Kerala Ayurveda News & Views Vii PDF
34
st Date: 1 April 2008 No: 07 Vol: 02 Web site : E-mail : www.keralaayurveda.biz [email protected] [email protected] 3 0 n Frankly Speaking - n Darshan 2008-Kateegraha - 05 n An Exploration on Oushadhopayogakaalam - 1 7 n Male Sexual Dysfunction and.... - 19 n Mucuna or Cowhage - 24 n Kapikachu-Ayurvedic View - 29
-
Upload
nileshmanakikar -
Category
Documents
-
view
541 -
download
8
Transcript of Kerala Ayurveda News & Views Vii PDF

stDate: 1 April 2008
No: 07Vol: 02
Web site : E-mail :
30 � Frankly Speaking -
� Darshan 2008-Kateegraha - 05
� An Exploration on Oushadhopayogakaalam - 1 7
� Male Sexual Dysfunction and.... - 19
� Mucuna or Cowhage - 24
� Kapikachu-Ayurvedic View - 29

TM
4
EDITORIAL COMMITTEE
PATRONDr.K.Rajagopalan
ADVISORY COMMITTEESri. Sonjoy MohanthyDr.K.Anil KumarDr.C.I.JollyDr.C.R.AgnivesDr.Jacob Jayan B.
MANAGING EDITORDr.K.Sasidharan
EDITOR IN CHIEFDr.Sahny.M.Soman
EDITORSDr.Binoy D.DasDr.K.VasanthakumariDr.V.Jayakumar
EDITORIAL TEAMDr.Geetha.G.PillaiMrs.Dulari.S.SMr.Bose R.C.
PUBLICATION OFFICEKerala Ayurveda HospitalBank RoadAluva-01Tel : 0484-3221365, 2626119, 2623578E-mail : [email protected] [email protected]
1
FROM THE EDITORMeasuring the essence of Ayurvedic sciencein modern parameters sometimesculminates in success and sometimes infailure. This is a tough problem to all whomay work in the research field of any otherAlternative systems of medicine. Comparison on some areas may look irrati onal andridiculous. It is likely that a significantproportion of advantage from even rationalinterventions is due to nonspecific effects.Hence again the bias in comparative studiesaccumulates. Also in a good number ofsituations Ayurvedic treatment compli-ments the modern medicine. Specialevaluation methods should be generated insuch areas. Existing rules are rudimentaryand new ones have to be formed. It is oftena dynamic area where contributions andcomments are invited. In this point of viewI really want to congratulate Dr.San-deep.K.M for making a few modest steps inresearch activities designed by him and fewcolleagues (see the article in this issue ‘Anexploration on Oushadhopayogak-alam’).These types of scientific interventionscould culminate in triumph though thebeginning would be simple as here they haveput their scientific spirit as the only initialinvestment.
I think we shouldn’t move away from any ofthe positive things we plan to start; keep inmind the axiom ‘An expert is someone whohas made all of the possible mistakes in avery narrow field of study.’ So don’t wait insearch of inspiration to start with. Actionalways generates inspiration. Finding newmethods and translating the availableresearch methods to suit to our clinicalsettings are the current challenges ahead ofthe Clinical Research Wing. I seek co-operation from all in the upcoming activities.
Thanking you
Dr.Sahny.M.Soman BAMS, MBBS

2
LETTER TO THE EDITOR
It gives immense pleasure to read KeralaAyurveda News & Views. All the articlesare very informative and interesting. Isuggest that pharmacological actions ofkashaaya or lehya or coorna or vati can beincluded in every issue which would helpfreshers to rethink and guide them in the rightpath of treatment. My hearty wishes to allthose scholars whose hard work has yieldedthis bi-monthly in house journal.
Dr.Gija GangadharanTrainee Co-ordinatorKerala Ayurveda
Our knowledge is growing and now we arekeen in enhancing our abilities in managingdifferent clinical entities. In this regard thearticles in our in house magazine really helpemerging physicians like me. In order toelaborate our ideas and views and to exploreAyurveda, the articles in the columns “DrugReview” and “My Memorable Patient” servesas beckon of hope.
Dr.Pinchu Paulson BAMSHouse SurgeonALN Rao Memorial Ayurvedic MedicalCollege, Koppa, Karnataka
I have read the last two issues of KeralaAyurveda News & Views. The articles arevery impressive and useful also. I request youto include the rare cases of experiencedphysicians too.
Dr.Nishana.N.KTrainee Medical OfficerKerala Ayurveda Hospital, Aluva
The content in the magazine is reallyinformative and fascinating specially “MyMemorable Patient” and “Classical DrugReview”. It gives one the guidelines about thediagnosis and the approach according totextual references and Rasa, Guna, Veeryaand Vipaaka. But I think it is necessary toinclude the clinical diagnosis of diseases as permodern science with their lab investigationsalso. With this we can analyze the fate of thedisease and accordingly we can decidewhether patients needs Ayurvedic treatmentor the modern treatment.
Dr.Ranjan KapoorTrainee Medical OfficerKerala Ayurveda Hospital, Aluva
After joining Kerala Ayurveda Hospital as atrainee doctor, I got the opportunity to readfew issues of the in-house magazine. Theinformation provided in it were quiet helpfulto recall my knowledge regarding the giventopics. All the articles are very impressivespecially “Frankly speaking”. So I sincerelycongratulate the editorial team for letting ourancient path come up in such a simple waythat even a lay man can easily understand.
Dr.Anupama.R.BaraMedical Officer (Trainee)Kerala Ayurveda Hospital, Aluva

3
THE OBSTINATE DOCTOR
Dr. C.R.Agnives B.Sc, MD(Ay)Chief Editor, Kerala Ayurveda Vaidyam
Frankly speaking, at times I am an obstinatedoctor. I insist that my patient should do thisor that and I now regretfully admit that mostof my such obstinacies were prompted by myconvictions, the majority of those erroneous.I may explain one or two of such obstinacies.
After coming from Moscow, once I chancedto travel in an autorikshaw. On reaching thedestination, the young driver did not receivethe fare from me. I insisted him to receivethe fare. But at any cost he will not receive it.He said, “ Don’t you remember me Sir. Youhave treated my mother. I am highly thankfulto you and how can I receive any money fromyou?”
I scanned my memory in futility. He added.“She had such a severe consistent headacheand you have treated her.” On hearing this Iwas happy that I have cured a chronicheadache. But my happiness was short lived.I asked him. “How is the headache now?” Tothis he answered. “My mother is no more sir.She had brain tumor.” I immeadiately realizedmy folly of not recognizing the headache asthe herald of a brain tumor. It is a clear caseof wrong diagnosis from the part of thephysician. Regaining my wits I askedhim. “Anyhow, I did not cure theheadache of your mother. Then whyshould you be thankful to me?”.
He answered with a smile. “Yet you have donea great service to me. You insisted that theroot cause of her headache was rotten teethwhich she had many. You made her extractthe teeth one by one excepting one or two.When it was diagnosed as brain tumor, theoncologists insited in removing the remainingteeth too to aid radiation treatment. If you
haven’t made her extract most of the teeth, itwould have been difficult to extract them allat a stretch. Hence your obstinancy that theteeth shall be extracted to cure the headachewas very useful.”
I hoped I could vanish into thin air using someold magical measure such as Indian vanishingtrick. For a few seconds I felt I was notexisting in this world. When I came torecognize the surroundings and theseriousness of my erroneous obstinacy, thankGod!, he had left with his vehicle leaving asmall cloud of exhaust fumes.
On recap, I remembered the case and manyother similar cases of headache. During mydays as a Saalaakya doctor in Kottakkalcollege, all sorts of headaches were referredto me. This was not because I was an expertcurer of headaches, but doctors who attendedthe general OPD wanted to reduce the crowdthere by shunning some cases to otherdepartments. Most of the cases thus directedto attend Saalaakya OPD were cases eitherof fever or constipation which could be verywell managed in gneral OPD. But I admit thatthere is no harm in examining the visual acuityof the person complaining of headache. Butwhen there was a palpable temperature above102o F, it is not reasonable for a GP to referthe case to an ophthalmologist. This sort ofirresponsible referring usually irritated meand I had expressed my disapproval to thereferring doctors only to add their disapprovalof me and to confirm their conviction that Iam a horrible personality.
Cutting the tale short, on those days I had toattend a lot of headache cases. It became thepart of my diagnostic ritual of headache to ask
Frankly speaking

4
the patient to open his or her mouth widelyso that I can count the carious teeth.Whenever I find a carious tooth it was myroutine to advise the patient to consult adental surgeon. On those days, most of thedental surgeons extracted the carious toothor teeth. Today they won’t do so. They willtry to retain the defective tooth to themaximum, as now they have recognized thatteeth, especially defective teeth, are theirbread and butter. So, now they try to retainthe teeth as far as possible. All the dentalsurgeons of the viscinity were highly thankfulto me for providing them ample supply ofpatients and became my friends. It was onsuch a back drop that this mother of theautorikshaw driver came to me with a chronicheadache and thirtytwo carious teeth. Mostof the teeth were dead and she felt notoothache at all. She too was insistant not toextract the teeth. I had to convince her bythreatening and lecturing about theconsequences of carious teeth left intact inmouth. She tried to defend stating that shehad no toothache. I retorted blatantly that theteeth are not aching as they are dead and sheis carrying corpses of teeth in her mouth thoserot and damage the general health. I am awareof the hesitation of Muslim women to extractteeth as they are age conscious and losingteeth meant to them as aging and thisnaturally posed a threat to marital harmonyas the husband was free to choose a youngerwife. But I usually promise them thepossibility of having more beautiful andconvenient artificial dentition as an additionalattractiveness to their charm and after aseries of arguments and counter argumentsmost of them succum to my obstinacy. This,incidentally is such a case that has finally fellvictim to my obstinate conviction.
Headache is a difficult complaint. Anythingmay cause a headache. It may be a minor errorof visual acuity, it may be an alcoholic
husband, it may be a mischievous son, it maybe a loving husband who died early, it may bea guilt complex, it may be a tiresome job, itmay be an extra marital relation ship of thespouse, it may be an unrewarding job, asinusitis, constipation, a carious tooth, a spaceoccupying lesion in brain or its viscinityconducive to increase of intracranial pressure,a chronically infected ear, hyperpyrexia andwhat not? So to me who consider thattreatment is discarding the etiology, thetreatment of headache consisted of making achecklist of probable causes and discardingthem one by one. When no other etiologicalfactor is evident and when a carious tooth isspotted, it is too natural to accuse the toothas the culprit. I have did so here too. But Ishould have also thought of a silent tumor inthe brain.
Usually brain tumors notify their existance byheadache. But headaches of brain tumorsusually are accompanied by sickness orvomiting, papilledema and even exophthalmia(if the tumor is retrobulbar or if it generateshydrocephaly). Very rarely the headache ofa brain tumor may be withoutaccompaniments. This was such a case. TodayI will send such patients for scanning. But onthose days, scanning was not that popularamong Ayurvedic physicians. Hence the follyof diagnosis.
Another victim of my obstinate diagnosis wasa muslim girl of eighteen years. She wasbrought to me for severe pain in both theankle joints and difficulty to walk. She wascarried on hands and was unable even tostand. I conducted a thourough check up andfound nothing to substantiate her claim of pain.There was no tenderness, edema or rednessin both the joints. Hence to me the severe painwas not supported by any organic findings. Onthose days I was simply convinced that whenthere is no organic evidence to support the
Frankly speaking
(Contd. on page 13)

