Iodine deficiency disorders zIodine is an essential component in thyroid hormone production zThyroid...
58
Iodine deficiency disorders Iodine is an essential component in thyroid hormone production Thyroid hormone regulates basic metabolism :energy consumption, cellular activity, growth and in particular brain development. Hypothyroidism: slow, cold, sluggish brain function, short stature, mental and motor development delayed or slowed. In extremes general neurological development delayed.
-
Upload
octavio-manger -
Category
Documents
-
view
234 -
download
1
Transcript of Iodine deficiency disorders zIodine is an essential component in thyroid hormone production zThyroid...
Iodine deficiency disorders
Iodine is an essential component in thyroid hormone production
Thyroid hormone regulates basic metabolism :energy consumption, cellular activity, growth and in particular brain development.
Hypothyroidism: slow, cold, sluggish brain function, short stature, mental and motor development delayed or slowed. In extremes general neurological development delayed.


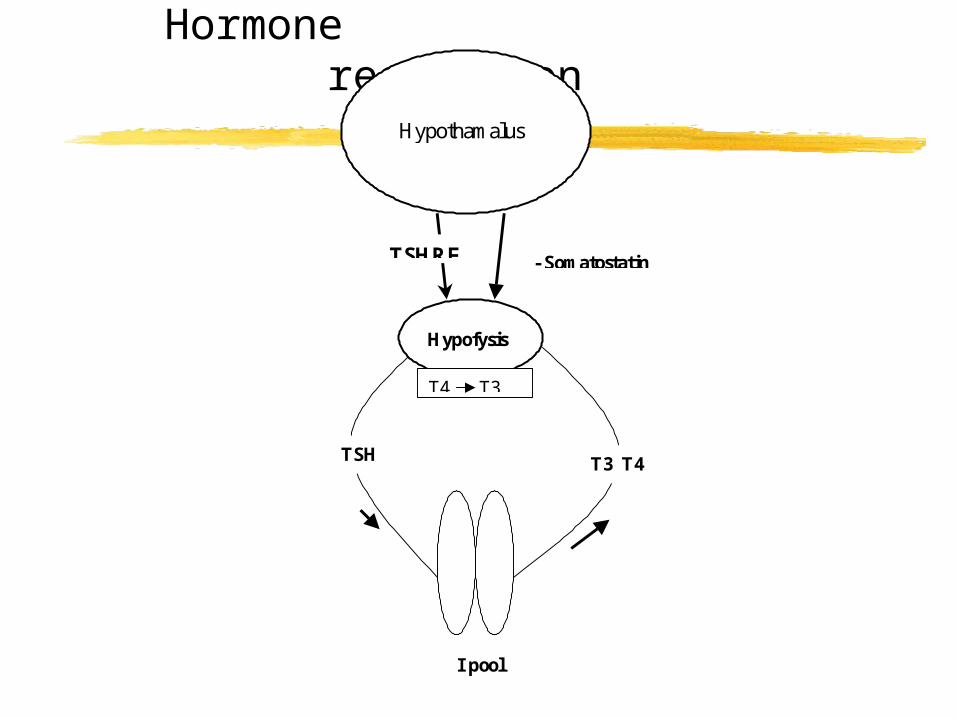
Hormone regulationHypothamalus
TSH T3 T4
Hypofysis
- SomatostatinTSHRF
T4 T3
I pool
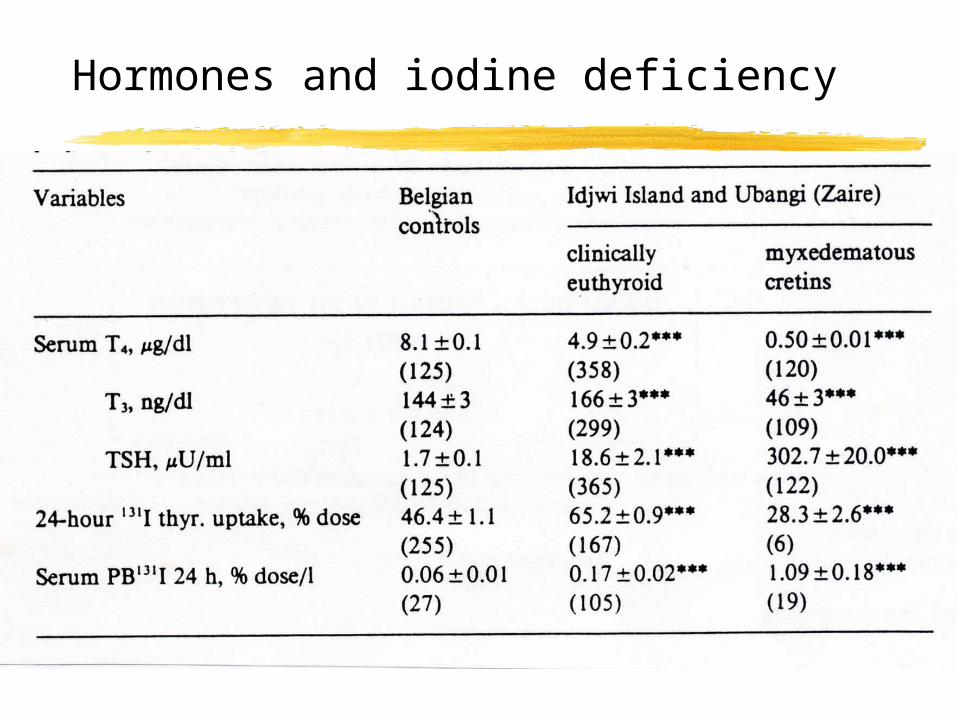
Hormones and iodine deficiency

Spectrum of diseaseTable 1. The Spectrum of Iodine Deficiency Disorders, IDD.Fetus Abortions Stillbirths
Congenital anomaliesIncreased perinatal mortalityEndemic cretinism
