
Journal of International Dental and Medical...
10
ISSN: 1309-100X Journal of International Dental and Medical Research 2016 - Vol. 9 – Special Issue Universitas Indonesia 1 st International Workshop on Dental Research 2016 http://www.ektodermaldisplazi.com/journal.htm
Transcript of Journal of International Dental and Medical...

ISSN: 1309-100X
Journal of
International
Dental and Medical
Research
2016 - Vol. 9 – Special Issue
Universitas Indonesia 1st International Workshop on Dental Research 2016
http://www.ektodermaldisplazi.com/journal.htm

TABLE OF CONTENTS / 2016; 9 (Special Issue, U.I. 1st International Workshop on Dental Research)
J Int Dent Med Res
Journal of International Dental and Medical Research / ISSN: 1309-100X
DENTISTRY
CLINICAL ARTICLE
1. Validation of Stress Screening Questionnaire in Temporomandibular Disorders Patient
Ira Tanti, Laura S. Himawan, Lindawati Kusdhany, Adang Bachtiar, RadenIrawati Ismail
Pages 272-276
CLINICAL ARTICLE
2. The Behavior Change on Brushing Teeth of Children by Mothers Using a Periodic Dental Health
Evaluation Card
Risqa Rina Darwita, Anton Rahardjo, Peter Andreas, Febriana Setiawati, Melissa Adiatman,
Diah Ayu Maharani
Pages 273-281
CLINICAL ARTICLE
3. Dentocraniofacial Morphology in Unilateral and Bilateral Cleft Lip and Palate Following Labioplasty
and Palatoplasty; Analysis at First and Second Cervical Vertebral Maturation Stage
Devina Yastani, Maria Purbiati, Ida Ayu Astuti, Krisnawati
Pages 282-286
CLINICAL ARTICLE
4. Impact of Using Denture on Cognitive Function in the Elderly
Lindawati S Kusdhany, Michael Nathanael, Ramon Dyas, Muslita Indrasari,Chaidar Masulili,
Tri Budi Rahardjo, Dinni Agustin, Eef Hogervorst
Pages 287-292
CLINICAL ARTICLE
5. Association Between Masticatory Performance and Body Mass Index (BMI)
Muslita Indrasari, Tasya Shakina, Chaidar Masulili
Pages 293-298
CLINICAL ARTICLE
6. Etiology of Temporomandibular Disorders Index
Ira Tanti, Laura Susanti Himawan, Lindawati Kusdhany
Pages 299-305
CLINICAL ARTICLE
7. Oral Findings in Children with Human Immunodeficiency Virus Treated with Highly Active
Antiretroviral Therapy: an Institutional Study in Indonesia
Manuel Dwiyanto H Lugito, Harum Sasanti, Nia Kurniati, Yuniardini Septorini Wimardhani
Pages 306-311
CLINICAL ARTICLE
8. Prediction Index of Total Blood Testosterone Level in Elderly Men
Maria G Ernawati, Lindawati S Kusdhany, Hanna HB Iskandar
Pages 312-316
CLINICAL ARTICLE
9. Relation between Tooth Loss and Denture Wearing toward Nutritional Status
Melia Felicita, Henni Koesmaningati, Ratna Sari Dewi
Pages 317-321
CLINICAL ARTICLE
10. Association of Maxillary Transverse Discrepancies and Impacted Maxillary Canines in Patients 10 – 25
Years Old
Evy Eida Vitria, Iwan Tofani, Endang Winiati Bachtiar, Lindawati Kusdhany
Pages 322-328
TABLE OF CONTENTS / 2016; 9 (Special Issue, U.I. 1st International Workshop on Dental Research)
J Int Dent Med Res
Journal of International Dental and Medical Research / ISSN: 1309-100X
CLINICAL ARTICLE
11. Gingival Crevicular Fluid Levels of Resistin and Adiponectinin Chronic Periodontitis with Type 2