(In Darshan 2008 held on March 4 Dr.Sreeraj.I.P, Medical Officer, Kasargod haddelivered an elaborative presentation on Kateegraha. In an one hour lengthy presentation henarrated the anatomy of lower spine, causes of low back ache, IVDP of lower spine in detail,differential diagnosis of low back ache, clinical examination of the lumbar spine and mentionedthe management of low back ache and presented a few case summaries and prevention oflow back pain. The anatomical aspects covered vertebral bodies, anterior elements and posteriorelements of vertebral bodies, the pedicles, joints, inter vertebral disc, ligaments and muscles.Every one enjoyed the presenter’s mind-set to share his clinical cases with others. Due tospace limitations we are able to publish only the summary of the presented paper.)
KATEEGRAHA (LOW BACK PAIN)ABSTRACT
Kateegraha is a very common disease wecome across in clinical practice. A thoroughknowledge of the disease is necessary for itsdiagnosis and treatment. Brhath Trayees sayKateegraha as a symptom of PakvaasayaVaatakopa.
‘Tatra Pakvasaye Krudha Soolanaahaandhra koojanm
Malarodhasma vardha trika prshta Kateegraham
Karothi adhara kayeshu tamstaan krchraanupadravan’.
Kateegraha (Low back pain) is said to be theprice man pays for his erect posture. Actuallylow back pain is not a disease but a symptom.There are many causes for this. The mostcommon cause for LBA is Inter Vertebral DiscProlapse (IVDP). Ayurveda has very effectiveand safe treatment for the same compared toother systems.
DARSHAN 08
Causes of Low Back Pain
1. IVDP2. Local Lesions (In the Back)
Congenital Functional defect Degenerative
Traumatic Inflammatory Neoplastic
3. Remote Lesions (Other than the back)
Abdominal disorder Genito UrinaryCauses
Pelvic disorders Vascular disorders
5
Somatoform disorders

Lumbar Disc Diseases
Physicians interested in back pain are notinclined to read essays on anatomy; they aremore interested in the bottom line how do Itreat? However physicians need anunderstanding of Anatomy to appreciatewhich element of the lower spine can beinjured and to offer treatment on a rationalbasis.
Bio Mechanics:
The cardinal movements of the lumbar spineare flexion, extension, compression, axialrotation and lateral flexion. Our day to daylife gives compression, bending, and torsionto the discs. Flexion, extension, lateral flexiongives compressive stress to the discs. Rotationgives shear stress. The vertebral end platesare only weakly attached to the vertebralbody so that the disc weakly react, withhorizontal shearing forces. Compressioninjuries of the IVD may result from excessiveaxial loading. One of compression injury is
fracture of the end plates. It initiates theprocess - internal disc disruption. In the firststage of disc degeneration fibrillation occursin annulus fibrosus producing radial fissureswithout affecting disc height. There are threetypes of nucleus herniation.
1. Protrusion (without tear on annulus)2. Extrusion (Tear occurs in annulus but
inside posterior longitudinal ligament)3. Sequestration (Go to spinal canal)
Lumbar Disc Diseases
The main cause of back pain in age group of30-50 is lumbar disc problems. Heavymanual work, lifting weight may be the acutereason. The pain starting from hip regionextends to sacroiliac region, then buttocks andback of thigh.
Symptoms of Disc Herniation:
. Severe pain. Pain reduces when takingrest, increases while bending. Pain ismore in legs. Pain increases while
Common causes of back pain in various age groups.
Children Adolescents Young Adults Middle Age
Scoliosis Scheuermann’s disease Mechanical Back Mechanical Back disease pain pain
Spondylolisthesis Scoliosis Prolapsed Mechanical back intervertebral Primary osteo
Pyogenic pain disc. arthritis.infections Intervertebral disc- Spondylolisthesis
syndrome Spinal fracture Prolapsed interTuberculosis Pyogenic or- Ankylosing vertebral disc.
tuberculous spondylitis.Calve’s disease infections. Coccydynia
Pyogenic infectionsTuberculosisSpinal stenosis
DARSHAN 08
6

sneezing and coughing. Pain may occurin scrotum and perineum.
. Numbness
. Weakness may occur according to theneurological level of involvement.
. If the herniation of disc is high it maycompress cauda equina. In suchcondition numbness occur in legs, rectalpain, numbness in perineum,incontinence of bowel and bladder arethe symptoms. This is an emergencycondition.
. In acute IVDP case, there is paraspinalspasm while moving and walking. Whenpressed with finger there will be pain atthe region of spinous process of thecorresponding disc. If there is nerve rootirritation as a result of compression ofsciatic nerve there will be symptoms ofsciatica. There is pain in the sciatic notchand popliteal space. SLR test will bepositive in this case. Lassegue’s sign willalso be positive. We can correlate sciaticaas Grdhrasi.
“Parshnim Pratyanguleenaam ya kandaramaarutardita
Saktyulkshepa Nigrhnaati Grdhraseemtaam pracakshate”
. In L3-L4 Disc herination L4 nerve rootis affected and pain will be in the medialside of the leg. Numbness in anteromedial side of the leg would be present.There will be weakness of Quadricepsand hip adductors. Sensation will be lessin L4 dermatomes.
. In L4-L5 disc herniation, L5 nerve rootis affected. Numbness and pain will beon anterolateral side of leg and dorsumof foot.
. In L5 SI disc rupture S1 nerve isaffected.
. 90% of Lumbar disc prolapse occursbetween L4 and L5.
Differential Diagnosis
History taking plays an important role inthe diagnosis of causes of low back pain.History in LBA will give the diagnosis 80%of the time. A doctor who cannot take agood history and a patient who cannotgive one are both danger, for a betteroutcome expected. An accurate diagnosisis exceedingly important. Short andobese people have a greater chance ofIVDP and tall and lean people are alsoprone for IVDP.
. If it is a case of LBA in the earlydecades of life look for
a. Spina bifida - due to failure of fusion ofthe posterior part of the spine.Usually it affects one vertebra, mostcommonly in Lumbo sacral region.
b. Spondylolisthesis
This means forward shift of the spine. Theshift nearly always takes place between L4and L5 or between L5 and S1. 75% of the caseis congenital. Degenerative variety constitutesabout 20% of the cases. Traumatic varietyconstitutes about 5% of cases. In congenitalvariety there is developmental defect of thepedicle of the 5th lumber vertebra. This partwhich is called ‘pars interarticular’ is dividedinto two parts being connected by fibroustissue. The lower articular process remainswith the sacrum insitu while the upperarticular processes along with the spinalcolumn above move forward. The maincomplaint is the back ache which becomes
DARSHAN 08
7

more obvious after exercise or strain. Thepain may radiate down to the legs and theremay be weakness of the lower extremities.This is due to the pressure on the caudaequina and the emerging root. Disc prolapseis liable to occur. This condition may affectany age. But degenerative variety isobviously rare before the age of 40.
The upper angle of sacrum forms a distinctprominence on the back with depression justabove it. On palpation a definite prominenceat the upper angle of the sacrum will beobvious when the clinician runs the fingersdown along the spinous process.
In all cases of LBA rule out
A. Clinical conditions arising fromthe regions other than the back:
(a) Abdominal Disorders:(a) Pancreatitis - Pain occurs in
the middle of vertebral column.Increased serum amylase level inblood is an indication.
(b) Cholecystitis - inflammation of gallbladder.
(c) Biliary calculi(d) Peptic ulcer.
(b) Pelvic Disorders:Inflammatory condition of the ovariesand tubes.
(c) Genito Urinary Causes:Renal infection, Renal or ureteric calculus
Prostatitis, Prostatic carcinoma.(d)Vascular Disorders:Ischaemic pain from occlusion of aorta or
iliac arteries.(e). Somatoform disorders
B. Functional Defect:a) Scoliosis - This means deviation of the
spine to one side. In all cases of scoliosisone must not forget to examine the heart
and lungs as congenital heart disease maybe associated with this condition.
b) Kyphosis - excessive posterior convexityof the thoracic spine.
c) Antero posterior imbalance due topregnancy, pot belly etc.
C. Inflamatory conditions:
a) Tuberculosis of spine (Pott’s disease)It affects children and adolescents morecommonly than the adults.
b) Osteomyelitis of the spine - very rare.Characterized by sudden onset of fever andsevere local pain.
c) Ankylosing spondylitis.d) Myositis, Fibrositis.e) Rheumatoid arthritis.
D. Degenerative diseases:
a) Osteo arthritis (spondylosis)b) Senile osteoporosisc) Degenerative Disc disease.
E. Traumatic:
a) Lumbo Sacral strainb) Injury to Intervertebral joints and
musclesc) Spondylo listhesis.d) Compression fracturee) Vertebral process fracturef) Ruptured disc.
F. Neoplastic:a) Primary tumours - eg. multiple
myelomab) Metastatic tumours from breast,
bronchus, kidney etc.Examination of the Lumbar Spine1. Darsana Pareeksha - According to the
posture of the patient.2. Sparsana Pareeksha - Contour of spine,tenderness, SLR test.SLR Test: The patient lies supine on theexamination table. The patient is now askedto raise one lower limb keeping knee straight.He should continue to raise the leg till he
DARSHAN 08
8

