.9 7505.5 ± 2391.9
*P<0.05 when compared to Non-OSA group
37
Table 3. Subject characteristics between high and low Lp-PLA2 groups
Low Lp-PLA2
(n=20)
High Lp-PLA2
(n=19)
Age 31.6 ± 12.9 34.7 ± 14.0
AHI 3.4 ± 4.7 5.9 ± 7.6
BMI 28.5 ± 5.5 31.8 ± 5.4
Waist (cm) 87.8 ± 12.2 100.1 ± 11.9*
Total % Fat 32.7 ± 11.1 36.9 ± 11.9
*P<0.05 when compared to low Lp-PLA2 group
Table 4. Physical activity minutes between high and low Lp-PLA2 groups
Low Lp-PLA2
(n=14)
High Lp-PLA2
(n=11)
Sedentary 645.4 ± 161.3 937.3 ± 219.1*
Light 187.9 ± 84.5 94.6 ± 27.0*
Moderate 35.1 ± 17.7 42.6 ± 20.1
Vigorous 4.1 ± 9.3 1.1 ± 1.7
Total MVPA 39.4 ± 24.7 43.9 ± 20.7
Step Counts 7175.4 ± 2310.3 7051.1 ± 2108.4
*P<0.005 when compared to low Lp-PLA2 group
38
Figure 1. Lp-PLA2 mass values for the OSA and Non-OSA groups
Figure 2. Lp-PLA2 in relation to number of sedentary minutes per day.
0
100
200
300
400
500
600
200 400 600 800 1000 1200
Lp-P
LA2
mas
s (n
g/m
L)
Sedentary Minutes per Day
r=0.405
P<0.05
39
Appendix A. Informed Consent
Project Title: Does an Acute Bout of Exercise Reduce Exhaled Nitric Oxide Levels in Individuals with
Obstructive Sleep Apnea?
Consent to Participate in Research
Identification of Investigators & Purpose of Study You are being asked to participate in a research study conducted by Drs. Stephanie Kurti and Trent
Hargens from James Madison University. To participate, you must be in good health and not diagnosed
with any cardiovascular, pulmonary, or metabolic diseases (with the exception of Obstructive Sleep Apnea
(OSA)).
Previous research suggests that a bout of nighttime exercise was effective in reducing exhaled nitric oxide
levels in inactive asthmatic patients, which translated to improvements in pulmonary outcomes. However,
there is no literature that has shown if an acute bout of exercise lowers airway and systemic inflammation,
and improves vascular health in individuals with OSA. Therefore, the purpose of this study is to determine
whether an acute bout of exercise will reduce exhaled nitric oxide levels in individuals with OSA. This
study will contribute to the knowledge of both practitioners and clinicians, and may provide an important
public health message in providing exercise recommendations for those with elevated airway inflammation,
particularly in individuals with OSA. Should you decide to participate in this research study, you will be
asked to sign this consent form once all your questions have been answered to your satisfaction.
Research Procedures This study consists of four questionnaires, a body composition scan, an incremental exercise test to
exhaustion on a cycle ergometer, a home sleep evaluation device, a 7-day physical activity recording
device, and various physiological tests administered to individual participants in the Human Performance
Laboratory at James Madison University. The total time required for participation in the research study is
outlined on the following page (time required section).
Your will visit the laboratory a total of two times. The specific procedures during each visit are included
below:
Initial visit : On the first visit to the laboratory, you will be briefed on the study and asked to read and sign
a consent form and complete a health history questionnaire, as well as questionnaires assessing your
physical activity habits, daytime sleepiness, and snoring habits. If you’d like to see any of these
questionnaires prior to consenting, please ask a researcher and we’ll be happy to provide one for you.
After completion of the questionnaire, height, weight, and neck/waist circumference measurements will be
taken. We will then perform a fasted blood draw for Lp-PLA2. Following the blood draw, you will
complete two non-invasive breathing tests that will assess pulmonary function and airway inflammation.
Next, you will be asked to complete a maximal ramping exercise test, in which the resistance on the bike
will increase steadily until you say that you can no longer continue or cannot keep up, which should take
around 8 -15 minutes. We will be measuring some of your physiological responses continuously throughout
this test. At the end of this visit, you will be instructed how to properly set up and wear a home sleep
evaluation device to assess OSA. You will be asked to return with the device one day later.
Second visit: After returning with the sleep evaluation device one day after the initial visit, we’ll perform a
blood draw for Lp-PLA2. Then, we will perform a DEXA scan to assess your body composition (how
much of your body is fat vs. lean mass). Next, we will record your resting heart rate, heart rate variability,
and blood pressure, which will be obtained in the supine position. You will then be instructed how to
properly wear an accelerometer device (Actigraph GT-3X) to assess your 7-day physical activity. You will
return 8 days later for your control (CON) or Nighttime Exercise (NE) session

40
Participation in this study will require approximately 2 hours of your time in the lab over the course of 2
separate visits. The visits are outlined below:
Initial Visit : On the first visit to the laboratory, you will be asked to complete the required questionnaires
and have height, weight, and neck/waist circumference measurements taken. We will then complete a blood
draw and two non-invasive breathing tests. Also during the initial visit, you will be asked to complete the
incremental test to exhaustion. The entire testing day should take approximately 90 minutes.
Visit 2: You will be asked to return an ApneaLink device one day after your initial visit. Resting heart rate
and blood pressure and heart rate variability will be assessed followed by a DEXA scan. During this time,
you will also be instructed how to properly wear an accelerometer device. This visit should take
approximately 30 minutes.
Risks
Participation in this study does have some risks, although they are small. The risk of any serious event
during this study is very small. Possible risks include:
DEXA: The DEXA scan entails a low dose of radiation equivalent to approximately one transatlantic flight
(0.015 mSv= milliseievert). While there is no validated questionnaire to define extensive exposure,
radiation exposure is cumulative (200 DEXA scans is equal to the cumulative exposure of living at sea
level for a year (3 mSv). DEXA scans carry minimal X-ray exposure. To minimize exposure, the DEXA
scan will only be performed once. All body composition assessment will be performed according to the
American College of Sports Medicine guidelines for body composition assessment).
Blood sampling: The risks of blood sampling using venipuncture include possible mild bruising, and the
risk of transfer of blood-borne pathogens, as well as possible risks of infection or skin irritation. These risks
are considered to be minimal, and all safety precautions for handing blood samples will be followed
according to Occupational Safety and Health Administration (OSHA) protocols.
Benefits
By participating in this study, you may benefit by gaining knowledge of inflammatory markers, airway
inflammation (exhaled nitric oxide) and airway hyperresponsiveness, which provide important information
about your current cardiovascular and pulmonary health. You will learn your VO2peak, body composition,
and pulmonary function scores (forced expiratory flow in 1-sec, forced vital capacity, forced expiratory
flow at 25-75% of vital capacity). Society will benefit from more knowledge about how acute and chronic
exercise may benefit vascular and pulmonary outcomes in individuals with OSA.
Confidentiality The results of this research will be presented at the American College of Sports Medicine Annual meeting
as well as the American Society of Nutrition annual conferences. The results of this project will be coded in
such a way that the respondent’s identity will not be attached to the final form of this study. The researcher
retains the right to use and publish non-identifiable data. While individual responses are confidential,
aggregate data will be presented representing averages or generalizations about the responses as a whole.
All data will be stored in a secure location accessible only to the JMU researchers. Upon completion of the
study, all information that matches up individual respondents with their answers will be destroyed.