Diabetes Mellitus
Natalina, Sri Lelyati C Masulili, Nadhia Anindhita Harsas, Imam Subekti, Elza Ibrahim Auerkari
Pages 329-333
CLINICAL ARTICLE
12. Occlusal Vertical Dimension Index to Simplified Vertical Dimension Measurement
Lindawati S Kusdhany, Muslita Indrasari, Henni Koesmaningati, Max B Leepel, Indriani Oktaria
Pages 334-338
CLINICAL ARTICLE
13. Serotype C and E Streptococcus Mutans from Dental Plaque of Child-Mother Pairs With Dental Caries
Amrita Widyagarini, Heriandi Sutadi, Sarworini B. Budiardjo
Pages 339-344
CLINICAL ARTICLE
14. The Duration of Bracket Detachment at Public Health Center Jakarta and Dental Hospital Universitas
Indonesia
Gina Maringka, Ellyza Herda
Pages 345-350
CLINICAL ARTICLE
15. The LEPR Q223R Polymorphismas a Potential Bioindicator of Class II Malocclusion
Fadli Jazaldi, Endah Dwi Handayani, Yossi Nurul Utami Damayanti, Agoeng Tjahajani Sarwono,
Benny Mulyono Soegiharto, Nurtami Soedarsono, Elza Ibrahim Auerkari
Pages 351-355
CLINICAL ARTICLE
16. The Comparison of Space Closure Rate between Conventional and Passive Self-ligating System Using
Elastomeric Chain in Maxilla
Sabrina, Krisnawati, Benny Mulyono Soegiharto
Pages 356-361
EXPERIMENTAL ARTICLE
17. Mangosteen Extract Inhibits LPS-Induced Bone Resorption by Controlling Osteoclast
Erik Idrus, Bramma Kiswanjaya
Pages 362-367
EXPERIMENTAL ARTICLE
18. Increased Endothelial Cell Growth in Culture Supplemented with Outdated Human Platelet Lysate
Lisa Rinanda Amir, Endang Winiati Bachtiar, Ria Puspitawati, Agnes Henny Puspitasari, Benita Kurniawan
Pages 368-375
EXPERIMENTAL ARTICLE
19. Low Resonance Frequency Analyzer (Lrfa) as a Potential Tool for Evaluating Dental Implant
Osseointegration
Ratna Sari Dewi, Laura Susanti Himawan, Sri Angky Soekanto, Lindawati S. Kusdhany
Pages 376-381
EXPERIMENTAL ARTICLE
20. Exposure of Gel Emulsion Zoledronate Bisphosphonateolive Oil Increase Osteoclast Apoptosis
Dini Anggraini, Retno Widayati, Erni H Purwaningsih, Ahmad Aulia Jusuf
Pages 382-386

TABLE OF CONTENTS / 2016; 9 (Special Issue, U.I. 1st International Workshop on Dental Research)
J Int Dent Med Res
Journal of International Dental and Medical Research / ISSN: 1309-100X
CASE REPORT
21. Oral Mucosal Burn Caused by Topical Application of 36% Policresulen Solution – A Case Series
Indriasti Indah Wardhany, Yuniardini Septorini Wimardhani, AnandinaIrmagita Soegyanto
Pages 387-391
CASE REPORT
22. The Clinical Management of Nd-YAG LASER Combined with Endodontic Treatment in Localized
Severe Periodontitis Patient: Case Evaluation
Benso Sulijaya, Yuniarti Soeroso, Hari Sunarto, Putie Ambun Suri, Kamizar Nazar
Pages 392-397
CASE REPORT
23. Successful Treatment of Persistent Oral Ulcers in Patients with HIV / AIDS
Ellis Eka Ramadian, Siti Aliyah Pradono, Yuniardini Septorini Wimardhani
Pages 398-402
CASE REPORT
24. Oral Manifestations of Hemolytic Anemia: A Case Report
Istiqamah Yusuf, Anandina Irmagita Soegyanto, Harum Sasanti, Hamzah Shatri
Pages 403-407
CASE REPORT
25. A Rare Case of Ranula on Ventral Surface of the Tongue
Nissia Ananda, Arfan Badeges, Pradono
Pages 408-412
CASE REPORT
