least developed nation. Philosophical foundations of ...
20
Page 1/20 Philosophical foundations of research, and the case of the epistemic well, in a least developed nation. Avaniendra Chakravartty ( [email protected] ) B.P. Koirala Institute of Health Sciences perspective Keywords: philosophical, research, neoliberal, Nepal Posted Date: March 24th, 2021 DOI: https://doi.org/10.21203/rs.3.rs-352233/v1 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License
Transcript of least developed nation. Philosophical foundations of ...
Page 1/20
Philosophical foundations of research, and the case of the epistemic well, in aleast developed nation.Avaniendra Chakravartty ( [email protected] )
B.P. Koirala Institute of Health Sciences
perspective
Keywords: philosophical, research, neoliberal, Nepal
Posted Date: March 24th, 2021
DOI: https://doi.org/10.21203/rs.3.rs-352233/v1
License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License

Page 2/20
AbstractInspired by an ancient tale of kupamanduka (Well Frog) that never ventures out of the well and lives to think the well as the world and see nothing beyond it.This article conceptualises the ‘Epistemic Well’ and the native epistemic community that dwells in it remains within the con�nes of the epistemic well.Philosophical foundations are the core of each individual researcher and all research questions, hypothesis, methodologies, recommendations are shaped byit. Particular modes of governance instil particular modes of philosophies. Under neoliberalism the prevailing philosophical foundations have been identi�edas, detached, decontextualized, depoliticized, dehistoricized, dissocialized, deproblematized, reductionist/individualist, instrumentalization, separation,marketisation, positivist and objectivist. The combination of these attributes builds the epistemic well. The epistemic well of research is not absolute and isnot meant to provide quanti�cation data. The epistemic well is a re�exive tool that can be used to evaluate a research especially for a nation like Nepal. Theresearch funds or the bene�ts that ensues a researcher are important criteria for research. When thinking of a research topic, the primary determining factorbecomes the amount of fund available the gaze of a native researcher can overlook various conditions and processes. The epistemic community that isformed by these researchers maintain and sustain particular epistemes. The NCD’s were selected primarily to stick to a cohort but this does not limit the scopeand purpose of the epistemic well.
1. Introduction The rationales, objectives, methodologies/methods, results and recommendations are predominant and evident aspects of most research. Followingthese are the philosophical foundations which remain usually invisible and which also build up the visible components of most research. Philosophicalunderstandings about nature of reality are crucial to understanding from an overall perspective from which studies are designed and carried out(Krauss andPutra, 2005). Methodology and methods are determined by researcher’s world view and bias(Brown, 2003), re�exivity and researcher positionality(Walt et al.,2008), ontological & epistemological positions(Rowe and Oltmann, 2016)(Weed, 1999) and axiological positions(Carter and Little, 2007).
A basic component of deciding on methodology is the philosophical foundation one possesses regarding beliefs, values, ontology, epistemology andrelationality. Over the years a range of philosophical perspectives have emerged such as methodological individualism, empiricism, positivism, Cartesianism,reductionism, methodological holism, political economy, Marxism, pragmatism, existentialism, constructionism and in contemporary era philosophy,postmodernism, post-colonialism, post-positivism, post-foundationalism, postneoliberalism, post-structuralism. These different philosophies sometimescontradicting and sometimes over-lapping have been providing the foundations of research in varied areas.
The scope of this article is not to discuss about these varied philosophies and its strengths and weakness and neither is the scope to discuss whichphilosophical perspective is better. The attempt here is to explore the philosophical foundations and the assumptions that inform researchers (epistemiccommunity of researchers) under neoliberalism. Research is an outcome of prevailing epistemes. Epistemes are crucial in maintaining, establishing andsustaining the prevailing knowledge. An episteme is the accepted and leading method of gaining and organizing knowledge in a given historical epoch.Epistemes are ‘manners of justifying, explaining, solving problems, conducting enquiries, and designing and validating various kinds of products oroutcomes’(Land, H.F.Meyer and Baillie, 2010). An episteme controls and regulates the way in which conceptualisation can occur(Howson, 1993). Episteme isthe historical a priori that grounds knowledge and its discourses and thus represents the condition of its possibility within a particular, historical context(Ungeret al., 2011). Dominating epistemes or world views are articulated in part through institutions, such as healthcare settings, education systems and throughspeci�c scienti�c disciplines such as public health, nursing, psychiatry, endocrinology, engineering etc(Murray, Holmes and Rail, 2008). Epistemes areestablished and sustained through processes of epistemi�cation by epistemic communities. “Epistemic communities are recognized by four central elements—shared causal ideas, shared principled beliefs, shared notions of validity, and a common policy enterprise”(Dunlop, 2012). “An “epistemic community ispolitically neutral, and has been described as a community who apply their standards of credibility, and epistemic values, to the practice of theory choice andknowledge production”(Kinsella and Whiteford, 2009). It has also been described as “a professional group that believes in the same cause-and-effectrelationships, truth tests to assess them, and shares common values”(Maffra and C, 2013).
Based on available literature on epistemic communities and the features that characterise an epistemic community as mentioned in the aboveparagraph the National Health Research Council (NHRC) can be identi�ed as an epistemic community. The Second National Summit of Health and PopulationScientists in Nepal which was held from April 11-12, 2016, with the theme, “Health and Population Research for Achieving Sustainable Development Goals inNepal” provides the background and the data needed for the study. One hundred and sixty �ve papers were presented. The research papers were classi�edinto nine different themes. The summit was attended by a rich diversity of participants from academia, research institutes, government, I/NGOs and externaldevelopment partners(Bahadur Karki Dharma Kanta Baskota, 2017). This diversity of views available in an event present an excellent opportunity to build theobjective of this article which is to explore the philosophical foundations and the assumptions that guide researches done on health issues by a nativeepistemic community of researchers in an era of neoliberalism.
2. Rationale The indiscriminate and uncritical use of questionnaire surveys to gather information was raised more than three decades ago in 1979 in the �rst editionof the book, ‘Use and misuse of social science research in Nepal’(Campbell, Shrestha and Stone, 2010). More recently others have also expressed the fact thatthe overwhelming majority of articles reported on quantitative(Karmacharya, 2011) and calls for making health a public health agenda have also beenmade(Subedi Sharma Madhusudan, 2016). Others have discussed issues that re�ect a particular political economy of research - where funding comes from,who de�nes the research agenda, the costs of review, developing Nepal’s research capacity, through to the politics of publication of research �ndings - andincludes questions relevant to emerging regulatory and ethical frameworks(Sharma, Khatri and Harper, 2016). The public health education has also beencharacterised as having its stress on managerial, administrative and project speci�c and lacking academically the public health graduates are trained to workas public health practitioners in districts(Mahat et al., 2013). Studies of philosophical nature in dealing with ontological and epistemological issues on Nepal

Page 3/20
have been few and those that do deal with caste, religion, semantics and forestry(Ahlborg and Nightingale, 2012) (Schulz and Siriwardane, 2015) (Ojha et al.,2016) (Campbell, Shrestha and Stone, 2010). Working with an epistemic community to generate a range of options for further analysis may itself yieldimportant insights into policy, as well as into how the epistemic community operates, perceives the problem(s) and proposed solutions. The rationale of thestudy to explore the philosophical foundations of research arose due to three primary reasons.
The �rst reason is due to the historical processes that has conditioned contemporary Nepal. The second reason is due to the in�uence of neoliberalvalues and the third reason is due to the empirical experiences of the author. A very brief history of Nepal is discussed since; a historicized understanding ofthe present condition has been deemed an important approach(Rosenberg, 2003). Nepal though never colonized has been substantially affected bycolonialism in ways which are different from other past colonial nations. The Rana period from 1848 to 1950 pushed Nepal towards isolation by deliberatelykeeping the population away from the modern ideas of development such as education. Literacy rate in 1950 was approximately two percent(Kernot,2006).
More than one hundred years ago in 1887 when various inventions, discoveries were taking place around the world, Richard Temple had declared Nepalto be ‘closed to the eyes of science’(Chene, 2007). The year 1956 marks the end of oligarchy, the beginning of an egalitarian political system, introduction ofuniversal access to education, introduction of the General Health Plan, becoming an aid-recipient country and the launch of the First Five- year Plan (1956–1961)(Pherali and John, 2011) (World Health Organization, 2006) (Rai et al., 2001). The late advent of modern liberal democratic ideas, the poor livingconditions, and the implementation of the banking model of education with its emphasis on accumulation of knowledge demobilized the people within theexisting establishment of power by conditioning them to accept the cultural, social, political status quo of the dominant culture which also led to increaseddependency on others for its development(Campbell and Jovchelovitch, 2000) (Sharma, 2010) (Kernot, 2006) (Van Teijlingen et al., 2015).
Nepal began neoliberalising from the late eighties onwards. In the early 1990’s Nepal was subjected to structural adjustment policies (SAP) in line withneo-liberal principles(Sugden, 2009). As a process, neoliberalization is variegated, un�nished, and contingent(Annetts et al., 2017). It is a slippery concept totheorize(Nik-Khah and Van Horn, 2016), let alone study empirically(Nik-Khah and Van Horn, 2016). Most scholars tend to agree that neoliberalism is “broadlyde�ned as the extension of competitive markets into all areas of life, including the economy, politics, and society”(Porter, 2005a). Key to this process is “anattempt to instil a series of values and social practices in subjects(Petersen and Davies, 2010) and by virtue of being embedded in practices of governance atthe local level often leads to a sense of neoliberalism being everywhere”(Castree, 2011).
Depending upon the social, economic and political conditions of a nation, the adoption of free-market and neoliberalism can have varied affects andconsequences. Neoliberal values and principles like, survivor of the �ttest philosophy has taken hold in all sectors including academic, research andeducation. In academics and research the ‘publish or perish’ philosophy prevails as a result of which hundreds of researches are being done every year inNepal. Rei�cation of research has led to research being done for ful�lling objectives leading to personal gain. Research is done to know about a particularcondition that we do not know much about by using methods that are scienti�cally based. But how do we know what needs research? And what are thereasons for doing a research? Even before identifying the research topic, subject or object they are cognitive processes that in�uences us to decide on aparticular research topic, research questions and the research hypothesis.
In �gure one the research process shows, the researcher at one end of the process and the results, recommendations and the knowledge generationthat the research provides at the other end. In between these two, lay the other determining factors that affect the research output. The researcher is at thebottom as shown in the �gure one. Varied range of classi�cations have been done on the different factors that affect and guide our research at differentstages such as, ontology(metaphysics), axiology, epistemology in totality our philosophy or paradigm. Though ontology and epistemology have been shownseparately, claims have been made that these cannot be considered separable as axiology, epistemology and ontology co-evolve(Allen and Varga, 2007).Theoretically the research process �ows within the framework of research process as shown in �gure one. The sections highlighted in bold are the mostvisible outcomes of research. The philosophical aspects of research are usually invisible (ontological epistemological and axiological conditions). The focusof this article is on factors that guide us to choose a particular methodology and through which results are generated, �ndings are made andrecommendations done.
Since the neoliberal environment condition our ideas, it is imperative that neoliberalism and its ideology, its assumptions and its processes be discussed andunderstood. Since its coinage the term has been in constant use and its popularity can be fathomed by the fact that a Google scholar search of the termneoliberal in its title since 2019 yielded more than 1500 results. With so much use of the term, neoliberalism risks being tagged as just anotherbuzzword(Noonan, 2018) or fuzz word, or is it already one? Use of the term neoliberal has also led to some describing as being lazy, too vague, too ready todenounce, frequently unde�ned, unevenly employed, too overblown and the need for it to be ‘severely circumscribed’ has been called for(Clack and Paule,2019). Despite the allegations, neoliberalism still holds an important place as evident by the large number of publications which mention the term.
The term neoliberalism resulted from the participants during the Walter Lippmann Colloquium held in Paris in 1938 to discuss the French publicationof, An Inquiry into the Principles of the Good Society by Lippmann(Cahill et al., 2018). The central presuppositions of neoliberalism include the rational self-interested individual, free market economics, a commitment to laissez-faire and a commitment to free trade(Olssen and Peters, 2005). Neoliberalism hasshaped our cognition and it espouses neoliberal ideologies that emphasize individual-level decision making about economics and healthcare(Sanders andMcKay, 2013). Neoliberal view and practise has directly implicated in shaping the way health is promoted(Ayo, 2012) and thoughts are shaped(Rose,2001).The neoliberal ontological project supposes homo economicus as principal model for individual behaviour which occurs from subject’s economicrationality functioning in a world of perfect information and inert notions of equilibrium(Madra and Adaman, 2014). Neoliberalism touches all aspects of lifeincluding research.

