Ipecac myopathy cardiomyopathy · that ipecac cardiomyopathy is largely reversi-ble. The lethal...
3
50ournal of Neurology, Neurosurgery, and Psychiatry 1992;55:560-562 SHORT REPORT Ipecac myopathy and cardiomyopathy Lee P Dresser, E Wayne Massey, Eric E Johnson, Edward Bossen Abstract Two cases of ipecac myopathy, one with associated cardiomyopathy are reported. Both patients were young women with eating disorders who came to medical attention because of diffuse muscle weak- ness. Clinical and electromyographic data suggested ipecac myopathy and muscle biopsies confirmed this diagnosis. One patient had associated clinical and echo- cardiographic evidence of significant car- diomyopathy. The myopathy resolved and the echocardiogram returned to normal after discontinuing the use of ipecac. (7 Neurol Neurosurg Psychiatryl992;55:560-562) The abuse of syrup of ipecac by patients with major eating disorders has been shown to have toxic effects on skeletal and cardiac muscle.'7 These effects are most likely secondary to emetine, one of the major alkaloids in syrup of ipecac. Emetine is well known to produce myopathy in skeletal muscle,8 and is toxic to cardiac muscle,5 and may produce electrical disturbances and heart failure.4 Syrup of ipe- cac has been responsible for several deaths in patients with the binge-purge type eating pattern of bulimia.23 The use of syrup of ipecac by bulimic patients to stimulate emesis is now recognised to be widespread.6 It is important for. physicians to be vigilant in seeking evidence of ipecac-induced myopathy and cardiomyopathy, especially in young women, because these disorders are potentially reversible. This report describes two patients with ipecac-induced myopathy and provides echocardiographic evidence of the reversibility Divisions of Neurology of an associated cardiomyopathy. and Cardiology, Department of Medicine, and the Case reports Department of Pathology, Duke Patient 1 University Medical This was a 26 year old female admitted for Center, Durham, NC evaluation of progressive muscle weakness. At 27710, USA L P Dresser the time of presentation, she had a two month E W Massey history of progressive difficulty climbing stairs, E E Johnson carrying a laundry basket, and holding her E Bossen head up while seated at work. She admitted to Correspondence to: Dr Dresser, Division of mild myalgia and had noted mild atrophy of Neurology, Duke University her thigh and arm musculature. She had Medical Center, Box 2905, Durham, NC 27710, USA occasional palpitations, increased sweating, Received 11 December 1990 and mild pedal oedema. She denied chest pain 25 February 1992. or dyspnoea on exertion. She had a history of Accepted 2 March 1992 asthma, mild hypertension, depression and anorexia nervosa. At the time of her father's death, four years before evaluation, she had lost 18 kilograms, dropping from 61 kilograms to 43 kilograms. Since then, her weight had increased to 57 kilograms and remained stable (height 165 cm). For the six month period before her evaluation, she had ingested several 30 ml doses of syrup of ipecac (containing approximately 21 mgs of emetine) per week to induce emesis after eating. She claimed only occasional alcohol use. Her general physical examination revealed a well nourished, young, white woman. Her resting heart rate was 104 with S3 and S4 heart sounds present. Lungs were clear. Icthyosis was present on the extensor surface of her arms and legs. Her neurological examination was remarkable for diffuse mild extremity atrophy and moderate diffuse weakness, greater proxi- mally. Her sensory examination was normal. Laboratory evaluation revealed blood counts, serum electrolytes, LDH, SGOT, SGPT, and alkaline phosphatase to all be within normal limits. A rheumatoid factor and antinuclear antibody were negative. A serum creatinine kinase (CK) level was elevated, with a peak at 1027 units/I. An ECG showed sinus tachycardia with a prolonged QT interval and T-wave inversion in the lateral leads. An echocardiogram showed left ventricular dilata- tion and diffuse hypocontractility with an ejection fraction of 36-5% (see table). Electro- myography showed low-amplitude, polyphasic units in proximal muscles, without increased spontaneous activity. A left deltoid biopsy showed slight variation in fibre size without evidence of inflammation. ArPase and NADH stains showed targetoid changes in both type 1 and 2 fibres with Table I Echocardiogram results (patient 1) Study I Study 2 (15 months after discontinuing ipecac) LVIDd 5-1 cm 4-6 cm (short axis) LVIDs 4-2 cm 3-4 cm (short axis) EDV 109-4 ml 120-5 ml (apical view) ESV 69-5 ml 65-1 ml (apical view) EF 36-5% 46-0% FS 17-6% 26-1% Abbreviations: LVIDd (left ventricular internal dimension, diastole), LVIDs (left ventricular internal dimension, systole), EDV (end diastolic volume), ESV (end systolic volume), EF (ejection fraction), FS (fractional shortening). 560 on June 3, 2020 by guest. Protected by copyright. http://jnnp.bmj.com/ J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.56.5.560 on 1 May 1993. Downloaded from
Transcript of Ipecac myopathy cardiomyopathy · that ipecac cardiomyopathy is largely reversi-ble. The lethal...

