Introduction to Neuro Rehab Modalities
15
Introduction to Neuro Rehab Modalities Paul Chuwn Lim, M.D. Medical Director of Swedish Rehabilitation Services Swedish Health Services Swedish Physical Medicine & Rehabilitation Medical Director of Swedish Neurological Rehabilitation Medicine Swedish Medical Group May 14 th , 2021 14 th Annual Cerebrovascular Symposium
Transcript of Introduction to Neuro Rehab Modalities
Introduction to
Neuro Rehab Modalities
Paul Chuwn Lim, M.D.Medical Director of Swedish Rehabilitation Services
Swedish Health Services
Swedish Physical Medicine & Rehabilitation
Medical Director of Swedish Neurological Rehabilitation Medicine
Swedish Medical Group
May 14th, 2021
14th Annual Cerebrovascular Symposium
Outline
• Understand the evolution of rehab modalities & devices
• Cursory description of devices (low → high tech)
• Compare conventional rehab to newer strategies
• Barriers to wide-spread use of newer modalities
• No Disclosures
2

What path?
3
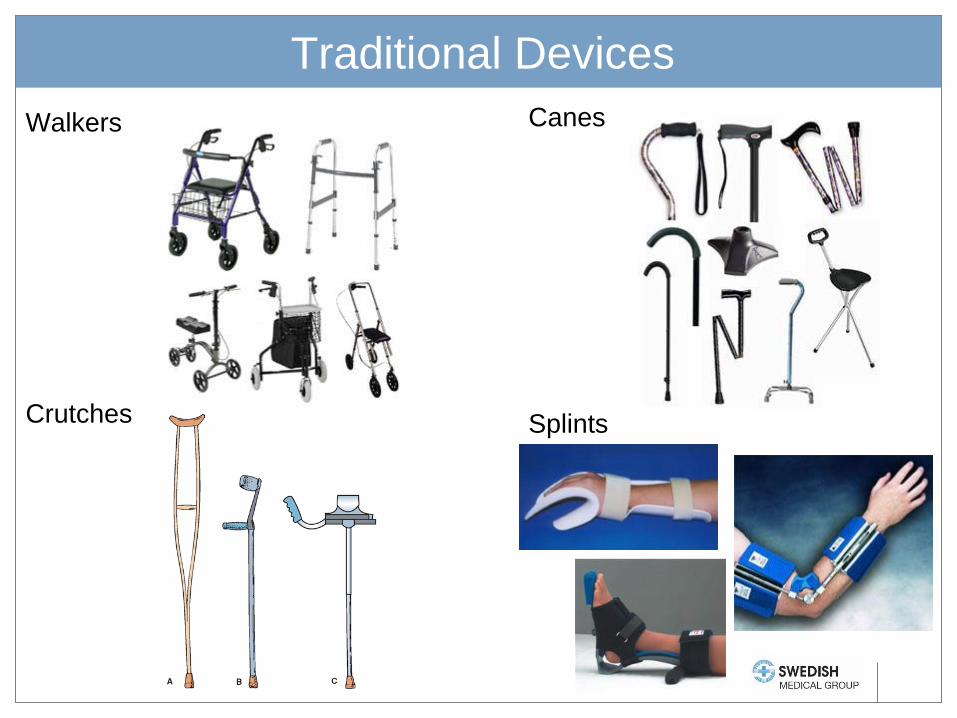
Traditional Devices
Walkers
Crutches
Canes
Splints

Widely Available Devices
Body Weight Wheelchairs
Supported Treadmill
Orthotics
FES
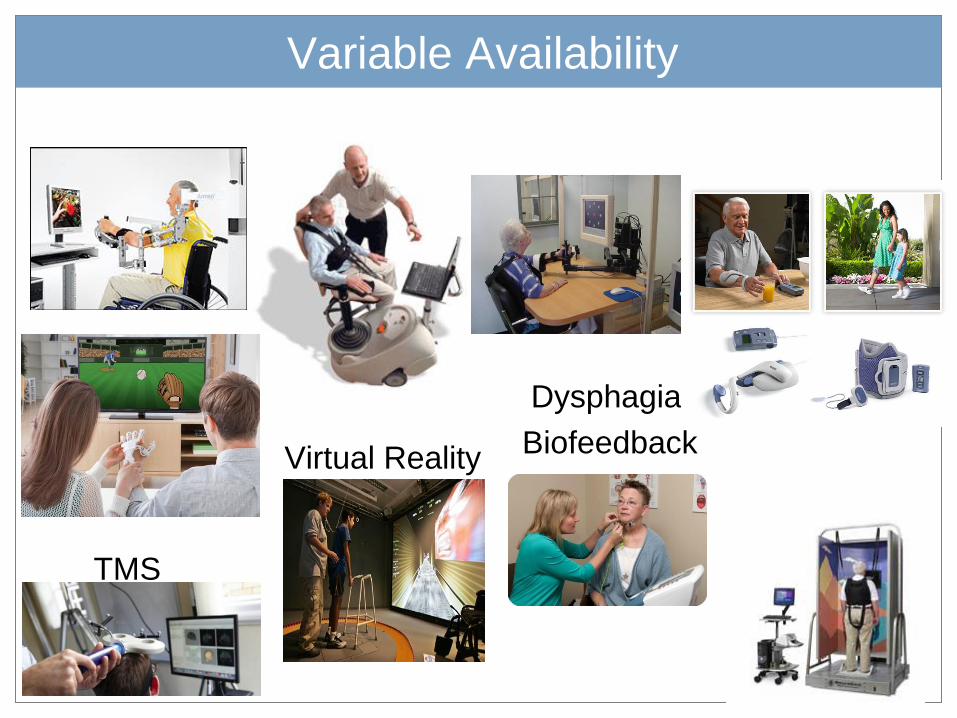
Variable Availability
Virtual Reality
TMS
Dysphagia
Biofeedback

