
leslieandersonprofessionalportfo.weebly.comleslieandersonprofessionalportfo.weebly.com/uploads/1/3/... ·...
33
Ketogenic Diet as Treatment for Seizures A Case Study
Transcript of leslieandersonprofessionalportfo.weebly.comleslieandersonprofessionalportfo.weebly.com/uploads/1/3/... ·...
Ketogenic Diet as Treatment for SeizuresA Case Study

Introduction:
GH was a child admitted to the Primary Children’s Medical Center (PCMC) for four-day
consistent fever and a purple macular rash on her face and upper extremities on August 25, 2011. While
in the emergency department (ED) she experienced a tonic clonic seizure. She was then admitted to the
pediatric intensive care unit (PICU) for treatment. Several days previous to this, she was seen at urgent
care and tested positive for E. coli and was started on antibiotics. She reported symptoms of a fever,
decreased oral intake, and mild upper respiratory infection (URI) including a stuffy nose, sore throat,
swollen lymph gland on the left neck. Her mother called her primary medical doctor (PMD) and was
instructed to go to the ED on 8/23. She was seen, treated, and sent home with the belief that she had a
viral component to her illness. Her mother stated she appeared to be improving until 8/25 when she
awoke early in the AM confused and lethargic. Upon this time she was brought to the ED at PCMC. This
case study will discuss her past social and medical history and her treatment and progress at PCMC as
well as an overview of the use of the ketogenic diet (KD) for treatment of seizures.
Social History:
GH is a 9-year 2-month old Caucasian female residing with her father, mother, and younger
sister in the Syracuse, Utah. She recently started 4th grade and reportedly enjoys and does well in
school.
Medical History:
GH has a history of urinary reflux that was resolved by age 2. She has had no urinary tract
infections since. Other than this, GH is a previously healthy child. Family history is significant for
diabetes mellitus and heart disease. Maternal grandmother recently diagnosed with uterine cancer.
The Ketogenic Diet as Treatment for Seizures

The ketogenic diet (KD) is used as a form of treatment for seizures (1). An individual
participating in a KD is forced to produce ketones to provide energy for the body, specifically
acetoacetate and beta-hydroxybutyrate (BHB) for the brain (2). Originally, fasting was used as a way to
force individuals to undergo ketosis but the KD has provided a way to obtain nutrition while still
receiving the metabolic effects of fasting (2). The mechanism in which the KD produces an
anticonvulsant effect is not completely understood, but it is believed that the ketone bodies produced
by individuals undergoing treatment inhibit neurotransmissions that cause seizure episodes (1). Upon
initiation of the diet, strict adherence must be kept in order for it to remain effective as a treatment for
seizures (2).
The KD consists of high fat, moderate protein and low carbohydrates (2). Often it was begun
with fasting, but it has been found that fasting is not a necessary process in the initiation of KD (2).
Typically individuals would participate in a 24 to 72 hour fast, or until ketone levels of 4+ were present in
the urine (1). It has been found that there is no positive outcome with fasting to initiate the KD
treatment, as seizure reduction at three months was similar for those who initiated the KD with a fast
and those who did not (2). Individuals who did not participate in the typical fast, have fewer negative
side effects of hypoglycemia and emesis, which ultimately results in decreased length of hospital stay
(2).
When designing a KD treatment plan, there are several routes available to take. There are two
widely used types of KD plans, traditional and medium chain triglyceride (MCT) (2). Developed in the
1920s, the traditional, or classic, KD approach includes a 4:1 ratio for fat to non-fat calories (1). For
children, fat is typically given at 75% of total daily intake (1). The main sources of fat in a KD include
vegetable oil, butter, and heavy cream (2). The non fat calories include both protein and carbohydrate,
with protein provided at a higher percentage than carbohydrates in order to maintain ketosis as well as

provide needed amino acids for growth (1). Protein is typically provided around the range of 1 g/kg/day
(1). Low-carbohydrate fruits and vegetables are allowed, while sugar, breads, pastas, grains, and high-
carbohydrate fruits and vegetables are not allowed on the classic KD (2). Also, a fluid restriction of 2
L/day is used to prevent dilution of the ketone levels (1). To ensure adequate nutrition,
multi-vitamin/mineral and extra calcium supplements are included in the treatment plan (1).
The MCT-based KD is the second available approach to the treatment of seizures with ketosis
(1). MCT were first used due to their increased palatability over the traditional diet, as MCT oil is
odorless, colorless, and tasteless (1). MCTs are also a preferred source of fat due to more easily
achieved ketosis than with the long-chain triglycerides used in the traditional diet, resulting in a ratio of
fat to nonfat calories of 1:1 (1,2). In the MCT diet, 70% of calories come from fats (2). 50% of the fat
calories are MCT and the remaining 20% consist of polyunsaturated fatty acids (2). This allows for more
fruits and vegetables, and even small amounts of breads and other starches to be consumed on this diet
(1). Fluid restrictions are not warranted in the MCT KD plan (1).
Two newer versions of the KD treatment have emerged, the low-glycemic-index treatment and
the modified Atkins diet (2). The low-glycemic-index treatment plan consists of a diet with two main
guidelines to be followed: 60% of calories from fat and an elimination of foods with a glycemic index
rating greater than 50 (2). Protein is provided at the rate of 1 g/kg/day (2). The modified Atkins
treatment plan consists of a diet of 65% of calories from fat and limited carbohydrates (2). Both of the
newer variations of the KD have no published studies to assure their efficacy, however short term use
has shown positive outcomes (2).
Adherence to a KD may be difficult for some individuals, especially adolescents and teenagers,
due to decreased palatability and complexity of meal planning (1,2). As such, a ratio of 2:1 or 1:1 fat to
protein and carbohydrate may be used initially (2). Starting KD treatment earlier in life results in better

