La toxicity
26
The Way to Safe Local Anesthesia Dr. Mohamed Sayedalahl, MD Mansoura University, Egypt Ass.Consultant, KAMC Monday, February 23, 2015
-
Upload
mohammed-sayedalahl -
Category
Health & Medicine
-
view
85 -
download
0
Transcript of La toxicity
The Way to Safe Local Anesthesia
Dr. Mohamed Sayedalahl, MD
Mansoura University, Egypt
Ass.Consultant, KAMC
Monday, February 23, 2015
Wide spread use of LA
Toxicity is prevalent
Lack of awareness
Why This Subject ?

Wide spread use of LANurses, General surgeons, Plastic surgeons, ENT surgeons, Orthopedic surgeons, Obstetricians & Gynecologists, Dentists, Ophthalmologists, Radiologists, Cardiologists, ER physicians, Anesthetists.
Why This Subject ?

Toxicity is prevalent
Why This Subject ?

Lack of awarenessRecent survey in UK, 2010
Less than 50%→ Calculate dose
Less than 25%→ Recommended safe dose
Less than 7% → Intralipid
Less than 3% → Initial dose of Intralipid
Why This Subject ?

Retaining consciousnessNo need for Airway securingLess risk of AspirationLess hemodynamic variationsLess MedicationsLess need for complex MonitoringSuperior Pain controlFaster smooth Recovery & DischargeLess risk of perioperative complicationsLess Cost
Why WE prefer LA ?

1860 cocaine isolated Albert Niemann
1884 Carl Koller, local anesthesia, glaucoma patient
200 cases systemic toxicity & 13 deaths
1904 Novocaine (procaine) by Alfred Einhorn
1943 Lidocaine by Lofgren & Lundquist
1957 Bupivacaine by Ekenstam