experienced pain. The angle in which the painis experienced is noted. If the pain is evokedunder 40o it suggests impingement of theprotruding inter vertebral disc on a nerveroot. If it is above 40o it is not necessarilydue to IVDP.Lassegue’s Sign: In SLR, at the angle whenthe patient experiences first twinge of painthe ankle is passively dorsiflexed. This causeaggravation of the pain. It suggests irritationon one or more nerve roots either by IVDPor from some space occupying lesion.Femoral nerve stretch test: Patient isasked to lie on his abdomen and flex the kneeof affected side. If pain in thigh regionincreases it is positive. L2-L3 IVD isprotruded in this case.Special Investigations:1 LabHb,TC,DC, ESRS.Alkaline PhosphataseS.Acid Phosphatase2. Roentgenography (X-rays)Usually done in AP view and lateral view in
some cases oblique view is also taken.3. Myelography:
Now it is very rarely used.4. Computed Tomography (C.T.Scan)5. Magnetic Resonance Imaging (MRI)
The accuracy of MRI is said to be—88%
6. Positron Emission Tomography (PET)
Treatment of IVDP
We can treat disc prolapse according to thetreatment principles of Vrna Cikitsa, BhagnaCikitsa and Vaatavyaadhi Cikitsa.. While considering disc prolapse it can be
taken as Vrna. The nucleus is coming outthrough annulus making a tear in it.
. The joint including two vertebrae anddisc can be considered as one unit. The
changes in this joint due to trauma etc.can be taken as Sandhi Bhanga.
. The symptoms of IVDP is like that ofVaatavyaadhi- cheshtaahaani, Soolaetc.
So we should do the treatment for IVDP asa combination of Vrna cikitsa, Bhagnacikitsa and Vaatavyaadhi cikitsa.
Vrna Cikitsa in IVDP
Apatarpana, Alepa, Parisheka, Abhyanga,Sveda, Vimlaapana, Upanaaha, Visraavana,Snehana, Virecana. These Kriyaas in VrnaCikitsa can be used.
Apatarpana - Restriction of food. To avoidoily food etc. To reduce body wt in obesepatients.
Alepana - Lepam with medicines in Kadeepradesa. We can do lepa with NagaraadiCoornam, Jadamayaadi Coornam,Karuttamarmani etc. in Dhanyaamla. It willreduce the oedema in Kadeepradesa and willreduce pain also.Parisheka- If there is severe pain Parisheka(Dhara) with Dhanyaamla have very goodeffect
Abhyangam - Also found to be useful whendone with vaatahara preparations
Svedana - After Abhyanga we can doSvedana. It will give very good result inIVDP case. Usually we are doing Patrapotalasvedam, Jambeera pinda svedam, Valukaasvedam etc.
Vimlaapana - We can do spinal massage,Traction massage etc. Traction with pelvictraction belt can be used. Skin traction is also
DARSHAN 08
9

beneficial. We can decide the weight oftraction according tot the weight of the patient.Usually 2Kg + 2Kg, 2.5Kg + 2.5Kg is used.From my experience, my advice is not to usetraction weight more than 2.5Kg + 2.5Kg. Ifwe are using more weight, it may lead to neckpain.
Upanaaha - Upanaaha with JadaamayaadiCoorna is good. We can use Eranda leaf forUpanaaha Karma. Datura fruit or Erandaseed and sesamum made into a paste withmilk can be used for Upanaaha. It gives goodresult.
Visraavana - Raktamoksha can be done insuitable patients.
Snehapaana - We can use IndukaantaGhrtam, Thiktaka Ghrtam for Snehapaanam.
Virecana - It is a very important treatmentmethod in IVDP cases. Virecana can be donewith Gandharvahastaadi Erandam, TrvrutLehyam or Avipatti Coornam. We can giveGandharvahastaadi Kashaayam withGandharvahastaadi Erandam in emptystomach for Doshanulomana.
Bhagnacikitsa in IVDP
Angchana, Bandhana, Kapaatasayana andSnehavasty is used here.
Angchana - Traction is mentioned here.Traction massage, pelvic traction, skintraction etc have great importance in thetreatment of disc prolapse.
Bandhana- Bandage in Kadeepradesa is animportant treatment. Usually we are doingbandage with Murivenna. We are advisingthe patient to wear L.S. corset while sittingor walking.Kapatasayanam - Taking full rest in bed. Itwill reduce the muscle spasm.
Snehavasty - Snehavasty or Mathravasty isa good treatment here. Snehavasty can bedone with Sahacharadi Sevyam, orDhanvantaram Sevyam. Usually we can doMaatravasty with 75ml Sneham.
Principles of Vaata Vyaadhicikitsa inIVDP
Snehanam, Svedanam and Sodhanam arethe principles of treatment here.These are done in disc prolapse. In Snehanawe can use Vaatasamana tailam. Here Iwould like to say about Kerala Ayurveda’sproduct- Myaxyl oil. In my experience it givesquick relief and a highly compliant drug.Patrapodala svedam, Jambeera Svedam etc.can be used here. After that we can selectVasty or Virechana. Usually we are doingYogavasty ie 5 Snehavasty and 3Kashaayavasty. Sahacaraadi Sevyam,Dhanvantaram Sevyam can be used forSnehavasty. Madhuthailika Vasty is used fornirooha. In some cases Vaitarana Vasty andKsheeravasty can also be used. In some caseswhere Vaatakopa is more Mathravasty withGandharvahastaerandam gives very goodresult, usually applied in 60ml dose.
Kadeevasty:
Kadeevasty has a very important role in thetreatment of Kateegraham. In the beginningstage we can do Kadeevasty. Kadeevastywith Murivenna gives very good result. Picualso gives good result. As Samanoushadhawe can give Sahacaaradi Kashaayam,Gandharvahastaadi Kashaayam, Guggulutiktakam Kashaayam, GuggulutiktakamGhrtam, Maharaasnaadi Kashaayam,Raasnasaptakam Kashaayam etc.
. Yogasanaa like Bhujangaasana, Pavanamuktaasana etc. give good relief in mostof the IVDP cases.
DARSHAN 08
10

History taking plays an important role in thediagnosis of causes of low back pain. Historyin LBA will give the diagnosis 80% of the time.A doctor who cannot take a good history anda patient who cannot give one are both danger- in danger of bad treatment. An accuratediagnosis is exceedingly important. Short andobese people have a greater chance of IVDPand tall and lean people are also prone forIVDP.References1. A practical guide for the primary care
Clinician By Cole &Herring
2. Clinical Orthopaedics India. By. Dr.C.S.Kulkarni
3. Clinical Surgery By. S.Das4. Short practice of Surgery By. Bailey and
Love5. Atlas of Orthopaedic Anatomy By. Frank
H. Netter6. Seminar Report. AVS7. Susruta Samhita Cikitsa Staana8. Ashtaanga Hrdayam
How to Prevent back ache:
1. Maintain your weight/height ratio with in normal limits.2. Do regular exercise. Avoid continuous sitting for more than one
hour.3. Avoid lifting over weight, loads.4. Keep good posture while sitting and standing while sitting use back
support always.5. Do Abhyangam regularly
DARSHAN 08
11
treatment offered in each individual cases.In future the processing of data may helpin better clinical performance, researchactivities and business purposes.Consequently Clinical Research Wing,Aluva Hospital had developed a protocol for
this purpose named ElementaryAssessment form on Clinicalmanagement. This assessment format isgoing to be implemented at Aluva hospitalfrom 01/04/2008on a trial run.
Clinical News
(Contd. from page 30)

Case 1
One male patient 38 yrs came to KeralaAyurveda Hospital, Kasargode with severepain on Low back region. The pain startedwhile lifting weight. He was working in UAE.He was suffering from severe pain. He couldnot walk without support. There was severeback pain while coughing and sneezing. He wasadmitted in a hospital at UAE for IP Allopathictreatment care. But pain didn’t subside after10 days. So he approached me. MRI reportsuggests L4-L5 IVDP. The patient wasadmitted. O/E-SLR positive. He couldn’tmove both legs mainly right leg. On the firstday I gave him Patrapodala svedam withSahacaaradi Tailam & Myaxyl oil. The sameday evening Kadeevasty was also done.Lumbar Traction with 2kg+2kg weight wasalso done. The same day evening he gotremarkable changes. He got considerablerelief in pain and could move his leg. Icontinued the treatment. With in 7 days hegot 90 % relief. He could walk. SLR becamenegative. Virecana with Avipaty coornamwas done on the last day. I advised him tocontinue medicines for 3 months.
Medicines used were
. Gandharva hastaadi Kashaayam
. Dhanvantaram Gulika
. Balaarishtam
. Gandha Tailam 5 drops twice daily withmilk
Case 2
A 28 year old female patient came to me withalmost same symptoms as that of case 1. Thepatient was lean and her body wt.34 kg.
MY PRACTICE - MEMORABLE CASES IN LOW BACK ACHE
(These cases were presented by Dr. Sreeraj.I.P. in Darshan 08 held on March 4th)
Before approaching me she had takenAllopathic Treatment and got temporaryrelief.O/E-SLR found positivePatrapodala svedam done. Lumbar tractionwith 1.5kg +1.5 kg done.I tried to do Kadeevasty, but she couldn’t lieon prone position at least for two minutes. Forthe first 3 days there were no remarkablechanges. On the 3rd day I started Matravastywith Dhanvantara Sevyam +Gandharvahastaadi Erandam (30ml+30ml).On the same day evening she got some relief.I decided to administer Yogavasty in thatpatient. Subsequently I have completed thesame. Maadhutailikam was selected as theKashaayavasty. After this Njavara Kizhi wasapplied for three days. Traction was given onall days. On the 10th day she was discharged.Almost all symptoms were reducedconsiderably and SLR became negative.
Medicines used were. Sahacaraadi Kashaayam. Balaarishtam + Asvagandhaarishtam. Yogaraajaguggulu gulika 1—-0—-1. Gandha Tailam 5 drops twice a day with
milk.. Trvrut Lehyam at bed time.. Asvagandhaadi Lehyam 2 tsp twice daily.
Case No.3
Here I remember one female Patient who wasat her eighties, from Asok Nagar Kasaragod.Her family members brought her to ourhospital. Previously she was admitted in anearby Allopathic Hospital for 5 days. She hadvery severe pain on Low back region, radiatingpain to both hip region and legs. They said she
DARSHAN 08
12
Memorable Cases