compliance (2). This makes it advisable to initiate the KD as early as possible with individuals suffering
from seizures (2). Participating in KD treatment is not only complex due to the limitation on foods
individuals are able to consume, but also because individuals and their caregivers must learn to read
labels and weigh their foods to ensure the adequate ratio of fat to nonfat grams (2).
Adherence to the KD treatment may be negatively affected by the side effects (2). Constipation
is the most commonly reported side affect of KD (2). Other undesirable side effects include: diarrhea,
abdominal pain, gastroesophageal reflux disease, nephrolithiasis, growth retardation and abnormal
laboratory values(1,2). As the individual is unable to consume a well balanced diet, nutritional side
effects such as hypoproteinemia and micronutrient deficiencies occur (2). More complex problems that
can be caused by following a KD include pancreatitis, hemolytic anemia, and Fanconi renal tubular
acidosis (2). These negative side affects must be weighed against the positive outcomes of seizure
reduction to determine if the KD is an effective treatment for each individual (1).
In a study of infants with a mean age of 1.2, both length and weight were lower than normal
after six months of participating in the KD treatment (3). Over the six month period normal length and
weight growth for age was 6.1 cm and 1.5 kg respectively, with infants on the KD only gaining 5.1 cm
and 1.4 kg (3). A long-term survey consisting of questionnaires completed by individuals or caregivers
has shown a limited catch-up growth (4). Although the majority of individuals who had participated in
KD treatment were smaller in stature and weight, their complete metabolic panel laboratory values
were generally found to be normalized upon cessation of the diet (4). Abnormal lipid levels were also
found to normalize with time even for those still actively following the KD (4).
Although there are various unpleasant side effects of following a KD, the positive effect of
decreased seizures may likely outweigh the negative (1). Decreased events may be seen as quickly as
one to three months of initiating the diet (2). The study of infants showed a greater than 50%

improvement in spasms for 64% of study participants after 6 months, which increased to 77%
improvement after 1-2 years (3). After a median of 2.4 months, 37% of infants were seizure-free for a
period of six months (3). Developmental improvements were found in 67% of infants and
electroencephalogram (EEG) improvement was found in 32% of infants (3). Thirty percent of study
participants were able to decrease the number of anticonvulsants while on KD (3). Also important to
note, is the greater than 90% improvement in spasms for infants starting the KD treatment who had
tried fewer anticonvulsant medications and were older at onset of spasms (3). As reported by caregivers
and individuals in the long-term survey, 80% experienced fewer seizures than before starting the KD (4).
Although most individuals and caregivers would not use the KD as a first-line treatment, they
would use it after no more than two other treatment options had unsuccessfully been tried (4). The diet
is discontinued immediately if episodes worsen or the adverse effects are not handled well by the
individual (2). If no progress has been made with seizures after three and a half months on the KD, a
rapid discontinuation is recommended (2). If KD is effective as a treatment for seizures, the diet is
tapered to a more normalized after two years (1). The fat to nonfat ratio is gradually decreased,
allowing more carbohydrates and protein in the diet until ketosis no longer occurs (2).
Anthropometrics:
GH was 142.2 cm (91%ile) and weighed 28.8 kg (46%ile) upon admit. Her BMI was calculated to
be 14.3, which is at the 11%ile for age. Her IBW was36 kg, with an IBW of 80%. No previous weights
were available as this was her first hospitalization. Mother reported no concerns with growth prior to
hospitalization.
Medications:

GH was currently receiving several medications while at PCMC. She was receiving vitamin D,
calcium and carnitine dietary supplements. Her vitamin D supplementation was in the form of calciferol
and her calcium supplementation was in the form of calcium carbonate. She also received carnitor to
increase her carnitine levels, as her levels were being depleted by Depakote, an antiepileptic
medication. She was receiving Pentobarbital and Versed to keep her sedated. Norcuron was given pro
re nata (prn) to assist in muscle relaxation for her endotracheal intubation as well as another paralyzing
agent. She was receiving methylpredisone and cellcept to assist in autoimmune and inflammation
control. She was receiving several medications to assist in preventing epileptic episodes including:
Topamax, Lacosamide, Keppra, Depakote, Vimpat, and Felbatol. The ketogenic diet (KD) was also
initiated as treatment for epilepsy. Chlorhexidine was used as an antibacterial oral rinse and
Triamcinolone Acetonide was used to treat tongue ulcers. Potassium citrate was being administered as
a urinary alkilizer. She was also receiving several maintanence medications including Prevacid for
gastrointestinal (GI) ulcer prophylaxis and Lacrilube as an ocular lubricant. PRN she was receiving
intravenous (IV) fluids of NaCl 0.9%, Tylenol, Motrin, Zantac, Benadryl and Miralax.
Laboratory Data:
The following tables contain laboratory data pertinent to current diagnosis:
Date Ketones, Urine (mg/dl)
Normal Negative, Desired level while on
Ketogenic Diet is 4+
9/29 Negative
9/28 1+ H
9/27 1+ H
9/26 Negative
9/25 Negative
9/24 Negative

