Jackpot! Jackpot! Brenda Larson RN, BSN Chest Pain Clinical Program Coordinator University of...
26
Jackpot! Jackpot! Brenda Larson RN, BSN Brenda Larson RN, BSN Chest Pain Clinical Program Chest Pain Clinical Program Coordinator Coordinator University of Wisconsin University of Wisconsin Hospital Hospital
-
Upload
reginald-banks -
Category
Documents
-
view
215 -
download
0
Transcript of Jackpot! Jackpot! Brenda Larson RN, BSN Chest Pain Clinical Program Coordinator University of...
Jackpot!Jackpot!
Brenda Larson RN, BSNBrenda Larson RN, BSN
Chest Pain Clinical Program Chest Pain Clinical Program CoordinatorCoordinator
University of Wisconsin Hospital University of Wisconsin Hospital
4
Historical PerspectiveHistorical Perspective
Coronary artery disease remains the Coronary artery disease remains the leading killer in the U.S.leading killer in the U.S.
Heart attacks occur when a blood clot Heart attacks occur when a blood clot forms in a blood vessel in the heart – forms in a blood vessel in the heart – starving the downstream muscle of starving the downstream muscle of oxygen. oxygen.
Time is critical! Every minute the artery Time is critical! Every minute the artery is blocked, heart muscle is damaged.is blocked, heart muscle is damaged.
Time is muscle!!Time is muscle!!
5
3/6/20083/6/2008Dispatched - 14:39Dispatched - 14:39
Dejope CasinoDejope Casino
71 year old male71 year old male
pale, c/o chest pain, difficulty pale, c/o chest pain, difficulty breathingbreathing

8
Initial EMS AssessmentInitial EMS Assessment
Arrived on scene: 14:49
• 71 year old male
• sitting in a wheelchair
Chief Complaint:
“Arms and legs hurt bad and terrible pains in the chest.”
“Didn’t feel like himself”
9
Primary AssessmentPrimary Assessment Mentation:Mentation: A&O x4 A&O x4 Airway/Breathing: Airway/Breathing:
RegularRegular Circulation:Circulation:
SkinSkin color: pinkcolor: pink temperature: normaltemperature: normal moisture: drymoisture: dry
Cap Refill: <2 secondsCap Refill: <2 seconds No major bleedsNo major bleeds
Determine Priority:Determine Priority:
Vital signs:
BP: 142/100
HR: 68
RR: 18
SaO2: 98%
ECG: NSR
12
HistoryHistory
Signs/symptoms:Signs/symptoms: O: playing slotsO: playing slots P: walking made pain worseP: walking made pain worse Q: dull pain, substernalQ: dull pain, substernal R: left arm and jaw/neckR: left arm and jaw/neck S: 5/10S: 5/10 T: 2:00 PM T: 2:00 PM

13
HistoryHistory Allergies: Allergies: NKDA
Medications: Medications: Glipizide
Pertinent past medical history: Pertinent past medical history: Type II DM
Last oral intake:Last oral intake: Unknown
Events:Events: playing slots chest pain is getting worse asks wife to take him home

16
InterventionsInterventionsTimTim
eeBP - HR - RR - BP - HR - RR -
SaO2SaO2Assessment Assessment InterventionsInterventions
14:3614:36 911 called911 called
14:3914:39 DispatchedDispatched
14:4914:49 Arrived on SceneArrived on Scene Initial Assessment Initial Assessment & History& History
12 lead ECG: SR & ST 12 lead ECG: SR & ST elevationelevation
ASA 324 mg PO ASA 324 mg PO (chewed) (chewed)
O2: 3L NCO2: 3L NC
18 gauge IV started x 1 18 gauge IV started x 1 with 0.9 NS at TKOwith 0.9 NS at TKO
14:5914:59 142/100 - 68 -18 - 142/100 - 68 -18 - 98%98%
Neuro: GCS 15, PERLLungs: Clear BilatSkin: unchanged
NTG SL 0.4 mgNTG SL 0.4 mg
Faxed 12 lead to UWFaxed 12 lead to UW
Leave SceneLeave Scene