26. Root Coverage Treatment in Bilateral Miller’s Class I Using Subepithelial Connective Tissue Graft in a
Smoker Patient
Nadhia Anindhita Harsas, Putri Lenggogeny, Robert Lessang, Antonius Irwan
Pages 413-419
REVIEW
27. A Review of Speech Function and Maxillary Growth in Cleft Palate Patients
Dwi Ariawan, Diah Ayu Maharani, Anton Rahardjo, Iwan Tofani
Pages 420-426
REVIEW
28. The Use of Coral Scaffold in Oral and Maxillofacial Surgery: A Review
Vera Julia, Diah Ayu Maharani, Rahmana Emran Kartasasmita, Benny Sjariefsjah Latief
Pages 427-435
REVIEW
29. Genetic Role in Ameloblastoma: A Systematic Review
Fiona Verisqa, Lilies Dwi Sulistyani, Pradono, Iwan Tofani
Pages 436-440
REVIEW
30. Genes Contributing in Cleft Lip and Cleft Palate: A Literature Review
Stella Lesmana, Elza I. Auerkari
Pages 441-448

Journal of International Dental and Medical Research ISSN 1309-100X Nd-YAG LASER Combined with Endodontic Treatment http://www.ektodermaldisplazi.com/journal.htm Benso Sulijaya, and et al
Volume ∙ 9 ∙ Special Issue (U.I. 1st International Workshop on Dental Research) ∙ 2016 Page 392
The Clinical Management of Nd-YAG LASER Combined with Endodontic Treatment in Localized Severe Periodontitis Patient: Case Evaluation
Benso Sulijaya1*, Yuniarti Soeroso2, Hari Sunarto3, Putie Ambun Suri4, Kamizar Nazar5
1. BDS, DDS, Specialist in Periodontology; Lecturer in Department of Periodontology, Faculty of Dentistry, Universitas Indonesia. 2. BDS, DDS, Specialist in Periodontology, PhD; Senior Lecturer in Department of Periodontology, Faculty of Dentistry, Universitas Indonesia. 3. BDS, DDS, Specialist in Periodontology; Senior Lecturer in Department of Periodontology, Faculty of Dentistry, Universitas Indonesia. 4. BDS, DDS, Specialist in Conservative Dentistry. 5. BDS, DDS, Specialist in Conservative Dentistry; Senior Lecturer in Department of Conservative Dentistry, Faculty of Dentistry, Universitas Indonesia.
Abstract
This report is purposed to provide a holistic perception on treating localized severe periodontitis case. Fifty-five years old male, complaining of recession on his lower incisors #42, #41, #31, #32. Tooth mobility was significantly in buccal-lingual aspects (grade III). Clinical attachment loss (CAL) is up to six mm. Radiograph findings, the height of the alveolar bone loss is up to the apical area. It showed a radiolucent area surround the apical tooth #42 and #32. He is refusing of any tooth extraction. Periodontics, endodontic and dental hygienist was elaborated as a team. The oral hygiene procedure, occlusal adjustment and also temporary splint were performed. Patient had root canal treatment. After evaluation phase, pocket debridement and sulcus conditioning were executed using Nd-YAG LASER. There was a significant enhancement in Bone Density (BD) and Bone Gain (BG). Tooth mobility was reduced. Comprehensive treatment plans are needed to achieve a satisfied long-term result. Case selection is important to give a predictable outcome. Adequate oral hygiene procedure, supportive periodontal therapy (SPT) and periodic recall are required to maintain the result.