9/23 Trace H
9/22 Trace H
9/21 Trace H
9/20 Trace H
9/19 Trace H
9/18 2+ H
9/17 3+ H
9/16 3+ H
9/15 2+ H
9/14 3+ H
9/12 1+ H
9/11 1+ H
9/10 1+ H
9/9 Negative
The ketones are present in the diet due to ketogenic diet administration, and are therefore
desirable. The desired level of 4+ was never reached upon the duration of the ketogenic diet
treatment.
Date Whole Blood GlucoseNormal 60-115 mg/dL
9/27 169 H
9/19 81
9/18 177 H
9/17 119 H
9/15 94
9/14 79
9/13 93
9/13 103
9/13 75
9/12 95
9/12 89

9/12 99
9/12 98
9/11 93
9/11 84
9/10 77
9/10 85
9/9 90
9/9 91
9/3 158 H
9/3 152 H
9/2 126 H
9/1 155 H
9/1 132 H
9/1 121 H
High blood glucose levels likely associated with stress as GH was in critical condition. Steroid
administration also likely contributed to elevated blood glucose levels.
Date Valproic Acid (ug/dl)Normal 50-125
9/28 58.9
9/27 73.8
9/26 55.4
9/25 57.5
9/24 67.9
9/23 63.9
9/22 71.4
9.21 67.4
9/20 60.6
9/19 50.6
9/18 52
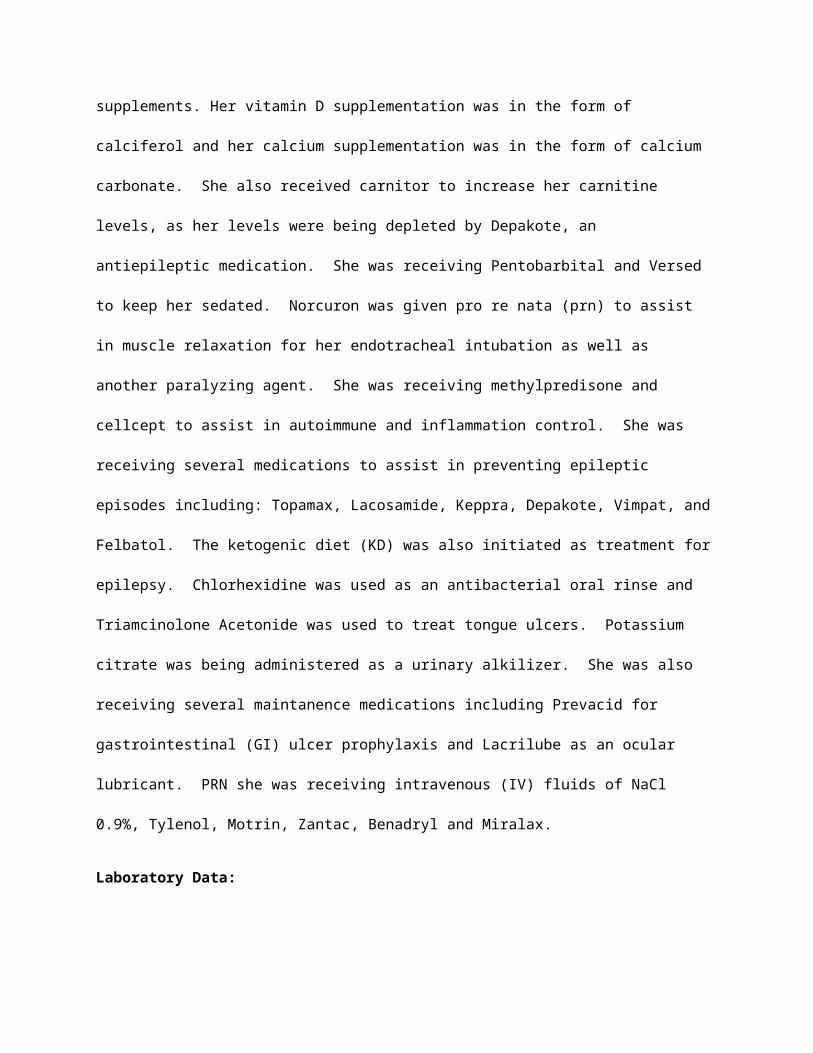
9/17 11 L
9/13 38.1 L
9/12 33.5 L
9/11 27.6 L
The valproic acid test is used to assess adequacy of the anticonvulsant medications she was receiving.
Low levels indicate inadequate administration of the medication. Levels increased to normal range
upon increased dosage of medication.
Comprehensive Metabolic Panel
Date Na K Cl CO2 Anion
Gap
Gluc BUN Crea
t
Ca Pro Alb Bili,
total
AL
P
ALT AS
T
Norma
l
137-
146
mmol/
L
3.4-4.7
mmol/
L
98-109
mmol/
L
17-25
mmol/
L
3-16
mmol/
L
60-
115
mg/d
L
7-18
mg/d
L
0.23-
0.61
mg/d
L
8.8-
10.1
mg/d
L
6.2-
8.1
g/dL
3.4-
5.3
g/dL
0.2-
1.3
mg/d
L
175
-
420
U/L
10-
35
U/L
15-
40
U/L
9/28 145 3.6 104 28 H 13 121
H
7 0.3 1 7.5 L 7.1 2.5
L
0.2 10
8 L
20 39
9/26 143 3.8 106 27 H 10 83 11 0.37 7.4 L 7.2 2.3
L
0.1 L 98
L
18 47
H
9/24 141 3.8 99 30 H 12 106 10 0.37 8.4 L 6.1
L
3.0
L
0.1 L 12
0 L
21 33
9/22 137 5.3 H 100 23 14 93 12 0.4 8.8 7 3.3
L
0.3 11
3 L
12 35
9/20 142 4 110 H 21 11 106 13 0.35 8.5 L 6.4 3.0
L
0.2 93
L
27 36
9/16 128 L 3.9 85 L 30 H 13 115 3 L 0.23 8.3 L 6.6 3.0
L
0.3 10
3 L
32 56
H
9/13 138 3.5 102 23 13 76 9 0.38 7.9 L 6.7 2.9
L
0.3 11
6 L
18 62
H
9/9 139 4.4 102 28 H 9 100 17 0.5 8 L 6.2 2.7
L
0.2 10
3 L
19 38

8/29 137 2.8 L 105 25 7 1000 5 L 0.42 7.1 L 4.3
L
2.0
L
<0.1
L
78
L
33 68
H
8/25 138 4 107 22 9 103 6 L 0.40 7.6 L 5.1
L
2.7
L
<0.1
L
11
1 L
33 61
H
The abnormal electrolyte levels are likely iatrogenic and were never a big problem with GH. Bicarbonate
(CO2) was elevated possibly due to respiratory depression as well as seizures producing lactic acid.
Glucose (Gluc) was normal throughout most of hospitalization, but did go high occasionally. Elevated
blood glucose can likely be attributed to stress and steroid administration. Blood urea nitrogen (BUN)
was low upon admit, likely due to poor per os (PO) prior to admit. Serum calcium (Ca) low due to low
albumin, as Ca binds to albumin (alb) in the blood. Low albumin and protein (pro) likely due to low PO
intake prior to admit. Albumin stayed low throughout hospital stay, likely due to decreased production
as it is a negative acute phase protein. As C-reactive protein (CRP) was consistently elevated, albumin
was consistently low. Bilirubin (bili) likely fell below normal ranges due to pentobarbital medication,
which causes low bilirubin levels. Alkaline phosphatase (ALP) levels were consistently low, which can be
a sign of low zinc status however zinc was checked and level was found to be normal. It is especially
interesting for her ALP to be low because many anti-epileptic medications may cause higher ALP levels.
Low ALP due to unknown etiology. Aspartate transaminase (AST) was high likely due to the seizures GH
was experiencing.
Complete Blood Count
Date WBC RBC HGB Hct MCV MCH MCHC RDW PLTS MPV Nucleate
d RBCs
Normal 4.5-
13.5
K/uL
4-5.2
M/uL
11.5-
15.5
g/Dl
35-
45%
77-95
fL
25-33
pg
32-36
g/dL
11.3-
15.6%
150-400
K/uL
6.6-
10.1
fL
/100 WBCs
9/28 7.5 2.68 L 8.3 L 27 L 100.7
H
31 30.7 L 22.4
H
327 8.7 0.3
9/18 18.3
H
2.97 L 8.8 L 27 L 90.9 29.6 32.6 19.9
H
370 9.2 0
9/5 7 3.02 L 8.6 L 26.5
L
87.7 28.5 32.5 13.9 497 H 9.2 0

