Scaphoid non-union? SLIL (Scapho-Lunate Interosseus Ligament) avulsion?
Upload
nikos-darlisCategory
view
1.422download
5description

Kienböck’s disease(what we haven’t learned in the first
100 years…)
Nickolaos A. Darlis, MD, PhD
To access this presentation on the web:

“Traumatic Malacia”
Robert Kienböck

Courtesy Dr Stephanie Low


Contributing Factors:• Trauma/stress May simply aggravate a pre-
existing condition (catalyst)
– Acute Fracture– Occupational– Anatomic variations
• Vasculopathies– Septic emboli– Vasculitis– Raynaud’s– Scleroderma– SLE
• Viral disorders– Reactive arthritis (Hepatitis,
HIV)
• Coagulopathies– Sickle cell anemia– Secondary factor
• Miscellaneous stuff– Steroid exposure– Caisson’s disease– Fat storage
• Role of Genetics• Role of Osteoclasts

Pathophysiology
Early – Vascular• Ischemia• Necrosis• Revascularization
Intermediate – Osseous• Sclerosis• Subchondral collapse• Coronal fracture• Remodeling
Late – Chondral• Subchondral bone collapse• Articular surface non-functional• Opposing surface non-
functional

Vascularity• Palmar vs Dorsal
• Intraosseous pattern Gelberman, JHS, 1980

Morphology
Trabecular pattern weakest
Zapico 1966

Ulnar variance- Radial inclination
Negative ulnar variance and flattened radial inclination may predispose certain patients to develop Kienböck's disease, but neither is likely the sole cause
(Allan, JAAOS, 2001)

MRI

Not all MRI abnormalities = Kienbock’s


Pronated grip view
Highlight ulnacarpal impaction

Pronated Grip View Radiographs




Stage INormal radiographs or linear fracture, MRI changes in vascularity

Stage IILunate sclerosis, one or more fracture lines with possible early collapse of lunate on radial border

Stage IIIALunate collapse normal carpal alignment and height

Stage IIIBLunate collapse, carpal collapse, scaphoid rotation, carpal height decreased, capitate migration proximally•SL angle > 600

Stage IVSevere lunate collapse with intra-
articular degenerative changes at the midcarpal joint, radiocarpal joint, or
both

Is Stage I really “The Beginning”?
• There may be (probably is) an earlier stage when…wrist pain is present only with stress, and…the standard MRI is still normal.
“Angina of the wrist”

Lunate Stress Test(Similar in concept to coronary stress
test)
• Repetitive axial wrist loads followed by:
• Gd. enhanced fat suppressed T-1 sequences– Normal signal at rest– Schmitt-Lanz pattern A (bone edema) with
stress
• Gd. perfusion scan – compare bilateral flow rates pre and post
exercise

Stage “III-C” Kienböck’s
• Coronal plane fracture:– Poor prognosis (even if it otherwise resembles stage II
or III-A)

Stage “III-C” Kienböck’s
More aggressive treatment
• Lunate excision w. fusion (STT/SC)
• PRC

Different pathway in children?
Irisarri:
Infantile Kienböck’s (5-10 yrs) Excellent prognosis with non operativemanagement Juvenile Kienböck’s10 -15 yrs – similar to infantile >15 yrs – more likely to need surgical Rx, butbetter prognosis than adult as seen on MRI“Teenböck’s” disease?

16 y.o. female gymnast
• 5 months wrist pain @ diagnosis

16 y.o. female gymnast
• @ diagnosis

16 y.o. female gymnast• 2 month post diagnosis (7 mo post presentation)

16 y.o. female gymnast
• 9 month post diagnosis (14 mo post presentation)

15 yo male stage IIIA

Kienböck’s in the “Elderly”Taniguchi et al…Studied 14 pts with onset >60
• Etiology different?– Ulnar minus less frequent– Women more frequent
• Related to osteoporosis?• Natural history different?
– Collapse progressed in all
Conservative treatment

Treatment by Stage/Variance
CurrentStage Variance TreatmentI (+/-) Immobilization (3-6 mos)II/III-A (-) Radial shorteningII/III-A (+) VBG /Capitate shorteningIII-B (+/-) PRC or STT/SC fusionIV (+/-) Wrist Arthrodesis/PRC

Non-operativeTreatment(I/II/IIIA)
• Conservative vs operative (various) in 43 pts at 5 years found no superiority of surgery over non-surgical outcomes
(Delaere, JHS Br, 1998)
• Non-operative trial and careful selection of operative candidates
• However… the natural history is PROGRESSION

REVASCULARIZATION
UNLOADING
SALVAGE
Stage II Stage II, IIIA
Stage IIIB, IV

DRILLINGVBG
FREE PEDICLELT ARTHRODESIS
RADIAL SHORTENING
WEDGE OSTEOTOMIES
CAPITATE SHORTENING
STT/SC ARTHRODESIS
EX-FIXPRCWRIST FUSION
LUNATE EXCISIONWRIST
DENERVATION

Metaphyseal Core Decompression(II/IIIA negative ulnar variance)
• 22 patients, 10 year follow up– 16 patients pain free– Slightly improved ROM– 20 patients returned to
occupation– No patients underwent additional
surgical procedure (Illarramendi,
JHS, 2001)
• No Biomechanical analysis

Treat or Salvage?