developed severe pain after a fall. Even ifAllopathic treatment was taken pain persistedand she couldn’t walk. There she was giventreatment for IVDP–Traction PhysioTherapy etc. After examining the patient Isuggested to take an X-ray of lower spine. Butdue to severe pain, we failed to move her tothe imaging centre. Kaadidhaara done on the1st day and Balm Myaxyl was used for externalapplication. She got some relief. But the next
day also she had severe pain. I again insistedto do X-ray, routine blood and urineexamination. In the X-ray there were so manypatches in and hip bone vertebrae. ESR was154 mm/hr, Hb-6 mg%. Urine-Bence JonesProtein +ve. It was a case of MultipleMyeloma. I told the bystander about hercondition and referred her to Medical CollegeMangalore.
DARSHAN 08
13
peril of the patient it was having a psychicfactor involved. I tried to assess thepsychological status of the patient. On doingso I was fairly confident that the girl is a bitshowy or even hysteric and the inability towalk is just a subconscious trick to attractattention of the loving relatives. I wanted toprovide psychologic assistance to the patient.For this I had to prove that she can walk, ifshe realy wanted to do so. I made the girlstand up on the floor. This she was able to dowith support under shoulder from tworelatives. I insisted that the support shouldbe withdrawn. The relatives hesitated a bitand the patient beggd me not to do so. Butyou know, I am a committed physician andonce I decided to do something, I did it. Thesupport was withdrawn. Oh! She was able tostand without support. I considered this as amark of my success. I have proved that thepatient could stand without support. But thepatient was in pain and tears rolled down hercheek as though she is suffering fromexcruciating pain. This I considered to be anact of the malicious mind of the patient sinceI was convinced that the patient is showy. Iordered her to walk. She walked a few stepsyelled and fell down. The byestanders
interfered in time and captured her so thatthe fall was promptly checked. She was takenback to her cot on arm cradle. In the eveningthere was swelling and redness of both theankles! I was wrong. She was cent percentcorrect. There is now organic evidence of herpain. She was a patient of rheumatoid disease.When I recapitulate the case, I regretmy obstinacy and I shrink of shyness.I was rather inhuman and brutal ininsisting that the patient should walkbefore me. I could have simply believedthe words of the patient.What would have I lost if I believed her wordsand put her on therapy for pain? Nothing!Instead I insisted on evidence. It was a casewhich taught me a valuable lesson. I learnedto believe the patient, as far as possible. Theincident taught me that I should not beoversmart and I should have more humilityin regarding the patients. But believing thepatient also may be risky. (That may bediscussed in a later issue.) So the doctorshould have discriminative intelligence in believing the patient. In mostcases it is wise to believe them, if youhave no reason to believe that there ismalicious motive.
Frankly speaking(Contd. from page 4)
Memorable Cases

(Dr. Jacob Jayan.B. BAMS, MBBS, MD, Dip.GM (Geri.Med) had done a presentation onthe modern clinical approaches in back pain in Darshan 2008 held on March 4th. Due to spacelimitations we are able to publish only the summary of the presented paper. )
BACK PAIN- CLINICAL APPROACH
Causes
• C o n g e n i t a l / D e v e l o p m e n t a l :Spondylolysis/listhesis, kyphoscoliosis,spinabifida occulta, teathered cord
• Traumatic: Strain/sprain–Falls/RTA,IVDP
• Atraumatic: Osteoporosis, Neoplasticdiseases, Steroid use, IVDP
• Neoplastic: Metastatic,hematologic,Primary bone tumors.
• Arthritis: Spondylosis,Facet/Sacroiliacarthropathy & Autoimmune (Ankylosingspondylitis, Reiters syndrome)
• Degenerative: Disk osteophyte complex,internal disk disruption, spinal canalstenosis with neurogenic claudication.
• Infection/Inflammation: Vertebralosteomyelitis, Spinal epidural abscess,septic disc, menigitis, lumbar arachnoiditis.
• Metabolic: Osteoporosis-Hyperparathyroidism, Immobility &Osteosclerosis (Paget’s disease)
Other causes:
1. Referred pain from other visceraldisease.
2. Postural.3. Psychiatric – Malingering, chronic pain
syndrome.4. Abdominal aortic dissection.
Back pain- Evaluation
• “It is important to know as much aboutthe man who has the pain as it is to knowabout the pain the man has.” - Great GreekPhysicians
Back pain is
• A symptom not a disease.
• A common problem affects both sex andall ages.
• The final common pathway of manyprocesses.
• The pathologic basis may be within oroutside spine.
“Seek facts and classify them and you willbe the workmen of the science.”
- Nicholas Maurice Arthus.
Classification
• Spondylogenic – pain from spinal columnand associated structures.
• Neurogenic – Pain from nerve roots dueto compression irritation or tension andmay radiate.
• Viscerogenic – Pain derived fromdisorders of visceral organs.
• Vascular – Regional vascular problems(aneurysms, POVD etc) pain may mimicneurogenic pain.
• Psychogenic – Though rare it is notuncommon. No organic cause can belocated. Clouding and confusion of clinicalpicture by emotional overtones.
DARSHAN 08
14

Pain: An unpleasant sensory and emotionalexperience, associated with actual orpotential tissue damage, or described in termsof such damage.
• Local pain.• Pain referred to the back.• Pain of spinal origin.• Radicular pain origin.• Pain associated with muscle spasm.• Pain at rest.• Postural pain
Pain Sharp, Cramp Vague, Radicular
Location Exercised Radicular/Diffusemuscle
Radiation Rare after onset Very Commonproximal to distal
Aggravation Walking (up) Walk or stand
Relief Stop Activities Lying/Sitting(rest) Quick Slow ReliefRelief
Focal NeurologicalDeficit Not seen Usually seen
Pulse Absent Present
SLR Negative May + ve /- ve
Examination of the back
• Abdomen, rectum, costo-vertebralangles
• Spine-curvatures
• Para spinal muscles
• Hip movements
• SLR test
• Neurological / Vascular
• Pelvic examination
*It is highly important to differentiateclaudication of vascular origin from that ofNeurogenic origin
Diagnostic criteria for AcuteRadicular Syndrome (ARS)
Acute Lumbosacral radicular syndrome(LRS) is defined as pain, radiating from theback into the leg to below the knee, incombination with either Lassegue’s sign, orwith segmental disorder characterized byparesis, sensory disorders and/or changes inreflexes reducible to a single nerve root. It is
most commonly caused by protrusion of a lowlumbar intervertebral disc.
• Leg pain including buttock is dominant tothat of LBA.
• Neurologic symptoms seen(parasthesiain dermatomes)
• Significant SLR changes.• SLR<50% of normal• Bowstring discomfort• Crossover pain• Focal Neurological Deficit
CLAUDICATION
Features Vascular Neurogenic
DARSHAN 08
15

Cauda equina syndrome (BilateralARS)
Even though low back pain is common andusually subsides without surgery, caudaequine syndrome, a rare disorder affecting thebundle of nerve roots (cauda equina) at thelower (lumbar) end of the spinal cord, is asurgical emergency. Cauda equina syndrome
occurs when the nerve roots are compressedand paralyzed, cutting off sensation andmovement. Nerve roots that control thefunction of the bladder and bowel areespecially vulnerable to damage.
• Back pain (sudden worsening)
• B/L leg pain
• Saddle anesthesia
• B/L lower extremity weakness
• Bowel, bladder involvement
* Emergency MRI for diagnosis and Surgicaldecompression are unavoidable in themanagement of A/c Compression at L3-L4,L4-L5 /L5-S1Back pain- patterns
• Juveniles & adolescents (10-20yrs) –Infection, tumor, scheuermann’s d/s,spondylolysis.
• Y o u n g a d u l t s ( 2 0 - 4 0 y r s ) - S p o n d yloarthropathy, fracture(trauma)
• Middle age(35-70yrs) - Degenerative discdiseases
• Elderly (65 - 85yrs) - Compressionfracture, tumor, infection
Conclusion
• LBA common problem• DD are broad• Precise diagnosis is not very easy• Identify patients who require more/
urgent detailed evaluation• Differentiate infection/cancer/
inflammation/degeneration with ARSand vascular.
• Conservative management needed inmajority.
“Physicians think that they do a lot for apatient when they give his disease a name”-IMMANUEL KANT.
FeaturesAffected nerve roots
L4 L5 S1
Motor weakness Knee extension Ankle dorsi Ankle plantarflexion flexion
Sensory loss Middle shin toknee
Dorsum of footand lateral calfregion
Lateral borderof feet and posterior calfregion
Reflexes Knee jerk- diminished
Ankle jerk-diminished
Ankle jerk-diminished
Wasting ThighTibialisposterior andCalf, Minimumin thigh
Calf, Minimumin thigh
Common neurological changes in ARS
DARSHAN 08
16

Chronobiology is the study of biologic rhythmand their underlying mechanisms. Manynormal human biologic functions exhibitpredictable cyclic patterns or rhythms thatcan be defined in terms of specificcharacteristics (cyclic length) and amplitude(peak trough ratio). A daily reproduciblepattern of peak and troughs is seen in manyphysiologic variables. A well known exampleis the secretion of growth hormone. It will bein its peak during sleep. Levels of plasmatestosterone and the cortisol which typicallypeaks at the early morning are otherexamples.
Human body have a built in 24 hours cycleknown as Circadian rhythm. Researchers havestarted to realize that these natural rhythmsalso apply to medical conditions and haveimplications for treatment. When a medicineis administered in a particular time, theefficacy of the medicine will be more.
So keeping the goal to match the timing of thetreatment with the intrinsic timing of illnesswould be clinically significant. Theoreticallyoptimum therapy is more likely to result whenthe right amount of drug is delivered to thecorrect target organ at the most appropriatetime. In contrast many side effects can beminimized if a drug is not given when it is notneeded. The above said principles bear somesimilarity with the Ayurvedic principles. Ithought it would be worthwhile if I could applythis principle to verify the directions regardingtimes of usage of drugs (OushadhopayogaKaalam) in classical Ayurvedic texts.
Incidentally I found some interesting factsabout Galaganda. Vaagbhataacaarya hasexplained types of galaganda. In kaphaja
AN EXPLORATION ON OUSHADHOPAYOGAKAALAMDr.Sandeep.K.M
Physician Kerala Ayurveda
galaganda he says there will be increase inthe body weight, Ghurghurata - hoarsenessof voice and Krchra vaakyata - difficult tospeak. While explaining the Kaphaja disordersSaarangadhara point out the followingsymptoms; Thandra - drowsiness, atinidrata- disturbed sleep, gaurava – feeling ofheaviness, saitya - cold feeling, aalasya -laziness, manda budhitva – reducedintelligence acetana - loss of concentrationand swinging of mood, Ghurghurata -hoarseness of voice, avakyata-difficult tospeak.
An eager team of physicians including mecorrelated these to Hypothyroidism. Weworked out on the possibility of when therewill be increase in kapha. It is said thatmorning is the kapha kaala and in morningand cold hours there will be increased secretionof TSH and T4 levels.
“Madhura snighdha seetaadi bhojyairdivasa nidraya.
Mande agnau ca prabhate ca bhuktamatre tathaa sramaat
Sleshma prakopam yatyebhipratyaneekaisca saamyathi.”
Sha 2/35.
Also Kapha attains Prakopa
. By intake of sweet, oily, fatty, coldfood items
. By day sleep
. Physical inactivity
. In the morning and immediately after themeals.
It is said that in kaphaja diseases oushadhahas to be given in morning before the food.
17

“Kaphodrake gade annam pratha: “AH 21
Saarngadhara also says that in diseases ofkapha and pitta and for purpose of vamana,virecana and lekhana medicines should begiven in the morning.
“praya: pitta kaphodraeke virekavamanarthayo:
Lekhanartham ca bhaishajyam prabhathethat samaharet”
Sh 2/3
And also in Kaanjcanaara Yoga preparationits indication and time of administration isexplained as he says … KaanjcanaaraGuggulu has to be given in morning time.
Kaanjcanaara tvaco graahyam palaanaamdasakam budhai:
………….Gudika saana maatrena praatargraahya
yathocitamGandamaalanaam jayati atyugram apaci
arbudaani caSh 4/15-129.
Consequently we the group of doctors made aclinical assessment on cases of Kaphajagalaganda correlated to hypothyroidism. Westudied the efficacy of administeringKaanjcanaara Guggulu in morning time onempty stomach against administering it afterfood.
Considering all the above factors weconcluded that for kapha roga and forlekhanaartha the administration ofKaanjcanaara Guggulu in the morning andbefore break fast would be the most effectiveas far as time of administration is concerned.To reestablish the above principles we havedivided the patients into 2 groups. And for onegroup we have given treatment according tothe Oushadhopayoga kaalam, as mentionedabove. In the second group, we have givenKaanjcanaara Guggulu after food we haveconducted the study only in a limited no ofpatients, but the outcome was well along thelines of the classical Oushadhopayogakaalam. See the tables given below.
Drug given inGroup I (Early morning and Empty stomach)
No of Age Sex Treatment Initial Interim FinalPatients duration Value Value ValueP I 45 yrs F 12 weeks T3 - 1.6 1.8 1.8
T4 - 7.0 6.8 7.0TSH - 6.9 6.6 6.6
P II 26 yrs F 5 weeks T3 - 0.6 — 0.9T4 - 4.2 — 4.8TSH - 10.2 — 10.0
P III 34 yrs F 8 weeks T3 - 0.9 3.2 13.5T4 - 0.8 3.6 10.2TSH - 0.8 3.7 10.0
P IV 22 yrs F 5 weeks T3 - 1.1 — 1.2T4 - 5.2 — 5.5TSH - 11.0 — 10.6
[* T3-ng/dl, T4-µg/dl, TSH-mIU/L]
18
(Contd. on page 32 )

Aphrodisiac
Aphrodisiac was named after Aphrodite, theGreek goddess of sexual love, beauty andfruitfulness identified in Roman Mythologywith the goddess Venus, who was thedaughter of Zeus and Dione. However, theGreek word ‘aphros’ means ‘foam’ andaccording to the tradition recounted byHesoid, Aphrodite arose from the foamgenerated when the severed genitals ofUranius personification of Heavens werethrown into the sea. Several ancientauthorities agreed that she was the wife of thelame blacksmith, Hephaestus. An aphrodisiaccan therefore be described as any substancethat enhances sex drive and or sexualpleasure. The Kama Sutra suggested that oneboils the testicle of a ram or goat and add milkand sugar before consumption. In England, itwas believed that plants with any phallic-likefeatures such as asparagus, parsnips andcarrots were likely to be aphrodisiac in theireffect. Ukrainians celebrate carrots and celeryas folk aphrodisiac. In Chinese culture, muchof the aphrodisiac power of ginseng andrhinoceros horn comes from their appearancerather than their chemical composition.Sexual dysfunction, that is the repeatedinability to achieve normal sexual intercourse,which include various forms like prematureejaculation, retrograded, retarded orinhibited ejaculation, erectile dysfunction,arousal difficulties (reduced libido),compulsive sexual behaviour, orgasmicdisorder and failure of detumescence are on
MALE SEXUAL DYSFUNCTION AND MEDICINAL PLANTS WITHAPHRODISIAC POTENTIALS
Mr. Bose R. C., Dr. Sarala Samuel, Dr. C. I. JollyR&D, Kerala Ayurveda
the increase world wide, because of agingpopulation and other increasing etiologicalfactorsOne of the main aims of marriage is theprocreation (reproduction) and moreimportantly for sexual fulfillment of bothpartners. For life to continue, an organismmust reproduce itself before it dies. In Homosapiens, reproduction is initiated by themating of a male with a female in sexualintercourse which facilitates the comingtogether of sperm and egg for the purpose offertilization, for there to be a normal sexualintercourse and sexual fulfillment in males,the male sexual organs (the copulatory organ,the penis) and factors relating to erection mustfunction normally. Inability to perform thisfunction effectively is a major problem facingthe reproductive process. This is known assexual dysfunction
Aphrodisiac can also be viewed as any food,drug, scent or device that can arouse orincrease sexual drive or libido.
Male sexual function
Sexuality is a complex, multi-dimensionalphenomenon that incorporates biological,psychological, interpersonal and behaviouraldimensions. For better sex, a person shouldhave good balanced hormone, physicalcondition, mental condition, and neuronalfunction.
19

Male Sexual act
Control of Male sexual function byhormones;A major share of the control of sexualfunctions in both the male and the femalebegins with secretion of gonadotropin –releasing hormone (GnRH) by thehypothalamus. This hormone in turnstimulates the anterior pituitary gland tosecrete two other hormones calledGonadotropic hormones (luteinizinghormones (LH) and Follicle stimulatinghormones). The LH is the primary stimulusfor the secretion of testosterone by the testisand FSH is mainly for the production of newsperm cells.
Neuronal stimulus to perform themale sexual actThe most important source of sensory nervesignals for initiating the male sexual act is the
glans penis. The glans contains a specialsensitive sensory end organ system thattransmits into the central nervous system.The erection is triggered and controlled by thevarious events. Impulses may also enter thespinal cord from areas adjacent to the penisto aid in stimulating the sexual act.
Emission and Ejaculation-Function ofthe Sympathetic Nerves.
Emission and ejaculation are the culminationof the male sexual act. When the sexualstimulus becomes extremely intense, thereflex centers of the spinal cord begin to emitsympathetic impulses that leave the cord andpass to the genital organs through the nerveplexuses to initiate emission, the forerunnerof ejaculation.
20

Emission begins with contraction of the vasdeferens and the ampulla to cause expulsionof sperm into the internal urethra. Then,contractions of the muscular coat of theprostate gland followed by contraction of theseminal vesicles expel prostatic and seminalfluid also into the urethra, forcing the spermforward. All these fluids mix in the internalurethra with mucus already secreted by thebulbourethral glands to form the semen. Theprocess up to this point is emission.
Possible cause of Impotency
Many common medicines produce impotenceas a side effect. These include high bloodpressure drugs, antihistamines,antidepressants, tranquilizers, appetitesuppressants, and cimetidine (an ulcer drug).
It is believed that psychological factors cause10 to 20 percent of cases of impotence. Thesefactors include stress, anxiety, guilt,depression, low self-esteem, and fear ofsexual failure. Such factors are broadlyassociated with more than 80 percent of casesof impotence, usually as secondary reactionsto physical causes.
Other possible causes of impotence aresmoking, which affects blood flow in veins andarteries, and hormonal abnormalities, such asinsufficient testosterone.The normal male sexual response cycle canbe functionally divided into five interrelatedevents that occur in a defined sequence:libido, erection,ejaculation,orgasm, and detumescence.
1. Libido or sexual desire- Libido isdefined as the biological need for sexualactivity (the sex drive) and frequently isexpressed as sex-seeking behaviour. Itsintensity is variable between individuals aswell as within an individual over a given time.Higher serum testosterone appears to be
associated with greater sexual activity inhealthy older but not younger men.
2. Erection- Erection is the enlarged andrigid state of the sexually aroused penissufficient enough for vaginal penetration. Itresults from multiple psychogenic andsensory stimuli arising from imaginative,visual, auditory, olfactory, gustatory, tactile,and genital reflexogenic sources.
3. Ejaculation- Ejaculation is the act ofejecting semen. It is a reflex action that occursas a result of sexual stimulation. It is made upof two sequential processes. The first processcalled emission is associated with depositionof seminal fluid into the posterior urethrawhile the second process is the trueejaculation, which is the expulsion of theseminal fluid from the posterior urethrathrough the penile meatus.
4. Orgasm- This is the climax of sexualexcitement. The entire period of emission andejaculation is known as the male orgasm.
5. Detumescence- This is the subsidenceof an erect penis after ejaculation.
Male sexual dysfunction
Sex disorders of the male are classified intodisorders of sexual function, sexualorientation, and sexual behaviour. In general,several factors must work in harmony tomaintain normal sexual function. Such factorsinclude neural activity, vascular events,intracavernosal nitric oxide system andandrogens. Thus, malfunctioning of at leastone of these could lead to sexual dysfunctionof any kind. Sexual dysfunction in men refersto repeated inability to achieve normal sexualintercourse. It can also be viewed as disordersthat interfere with a full sexual response cycle.These disorders make it difficult for a personto enjoy or to have sexual intercourse. Whilesexual dysfunction rarely threatens physical
21

health, it can take a heavy psychological toll,bringing on depression, anxiety, anddebilitating feelings of inadequacy.Unfortunately, it is a problem often neglectedby the health care team who strive more withthe technical and more medically manageableaspects of the patient’s illness. Sexualdysfunction is more prevalent in males thanin females and thus, it is conventional to focusmore on male sexual difficulties. It has beendiscovered that men between 17 and 96 yearsold could suffer sexual dysfunction as a resultof psychological or physical health problems.
Sexual dysfunction takes different forms inmen. A dysfunction can be life-long andalways present, acquired, situational, orgeneralized, occurring despite the situation.A man may have a sexual problem if he:
Ejaculates before he or his partner desiresDoes not ejaculate, or experiences delayedejaculationIs unable to have an erection sufficient forpleasurable intercourseFeels pains during intercourseLacks or loses sexual desire.
Male sexual dysfunction can be categorizedas disorders of desire, disorders of orgasm,erectile dysfunction, disorders of ejaculationand failure of detumescence.
A. Disorders of desire: Disorders of desirecan involve either a deficient or compulsivedesire for sexual activity.
B. Erectile dysfunction (ED): This is aproblem with sexual arousal. ED can bedefined as the difficulty in achieving ormaintaining an erection sufficient for sexualactivity or penetration, at least 50% of thetime, for a period of six months
C. Disorders of ejaculation: There existsa spectrum of disorders of ejaculation ranging
from mild premature to severely retarded orabsent ejaculation.
D. Disorders of orgasm: Male orgasmicdisorder is defined as a persistent or recurrentdelay in, or absence of orgasm after a normalsexual excitement phase during sexualactivity.
E. Failure of detumescence: is aprolonged erection usually lasting for between4 h or greater. It is painful and alwaysunaccompanied by sexual desire despite thefact that it is often preceded by usual sexualstimuli.
General Methods used in AssessingAphrodisiac PropertiesA. Physical Methods
1. Mating Behaviour TestI. Mount frequencyII. Intromission frequencyIII.Mount latencyIV. Intromission latencyV. Ejaculatory latencyVI. Post-ejaculatory intervalVII. Index of libido2. Test for libido3. Test for potency4. Penile microcirculation study5. Intracavernous Pressure (ICP)
Study
B. Biochemical Methods
1. Determination of Testicular andSerum Cholesterol
2. Hormonal Determination3. Assay for Neuronal Nitric Oxide
Synthase and Androgen ReceptorProtein
Sexual function is an important component ofquality of life and subjective well being inhumans. Sexual problems are widespread andadversely affect mood, well being, and
22

interpersonal functioning. Sexual problemsare related to sexual desire and male erectiledysfunction. Successful treatment of sexualdysfunction may improve not only sexualrelationships, but also the overall quality oflife.
Treatments Available
Vasoactive injection, Sex Therapy, OralMedication Viagra, Yohimbine, Self-Injection& Urethral suppositories containingprostaglandin, Vacuum Devices, SurgicalTreatments, Penile Implants, VascularReconstructive Surgery, Naturopathic
(Natural) Treatment, Herbal Medicine,psychotherapy and Yoga.
AJAX
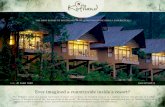
Ajax is a unique formulation of herbalcombination of highest quality introduced bythe department of Kerala Ayurveda Ltd. Thisis one of a kind, potent and extraordinarilyeffective natural sex enhancer which helps toincrease libido and sexual desire and worksas a powerful male sex stimulant. This ignitesthe passion, love and romance in ones life andhelps to achieve new levels of erotic intimacyand emotional closeness in the relationships.
Benefits• Improves Vigour and virility in male• Prevents Premature ejaculation• It helps to restore potency and Increase Libido• Helps to Make more Sustained erections• Increase Sexual desire
23
SN Ingredients Sanskrit Hindi Malayalam Qty
1 Curculigo orchioides Musli Musli Musli 100 mg
2 Astercantha
longifolia Kokilaksha Talimakhava Vayalchulli 100 mg
3 Mucuna pruriens Atmagupta Kaunch Naykkorna 100 mg
4 Tribulus terrestris Gokshura Gokharu Nerinnil 100 mg
5 Withania somnifera Aswagandha Asgandh Amukkuram 50 mg
6 Yasadha bhasmam Yasadha Yasadha 30mg
bhasmam bhasmam
Your valuable responses can be sent to us either in our postal address or in e-mail.
Kerala Ayurveda News & Views
Kerala Ayurveda HospitalBank RoadAluva-01Tel : 0484-3221365, 2626119, 2623578E-mail : [email protected]

In recent years science has madebreakthroughs in the understanding of sexualdysfunction. But, for hundreds of years,civilizations around the world have knownabout locally grown herbs that achievewonderful results with far fewer side effectsthan prescription drugs. One such plant, whichclaims various medicinal properties is Mucunapruriens Linn. belonging to the botanicalfamily Leguminoseae. It is one of the popularand important medicinal plants of India. It isa constituent of more than 200 indigenousdrug formulations. The plant is an importantcover crop (or green manure crop) in manyparts of the world, especially amongsubsistence farmers. .
MUCUNA OR COWHAGEDr.Sarala Samuel, Dr.C.I.Jolly andRemya.M.B.
R&D, Kerala Ayurveda
Where is it found?
It is indigenous to tropical regions, especiallyAfrica, India, and the West Indies. It is widelyspread over most of the subcontinent and isfound in bushes, hedges, and dry-deciduous,low forests throughout the plains of India.In India, 14 species of Mucuna are found inthe foothills of the Himalayas, the plains ofwest Bengal, Madhya Pradesh, Karnataka,Kerala, Andhra Pradesh, Uttar Pradesh, theAndaman & Nicobar islands and Srilanka .
How does it look like?
Cowhage or Velvet bean (Mucuna pruriens)is an annual herbaceous twining, climbinglegume with long, thin branches and opposite,trifoliolate, lanceolate leaves 15 to 30 cmlength. Leaflets are broadly ovate, elliptic orrhomboid ovate, unequal at base. Its flowersare white to dark purple and hang in longclusters or pendulous racemes. The fruit ofthe plant is a pod, which is thick and leathery.It is covered with reddish-orange colouredlong stiff hairs that are readily dislodged andresponsible for itching in workers involved incollection of the plant. The species name‘pruriens’ (from Latin, “itching sensation”)refers to the results from contact with theseedpod hairs. Pods curved, 5-10 cm x 1.5-1.8 cm, longitudinally ribbed, turgid, denselyclothed with persistent pale brown or gray,irritant bristles. Seeds, known as Mucunabeans are black, 4-6 in a pod, hilum ovoid (6-12 mm long) with funicular hilum.
What does it contains?
The plant is reported to have L-Dopa as amajor constituent mainly in seeds. Alkaloidalconstituents viz., mucunadine, mucunine,
This plant is widely used in Ayurveda, whichis the ancient traditional medicinal system inIndia. All parts of Mucuna pruriens possessvaluable medicinal properties and there is aheavy demand of Mucuna in Indian andInternational drug markets.
24

prurienidine, prurienine are reported fromseeds. Numbers of amino acids are reportedfrom this plant. Epoxy fatty acids viz., cis-12,13- epoxyoctadec-trans-9-cis-acid, cis-12,13-epoxyoctadectrans-
9-enoic acids are reported. Lecithin isreported to be present in seed. According toDr. Duke’s phytochemical and ethnobotanicaldatabases Mucuna pruriens contains manydiverse phytochemicals like 1-methyl-3-carboxy-6,7-dihydroxy-1,2,3,4-tetrahydroisoquinolone,5-hydroxy tryptamine,5-methoxy-n,n-dimethyltryptamine-noxide, 5-oxyindole-3-alkylamine, 6-methoxyharman,alanine, arachidic acid, arginine, aspartic acid,
behenic acid, H-carboline, H -sitosterol,bufotenine, choline, cystine, leucine, linoleic acid, myristic acid, n,ndimethyltryptamine,n,n-dimethyltry ptamine-n-oxide, nicotine, oleicacid, palmitic acid, palmitoleic acid,phenylalanine, phosphorus, proline, protein,saponins, serine, stearic acid, threonine,tryptamine, tyrodine, valine and vernolic acid. Recently three new lipid derivatives werereported from n-hexane extract of seeds ofMucuna pruriens, namely (Z)-Triactont-5,7,9- triene; (Z)-Docos-2,4,6-trien-1,8-dioland (Z)-Docos-5- en-1-oic acid. Misra andWagner reported isolation of four 1,2,3,4 tetrahydroisoquinoline alkaloids from the seed.
Ayurvedic Properties and Uses:Seeds of the mucuna are usually prescribedin the Indian traditional system of medicine,especially in Ayurveda, for sexual andnervous diseases. Seeds has a long history ofuse in Ayurvedic medicine, where it is used
for worms, dysentery, diarrhea, snakebite,sexual debility, cough, tuberculosis,impotence, rheumatic disorders, muscularpain, gonorrhea, sterility, gout, delirium,dysmenorrhea, diabetes, and cancer. In India,it is considered as an aphrodisiac,
25