White blood cell (WBC) high likely due to stress and infection in the hospital. Consistently low red blood
cell (RBC) levels partially due to blood draws, but mostly due to immunosupressed state of GH due to
medications received. Hemoglobin (HGB) and hematocrit (Hct) likely low due to the low levels of RBC’s.
Mean cell volume (MCV) can be increased with use of anticonvulsant drugs, as is likely the case with GH.
Mean cell hemoglobin concentration (MCHC) decreased upon last testing due to decreased HGB, which
is due to decreased levels of RBC. Red blood cell distribution width (RDW) high likely due to low levels
of circulating RBC’s. Platelets (PLTS) high upon first week of hospitalization but normalized upon
duration of admit. This laboratory value was likely reactive thrombocytosis, possibly elevated due to
infection and inflammation.
Date CRP Zinc Carnitine,
Total
Vitamin D,
25 Hydroxy
Normal <0.8 mg/dL 60-120 ug/dL 31-78 umol/L 30-80 ng/mL
9/9 1.9 H 103 64 35
Zinc, carnitine, and vitamin D, 25 hydroxy were all found to be in the normal range when tested. The
CRP was elevated at the time, which can affect the readings of the zinc levels, but as CRP was below 6
mg/dL, the zinc is truly normal.
Date Calcium, Ionized
Normal 1.22-1.48 mmol/L
9/28 1.14 L
9/26 1.2 L
9/25 1.22
9/24 1.18 L
9/22 1.21 L
9/20 1.25
9/18 1.15 L
9/3 1.3
8/31 1.19 L
8/28 1.25
Ionized calcium (iCa) is low throughout periods of GH’s hospitalization. This could indicate acute
inflammation of the pancreas. This could also be iatrogenic, due to inadequate calcium.
Date CRP Prealbumin
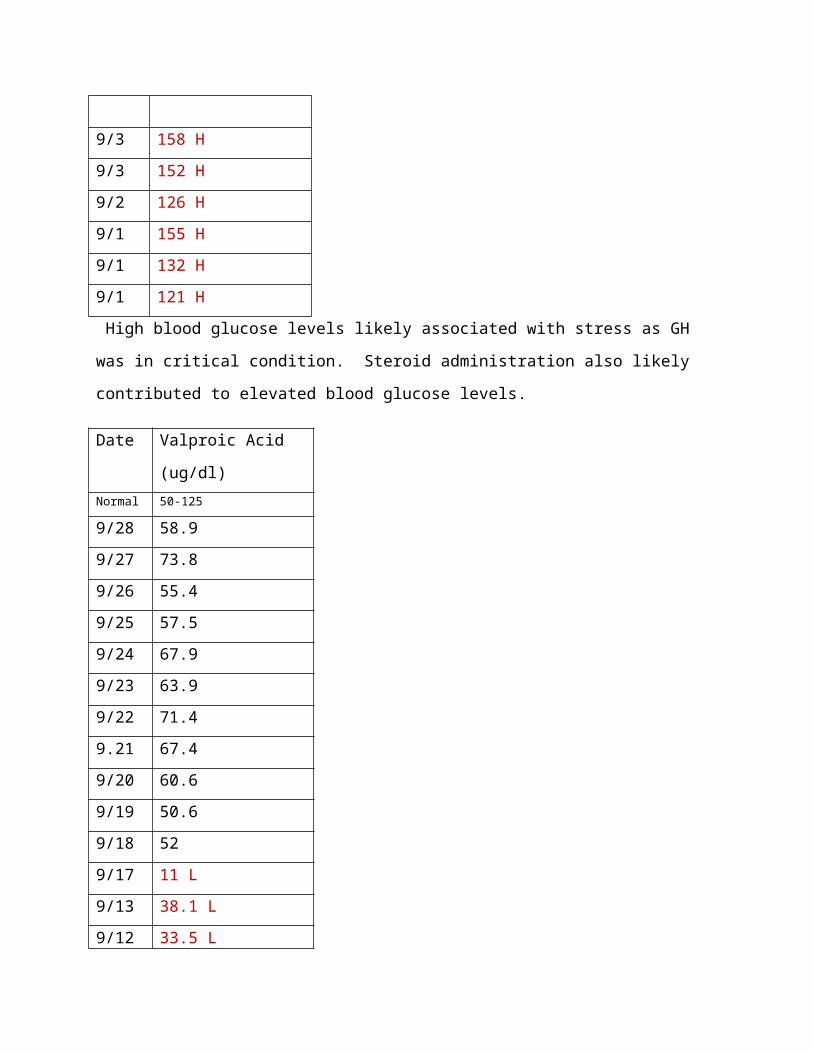
Normal <0.8 mg/dL 12-42 mg/dL
9/28 0.6
9/26 1.6 H
9/23 46 H
9/20 1.5 H 38
9/12 34
9/11 5.9 H
9/9 1.9 H 50 H
9/3 0.8 H
8/28 1.9 H
8/25 1.6 H
CRP likely elevated due to high stress of GH due to critical condition. High prealbumin may be
associated with prednisone administration to GH.
Date Triglycerides Cholesterol
Normal 35-110 mg/dL 107-199 mg/dL
9/9 209 H 193
8/29 90
8/28 127 H
Triglycerides and Cholesterol are typically checked previous to starting a ketogenic diet. GH’s
cholesterol was normal, while her triglyceride levels were elevated. They could likely be high due to
high blood glucose levels for several days prior to testing.
Date Potassium Magnesium Phosphorus
Normal 3.4-4.7 mmol/L 1.6-2.3 mg/dL 3.7-5.6 mg/dL
9/28 2.1
9/22 4.2 2.1

9/20 2.1 3.5 L
9/18 3.8 2.9 H
9/17 4.9 H
9/14 4.5
9/13 3.6 H
9/9 2.2 5.0
9/4 2.3 3.1 L
9/2 2.5 H 3.7
9/1 2.3 4.3
8/29 3.3 L 1.7 2.9 L
Elevated magnesium levels are likely due to respiratory depression caused by induced sedation.
Phosphorus levels likely iatrogenic, due to inadequate intake as no reported diuretics were used prior to
low lab values. Potassium levels were slightly low upon first of hospitalization, but normalized and
stayed wnl. As such, there is little concern for initial decreased potassium level.
Treatment and Progress:
On 8/26 GH was admitted to PICU where she was tested to determine etiology of seizures. She
was diagnosed with encephalopathy and refractory status epilepticus. An electroencephalogram (EEG)
was set up and testing and close observation of GH continued for several days in order to determine
etiology of seizures. She was NPO until 8/27 when a NJ tube was placed and Nutren Jr @ 50 ml/hr was
ordered. The following day (8/28) GH was sedated with pentobarbol to suppress epileptic bursts and
placed on a mechanical vent. NJ feeds were increased. Over the next few days, NJ feeds were
monitored for tolerance. Seizures continued and anticonvulsant medications were administered
throughout hospitalization. Etiology of seizures remained unknown despite extensive testing. On 9/1