1979, 5 reports of cardiac arrests, prolonged unsuccessful CPR.
1983, FDA , 49 cases of cardiac arrests, 0.75% bupivacaine.
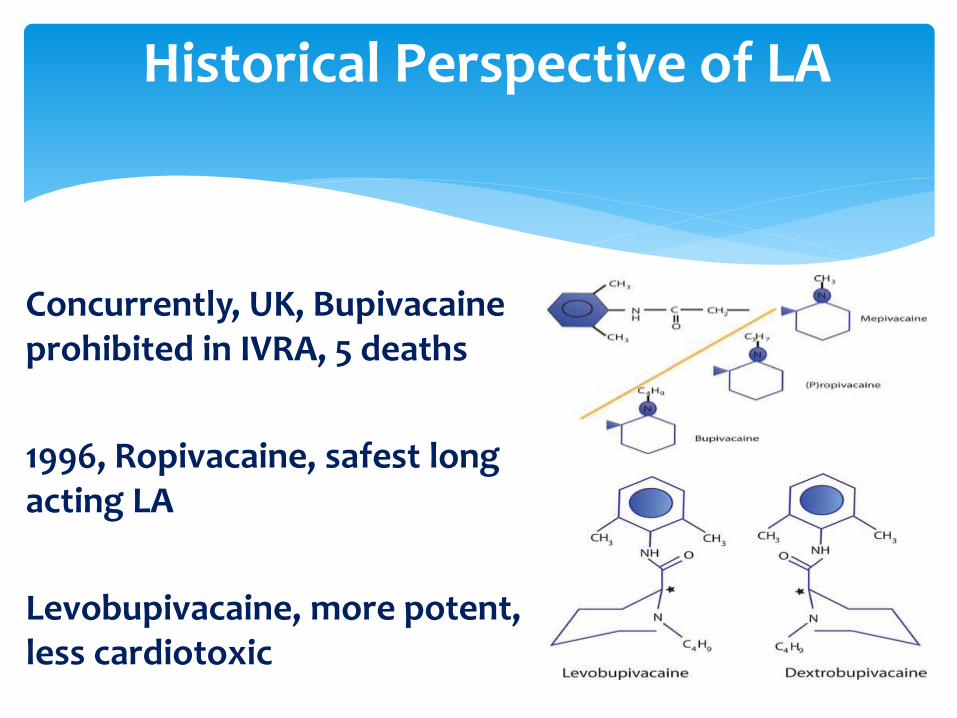
Historical Perspective of LA
Historical Perspective of LA
Concurrently, UK, Bupivacaine prohibited in IVRA, 5 deaths
1996, Ropivacaine, safest long acting LA
Levobupivacaine, more potent, less cardiotoxic
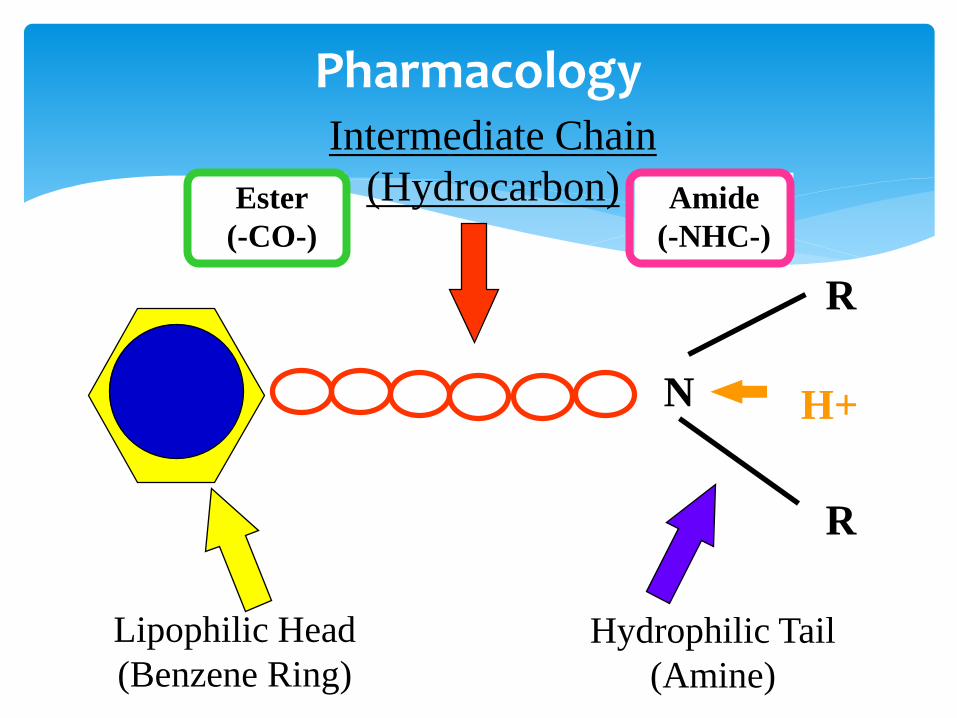
N
Lipophilic Head
(Benzene Ring)
Hydrophilic Tail
(Amine)
Intermediate Chain
(Hydrocarbon)Ester
(-CO-)
Amide
(-NHC-)
R
R
H+
Pharmacology

Pharmacology
Lidocaine
Bupivacaine
Etidocaine
Mepivacaine
Prilocaine
Ropivacaine
Chloroprocaine
Cocaine
Procaine
Tetracaine
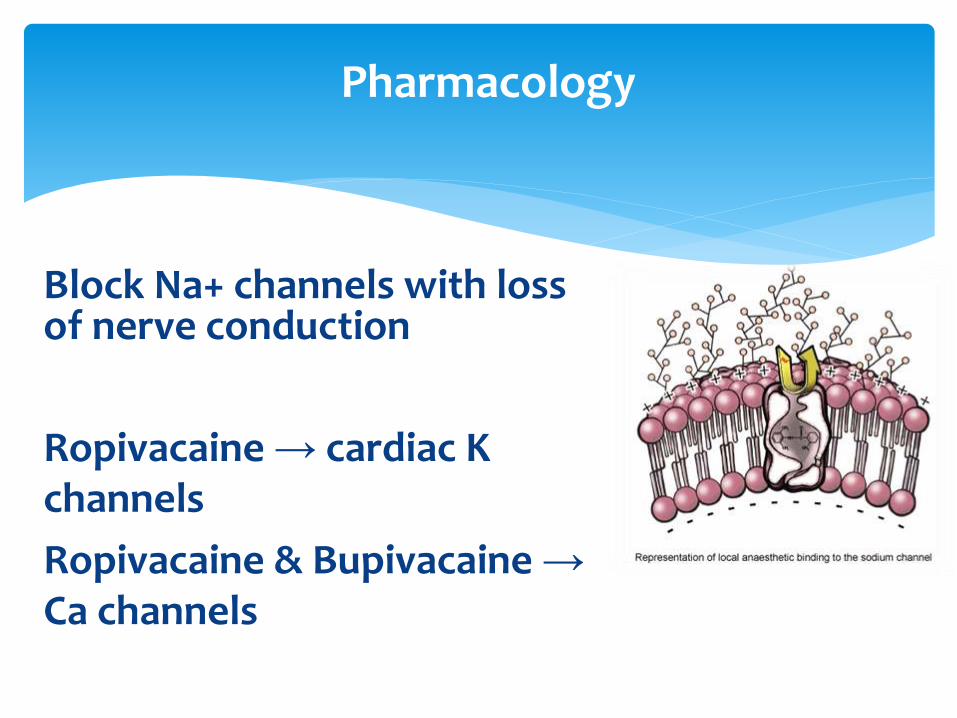
Block Na+ channels with loss of nerve conduction