Page 4/20
Neoliberalism and its ‘regime of truth’ values characteristic features like individualisation(Clack and Paule, 2019), marketisation(Dutta, 2016),�nancialisation(Rossi, 2013), commoditisation(Fisher, 2009), commodi�cation(Esposito and Perez, 2014), commercialisation(Pinto, 2017), privatisation,accumulation(Subramaniam, 2014), dispossession(Subramaniam, 2014), adaptation(Phillips, McMichael and O’Keefe, 2018), freedom(Odysseos, 2010),competition(Baronov, 2012), monetisation(Fox, 2017), disimagination, melioration(Birn, 2014) and de-democratization(Brown, 2006). Humans being rational,independent, entrepreneurial, pro�t seeking and opportunity maximising humans will thrive competitively in a free market where the “invisible hands of themarket” will take care of it all. It has been seen as a “hard-wired reality”, a doctrine, an ideology which sees institutions adapting to variegated strands ofcapitalism(Fine and Saad-Filho, 2017).
Under neo-liberal in�uence research is predominantly positivist(Esposito and Perez, 2014) by nature and the recommendations, �ndings; interventions arepredominantly individualist in nature(Rentmeester and Dasgupta, 2012). This knowledge of interventions stems from the ontological and epistemologicalassumptions one has and under neoliberalism it has been predominantly guided by, “a positivist ontology which suggests that all things exist in some sort ofobjective universe and this includes human beings”(Stahl, 2007). A positivist ontological approach, “presumes the existence of a ‘‘real,’’ apprehendable realitydriven by immutable natural laws and mechanisms and that researchers are capable of studying objects without in�uencing them or being in�uenced bythem”(Carpiano and Daley, 2006). “Positivism relies on a reductionist view in its search for universal mechanistic rules that are not contextually bounded andseeks to verify hypotheses”(Carpiano and Daley, 2006). Positivists view the individual as an essentially biophysiological and neurophysiological system, areductionist view(Yadavendu, 2013). An offshoot of the positivist school of thought is methodological individualism (MI) which, “emphasises; homoeconomicus, based on assumptions of individuality, rationality, self-interest; and the doctrine of spontaneous order”(Roberts and Peters, 2019).Methodological individualism has been the “central monistic-ideological stand of existing economic theory, from which individual economic policiesfastidiously acquire neoliberal basis”(Draskovic, 2016).
Methodological individualism as a position and process consists of several assumptions. Some of the assumptions inherent within the approach whichhave been identi�ed are ontological assumptions(Prozorov and Rentea, 2016), epistemological assumptions(Cosgrove and Karter, 2018), fundamentalistassumptions(Sparke, 2020), atomistic assumptions(Mcdowell, 1994), methodological assumptions(Rillo, 2018), observability assumptions(Backhouse, 2007)and axiological assumptions(de Camargo, Ortega and Coeli, 2013). A “positivist ontological approach combined with methodological individualism can createa disposition to treat humans as objects”(Stahl, 2007). “Treating humans as things means that one can treat them as means rather than ends, thus violatingKant’s well-known account of the categorical Imperative”(Amstutz, 2013), “according to which humans should never be treated as means or to put it in morecontemporary words”: "Such research may end up by recommending most people to be handled like billiard balls”(Nissen, 1985).
This combination of methodological individualism and positivism has been incorporated in epidemiology, the discipline most actively involved in thestudy of health problems(Breilh, Campana and Hidalgo, 2005). Claims against mainstream/traditional epidemiology being “too dull to analyse thecomplexities of today’s health problems was made in 1994”. The Leeds declaration “emphasized the need to refocus upstream and to use research methodsthat are appropriate to the level at which intervention will take place”(Pearce, 1996). “Epidemiologic techniques can be used in other settings (e.g., clinicalepidemiology) and for other purposes (e.g., studies of disease progression and prognosis), but the key contribution of epidemiology to public health is itspopulation focus”(Pearce, 1996). Citing the Leeds declaration in 1994, “the Lancet editors concluded that common epidemiological research has always beenbased on simplistic notions of causality”(van Der Maesen and Nijhuis, 2000). “The Research Unit in Health and Behavioural Chance at Edinburgh Universityconstrued that mainstream epidemiology has little to offer in modernising public health, that its positivistic orientation highlights a key �aw in its recognitionof the social dynamics of health and disease, therefore weakening its potential to achieve transformation in public health”(van Der Maesen and Nijhuis, 2000).
The dominant risk factor epidemiology prevailing has several limitations(Pearce, 1996)(Goldberg, 2013) and operates under ‘atomistic metaphysics’(deCamargo, Ortega and Coeli, 2013) and individualistic suppositions(Wemrell et al., 2016). “The principal approach of epidemiological explanation takes placeentirely within the con�nes of a scienti�c way that has been termed Cartesian reductionism, an analytical advance categorized by a focus on factorsmeasured in seclusion from their context”(McPherson, 1998). “The dominant theoretical developments in epidemiology have effectively ignored the truedialectic that exists between people’s actual chances and their real possibility of making choices”(Doll, 1999).
The practise of victim blaming does not question, structural, social and other external forces that puts an individual at risk. Individualistic approaches do notdeal with the root causes, “which not only include industrial activity but also elements of the global political economy that give rise to the crisis in the �rstplace”. Occasionally called the ‘causes of the causes of the causes’, “several commentators argue that these broader societal factors can be tackled only bypassing policies that deal with structural drivers, particularly those that generate poor nutrition: liberalisation of food trade; the acceleration of foreigninvestment by transnational food companies; the rapid spread of cheap, ultra-processed food that affect the availability, affordability and acceptability ofwhat people eat; and deregulation of commodities markets that cause food price instability and dietary dependency” .
The hallmark trait of contemporary public health has been dominated by behavioralism(Staddon, 2004) and the individualization of risk(Peet,Robbins and Watts, 2010). This individualization along with the belief in positivist ontology and epistemology has resulted in the much acclaimed evidence-based medicine or to put it more broadly evidence-based practise. The materialization of Evidence-based medicine (EBM) as the gold-standard practice wasfollowed by Evidence-based public health (EBPH) which resulted in signi�cant ontological and epistemological shift which resulted in “proactive use ofevidence conducted within a realist ontology using positivistic empirical strategies”(Gray and Mcdonald, 2006). The emergence of evidence-based practicemust be appreciated within the context of neo-liberalism(Gray and Mcdonald, 2006). The EBPH like EBM tries, “to position health policies and interventions on‘sound facts’ and this uncritical acceptance of evidence-based medicine by the public health �eld has been seen to substantiate blaming individual patientsfor health problems ensuing from social conditions or that the EBPH approach may rationalize cuts in public health spending”(Nadav and Dani, 2006). BothEBM and EBHP presuppose universal biological response and hence do not take into account the social and historical grounds of the researched sample, andthus they assume that conclusions of a speci�c set of researches can be generalized to any population(Victora, Habicht and Bryce, 2004).

Page 5/20
“The critics of EBP warn that the concept of ‘what works’ evidence is parochial and myopic, because it de�nes ‘evidence’ scienti�cally and mechanicallythat is too limited from public health perspective”(Ahmed, 2014). The evidence-based approach has been claimed to have led to the commodi�cation of healthcare and public health(Nadav and Dani, 2006). The “model’s limitations are especially salient in the �eld of public health, where conditions consideringproblems to be the result of simple, one-directional, causal relationship, is even more reductionist”(McGuire, 2005). “Commonly ignored, yet seriously health-damaging, contextual factors include: being a second-class citizen or being made to feel like a second-class citizen”(Monaghan, 2013). Epidemiologicallyinformed ‘lifestyle’ approaches thus obscure how health is an embodied multi-dimensional construct. As a social construct, health also comprises differentmeanings to different people”(Rich, Monaghan and Aphramor, 2010).
Most theoretical debates about the pros and cons of public health approaches are con�ned to the methodological scienti�c level. “Philosophical foundationssuch as fundamental ontological notions are seldom part of public health debates, but these are always inherent and lie behind the opinions andinterpretation of diverse standpoints or traditions”(Nijhuis and van der Maesen, 1994). “In empiricist science, dominant in contemporary epidemiology,exposure and risk assessment, the principal accepted philosophical approach is that of the positivist paradigm —unbiased examination; the separation of‘facts’ from ‘‘values’’; and the stress on veri�cation to build up universal laws”(Briggs, Sabel and Lee, 2009).
The combined empirical experiences of the authors gained in day to day academic activities such as classroom interactions, seminars and research activitieshave also considerably prompted us to explore research philosophy in the �eld of health. Experiences such as when teaching public health and communitymedicine at the post-graduate level in the �rst semester when asked what causes an individual to have ischemic heart disease or any other diseases that havebeen historically linked to social, economic and environmental conditions? The answers received comply with the dominant paradigm of proliferating blamethe victim ‘life-style’ theories which emphasize individual’s responsibility to choose so called healthy life-styles and to cope better with stress, illiteracy,ignorance, superstition and other individual attributes. The principal causes of ill-health are situated at the micro level. The lack of historically informedanalysis is absent and this lacuna manifests itself when doing health research.
3. Methodological ApproachInspired by an ancient folklore originating in China(‘Chinese Stories_The frog of the well - Wikibooks, open books for an open world’, no date) and India(kupamanduka – in Sanskrit it means, ‘well frog’)(Sen, 2003) about a ‘frog in the well’, this article attempts to conceptualise an epistemic well. The frog fromthe well does have a ‘world view’ but it is a world view con�ned to the stale water of the well and the frog knows nothing else outside the well. Similarly theinhabitants (in this case an epistemic community) of an epistemic well also have a world view but this world view too is limited. The inhabitants of the wellare conditioned by seeing only what can be seen from within the depths of the well. The concept of epistemic well has been in�uenced by concepts such asepistemic obstacles(Brassolotto, Raphael and Baldeo, 2014a), epistemic violence(Richardson, 2019), epistemic dependence(Carter, 2020), epistemicracism(Monzó and Hoo, 2014), epistemic pollution(Levy, 2018), epistemic dominance(Schillmeier, 2006), epistemic ignorance(Faber, Manstetten and Proops,2007) and epistemic injustice(Kidd and Carel, 2017).
The methodological approach to explore the philosophical foundations of health research and to conceptualise the epistemic well largely rests on criticalre�exivity and an autoethnographic approach. The �rst step in the methodological process was to identify the characteristics that have been associated withhealth research under neoliberalism. Neoliberalism touches all aspects of life and research is no exception. Under neoliberalism, the dominant philosophy ingeneral has been characterized as detached(Kelly, Keck and Lynteris, 2019), decontextualized(Kirmayer, 2012), depoliticized(O and A, 2010),dehistoricized(Dunn, 2000), dissocialized/desocialized(Matusitz and Breen, 2007), deproblematized(Juul Nielsen and Grøn, 2012),reductionist/individualist(Lencucha and Thow, 2019), instrumentalization(Engel and Susilo, 2014), separation(Fisher and Lees, 2016), marketisation(Sell andWilliams, 2020), positivist(Smith, 2019) and objectivist(Glasgow, 2012). These dozen features identi�ed in the study can be said to make an imaginary well,which the authors try to conceptualise as epistemic well of research (see �gure two).
The epistemic well a product of neoliberalism can exist in any discipline. The dozen features of the epistemic well when viewing health does not questionthe social, economic and political structures; it takes them as given and deals with health issues from within these pre-existing structures. The epistemic wellis not absolute in nature and not all researches will display all the twelve characteristics of the epistemic well. Some of the characteristics of the epistemicwell like positivism as a trait of a research may not mean that a research is in�uenced by the epistemic well. The epistemic community that dwells in theepistemic well produces the researches. The epistemic well exists but due to its invisibility and the processes through which it exists, makes discerningresearches in�uenced by the epistemic well a re�exive exercise. The researches that are affected by the epistemic well can produce results andrecommendations that may serve no purpose, other than some instrumentalist purpose bene�tting the self. The epistemic well of research is not absolute andis not meant to provide quanti�cation data. The epistemic well is a re�exive tool that can be used to evaluate a research especially for a nation like Nepal. Theresearch funds or the bene�ts that ensues a researcher are important criteria for research. When thinking of a research topic, the primary determining factorbecomes the amount of fund available, the gaze of a native researcher can overlook various conditions and processes.
From the depths of the epistemic well when researches are done, health issues are assumed to be self-evident problems(Krieger, 2010). The process ofnaturalisation of socially produced risk(Schulz and Siriwardane, 2015), (re)production and normalisation of social divisions(Steinberg, 2002), neutralizationof negative health impacts(Nilsson, 2009) shapes researches in�uenced by neoliberalism. “Wayne Brekhus referred to this as the process of ‘unmarking’problems so that what was marked as clear and evident becomes virtually unnoticed and, by virtue of that, ‘unremarkable’”(Gubrium and Järvinen, 2013). “Theprevailing dominant discourse in the health profession is biomedical, micro level, individualized and depoliticized and this tradition treats health as theabsence of illness or disease in individuals and pursues to improve quanti�able aspects of their lives through the lessening of risk factors via indicators ofmorbidity and mortality”(Brassolotto, Raphael and Baldeo, 2014b). Those espousing this world view typically accept that work against disease is empiricallydesirable hence necessitating no additional rationalization: the epidemiology (the evidence) is normally believed to "speak for itself"(Seedhouse, 2004)(Battersby, 2008).

Page 6/20
In order to explore the philosophical foundations that guide the philosophical foundations of health research of native researches an analysis of thehealth researches on noncommunicable diseases presented during the NHRC conference in 2016 was conducted. The book of abstracts for the year 2016 wasavailable from the NHRC website for public use. In total twenty two researches were presented under the theme of NCD in the conference. Amongst these twowere excluded one was on a clinical study of Maxillary Anterior Teeth and the other was on gender-based study of pattern reversal visual evoked potential.
Based on pragmatism we hold that the most important determinant of the research philosophy adopted are the research questions which also guidethe other aspects of the research(Higgs, Horsfall and Grace, 2019). The �nal and visible product of any research are the �ndings, results andrecommendations which are shaped by the methodologies and methods adopted, but behind these lie the usually invisible part which are the ‘ontologicalnature of social reality’, the epistemological nature and understanding of knowledge and the axiological position of the researcher(Held, 2019). A researchquestion or a hypothesis, (hypothesis serves as an extension of the research question) can be looked at from different angles and using different methods toprovide different types of answers(Carpiano and Daley, 2006). Research methods are linked through methodology and epistemology, to an ontologicalposition(Johnstone, 2004). It is impossible to engage in any form of research without committing (often implicitly) to ontological and epistemologicalpositions. Researchers’ differing ontological and epistemological positions often lead to different research approaches towards the samephenomenon(Mingers, 2003)(Grix, 2002).
The selected twenty researches were analysed of their a) research objectives, aims or goals b) methodology and methods used and c) conclusions,discussions and recommendations made (see �gure3). Each research was approached with the following questions.
What are the stated objectives, justi�cation, rational, aim or purpose of the research?
What or who are the subjects of study of the research?
What are the methodologies and methods followed in the research?
What type of data does the methodology aim to generate?
What are the �ndings of the research?
What are the recommendations of the research?
After obtaining the answers to the above mentioned questions these components were then subjected to questions philosophical in nature. Thesequestions were framed by keeping in mind the different stages of research. Since assumptions are inherently present in any research here too the primaryquestion asked was, what are the assumptions in the research?
1. “What are the ontological assumptions? What is the nature and constitution of objects in the external world? What is the form and nature of reality and,therefore, what is there that can be known about it”?(Sławecki, 2017)
2. “What are the epistemological assumptions? How can we as researchers gain knowledge about the external world? What is the nature of the relationshipbetween the knower or would-be knower and what can be known”?(Sławecki, 2017)
3. “What are the methodological assumptions? How research should or ought to proceed given the nature of the issue it seeks to address? How can theinquirer (would-be knower) go about �nding out whatever he or she believes can be known”?(Sławecki, 2017)
4. What are the axiological assumptions? How has ethics been maintained and what are the values of the research? (Sławecki, 2017) “Whether researchshould be “neutral” or valued-oriented and pragmatic/utilitarian, about the utility and application of the produced knowledge”?(de Camargo, Ortega andCoeli, 2013)
The �rst question deals with ontology and involves the philosophy of reality(Last, 1986). Ontology is the study of reality/being and it shapes ourviews and affects our sight(also called metaphysics)(Rychetnik et al., 2004). “The researcher’s view of reality is the corner stone to all other assumptions, thatis, what is assumed here predicates the researcher’s other assumptions. As applied to healthcare research, ontology is about the nature of reality that is worthinvestigation” (Turyahikayo, 2014). For instance, one could view poverty as the result of individual attributes like laziness, drunkenness, ignorance or one couldview poverty as the result of the development model followed.
The second question deals with epistemological beliefs that the researcher has about the nature of knowledge what counts as educationalknowledge and how is it obtained’ or ‘how can we as researchers gain knowledge about the external world?’(Bryant, Raphael and Travers, 2007) Epistemology addresses how we come to know the reality(Onoruoiza et al., 2015). Researcher’s differing ontological and epistemological positions lead todifferent research approaches towards the same phenomenon(Voros, 2008). For instance the differing ontological views on poverty as mentioned in the aboveparagraph leads to different epistemic beliefs. The �rst view on poverty can lead the researcher to believe that knowledge about proper counselling andknowledge that can bring about behavioural change is desired. The second view on poverty can lead the researcher to believe that the limitations of theparticular developmental model be identi�ed and acted upon so as to reduce poverty.
The third question deals with the methodological approaches, the researcher uses. Methodology can be individualist, holist, quantitative, qualitative,inductive, deductive and mixed. Continuing with the example on poverty, the differing positions will pursue different methodology. The �rst view that poverty isthe result of individual attributes can employ methods such as in-depth interviews and study the life style practices that act as hindrances to lesseningpoverty. The second view can look at the reasons why a particular developmental model is followed and in the process could interview policy makers anddevelopment experts. The chosen methodology and “methods can be traced back, through methodology and epistemology, to an ontological position”. Theresearcher’s ontological and epistemological perspective affects the topic selection of the research. “Researchers’ ontological and epistemologicalassumptions are apparent in the questions and methodological approaches that they select. If one’s answer to the ontological query is that a knowable reality

Page 7/20
exists, then his or her research will vary greatly from researchers who hold the conviction that reality is individually or socially constructed. ”(Marley and Levin,2011)
The fourth question deals with the axiological nature of the researcher and focuses on values in the research process or morals and ethics. Axiologyis the theory of values, and values are aspects of human behaviour that emerged during evolution and gave us aims, goals and opinions which through ourknowledge direct our actions. The axiological nature of the research is inherently present during all stages of a research. In (See �gure 1) the process ofresearch has been shown.
The characteristics of the epistemic well can affect a research at different levels. The research could be giving us the true nature of the problem inquantitative measure but the understanding of the problems could be decontextualized, deproblematized and detached. For example if a research was done tostudy the breast feeding practices of mothers with children up to six months in an industrial/manufacturing region. I do house hold visits and collect data onbreast feeding practices and I conclude that breast feeding is low since mothers are ignorant and need to be motivated through health literacy and healthpromotion programs. Also I suggest proper counselling to the mothers about the importance of breast feeding. My methods of data collection were semi-structured questionnaire and interviews. I visit the houses on a Saturday since it is a holiday and hence informant would be at home. Based on therecommendations of the study an intensive promotional program was developed and mothers were given health literacy awareness, awareness programs inlocal radio and posters and pictures in schools to increase awareness among the children who in turn would diffuse the message in the family. Now anotherresearcher comes to the same study site and studies the same issues on breast feeding among the same sample population. The researcher goes to the siteand does an ethnographic study and comes up with the conclusion that women giving birth only get 40 days of leave with salary from the factories. After fortydays the mother’s have to work 9 hours shift and if they start taking leave after the allotted 40 days of leave their daily wage or salary will be subtracted.Moreover if she does not join the work after a maximum of two months their job contract will be terminated and she will be replaced. The researcher �nds thatmothers know the importance of breast feeding for the �rst six months but she is faced with a choice, the choice of losing a job in a region with highunemployment. The researcher sees the solution in having a collaborative effort at solving the problem by bringing in the factory management, local andnational government, the mothers and health workers.
In �gure three the methodological process has been shown. The epistemic well informs the researcher as a result of which the research methods,�ndings and recommendations display certain assumptions on which the research is built. These assumptions of different nature that exist at different levelswhen taken together can be identi�ed as the philosophical foundations of the researcher. The philosophical foundations of a researcher when shaped bycomponents of the epistemic well can produce research that is detached from the reality it studies. For instance, how useful is a research if a researcherconducts a research on effects of teaching hand washing practices among school going children, how valid will the research objectives, research questionsand the �ndings be if the researcher were to discover that the school has no regular and constant water supply.
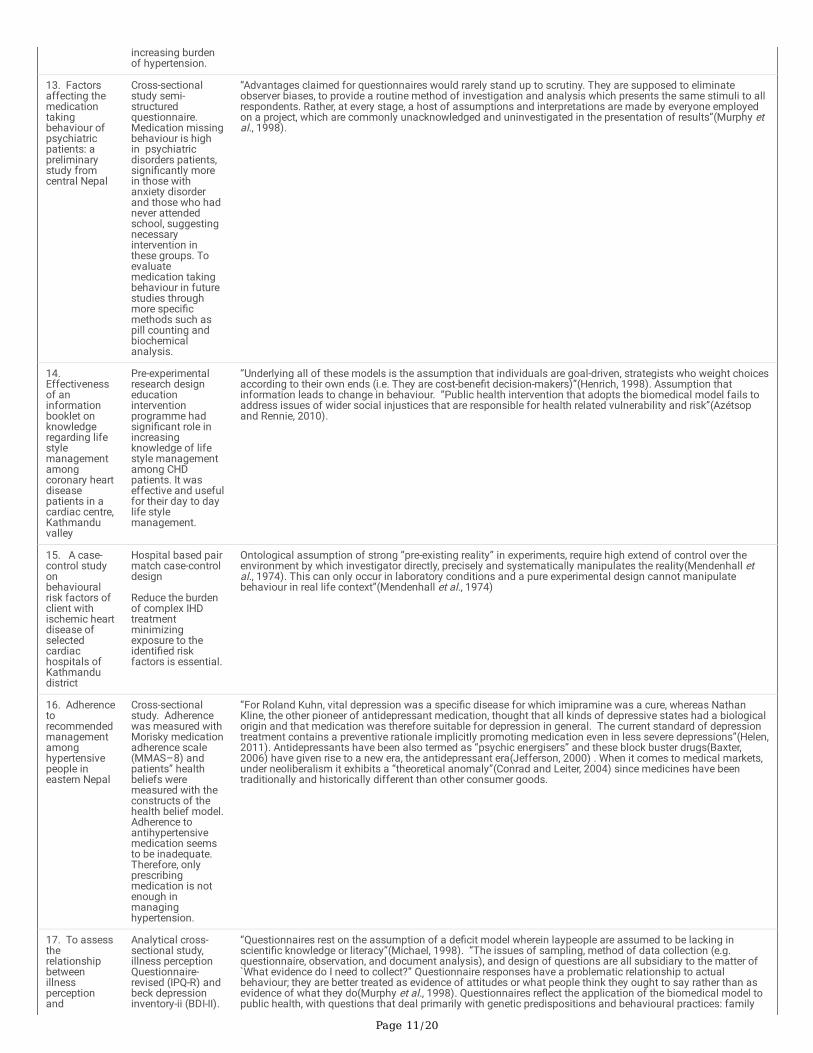
4. FindingsThe �ndings of the study are discussed in table one. The �rst column mentions about the research title, objectives and rationales for the selected researchpresentations. The second column mentions about the research methodologies, methods, recommendations and conclusions of the selected researches. Thethird column contains arguments made by the author about the selected researches. The author seeks to identify the assumptions inherent in the researchesand also seeks to discern the traits of the epistemic well displayed by the researches. The comments have been informed by literature review and theontological understanding possessed by the authors. Being a native the authors attempt to look at the researches not by detaching one’s self but byincorporating the real lived empirical experiences of the authors.
Analysis of the researches

Page 8/20
Table – 1 Table on non communicable diseases researches and their assumptions
Objectives,aim s, goals
Methodology andmethodsRecommendationsand conclusions
Assumptions inherent in the research and characteristic features of epistemic well displayed
1. Mothersknowledge,attitude,behaviourregarding dietphysicalactivity of pre-schoolchildren
Cross-sectionalstudy, interviewedall mothers havingchildren aged 2 to 7years, knowledge,attitude andbehaviourresponses. Poorcorrelation ofmothers”knowledge andattitude withchildren’s behaviourregarding diet andphysical activity.Barriers, facilitatorsthat affectmothers” practicestowards theirchildren beexplored andaddressed.
Historically from the 1916 onwards the understanding that ignorance of the mother was the primary cause forpoor health conditions of the children was accepted as a truism(Porter, 2005b). This understanding hascontinued strongly and under a neoliberal system when commodi�cation is the norm, “women are oftenassumed to have no speci�c health needs outside of their mothering roles, an assumption borne out by most ofthe existing health programmes that target women only during their reproductive years”(Parsitau, 2008). Thevicious cycle of ill health, ignorance, and poverty starts in the womb(Green, 2012). The mother’s apparent lack ofinterest can be appreciated when one realizes that parents in highly impoverished families have varied andtremendous burdens to bear”(Fox, 2002). The ontological assumption that ignorance of mother’s knowledgeattitude is barrier regarding children’s eating behaviour. The epistemological assumption that barriers can bestudied epidemiologically and facilitating factors can be explored at the individual level. Methodologicalassumption that the process of study and data collection at the individual level will provide a true picture.Atomistic nature dealing at the individual behavioural level. “Cross-sectional studies do not resolve problemsrelating to health care systems or the results of quantitative research methods are often not implemented inclinical practice, particularly using cross sectional studies in examining attitudes, beliefs, and values and quasi-experimental designs”(Tavakol and Aa, 2004).
2. Prevalence ofdepression,identifyfactorsassociatedwithdepressionamonginmates
Cross-sectionalstudy, depressionassessed usingcentre forepidemiologicstudies depressionscale CESD). Highrate of depression,needmedical/psychiatriccare.
. The epistemological and “ontological problems in de�ning the concept mental disorder and in delineatingclinical entities are conspicuous, and many clinicians and psychotherapists �nd the categories and diagnosticcriteria of both the DSM and the WHO’s ICD-10 in many ways inconvenient or trivial when applied to individualcases in clinical practice”(Helen, 2011). “The general way in which the questions are asked raises the suspicionthat even people who would not fall into the category of “depression” if diagnosed by a professional psychiatristmight be pushed to believe that they are depressed and in need of medicines”(Ecks, 2005). The murkyrelationship between the universalistic biomedical perspective of psychiatric problems and a locally informedone Has been discussed by Harper. Much psychiatric research in Nepal is a direct outgrowth of the former,wherein statistics that suggest how prevalent conditions like “depression,” etc. are generated. Such research notonly contributes to the Westernization of psychiatric problems, but in Nepal also perpetuates structural inequalityby the very categories used in statistical studies(Harper, 2014). The “pharmaceutical industry is increasinglyemploying strategies of direct- to-consumer marketing, aiming to create a popular recognition of depressivesymptoms, to “grow the market”, and to foster a demand for speci�c medications”(Ecks, 2005). The increasingtrend of the use of pharmaceutical products for various mental conditions has termed this era as “theantidepressant era”(Jefferson, 2000).Assumptions that a questionnaire will give the correct answers. Prisonerswill give the correct answers irrespective of their present mood condition. “Subjectifying nature” of thequestionnaire has been criticized on many counts. “Interest in depression in the �eld of international health wasintertwined with the emergence of a new generation of antidepressant drugs, the serotonin reuptake inhibitors(SSRI)”(Ecks, 2005). The pharmaceuticalization(Williams, Gabe and Davis, 2008), medicalization andbiomedicalization,(Clark, 2014a) of everyday life conditions including mental health have been addressed.
3. Determinantsof healthrelated qualityof life in COPDchronicobstructivepulmonarydisease
Hospital basedsurvey
Older age, �nancialdi�culties,smoking status,increasing dyspneascore, number ofexacerbations, selfperceived declininghealth status, andperceived impacton workingcapacity.
The “concepts of perceived health status, quality of life and health-related quality of life can be complex toanalyse as they might be mediated by several interrelated variables, including self-related constructs (e.g. self-e�cacy, self-esteem, perceived control over life) and subjective evaluations could be in�uenced, in theory, bycognitive mechanisms (e.g. expectations of life, level of optimism or pessimism, social and cultural values,aspirations, standards for social comparisons of one’s circumstances in life)”(Bowling, 2001). Without takinginto consideration “political unrest, environmental disaster, declining economic performance, the introduction ofstructural adjustment programmes, un-responsive governance, and weak public-health infrastructure changingpopulation dynamics, the advent of HIV/AIDS, and the onset of globalisation”. The HRQL is limited. “A universalquestionnaire to elicit the relevant information for a number of conditions would need to be of enormouslength”(Bowling, 2001).Assumes checklists and “HRQL (health related quality of life) instruments are enough togather information. Controversy around validity of these measures; investigators concerned with the question ofwhether these systems are measuring what they intend to measure. Given an absence of a benchmark of health,determining criterion validity—comparing the results achieved to an accepted gold standard—is impossible”(Gold,Stevenson and Fryback, 2002). “HRQL measures placed a greater emphasis on issues such as measureresponsiveness, sensitivity and reliability, paying less attention to generating overall models of diseasedistribution, severity, and mortality"(Gold, Stevenson and Fryback, 2002).
4. Perceptionsand beliefs ofpeople livingwith type 2diabetes
In-depth interview,individual interviewwith policy levelpeople.
Unhealthy life styleis the main causeof diabetes,awareness programshould be initiated,should be kept inthe school levelcurriculum also.
The awareness program that it talks about is with an ontological understanding of the reality guided by theindividualist, reductionist and de-politicized philosophy. Without taking into account the structure ofneoliberalism and by naturalising the commodi�cation and marketisation the school level curriculum basedawareness program will focus on individual habits, morals and life-style. Assumption at an ontological level ofthe reality and the epistemological assumptions about the knowledge generated. Atomistic, individualistic andreductionist in nature. The life-style one acquires must be based on rational choices and if one gets diabetes it isbecause of the individual who makes wrong decisions. Public health in�uenced by the biomedical model has atendency of victim blaming,(Lupton, 2015) which locates the cause and cure of disease as exclusively within theindividual.

Page 9/20
5. Factorsassociatedwith physicalactivities,experiences ofelderlyregardingfunctionalactivities
Cross sectionalsurvey, individualinterviews usingstructured pretestedinterview guideline,hermeneuticalphenomenologicalapproach, Gibson’squalitative analysismethod.
Functionallimitation in basicand intermediateactivities. Nationalpolicy needs toconsider the factorsfor enhancingfunctionalactivities, alsopromote role of thefamily members forelderly care.
Assumptions that government has full control and power along with willingness. The policies it implements suchas removal of subsidies, cutbacks in social expenditures and austerity measures indicate a contradictoryapproach to welfarism. Ontological assumptions regarding functional activities. For example, A has to share acommon toilet where as B has a private bathroom and hence their functional needs are different.Epistemological assumptions seen when physical activities and functional activities are considered asknowledge that is desirable and needed.
6. Find thehealth literacyandknowledge ofdiseaseamong thepatients withchronicdisease.
Cross sectionalstudy wasconducted,interviewed face toface, translated,pretested, validatedEuropean healthliteracy survey(HLS-EU-ASIA-Q)2questionnaire.
Respondents withsu�cient healthliteracy knewsigni�cantly moreabout the diseasethan those withinadequate healthliteracy. Healthliteracy isindependentlyassociated withdisease knowledge.
Health literacy or mass education strategies is an individualistic approach which views the “responsibility forreducing exposure to risk factors in individuals, and is emblematic of a medicalized framing of healthproblems”(Clark, 2014a). Assumptions that increased knowledge and health literacy will translate to betterpractise. The “upstream social determinants of health such as marketing of unhealthy foods to children andlater drift downstream by relying on strategies to directly change the behaviour of individuals has beendescribed as a lifestyle drift” promoted by the policy makers as reductionist in nature”(Clark, 2014a). Theneoliberal philosophy where the invisible hands of the market will su�ce to create a developed nation seemsrather tempting but these activities have a lasting effect especially as NCD’S are often interconnected and requirelong term solutions(Clark, 2014b).
7. Reliabilityand factorstructure ofperceivedstress scale-14 (PSS-14)amongNepaleseadolescents.
Cross-sectional andschool-basedsurvey wasconducted inMyagdi district inNepal in 2015.Reliable tool withcaution to measurestress.
Assumptions that PSS-scale and questionnaires can be used for stress amongst adolescents. “Questionnairesare supposed to eliminate observer biases, to provide a routine method of investigation and analysis whichpresents the same stimuli to all respondents. Rather, at every stage, a host of assumptions and interpretationsare made by everyone employed on a project, which are commonly unacknowledged and uninvestigated in thepresentation of results”(Murphy et al., 1998).
8. Prevalence of depressionamongsurvivors offemaletra�cking inshelter homesof Kathmanduvalley
Clinical diagnosisaccording to ICD-10classi�cation ofmental andbehaviouraldisorders-diagnostic criteria.Hamilton ratingscale fordepression (HAM-D) was used toassess the severityof depression (mild,moderate andsevere).
Evidence ontra�cked people’sexperiences ofviolence and ofdepression andother mental healthproblems isextremely limited. Requires acoordinatedresponse by healthcare providers andother supportservices.
The thousand-fold increase in the prevalence of depression and it becoming a public health problem happenedlargely due to the development of psychiatric epidemiology since 1950”s(Helen, 2011). The sale of psychotropicdrugs is big business(Wong, 2006). The current depression paradigm is the tendency to think of depression aswell as other mood disorders as objects instead of as an experience with a speci�c context. Movement towardthing-like status makes mania and depression seems possible to identify, manipulate, and optimize through thetechnology of psychotropic drugs and through taxonomic apparatuses(Helen, 2011).
9. The Descriptive cross- “Questionnaires in effect �lter the social processes under study through a pre-de�ned “grid” of categories

Page 10/20
prevalence ofdepressionand theircorrelates andassociation ofphysicalactivity withphysicalactivityamong highersecondarystudents
sectional study wasdesigned globalphysical activityquestionnaire(GPAQ) for physicalactivity and beckdepressioninventory IBDI-IA)for depressionalong with somesocio-demographicvariables.
Global physicalactivityquestionnaire(GPAQ) for physicalactivity and beckdepressioninventory IBDI-IA)for depressionalong with somesocio-demographicvariables.
assumed to represent the range of possible alternative responses appropriate to the area of research. Fixedchoice (yes/no) questions represent the extreme in this respect, but scaling techniques may be no lessinappropriate. It is meaningless to produce measurements or quali�cations of phenomena whose dynamics arenot yet understood”(Murphy et al., 1998). Most studies of area effects on health are cross sectional; that is;measures of the place and of the residents’ health are collected at roughly the same time. When one starts tothink about socially and biologically plausible causal pathways by which place might in�uence health thesecross-sectional designs often appear inappropriate(Macintyre, Ellaway and Cummins, 2002). In the attempts tomake psychiatry more scienti�c the triumph of the styles of reasoning familiar from epidemiology and socialmedicine–statistical induction, probability calculus and risk estimation– has been much more crucial than therise of psychopharmacology and neuropsychiatry. “It is nowadays almost impossible to present claims aboutmental health facts without supporting them by statistical analysis of data from epidemiological questionnairesor randomised clinical trials”(Helen, 2011).
10. To assessthe utilizationof health careservicesamong theelderly
Quantitativedescriptive-crosssectional study,using anintervieweradministered semi-structuredquestionnaire
Monthly familyincome, chronicdisease, elderly onmedication and selfrated health arestrongly associatedwith utilization ofhealth care servicesby elderly peopleand suggestsfurtherinterventions toimprove the healthcare serviceutilization byelderly people.
This suggestion is based upon the idea that “individuals should have the opportunity to live to the same age asothers—that there is a prima facie right to a minimum number of life-years”. The limitations of conventionalhealth care systems are obvious. The narrowly technological approach to health care serves to block theintegrated utilization of health economic and other resources. In fact highly professionalized and technologicalhealth services cannot be equitably distributed as it is neither possible nor desirable to have a hospital in everyvillage. The task rather, is to attempt to change the composition of health services-away from hospitals andtowards primary care-through their more equitable distribution and to make them part of overall economic andsocial development(Gish, 1979). “Since access to such public provision is often heavily unequal acrosslocations, and within communities, this gap constitutes a signi�cant weakness, especially in the context of cross-sectional or inter-temporal comparative analysis. In many situations, even households that have the �nancialcapacity might �nd it impossible to obtain adequate education and health services simply because thoseservices are not available locally. The poverty-line approach implicitly assumes that money can buy health,education and other services at any time and in any place or that these are provided by the State”(Novak, 1995).
11. To explorethe quittingattemptsamongadolescentsmokers inDharanmunicipalityof easternNepal
Cross sectionalstudy wasconducted usingpre-tested selfadministeredquestionnaireadapted fromglobal youthtobacco survey toassess currentsmokers andquitting attempts
Relapse oftenoccurs. Tobaccofocusedinterventions tosupport abstinenceare of potentialvalue.
“Self-report surveys share certain limitations that are characteristic of the self-report method. The primaryweaknesses of self-report surveys are a function of the adequacy of the sample and the accuracy ofmeasurement. The issues bearing on the adequacy of a survey’s sample are ensuring representative participationand receiving cooperation throughout the survey questionnaire. Measurement accuracy is an outcome of askingquestions correctly and respondent candor and memory. Although it appears that respondents are generallytruthful in reporting their experiences underreporting is a threat to validity for self-report studies”(Bryant et al.,2007).
12. To �ndout theprevalence ofhypertensionalong withotherassociatedcardiovascularrisk factors ina ruralcommunity ofeastern Nepal
Cross sectionalstudy, WHO stepquestionnaire used.
Prevalence ofhypertension in therural setting wasfound to be as highas 38.6%. Effectiveinterventionregardingprevention alongwith earlydiagnosis andtreatment isnecessary forcontrol of
The “focus on practitioner cultural competence is based on assumptions that: (a) mental health services andinterventions can reduce health disparities; (b) that these interventions are more accessible, acceptable andeffective when they are culturally adapted; and (c) that practitioners can acquire speci�c knowledge, attitudesand skills that will improve their delivery of effective culturally appropriate and responsive mental healthservices”. There is modest evidence for each of these propositions. “Questionnaires rest on the assumption of ade�cit model wherein laypeople are assumed to be lacking in scienti�c knowledge or literacy”(Michael, 1998). “The issues of sampling, method of data collection (e.g. questionnaire, observation, and document analysis),and design of questions are all subsidiary to the matter of `What evidence do I need to collect?”
Page 11/20
increasing burdenof hypertension.
13. Factorsaffecting themedicationtakingbehaviour ofpsychiatricpatients: apreliminarystudy fromcentral Nepal
Cross-sectionalstudy semi-structuredquestionnaire.Medication missingbehaviour is highin psychiatricdisorders patients,signi�cantly morein those withanxiety disorderand those who hadnever attendedschool, suggestingnecessaryintervention inthese groups. Toevaluatemedication takingbehaviour in futurestudies throughmore speci�cmethods such aspill counting andbiochemicalanalysis.
“Advantages claimed for questionnaires would rarely stand up to scrutiny. They are supposed to eliminateobserver biases, to provide a routine method of investigation and analysis which presents the same stimuli to allrespondents. Rather, at every stage, a host of assumptions and interpretations are made by everyone employedon a project, which are commonly unacknowledged and uninvestigated in the presentation of results”(Murphy etal., 1998).
14. Effectivenessof aninformationbooklet onknowledgeregarding lifestylemanagementamongcoronary heartdiseasepatients in acardiac centre,Kathmanduvalley
Pre-experimentalresearch designeducationinterventionprogramme hadsigni�cant role inincreasingknowledge of lifestyle managementamong CHDpatients. It waseffective and usefulfor their day to daylife stylemanagement.
“Underlying all of these models is the assumption that individuals are goal-driven, strategists who weight choicesaccording to their own ends (i.e. They are cost-bene�t decision-makers)”(Henrich, 1998). Assumption thatinformation leads to change in behaviour. “Public health intervention that adopts the biomedical model fails toaddress issues of wider social injustices that are responsible for health related vulnerability and risk”(Azétsopand Rennie, 2010).
15. A case-control studyonbehaviouralrisk factors ofclient withischemic heartdisease ofselectedcardiachospitals ofKathmandudistrict
Hospital based pairmatch case-controldesign
Reduce the burdenof complex IHDtreatmentminimizingexposure to theidenti�ed riskfactors is essential.
Ontological assumption of strong “pre-existing reality” in experiments, require high extend of control over theenvironment by which investigator directly, precisely and systematically manipulates the reality(Mendenhall etal., 1974). This can only occur in laboratory conditions and a pure experimental design cannot manipulatebehaviour in real life context”(Mendenhall et al., 1974)
16. Adherencetorecommendedmanagementamonghypertensivepeople ineastern Nepal
Cross-sectionalstudy. Adherencewas measured withMorisky medicationadherence scale(MMAS–8) andpatients” healthbeliefs weremeasured with theconstructs of thehealth belief model.Adherence toantihypertensivemedication seemsto be inadequate. Therefore, onlyprescribingmedication is notenough inmanaginghypertension.
“For Roland Kuhn, vital depression was a speci�c disease for which imipramine was a cure, whereas NathanKline, the other pioneer of antidepressant medication, thought that all kinds of depressive states had a biologicalorigin and that medication was therefore suitable for depression in general. The current standard of depressiontreatment contains a preventive rationale implicitly promoting medication even in less severe depressions”(Helen,2011). Antidepressants have been also termed as “psychic energisers” and these block buster drugs(Baxter,2006) have given rise to a new era, the antidepressant era(Jefferson, 2000) . When it comes to medical markets,under neoliberalism it exhibits a “theoretical anomaly”(Conrad and Leiter, 2004) since medicines have beentraditionally and historically different than other consumer goods.
17. To assesstherelationshipbetweenillnessperceptionand
Analytical cross-sectional study, illness perceptionQuestionnaire-revised (IPQ-R) andbeck depressioninventory-ii (BDI-II).
“Questionnaires rest on the assumption of a de�cit model wherein laypeople are assumed to be lacking inscienti�c knowledge or literacy”(Michael, 1998). “The issues of sampling, method of data collection (e.g.questionnaire, observation, and document analysis), and design of questions are all subsidiary to the matter of`What evidence do I need to collect?” Questionnaire responses have a problematic relationship to actualbehaviour; they are better treated as evidence of attitudes or what people think they ought to say rather than asevidence of what they do(Murphy et al., 1998). Questionnaires re�ect the application of the biomedical model topublic health, with questions that deal primarily with genetic predispositions and behavioural practices: family

Page 12/20
depressionamongpatients withdiabetes
High prevalence ofdepressivesymptoms amongdiabetic patients inKathmandu Nepalneedcomprehensivediabetes educationprogram forchanging poorillness perception,which ultimatelyhelps to preventdevelopment ofdepressive.
history of CVD, hypertension, and diabetes; patterns of smoking and alcohol consumption; physical activity levels(including work and leisure); dietary patterns and history of weight gain; and the presence of symptoms of CVD.Questionnaire must be designed to collect data that meet the statistical assumptions of the quantitativetechniques to be used(Glasgow, 2005).
18. Todetermine theprevalence ofCAD riskfactors amonga targetfemalepopulation inNepal
Semi-structuredinterview schedulewas followed forthe data collection.
Diabetes, drinkingalcohol, LDL-C andgeneralized obesitywere found as thesigni�cantpredictors of cadneed of appropriatecontrol strategiesand measuresamong women.
Yach and Beaglehole say that globalization has contributed to the rise in chronic diseases and blame majortransnational corporations and the global communications media for the marketing of tobacco, alcohol, sugaryand fatty foods in nearly all parts of the world(Yach, Beaglehole and Hawkes, 2005). “Emphasising such animperative for behaviour choice, however, obscures the circumstances in which individuals make that choice orindeed have their choices constrained”. The “pricing, availability, marketing and perceptions of costs and bene�tsstrongly in�uence choice of unhealthy product consumption”. “Dietary risk factors and physical inactivity areonly partially determined by individual preferences and are more so “substantially in�uenced by themanufacturing and marketing practices of the food industry and by the built and social environments that permitor impede physical activity”. Adopting the values of a medicalized approach immediacy, e�ciency and controlthe use of “quick �x” or “magic bullet” strategies designed to in�uence individual choices rather than governmentpolicies or the activities of manufacturers is tempting in the short term, but will not have a lasting impact,especially as NCDs are often interconnected and require long-term solutions”(Clark, 2014b). Focus is on theupper, super�cial, echelons of the process and is rarely of the process itself. It stands in contrast to the viewdubbed "holistic" or "physiological" that stresses individuals and their adaptation - physical, psychological, social- to their environment(Baxter, 2006).
19. To assessthe stages,self- e�cacy,motivationand decisionmaking ofsmokingcessationamongadolescents inselectedschools ofPokhara
Cross-sectionaldescriptive designusing quantitativeapproach, self–administered semi-structuredquestionnaire
Smokers were notprepared to quitbecause they wereless motivated, notwanting to changewas foundassociated withlower self- e�cacy.
“Public health workers are determined to focus on problems that interest them as researchers and not on theproblems of concern to individuals”(Syme and Ritterman, 2009). “Much of public health continues to treatbehaviours such as diet, smoking, violence, drug use, and sex work as if they were voluntary decisions, withoutregard to social constraints, inducements, or pressures”(Glass and McAtee, 2006).
20. Toidentify theprevalenceand the riskfactorsassociatedwith eldermistreatmentin urbanNepal.
Descriptive cross-sectional study,information wascollected using anintervieweradministered Semi-structuredquestionnaire.
Older adults inurban Nepal self-reported a higherrate ofmistreatment.Awareness,intervention andpreventionstrategies targetingelder populationand their family isrequired to addresssuch mistreatment.
“Elders generally felt that improved health should “start at home”, partnerships at the community and systemslevels were often referred to as more likely solutions than individual and interpersonal ones”(Hermann et al.,2010). The part by part solution to identify risk factors for anything pathological has been the trend followed byresearchers. Mistreatment occurs due to lack of awareness and prevention, intervention and awarenessstrategies are sought for solving the problem. Mistreatment for one could be not getting to see a favouritetelevision program and for another could be not having money for medicines. More than lack of awareness, eldermistreatment is more about values.
5 Conclusion The neo-liberal research, researcher, universities, organisations are all in sync with one another and this creates a culture of doing research projectsone after another. The neo-liberal researcher is bound by practices set by councils, universities, committees and so on. Since the promotion criteria of a facultydepends mainly on the number of research publications in peer review journals, the number of research projects completed, number of conferences attendedand so on, the pressure of doing research and publishing them is omnipresent. Hence for example “A” an assistant professor joins a university after �nishingMD or PhD and in three years time “A“ can become an associate professor with an increase in pay and other facilities such as conference grants. But they aresome basic conditions that “A” will have to ful�l in order to get promoted such as “A” needs three research publications in peer reviewed indexed journals,received one project grant and completion of one project or study. If “A” has ful�lled this in paper “A” gets promoted. This process continues till “A” becomes aprofessor. The other indispensible function that “A “does is teaches students a course in the university. And if “A” since as a physician “A” also caters to thepatients. Now what is perplexing is the role of a teacher and a surgeon are not given any signi�cant weight. “A” may be an excellent teacher and surgeon butwithout the minimum number of research publications “A” cannot be promoted. So despite the busy schedule “A” has, starts doing a questionnaire survey