Pedialyte @20 ml/hr was added to dietary order. This was a mistake as it was not recommended by
dietary staff and the nurse practitioner notice and had it discontinued. Constipation became an issue for
GH, with medications started to assist in bowel motility. GH also became hyperglycemic due to steroid
therapy, but insulin was not required for treatment. GH became at risk for decreased GI motility
secondary to narcotics and pentobarb. Fleets enema was given, miralax administration was increased to
bis in die (BID) and glycerin suppository was started once a day. Stool output was reported within
normal limits (wnl). Proton pump inhibitors (PPI) were added for additional GI protection while on
steroid therapy. On 9/9 GH appeared euvolemic on current diet and fluid intake and was started on
ketogenic diet (KD). The KD was started at a 4:1 ratio of fat to nonfat calories, using 149 grams of
ketocal powder mixed with water administered at a rate of 70 ml/hr. Phosphorus, calcium, and Vitamin
D supplements were provided in addition to the KD dietary order. Laboratory values were checked as
protocol. GH tolerated initation of the KD with stable BG but without ketosis at this point. Glucose and
ketones were checked every four hours per protocol, with instructions for glucose levels less than 50
being treated with 1 ounce of apple juice. Blood glucose never went below 50 so no corrective action
was necessary. The KD treatment was monitored by taking frequent laboratory tests to determine
effectiveness and safety of KD. On 9/14 the NJ tube was replaced after pt had emesis and plain frontal
supine radiograph of the abdomen (often referred to as a KUB for kidneys, ureter, bladder)
demonstrated the NJ was not deep enough. This was the first day a ketone level of 3+ was found in the
urine, indicating higher levels of ketosis occurring in the body. On 9/16 GH was diagnosed with
respiratory failure related to seizure management (sedation, pentobarbital coma). On 9/17 magnesium
was infused to keep serum levels greater than 3 to help with seizure management. Propofol was also
started at 150 mcg/kg/min in her IV. On 9/18 GH was diagnosed with hypertension (HTN) and propofol
was weaned and was off by 9/19. Electrolytes were managed throughout course of stay with
supplements as hypokalemia did occur on 9/20. On 9/22 HTN was no longer issue with GH, and inability

to maintain ketosis was discussed and per dietary the reason was believed to be related to steroid use
and pentobarb coma. A UTI developed and on 9/23 GH was given antibiotics as treatment. A clot
formed in GH’s right arm around the PICC line on 9/24, so lovenox was started and a left PICC line was
placed. On 9/29 the plan was to continue the ketogenic diet at least through the weekend and reassess
the following week about possible discontinuation of the diet if desired ketosis not achieved.
Clinical Evaluation:
GH was sedated upon time of assessment. She was on a mechanical vent for assistance in
breathing. She was experiencing ulceration in the middle, left side of her tongue. Her skin showed no
signs of breakdown. She had experienced muscle wasting due to decreased activity and believed
gluconeogenesis occurring. She currently had a foley, and a left brachial PICC DL and PIV in left arm. No
clinical seizure activity was noted at time of assessment.
Dietary:
GH’s acute dietary needs were calculated using PCMCs standard formulations. Her estimated
nutrition needs were 1200 kcals (42 kcal/kg), 43-58 g pro (1.5-2.1 g/kg), and 1676 ml fluid (58 ml/kg).
Calculations were based on her actual body weight (ABW) of 28.8 kg. GH received increased protein per
kg, per critical illness standard values. Calories were increased as well, due to her critical state. Fluid
was calculated based on standard equation and was not increased.
Date Diet order PO % Assess tolerance to diet
Is diet adequate to meet patient’s needs?
9/9/11 13:19 Continuous NJ Feed: Ketocal @ 50 ml/hr with free water at
N/A Poor – Ketones not at desired 4+ level
No, Inadequate supply of proteins, carbohydrate, and micronutrients provided.