Ropivacaine → cardiac K channels
Ropivacaine & Bupivacaine →Ca channels
Pharmacology
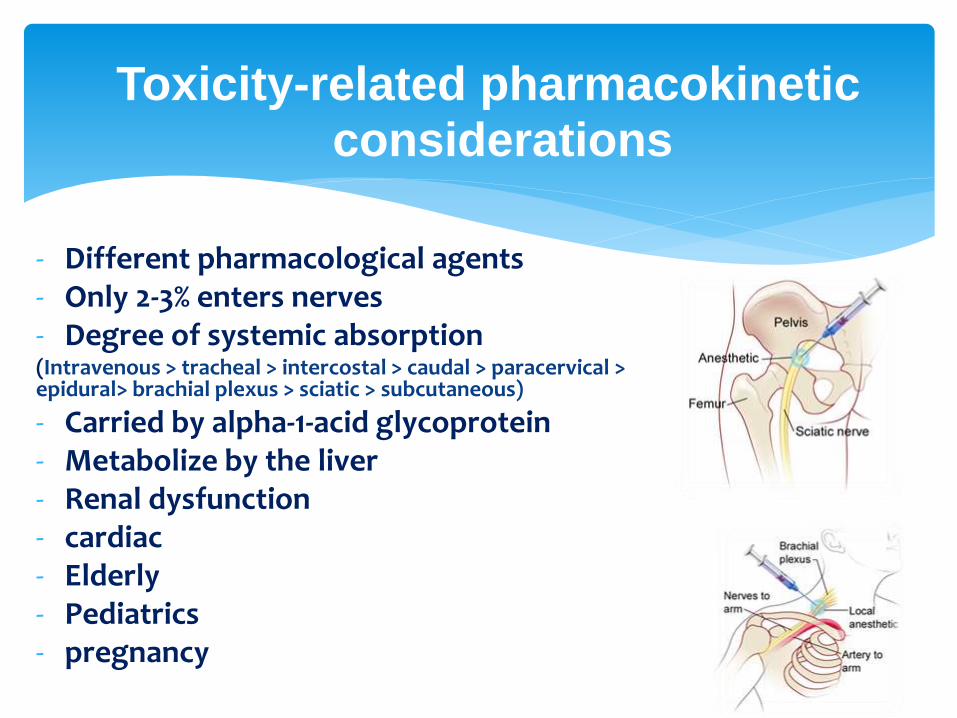
- Different pharmacological agents- Only 2-3% enters nerves- Degree of systemic absorption(Intravenous > tracheal > intercostal > caudal > paracervical > epidural> brachial plexus > sciatic > subcutaneous)
- Carried by alpha-1-acid glycoprotein- Metabolize by the liver- Renal dysfunction- cardiac- Elderly- Pediatrics- pregnancy
Toxicity-related pharmacokinetic considerations
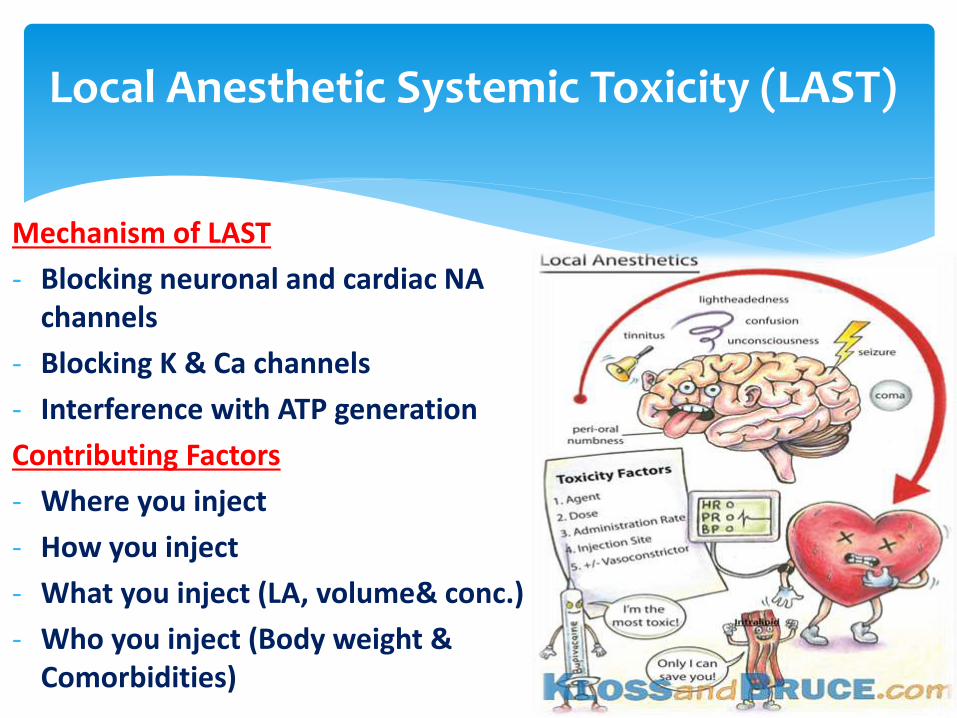
Mechanism of LAST
- Blocking neuronal and cardiac NA channels
- Blocking K & Ca channels
- Interference with ATP generation
Contributing Factors
- Where you inject
- How you inject
- What you inject (LA, volume& conc.)
- Who you inject (Body weight & Comorbidities)
Local Anesthetic Systemic Toxicity (LAST)
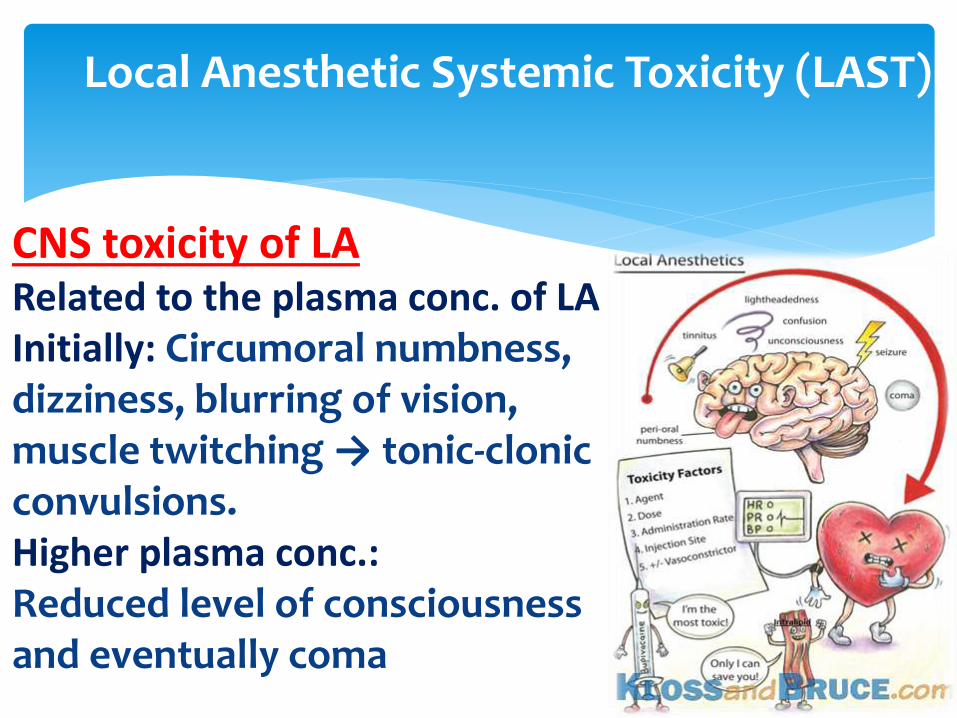
CNS toxicity of LARelated to the plasma conc. of LAInitially: Circumoral numbness, dizziness, blurring of vision, muscle twitching → tonic-clonic convulsions.Higher plasma conc.:Reduced level of consciousness and eventually coma
Local Anesthetic Systemic Toxicity (LAST)

Cardiac toxicity of LA
Initially: ↑ BP & tachycardia
Higher Conc.: conduction delay, ↑ PR, wide QRS,
ventricular arrhythmia, profound contractile dysfunction → cardiovascular collapse.
Possible contributory mechanisms :
direct –ve intotropic effect
Vasoactivity of LA:Lidocaine
Bupivacaine & levobupivacaine
Ropivacaine
Local Anesthetic Systemic Toxicity (LAST)

Toxicity profile of common LA
Lidocaine Vs Bupivacaine
Order of safety:
Lidocaine˃Ropivacaine˃Levobupivacaine˃Bupivacaine.
Peditric: Cardiac toxicity; 1st.
Local Anesthetic Systemic Toxicity (LAST)

Intralipid20%
FK, 200 gms purified soya bean, 12 gmpurified egg phospholipids, 22 gmanhydrous glycerol, omega 3 & omega 6 FA.
Discovered by chance
↑ bupivacaine cardiac toxicity # protective against toxicity.
Experimental & case reports proof.