emmenagogue, uterine stimulant, nervetonic, diuretic, and blood purifier. Seeds areastringent, laxative, anthelmintic, aphrodisiac,alexipharmic and tonic. They are useful ingonorrhoea, sterility, vitiated conditions ofvaata and general debility.Mucuna pruriens can improve sexualbehavior, libido, and performance. Mucunapruriens when administered in a dose of 75mg/kg body weight daily increased the sexualactivity of male albino rats considerably bystimulating testosterone level. A ten foldincrease in the mounting frequency wasobserved. Research shows that sexuallyactive animals had increased sexual desire andimproved sexual performance after 21 to 28days. However, impotent animals did notderived any benefits.(AminKMY)Another research shows that Mucunapruriens heightened arousal and increasedsexual activity to a moderate extent but alsosustains it for a longer time as indicated bythe increase in below Ejaculation Latency anddecrease in Post Ejaculatory Interval. Mucunaprueins is shown to possess central depressantactivity. The delay in ejaculation could be dueto toning down of hypersensitity of genitalsand hyperexcitation of the regulatory centers.This study show that Mucuna pruriens canbe used to improve libido and delaypremature ejaculation ( Giuliano F).
The traditional aphrodisiac property of thisplant is scientifically analyzed and proved byseveral experiments using seeds of M.pruriens. According to the studies of Amin etal , Mucuna pruriens stimulates sexualfunction in normal male rats which wasobserved by increase in mounting frequency,intromission frequency and ejaculationlatency where as, Rajendran et al proved thedecrease in sexual function in female rats.How to grow it in your garden?Velvet bean is a minor leguminous crop, manycultivars of which are suitable for the more
humid regions of the tropics, while others, e.g.the Mauritius velvet bean, are suitable for dryland farming. They can be grown successfullyon soils unsuitable for cowpeas, but have thedisadvantage of a longer growth period andare more difficult to thresh. Moreover, the seedis not highly valued for human or animalfeeding, because of the prolonged soaking and,or, boiling required before it can be consumedsafely. The leaves and vines make an excellentfodder. Velvet beans are frequently grown mixed withother vigorous growing crops such assugarcane or maize. They are also grown as agreen manure or cover crop and are
particularly valuable as an anti-erosion crop.In India the wild species is often used as acover crop in coconut plantations. When grownas a mixed crop with cereals, such as maize ormillet, it is usual to plant every alternate orthird row with velvet beans.
For optimum results the seedbed should bewell prepared to a depth of at least 15 cm andcompletely free from weeds. Little is knownof the crop’s precise requirements, but itresponds to applications of phosphate.
Harvest: When grown for seed the crops canbe harvested approximately 180 to 270 daysafter planting. When grown for forage, theplants are usually harvested between 90 and120 days after sowing. The pods should bethoroughly ripe before being harvested. Asthey are liable to shatter, they are often hand-picked and are usually left to dry for severaldays before being threshed. Threshing can becarried out by hand or machine, butwhichever method is used only fully mature,dry pods can be threshed without difficulty.
PropagationMultiplication: Seeds are used, germination ishypogeal and usually occurs within 5-7 days,with a rate of between 90-95%. Inoculationof the seed is not usually necessary if velvet
26

beans are grown in areas where the cowpeahas been cultivated, otherwise inoculationwith a commercial cowpea inoculum may benecessary.Planting: When grown for the production ofseed, planting is usually in rows, but whengrown as a fodder or green manure crop, theseeds are often broadcast. Adapted maizeplanters with thick plates and enlarged holesare sometimes used for planting in countriessuch as USA, S. Africa and Australia. In Asiathe crop normally receives little attention, butthe suppression of weeds during the earlystages of growth and the provision of supportsfor the vines to climb is beneficial. Whengrown for seed, velvet beans are frequentlyplanted in rows 90-180 cm apart, with 15-90cm between the plants. In India the averageseed-rate is reported to vary between 28-50kg/ha, in most other countries it normallyvaries from 11-22 kg/ha, when the crop isplanted in rows, and from 45-90 kg/ha whenbroadcast.
What are the vernacular names?
It is referred to as Aatmagupta/Kapikachuin Sanskrit. Gonca is the Hindi name. InSouth Indian languages it is known asPunaikkali, pillaidugu or Masuganni. InMalayalam it is commonly known asNaykkurana and in English it is commonlycalled as cowhage or velvetbeanForklore Uses:. In Central America, velvet beans have
been roasted and ground to make a coffeesubstitute for decades; its goes by thecommon name of “nescafé” in theseregions, as well as in Brazil, for this reason.
. It is still grown as a food crop by theKetchi indigenous people in Guatemala;the bean is cooked as a vegetable.
. In Brazil the seed has been used internallyfor Parkinson’s disease, edema,impotence, intestinal gas, and worms. It
is considered a diuretic, nerve tonic, andaphrodisiac. Externally it is applied toulcers.
. Velvet bean has a long history of use inIndian Ayurvedic medicine, where it isused for cancer, catarrh, cholera, cough,debility, delerium, diabetes, diarrhea,diuretic, dysentery, edema, fertility, gout,impotency, kidney stones, menstrualdisorders, nervousness, scorpion sting,snakebite, sterility, tuberculosis, worms,and as an aphrodisiac and uterinestimulant
REFERENCES1. D. Buckles. Velvet bean(Mucuna pruriens)
: A “new” plant with a history.Economic Botany 49(1): 13-25 (1995).
2. J.F. Caius. The medicinal and poisonouslegumes of India, (Scientific Publishers,Jodhpur, 1989) pp. 70-71.
3. The Wealth of India. Raw materials Vol.6, (CSIR, New Delhi, 1985) pp. 442.
4. P.K. Warrier, Nambiar and Ramakutty.Indian medicinal plants-a compendium of500species, Vol. 4, (Orient Longman Ltd,Madras, 1995) pp. 68-72.
5. R.P. Rastogi and B.N. Mehrotra.Compendium of Indian medicinal plants,Vol.5,(CDRI, Lucknow, 1994) pp.554.
6. A.A. Farooqi, B.S. Sree Ramu. Cultivationof medicinal and aromatic crops,(Universities Press, New Delhi, 2001)pp.74.
7. S. P. Agharkar. Medicinal plants ofBombay presidency, (Scientificpublishers,Jodhpur, 1991) pp. 1-2.
8. Amin KMY, Khan MN, Zillur-Rehman S,et al. (1996).”Sexual function improvingeffect of Mucuna pruriens in sexuallynormal male rats”. Fitoterapia, jrg.67(nr.1): pp. 53-58. Quote: The seeds of
27

Mucuna pruriens are widely used for treatingmale sexual dysfunction in Tibb-e-Unani(Unani Medicine), the traditional systemof medicine of Indo-Pakistan sub-continent.
9. Giuliano F, Allard J. Dopamine and malesexual function. 2001. Eur Urol 40:601-608. PMID 11805404
10. Giuliano F, Allard J. Dopamine and sexualfunction. 2001. Int J Impot Res 13 Suppl3 : S 1 8 - S 2 8 . D O I 1 0 . 1 0 3 8 /sj.ijir.3900719PMID 11477488
11. C.S.T. Sastry and Y.Y. Kavathekar. Plantsfor reclamation of wastelands,(Publications and InformationDirectorate, New Delhi, 1990) pp. 317-318.
12. D.M. Verma, N. Balakrishnan and R.D.Dixit. Flora of Madhya Pradesh.(BotanicalSurvey of India, Lucknow, 1993) pp.190-191.
13. G.V. Satyavati, A.K. Gupta and N. Tandon.Medicinal Plants of India. Vol II, (IndianCouncil of Medical research, New Delhi,1987) pp. 282-289.
14. P.C. Sharma, M.B.Yelne and T.J.Dennis.Database on medicinal plants used inAyurveda. Vol 1. (Central council forResearch in Ayurveda and Siddha, NewDelhi,2000) pp. 200.
15. E.A. Bell and D.H. Janzen. Medical andecological considerations of L-Dopa and 5-HTP in seeds. Nature 229: 136-7 (1971).
16. M. Damodaran and R. Ramaswamy.Isolation of 1-3,4dihydroxyphenylalanine
from the seeds of Mucuna pruriens .Biochem. J. 31: 2149-52 (1937).
17. M.E. Daxenbichler, C.H. VanEtten, E.A.Hallinan, F.R. Earle and A.S. Barclay.Seeds as sources of L-dopa. Journal ofMedicinal Chemistry 14: 463-465 (1971).
18. J.C. Mehta and D.N. Majumdar. Indianmedicinal plants. Part V. Mucunapruriensbark. (N.O. Papilionaceae) Part I. IndianJ pharm. 6: 92-95 (1944).
19. D.K. Santra and D.N. Majumdar. TheMucuna pruriens D.C. Part II. Isolationofwater soluble alkaloids. Indian J pharm.15: 60-61 (1953).
20. D.N. Majumdar and C.D. Zalani. Mucunapruriens , D.C. Alkaloidal constituents.Part III. Isolation of water solublealkaloids and a study of their chemical andphysiological charaterisations. Indian.J.Pharm. 15: 62-65 (1953).Pharmacognosy ReviewsVol 1, Issue 1,Jan- May, 2007 PHCOG REV.An officialPublication of Phcog.Net
21. R. Pant, C. Rajagopalan Nair, K.S. Singhand G.S. Koshti. Amino acid compositionof some wild legumes. Curr Sci. 43: 235-239 (1974).
22. G.S. Niranjan and S.K. Katuyar. Chemicalcomposition of some legumes. J. Indian.Chem. Soc. 56: 822-823 (1979).
23. S.Q. Hasan, M.R.K. Sherwani, I. Ahmad,F. Ahmad and S.M. Osman. Epoxy acidsofMucuna prurita seed oil. J. Indian ChemSoc. 57(9): 920-923 (1980).
28