Case report (J Int Dent Med Res 2016; 9: (Special Issue), pp. 392-397) Keywords: Nd-YAG, laser, severe periodontitis, periodontal, endodontic. Received date: 28 September 2016 Accept date: 29 October 2016
Introduction Severe periodontitis is characterized by massive destruction of the dental supporting tissues and tooth mobility that leading to tooth loss.1,2 It is almost always accompanied by traumatic occlusion as predisposing factor. The prevalence of severe periodontitis in 2010 has been reported reaching 11.2% of adult population worldwide and 13.1% in South East Asia.3 The incidence of periodontal disease (2012) in Indonesia was informed about 157.485 new cases (18.5%).4 Treating severe periodontitis is a challenge. In some situation, some patient refused to get their hopeless tooth
being extracted. Instead of extract the tooth, they prefer to preserve it. Samet et al. (2009) explained the prognosis classification based on periodontal tissue support, remaining tooth’s structure, endodontic condition, occlusal plane and also tooth position.5 Lang et al. (2015) in his meta-analysis report stated that the result of the periodontal therapy may be individual.6 Recently, non-invasive therapy has developed to approach this situation. New perspective of comprehensive teamwork management could be applied. Minimizing trauma, reducing patient’s anxiety and predictable result are gained with this approach. In order to maintain the long term success of hopeless tooth management, supportive periodontal therapy (SPT) is an take an crucial part.7,8 This report is purposed to provide a holistic perception on treating localized severe periodontitis case.
*Corresponding author:
Dr. Benso Sulijaya, BDS, DDS, Specialist in Periodontology; Lecturer in Department of Periodontology, Faculty of Dentistry, Universitas Indonesia. E-mail: [email protected]

Journal of International Dental and Medical Research ISSN 1309-100X Nd-YAG LASER Combined with Endodontic Treatment http://www.ektodermaldisplazi.com/journal.htm Benso Sulijaya, and et al
Volume ∙ 9 ∙ Special Issue (U.I. 1st International Workshop on Dental Research) ∙ 2016 Page 393
Case Report Fifty-five year old male is complaining of recession on his lower incisor. Patient fells difficulty in biting and fear of tooth loss. The mobility of the incisor tooth was significantly buccal-lingual movement (grade III). Periodontal examination reveals clinical attachment loss (CAL) is about 5-6 mm. From the radiograph findings, the height of the alveolar bone loss is on the apical. There is radiolucent surround the apical of tooth #42 and #32. He is refusing of any tooth extraction. This lower incisor was categorized as a hopeless tooth and diagnosed as severe localized periodontitis inducing by traumatic occlusion. Tooth #31 and #32 had a primary periodontal-secondary endodontic lesion.
The vitality tooth #31 and #32 is non-vital with apical blackening as seen in the radiograph (figure.1). His medical history was observed and he was free of systemic diseases.
Figure 1. First clinical appearance and dental radiograph. Case Management: We do comprehensive teamwork, periodontics and endodontic. The
information about the disease condition, treatment’s option, prognosis, risk of failure and complication was given through the inform consent form and signed by the patient. Oral hygiene procedure, occlusal adjustment and also temporary splint are performed initially (figure 2).
No medication was given to this patient. On this phase, patient was told to perform a good oral hygiene procedure at home. Considering about the blackening appearance on the apical #42 and #32, then we referred it to the conservative department. Patient had a root canal treatment (RCT) on tooth #31 and #32 subsequently. The consideration to did RCT is because the vitality of tooth #31 and #32 were non-vital. It might become worse because there might be some infection spread from periodontal tissue into the pulp tissue leads to pulp necrosis. Even though from the radiograph examination, we note the blackening appearance on the apical tooth #42, but the tooth was vital. Therefore, we just evaluate the vitality of tooth #42. After the evaluation phase, pocket debridement and sulcus conditioning are executed using Nd-YAG LASER (figure 3).
Figure 2. Initial periodontal therapy was performed.

Journal of International Dental and Medical Research ISSN 1309-100X Nd-YAG LASER Combined with Endodontic Treatment http://www.ektodermaldisplazi.com/journal.htm Benso Sulijaya, and et al
Volume ∙ 9 ∙ Special Issue (U.I. 1st International Workshop on Dental Research) ∙ 2016 Page 394
Figure 3. Pocket debridement and sulcus conditioning were executed after endodontic treatment using Nd-YAG LASER.
Nine months after, we evaluate the
condition of gingiva and the mobility of the tooth. Patient shows good oral hygiene maintenance. Dental radiograph display a reducing of apical blackening on tooth #31 and #32 (figure 4).
The patient remains motivated to have a periodically recall periodontal visit. This is aimed to maintain good oral hygiene and also to confirm the long term success of severe periodontitis tooth. Two years follow-up, the periodontal pocket is reduced and the inflammation sign was absent.
Tooth mobility is also decreased. Dental radiograph shows a thickening of cortical bone and increasing of trabecular bone density (figure 5).
Figure 4. Clinical and radiograph appearance nine months after initial treatment.
Figure. 5. Clinical and radiograph appearance
two years after initial treatment.

Journal of International Dental and Medical Research ISSN 1309-100X Nd-YAG LASER Combined with Endodontic Treatment http://www.ektodermaldisplazi.com/journal.htm Benso Sulijaya, and et al
Volume ∙ 9 ∙ Special Issue (U.I. 1st International Workshop on Dental Research) ∙ 2016 Page 395
Discussion
Treating a severe periodontitis tooth is still a controversial issue whether to extract or to preserve it. For some patients, they insist to keep their own tooth rather than change with a denture. As a consequence, the patient had to performed adequate oral hygiene maintenance and to have periodically dental visit. Tooth #32, #31, #41, #42 in this case is characterized as severe localized periodontitis with hopeless prognosis. As seen in figure 1, the dental radiograph shows a massive horizontal bone destruction caused by traumatic occlusion. At the first visit, the patient is explained about the condition and the possibility risk on preserving the tooth. On tooth #32, there is almost no bone left surround the apical area. The ideal treatment plan for this patient would have been extraction of the hopeless tooth followed by removable denture, but keeping in mind the preference of the patient about preserving the tooth rather than extraction. Samet et al. (2009) explained the prognosis classification of this similar case. Based on Samet’s classification, this case was classified as a non-salvageable tooth or ―class x‖ due to less than 30% of alveolar bone support available. According to the Samet’s report, its indication therapy for that tooth is extraction.5 Lang et al. (2015) in his meta-analysis report concluded that the immune response to the periodontal therapy outcomes may be individual and vary amongst periodontitis patients.6 From that report, we may assumed that there might be a periodontal tissue improvement if the patient’s host response was positive to the treatment. Therefore, periodic clinical evaluation and supportive periodontal therapy are important to determine the prognosis for disease progression and the long-term maintenance.9-11
In managing this situation, almost similar management has been done by Rajpal et al (2013).12 He reported the therapy of hopeless tooth due to advanced periodontal disease by extracting the tooth, treating the root canal outside mouth and replanting it back to the socket technique by Lu DP13. Three months follow-up showed the replanted tooth was stable, health gingiva with no present of inflammation.12 In contrast with our case management, we did the root canal treatment inside the mouth without any extraction procedure. In our consideration by did the pocket debridement and sulcus
conditioning using Nd-YAG LASER, it will eliminate the bacterial activity and will directly promote the healing process. Seyyed A et. Al (2012) mention some application of LASER Nd-YAG in periodontology field such as soft tissue incision, ablation, sub-gingival curettage, bacterial elimination, sulcular debridement, melanin pigment removal and also treatment of dentine hypersensitivity.14 Tooth #31 and #32 need non-invasive periodontal therapy that could be given by using Nd-YAG LASER. LASER known has its ability as photo-bio-stimulator in promoting regeneration of fibroblast. Even though there is a severe bone loss, but the use of bone graft is not recommended in this kind of situation. Then use of bone graft as a regenerative material or guided tissue regeneration (GTR) was recommended better in three-wall bony defect or infra bony defect. Kanwal et al. (2014) stated that bone graft needs a vascularization to survive and attract undifferentiated mesenchymal cells and osteoblast.15 In our case, one-wall bony defect might be a challenge in the future to raise or develop a periodontal tissue vertically. Without taking a risk of periodontal tissue collapse due to invasive surgery, then we decided to perform in non-invasive way by Nd-YAG LASER.
