Laura Mucci, Pharm.D. Candidate Mercer University 2012 Preceptor: Dr. Rahimi February 2012.
26
Laura Mucci, Pharm.D. Candidate Mercer University 2012 Preceptor: Dr. Rahimi February 2012
-
Upload
howard-tate -
Category
Documents
-
view
217 -
download
2
Transcript of Laura Mucci, Pharm.D. Candidate Mercer University 2012 Preceptor: Dr. Rahimi February 2012.
Laura Mucci, Pharm.D. Candidate Mercer University 2012Preceptor: Dr. RahimiFebruary 2012
Limited data available for use of statins for primary prevention of cardiovascular disease in older adults
The association between elevated cholesterol and CV disease weakens with age Framingham coronary heart disease risk score
for patients with total cholesterol ≥ 250 mg/dL Age 40 years: men 6 points, women 8 points Age 75 years: men 1 point, women 2 points
Age is the dominant risk factor of first cardiovascular event in people without diabetes Framingham risk score for persons over
age 75▪ Men: 13▪ Women: 16

Secondary analysis of the JUPITER trial Funded by AstraZeneca, maker of Crestor Randomized, double-blind, placebo controlled
trial conducted at 1315 sites in 26 countries 17,802 total participants Analysis focused on participants aged 70
years or older, which was 5695 participants (32% of total)
Trial took place between March 2003 – August 2008
Men age 50 years or older Women age 60 years or older No prior history of cardiovascular
disease or diabetes LDL cholesterol level < 130 mg/dL High-sensitivity C-reactive protein level
≥ 2.0 mg/L 4-week placebo run-in phase to test
adherence
LDL ≥ 130 mg/dL C-reactive protein level < 2.0 mg/L Patients with diabetes, prior history of
CV disease, hypothyroid, liver disease, triglycerides > 500 mg/dL
Lipid lowering therapy within 6 weeks of randomization
Current use of hormone replacement therapy
Cancer within last 5 years Poor compliance
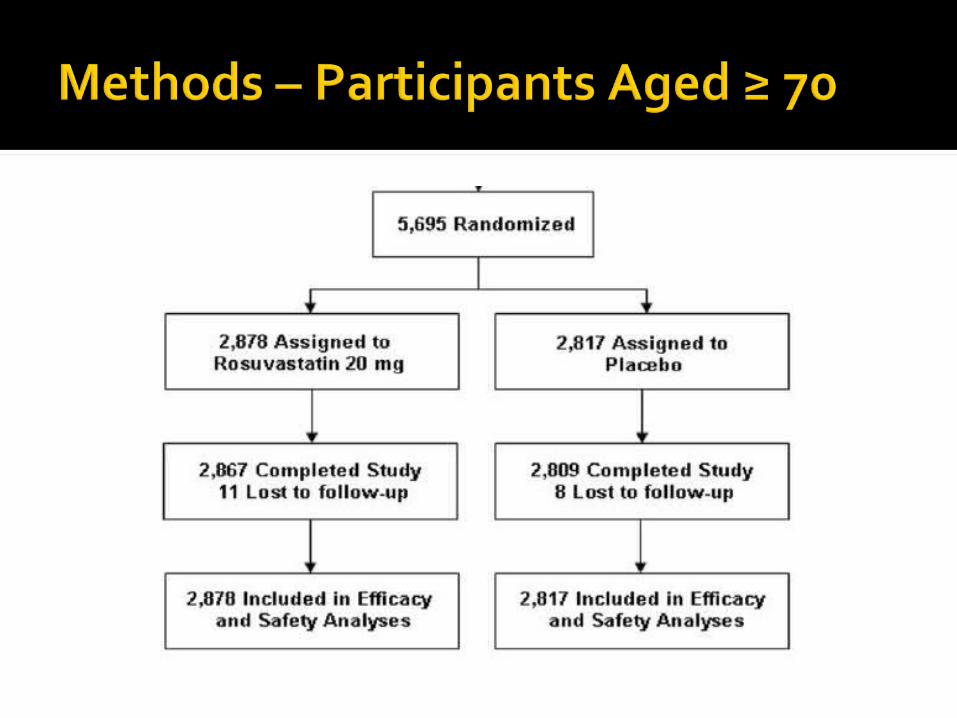
Intervention: participants randomized to 2 groups in a ratio of 1:1 Crestor (rosuvastatin) 20mg daily Placebo
Follow-up visits at 13 weeks, then 6, 12, 18, 24, 30, 36, 42, 48, 54, and 60 months
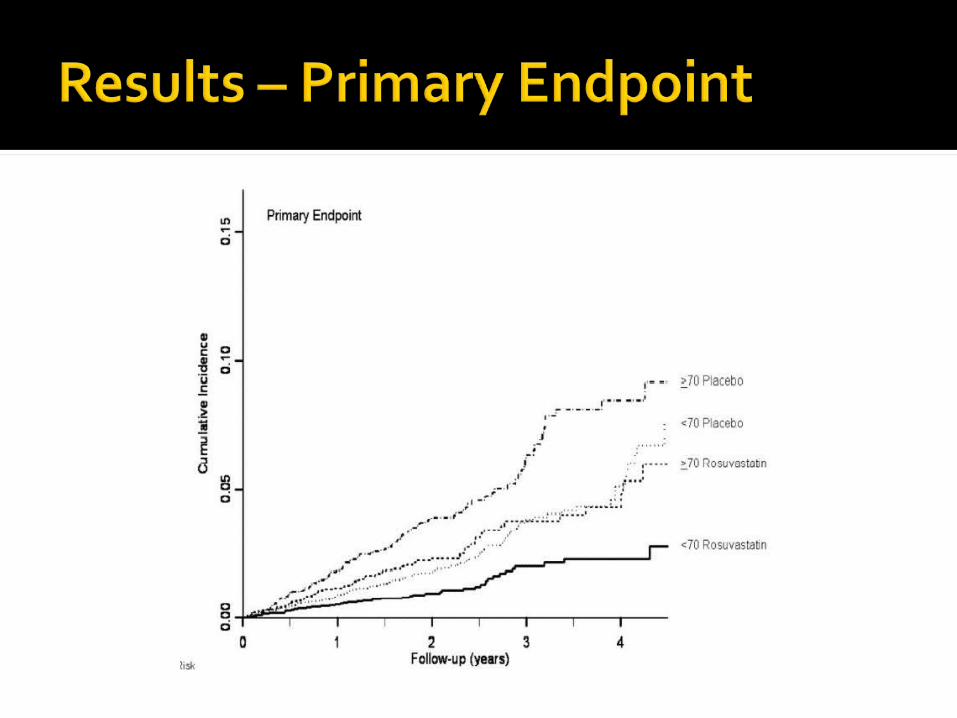
Primary end-point: occurrence of first cardiovascular event Myocardial infarction (non-fatal) Stroke (non-fatal) Arterial revascularization Hospitalization for unstable angina Death from cardiovascular causes
Secondary end-points Death from any cause Venous thromboembolism Incident diabetes
Safety end-points Incident diabetes Adverse events
Endpoints analyzed with the intention-to-treat principle
Cox proportional hazards model used to estimate treatment effects by age group
Likelihood ratio test of age groups by treatment interaction evaluated possible heterogeneity in the treatment effect by age
Number needed to treat to prevent 1 event based on Kaplan-Meier estimates of cumulative risk at 4 years
Median LDL cholesterol in the rosuvastatin group (54 mg/dL) was half that of the placebo group
Median C-reactive protein in the rosuvastatin group (2.3 mg/L) was 36% lower than the placebo group
For all ages, rosuvastatin was associated with a 44% reduction in the primary endpoint (95% CI 0.46-0.69, P<0.001)
32% of trial participants were aged 70 or older
They comprised 49% (194 of 393) of the total primary cardiovascular endpoints
Absolute reduction in the incidence of primary endpoints was 0.77 events per 100 person-years

Number of adults ≥ 70 years needed to treat for 4 years to prevent 1 primary end point was 24 (95% CI: 15-57)
Number of adults < 70 years needed to treat for 4 years to prevent 1 primary end point was 36 ( 95% CI: 23-77)
To prevent secondary endpoints: NNT was 17 in those aged ≥ 70 and 27 in those < 70 years (95% CI: 12-33, 17-57, respectively)
Clear treatment benefit was seen in older adults with hypertension and those with a Framingham risk > 10%
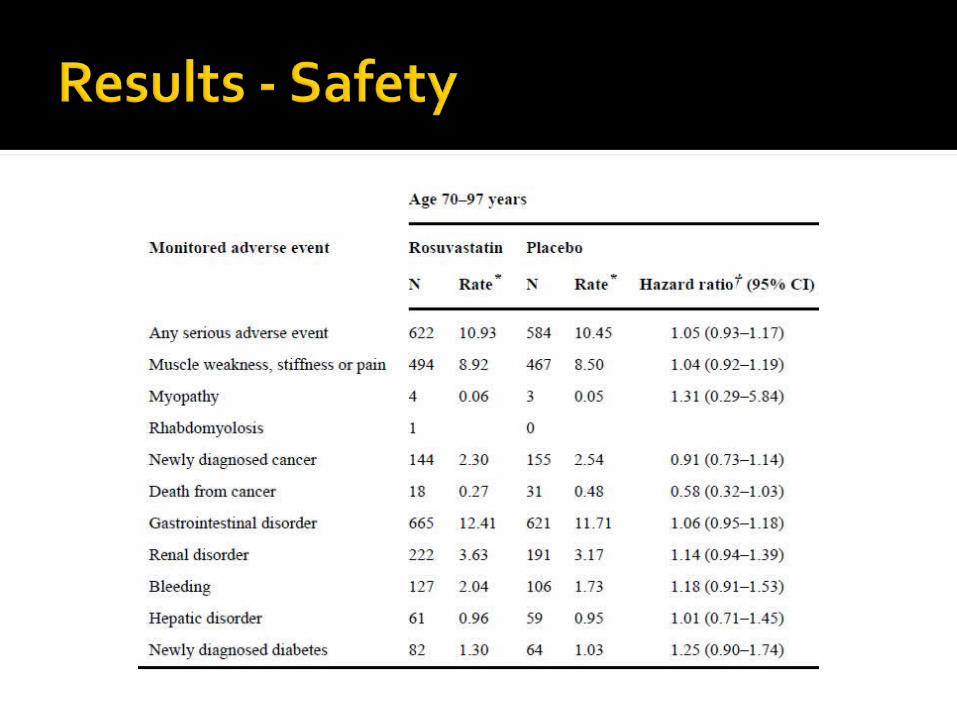
Older participants assigned to placebo had higher rates of serious adverse events