Participation & Withdrawal Your participation is entirely voluntary. You are free to choose not to participate. Should you choose to
participate, you can withdraw at any time without consequences of any kind.
41
Questions about the Study If you have questions or concerns during the time of your participation in this study, or after its completion
or you would like to receive a copy of the final aggregate results of this study, please contact:
Researcher’s Name:
Dr. Stephanie Kurti Department of Kinesiology
Email Address: [email protected] James Madison University Cell-Phone number: 630-205-6363
Telephone: 540-568-3947
Researcher’s Name:
Dr. Trent Hargens Department of Kinesiology
E-mail Address: [email protected] James Madison Univeristy
Telephone: 540-568-5844
Questions about Your Rights as a Research Subject
Dr. Taimi Castle
Chair, Institutional Review Board
James Madison University (540) 568-5929 [email protected]
Giving of Consent I have read this consent form and I understand what is being requested of me as a participant in this study. I
freely consent to participate. I have been given satisfactory answers to my questions. The investigator
provided me with a copy of this form. I certify that I am at least 18 years of age. ______________________________________
Name of Participant (Printed)
______________________________________ ______________
Name of Participant (Signed) Date
______________________________________ ______________
Name of Researcher (Signed) Date
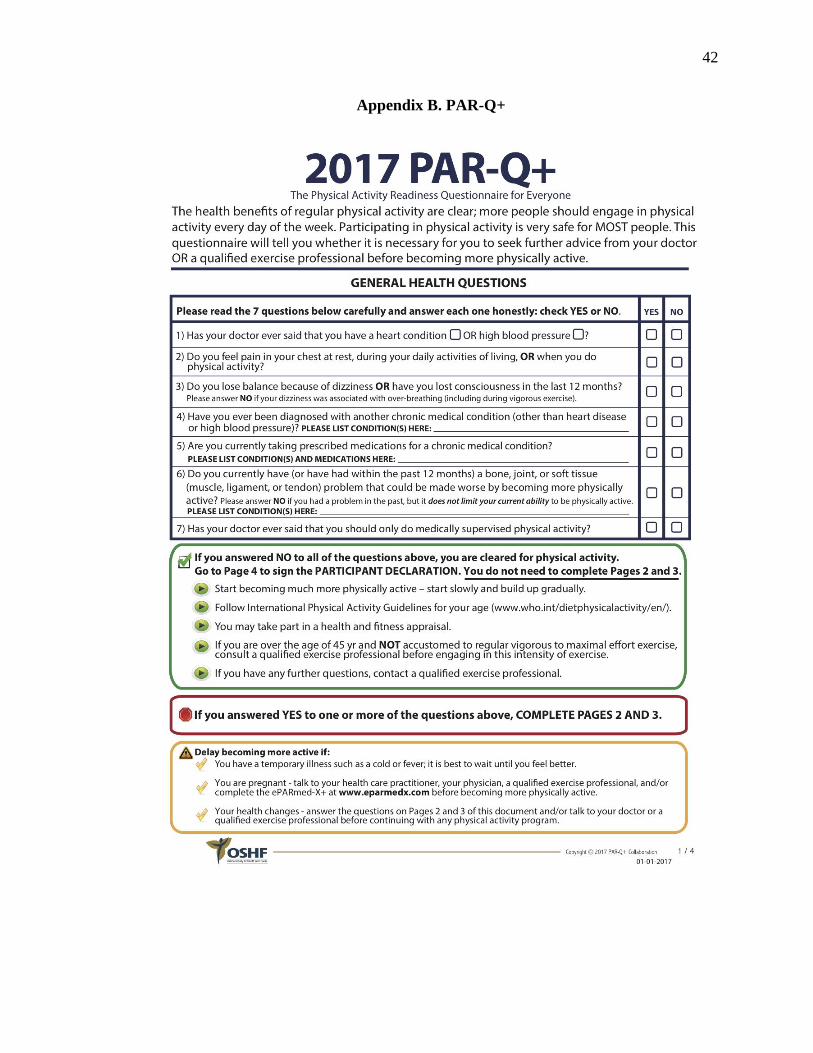
42
Appendix B. PAR-Q+
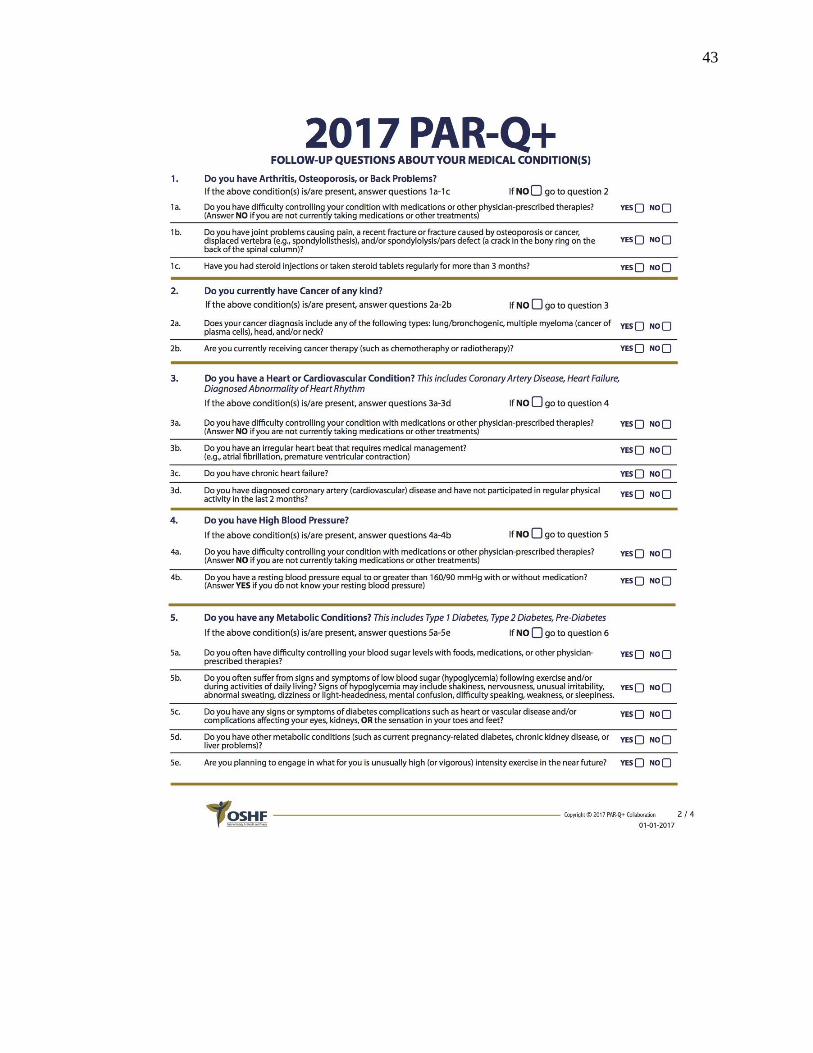
43
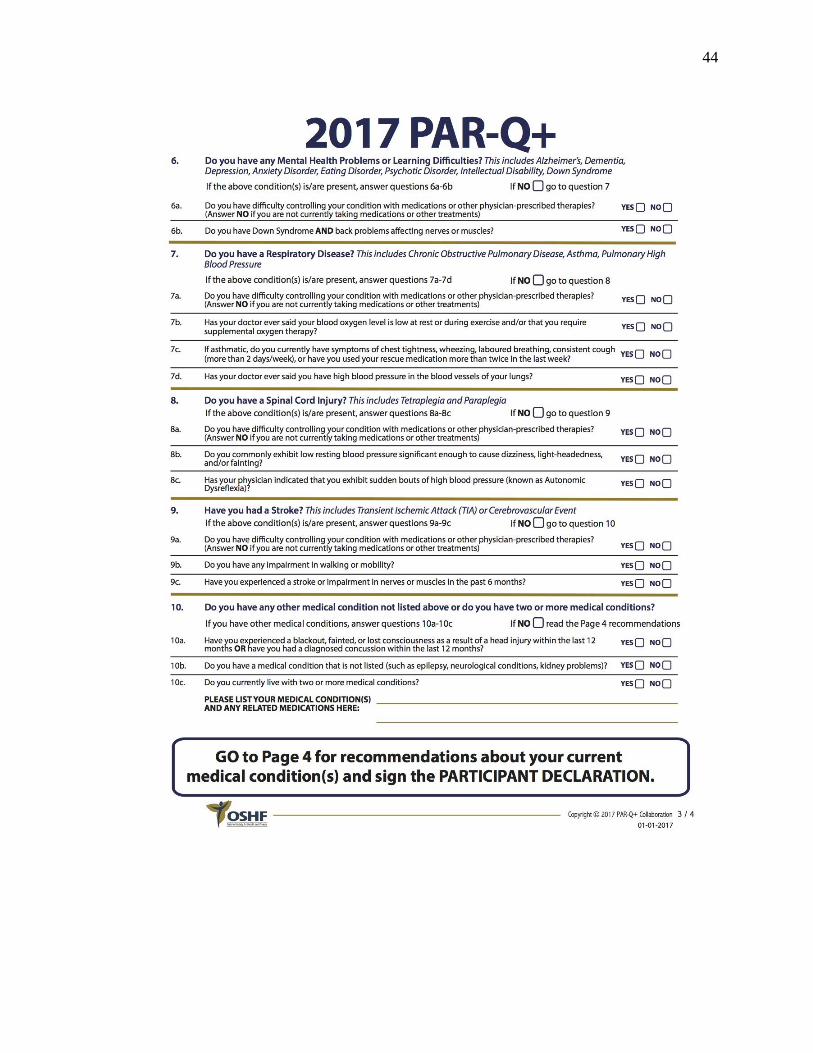
44
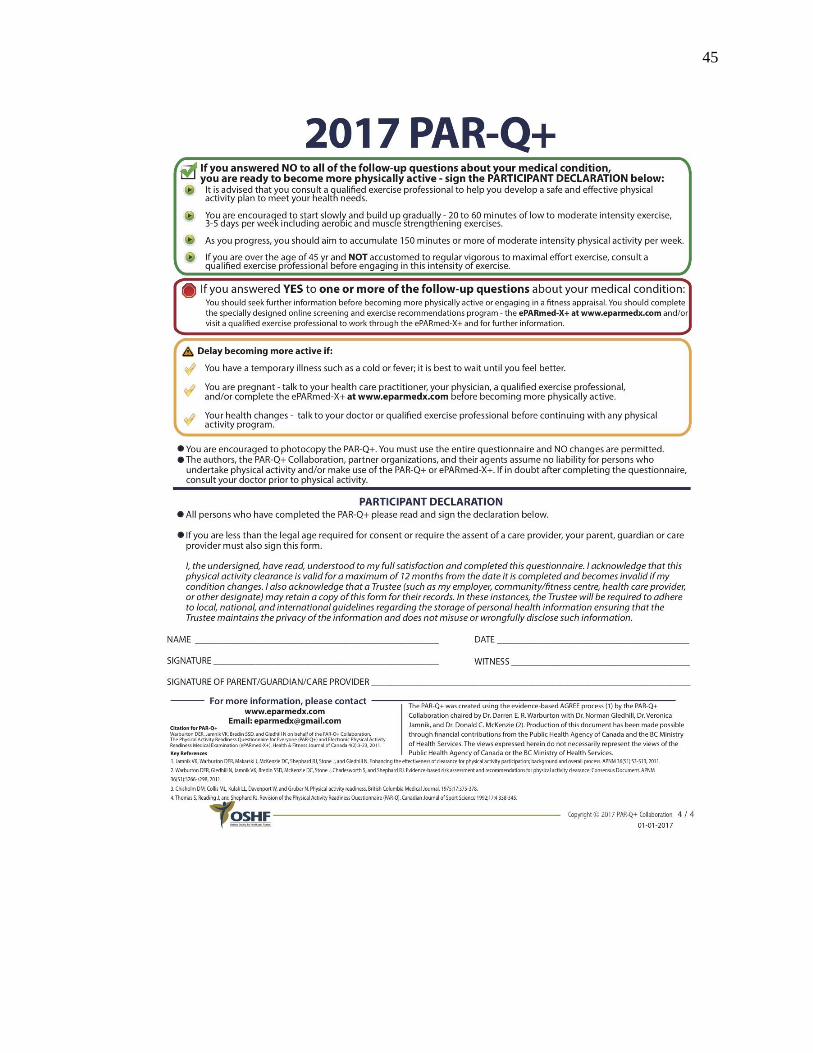
45
46
Appendix C. IPAQ
INTERNATIONAL PHYSICAL ACTIVITY QUESTIONNAIRE (October 2002)
LONG LAST 7 DAYS SELF-ADMINISTERED FORMAT
FOR USE WITH YOUNG AND MIDDLE-AGED ADULTS (15-69 years)
The International Physical Activity Questionnaires (IPAQ) comprises a set of 4 questionnaires. Long (5 activity domains asked independently) and short (4 generic items) versions for use by either telephone or self-administered methods are available. The purpose of the questionnaires is to provide common instruments that can be used to obtain internationally comparable data on health–related physical activity.
Background on IPAQ The development of an international measure for physical activity commenced in Geneva in 1998 and was followed by extensive reliability and validity testing undertaken across 12 countries (14 sites) during 2000. The final results suggest that these measures have acceptable measurement properties for use in many settings and in different languages, and are suitable for national population-based prevalence studies of participation in physical activity.
Using IPAQ Use of the IPAQ instruments for monitoring and research purposes is encouraged. It is recommended that no changes be made to the order or wording of the questions as this will affect the psychometric properties of the instruments.
Translation from English and Cultural Adaptation Translation from English is encouraged to facilitate worldwide use of IPAQ. Information on the availability of IPAQ in different languages can be obtained at www.ipaq.ki.se. If a new translation is undertaken we highly recommend using the prescribed back translation methods available on the IPAQ website. If possible please consider making your translated version of IPAQ available to others by contributing it to the IPAQ website. Further details on translation and cultural adaptation can be downloaded from the website.
Further Developments of IPAQ International collaboration on IPAQ is on-going and an International Physical Activity Prevalence Study is in progress. For further information see the IPAQ website.
More Information More detailed information on the IPAQ process and the research methods used in the development of IPAQ instruments is available at www.ipaq.ki.se and Booth, M.L. (2000). Assessment of Physical Activity: An International Perspective. Research Quarterly for Exercise and Sport, 71 (2): s114-20. Other scientific publications and presentations on the use of IPAQ are summarized on the website.
47
INTERNATIONAL PHYSICAL ACTIVITY QUESTIONNAIRE
We are interested in finding out about the kinds of physical activities that people do as part of their everyday lives. The questions will ask you about the time you spent being physically active in the last 7 days. Please answer each question even if you do not consider yourself to be an active person. Please think about the activities you do at work, as part of your house and yard work, to get from place to place, and in your spare time for recreation, exercise or sport.
Think about all the vigorous and moderate activities that you did in the last 7 days. Vigorous physical activities refer to activities that take hard physical effort and make you breathe much harder than normal. Moderate activities refer to activities that take moderate physical effort and make you breathe somewhat harder than normal.
PART 1: JOB-RELATED PHYSICAL ACTIVITY
The first section is about your work. This includes paid jobs, farming, volunteer work, course work, and any other unpaid work that you did outside your home. Do not include unpaid work you might do around your home, like housework, yard work, general maintenance, and caring for your family. These are asked in Part 3.
1. Do you currently have a job or do any unpaid work outside your home? Yes
No Skip to PART 2: TRANSPORTATION
Yes
No Skip to PART 2: TRANSPORTATION
The next questions are about all the physical activity you did in the last 7 days as part of your paid or unpaid work. This does not include traveling to and from work.
2. During the last 7 days, on how many days did you do vigorous physical activities like heavy lifting, digging, heavy construction, or climbing up stairs as part of your work? Think about only those physical activities that you did for at least 10 minutes at a time.
_____ days per week
No vigorous job-related physical activity Skip to question 4
3. How much time did you usually spend on one of those days doing vigorous physical activities as part of your work?
_____ hours per day
_____ minutes per day
48
4. Again, think about only those physical activities that you did for at least 10 minutes at a time. During the last 7 days, on how many days did you do moderate physical activities like carrying light loads as part of your work? Please do not include walking.
_____ days per week
No moderate job-related physical activity Skip to question 6
5. How much time did you usually spend on one of those days doing moderate physical activities as part of your work?
_____ hours per day
_____ minutes per day
6. During the last 7 days, on how many days did you walk for at least 10 minutes at a time as part of your work? Please do not count any walking you did to travel to or from work.
_____ days per week
No job-related walking Skip to PART 2: TRANSPORTATION
7. How much time did you usually spend on one of those days walking as part of your work?
_____ hours per day
_____ minutes per day
PART 2: TRANSPORTATION PHYSICAL ACTIVITY
These questions are about how you traveled from place to place, including to places like work, stores, movies, and so on.
8. During the last 7 days, on how many days did you travel in a motor vehicle like a train, bus, car, or tram?
_____ days per week
No traveling in a motor vehicle Skip to question 10
49
9. How much time did you usually spend on one of those days traveling in a train, bus, car, tram, or other kind of motor vehicle?
_____ hours per day
_____ minutes per day
Now think only about the bicycling and walking you might have done to travel to and from work, to do errands, or to go from place to place.
10. During the last 7 days, on how many days did you bicycle for at least 10 minutes at a time to go from place to place?
_____ days per week No bicycling from place to place Skip to question 12
No bicycling from place to place Skip to question 12
11. How much time did you usually spend on one of those days to bicycle from place to place?
_____ hours per day
_____ minutes per day
12. During the last 7 days, on how many days did you walk for at least 10 minutes at a time to go from place to place?
_____ days per week
No walking from place to place Skip to PART 3: HOUSEWORK, HOUSE MAINTENANCE, AND CARING FOR FAMILY
13. How much time did you usually spend on one of those days walking from place to place?
_____ hours per day
_____ minutes per day
PART 3: HOUSEWORK, HOUSE MAINTENANCE, AND CARING FOR FAMILY
This section is about some of the physical activities you might have done in the last 7 days in and around your home, like housework, gardening, yard work, general maintenance work, and caring for your family.

50
14. Think about only those physical activities that you did for at least 10 minutes at a time. During the last 7 days, on how many days did you do vigorous physical activities like heavy lifting, chopping wood, shoveling snow, or digging in the garden or yard?
_____ days per week
No vigorous activity in garden or yard Skip to question 16
15. How much time did you usually spend on one of those days doing vigorous physical activities in the garden or yard?
_____ hours per day
_____ minutes per day
16. Again, think about only those physical activities that you did for at least 10 minutes at a time. During the last 7 days, on how many days did you do moderate activities like carrying light loads, sweeping, washing windows, and raking in the garden or yard?
_____ days per week
No moderate activity in garden or yard Skip to question 18
17. How much time did you usually spend on one of those days doing moderate physical activities in the garden or yard?
_____ hours per day
_____ minutes per day
18. Once again, think about only those physical activities that you did for at least 10 minutes at a time. During the last 7 days, on how many days did you do moderate activities like carrying light loads, washing windows, scrubbing floors and sweeping inside your home?
_____ days per week
No moderate activity inside home Skip to PART 4: RECREATION, SPORT AND LEISURE-TIME PHYSICAL ACTIVITY
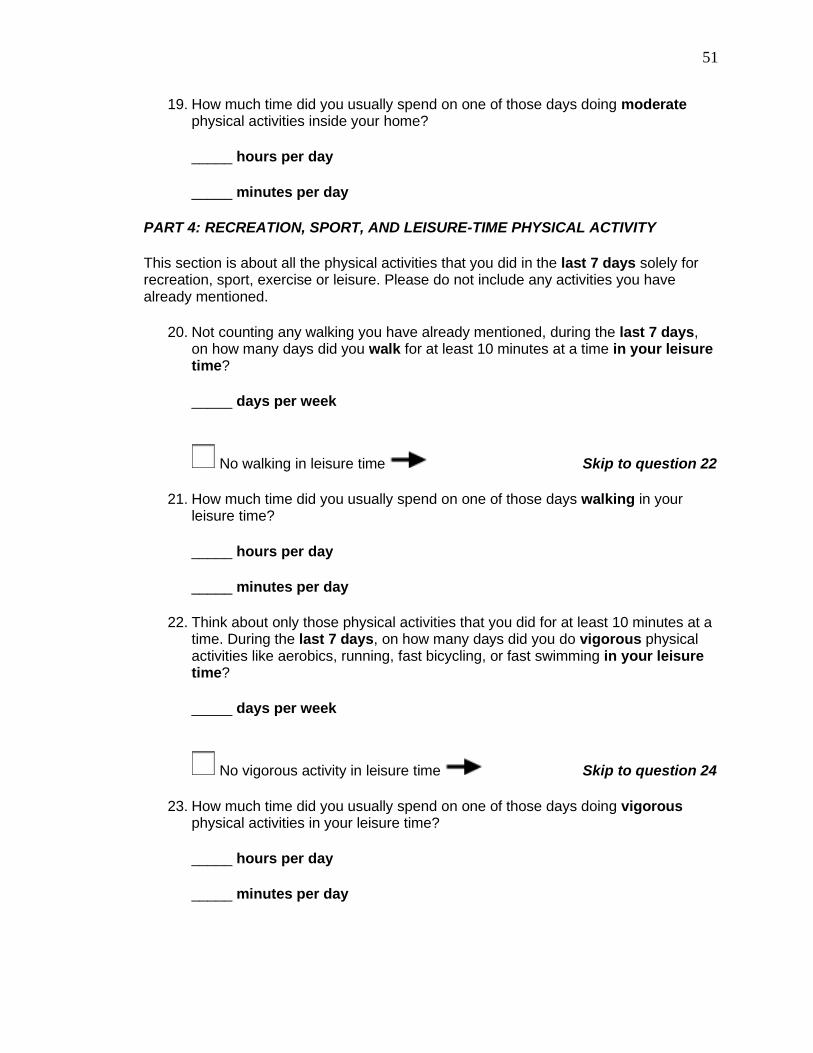
51
19. How much time did you usually spend on one of those days doing moderate physical activities inside your home?
_____ hours per day
_____ minutes per day
PART 4: RECREATION, SPORT, AND LEISURE-TIME PHYSICAL ACTIVITY
This section is about all the physical activities that you did in the last 7 days solely for recreation, sport, exercise or leisure. Please do not include any activities you have already mentioned.
20. Not counting any walking you have already mentioned, during the last 7 days, on how many days did you walk for at least 10 minutes at a time in your leisure time?
_____ days per week
No walking in leisure time Skip to question 22
21. How much time did you usually spend on one of those days walking in your leisure time?
_____ hours per day
_____ minutes per day
22. Think about only those physical activities that you did for at least 10 minutes at a time. During the last 7 days, on how many days did you do vigorous physical activities like aerobics, running, fast bicycling, or fast swimming in your leisure time?
_____ days per week
No vigorous activity in leisure time Skip to question 24
23. How much time did you usually spend on one of those days doing vigorous physical activities in your leisure time?
_____ hours per day
_____ minutes per day

52
24. Again, think about only those physical activities that you did for at least 10 minutes at a time. During the last 7 days, on how many days did you do moderate physical activities like bicycling at a regular pace, swimming at a regular pace, and doubles tennis in your leisure time?
_____ days per week
No moderate activity in leisure time Skip to PART 5: TIME SPENT SITTING
25. How much time did you usually spend on one of those days doing moderate physical activities in your leisure time?
_____ hours per day
_____ minutes per day
PART 5: TIME SPENT SITTING
The last questions are about the time you spend sitting while at work, at home, while doing course work and during leisure time. This may include time spent sitting at a desk, visiting friends, reading or sitting or lying down to watch television. Do not include any time spent sitting in a motor vehicle that you have already told me about.
26. During the last 7 days, how much time did you usually spend sitting on a weekday?
_____ hours per day
_____ minutes per day
27. During the last 7 days, how much time did you usually spend sitting on a weekend day?
_____ hours per day
_____ minutes per day
This is the end of the questionnaire, thank you for participating.
LONG LAST 7 DAYS SELF-ADMINISTERED version of the IPAQ. Revised October 2002.
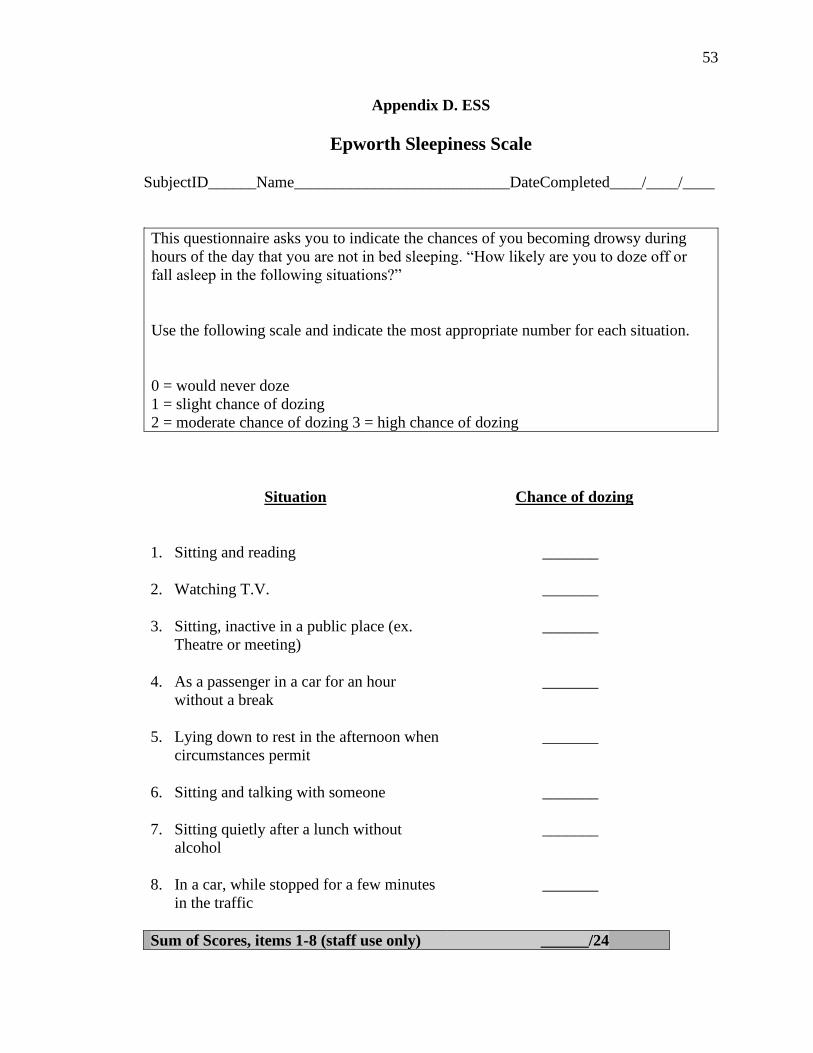
53
Appendix D. ESS
Epworth Sleepiness Scale
SubjectID______Name___________________________DateCompleted____/____/____
This questionnaire asks you to indicate the chances of you becoming drowsy during
hours of the day that you are not in bed sleeping. “How likely are you to doze off or
fall asleep in the following situations?”
Use the following scale and indicate the most appropriate number for each situation.
0 = would never doze
1 = slight chance of dozing
2 = moderate chance of dozing 3 = high chance of dozing
Situation Chance of dozing
1. Sitting and reading
_______
2. Watching T.V. _______
3. Sitting, inactive in a public place (ex.
Theatre or meeting)
_______
4. As a passenger in a car for an hour
without a break
_______
5. Lying down to rest in the afternoon when
circumstances permit
_______
6. Sitting and talking with someone _______
7. Sitting quietly after a lunch without
alcohol
_______
8. In a car, while stopped for a few minutes
in the traffic
_______
Sum of Scores, items 1-8 (staff use only) ______/24
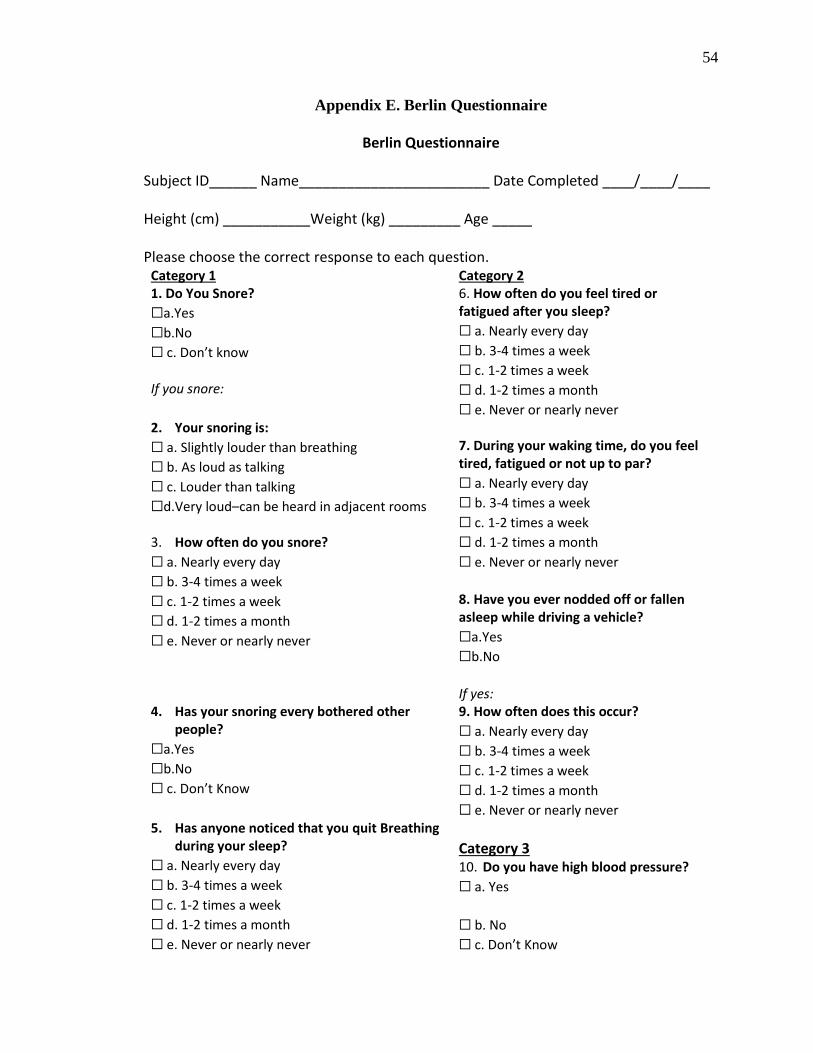
54
Appendix E. Berlin Questionnaire
Berlin Questionnaire
Subject ID______ Name________________________ Date Completed ____/____/____
Height (cm) ___________Weight (kg) _________ Age _____
Please choose the correct response to each question. Category 1 Category 2 1. Do You Snore?
☐a.Yes
☐b.No
☐ c. Don’t know
6. How often do you feel tired or fatigued after you sleep?
☐ a. Nearly every day
☐ b. 3-4 times a week
☐ c. 1-2 times a week
☐ d. 1-2 times a month
☐ e. Never or nearly never
If you snore:
2. Your snoring is:
☐ a. Slightly louder than breathing
☐ b. As loud as talking
☐ c. Louder than talking
☐d.Very loud–can be heard in adjacent rooms
7. During your waking time, do you feel tired, fatigued or not up to par?
☐ a. Nearly every day
☐ b. 3-4 times a week
☐ c. 1-2 times a week
☐ d. 1-2 times a month
☐ e. Never or nearly never
3. How often do you snore?
☐ a. Nearly every day
☐ b. 3-4 times a week
☐ c. 1-2 times a week
☐ d. 1-2 times a month
☐ e. Never or nearly never
8. Have you ever nodded off or fallen asleep while driving a vehicle?
☐a.Yes
☐b.No
If yes:
4. Has your snoring every bothered other people?
☐a.Yes
☐b.No
☐ c. Don’t Know
9. How often does this occur?
☐ a. Nearly every day
☐ b. 3-4 times a week
☐ c. 1-2 times a week
☐ d. 1-2 times a month
☐ e. Never or nearly never 5. Has anyone noticed that you quit Breathing
during your sleep?
☐ a. Nearly every day
☐ b. 3-4 times a week
☐ c. 1-2 times a week
☐ d. 1-2 times a month
☐ e. Never or nearly never
Category 3 10. Do you have high blood pressure?
☐ a. Yes
☐ b. No
☐ c. Don’t Know
55
References
Acevedo M, Varleta P, Kramer V, et al. Comparison of lipoprotein-associated
phospholipase A2 and high sensitive C-reactive protein as determinants of
metabolic syndrome in subjects without coronary heart disease: In search of the
best predictor. International Journal of Endocrinology 2015;2015:934681.
Aiello KD, Caughey WG, Nelluri B, Sharma A, Mookadam F, Mookadam M. (2016).
Effect of exercise training on sleep apnea: a systematic review and meta-analysis.
Respiratory medicine. 2016;116:85-92.
Atkeson A, Yeh SY, Malhotra A, Jelic S. (2009). Endothelial function in obstructive
sleep apnea. Progress in cardiovascular diseases. 2009;51(5):351-362.
Awad KM, Malhotra A, Barnet JH, Quan SF, Peppard PE. Exercise is associated with a
reduced incidence of sleep-disordered breathing. The American journal of
medicine. 2012;125(5):485-490.
Badr EA, Yousif M, Hazzaa SM. Lipoprotein-associated phospholipase A2 levels as a
predictor of cardiovascular risks in patients with COPD and obstructive sleep
apnea. Egyptian Journal of Chest Diseases and Tuberculosis, 2014;63(2):405-
410.
Bekci TT, Kayrak M, Kiyici A, et al. The association among lipoprotein-associated
phospholipase A2 levels, total antioxidant capacity and arousal in male patients
with OSA. International journal of medical sciences. 2011;8(5):369.
Benitez S, Camacho M, Arcelus R et al. Increased lyso phosphatidylcholine and non-
esterified fatty acid content in LDL induces chemokine release in endothelial
cells: relationship with electronegative LDL. Atherosclerosis. 2004;177(2):299–
305.
Bratel T, Wennlund A, Carlstrom K. Pituitary reactivity, androgens and catecholamines
in obstructive sleep apnoea: effects of continuous positive airway pressure
treatment (CPAP). Respir Med. 1999;93(1):1–7.
Brilakis ES, Khera A, McGuire DK, et al. Influence of race and sex on lipoprotein-
associated phospholipase A2 levels: observations from the Dallas Heart Study.
Atherosclerosis. 2008;199(1):110-5.
56
Cai A, Zheng D, Qiu R, Mai W, Zhou Y. Lipoprotein-associated phospholipase A2 (Lp-
PLA2): a novel and promising biomarker for cardiovascular risks assessment.
Disease Markers. 2013;34(5):323-331.
Caslake MJ, Packard CJ, Suckling KE, Holmes SD, Chamberlain P, Macphee CH.
Lipoprotein-associated phospholipase A2, platelet-activating factor
acetylhydrolase: a potential new risk factor for coronary artery disease.
Atherosclerosis. 2000;150(2):413–419.
Chastin SF, De Craemer M, De Cocker K, et al. How does light-intensity physical
activity associate with adult cardiometabolic health and mortality? Systematic
review with meta-analysis of experimental and observational studies. Br J Sports
Med. 2019;53(6):370-376.
Corson MA, Jones PH, Davidson MH. Review of the evidence for the clinical utility of
lipoprotein-associated phospholipase A2 as a cardiovascular risk marker. Am J
Cardiol. 2008;101(12):S41–S50.
Craig CL, Marshall AL, Sjöström M, et al. International physical activity questionnaire:
12-country reliability and validity. Medicine & science in sports & exercise.
2003;35(8):1381-1395.
Dada N, Kim NW, Wolfert RL. Lp-PLA2: an emerging biomarker of coronary heart
disease. Expert review of molecular diagnostics. 2002;2(1):17-22.
Davidson MH, Corson MA, Alberts MJ, et al. Consensus panel recommendation for
incorporating lipoprotein-associated phospholipase A2 testing into cardiovascular
disease risk assessment guidelines. The American journal of cardiology.
2008;101(12):S51-S57.
Delgado P, Chacón P, Penalba A, et al. Temporal profile and prognostic value of Lp-
PLA2 mass and activity in the acute stroke setting. Atherosclerosis.
2012;220(2):532-536.
Dohrn M, Sjöström M, Kwak L, Oja P, Hagströmer M. Accelerometer-measured
sedentary time and physical activity—a 15 year follow-up of mortality in a
Swedish population-based cohort. Journal of science and medicine in sport.
2018;21(7):702-707.