50ournal of Neurology, Neurosurgery, and Psychiatry 1992;55:560-562
SHORT REPORT
Ipecac myopathy and cardiomyopathy
Lee P Dresser, E Wayne Massey, Eric E Johnson, Edward Bossen
AbstractTwo cases of ipecac myopathy, one withassociated cardiomyopathy are reported.Both patients were young women witheating disorders who came to medicalattention because of diffuse muscle weak-ness. Clinical and electromyographic datasuggested ipecac myopathy and musclebiopsies confirmed this diagnosis. Onepatient had associated clinical and echo-cardiographic evidence of significant car-
diomyopathy. The myopathy resolved andthe echocardiogram returned to normalafter discontinuing the use of ipecac.
(7 Neurol Neurosurg Psychiatryl992;55:560-562)
The abuse of syrup of ipecac by patients withmajor eating disorders has been shown to havetoxic effects on skeletal and cardiac muscle.'7These effects are most likely secondary toemetine, one of the major alkaloids in syrup ofipecac. Emetine is well known to producemyopathy in skeletal muscle,8 and is toxic tocardiac muscle,5 and may produce electricaldisturbances and heart failure.4 Syrup of ipe-cac has been responsible for several deaths inpatients with the binge-purge type eatingpattern of bulimia.23 The use of syrup ofipecac by bulimic patients to stimulate emesisis now recognised to be widespread.6 It isimportant for. physicians to be vigilant inseeking evidence of ipecac-induced myopathyand cardiomyopathy, especially in youngwomen, because these disorders are potentiallyreversible. This report describes two patientswith ipecac-induced myopathy and providesechocardiographic evidence of the reversibility
Divisions of Neurology of an associated cardiomyopathy.and Cardiology,Department ofMedicine, and the Case reportsDepartment ofPathology, Duke Patient 1
University Medical This was a 26 year old female admitted forCenter, Durham, NC evaluation of progressive muscle weakness. At
27710, USA
L P Dresser the time of presentation, she had a two monthEW Massey history of progressive difficulty climbing stairs,E E Johnson carrying a laundry basket, and holding herE Bossen
head up while seated at work. She admitted toCorrespondence to:Dr Dresser, Division of mild myalgia and had noted mild atrophy ofNeurology, Duke University her thigh and arm musculature. She hadMedical Center, Box 2905,
Durham, NC 27710, USA occasional palpitations, increased sweating,Received 11 December 1990 and mild pedal oedema. She denied chest pain25 February 1992. or dyspnoea on exertion. She had a history ofAccepted 2 March 1992 asthma, mild hypertension, depression and
anorexia nervosa. At the time of her father'sdeath, four years before evaluation, she hadlost 18 kilograms, dropping from 61 kilogramsto 43 kilograms. Since then, her weight hadincreased to 57 kilograms and remained stable(height 165 cm). For the six month periodbefore her evaluation, she had ingested several30 ml doses of syrup of ipecac (containingapproximately 21 mgs of emetine) per week toinduce emesis after eating. She claimed onlyoccasional alcohol use.Her general physical examination revealed a
well nourished, young, white woman. Herresting heart rate was 104 with S3 and S4 heartsounds present. Lungs were clear. Icthyosiswas present on the extensor surface ofher armsand legs. Her neurological examination wasremarkable for diffuse mild extremity atrophyand moderate diffuse weakness, greater proxi-mally. Her sensory examination was normal.
Laboratory evaluation revealed bloodcounts, serum electrolytes, LDH, SGOT,SGPT, and alkaline phosphatase to all bewithin normal limits. A rheumatoid factor andantinuclear antibody were negative. A serumcreatinine kinase (CK) level was elevated, witha peak at 1027 units/I. An ECG showed sinustachycardia with a prolonged QT interval andT-wave inversion in the lateral leads. Anechocardiogram showed left ventricular dilata-tion and diffuse hypocontractility with anejection fraction of 36-5% (see table). Electro-myography showed low-amplitude, polyphasicunits in proximal muscles, without increasedspontaneous activity.A left deltoid biopsy showed slight variation
in fibre size without evidence of inflammation.ArPase and NADH stains showed targetoidchanges in both type 1 and 2 fibres with
Table I Echocardiogram results (patient 1)
Study I Study 2(15 months afterdiscontinuing ipecac)
LVIDd 5-1 cm 4-6 cm(short axis)
LVIDs 4-2 cm 3-4 cm(short axis)
EDV 109-4 ml 120-5 ml(apical view)
ESV 69-5 ml 65-1 ml(apical view)
EF 36-5% 46-0%FS 17-6% 26-1%
Abbreviations: LVIDd (left ventricular internal dimension,diastole), LVIDs (left ventricular internal dimension, systole),EDV (end diastolic volume), ESV (end systolic volume), EF(ejection fraction), FS (fractional shortening).