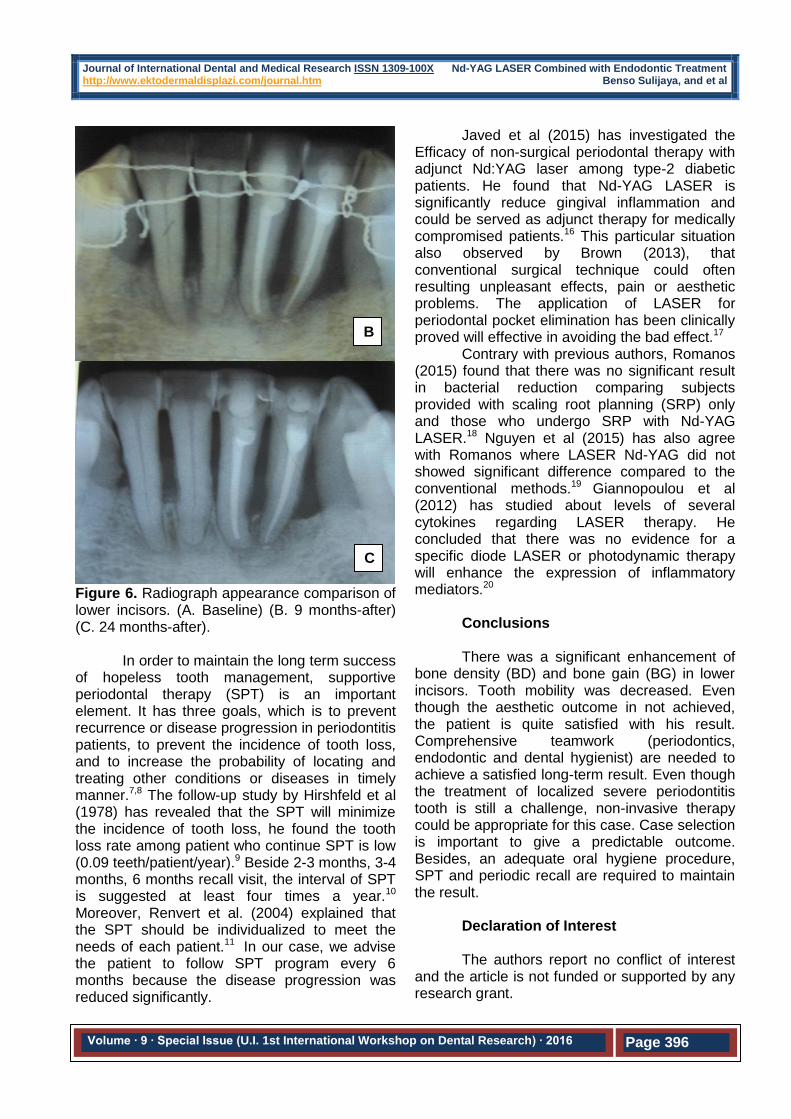
Figure 6. Shows the significant improvement of bone density (BD) and bone gain (BG). BD in the apical lower incisors (tooth #41, #42, #31, #32) at baseline compared to 9 months and 24 months-after showed significant improvement of radio-opacity. In harmony with BD, BG in all tooth showed an improvement, especially tooth #32 and #31.
A
Journal of International Dental and Medical Research ISSN 1309-100X Nd-YAG LASER Combined with Endodontic Treatment http://www.ektodermaldisplazi.com/journal.htm Benso Sulijaya, and et al
Volume ∙ 9 ∙ Special Issue (U.I. 1st International Workshop on Dental Research) ∙ 2016 Page 396
Figure 6. Radiograph appearance comparison of lower incisors. (A. Baseline) (B. 9 months-after) (C. 24 months-after).
In order to maintain the long term success of hopeless tooth management, supportive periodontal therapy (SPT) is an important element. It has three goals, which is to prevent recurrence or disease progression in periodontitis patients, to prevent the incidence of tooth loss, and to increase the probability of locating and treating other conditions or diseases in timely manner.7,8 The follow-up study by Hirshfeld et al (1978) has revealed that the SPT will minimize the incidence of tooth loss, he found the tooth loss rate among patient who continue SPT is low (0.09 teeth/patient/year).9 Beside 2-3 months, 3-4 months, 6 months recall visit, the interval of SPT is suggested at least four times a year.10 Moreover, Renvert et al. (2004) explained that the SPT should be individualized to meet the needs of each patient.11 In our case, we advise the patient to follow SPT program every 6 months because the disease progression was reduced significantly.
Javed et al (2015) has investigated the Efficacy of non-surgical periodontal therapy with adjunct Nd:YAG laser among type-2 diabetic patients. He found that Nd-YAG LASER is significantly reduce gingival inflammation and could be served as adjunct therapy for medically compromised patients.16 This particular situation also observed by Brown (2013), that conventional surgical technique could often resulting unpleasant effects, pain or aesthetic problems. The application of LASER for periodontal pocket elimination has been clinically proved will effective in avoiding the bad effect.17
Contrary with previous authors, Romanos (2015) found that there was no significant result in bacterial reduction comparing subjects provided with scaling root planning (SRP) only and those who undergo SRP with Nd-YAG LASER.18 Nguyen et al (2015) has also agree with Romanos where LASER Nd-YAG did not showed significant difference compared to the conventional methods.19 Giannopoulou et al (2012) has studied about levels of several cytokines regarding LASER therapy. He concluded that there was no evidence for a specific diode LASER or photodynamic therapy will enhance the expression of inflammatory mediators.20
Conclusions
There was a significant enhancement of bone density (BD) and bone gain (BG) in lower incisors. Tooth mobility was decreased. Even though the aesthetic outcome in not achieved, the patient is quite satisfied with his result. Comprehensive teamwork (periodontics, endodontic and dental hygienist) are needed to achieve a satisfied long-term result. Even though the treatment of localized severe periodontitis tooth is still a challenge, non-invasive therapy could be appropriate for this case. Case selection is important to give a predictable outcome. Besides, an adequate oral hygiene procedure, SPT and periodic recall are required to maintain the result. Declaration of Interest The authors report no conflict of interest and the article is not funded or supported by any research grant.
B
C

Journal of International Dental and Medical Research ISSN 1309-100X Nd-YAG LASER Combined with Endodontic Treatment http://www.ektodermaldisplazi.com/journal.htm Benso Sulijaya, and et al
Volume ∙ 9 ∙ Special Issue (U.I. 1st International Workshop on Dental Research) ∙ 2016 Page 397
References 1. Petersen PE, Ogawa H. The Global Burden of Periodontal
Disease: Towards Integration with Chronic Disease Prevention and Control. Periodontol 2000. 2012;60:15-39.
2. Petersen PE, Ogawa H. Strengthening The Prevention of Periodontal Disease: The WHO Approach. J Periodontol. 2005;76:2187-93.
3. Kasebaum NJ, Bernabe E, Dahiya M, Bhandari B, Murray CJL, Marcenes W. Global Burden of Severe Periodontitis in 1990-2010: A Systemic Review and Meta-regression. J Dent Res 2014;93(11):1045-53.