Gadolinium Infused MRI (fat suppressed T-1)Patterns (Schmitt and Lanz) :
Pattern A - Marrow edema with intact (viable) bone trabeculae
- Increased (homogenous) signal
Pattern B - Early marrow necrosis with fibro-vascular reparative tissue
- Mixed (inhomogenous) signal zones
Pattern C - Necrotic bone marrow with collapse
- Decreased (homogenous) signal

A
B
C

Stage II-b: Poor prognosis>> PRC
Arthroscopic assessment
Courtesy, Gregory Bain, MD

Arthroscopic assessment
• Differentiate between Lichtman IIIA-B and IV disease
• Exact location of arthrosis in stage IV– is PRC indicated?
• Diagnose stage IIIC– Poor prognosis

Radial Shortening Osteotomy (II/IIIA negative ulnar variance)
• Only 2-4 mm of shortening – consider saw kerf
size (1-2mm)– beware of ulnocarpal
impaction
• Diaphyseal straight plate
• Distal metaphyseal w fixed angle plate
UNLOAD

Radial Shortening Osteotomy (II/IIIA negative ulnar variance)
UNLOAD

Radial Wedge Osteotomy (closed)
(II/IIIA positive/neutral ulnar variance)
Giannikas 1968
Biomechanics
• 2-D Mathematical model– Lunate offloaded by 23% (Wantanabe, JHS, 1993)
• Cadaveric– 24% increased lunate strain in extension (Kam, JHS, 2002)
• Pressure sensitive film– Increased lunate fossa pressure on
radius (Werner, Hand Clinics, 1993)
UNLOAD

Courtesy Prof A. Beris

Radial Wedge Osteotomy (opening)
(II/IIIA negative ulnar variance)
• Increased forces across ulna and nearly eliminated forces across radiolunate joint
(Viegas, JHS, 1989)
• 26% decrease on lunate cortical strain
(Kam, JHS, 2002)
• Decreased pressure across lunate fossa measured on pressure sensitive film
(Werner, Hand Clin, 1993)
UNLOAD

2D Radial Wedge Osteotomy (II/IIIA negative ulnar variance)
UNLOAD

Capitate Shortening (II/IIIA positive/neutral ulnar variance)
• Must ensure hamate does not abut on the lunate after shortening
• If present, removal of proximal tip of hamate
• Usually requires capitohamate fusion– ? Impact on ROM
UNLOAD

Capitate Shortening (II/IIIA positive/neutral ulnar variance)
UNLOAD

STT Fusion(Stage IIIB)
• Decreases lunate loading– Significant decrease in wrist
ROM (Trumble, JHS,
1986)
• Increased force transmission through radioscaphoid and midcarpal joints may lead to early degenerative changes
(Iwasaki, JOR, 1998)
SALVAGE
UNLOAD

Arthroscopic directed forage (drilling) of the lunate in a patient with an arthroscopic grade O Kienbock’s disease. (from Bain and Durrant, THUES 2011.)
DrillingREVASC

Reverse Flow Pedicle/Bone Graft from Distal Radius
REVASC


15 yo male stage IIIA

Courtesy D.G. Sotereanos, MD

Capsular Based Bone Graft from Distal Radius
REVASC
Sotereanos, Darlis et al. , JHS(A), 2006

Capsular Based Bone Graft from Distal Radius
REVASC

Capsular Based Bone Graft from Distal Radius
REVASC

Vascular Pedicle with Cancellous Bone Graft
(
Moneim, Iowa Ortho J, 1998Hori, Tami
REVASC

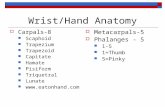
Vascularized Bone Graft from Metacarpals
Bengoechea-Beeby, JHS, 2001
REVASC

Vascular Grafts
• Cartilage shell of lunate must not be compromised
• Post op immobilize & unload lunate– Ex-fix– Temporary STT fusion
• Does not preclude other treatment options (revasularize + unload)
REVASC

Lunotriquetral Arthrodesis Unpublished data
rationale based on bone grafting a scaphoid nonunion with AVN of the proximal fragment where healing is achieved by “creeping substitution”
Courtesy: Martin Posner, Steve Green
REVASC

1 year Post-Op

Proximal Row Carpectomy(Stage IIIB)
• Relative Contraindication if capitate head or radiolunate fossa demonstrate degenerative changes – Can be technically overcome
• Beware of palmar ligaments (RSC), avoid ulnar tanslocation of the wrist
• Not universally accepted– Better pain relief, ROM, and strength
with limited wrist arthrodesis (Nakamura,
JHS, 1998)
SALVAGE

Lunate Excision(Stage IIIB)
• Tendon Ball Implant (palmaris longus, plantaris)
• Silicone Replacement Arthroplasty, Titanium Implant
– No longer widely used
SALVAGE

Stage IV
• Proximal row carpectomy • Wrist fusion• Wrist denervation• Wrist arthroplasty?
SALVAGE

Take home messages
• Simple surgery –patient tailored
– Etiology? Ulnar plus? Inclination?
• Get as much info as you can – Gd MRI, Arthroscopy
• VBGs do not restore cartilage• Radial Shortening and PRC time
tested operations

THANK YOU
To access this presentation on the web: