
Laboratory Diagnosis of HSV Infection Peter Leone, MD Associate Professor of Medicine University of...
30
Laboratory Diagnosis of HSV Infection Peter Leone, MD Associate Professor of Medicine University of North Carolina
-
Upload
jude-voshall -
Category
Documents
-
view
222 -
download
0
Transcript of Laboratory Diagnosis of HSV Infection Peter Leone, MD Associate Professor of Medicine University of...
Laboratory Diagnosis of HSV Infection
Peter Leone, MD
Associate Professor of Medicine
University of North Carolina
Why Diagnose Genital Herpes?
Epidemic Most HSV-2 seropositive persons are
symptomatic Transmission occurs from undiagnosed
persons HSV-2 increases risk of HIV acquisition
and transmission Pregnancy management
Underrecognition by Clinicians and Patients: What Should We Do?
Recognize that prevalence within our practices is higher than anticipated
Appreciate that genital HSV-2 does not discriminate Elevate our “index of suspicion” in all sexually
active patients Provide patient education about signs and symptoms
of genital herpesMany patients with unrecognized disease “become symptomatic” once they receive adequate counseling1,2
1. Lowhagen GB, et al. Acta Derm Venereol 2005;85(3):248-252. 2. Wald A, et al. N Engl J Med 2000;342(12):844-850.
Diagnosing Herpes
…The clinical diagnosis of HSV is no longer considered an adequate method for diagnosis of genital herpes.
Both virologic tests and type-specific serologic tests for HSV should be available in clinical settings that provide care for patients with STDs or those at risk for STDs.
–2002 CDC STD Treatment Guidelines
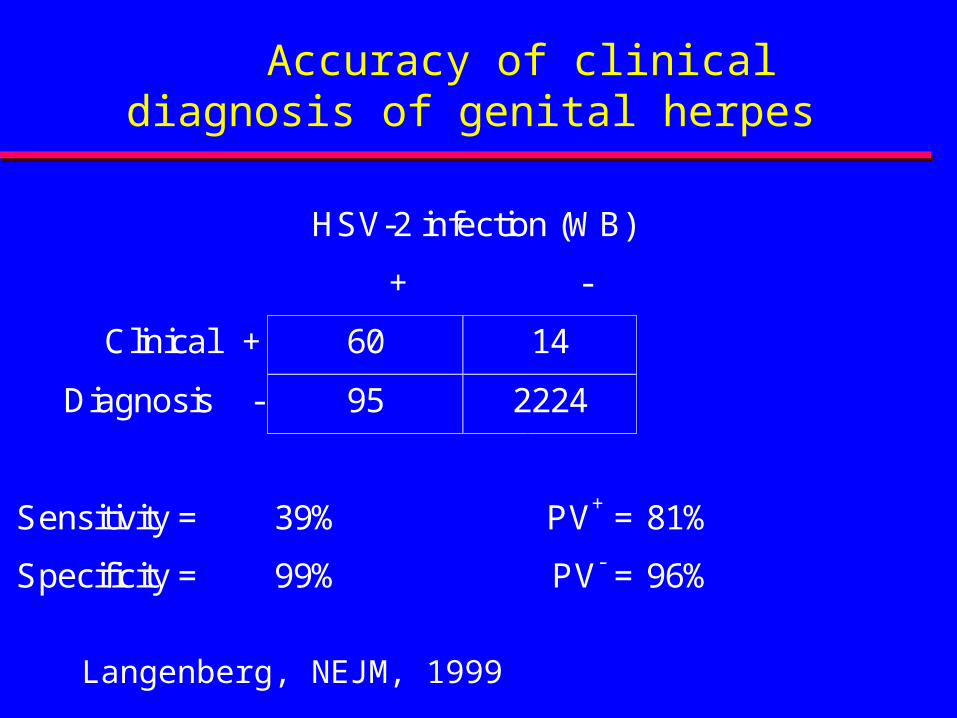
Accuracy of clinical diagnosis of genital herpes
HSV-2 infection (WB)
+ -
Clinical + 60 14
Diagnosis - 95 2224
Sensitivity = 39% PV+ = 81%
Specificity = 99% PV- = 96%
Langenberg, NEJM, 1999
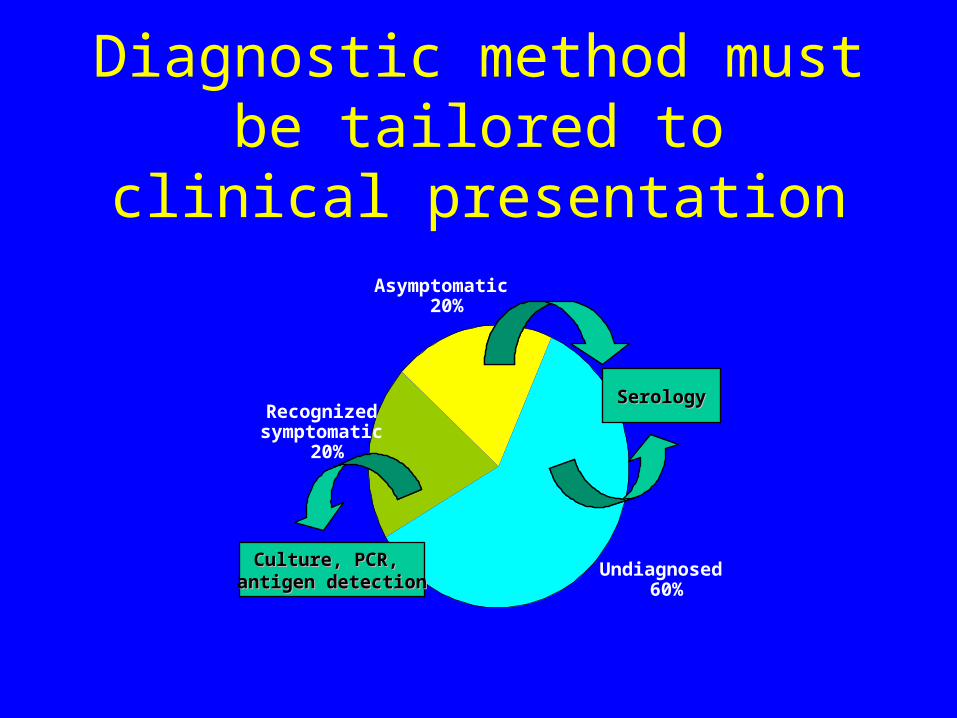
Diagnostic method must be tailored to clinical presentation
Recognized symptomatic
20%
Asymptomatic 20%
Undiagnosed 60%
SerologySerology
Culture, PCR, Culture, PCR, antigen detectionantigen detection
Lesion Evaluation
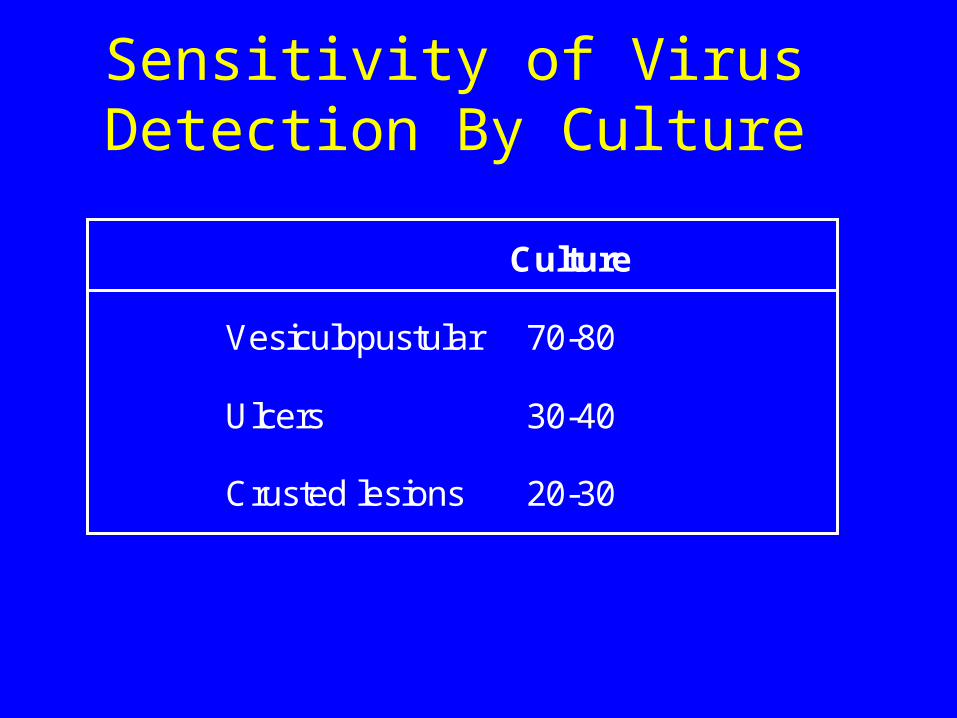
Sensitivity of Virus Detection By Culture
Culture
Vesiculopustular 70-80
Ulcers 30-40
Crusted lesions 20-30
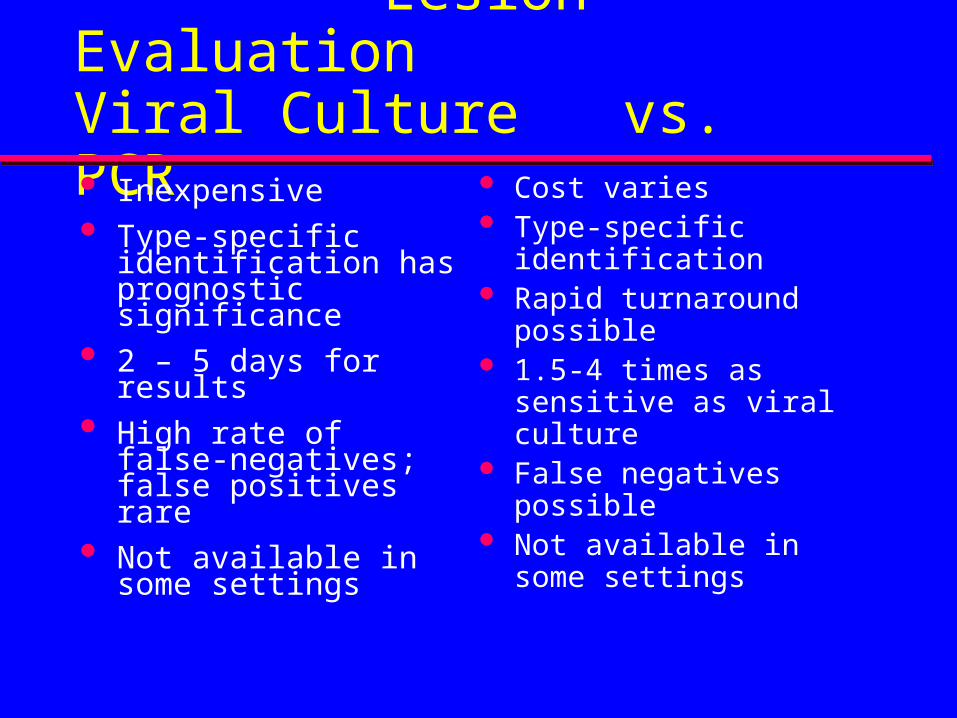
Lesion EvaluationViral Culture vs. PCR Inexpensive Type-specific
identification has prognostic significance
2 – 5 days for results High rate of false-
negatives; false positives rare
Not available in some settings
Cost varies Type-specific
identification Rapid turnaround
possible 1.5-4 times as sensitive
as viral culture False negatives
possible Not available in some
settings
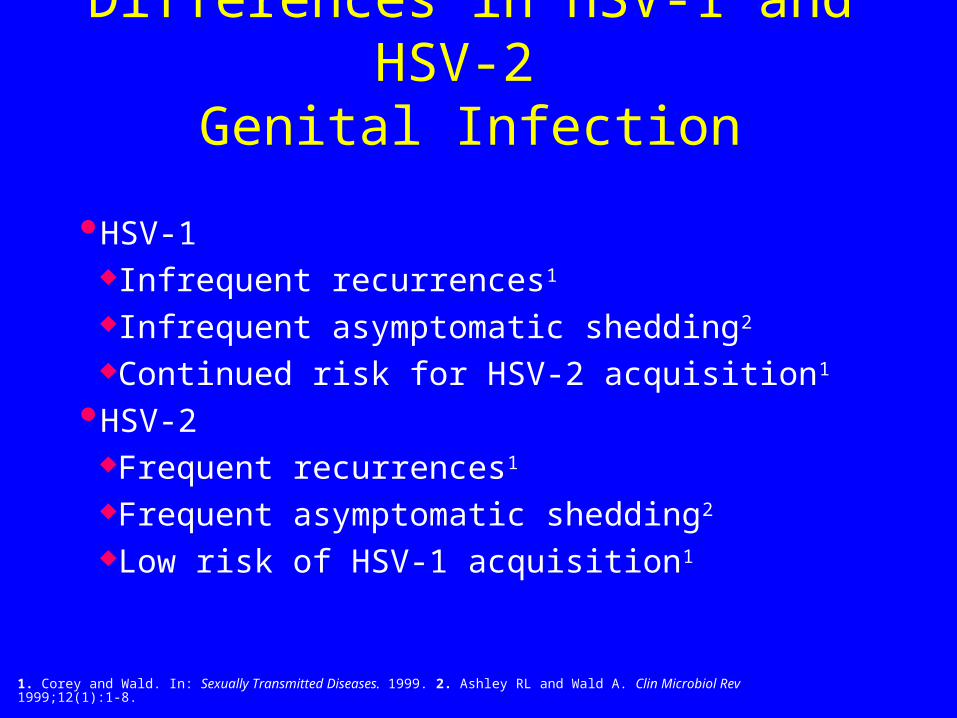
Differences in HSV-1 and HSV-2 Genital Infection
HSV-1Infrequent recurrences1
Infrequent asymptomatic shedding2
Continued risk for HSV-2 acquisition1
HSV-2Frequent recurrences1
Frequent asymptomatic shedding2
Low risk of HSV-1 acquisition1
1. Corey and Wald. In: Sexually Transmitted Diseases. 1999. 2. Ashley RL and Wald A. Clin Microbiol Rev 1999;12(1):1-8.
Serologic Evaluation
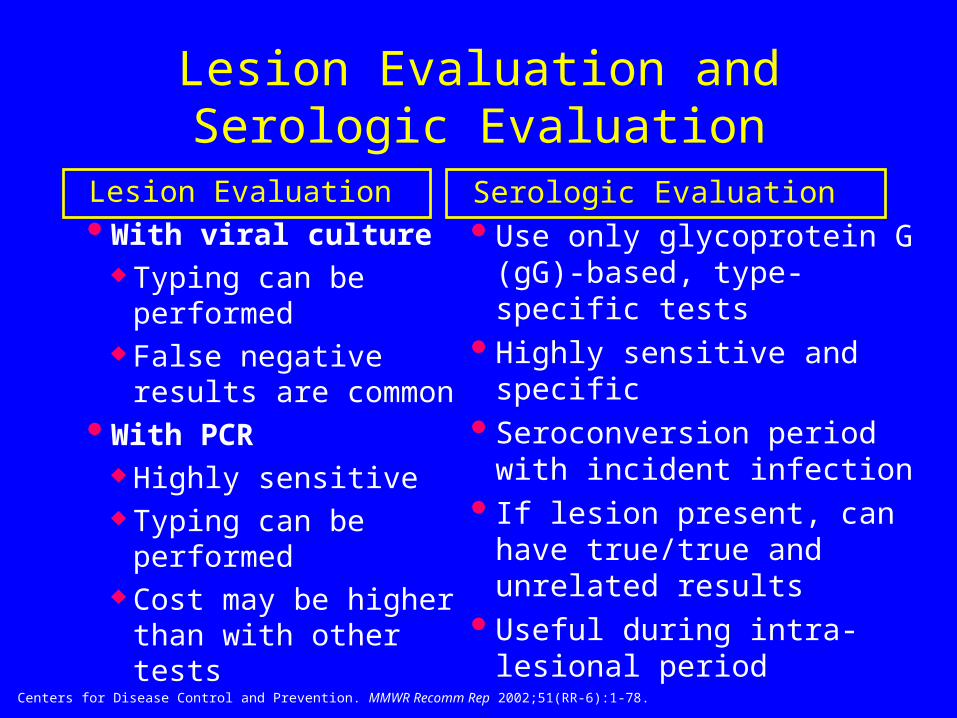
Lesion Evaluation and Serologic Evaluation
Lesion Evaluation With viral culture
Typing can be performed
False negative results are common
With PCR Highly sensitive Typing can be
performed Cost may be higher than
with other tests
Serologic Evaluation Use only glycoprotein G
(gG)-based, type-specific tests
Highly sensitive and specific Seroconversion period with
incident infection If lesion present, can have
true/true and unrelated results
Useful during intra-lesional period
Centers for Disease Control and Prevention. MMWR Recomm Rep 2002;51(RR-6):1-78.
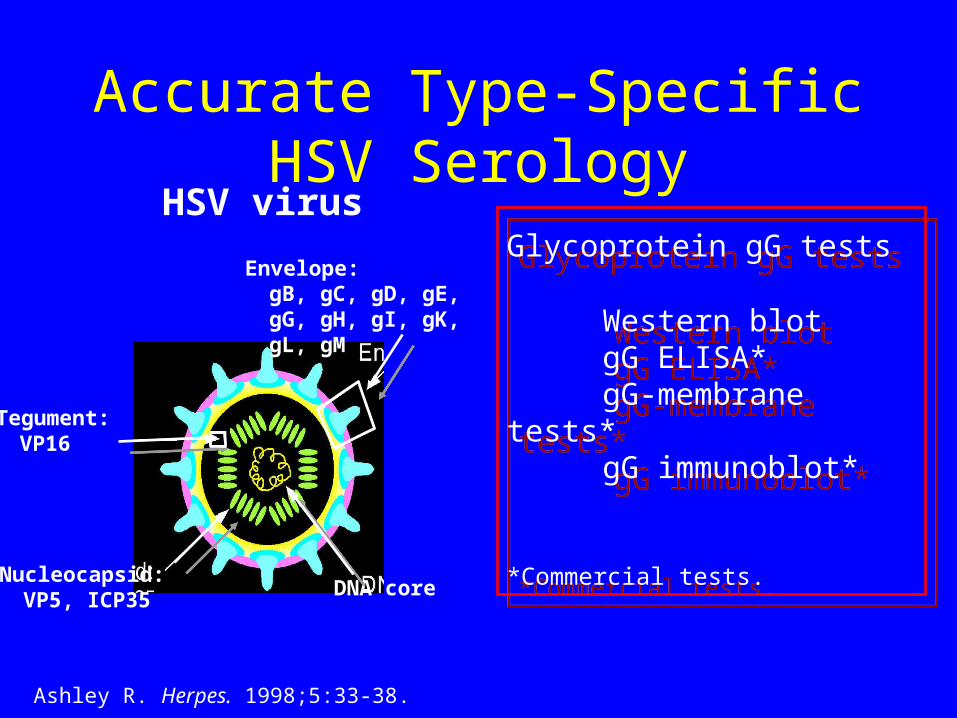
Glycoprotein gG tests
Western blotgG ELISA*gG-membrane tests*gG immunoblot*
*Commercial tests.
Glycoprotein gG tests
Western blotgG ELISA*gG-membrane tests*gG immunoblot*
*Commercial tests.
Envelope:gB, gC, gD, gE,gG, gH, gI, gK,gL, gM
Tegument:VP16
Nucleocapsid:VP5, ICP35
DNA core
HSV virus
Accurate Type-Specific HSV Serology
Ashley R. Herpes. 1998;5:33-38.
Performance and interpretation of serologic tests
What is the Gold Standard? Interpretation of Western Blot is still part
art Discrepant analysis Time to seroconversion
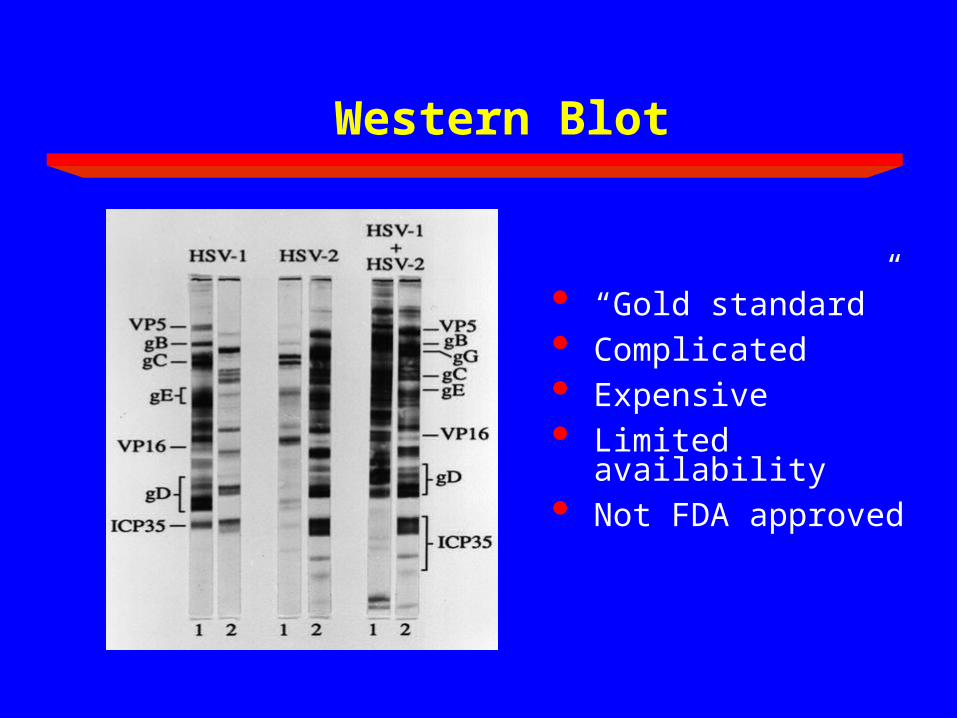
Western Blot
“Gold standard” Complicated Expensive Limited availability Not FDA approved
Discordant Results Between
the ELISA and Western blot.
In pre-selected serum panels, 31 of 96 WB negative sera were HSV-2 positive when tested by an inhibition assay; therefore, using the WB to confirm positive results may overestimate false positive rates in the original ELISA.
Hogrefe et al., IHMF 2005
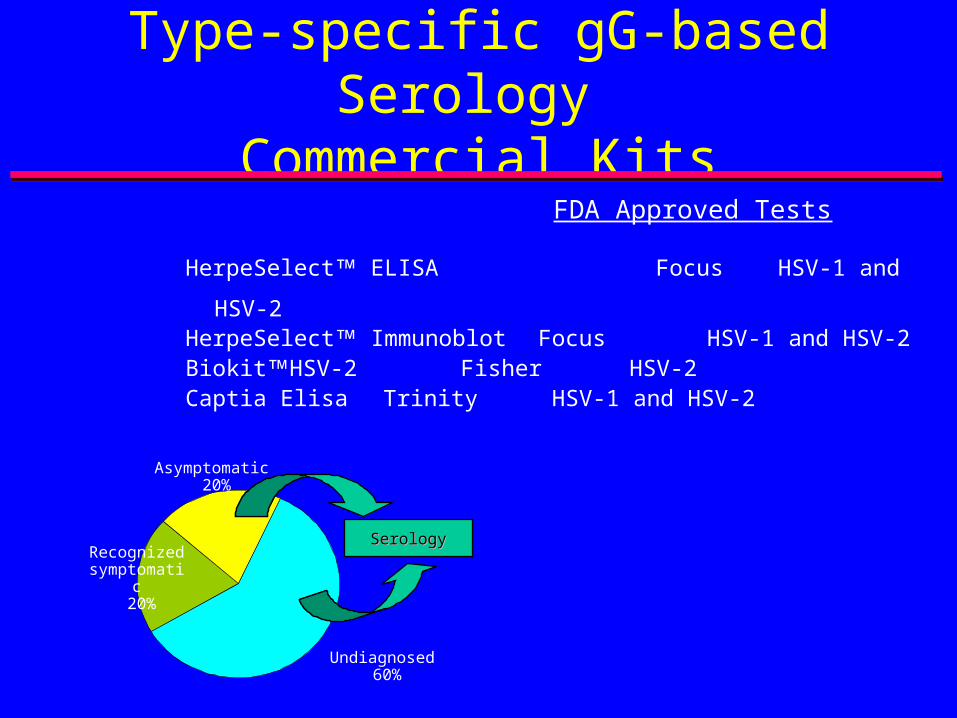
Type-specific gG-based Serology
Commercial Kits FDA Approved Tests
HerpeSelect ELISA Focus HSV-1 and HSV-2HerpeSelect Immunoblot Focus HSV-1 and HSV-2BiokitHSV-2 Fisher HSV-2Captia Elisa Trinity HSV-1 and HSV-2
Recognized symptomatic
20%
Asymptomatic 20%
Undiagnosed 60%
SerologySerology
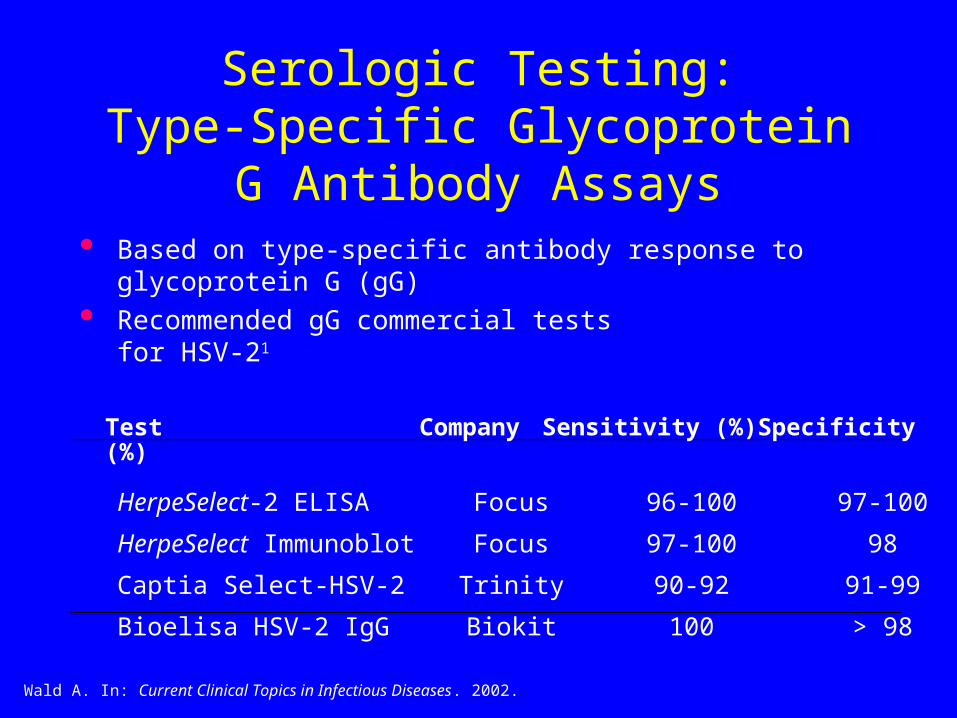
Serologic Testing:Type-Specific Glycoprotein G
Antibody Assays Based on type-specific antibody response to glycoprotein G
(gG) Recommended gG commercial tests
for HSV-21
Test Company Sensitivity (%) Specificity (%)
HerpeSelect-2 ELISA Focus 96-100 97-100
HerpeSelect Immunoblot Focus 97-100 98
Captia Select-HSV-2 Trinity 90-92 91-99
Bioelisa HSV-2 IgG Biokit 100 > 98
Wald A. In: Current Clinical Topics in Infectious Diseases. 2002.
Is IgM Useful in Distinguishing New vs. Recurrent GH Infection?
• No! Do not order IgM antibodies to diagnose new vs.
recurrent GH infection. Often laboratories automatically do IgM test
• Why aren’t IgM tests helpful in determining the recency of
GH infection?
- IgM tests are not type-specific – IgM could be from HSV-1
or HSV-2!
- Each of the many episodes of viral reactivation can
produce new IgM and IgG, making it difficult to interpret
results as to acuity of infection.
•IgM has role in Dx of neonatal HSV
Ashley RL. Herpes 1998;5:33–38.
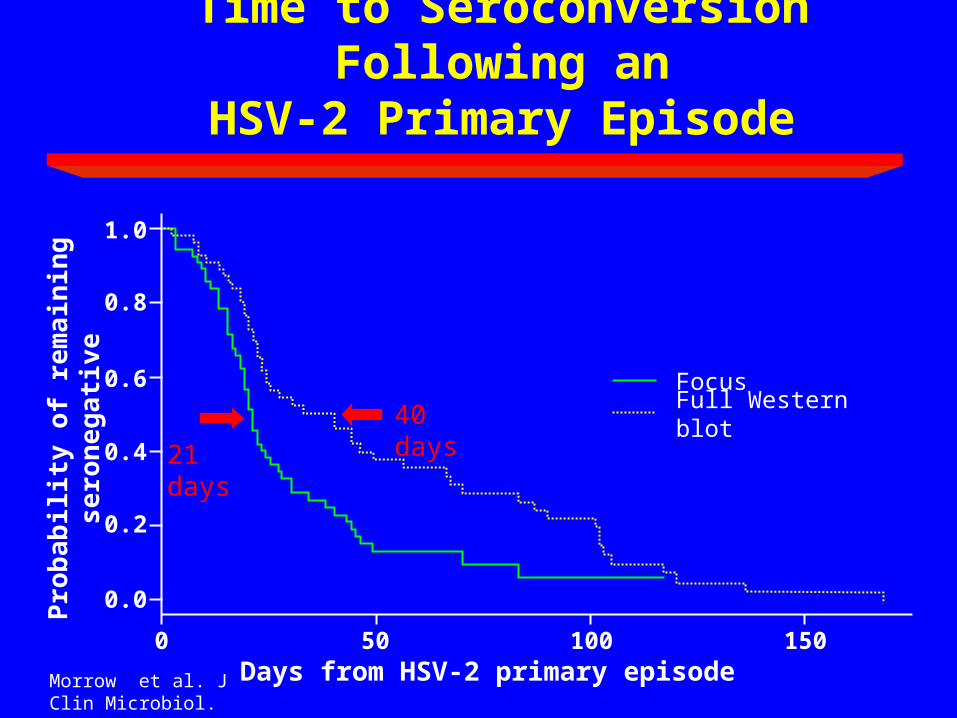
Time to Seroconversion Following anHSV-2 Primary Episode
40 days
21 days
Days from HSV-2 primary episodePro
bab
ility
of
rem
ain
ing
se
ron
eg
ati
ve
Full Western blotFocus
150100500
0.0
0.2
0.4
0.6
0.8
1.0
Morrow et al. J Clin Microbiol. 2003
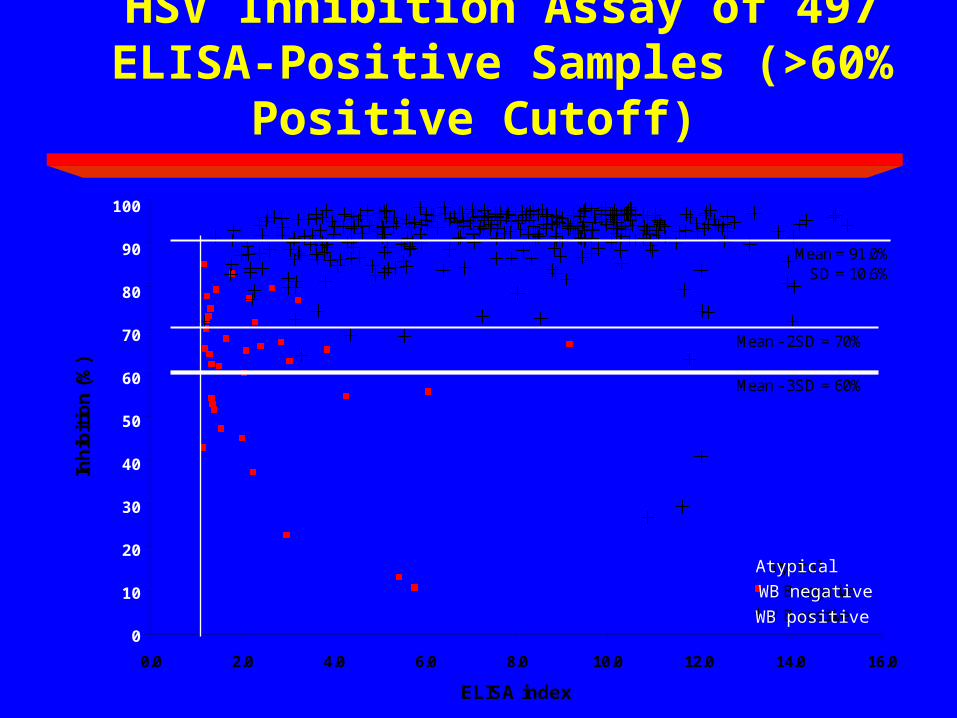
HSV Inhibition Assay of 497 ELISA-Positive Samples (>60% Positive Cutoff)
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0.0 2.0 4.0 6.0 8.0 10.0 12.0 14.0 16.0
ELISA index
Inh
ibit
ion
(%
)
atypical
WB negative
WB positive
Mean = 91.0%SD = 10.6%
Mean - 3SD = 60%
Mean - 2SD = 70%
Atypical
WB negative
WB positive
100
90
80
70
60
50
40
30
20
10
0
Performance of the 2 Generation Focus HerpeSelect HSV-2 IgG ELISA on
Selected Serum Panels
Hogrefe et al., IHMF 2005
The 2 generation HerpeSelect HSV-2 ELISA reduced
the number of false positive results by ~40% when the WB used as the gold standard respectively.
Confirmation of HerpeSelect® HSV-2 ELISA Positive Results (N=313)
Worldwide study: women (33% prevalence)
Positive samples by HerpeSelect HSV-2 ELISA270 (86%) confirmed by WB for HSV-2 43 (14%) not confirmed by WB for HSV-2
Median index of confirmed: 8.1 (1.36-25.5)
Median index of unconfirmed: 2.5 (1.2-14.2)
Majority of unconfirmed are between 1.1 and 2.0
Confirmation of HerpeSelect® HSV-2 ELISA Positive Results
(N=103)Seattle STD clinic: men (13% seroprevalence) Positive samples (106) by HerpeSelect HSV-2
ELISA
80%(80) confirmed by WB for HSV-2
16%(17) not confirmed by WB for HSV-2
Median index of confirmed: 8.0 Median index of unconfirmed: 2.0
Golden et al Sex Transm Dis Dec. 2005
Interpretation of ELISA in Low Prevalence Population
In low-prevalence populations (<10%), should consider selectively using a higher index (2.2 or 3.5) value to define positivity based either on the presence or absence of clinical findings suggestive of genital herpes or clinical risk history.
Confirmation either by WB or by Biokit (increased PPV 80% to ~96%)
Golden et al Sex Transm Dis Dec. 2005
Laeyendecker et al., J Clin Microbiol 2004
Morrow BMC Infectious Diseases 2005
Interpretation of Test Results
In patients with culture-positive or PCR-positive genital lesions You have a confirmed type-specific, site-specific
diagnosis If seronegative for the type identified on culture, assume
new infection In pregnant patients, it is important to distinguish new
infection from established infection IgM-based tests are not reliable for distinguishing new
infection from established infection and should never be used for this purpose
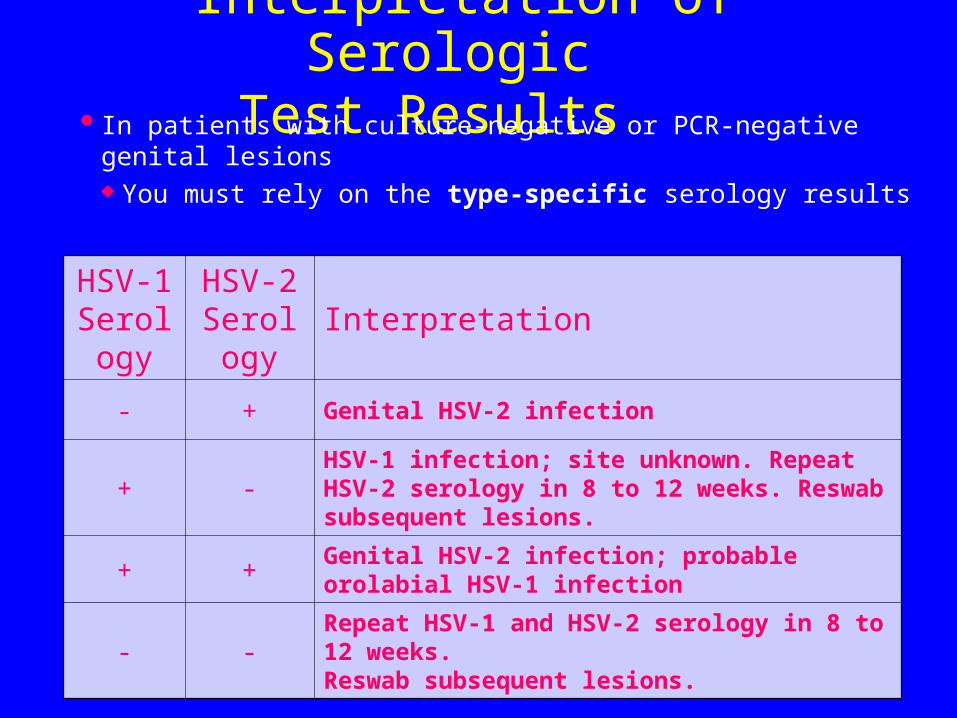
Interpretation of Serologic Test Results
In patients with culture-negative or PCR-negative genital lesions You must rely on the type-specific serology results
HSV-1 Serolo
gy
HSV-2 Serolog
yInterpretation
- + Genital HSV-2 infection
+ -HSV-1 infection; site unknown. Repeat HSV-2 serology in 8 to 12 weeks. Reswab subsequent lesions.
+ +Genital HSV-2 infection; probable orolabial HSV-1 infection
- -Repeat HSV-1 and HSV-2 serology in 8 to 12 weeks. Reswab subsequent lesions.
Undiagnosed Patients: What Should We Do?
Inform patients about the importance of testingReassure patients that if they are diagnosed,
they have many available management options and resources
Offer HSV type-specific testingProvide patient-sensitive and timely follow-up
care after testing is performed
Candidates for Serologic Testing
Patients With recurrent genitourinary symptoms With a culture-negative lesion or clinical diagnosis
only Presenting for STI screening or requesting herpes
testing Diagnosed with an STI With a current or past partner with genital herpes With HIV-infection Who are pregnant? (not in ACOG guidelines)
Centers for Disease Control and Prevention. MMWR Recomm Rep 2002;51(RR-6):1-78.
Summary
Work-up genital lesions Confirm all clinical diagnosis with Type-
specific test Don’t be afraid to use Type –specific serology When screening for GH, keep in mind clinical
history and local prevalence with low (1.1 to 2.0 or 3.0) serologic ELISA index assay


















