Codeine the basics The History What is codeine? Group of drugs narcotic pain medicines.
Upload
millicent-wilcoxCategory
view
219download
5
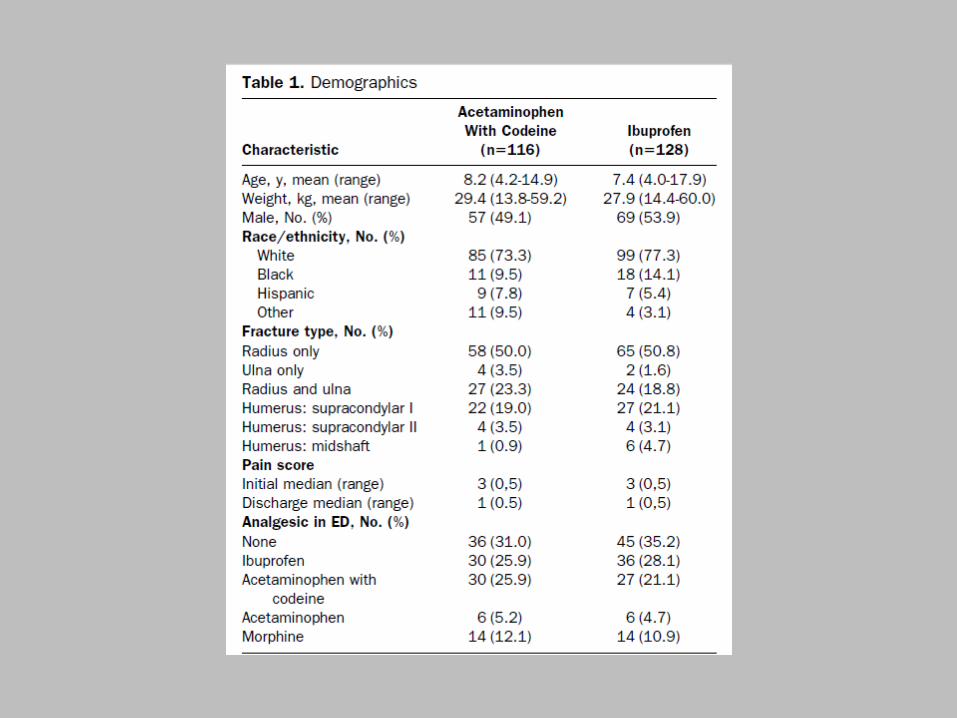
Journal Club byDr Mohammad Al-Busafi R4
Compare efficacy of Ibuprofen 10 mg /kg Paracetamol and codeine ( cocodamol ! ) 1mg/kg
(codeine component ) For outpatient treatment of pain in Paeds
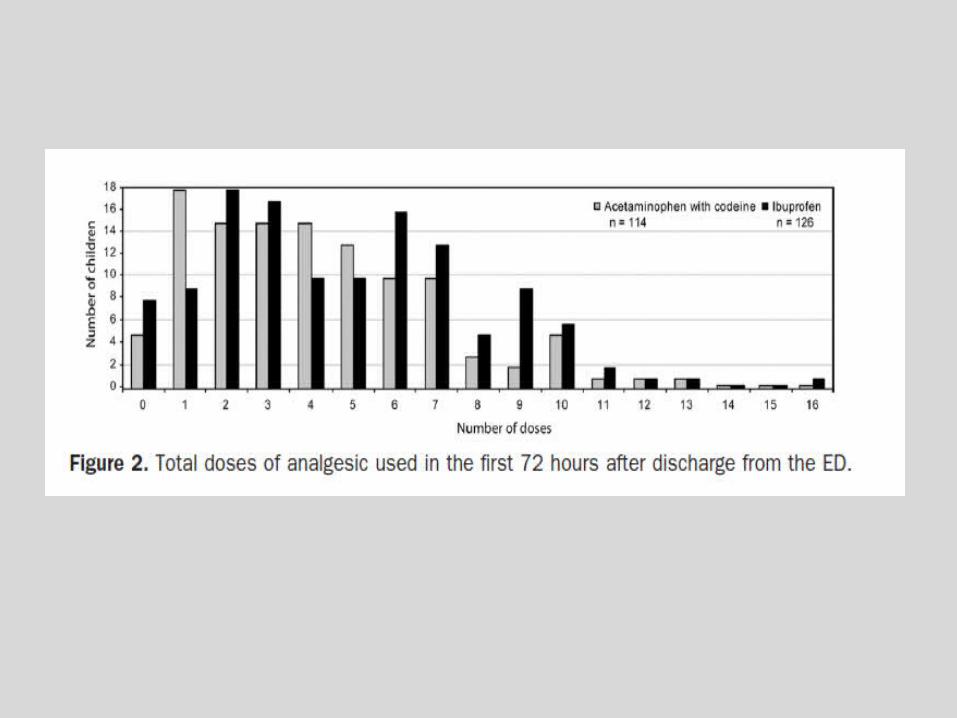
patients in the 1st 72 hours after injury Primary outcome
Treatment failure of assigned drug and use of rescue medication
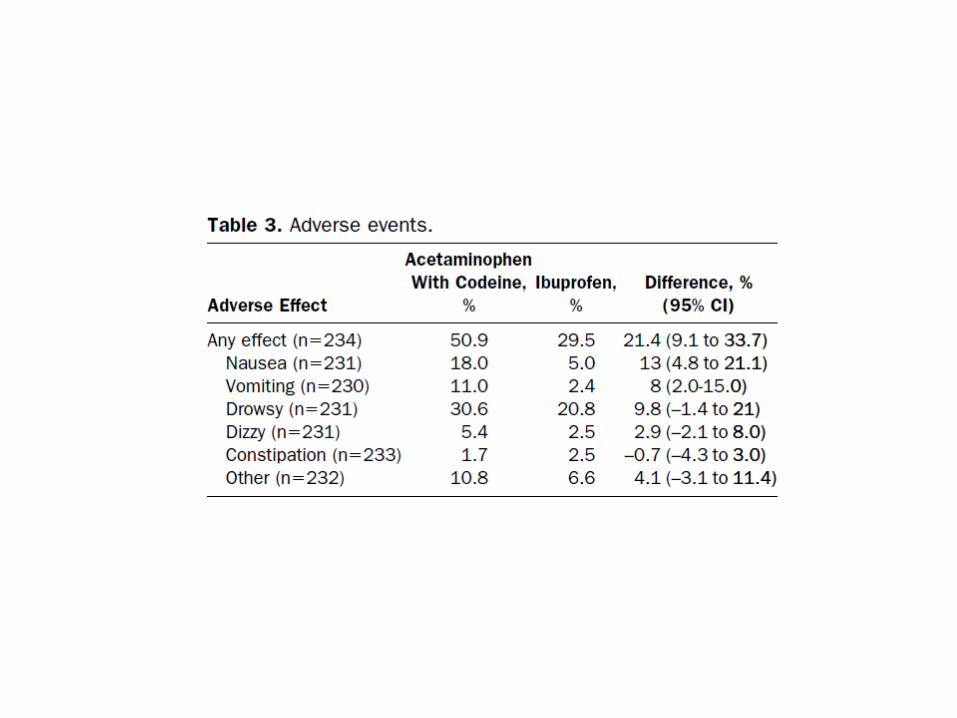
Also compare Pain scores Pain-related functional limitations Adverse effects satisfction
Randomised , double-blind ,multidose , trial
Data collected prospectively by the child & family in 1st 72 hrs after disharge from ED
Conducted in a children’s hospital Level 1 trauma center ED between August 2003 & September 2007
Children 4-18 yrs oldDx w # radius,ulna or humerus
visualised on standard 2-view radiograph
All # confirmed by pediatric radiographer
# not requiring reduction or manipulation
Children weighing > 60 kg ( requiring larger doses
h/o GI bleed/ulcer , low platelets , bleeding disorder ,kidney disease , uncontrolled chronic disease ,allergy to paracetamol or regular use
Inability to understand English
Daily diary for data collection given to parents and children
Daily data collection and returned in stamped envelope
Two standard telephone calls during 1st 72 hrs Random-number table used to assign patients to
ibuprofen / acetaminophen+codeine Physician ,parent ,all researhers blinded to
treatement Unblinded only if need 4 rescue RX ( opposite RX ,
i.e ibuprofen /acetaminophen+codeine ) ( 1hour after giving study RX
Blinding for color , volume not taste !!