4. Oral and Dental Examination Data in Hospital Based on States (2010). Jakarta: Department of Health Promotion, Ministry of Health Republic of Indonesia, 2012;S4.31.
5. Samet N, Jotkowitz A. Classification And Prognosis Evaluation Of Individual Teeth—A Comprehensive Approach. Quintessence Int. 2009;40:377–87.
6. Lang NP, Suvan SJ, Tonetti MS. Risk Factor Assessment Tools For The Prevention Of Periodontitis Progression A Systematic Review. J Clin Perio. 2015;42:16: 59–70.
7. RK Petra, Mahl D, Deimling D et al. Er:YAG laser treatment in supportive periodontal therapy. J Clin Perio. 2012. 39(5):483–9.
8. Cohen RE; Research, Science and Therapy Committee, American Academy of Periodontology. Position Paper. Periodontal Maintenance. J Periodontol 2003;74:1395-401.
9. Hirschfeld L, Wasserman B. A Long-term Survey of Tooth Loss in 600 Treated Periodontal Patient. J Periodontol 1978;49:225-37.
10. Kwok-Chi D, Da-Wei DK, Keung WL. Supportive Periodontal Care for Hong Kong Population. Hong Kong Dental Journal. 2008;5:110-7.
11. Renvert S, Persson GR. Supportive Periodontal Therapy. Periodontol 2000; 2004;36:179-95.
12. Rajpal J, Gupta KK, Gupta MM, Garg J. Hope To Save The Hopeless Teeth With Intenional Replantation – A Case Report. International Journal of Oral Health Research & Review. 2013;1(2);19-23.
13. Lu DP. Intentional replantation of periodontally involved and endodontically mistreated tooth. Oral Surg Oral Med Oral Pathol 1986; 61:508-13.
14. Seyyed Amir Seyyedi, Ehsan Khashabi, Falaki F. Laser Application in Periodontics. Journal of Lasers in Medical Sciences. 2012;3(1):26-32.
15. Kandwal A, Bhardwaj J, Sunny, Batra M. Bone Grafts In Periodontal Surgery: A Review. Journal of Dental Herald. 2014;3(1):30-2.
16. Fawad Javed, Mohammad D. Al Amri, Abdulaziz A. Al-Kheraif, Talat Qadri, Asma Ahmed, Alexis Ghanem, José Luis Calvo-Guirado, Georgios E. Romanos. Efficacy of non-surgical periodontal therapy with adjunct Nd:YAG laser therapy in the treatment of periodontal inflammation among patients with and without type 2 diabetes mellitus: A short-term pilot study. Journal of Photochemistry and Photobiology B: Biology. 2015 (149):230–4.
17. Stephen Brown. Current Advances in the Use of Lasers in Periodontal Therapy: A Laser-Assisted New Attachment Procedure Case Series. Journal of Periodontology. 2013;3 (2):96-104.
18. Georgios Romanos. Current concepts in the use of lasers in periodontal and implant dentistry. J Indian Soc Periodontol. 201.19(5): 490–4.
19. Naomi - Trang Nguyen, Matthew R. Byarlay, Richard A. Reinhardt, David B. Marx, Trudy A.Meinberg, Wayne B. Kaldahl. Adjunctive Non-Surgical Therapy of Inflamed Periodontal Pockets During Maintenance Therapy Using Diode Laser: A Randomized Clinical Trial. Journal of Periodontology. 2015; 86 (10): 1133-40.
20. Catherine Giannopoulou, Isabelle Cappuyns, Jose Cancela,
Norbert Cionca, Andrea Mombelli. Effect of Photodynamic Therapy, Diode Laser, and Deep Scaling on Cytokine and Acute-Phase Protein Levels in Gingival Crevicular Fluid of Residual Periodontal Pockets. Journal of Periodontology. 2012; 83(8): 1018-27.


