Kapikachu enjoys an important place amongaphrodisiac herbs in India since ancient times.Susrutha mentions the use of its seeds aspromoters of virility, as also Bhaavamisra.Yogaratnaakara has reference of its use informulations for tremors.
Kapikachu literally means one whoscratches the body like a monkey. The surfaceof pods of this climber is covered with bristles,which are allergic to skin. On touching, it givesintensive itching sensation. Hence aptly it isnamed as Kapikachu.
It is categorized as Vrshya – thesubstance that improves sexual vitality andfunctioning. Use of Kapikachu as antihelmenthic has also mentioned in older bookson traditional medium.
Synonyms of Kapikachu are ‘Makati’,‘Kauca’, ‘Aatmagupta’.
Its seed contains L-3, 4 dihydroxyphenylalanines (L-Dopa) which is found to beeffective in Parkinsonism disease. The plantextract showed marked hypotensive andhypocholestremic effect in normal rats.
PROPERTIES
• Rasa-Madhura, Tikta• Guna-Guru, Snigdha• Vipaaka-Madhura• Veerya-Ushna
USES
• Alleviates Vaata, Pitta and Kapha• Daatupushti
It is seldom used externally. Seeds arethe most tonics for impotency and forenhancing sexual vitality. It works well asrestorative for conditions of debility andweakness. It has been shown to increase thetestosterone levels, helps the deposit ofproteins in muscles and increase muscle massand strength. Its extract is known to enhancemental alertness and improve co-ordination.
• Balavardhaka• Maintains blood circulation• It is said that Kapikachu and Kokilaksha
impart very potent effect on sexualfunction, when taken with sugar andfollowed by milk. It augments the seminalfluids, vitality and vigor.
• The hot Kashaaya of the Beeja is anexcellent panacea for prematureejaculation in men seed is useful asGalactogouge in lactating mothers.
• Roots are mootrala and helps to regulatethe Aartavacakra. The Kashaaya ofmoola is beneficial for renal problem anddysuria.
• In Vaata vikaara like Ardita,Apabaahuka, Kampavaata,Pakshaaghaata etc, the decoction ofKapikachu is rewarding.
• In bronchial Asthma the seed powder,honey and ghee are an effectivecombination.
KAPIKACHU (Mucuna pruriens) -AYURVEDIC VIEW
Dr.Pinchu Paulson, House SurgeonALN Rao Memorial Ayurvedic
MC Koppa, Karnataka
29

• A work out on hyper cholesterolemia
An in house study on Hypercholesterolemiaplanned in the 2nd week of December 2007was started on 1st of January 2008 wassuccessfully completed on 3rd week ofFebruary. The study intended to focus on thecardiovascular health profile of KeralaAyurveda’s staffs and relatives with apreferred age group of 35 years and above.The study faced an over whelming responseof participation of 41 subjects. Inclusioncriterion primarily poised the value of Totalcholesterol, of 200mg/dl and above. Fiftypercentage of cases fell outside the inclusioncriterion and most of them where having asafe lipid level status. An appealing thingnoted among them was fish items (currypreparations) formed the bulk in the nonvegetarian part of their diet; mainly smallfishes like Indian mackerel or scomber (Mal-Ayala) and Sardinella (Mal-Caala/Mathi).The incorporated subjects were randomizedand included in 3 groups, where in one groupTab.Liposem was administered and inanother group Rasonaadi Kashaayam wasadministered. Both these were comparedagainst the third one where RasonaadiKashaayam + Tab.Liposem were given. Totalduration of the study was 4 weeks offered asa complete free of cost programme. Best curein controlling Total cholesterol was met withgroups Liposem and Rasonaadi + Liposem.Best cure in controlling LDL was met withgroup Liposem. Best cure in controllingTriglycerides was met with group Rasonaadi+ Liposem and Rasonaadi Kashaayam wasfound to be superior over Liposem incontrolling Triglycerides. In elevating HDL tosafe level a mild to moderate effect wasobserved with the group Rasonaadi +Liposem. A final and detailed report will bepublished soon. Dr.Sahny.M.Soman, ClinicalResearch Co-ordinator was the investigator
of the study. Support from Department ofR&D and Mr.Bose.R.C, Deputy Manager,Clinical Research helped in completing thestudy within the stipulated time. A morepredictive study is planned and beingconducted in another group to bring out moresubstantiating outcome.
• Protocol on LBA
From the monthly clinical data received fromKAL clinics it was found that 60% of the totalcases reported were related with lower spinediseases. Out of which 80% fall underdegenerative diseases of lower spine. As perthe discussions conducted among the panel ofphysicians in Kerala Ayurveda Hospital Aluvathose cases where diagnostically included asGambheeravaatarakta and again more than75% of such cases of were age group 35 yearsand above. These scientific data temptedclinical research wing to conduct a structuredstudy on spondylosis of lumbosacral spine. Inthis perspective a common workup protocolnamed “Degenerative Diseases of LowerSpine Evaluation” was developed by theclinical research wing. It was presented to thedoctors of Kerala cluster on 4th March 2008Darshan. Doctors are expected to interactwith the clinical research wing for thesuccessful implementation of the same.
• Elementary assessment form
In a research review meeting held at KeralaAyurveda Hospital, Aluva on 27/03/2008under the presidency of Dr.K.Anilkumar (Theparticipants were Dr.K.Sasidharan, Dr. SahnyM.Soman and Dr.K. Vasanthakum ari) it wasdecided to do assessment on the clinicalmanagement on all the patients attending ourclinics, by working on a common protocol. Thisaims to report the safety and efficacy of
Clinical News
30
(Contd. on page 11)

Profession and Economy
Kerala Ayurveda had newly opened two clinics in Koramangala and Pondichery. TheKoramangala Clinic inaugurated by Mr.Jithu Mehta, President of Katra Group on 19th March2008, at 9.30 am and the Pondichery Clinic inaugurated by Mr.Sonjoy Mohanty, MD & CEO,Kerala Ayurveda Ltd, on 24th March 2008, at 9.30 am. Franchise operation division receivedappreciation from all in putting their untiring efforts to place Kerala Ayurveda as a uniqueentrepreneur in the Ayurvedic field. The clinics’ addresses are given below
Kerala Ayurveda Clinic Kerala Ayurveda Clinic
Darshan-2008 – Report
Profession and Economy
Old No.21, New No.33LalliTollendaStreet,Pondichery605 301, Tel: 0413-2221100
NSS Enterprises, No.400, 18th Main,6th Block, Koramangala Bangalore560 095, Tel: 080 6532005566
Kerala Ayurveda Health Service divisionorganized a one day interactive session for thedoctors of Kerala cluster on 4th March 2008 atAluva as a part of continuing medical educationprogramme (CME) “DARSHAN-2008”. Theprogramme started with a prayer ofDr.K.Vasanthakumari and inaugurated by wellknown physician Padmasree Dr.K.Rajagopalanin the presence of Dr.K.Anilkumar ED&T,Kerala Ayurveda Ltd, Dr.K.Sasidharan,Medical Superint endent Kerala AyurvedaHospital, Aluva and Ms.Dulari.S.S, Manager(M&A). Twenty two doctors participated in the function. After that Dr.I.P.Sreeraj, Managerand Physician, Kerala Ayurveda Clinic, Kasargod presented a paper on “KATEEGRAHA”.Dr.K.Rajagopalan and Dr.K.Sasidharan were the moderators of all the sessions. Dr Jacob Jayanpresented a papaer on the clinical approaches in back pain. Dr Sahny. M. Soman, Clinicalresearch co-ordinator explained about the data management of Kateegraha and presented aprotocol on “Degenerative Diseases of Lower Spine Evaluation”. The interactive session startedat 4 PM with an introductory speech on the topic by Padmasree Dr K Rajagopalan. He remindedthe importance of sticking to the basic principles of Ayurvedic pathophysiology and treatmentthough it is vital to utilize the modern knowledge and tools for patients’ benefit.
After the interactive session the certificate of merit was given to Dr.I.P.Sreeraj. Otherparticipants were given certificates for their participation. Ms.Dulari.S.S extended the votefor thanks to all participants. The programme was coordinated by Dr.Tiju.M.Thomas. Oneand all congratulated the health service and the organizing chairman Dr.K.Sasidharan for theaccomplishment of the program.
31

Freshly promoted
Dr.Induchoodan has been recently promoted as Manager (Marketing & Administration). Hehas been working with Kerala Ayurveda for the past one year. During this period he hadproven his talent in practice and academic activities. His last assignment was as Asst.Managerin Health service. Everybody wished him success in his new endeavor.
Darshan 08-Chennai
The program of “Darshan 2008” in Chennai cluster is planned on 22nd of April. The presenterwould be Dr.P.V.Haridas Warrier, Adayar Clinic. All the doctors from Chennai are expectedto participate in this program. The topic of presentation selected is “Stress Management”.The presenter will be awarded the certificate of merit and each participants will be given thecertificate of participation. Dr.K.Sasidharan, Medical Superintendent would be the moderator.
32
Drug given inGroup II (After food)
No of Age Sex Treatment Initial Interim FinalPatients duration Value Value Value
P I 26 yrs F 3 months T3 - 1.8 — 1.9T4 - 7.1 — 7.5TSH - 12.1 — 9.2
[* T3-ng/dl, T4-µg/dl, TSH-mIU/L]
Unfortunately due to the lack of researchsettings and patient preferences we wereunable to conduct the study in a properlydesigned form, including the total durationthere by standardizing the treatment.However the observed values are enlisted inthe table.
From the observations it was found that theadministration of drug at Dosha prakopaav
asta will have more effect than the drugadministered not in the doshaprakopaavasta. The essence of circadianrhythm and the chronobiology were foundthousands of years back by our greataacaaryas in the form of Dosha avastha andOushadha Kaala. I think this chosen study ina considerable sample size, could bring moretrustworthy results, if conducted in a welldesigned form.
(Contd. from page 18)
Profession and Economy

A bimonthly in house journal
Kerala Ayurveda Ltd.
Regd. Off : Athani, ALuva - 683 585,
Tel : 0484 - 2476301 ( 4 Lines) Fax : 0484- 2474376
e-mail : [email protected]
�For private circulation only�
Printed at SJDM PRESS S.N. GIRI, PH : 0484-6595437






![From Vaidyam to Kerala Ayurveda - IIAS · India, a separate caste of vaidyas [āyurvedic physicians] did ... Kerala Ayurveda treatment room. It must be said that focusing on particular](https://static.fdocuments.us/doc/165x107/5f0342ad7e708231d4085536/from-vaidyam-to-kerala-ayurveda-iias-india-a-separate-caste-of-vaidyas-yurvedic.jpg)