Page 13/20
among visiting OPD patients and generates the hypotheses that, “patients coming to the hospital in red colour cars are more prone to diabetes than patientscoming in black colour cars”. So “A” selects the sample population, collects the data, generates the data and publishes the data in a peer review journal. Now“A” has to do several researches in this case let us keep it to three for every stage of promotion and with three years intervals. To be a professor, one begins asassistant professor then associate, additional and �nally a professor.
The mantra of faculty promotion is in�uenced by the practise of, “publish or perish” where for every level of promotion one needs to ful�l the requirednumber of publications. The pressure to climb up the hierarchy is desirable among all of us including academicians, researchers or any other profession. Sothe combination of this desire to climb up and along with the criteria set by universities the onus falls on the individual to publish. Under this system theevaluation is not affected by the views of those who are at the receiving end such as the community. To clarify my point here I again bring in “A” who quali�esfor promotion in three years time but without the minimum number of publications i.e. three “A” will not be promoted. To publish is a time consuming processand after teaching activities and clinical duties “A” has very less time. Also let me mention that “A” values the role of a teacher and spends time on preparingclasses which the students appreciate since they learn a lot. The patients that visit “A” are also very satis�ed. But soon “A” realises that it is researchpublications that counts and not the everyday dealings with students and patients. So “A” starts valuing research publications more and within a few years,the new students and the new patients that are affected by “A” have an opinion different than before. The students are not happy with the classes and neitheris the patient that “A” deal”s with. For “A” satisfying criteria’s set by the university are more important, like number of articles published and number of projectscompleted. As these are decisive factors for promotion and since no or a minimal value is given to opinions of patients and students, these processes begin tobe devalued. Citing bias as a factor if patients and students evaluations are given credence, the notion that if there are given any weight it could become abargaining tool. Publications are tangible products which can be seen and quanti�ed where as feelings are not.
Understanding the processes behind a phenomenon and identifying the causal factors and the actors are both important. The article is a call to thenative epistemic communities to climb out of the epistemic well and to develop a critical understanding. If one were to walk on the road and slip on a bananaskin and fall, and the recommendation and advice received were, ‘get your eye checked’, and ‘see where you walk’, how valid would be the suggestion?
References1. Ahlborg, H. and Nightingale, A. J. (2012) ‘Mismatch between scales of knowledge in Nepalese forestry: Epistemology, power, and policy implications’,
Ecology and Society, 17(4). doi: 10.5751/ES-05171-170416.
2. Ahmed, S. P. N. T. (2014) ‘In the Light of Epistemological Debates about Knowledge , is “ Evidence-Based ” Policy Making ( in the Britain ) Anything Morethan Political Rhetoric ?’, Public Policy and Administration Research, 4(4), pp. 111–119.
3. Allen, P. M. and Varga, L. (2007) ‘Complexity: The Co-evolution of epistemology, axiology and ontology’, Nonlinear Dynamics, Psychology, and LifeSciences, 11(1), pp. 19–50.
4. Amstutz, M. R. (2013) ‘International ethics: concepts, theories, and cases in global politics’, Choice Reviews Online. Rowman & Little�eld Publishers,51(02), pp. 51-1130-51–1130. doi: 10.5860/choice.51-1130.
5. Annetts, J. et al. (2017) Contesting neoliberalism:, Understanding social welfare movements. New York: The Guilford Press. doi: 10.2307/j.ctt1t890j0.17.
�. Ayo, N. (2012) ‘Understanding health promotion in a neoliberal climate and the making of health conscious citizens’, Critical Public Health, 22(1), pp. 99–105. doi: 10.1080/09581596.2010.520692.
7. Azétsop, J. and Rennie, S. (2010) ‘Principlism, medical individualism, and health promotion in resource-poor countries: Can autonomy-based bioethicspromote social justice and population health?’, Philosophy, Ethics, and Humanities in Medicine, 5(1), pp. 1–10. doi: 10.1186/1747-5341-5-1.
�. Backhouse, R. E. (2007) ‘The Politics of Method in the Human Sciences: Positivism and Its Epistemological Others’, History of Political Economy. DukeUniversity Press, pp. 167–169. doi: 10.1215/00182702-2006-028.
9. Bahadur Karki Dharma Kanta Baskota, K. (2017) ‘Abstract Book of First National Summit of Health and Population Scientists in Nepal Welcome LetterAbstract Book of First National Summit of Health and Population Scientists in Nepal Table of Contents’, in, p. 236.
10. Baronov, D. (2012) Rick Rowden, The Deadly Ideas of Neoliberalism: How the IMF has Undermined Public Health and the Fight against AIDS , InternationalSociology. Zed Books Ltd. doi: 10.1177/0268580911427999.
11. Battersby, M. (2008) ‘Applied Epistemology and Argumentation in Epidemiology’, Informal Logic, 26(1), p. 41. doi: 10.22329/il.v26i1.430.
12. Baxter, S. M. (2006) Medicine, metaphors and metaphysics: An interdisciplinary analysis of the ethical, medical and sociocultural questions raised bytherapeutic equivalence, ProQuest Dissertations and Theses. Simon Fraser University. Available at: http://ezproxy.cul.columbia.edu/login?url=https://search.proquest.com/docview/304942340?accountid=10226%0Ahttp://rd8hp6du2b.search.serialssolutions.com?ctx_ver=Z39.88-2004&ctx_enc=info:o�/enc:UTF-8&rfr_id=info:sid/ProQuest+Dissertations+%26+Theses+Global.
13. Birn, A.-E. (2014) ‘Philanthrocapitalism, past and present: The Rockefeller Foundation, the Gates Foundation, and the setting(s) of the international/globalhealth agenda’, Hypothesis, 12(1), pp. 1–27. doi: 10.5779/hypothesis.v12i1.229.
14. Bowling, A. (2001) Public health-Research-Methodology. 2. Community health services-Research-Methodology. I. Title. RA440.85 .B69, Research methodsin health(2th). Open University Press. Available at: www.openup.co.uk.
15. Brassolotto, J., Raphael, D. and Baldeo, N. (2014a) ‘Epistemological barriers to addressing the social determinants of health among public healthprofessionals in Ontario, Canada: A qualitative inquiry’, Critical Public Health. Emerald, 24(3), pp. 321–336. doi: 10.1080/09581596.2013.820256.
1�. Brassolotto, J., Raphael, D. and Baldeo, N. (2014b) ‘Epistemological barriers to addressing the social determinants of health among public healthprofessionals in Ontario, Canada: A qualitative inquiry’, Critical Public Health, 24(3), pp. 321–336. doi: 10.1080/09581596.2013.820256.
17. Breilh, J., Campana, A. and Hidalgo, F. (2005) Latin American Health Watch: Alternative Latin American Health Report.
Page 14/20
1�. Briggs, D. J., Sabel, C. E. and Lee, K. (2009) ‘Uncertainty in epidemiology and health risk and impact assessment’, Environmental Geochemistry and Health,31(2), pp. 189–203. doi: 10.1007/s10653-008-9214-5.
19. Brown, P. (2003) ‘Qualitative methods in environmental health research’, Environmental Health Perspectives, 111(14), pp. 1789–1798. doi:10.1289/ehp.6196.
20. Brown, W. (2006) ‘American nightmare: Neoliberalism, neoconservatism, and de-democratization’, Political Theory, 34(6), pp. 690–714. doi:10.1177/0090591706293016.
21. Bryant, C. D. et al. (2007) 21St Century Sociology: a Reference Handbook, Choice Reviews Online. doi: 10.5860/choice.45-0027.
22. Bryant, T., Raphael, D. and Travers, R. (2007) ‘Identifying and Strengthening the Structural Roots of Urban Health in Canada: Participatory Policy Researchand the Urban Health Agenda’, Promotion & Education, 14(1), pp. 6–11. doi: 10.1177/175797590701400101.
23. Cahill, D. et al. (2018) ‘Neoliberalism and the University’, in Cahill, D. and Cooper, M. (eds) The SAGE Handbook of Neoliberalism. Sage Publications IndiaPvt. Ltd., pp. 553–563. doi: 10.4135/9781526416001.n42.
24. de Camargo, K. R., Ortega, F. and Coeli, C. M. (2013) ‘Modern epidemiology and its discontents O mal-estar na epidemiologia moderna’, Revista de SaudePublica, 47(5), pp. 984–991. doi: 10.1590/S0034-8910.2013047004777.
25. Campbell, C. and Jovchelovitch, S. (2000) ‘Health, community and development: Towards a social Psychology of participation’, Journal of Communityand Applied Social Psychology, 10(4), pp. 255–270. doi: 10.1002/1099-1298(200007/08)10:4<255::AID-CASP582>3.0.CO;2-M.
2�. Campbell, J., Shrestha, R. and Stone, L. (2010) The use and misuse of social science research in nepal. Second. Mandala Book Point.
27. Carpiano, R. M. and Daley, D. M. (2006) ‘A guide and glossary on postpositivist theory building for population health’, Journal of Epidemiology andCommunity Health, 60(7), pp. 564–570. doi: 10.1136/jech.2004.031534.
2�. Carter, J. A. (2020) ‘Intellectual autonomy, epistemic dependence and cognitive enhancement’, Synthese. Springer Netherlands, 197(7), pp. 2937–2961.doi: 10.1007/s11229-017-1549-y.
29. Carter, S. M. and Little, M. (2007) ‘Justifying knowledge, justifying method, taking action: Epistemologies, methodologies, and methods in qualitativeresearch’, Qualitative Health Research, 17(10), pp. 1316–1328. doi: 10.1177/1049732307306927.
30. Castree, N. (2011) ‘Neoliberalism and the Biophysical Environment: A Synthesis and Evaluation of the Research’, Environment and Society, 1(1), pp. 5–45.doi: 10.3167/ares.2010.010102.
31. Chene, M. Des (2007) ‘Is Nepal in South Asia? The condition of non-postcoloniality’, Studies in Nepali History and Society, 12(November 1995), pp. 207–223. Available at: http://martinchautari.org.np/�les/1_ Mary Des Chene.pdf.
32. ‘Chinese Stories_The frog of the well - Wikibooks, open books for an open world’ (no date).
33. Clack, B. and Paule, M. (2019) Interrogating the Neoliberal Lifecycle, Interrogating the Neoliberal Lifecycle. New York, NY: Springer Berlin Heidelberg. doi:10.1007/978-3-030-00770-6.
34. Clark, J. (2014a) ‘Medicalization of global health 1: Has the global health agenda become too medicalized?’, Global Health Action, 7(SUPP.1). doi:10.3402/gha.v7.23998.
35. Clark, J. (2014b) ‘Medicalization of global health 3: The medicalization of the non-communicable diseases agenda’, Global Health Action, 7(SUPP.1), p. 9.doi: 10.3402/gha.v7.24002.
3�. Conrad, P. and Leiter, V. (2004) ‘Medicalization, markets and consumers.’, Journal of health and social behavior, 45 Suppl, pp. 158–176. Available at:http://gallyprotest.org/medicalization.pdf.
37. Cosgrove, L. and Karter, J. M. (2018) ‘The poison in the cure: Neoliberalism and contemporary movements in mental health’, Theory and Psychology,28(5), pp. 669–683. doi: 10.1177/0959354318796307.
3�. Doll, R. (1999) ‘The limits of epidemiology’, Journal of Radiological Protection, pp. 1–2. doi: 10.1088/0952-4746/19/1/001.
39. Draskovic, M. (2016) ‘Roots and paradoxes of neoliberal apologetics’, Economics and Sociology, 9(1), pp. 209–219. doi: 10.14254/2071-789X.2016/9-1/14.
40. Dunlop, C. A. (2012) ‘Epistemic communities’, in Routledge Handbook of Public Policy. Routledge, pp. 229–243.
41. Dunn, S. (2000) ‘Narratives and newscomers: rethinking culturally appropriate health care’, Nexus, 14, pp. 21–30. Available at:http://search.ebscohost.com/login.aspx?direct=true&db=ant&AN=XRAI02r1201z9162&site=ehost-live.
42. Dutta, M. J. (2016) Neoliberal Health Organizing, Neoliberal Health Organizing. Taylor & Francis. doi: 10.4324/9781315423531.
43. Ecks, S. (2005) ‘Pharmaceutical citizenship: Antidepressant marketing and the promise of demarginalization in India’, Anthropology and Medicine, 12(3),pp. 239–254. doi: 10.1080/13648470500291360.
44. Engel, S. and Susilo, A. (2014) ‘Shaming and sanitation in indonesia: A return to colonial public health practices?’, Development and Change, 45(1), pp.157–178. doi: 10.1111/dech.12075.
45. Esposito, L. and Perez, F. M. (2014) Neoliberalism and the Commodi�cation of Mental Health, Humanity & Society. doi: 10.1177/0160597614544958.
4�. Faber, M., Manstetten, R. and Proops, J. L. R. (2007) ‘Humankind and the Environment: An Anatomy of Surprise and Ignorance’, Environmental Values,1(3), pp. 217–241. doi: 10.3197/096327192776680089.
47. Fine, B. and Saad-Filho, A. (2017) ‘Thirteen Things You Need to Know About Neoliberalism’, Critical Sociology, pp. 685–706. doi:10.1177/0896920516655387.
4�. Fisher, J. A. (2009) ‘Medical research for hire: The political economy of pharmaceutical clinical trials’, Medical Research for Hire: The Political Economy ofPharmaceutical Clinical Trials, 28(3), pp. 1–259. doi: 10.1177/009430610903800530.
Page 15/20
49. Fisher, P. and Lees, J. (2016) ‘Narrative approaches in mental health: Preserving the emancipatory tradition’, Health (United Kingdom), 20(6), pp. 599–615.doi: 10.1177/1363459315600774.
50. Fox, C. (2002) Under the lens, Musical Times. Medico Friend Circle.Voluntary Health Association of India. doi: 10.2307/1004595.
51. Fox, N. J. (2017) ‘Personal health technologies, micropolitics and resistance: A new materialist analysis’, Health (United Kingdom), 21(2), pp. 136–153.doi: 10.1177/1363459315590248.
52. Gish, O. (1979) ‘The political economy of primary care and “health by the people”: An historical exploration’, Social Science and Medicine. Part C MedicalEconomics, 13(4), pp. 203–211. doi: 10.1016/0160-7995(79)90001-7.
53. Glasgow, S. M. (2005) The private life of public health: Managing chronic disease in an era of neoliberal governmentality, ProQuest Dissertations andTheses. University of Maryland. Available at: http://search.proquest.com/docview/304998915?accountid=14511%0Ahttp://sfx.ucl.ac.uk/sfx_local?url_ver=Z39.88-2004&rft_val_fmt=info:o�/fmt:kev:mtx:dissertation&genre=dissertations+&+theses&sid=ProQ:ProQuest+Dissertations+&+Theses+Global&atitle=&title=Th
54. Glasgow, S. M. (2012) ‘The politics of self-craft: Expert patients and the public health management of chronic disease’, SAGE Open, 2(3), pp. 1–11. doi:10.1177/2158244012452575.
55. Glass, T. A. and McAtee, M. J. (2006) ‘Behavioral science at the crossroads in public health: Extending horizons, envisioning the future’, Social Science andMedicine, 62(7), pp. 1650–1671. doi: 10.1016/j.socscimed.2005.08.044.
5�. Gold, M. R., Stevenson, D. and Fryback, D. G. (2002) ‘HALYs and QALYs and DALYs, oh my: Similarities and differences in summary measures ofpopulation health’, Annual Review of Public Health, 23(1), pp. 115–134. doi: 10.1146/annurev.publhealth.23.100901.140513.
57. Goldberg, D. (2013) ‘The preparation of a syllabus in social medicine: McKeown revisited’, Social Medicine, 7(3), pp. 147–156.
5�. Gray, M. and Mcdonald, C. (2006) ‘Pursuing Good Practice?: The Limits of Evidence-based Practice’, Journal of Social Work, 6(1), pp. 7–20. doi:10.1177/1468017306062209.
59. Green, D. (2012) From Poverty to Power Praise for this book. Practical Action Publishing and Oxford: Oxfam International.
�0. Grix, J. (2002) ‘Introducing Students to the Generic Terminology of Social Research’, Politics, 22(3), pp. 175–186. doi: 10.1111/1467-9256.00173.
�1. Gubrium, J. F. and Järvinen, M. (2013) ‘Turning troubles into problems: Clientization in human services’, in Gubrium, J. F. and Järvinen, M. (eds) TurningTroubles into Problems: Clientization in Human Services. Routledge Taylor & Francis Group, pp. 1–237. doi: 10.4324/9780203798010.
�2. Harper, I. (2014) ‘Development and public health in the Himalaya: Re�ections on healing in contemporary Nepal’, Development and Public Health in theHimalaya: Re�ections on Healing in Contemporary Nepal, 35(1–2), pp. 1–164. doi: 10.4324/9781315852508.
�3. Held, M. B. E. (2019) ‘Decolonizing Research Paradigms in the Context of Settler Colonialism: An Unsettling, Mutual, and Collaborative Effort’,International Journal of Qualitative Methods, 18, pp. 1–16. doi: 10.1177/1609406918821574.
�4. Helen, I. (2011) ‘The depression paradigm and beyond’, Science Studies: a Scandinavian journal published by the Finnish Society for Science Studies,24(1), pp. 81–112. Available at: https://helda.helsinki.�/bitstream/handle/10138/27385/Helen.pdf?sequence=2.
�5. Henrich, J. (1998) ‘Henrich Decision Making Cultural Transmission Economic Anthropology’, Theory in Economic Anthropology. Available at:https://deepblue.lib.umich.edu/bitstream/handle/2027.42/35691/b2036009.0001.001.pdf?sequence=2.
��. Hermann, J. et al. (2010) ‘Utilizing the Socioecological Model as a Framework for Understanding Elder Native Americans’ Views of Type 2 Diabetes for theDevelopment of an Indigenous Prevention Plan’, Education.
�7. Higgs, J., Horsfall, D. and Grace, S. (2019) ‘Framing Research Questions and Writing Philosophically’, in Higgs, J., Horsfall, D., and Grace, S. (eds) WritingQualitative Research on Practice. Sense Publishers, pp. 13–25. doi: 10.1163/9789087909086_003.
��. Howson, A. (1993) Regulating Bodies: Essays in Medical Sociology (Book)., Sociology of Health and Illness. Routledge. doi: 10.1111/1467-9566.ep11434442.
�9. Jefferson, J. W. (2000) The Antidepressant Era . David Healy , Isis. doi: 10.1086/384934.
70. Johnstone, P. L. (2004) ‘Mixed methods, mixed methodology health services research in practice’, Qualitative Health Research, 14(2), pp. 259–271. doi:10.1177/1049732303260610.
71. Juul Nielsen, A. and Grøn, L. (2012) ‘Standardising the Lay: Logics of Change in Programs of Disease Self-management’, Culture Unbound, 4(3), pp. 425–442. doi: 10.3384/cu.2000.1525.124425.
72. Karmacharya, B. M. (2011) ‘Shifting the paradigm: Nepal as a potential leader in the �eld of medical education’, Kathmandu University Medical Journal,pp. 1–2. doi: 10.3126/kumj.v9i1.6247.
73. Kelly, A. H., Keck, F. and Lynteris, C. (2019) The Anthropology of Epidemics, The Anthropology of Epidemics. Routledge Taylor & Francis Group. doi:10.4324/9780429461897.
74. Kernot, S. (2006) ‘Nepal: A development challenge’, South Asia: Journal of South Asia Studies, 29(2), pp. 293–307. doi: 10.1080/00856400600849167.
75. Kidd, I. J. and Carel, H. (2017) ‘Epistemic Injustice and Illness’, Journal of Applied Philosophy, 34(2), pp. 172–190. doi: 10.1111/japp.12172.
7�. Kinsella, E. A. and Whiteford, G. E. (2009) ‘Knowledge generation and utilisation in occupational therapy: Towards epistemic re�exivity’, AustralianOccupational Therapy Journal, 56(4), pp. 249–258. doi: 10.1111/j.1440-1630.2007.00726.x.
77. Kirmayer, L. J. (2012) ‘Cultural competence and evidence-based practice in mental health: Epistemic communities and the politics of pluralism’, SocialScience and Medicine. Elsevier Ltd, 75(2), pp. 249–256. doi: 10.1016/j.socscimed.2012.03.018.
7�. Krauss, S. E. and Putra, U. (2005) ‘Research Paradigms and Meaning Making : A Primer’, The Qualitative Report, 10(4), pp. 758–770. Available at:http://www.nova.edu/ssss/QR/QR10-4/krauss.pdf.