Older participants in the rosuvastatin group had higher incidences of muscle weakness, stiffness or pain, renal disorder, bleeding, GI disorder, hepatic disorder, and incident diabetes, but none were statistically significant
Rosuvastatin substantially reduced the incidence of major cardiovascular events
Benefits of rosuvastatin emerged shortly after initiation in older adults
Treatment effects in older adults were consistent with effects in younger adults, but absolute event rates and treatment benefits were greater in older adults
JUPITER trial differed from previous studies of statins Enrolled older population Included stroke in primary endpoints Participants had normal LDL levels Participants had higher C-reactive protein
levels Identified a population at risk (high CRP)
for stroke and heart disease who benefit from statin use despite low LDL levels
JUPITER also shows a need to include stroke prevention in evaluations of cost effectiveness Stroke causes a high personal and financial
impact and an increased percentage of total cardiovascular events with age
Practitioners often see comorbidities and proximity to death as barriers to primary prevention treatment in the older population
JUPITER shows that benefit emerges quickly and absolute risk is high in older adults
Fewer older patients need to be treated to prevent one event
Rosuvastatin was associated with a significant risk reduction in first CV event
Absolute treatment benefit is greater in older adults than younger ones
Large, randomized, blinded, multi-country trial
Average age of participants was 66 years
Results can be applied to our patients
Results were extrapolated from study, more research may be necessary in this population
Funded by Astra-Zeneca, only have evidence for Crestor

Glynn RJ, Koenig W, Nordestgaard BG, et al. Rosuvastatin for primary prevention in older individuals with high C-reactive protein and low LDL levels: exploratory analysis of a randomized trial. Ann Intern Med. 2010;152:488-496.