Many, Many More Devices
Limits of Conventional Therapies
• Requires hours of therapy time
– Increasing therapy labor costs
• UK: ~10% of national stroke budget
• Aging population (ex: Japan) relative to trained therapists
– Rural access to specialists
• Frequent safety risks for patients & therapists
• Lacks repetition found to optimize neuroplasticity
– Body Weight Supported training vs conventional over-ground
– Up to 1000 gait cycles in 30 min vs <50 cycles
• Low Compliance: home > hospital
– Less engaging/entertaining, 1:1 hands-on supervision
8
Benefits of Conventional Therapies
• Teaches compensatory strategies
– Hemi technique for walking, dressing, eating, and other ADLs
• Easily adaptable and personalized
• Whole body > segmental approach
• Compensate for abnormal movement patterns
• Accounts for emotional & clinical status quickly
• Accounts for cognitive and sensory deficits
– Complex tasks such as stairs, toileting, gait on uneven terrain, etc.
– Performance of actual tasks instead of simulated tasks
• Use of cheaper and more available assistive devices
9
Rehabilitation Methods
• Muscle Re-education Approach (1920s)
• Neurodevelopmental Approach (1940-70s)
– Sensorimotor Approach (Rood, 1940s)
– Movement Therapy Approach (Brunnstrom, 1950s)
– NeuroDevelopmental Technique (Bobath, 1960-70s)
– Proprioceptive Neuromuscular Facilitation (Knott/Voss, 1960-70s)
• Motor Relearning Program for Stroke (Carr/Shephard, 1980s)
• Constrained Induced Movement Therapy (Taub, 1980s)
• Contemporary Task-Oriented Approach (Shumway-
Cook/Woolacott, 1990s)
• High-Intensity Gait Training 2010s-present
High-Intensity Gait Training
• Conventional inpatient PT works on progressive function
– Static/dynamic sitting and standing balance, transfers, pre-gait
– If sufficiently improved enough, then will start gait activities
– Gait activities also slowly advanced progressively
• Emphasis shifting towards earlier and higher intensity gait
training – paradigm shift for older inpatient PTs
– Much more therapy minutes dedicated for gait >> pre-gait activities
• Practice, practice, practice – intensity makes perfect
• Aim to correct biomechanical and kinematic errors earlier
• Emphasis on repetition, gait efficiency, overall function
• Recommended by the Academy of Neurologic Physical
Therapy with a Clinical Practice Guideline in Jan 2020
11
Paradigm Shift
• Conventional therapy shifting
towards earlier gait and
technology assisted rehab
• Move away from hospital care to
home/clinic based care
• Technological advances– Smaller processors, more complex software
– Light weight/stronger materials, better batteries
– Telemedicine: distant supervision, multiple pts
– Innovative human-machine interfaces
– Accurate physiological sensors and actuators
• Haptics, gyroscopes, EMG, FES, electrocortical
12

Cutting Edge Technology
Exoskeleton Devices
Robotic Gait
Prosthetics
Brain Computer Interfaces
EEG Intracortical
EMG/FES NASA
+/- mirrors
Paradigm Shift
• Economic and marketing forces
– Marketing advantage for rehab facilities (East/Midwest > West)
– Widespread use leads to cheaper gaming devices
– Commercialization of devices
– Patients and families drawn to new technology
– ? ultimate rationale: escalating labor costs
• Debate on its inevitability
• Benefits of robotics
• Simulated tasks when actual tasks are dangerous
• More entertaining therapy (increase compliance)
• Increased repetition to promote neuroplasticity
• Replace missing or damaged body parts
• Psychological benefits
14
Barriers to Wide Spread Use
• Expensive devices generally not covered by insurance
– No compelling evidence of its superiority
• Primarily viewed as an adjunct to conventional therapy
– Era of healthcare cost containment
– Primarily at large rehab centers (east > mid-west > west)
• Generally from research or rehab facility marketing funds
• No additional therapy billing charges
• Marketing advantage primarily in competitive rehab environments
– Limited ability for out-of-pocket purchase by vast majority of pts
15