560
on June 3, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.56.5.560 on 1 May 1993. D
ownloaded from

Ipecac myopathy and cardiomyopathy
WkI
L~~~~~~
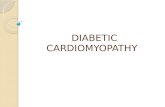
Figure 1 Electron micrograph shows electron-dense aggregates within fibres,apparently correspond to degenerating Z-band materiaL (Magnification x
! < s | l .~~~~~A
4i
.I
v--
As..
11.- x
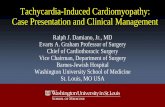
Figure 2 Trichome stain of muscle biopsy from patient 2 shows aggregationdense-staining bodies within fibres (arrows). (Magnification x 400).
normal fibre distribution. Phomyoadenylate deaminase, congo recstains were normal. Electron i
showed extensive disorganisation ofwith extreme smudging of Z-band n
1). The patient stopped using ipecathree months her strength returnnormal and she had no further coi
palpitations or ankle oedema. A recardiogram performed 15 month!first study demonstrated normaltricular function (see table).
561
Patient 2This was a 29 year old, white female who wasevaluated for muscle weakness during a psy-chiatric admission for an eating disorder. Shehad a several month history of progressivegeneralised weakness, exercise intolerance andamenorrhea. For the six months before evalu-ation, she drank approximately one bottle ofwine per day. During this period, she had apattern ofminimal food intake alternating withbinge eating, always followed by ipecac-induced emesis. General physical examinationshowed a thin white female with dry skin.Heart and lungs examination were normal.Diffuse moderate muscle atrophy and weak-ness were present, more prominent proximally.Sensory examination was normal.
Laboratory evaluation showed blood counts,serum chemistries, thyroid function test, andserum CK to be within normal limits. An ECGshowed nonspecific T-wave abnormalities.Electromyography showed long, polyphasicmotor units with no increased insertional or
which spontaneous activity.6,600). A biopsy of the left vastus laterlis muscle
showed foci of fibres with increased numbersof internal nuclei with minimal atrophy. Tri-chrome staining showed focal groups of fibreswith blurring of the myofibrillar network andaggregations of dense staining material (fig 2).These aggregates were seen by electronmicroscopy to represent Z-band streaming.NADH staining also showed loss of the myofi-brillar network in many fibres, resulting in atargetoid appearance similar to that seen inpatient 1. There was no evidence of inflamma-tion, and phosphorylase and myoadenylatestaining showed normal activity.
Discussion$ Ipecac is isolated from the root of Cephalis- ipecacuanha. It contains two major alkaloids,
emetine and cephaeline. Cephaeline is prima-rily responsible for producing nausea andemesis, whereas emetine is more toxic toskeletal muscle and the heart.4 Ipecac has longbeen used by natives of Brazil to treat diar-
/ rhoea and has had widespread use in thetreatment of amebiasis.4 It has also been usedin aversive therapy for alcoholism9 and has
Is of been employed experimentally as an antineo-plastic agent. In the USA, the only official useof ipecac is as an emetic to treat accidentalpoisoning. It is available without prescriptiononly in syrup form. Through experiences withits use as a treatment for amebiasis, ipecac hasbeen shown to cause a myopathy.'0
sphorylase, In one study, nearly 5% of high school age1, and lipid females admitted to bulimic activity.5 Theymicroscopy may resort to ipecac abuse if they cannotfmyofibrils effectively induce mechanical emesis. It isnaterial (fig estimated that there are one million bulimiclc and after women in America and that 35 000 abuseed to near ipecac.6'mplaints of Ipecac myopathy should be considered in allpeat echo- young women with progressive proximal mus-s after the cle weakness, atrophy, or stiffness, especially
left ven- when there is any suggestion of an eatingdisorder. Both of our patients had dry skin,
,-. I. -,
f
A on June 3, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.56.5.560 on 1 May 1993. D
ownloaded from

Dresser, Massey, J7ohnson, Bossen
and several other cases have been reported inwhich patients were noted to have dry or
erythematous skin. ' 7 The serum CK level maybe elevated, but it can also be within normallimits in the presence of significant weakness.The electromyogram shows nonspecific myo-
pathic changes, but a muscle biopsy will helpdistinguish ipecac myopathy from inflamma-tory or alcohol-induced myopathy.' '3 Nerveconduction velocity is normal.