17

18
InterventionsInterventionsTime BP - HR - RR -
SaO2Assessment Interventions
14:59
Leave Scene
15:05
130/P - 68 - 18 - 98%
Chest pain unchanged
Heart Attack Team activatedNTG SL 0.4mg
15:08
120/P - 62 - 18 - 98%
Chest pain “improved” but not gone. Assessment unchanged
NTG SL 0.4 mgMorphine IV 2 mg IV
15:16
Arrival to UW

19
Chest Pain ProtocolChest Pain Protocol
GeneralGeneral Assess ABCsAssess ABCs IV NSS, oxygen, pulse oximetry and ECG monitorIV NSS, oxygen, pulse oximetry and ECG monitor Vital signsVital signs Obtain a severity value of chest pain (1 to 10)Obtain a severity value of chest pain (1 to 10) Obtain and interpret 12 Lead ECG if patient Obtain and interpret 12 Lead ECG if patient
condition permitscondition permits Do not delay transport for 12 Lead ECG. Obtain Do not delay transport for 12 Lead ECG. Obtain
ECG during transport and transmit to receiving ECG during transport and transmit to receiving hospital if possible. Communicate your hospital if possible. Communicate your impression of ECG during report.impression of ECG during report.

20
Chest Pain ProtocolChest Pain Protocol
MedicationsMedications Aspirin 324 mg PO - chew and swallowAspirin 324 mg PO - chew and swallow NTG 0.4 mg SL (if SBP >90 mmHg and DBP >50 NTG 0.4 mg SL (if SBP >90 mmHg and DBP >50
mmHg) If no relief, may repeat NTG every 3-5 minutes mmHg) If no relief, may repeat NTG every 3-5 minutes up to a total of 4 doses.up to a total of 4 doses.
Morphine Sulfate 2-5 mg IVMorphine Sulfate 2-5 mg IV Treat dysrhythmias as appropriateTreat dysrhythmias as appropriate IV fluid – 300 ml NSS if SBP drops <90mmHgIV fluid – 300 ml NSS if SBP drops <90mmHg Reassess lung sounds and vital signsReassess lung sounds and vital signs Dopamine if SBP < 90 mmHg, if patient refractory to Dopamine if SBP < 90 mmHg, if patient refractory to
fluid challenge (s) or evidence of pulmonary edemafluid challenge (s) or evidence of pulmonary edema

21
Chest Pain ProtocolChest Pain Protocol
NotesNotes Elderly patients, diabetics and women Elderly patients, diabetics and women
are more likely to experience atypical are more likely to experience atypical symptoms.symptoms.
Do not administer NTG to patients Do not administer NTG to patients actively taking medications for Erectile actively taking medications for Erectile Dysfunction.Dysfunction.

What A DayWhat A Day!!
Within 29 minutes 3 STEMI Within 29 minutes 3 STEMI cases arrived to UW Cath cases arrived to UW Cath
Lab.Lab.
STEMI case start times:STEMI case start times:
1) 14:501) 14:50
2) 15:042) 15:04
3) 15:193) 15:19