Neonate Neonatal goiter Neonatal hypothyroidismEndemic mental retardationIncreased susceptibility of the thyroid glandto nuclear radiation
Child and Goiter adolescent (Subclinical) hypothyroidismImpaired mental functionRetarded physical developmentIncreased susceptibility of the thyroid glandto nuclear radiation
Adult Goiter with its complications HypothyroidismImpaired mental functionSpontaneous hyperthyroidism in the elderlyIodine-induced hyperthyroidismIncreased susceptibility of the thyroid glandto nuclear radiation
Adapted from Hetzel (1), Laurberg et al. (52, 171) and Stanbury et al. (158).
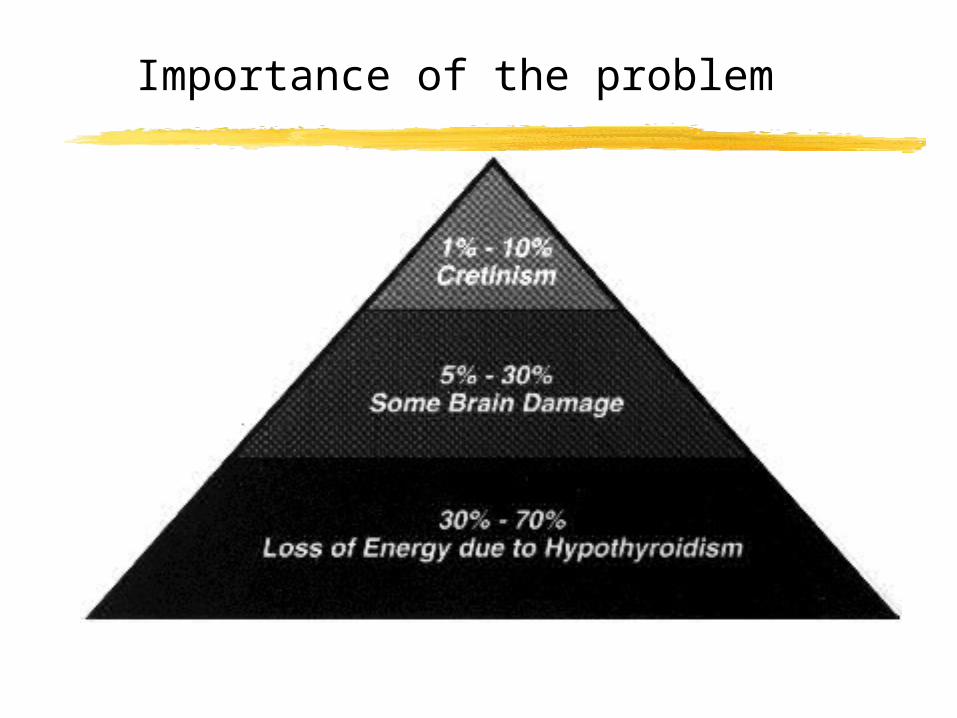
Importance of the problem

Prevalence
1 billion persons exposed200 million persons affected (goitres)26 million cases of mental problems6 million cases of cretinism

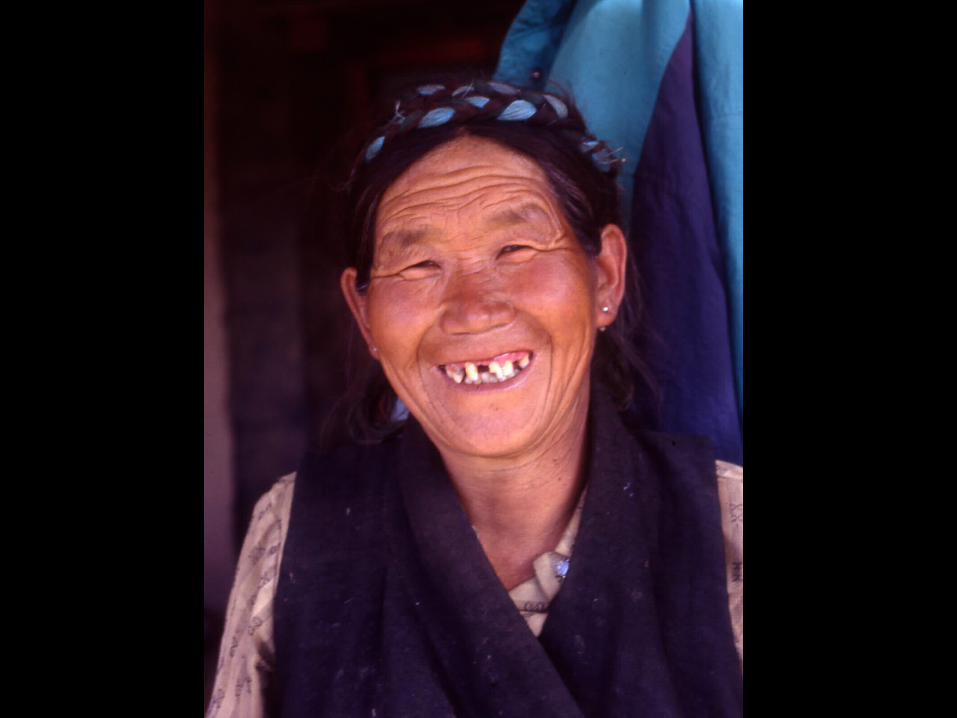
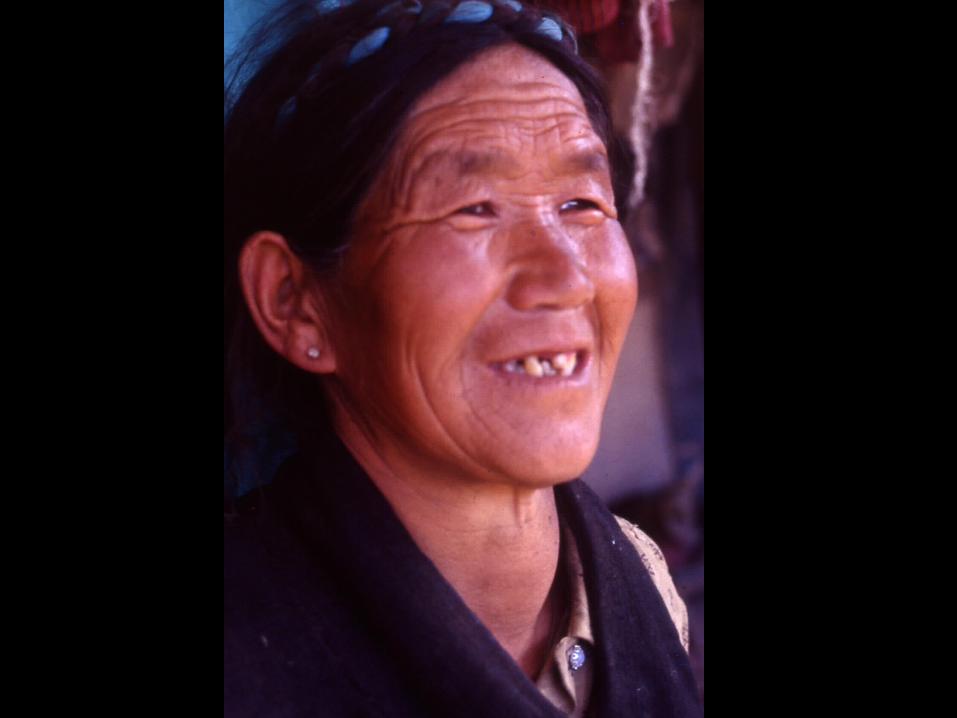
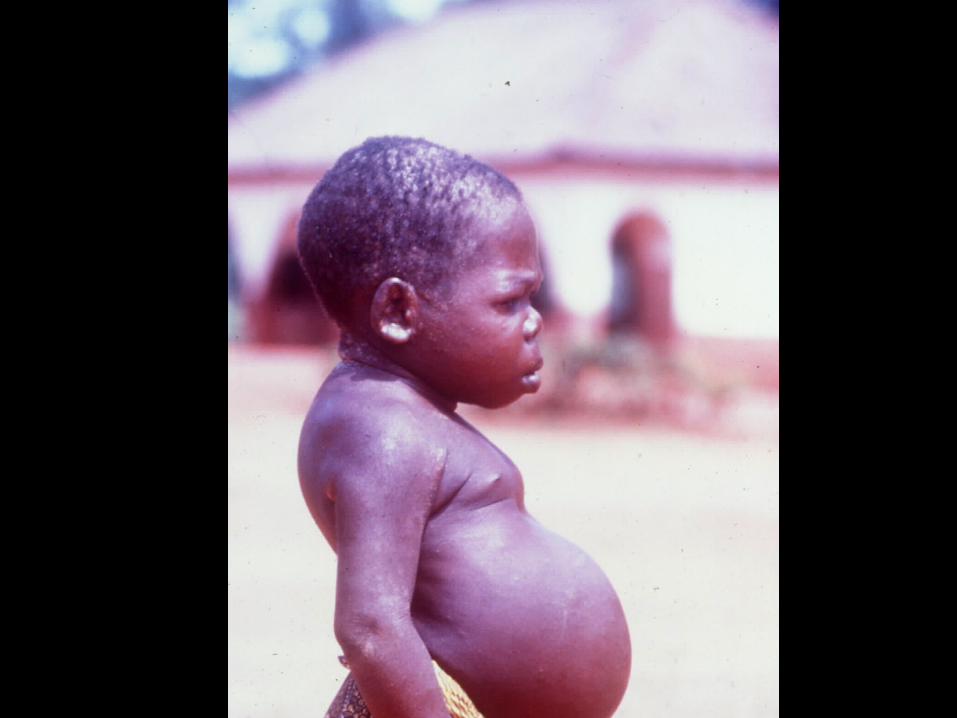
Goitre
Increase in size four to five times distal phalanx of the thumb
Aesthetic Compression Related hypothyroidism: is not a
compensation cancer Iod Basedow (hyperthyroidism) due to
hyperstimulation, mutation autonomous nodules







Iodine deficiency and the foetus
Brain development fast between 3-5 months pregnancy and from third trimester till end of second year
Maternal T4 essential for first 24 weeksFoetal T4 starts at 24 weeks30% cord blood is of maternal origin

Iodine and the neonate
Perinatal mortalityInfant mortalityLow birth weightBrain development needs T4Iodine deficiency mental retardation,
retarded motor development. General IQ decrease of 15 Points

Iodine deficiency and adults
Lack of energyapathy, slow brainsgoitre and mechanical complicationsNodular thyroidhyperthyroidismPregnancy and cretinism
Aethiology
Low iodine uptake. Soil dependent erosion, wash away: deltas
Goitrogens Manioc: linnamarin thiocyanate
Blocs uptake of Iodine at the thyroid, competitive inhibition
Traditional preparationsKonzo
Brassica family polutants




IDD and selenium deficiency
Se part of peripheral type I de-Iodinase (kidney and liver)
Se deficiency: slower T4 to T3 metabolisation
Se part of Glutathion peroxidase : protector of H2O2 damage Thyroid damage, disfunction of thyroid
Cerebral de-iodinase is not Se dependent Glutathion peroxidase stimulates T4
production
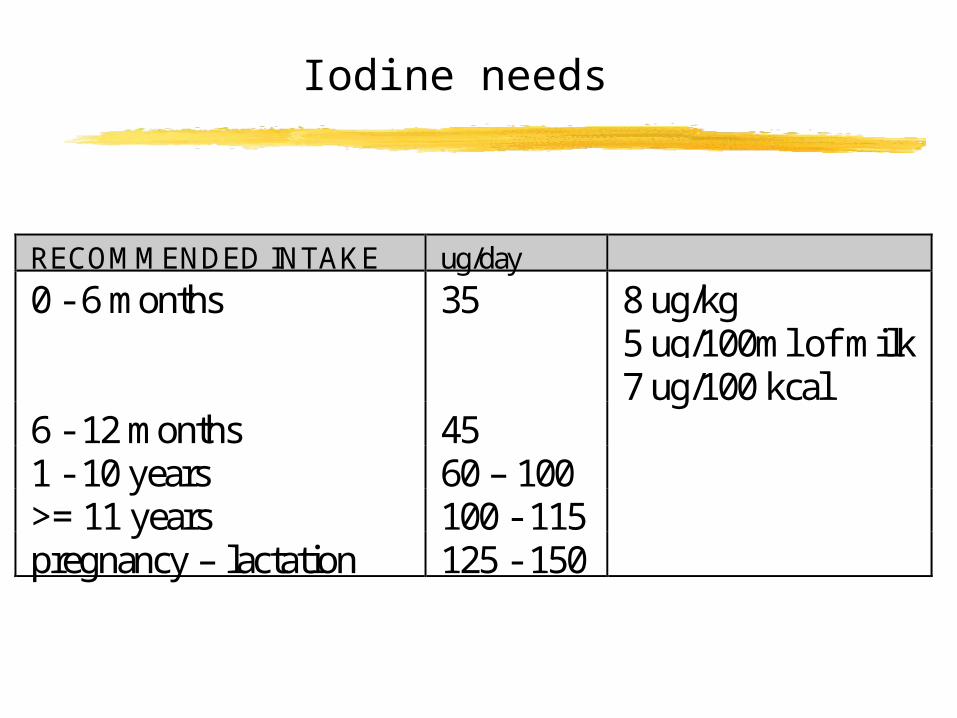
Iodine needs
RECOMMENDED INTAKE ug/day
0 - 6 months 35 8 ug/kg5 ug/100ml of milk7 ug/100 kcal
6 - 12 months 451 - 10 years 60 – 100>= 11 years 100 - 115pregnancy – lactation 125 - 150
Diagnosis of endemicity
Prevalence of goitreDosage of urinary iodineTSH dosagePrevalence of cretinism
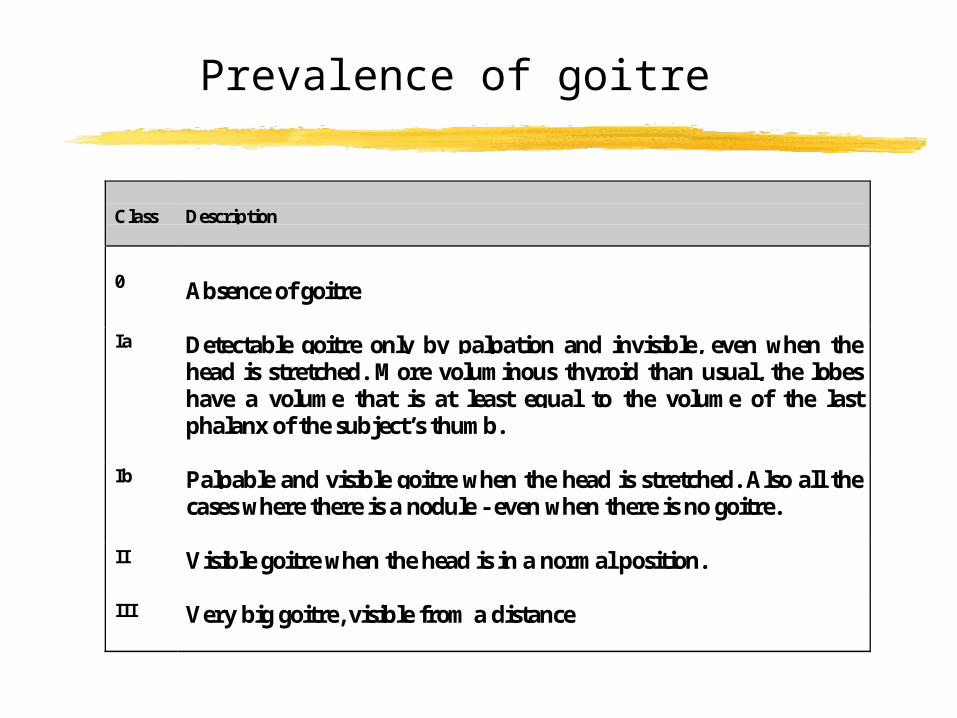
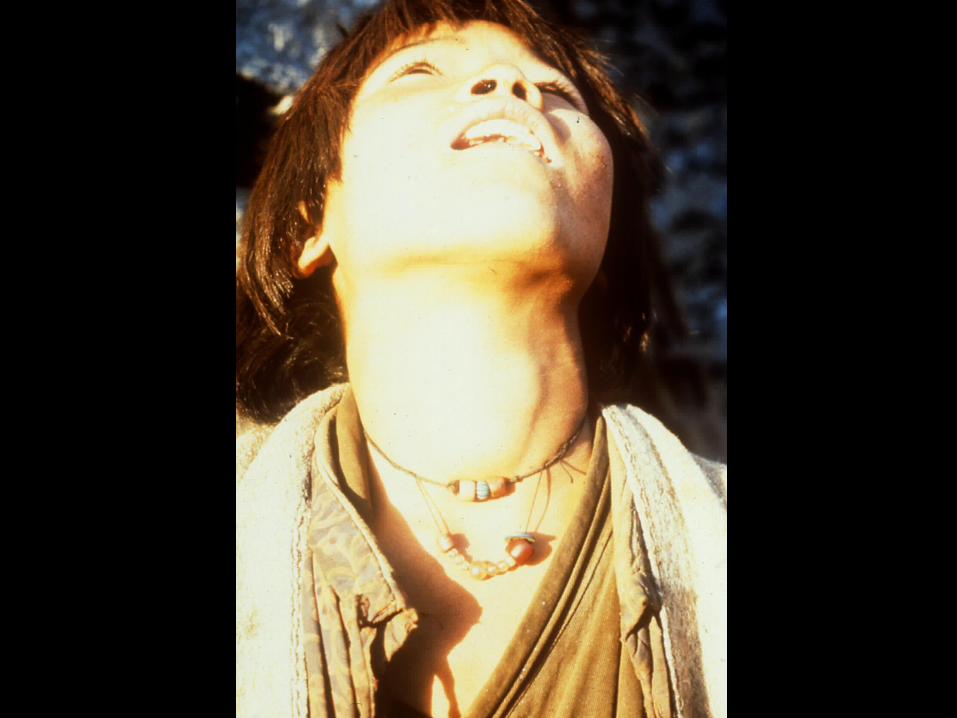
Prevalence of goitre
Class Description
0 Absence of goitre
Ia Detectable goitre only by palpation and invisible, even when thehead is stretched. More voluminous thyroid than usual, the lobeshave a volume that is at least equal to the volume of the lastphalanx of the subject’s thumb.