57
Ekelund U, Besson H, Luan JA, et al. Physical activity and gain in abdominal adiposity
and body weight: prospective cohort study in 288,498 men and women. The
American journal of clinical nutrition. 2011;93(4):826-835.
Guerra R, Zhao B, Mooser V, Stafforini D, Johnston JM, Cohen JC. Determinants of
plasma platelet-activating factor acetylhydrolase: heritability and relationship to
plasma lipoproteins. Journal of lipid research. 1997;38(11):2281-2288.
Hakkinen T, Luoma JS, Hiltunen MO, et al. Lipoprotein- associated phospholipase A(2),
platelet-activating factor acetylhydrolase, is expressed by macrophages in human
and rabbit atherosclerotic lesions. Arterioscler Thromb Vasc Biol.
1999;19(12):2909-17.
Hargens TA, Martin RA, Strosnider CL, Giersch GEW, Womack CJ. Obstructive sleep
apnea negatively impacts objectively measured physical activity. Sleep and
Breathing. 2019;23(2):447-454.
Hargens TA, Rhodes PG, VanReenen J, Kaminsky LA. Lipoprotein-associated
phospholipase A2 and carotid intima-media thickness in individuals classified as
low-risk according to Framingham. Cardiovascular diagnosis and therapy.
2014;4(6):487.
Healy GN, Matthews CE, Dunstan DW, Winkler EA, Owen N. Sedentary time and
cardio-metabolic biomarkers in US adults: NHANES 2003–06. European heart
journal. 2011;32(5):590-597.
Horner R, Mohiaddin R, Lowell D, Shea SA, Burman ED, Longmore DB, Guz A. Sites
and sizes of fat deposits around the pharynx in obese patients with obstructive
sleep apnoea and weight matched controls. Eur Respir J. 1989;2(7):613–622.
Huiguo L, Jin L, Shengdao X, Guanxin S, Zhenxiang Z, Yongjian X. The change of
interleukin-6 and tumor necrosis factor in patients with obstructive sleep apnea
syndrome. Journal of Tongji Medical University. 2000;20(3):200-202.
Iftikhar IH, Kline CE, Youngstedt SD. Effects of exercise training on sleep apnea: a
meta-analysis. Lung. 2014;192(1):175-184.
Jackisch L, Kumsaiyai W, Moore JD, et al. Differential expression of Lp-PLA2 in
obesity and type 2 diabetes and the influence of lipids. Diabetologia.
2018;61(5):1155-1166.
58
Janssen I, Katzmarzyk PT, Ross R. Waist circumference and not body mass index
explains obesity-related health risk. The American journal of clinical nutrition.
2004;79(3):379-384.
Johns, M. W. Reliability and factor analysis of the Epworth Sleepiness Scale. Sleep.
1992;15(4):376-381.
Kang K, Park KS, Kim JE, Kim SW, Kim YT, Kim JS, Lee HW. Usefulness of the Berlin
Questionnaire to identify patients at high risk for obstructive sleep apnea: a
population-based door-to-door study. Sleep and Breathing. 2013;17(2):803-810.
Kelly LA, McMillan DG, Anderson A, Fippinger M, Fillerup G, Rider J. Validity of
actigraphs uniaxial and triaxial accelerometers for assessment of physical activity
in adults in laboratory conditions. BMC medical physics. 2013;13(1):5.
Kline CE, Crowley EP, Ewing GB, et al. The effect of exercise training on obstructive
sleep apnea and sleep quality: a randomized controlled trial. Sleep.
2011;34(12):1631-1640.
Kokkinos P. Physical activity, health benefits, and mortality risk. ISRN cardiology. 2012.
Kolodgie FD, Burke AP, Skorija KS et al. Lipoprotein-associated phospholipase A2
protein expression in the natural progression of human coronary atherosclerosis.
Arterioscler Thromb Vasc Biol. 2006;26(11):2523–9.
Kubitz KA, LandersDM, Petruzzello SJ, Han M. The effects of acute and chronic
exercise on sleep: a meta-analytic review. Sports Med. 1996;21(4):277-291.
Lanman RB, Wolfert RL, Fleming JK, et al. Lipoprotein- associated phospholipase A2:
review and recommendation of a clinical cut point for adults. Prev Cardiol.
2006;9(3):138-43.
Lavi S, McConnell JP, Rihal CS, et al. Local production of lipoprotein-associated
phospholipase A2 and lysophosphatidylcholine in the coronary circulation:
association with early coronary atherosclerosis and endothelial dysfunction in
humans. Circulation. 2007;115(21):2715-21.
Lee IM, Paffenbarger Jr RS. Associations of light, moderate, and vigorous intensity
physical activity with longevity: the Harvard Alumni Health Study. American
journal of epidemiology. 2000;151(3):293-299.
59
Lee W, Nagubadi S, Kryger MH, Mokhlesi B. Epidemiology of obstructive sleep apnea:
a population-based perspective. Expert Rev Respir Med. 2008;2(3):349-364.
Mannheim D, Herrmann J, Versari D, et al. Enhanced expression of Lp-PLA2 and
lysophosphatidylcholine in symptomatic carotid atherosclerotic plaques. Stroke.
2008;39(5):1448-1455.
Moise LG, Marta DS, Raşcu A, Moldoveanu E. Serum Lipoprotein-Associated
Phospholipase A2 in Males With Metabolic Syndrome and Obstructive Sleep
Apnea. Acta Endocrinologica (Bucharest). 2018;14(1):36.
Narkiewicz K, Montano N, Cogliati C, van de Borne PJ, Dyken ME, Somers VK. Altered
cardiovascular variability in obstructive sleep apnea. Circulation.
1998;98(11):1071–1077.
National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation,
and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III).
Third Report of the National Cholesterol Education Program (NCEP) Expert
Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in
Adults (Adult Treatment Panel III) nal report. Circulation. 2002;106(25):3143-
421.
Ng SSS, Chan TO, To KW, et al. Validation of a portable recording device (ApneaLink)
for identifying patients with suspected obstructive sleep apnoea syndrome.
Internal medicine journal. 2009;39(11):757-762.
Norman JF, Von Essen SG, Fuchs RH, McElligott M. Exercise training effect on
obstructive sleep apnea syndrome. Sleep Res Online. 2000;3(3):121-9.
Paik JK, Kim M, Kim M, et al. Circulating Lp-PLA 2 activity correlates with oxidative
stress and cytokines in overweight/obese postmenopausal women not using
hormone replacement therapy. Age. 2015;37(2):32.
Park HS, Park JY, Yu R. Relationship of obesity and visceral adiposity with serum
concentrations of CRP, TNF-α and IL-6. Diabetes research and clinical practice.
2005;69(1):29-35.
Peker Y, Hedner J, Norum J, Kraiczi H, Carlson J. Increased incidence of cardiovascular
disease in middle-aged men with obstructive sleep apnea: a 7-year follow-up.
American journal of respiratory and critical care medicine. 2002;166(2):159-165.
60
Peled N, Greenberg A, Pillar G, Zinder O, Levi N, Lavie P. (1998). Contributions of
hypoxia and respiratory disturbance index to sympathetic activation and blood
pressure in obstructive sleep apnea syndrome. American journal of
hypertension. 1998;11(11):1284-1289.
Peppard PE, Young T, Barnet JH, Palta M, Hagen EW, Hla KM. Increased prevalence of
sleep-disordered breathing in adults. American journal of epidemiology.
2013;177(9):1006-1014.