If ipecac abuse is suspected, an evaluationfor cardiomyopathy is warranted. Historical or
physical evidence of cardiac failure may bepresent. The electrocardiogram may show rest-ing tachycardia, prolongation of the QT andPR intervals, inverted T-waves, and ST seg-
ment abnormalities.4 As in the case of patient1, significant depression of left ventricularfunction may be detected by echocardiogramor radionuclide tests. The serial echocardio-grams performed on our patient demonstratedthat ipecac cardiomyopathy is largely reversi-ble.The lethal dose of emetine has been esti-
mated to be 10 to 25 mgs, or approximately1 25 grams for an adult.'0 Death is usuallycaused by ventricular arrhythmias or heartfailure.4 Emetine is so slowly excreted from thebody that doses may accumulate over time toapproximate the lethal dose, even when emesisis stimulated.4 Syrup of ipecac is available in30 ml doses, each dose containing approx-imately 21 mgs of emetine. It is thereforepossible to accumulate a lethal amount ofemetine within the body over several monthswhen ipecac is used daily. It has been proposedthat emetine inhibits protein synthesis andmitrochondrial oxidative phosphorylation inskeletal muscle. These effects may cause
decreased ATP formation and a subsequentincreased release of calcium into the sarco-
plasm that, in turn, activates proteases whichcause Z-band lysis, granule formation, andmyofilament disorganisation.9 In the heart,emetine is thought to depress glycolysis andKreb's cycle, as well as inhibit synthesis ofcontractile proteins.4The microscopic pathological changes seen
in the muscle biopsies from our patients are
very similar to those reported in previous cases
of ipecac myopathy' 7 9and experimentalemetine-induced myopathy in rats.8 Lightmicroscopy reveals variation in fibre size,
internal nuclei, granular breakdown of myofi-laments, and central core changes or targetoidchanges in fibres with ATPase or NADHstains. Electron microscopy shows Z-bandstreaming and dense bodies." Inflammatoryinfiltrates are not seen.' These findings arecharacteristic of ipecac myopathy, but are alsoseen in a variety of other conditions.'2Although patient 2 was a heavy consumer ofalcohol, her muscle biopsy was quite similar tothat of patient 1 and demonstrated the charac-teristic targetoid changes and Z-band stream-ing of emetine myopathy. The characteristictype II fibre atrophy of chronic alcoholicmyopathy'3 was absent and therefore hermyopathy was likely predominately due toemetine toxicity. The effects on cardiac muscleare not as well documented, but interstitialoedema, inflammation, and degenerativechange of myocardial fibres have been repor-ted.3Therapy consists of discontinuing ipecac use
and employing supportive measures. If cardio-myopathy is significant, inotropic and afterloadreducing agents may be used. As shown inpatient 1, both the cardiomyopathy and myop-athy improved after discontinuing ipecacabuse. Electrical and pathological evidence ofmuscle recovery has also be demonstrated.9 12
1 Mateer JE, Farrell BJ, Chou SM, Gutmann L. Reversibleipecac myopathy. Arch Neurol 1985;42:188-90.
2 Dawson JA, Yager J. A case of syrup of ipecac resulting indeath. JAmer Coll Health 1986;34:280.;4
3 Adler AG, Walinsky P, Krall RA, Cho S Death resultingfrom ipecac syrup poisoning. J ., Amer Med Assoc1980;243: 1927-8.
4 Manno BR, Manno JE. Toxicology of ipecac: a review. ClinTox 1977;10:221-42.
5 Isner JM. Effects of ipecac on the heart. (Letter). New EnglJ7Med 1986;313:1253-5.
6 Pope HG, Hudson JI, Nixon RA, Herridge PL. Theepidemiology of ipecac abuse. (Letter) New Engl J Med1986;245-6.
7 Bennett HS, Spiro AJ, Pollock MA, Zueker P. Ipecac-induced myopathy simulating dermatomyositis. Neurol1982;32:91-4.
8 Bindoff L, Cullen MJ. Experimental (-) emetine myopathy.J Neurol Sciences 1978;39:1-15.
9 Sugie H, Russin R, Verity AM. Emetine myopathy: two casereports with pathobiochemical analysis. Muscle Nerve1984;7:54-9.
10 Anderson HH, Reed AC. Untoward affects of anti-ambeicdrugs. Am J Trop Med Hygiene 1934;14:269-81.
11 Halbig L, Gutmann L, Goebel HH, Brick JF, Schochet S.Ultrastructural pathology in emetine-induced myopathy.Acta Neuropath 1988;75:577-82.
12 Goebel HH. Neuropathological aspects of congenital myo-pathies. Prog Neuropath 1980:6:231-48.
13 Hanid A, Slavin G, Mair W et al. Fibre type changes instraited muscles of alcoholics. J Clin Pathol 1981;34:991-7.
562 on June 3, 2020 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.56.5.560 on 1 M
ay 1993. Dow
nloaded from