additional 20 ml/hr
9/1/11 Continuous NJ Feed: Nutren Jr @ 50 ml/hr with free water at additional 20 ml/hr plus Pedialyte @ 20 ml/hr
N/A Good Yes, Pedialyte added without dietary orders and was subsequently discontinued.
8/27/11 Continuous NJ Feed: Nutren Jr @ 50 ml/hr with free water at additional 20 ml/hr
N/A Good Yes
8/25/11 NPO N/A N/A No
Nutrition Screening:
Upon day of assessment, GH was at high nutrition risk, according to PCMC’s nutrition screening.
Nutrition screening total points were 9 points, with the breakdown as follows: Admit Dx (Seizures) 0 pts;
BMI (5-14.9%ile) 1 pt; Diet order (Enteral/TF) 2 pts; Respiratory Status (Mechanical Ventilation) 6 pts.
Nutrition Note:
Nutrition Assessment(s) and Follow-Up Note(s) based on PCMC format:
Assessment:
9/29: Pt still intubated/sedated in pentobarbol coma, on Ketogenic Diet. iCa and phos both
low at last test, will assess adequacy of diet/supplementation with Ketogenic Diet RD and
discuss need for increased supplementation. Although prealbumin is high, albumin is low and
trending down and BUN is normal, but trending down which can be markers of inadequate
protein intake. Ketones tested negative in urine today (9/28), with previous two days having +1
ketones in urine. With limited ketone production, ketogenic diet may be ineffective as
treatment for seizures. 7 day ave intake (9/22-9/28) equals 100% of est nutrtitional needs for
calories and fluid. Only receiving 1.24 g pro/kg, which is approx 70% of est protein needs.
9/22: Pt remains in PICU with status epilepticus. Currently on ketogenic diet (4.5:1) and in a
pentobarbitol induced coma. No new wt at this time. Nutrition labs show a normal Zinc, Vit D,
Pre Alb and Carnitine panel at this time. Pt currently has 0 ketones in her urine despite a very
high ratio and no carbohydrates in her IV fluids or Rx. Suspect the reasoning is two fold: 1) Pt is
on steroids. Steroids cause gluconeogenesis from visceral protein - pt is likely catabolizing her
visceral protein stores to make her own glucose and 2) Pt is in a pentobarbital coma. The
decreased brain activity limits the amount of glucose/ketones needed for energy. Per NP,
pentobarb coma will likely be lightened today and in the near future, but she will cont on
steroids for some time.
9/16: GH has started Ketocal and is now at 50 ml/hr with additional 20 ml/hr of water via NJ.
Current ratio is 4.5:1. Urine ketones were 2+ and now 3+. Valproic acid has been started.
Meds are in lowest carb form. Propofol (sourse of IL) is increasing. Vitamin D level was wnl

and zinc level was wnl. She is receiving additional vitamin D at 800 IU per day with Calcium
carbonate and K-Phos secondary to ketogenic diet.
9/9: GH is a nine year old female who is currently intubated, and in a medically-induced coma
with no positive affect of anti-seizure medications. The decision to trial the ketogenic diet for
seizure control has been made.
GH is currently NJ fed with Nutren Jr. to equal 1200 calories per day and ~36 grams of protein
per day, and 1680 ml per day with additional fluid of 20 ml per hour. Prealbumin is pending to
determine adequacy of current calorie/protein intake. Secondary to low calories because of
acute phase needs and high fat requirement of the ketogenic diet, 100% of protein needs are
not met by recommended ketogenic diet formula. Prealbumin with CRP and weight will need
to be checked while intubated and on the diet every 3-5 days to assess severity of potential
malnutrition. Once, calories can be increased, there will be more "room" for protein in her
formula.
GH will advance to a 4:1 ratio by Tuesday morning. Formula will advance in 3 stages to full
ratio, 1/3 ratio x 8 hours, then 2/3 ratio x 8 hours, then full ratio for 24 hours.
9/6: GH is in a chemically induced coma, orally intubated, receiving NJ feeds at goal rate.
Feeds are providing 42 kcal/kg/day and 1.3 gm proteinkg/day. Tolerating feeds. No new weight.
Prealbumin would be helpful in assessing adequacy of protein intake.
8/30: Pt admitted to PICU with new onset seizures, decreased LOC and encephalitis of
unknown etiology. Currently intubated and sedated. Post-pyloric feeding tube was placed and
enteral feeds have been initiated.
Nutrition Diagnosis:
9/29: Inadequate protein intake related to physiological causes increasing nutrient needs due
to prolonged catabolic illness as evidenced by elevated glucose and prevention of ketosis
despite ketogenic diet.
9/9: Risk for inadequate carbohydrate intake related to induction of the Ketogenic diet as
evidenced by anticipated low blood sugar and acetate levels.
8/30: Inadequate oral intake related to mech vent as evidenced by inability to independently
consume PO food/fluids.
Goals:
9/29: Non Ketogenic Diet NJ Feeding Goal: Compleat Pediatric @ 50 ml/hr plus 20 ml/hr
water. Feeds provide 1200 kcal and 45.6 g protein per day.
9/9: Promote seizure control by appropriately administering the Ketogenic diet.
8/30: Adequate intake to promote optimal growth and development for age/condition.
Interventions:
9/16: Ergocalciferol 800 IU daily; 1250 mg NJ calcium carbonate q 6 hrs; K-ph 500 mg daily.
Ketocal at 50 ml/hr with free water at additional 20 ml/hr to total 70 ml/hr continuous NJ
feeds.
Recommendations:
9/29: Recommend dc’ing ketogenic diet at this time. Pt is not in ketosis and appears to
continue to experience gluconeogensis (breaking down of muscle stores to produce