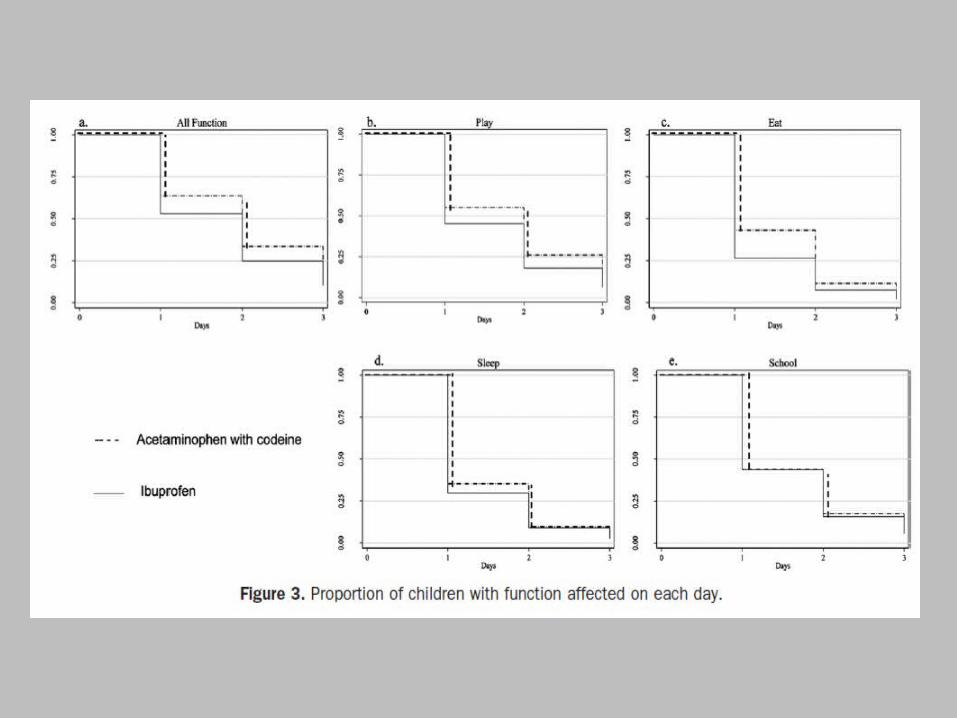
Children and care givers given diary to record whether play , school affected by pain
Record of side effectsParents satisfaction recorded daily
with 0 to 5 Likert scaleOn day 3 modified Total Quality Pain
Management instrucment used to measure parent and child satisfaction
Primary outcome was failure of the assigned study medication , leading to use of rescue medication
ibuprofen was 20.3 % less than acetaminophen w codeine of 31.0 %
Statistically not signficiant 10.7 % at Confidence interval of 95 %
No record kept of patient eligible for inclusion in study during reasercher absence so larger numbers could ‘ve been included
Doses of Rx used were based on local institution so ? Larger or less doses could ‘ve given more analgesia
Parents gave Rx to children on their own discretion
Was the allocation of Pts randomized?
Was the allocation concealed?Were the Pts in the two groups
similar at the start of the trial with respect to prognostic factors?
Were Pts analysed in the groups to which they were randomized?
Blinding :Were Pts aware of group
allocation?Were clinicians aware of group
allocation?Were outcome assessors aware of
group allocation?Were statisticians aware of group
allocation?
Were the follow up of Pts sufficiently long & complete?
Relative Risk Reduction (RRR):Proportional reduction in rates of bad
events between experimental & control group in trial .
RRR =(EER-CER)/CER =(20.3 % -31.0 % ) /31.0% =
34.5 %
Absolute Risk Reduction (ARR):
The absolute arithmetic difference in events rate .
ARR= EER – CER =20.3 % -31% = 10.7 %
Number Need to Treat ( NNT ):The number of Pts who need to be
treated to achieve one additional favourable outcome.
NNT = 1/ ARR =1/10.7 % = 9.34
Will the results help me in caring for my Pts?
Were the study Pts similar to Pts in my care?
Were all clinically important outcomes considered?
Are the likely benefits worth the potential harms & costs?