Page 16/20
79. Krieger, N. (2010) ‘Workers are people too: Societal aspects of occupational health disparities-an ecosocial perspective’, American Journal of IndustrialMedicine, pp. 104–115. doi: 10.1002/ajim.20759.
�0. Land, R., H.F.Meyer, J. and Baillie, C. (2010) ‘Editors’ Preface Threshold Concepts and Transformational Learning’, in Meyer, J. H. F., Land, R., and Baillie, C.(eds) Threshold Concepts and Transformational Learning. Sense Publishers, p. xxiii. Available at: http://dro.dur.ac.uk/26122/1/26122.pdf.
�1. Last, J. M. (1986) A dictionary of epidemiology. Sixth, International Journal of Epidemiology. Sixth. New York: Oxford. doi: 10.1093/ije/15.2.277.
�2. Lencucha, R. and Thow, A. M. (2019) ‘How neoliberalism is shaping the supply of unhealthy commodities and what this means for NCD prevention’,International Journal of Health Policy and Management, 8(9), pp. 514–520. doi: 10.15171/ijhpm.2019.56.
�3. Levy, N. (2018) ‘Taking responsibility for health in an epistemically polluted environment’, Theoretical Medicine and Bioethics. Springer Netherlands, 39(2),pp. 123–141. doi: 10.1007/s11017-018-9444-1.
�4. Lupton, D. (2015) ‘The pedagogy of disgust: the ethical, moral and political implications of using disgust in public health campaigns’, Critical PublicHealth, 25(1), pp. 4–14. doi: 10.1080/09581596.2014.885115.
�5. Macintyre, S., Ellaway, A. and Cummins, S. (2002) ‘Place effects on health: How can we conceptualise, operationalise and measure them?’, Social Scienceand Medicine, 55(1), pp. 125–139. doi: 10.1016/S0277-9536(01)00214-3.
��. Madra, Y. M. and Adaman, F. (2014) ‘Neoliberal reason and its forms: De-politicisation through economisation’, Antipode, 46(3), pp. 691–716. doi:10.1111/anti.12065.
�7. van Der Maesen, L. J. G. and Nijhuis, H. G. J. (2000) ‘Continuing the debate on the philosophy of modern public health: Social quality as a point ofreference’, Journal of Epidemiology and Community Health, 54(2), pp. 134–142. doi: 10.1136/jech.54.2.134.
��. Maffra, A. and C, L. De (2013) ‘Epistemic Communities: Study on the Regulation of the Use of Stem Cells in Brazil’, NET, e-journal of InternationalRelations, 4(1), pp. 73–83.
�9. Mahat, A. et al. (2013) ‘Assessment of graduate public health education in Nepal and perceived needs of faculty and students’, Human Resources forHealth, 11(1), pp. 1–12. doi: 10.1186/1478-4491-11-16.
90. Marley, S. C. and Levin, J. R. (2011) ‘When Are Prescriptive Statements in Educational Research Justi�ed?’, Educational Psychology Review, 23(2), pp.197–206. doi: 10.1007/s10648-011-9154-y.
91. Matusitz, J. and Breen, G. M. (2007) ‘Telemedicine: Its effects on health communication’, Health Communication, 21(1), pp. 73–83. doi:10.1080/10410230701283439.
92. Mcdowell, B. (1994) ‘An Examination of the Ecosystems Perspective in Consideration of New Theories in Biology and Thermodynamics’, The Journal ofSociology & Social Welfare, 21(2), p. 23.
93. McGuire, W. L. (2005) ‘Beyond EBM: New directions for evidence-based public health’, Perspectives in Biology and Medicine, pp. 557–569. doi:10.1353/pbm.2005.0081.
94. McPherson, K. (1998) ‘Wider “causal thinking in the health sciences”’, Journal of Epidemiology and Community Health, 52(10), pp. 612–613. doi:10.1136/jech.52.10.612.
95. Mendenhall, R. C. et al. (1974) Study research design, The American Journal of Cardiology. doi: 10.1016/0002-9149(74)90005-8.
9�. Michael, M. (1998) ‘Between citizen and consumer: Multiplying the meanings of the “public understanding of science”’, Public Understanding of Science,7(4), pp. 313–327. doi: 10.1088/0963-6625/7/4/004.
97. Mingers, J. (2003) ‘A classi�cation of the philosophical assumptions of management science methods’, Journal of the Operational Research Society,54(6), pp. 559–570. doi: 10.1057/palgrave.jors.2601436.
9�. Monaghan, L. F. (2013) ‘Extending the obesity debate, repudiating misrecognition: Politicising fatness and health (practice)’, Social Theory and Health,11(1), pp. 81–105. doi: 10.1057/sth.2012.10.
99. Monzó, L. D. and Hoo, S. S. (2014) ‘Translating the academy: Learning the racialized languages of academia’, Journal of Diversity in Higher Education,7(3), pp. 147–165. doi: 10.1037/a0037400.
100. Murphy, E. et al. (1998) ‘Qualitative research methods in health technology assessment: A review of the literature’, Health Technology Assessment, 2(16).doi: 10.3310/hta2160.
101. Murray, S. J., Holmes, D. and Rail, G. (2008) ‘On the constitution and status of “evidence” in the health sciences’, Journal of Research in Nursing, 13(4), pp.272–280. doi: 10.1177/1744987108093529.
102. Nadav, D. and Dani, F. (2006) ‘Reconstructing data: evidence-based medicine and evidence-based public health in context.’, Dynamis (Granada, Spain), 26,pp. 287–306. doi: 10.4321/114240.
103. Nijhuis, H. G. and van der Maesen, L. J. (1994) ‘The philosophical foundations of public health: an invitation to debate.’, Journal of epidemiology andcommunity health, 48(1), pp. 1–3. doi: 10.1136/jech.48.1.1-a.
104. Nik-Khah, E. and Van Horn, R. (2016) ‘The ascendancy of Chicago neoliberalism’, The Handbook of Neoliberalism, (May), pp. 27–38. doi:10.4324/9781315730660.ch2.
105. Nilsson, T. (2009) Inequality , Globalization and Health. Lund University.
10�. Nissen, H.-E. (1985) ‘Acquiring Knowledge of Information Systems: Research in a Methodological Quagmire’, Research Methods in Information Systems,pp. 39–51.
107. Noonan, J. (2018) Dissident Knowledge in Higher Education, Canadian Journal of Education. University of Regina Press.
10�. Novak, T. (1995) Rethinking poverty, Critical Social Policy. doi: 10.1177/026101839501504404.