endogenous glucose) b/o stress hormones inherent in critical condition. Increasing ratio of
ketogenic diet will likely increase gluconeogenesis and continue to prevent ketosis while pt is in
a critical state. Please cont to check ketones/BG levels to determine effectiveness of ketogenic
diet. Please check Vitamin E to ensure adequate levels and to r/o hemolytic anemia given hx/of
high LDH. Please check ammonia levels to help determine if metabolic protein breakdown is
occurring. Will as RN to zero bed and obtain new wt as last wt was taken at admit.
9/22: Cont to check ketones/BG over the next 3-4 days as pentobarb coma is lightened. Please
check Pre Alb and CRP now. If Pre Alb is declining/low, please consider dc'ing ketogenic diet
until pt is off steroids/not critically ill. (Inactive)
9/9: Initiate KD via Ketogenic formula on Friday, September 9, 2011. First 1/3 strenth ratio will
run for 50 ml per hour x 8 hours. An additional 20 ml per hour of free water may be administed
to reach maintenance fluid. Second 2/3 strenth ratio will run for 50 ml per hour x 8 hours. An
additional 20 ml per hour of free water may be administed to reach maintenance fluid. Full
strength ratio of 4:1 can be run at 50 ml per hour x 24 hours once 1/2 and 2/3 strength
formulas have been used. An additional 20 ml per hour of free water may be administed to
reach maintenance fluid. Please provide no more than 240 ml at each meal. Please provide no
more than 240 ml at a time, i.e. within a one hour period. Maintenance fluid is ~1676 mL.
Please minimize additional fluid to help with seizure control while on the ketogenic diet.
(Inactive)
Daily supplements are to include the following, 2 tablets K-Phos Neutral, 600mg Calcium, 800 IU
Vitamin D, 1 packet Cytra-K Crystals, and Carnitine per Paula Peterson. Please provide brand

name supplements as above to control carbohydrate content. Check CRP and prealbumin every
5 days. (Inactive) Change all current meds to be ketogenic diet friendly - minimize use of
liquids/syrups unless compounded. (Inactive)
9/6: Check Prealbumin, CRP with next labs. Continue 50 ml/hr Nutren Junior plus 20 ml/hr free
water NJ feeds. (Inactive)
8/30: Please decrease feeds to 50ml/hr to prevent overfeeding. If maintenance fluids are
desired, please run free water @ 20ml/hr. (Inactive)
Patient Follow-Up:
GH’s medical team continued to discuss possible etiology for seizures as well as reason
for inability to achieve ketogenesis. A weight was taken on 9/30, of 25.4kg showing weight loss.
On 10/1 pancreatitis was found and GH was taken off KetoCal. Her formula was changed to
Vivonex TEN at a rate of 55 ml/hr with a decrease in free water to 15 ml/hr in order to keep
fluid regimen the same. To account for the weight loss, estimated needs were calculated at
1350 kcals/day. On 10/4 GH’s NJ tube was replaced past the ligament of Tritez and NJ feeds
were continued. At this point in time, the goal is to determine etiology and stop occurrence of
GH’s seizures. Until this happens prognosis is poor for GH as she has received long-term
sedation with the inability to safely wean, as well as the ineffectiveness of several
anticonvulsant medications and the attempted ketogenic diet.
References:
1. Remig, Valentina. Medical Nutrition Therapy for Neurologic Disorders. In: Mahan LK, Escott-
Stump S, ed. Krause’s Food & Nutrition Therapy. 12 ed. St. Louise, MO: Saunders Elsevier;
2008:1088-1090.

2. Zupec-Kania BA, Spellman E. An Overview of the Ketogenic Diet for Pediatric Epilepsy. Nutr Clin
Pract. 2008;23:589-596.
3. Hong AM, Turner Z, Hamdy RF, Kossoff EH. Infantile spasms treated with the ketogenic diet:
Prospective single-center experience in 104 consecutive infants. Epilepsia. 2010;51(8):1403-
1407.
4. Patel A, Pyzik PL, Turner Z, Rubenstein JE, Kossoff EH. Longer term outcomes of children treated
with the ketogenic diet in the past. Epilepsia. 2010;51(7):1277-1282.



![KD-A645 / KD-R640 / KD-R540 / KD-R440 - Car Audio ...santafeautosound.com/uploads/product-manuals/JVC KD-R540.pdfKD-A645 / KD-R640 / KD-R540 / KD-R440 GET0829-001A [J/JW] ENGLISH ESPAÑOL](https://static.fdocuments.us/doc/165x107/5aaf5da87f8b9a25088d67c4/kd-a645-kd-r640-kd-r540-kd-r440-car-audio-kd-r540pdfkd-a645-kd-r640.jpg)





![KD-X470BHS / KD-X370BTS / KD-X37MBS / KD-X270BT ...Data Size: B6L (182 mm x 128 mm) Book Size: B6L (182 mm x 128 mm) ENGLISH FRANÇAIS ESPAÑOL B5A-3105-00a [K] KD-X470BHS / KD-X370BTS](https://static.fdocuments.us/doc/165x107/5fa2da61a08b9c64377c7b40/kd-x470bhs-kd-x370bts-kd-x37mbs-kd-x270bt-data-size-b6l-182-mm-x-128.jpg)




![KD-R981BT / KD-R889BT / KD-R881BT / KD-R784BT / KD ...Data Size: B6L (182 mm x 128 mm) Book Size: B6L (182 mm x 128 mm) ENGLISH FRANÇAIS DEUTSCH РУCCKИЙ B5A-1353-00 [E] KD-R981BT](https://static.fdocuments.us/doc/165x107/60f8a461e650da6d260a5f67/kd-r981bt-kd-r889bt-kd-r881bt-kd-r784bt-kd-data-size-b6l-182-mm-x.jpg)