Ib Palpable and visible goitre when the head is stretched. Also all thecases where there is a nodule - even when there is no goitre.
II Visible goitre when the head is in a normal position.
III Very big goitre, visible from a distance
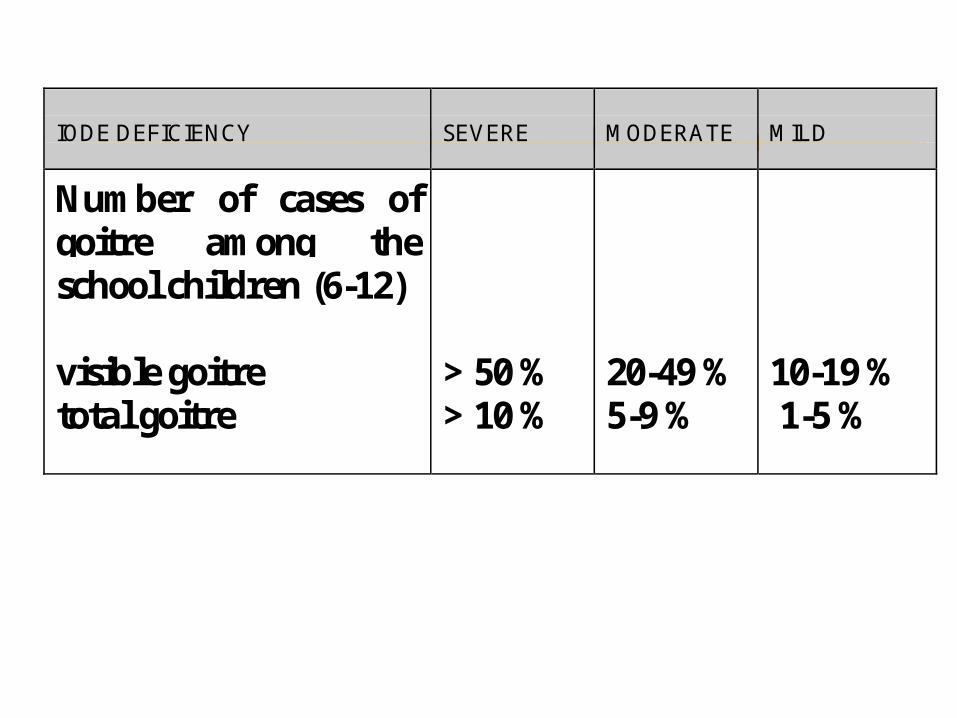
IODE DEFICIENCY SEVERE MODERATE MILD
Number of cases ofgoitre among theschool children (6-12)
visible goitretotal goitre
> 50 %> 10 %
20-49 %5-9 %
10-19 % 1-5 %

Urinary Iodine
Reflects directly intakeIs best to follow up programme response,
goitre takes time to decrease in sizeSamples needed are smallerTechnique is simple and not expensiveSamples can be taken easily, cheap,
acceptable and don’t need conservation techniques
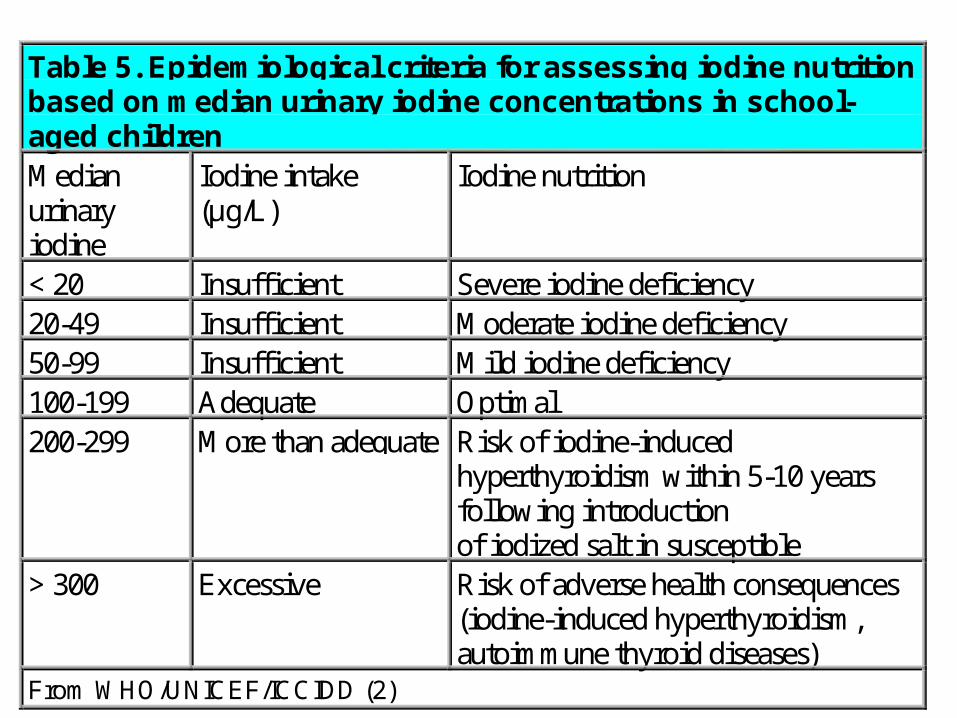
Table 5. Epidemiological criteria for assessing iodine nutritionbased on median urinary iodine concentrations in school-aged childrenMedianurinaryiodine
Iodine intake(µg/L)
Iodine nutrition
< 20 Insufficient Severe iodine deficiency20-49 Insufficient Moderate iodine deficiency50-99 Insufficient Mild iodine deficiency100-199 Adequate Optimal200-299 More than adequate Risk of iodine-induced
hyperthyroidism within 5-10 yearsfollowing introductionof iodized salt in susceptible
> 300 Excessive Risk of adverse health consequences(iodine-induced hyperthyroidism,autoimmune thyroid diseases)
From WHO/UNICEF/ICCIDD (2)

Endemic cretinism
Neurological Severe motor and mental deficit cerebral palsy deafness, mutism euthyroid
Myoedematous Severe mental deficit Hypothyroid, destruction of the thyroid Iodine deficiency combined with goitrogens
and Se deficiency













Control strategies
Supplementation: injections, oralFortificationchanging food habits

Supplementation
Need to start early in pregnancysupplement women of child bearing ageOperational difficultiesInjections and hepatitis and HIVCovers need for about 4 years injectionsOral covers needs for one year
Fortification
Add iodine to a vehicle: salt or waterAdditive must be stable, not change the carrierNo by-pass, centralised productionNeed for a comprehensive approachPackaging, evaporationAccess of all the population to the fortified
foodPolicy and protection of the marketWho pays?Success story of Iran


Food habits
Very limited approach, food reflects iodine soil content

Control complications
Need for intensive follow upChanging consumption patterns in saltVariations in salt consumption Transient hyperthyroidism