Approved: FDA, ASRA, AHA, AAGBI
Intravenous Lipid Emulsion(ILE) Intralipid
Mechanism of action
lipid sink theory: extract lipophilic LA
Metabolic theory: supply FA substrate
Risks :Anaphylaxis
Why Intralipid100% long chain FA # Medialipid & Structolipid
Intravenous Lipid Emulsion(ILE) Intralipid
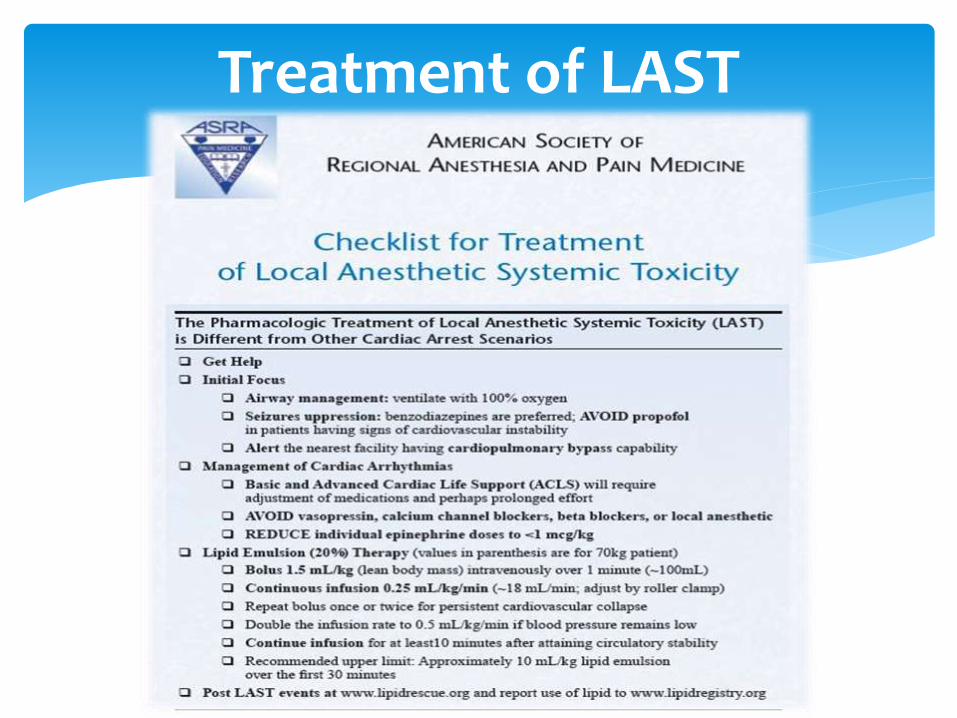
Treatment of LAST
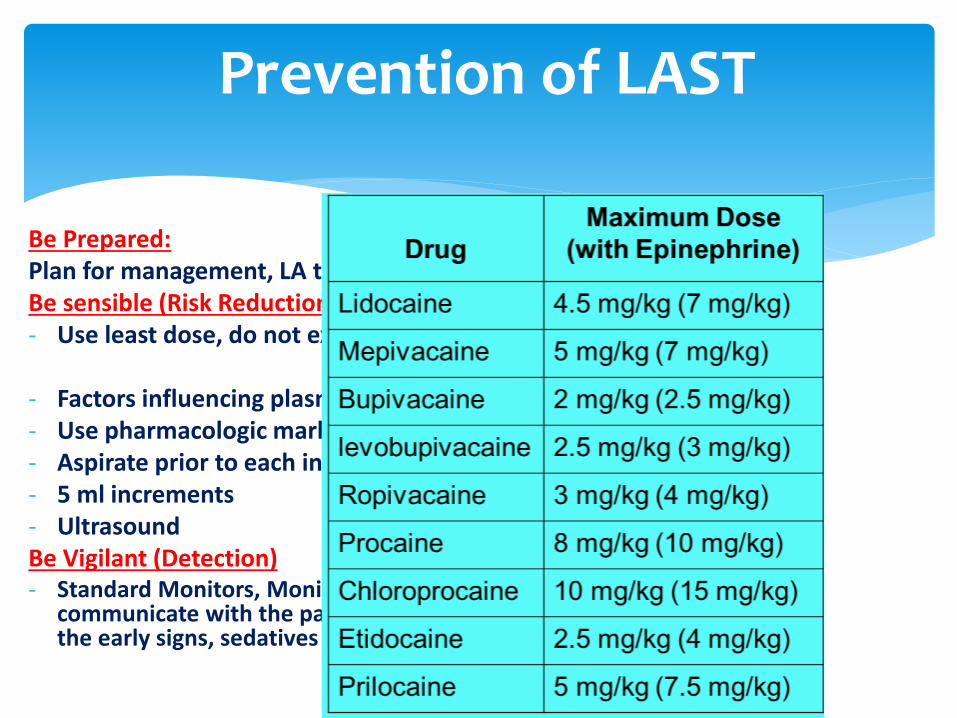
Be Prepared:Plan for management, LA toxicity KitBe sensible (Risk Reduction)- Use least dose, do not exceed max. dose
- Factors influencing plasma level- Use pharmacologic marker- Aspirate prior to each injection- 5 ml increments- UltrasoundBe Vigilant (Detection)- Standard Monitors, Monitor patient during & after injection,
communicate with the patient frequently, suspect LAST with the early signs, sedatives
Prevention of LAST

- Get help
crash cart
Trained personnel
Monitors & IV access
- Initial Focus
Airway securing
Seizure suppression (avoid propofol)