23
UW HospitalUW Hospital
15:05 Heart Attack Team activated15:05 Heart Attack Team activated 15:16 EMS arrival to UWED15:16 EMS arrival to UWED
15:19 Patient on table in Cath Lab15:19 Patient on table in Cath Lab
Door to wire insertion with flow: 18 Door to wire insertion with flow: 18 minutesminutes
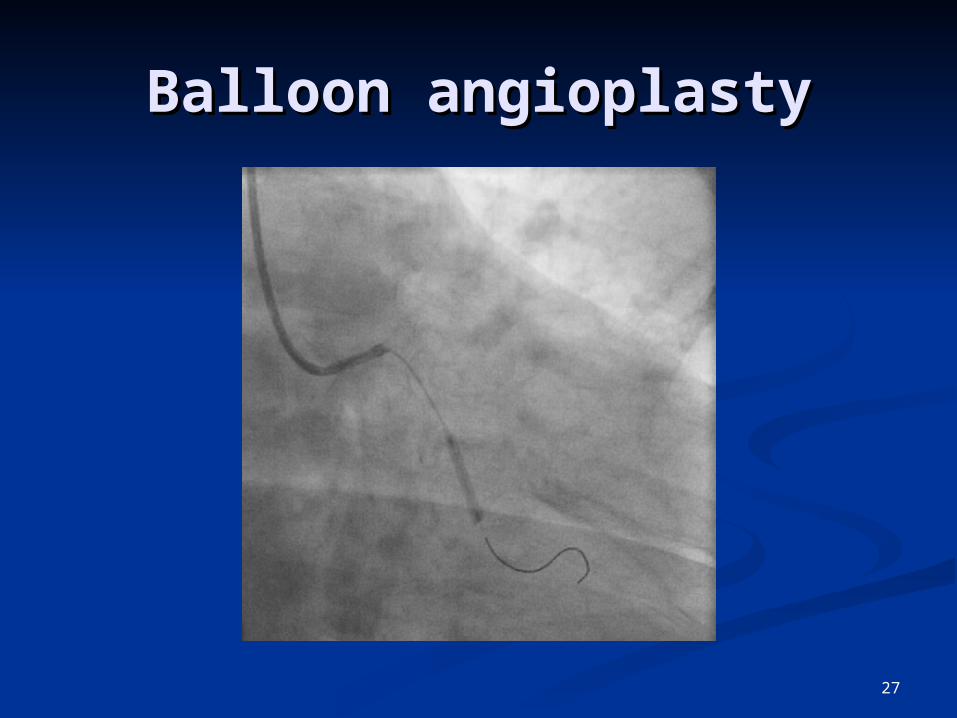
Door to balloon inflation: 23 minutesDoor to balloon inflation: 23 minutes

24
UW Cardiac Cath LabUW Cardiac Cath Lab

25
Pre procedurePre procedure
Staff involved:Staff involved: 2 Physicians2 Physicians Minimum of 2 RNs and 1 Cardiovascular Minimum of 2 RNs and 1 Cardiovascular
TechTech Consent is obtainedConsent is obtained
Patient prep:Patient prep: ECG, pulse oximetry, BPECG, pulse oximetry, BP Check pulses in feetCheck pulses in feet Remove all clothingRemove all clothing Table is only 22 inches wide (holds 500 lbs)Table is only 22 inches wide (holds 500 lbs)

26
Circumflex artery (on Circumflex artery (on arrival)arrival)
27
Balloon angioplastyBalloon angioplasty

28
Coronary stent Coronary stent deploymentdeployment

29
Stent deploymentStent deployment

30
Circumflex artery (post Circumflex artery (post procedure)procedure)

31
Summary of the Summary of the procedureprocedure
Stents:Stents: 2 bare-metal stents2 bare-metal stents
Sedation: Sedation: Fentanyl 50 mcg & Midazolam 2 mg IVFentanyl 50 mcg & Midazolam 2 mg IV
Uneventful case:Uneventful case: No N/VNo N/V No arrhythmiasNo arrhythmias
Procedure completed within 48 minutes Procedure completed within 48 minutes after arriving to the Cath Lab. after arriving to the Cath Lab.
The patient was pain free post procedure The patient was pain free post procedure and was transferred to the CCU in stable and was transferred to the CCU in stable condition.condition.

32
Discharge InstructionsDischarge Instructions
Discharged on 3/8/08Discharged on 3/8/08 follow up with PCP 1-2 weeksfollow up with PCP 1-2 weeks return for repeat PCI of RCA (3/17/08)return for repeat PCI of RCA (3/17/08) follow up with Cardiologist 4-6 weeksfollow up with Cardiologist 4-6 weeks cardiac rehab referralcardiac rehab referral nutrition consultnutrition consult lab worklab work return to work in 2-6 weeksreturn to work in 2-6 weeks

33
The PatientThe Patient
Works as a security guard at Allied Works as a security guard at Allied Automotive Automotive Group.Group.
““It’s my spending money for Dejope”It’s my spending money for Dejope”
Hobbies:Hobbies: Watching his 9 year old Grandson play Watching his 9 year old Grandson play
baseballbaseball Will celebrate his 46Will celebrate his 46thth Wedding Anniversary Wedding Anniversary
in Junein June Shoots pool every morningShoots pool every morning

37
How were you How were you doing?doing?
““I was coming out ahead!”I was coming out ahead!”
JACKPOT!JACKPOT!