Peppard PE, Young T, Palta M, Dempsey J, Skatrud J. Longitudinal study of moderate
weight change and sleep-disordered breathing. Jama. 2000;284(23):3015-3021.
Peppard PE, Young T, Palta M, Skatrud J. Prospective study of the association between
sleep-disordered breathing and hypertension. N Engl J Med. 2000;342(19):1378-
84.
Peppard PE, Young T. Exercise and sleep-disordered breathing: an association
independent of body habitus. Sleep. 2004;27(3):480-484.
Persson M, Hedblad B, Nelson JJ, Berglund G. Elevated Lp-PLA2 levels add prognostic
information to the metabolic syndrome on incidence of cardiovascular events
among middle-aged nondiabetic subjects. Arteriosclerosis, Thrombosis, and
Vascular Biology. 2007;27(6):1411-1416.
Persson M, Nilsson JÅ, Nelson JJ, Hedblad B, Berglund G. The epidemiology of Lp-
PLA2: Distribution and correlation with cardiovascular risk factors in a
population-based cohort. Atherosclerosis. 2007;190(2):388-396.
Phillips BG, Kato M, Narkiewicz K, Choe I, Somers VK. Increases in leptin levels,
sympathetic drive, and weight gain in obstructive sleep apnea. Am J Physiol.
2000;279(1):H234–H237.
Pichot V, Busso T, Roche F, et al. Autonomic adaptations to intensive and overload
training periods: a laboratory study. Med Sci Sports Exerc. 2002;34(10):1660e6.
Plat L, Leproult R, L’Hermite-Baleriaux M, et al. Metabolic effects of short-term
elevations of plasma cortisol are more pronounced in the evening than in the
morning. J Clin Endocrinol Metab. 1999;84(9):3082–92.
61
Punjabi NM, Shahar E, Redline S, Gottlieb DJ, Givelber R, Resnick HE. Sleep-
disordered breathing, glucose intolerance, and insulin resistance: the Sleep Heart
Health Study. Am J Epidemiol. 2004;160(6):521–530.
Punjabi NM. The epidemiology of adult obstructive sleep apnea. Proc Am Thorac Soc.
2008;5(2):136-143.
Quan SF, O’Connor GT, Quan JS, et al. Association of physical activity with sleep-
disordered breathing. Sleep and Breathing. 2007;11(3):149-157.
Quinn M, Parthasarathy S, Steinberg D. Lysophosphatidylcholine: a chemotactic factor
for human monocytes and its potential role in atherogenesis. Proc Natl Acad Sci.
1988;85(8):2805–9.
Rana JS, Arsenault BJ, Després JP, et al. Inflammatory biomarkers, physical activity,
waist circumference, and risk of future coronary heart disease in healthy men and
women. European Heart Journal. 2011;32(3):336-344.
Riebe D, Ehrman JK, Liguori G, Magal M. ACSM's Guidelines for Exercise Testing and
Prescription. 10th ed. Philadelphia: Wolters Kluwer; 2018.
Savransky V, Nanayakkara A, Li J, et al. Chronic intermittent hypoxia induces
atherosclerosis. Am J Respir Crit Care Med. 2007;175(12):1290-1297.
Schwartz AR, Gold AR, Schubert N, Stryzak A, Wise AR, Permutt S, Smith PL. Effect
of weight loss on upper airway collapsibility on obstructive sleep apnoea 1-3. Am
Rev Respir Dis. 1991;144(3 pt 1):494–498.
Sengul YS, Ozalevli S, Oztura I, Itil O, Baklan B. The effect of exercise on obstructive
sleep apnea: a randomized and controlled trial. Sleep Breath. 2011;15(1):49-56.
Shi Y, Zhang P, Zhang L et al. Role of lipoprotein-associated phospholipase A2 in
leukocyte activation and inflammatory responses. Atherosclerosis.
2007;191(1):54–62.
Silverberg DS, Oksenberg A. Are sleep-related breathing disorders important
contributing factors to the production of essential hypertension?. Current
Hypertension Reports. 2001;3(3):209-215.
Somers VK, White DP, Amin R, et al. Sleep apnea and cardiovascular disease: An
American heart association/American college of cardiology foundation scientific
statement from the American heart association council for high blood pressure
62
research professional education committee, council on clinical cardiology, stroke
council, and council on cardiovascular nursing in collaboration with the national
heart, lung, and blood institute national center on sleep disorders research
(national institutes of health). Journal of the American College of Cardiology,
2008;52(8):686-717.
Stafforini DM. Plasma PAF-AH (PLA2G7): Biochemical properties, association with
LDLs and HDLs, and regulation of expression. The Enzymes. 2015;38:71–93.
Sytkowski PA, Kannel WB, D’Agostino RB. Changes in risk factors and the decline in
mortality from cardiovascular disease: The Framingham Heart Study. N. Engl. J.
Med. 1990;322(23):1635–1641.
Thompson A, Gao P, Orfei L, et al. Lipoprotein-associated phospholipase A(2) and risk
of coronary disease, stroke, and mortality: Collaborative analysis of 32
prospective studies. Lancet. 2010;375(9725):1536-44.
Tudor-Locke C, Craig CL, Thyfault JP, Spence JC. A step-defined sedentary lifestyle
index:< 5000 steps/day. Applied physiology, nutrition, and metabolism.
2013;38(2):100-114.
Tzotzas T, Filippatos TD, Triantos A, Bruckert E, Tselepis AD, Kiortsis DN. (2008).
Effects of a low-calorie diet associated with weight loss on lipoprotein-associated
phospholipase A2 (Lp-PLA2) activity in healthy obese women. Nutrition,
Metabolism and Cardiovascular Diseases. 2008;18(7):477-482.
Vgontzas AN, Tan TL, Bixler EO, Martin LF, Shubert D, Kales A. Sleep apnea and sleep
disruption in obese patients. Arch Intern Med. 1994;154(15):1705–1711.
Vincent HK, Shanely RA, Stewart DJ, et al. Adaptation of upper airway muscles to
chronic endurance exercise. Am J Respir Crit Care Med. 2002;166(3):287-93.
Weaver TE, Grunstein RR. Adherence to continuous positive airway pressure therapy:
the challenge to effective treatment. Proc Am Thorac Soc. 2008;5(2):173-178.
Wolk R, Shamsuzzaman AS, Somers VK. Obesity, sleep apnea, and hypertension.
Hypertension. 2003;42(6):1067-1074.
Xu C, Yu F, Mao S, et al. Lipoprotein-associated phospholipase A2 predicted
cardiovascular disease in obstructive sleep apnea syndrome. Respiratory
Medicine. 2020;163:105881.
63
Young T, Peppard PE, Gottlieb DJ. Epidemiology of obstructive sleep apnoea: a
population health perspective. Am J Respir Crit Care Med. 2002;165(9):1217–
1239.
Zhu S, Wang Z, Heshka S, Heo M, Faith MS, Heymsfield SB. Waist circumference and
obesity-associated risk factors among whites in the third National Health and
Nutrition Examination Survey: clinical action thresholds. The American journal of
clinical nutrition. 2002;76(4):743-743.



![Secreted phospholipase A , lipoprotein hydrolysis, …...biochemistry and biology of the sPLA 2 family have been detailed in recent reviews [1, 2]. Lipoprotein hydrolysis by sPLA2s:](https://static.fdocuments.us/doc/165x107/5fcdd9bba9390b4c301838ae/secreted-phospholipase-a-lipoprotein-hydrolysis-biochemistry-and-biology.jpg)