Alert nearest facility having CPB capability
New 2012 ASRA Guidelines

- Manage Cardiac arrhythmia
Modified ACLS
Consider lower doses of epinephrine(˂1u/kg)
Prepare for prolonged effort
Avoid vasopressin, beta blocker, CCB, LA
Amiodarone
- Obtain Intralipid
New 2012 ASRA Guidelines
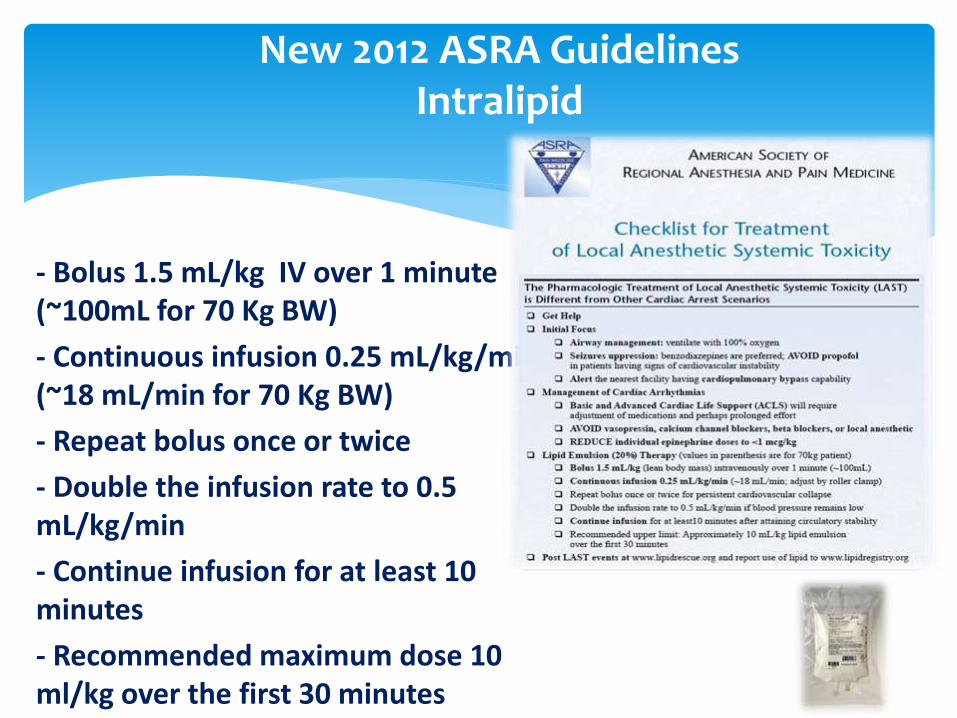
- Bolus 1.5 mL/kg IV over 1 minute (~100mL for 70 Kg BW)
- Continuous infusion 0.25 mL/kg/min (~18 mL/min for 70 Kg BW)
- Repeat bolus once or twice
- Double the infusion rate to 0.5 mL/kg/min
- Continue infusion for at least 10 minutes
- Recommended maximum dose 10 ml/kg over the first 30 minutes
New 2012 ASRA GuidelinesIntralipid

- Local anesthetic toxicity is a life threatening complication.
- Early detection & treatment is necessary for good patient outcome.
- 2012 ASRA Guidelines include: Monitoring, Emergency equipment, modified ACLS protocols & familiarity with the lipid emulsion.
Summary