Page 17/20
109. O, S. and A, I. (2010) A Conceptual Framework for Action on the Social Determinants of Health, Social Determinants of Health Discussion Paper 2 (Policyand Practice). Available at: http://apps.who.int/iris/bitstream/10665/44489/1/9789241500852_eng.pdf?ua=1&ua=1.
110. Odysseos, L. (2010) ‘Human Rights, Liberal Ontogenesis and Freedom: Producing a Subject for Neoliberalism?’, Millennium - Journal of InternationalStudies, 38(3), pp. 747–772. doi: 10.1177/0305829810364876.
111. Ojha, H. R. et al. (2016) ‘Policy without politics: technocratic control of climate change adaptation policy making in Nepal’, Climate Policy, 16(4), pp. 415–433. doi: 10.1080/14693062.2014.1003775.
112. Olssen, M. and Peters, M. A. (2005) ‘Neoliberalism, higher education and the knowledge economy: From the free market to knowledge capitalism’, Journalof Education Policy, 20(3), pp. 313–345. doi: 10.1080/02680930500108718.
113. Onoruoiza, S. I. et al. (2015) ‘Using Health Beliefs Model as an Intervention to Non Compliance with Hypertension Information among HypertensivePatient’, International Organization of Scienti�c Research Journal Of Humanities And Social Science, 20(9), pp. 11–16. doi: 10.9790/0837-20951116.
114. Parsitau, D. (2008) ‘The Impact of Structural Adjustment Programmes (SAPs) on Women’s Health in Kenya’, Governing Health Systems in Africa, (June),pp. 191–200.
115. Pearce, N. (1996) ‘Traditional epidemiology, modern epidemiology, and public health’, American Journal of Public Health, 86(5), pp. 678–683. doi:10.2105/AJPH.86.5.678.
11�. Peet, R., Robbins, W. P. and Watts, T. M. (2010) ‘Global political ecology’, Global Political Ecology, 9780203842, pp. 1–444. doi: 10.4324/9780203842249.
117. Petersen, E. B. and Davies, B. (2010) ‘In/Difference in the neoliberalised university’, Learning and Teaching, 3(2), pp. 92–109. doi:10.3167/latiss.2010.030206.
11�. Pherali, T. and John, L. (2011) A Political Economy Analysis of Education in, Governance An International Journal Of Policy And Administration.
119. Phillips, T., McMichael, C. and O’Keefe, M. (2018) ‘“We invited the disease to come to us”: neoliberal public health discourse and local understanding ofnon-communicable disease causation in Fiji’, Critical Public Health. Taylor & Francis, 28(5), pp. 560–572. doi: 10.1080/09581596.2017.1329521.
120. Pinto, M. F. (2017) ‘To know or better not to: Agnotology and the social construction of ignorance in commercially driven research’, Science andTechnology Studies, pp. 53–72. doi: 10.23987/sts.61030.
121. Porter, D. (2005a) Health, civilization and the state: A history of public health from ancient to modern times, Health, Civilization and the State: A History ofPublic Health from Ancient to Modern Times. London: Routledge. doi: 10.4324/9780203980576.
122. Porter, D. (2005b) Health, civilization and the state: A history of public health from ancient to modern times, Health, Civilization and the State: A History ofPublic Health from Ancient to Modern Times. Routledge Taylor & Francis Group. doi: 10.4324/9780203980576.
123. Prozorov, S. and Rentea, S. (2016) The Routledge handbook of biopolitics, The Routledge Handbook of Biopolitics. doi: 10.4324/9781315612751.
124. Rai, S. K. et al. (2001) ‘The health system in Nepal - An introduction’, Environmental Health and Preventive Medicine, 6(1), pp. 1–8. doi:10.1265/ehpm.2001.1.
125. Rentmeester, C. A. and Dasgupta, R. (2012) ‘Good epidemiology, good ethics: empirical and ethical dimensions of global public health.’, Indian journal ofmedical ethics, 9(4), pp. 235–241. doi: 10.20529/ijme.2012.081.
12�. Rich, E., Monaghan, L. F. and Aphramor, L. (2010) ‘Debating obesity: Critical perspectives’, in Debating Obesity: Critical Perspectives. Palgrave Macmillan,pp. 1–270. doi: 10.1057/9780230304239.
127. Richardson, E. T. (2019) ‘On the coloniality of global public health’, Medicine Anthropology Theory, 6(4), pp. 101–118. doi: 10.17157/mat.6.4.761.
12�. Rillo, A. (2018) ‘Methodological Horizon for Understanding the Health-disease Process’, Asian Journal of Medicine and Health, 9(3), pp. 1–21. doi:10.9734/ajmah/2017/38430.
129. Roberts, P. and Peters, M. A. (2019) ‘Neoliberalism, Higher Education and Research’, in Neoliberalism, Higher Education and Research. Sense, pp. 1–8. doi:10.1163/9789087906306_002.
130. Rose, N. (2001) ‘The politics of life itself’, Theory, Culture and Society, pp. 1–30. doi: 10.1177/02632760122052020.
131. Rosenberg, C. E. (2003) ‘What Is Disease? In Memory of Owsei Temkin’, Bulletin of the History of Medicine, 77(3), pp. 491-505+763. doi:10.1353/bhm.2003.0139.
132. Rossi, U. (2013) ‘On Life as a Fictitious Commodity: Cities and the Biopolitics of Late Neoliberalism’, International Journal of Urban and RegionalResearch, 37(3), pp. 1067–1074. doi: 10.1111/1468-2427.12063.
133. Rowe, M. and Oltmann, C. (2016) ‘Randomised controlled trials in educational research: Ontological and epistemological limitations’, African Journal ofHealth Professions Education, 8(1), p. 6. doi: 10.7196/ajhpe.2016.v8i1.683.
134. Rychetnik, L. et al. (2004) ‘A glossary for evidence based public health’, Journal of Epidemiology and Community Health, 58(7), pp. 538–545. doi:10.1136/jech.2003.011585.
135. Sanders, C. L. and McKay, K. H. (2013) ‘the Search for “Strong Medicine”: Pathways To Healthcare Development in Remote Nepal Using Gis’, Technology &Innovation, 15(2), pp. 109–124. doi: 10.3727/194982413x13650843068799.
13�. Schillmeier, M. (2006) ‘Othering blindness - On modern epistemological politics’, Disability and Society, pp. 471–484. doi: 10.1080/09687590600785910.
137. Schulz, K. and Siriwardane, R. (2015) Depoliticised and technocratic? Normativity and the politics of transformative adaptation, Earth SystemsGovernance Working Paper No.33. 33.
13�. Seedhouse, D. (2004) Health Promotion: Philosophy, Prejudice and Practice-Second Edition. second, John and Wiley & Sons, Ltd. second. John Wiley &Sons, Inc. Available at: https://books.google.ie/books?

Page 18/20
hl=en&lr=&id=53Oye1hbovsC&oi=fnd&pg=PR7&dq=Health+Promotion+Philosophy+Prejudice+and+Pract&ots=5Q4Y0ITjQq&sig=j4PZnCuOZ_8KXfzNvLGYPromotion Philosophy Prejudice and Pract&f=false.
139. Sell, S. K. and Williams, O. D. (2020) ‘Health under capitalism: a global political economy of structural pathogenesis’, Review of International PoliticalEconomy. Routledge, 27(1), pp. 1–25. doi: 10.1080/09692290.2019.1659842.
140. Sen, A. (2003) ‘The local and the global’, pp. 1–9. Available at: http://www.provincia.torino.gov.it/sviluppolocale/�le-storage/download/pdf/torinosen.pdf.
141. Sharma, G. (2010) ‘Bodhi : An Interdisciplinary Journal 4 ( 1 ) Criticalizing the pedagogy of English studies : A Nepalese perspective’, 4(1), pp. 111–135.
142. Sharma, J. R., Khatri, R. and Harper, I. (2016) ‘Understanding Health Research Ethics in Nepal’, Developing World Bioethics, 16(3), pp. 140–147. doi:10.1111/dewb.12109.
143. Sławecki, B. (2017) ‘Paradigms in qualitative research’, in Qualitative Methodologies in Organization Studies. SAGE, pp. 7–26. doi: 10.1007/978-3-319-65217-7_2.
144. Smith, J. (2019) ‘Commentary Towards Critical Analysis of the Political Determinants of Health’, International Journal of Health Policy ane Management,(November), pp. 1–3. doi: 10.15171/ijhpm.2019.102.
145. Sparke, M. (2020) ‘Neoliberal regime change and the remaking of global health: from rollback disinvestment to rollout reinvestment andreterritorialization’, Review of International Political Economy, 27(1), pp. 48–74. doi: 10.1080/09692290.2019.1624382.
14�. Staddon, J. E. R. (2004) ‘Scienti�c imperialism and behaviorist epistemology’, Behavior and Philosophy, 32(1), pp. 231–242. doi: 10.2307/27759479.
147. Stahl, B. C. (2007) ‘Positivism or Non-Positivism — Tertium Non Datur’, in Ontologies, pp. 115–142. doi: 10.1007/978-0-387-37022-4_5.
14�. Steinberg, D. L. (2002) ‘“Recombinant” bodies Narrative, metaphor and the gene’, in J.Williams, S., Gabe, J., and Calnan, M. (eds) Health, Medicine andSociety Key theories, future agendas. Routledge Taylor & Francis Group, p. 366.
149. Subedi Sharma Madhusudan (2016) ‘Making Health a Public Agenda in Nepal’, Sass, (April), pp. 73–96.
150. Subramaniam, M. (2014) ‘Neoliberalism and water rights: The case of India’, Current Sociology, 62(3), pp. 393–411. doi: 10.1177/0011392114523973.
151. Sugden, F. (2009) ‘Neo-liberalism, markets and class structures on the Nepali lowlands: The political economy of agrarian change’, Geoforum. Elsevier Ltd,40(4), pp. 634–644. doi: 10.1016/j.geoforum.2009.03.010.
152. Syme, S. L. and Ritterman, M. L. (2009) ‘The importance of community development for health and well-being’, Community Development InvestmentReview, 5(3), pp. 1–13. Available at: https://www.frbsf.org/community-development/�les/syme_ritterman.pdf.
153. Tavakol, M. and Aa, Z. (2004) ‘Medical Research Paradigms: Positivistic Inquiry Paradigm versus Naturalistic Inquiry Paradigm’, Journal of MedicalEducation, 5(2), pp. 75–80. doi: 10.22037/jme.v5i2.804.
154. Van Teijlingen, E. et al. (2015) ‘Learning from health care in other countries: the prospect of comparative research’, Health Prospect, 14(1), pp. 8–12. doi:10.3126/hprospect.v14i1.13036.
155. Turyahikayo, E. (2014) ‘Resolving the qualitative-quantitative debate in healthcare research’, Medical Practice and Reviews, 5(1), pp. 6–15. doi:10.5897/mpr.2013.0107.
15�. Unger, J.-P. et al. (2011) ‘The production of critical theories in Health Systems Research and Education. An epistemological approach to emancipatingpublic research and education from private interests’, Health, Culture and Society, 1(1), pp. 1–28. doi: 10.5195/hcs.2011.50.
157. Victora, C. G., Habicht, J. P. and Bryce, J. (2004) ‘Evidence-Based Public Health: Moving Beyond Randomized Trials’, American Journal of Public Health,94(3), pp. 400–405. doi: 10.2105/AJPH.94.3.400.
15�. Voros, J. (2008) ‘Integral Futures: An approach to futures inquiry’, Futures, 40(2), pp. 190–201. doi: 10.1016/j.futures.2007.11.010.
159. Walt, G. et al. (2008) ‘“Doing” health policy analysis: Methodological and conceptual re�ections and challenges’, Health Policy and Planning, 23(5), pp.308–317. doi: 10.1093/heapol/czn024.
1�0. Weed, D. L. (1999) ‘Towards a philosophy of public health’, Journal of Epidemiology and Community Health, pp. 99–104. doi: 10.1136/jech.53.2.99.
1�1. Wemrell, M. et al. (2016) ‘Contemporary Epidemiology: A Review of Critical Discussions Within the Discipline and A Call for Further Dialogue with SocialTheory’, Sociology Compass, 10(2), pp. 153–171. doi: 10.1111/soc4.12345.
1�2. Williams, S. J., Gabe, J. and Davis, P. (2008) ‘The sociology of pharmaceuticals: Progress and prospects’, Sociology of Health and Illness, 30(6), pp. 813–824. doi: 10.1111/j.1467-9566.2008.01123.x.
1�3. Wong, S. E. (2006) ‘Behavior Analysis of Psychotic Disorders: Scienti�c Dead End or Casualty of the Mental Health Political Economy?’, Behavior andSocial Issues, 15(2), pp. 152–177. doi: 10.5210/bsi.v15i2.365.
1�4. World Health Organization (2006) WHO Country Cooperation Strategy Uganda, World Health Organization.
1�5. Yach, D., Beaglehole, R. and Hawkes, C. (2005) Globalisation and Noncommunicable Diseases, Promoting Health. doi: 10.1007/978-0-230-21050-9_6.
1��. Yadavendu, V. K. (2013) Shifting paradigms in public health: From holism to individualism, Shifting Paradigms in Public Health: From Holism toIndividualism. Springer. doi: 10.1007/978-81-322-1644-5.
Figures

Page 19/20
Figure 1
Research Process
Figure 2
Epistemic Well
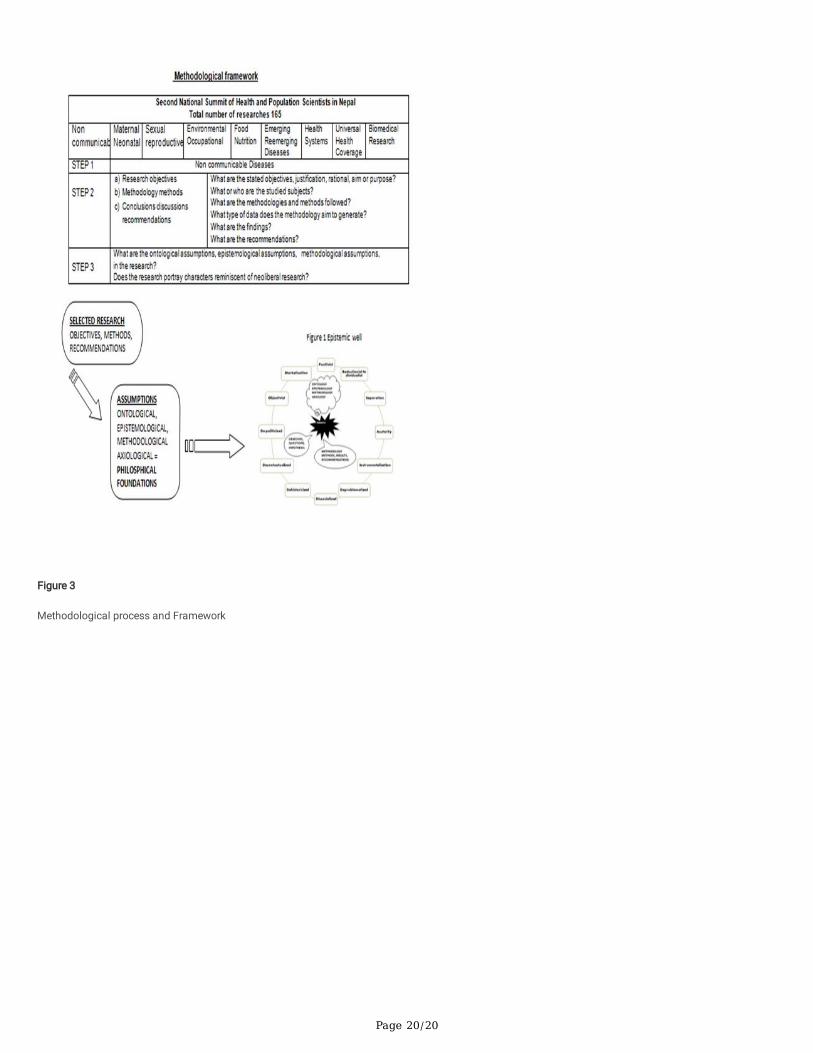
Page 20/20
Figure 3
Methodological process and Framework


















