
Into the Brain and Beyond
76
UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND DEPARTMENT OF NEUROSURGERY INTO THE BRAIN AND BEYOND PERFECTING THE NEUROSURGICAL HEALING OF TODAY INVENTING THE NEUROSURGERY OF TOMORROW
-
Upload
ucla-neurosurgery -
Category
Documents
-
view
232 -
download
5
description
An inside look at UCLA Neurosurgery
Transcript of Into the Brain and Beyond

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND
DEPARTMENT OF NEUROSURGERY
INTO THE BRAIN AND BEYONDPERFECTING THE NEUROSURGICAL HEALING OF TODAY
INVENTING THE NEUROSURGERY OF TOMORROW
TABLE OFThe New Gold StandardUCLA HEALTH: AN OVERVIEW
Message from the ChairmanNEIL A. MARTIN, MD, FAANS
Awards & RecognitionsUCLA NEUROSURGERY DEPARTMENT
A Truly Multidisciplinary TeamUCLA NEUROSURGERY FACULTY OVERVIEW
Mapping the Future of Neurosurgical HealingA YEAR IN REVIEW
Pioneers in Minimally-Invasive SurgeryCUTTING EDGE TECHNIQUES & PROCEDURES
The Perfect Patient ExperienceUCLA NEUROSURGERY CLINICAL QUALITY PROGRAM
World-Class, Patient-Centered CareBRAIN TUMOR PROGRAM
4
6
8
9
12
14
16
18
UCLA NEUROSURGERY
Cover image: White Matter Fibers, HCP Dataset Red Corpus Callosum courtesy of Scientific Visualization Team, Laboratory of Neuro Imaging.www.humanconnectomeproject.org
RECOGNITIONSAND
AWARDS
Top 10 Neurosurgery Department according to
U.S. News and World Report
No. 5 in the world for most research papers published in
medical journals
Joint Commission National Quality Approval awarded to
UCLA Stroke Center
The UCLA Stroke Center is a designated center of the NIH-funded
Specialized Programs of Translational Research in Acute Stroke (SPOTRIAS)
No. 2 in National Institutes of Health (NIH) Research Grants at
$5,943,956

CONTENTS24
28
30
34
42
44
50
52
54
60
66
72
74
Leaders In Next-Generation,Hi-Definition NeurosurgeryPITUITARY TUMOR PROGRAM
Revolutionizing Skull Base SurgeryUCLA SKULL BASE TUMOR PROGRAM
World-Renowned Pioneers & ExpertsSTEREOTACTIC RADIOSURGERY PROGRAM
World’s Most Comprehensive Stroke CenterUCLA STROKE CENTER
The Discovery of Stimulating Memory inthe Human BrainITZHAK FRIED, MD, PHD
More Than 50 Years of ExcellenceADULT EPILEPSY SURGERY PROGRAM
Saving Lives on the Battlefields,Sports Fields and PlaygroundsUCLA BRAIN INJURY RESEARCH CENTER
Inventing the Future of Neurocritical CareNEUROCRITICAL ICU
The Movement Disorder Experts NEUROMODULATION & NEUROBIONICS PROGRAM
A World-Class Team of Integrated SpecialistsUCLA SPINE CENTER
World-Class Pediatric Epilepsy ExpertsPEDIATRIC EPILEPSY SURGERY PROGRAM
Global Neurosurgery InstituteTHE EDIE & LEW WASSERMAN BUILDING
Global LeadersUCLA NEUROSURGERY: OUR DEPARTMENT IN SUMMARY
Linda M. Liau, MD, PhD, marked the milestones for two patients living 10 years beyond glioblastoma multi-forme, who were enrolled in the first personalized brain cancer vaccine de-veloped at UCLA and now in Phase III clinical trials in America and Europe. Dr. Liau recently received the presti-gious Athena Award.
Itzhak Fried, MD, PhD, was among the top 10 finalists for the Global B.R.A.I.N Prize competition (Break-through Research and Innovation for Neurotechnology) inspired by Israeli President Shimon Peres and Israel Brain Technologies. He is recognized among the top neuro-scientists in the world for his recent discovery of boosting memory in the gateway of the hippocampus, the mainframe of human memory.
Nestor Gonzalez, MD, received the Innovative Science Award from the American Heart Association for his pioneering research in the prevention and treatment of stroke.
Isaac Yang, MD, is honored to receive the Award for Excellence in Education for his continued bril-liance and innovation to teaching in clinics and the classroom.
Gary W. Mathern, MD, was appointed Co-Editor-in-Chief of Epilepsia, the official medical journal of the Interna-tional League Against Epilepsy (ILAE).
Dan Lu, MD, PhD, & V. Reggie Edger-ton, PhD, received a $6 million grant from the NIH to study groundbreaking stimulation for recovering function in patients with spinal cord injury.
Nancy McLaughlin, MD, PhD, re-ceived a grant from the University of California to improve and perfect neurosurgical care.
UCLA NEUROSURGERY
FACULTY AWARDSAND
GRANTS

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND4 | UCLA HEALTH: THE NEW GOLD STANDARD
“OUR PRESCRIPTION OF EXCELLENCE IS TO PROVIDE THE BEST PATIENT
EXPERIENCE WITH EVERY PATIENT, EVERY ENCOUNTER, EVERY TIME.”
Joint Commission Gold AwardCertified as a Comprehensive Stroke Center by the Joint Com-mission, receiving their Gold Award for quality.
Comprehensive Stroke CenterCertified as a Comprehensive Stroke Center by the American Heart Association/American Stroke Association.
Best in the West, U.S. News & World ReportRanked #1 hospital in the West for 23 consecutive years, top 5 in the nation, and Best Hospital Honor Roll for 24 consecutive years, Ronald Reagan UCLA Medical Center is the #1 hospital in California and the West Coast, receiving the Best in the West honor from US News & World Report.
t UCLA Health, our mission is to deliver leading-edge patient care, research and education. Our vision is to heal humankind,
one patient at a time, by improving health, alle-viating suffering and delivering acts of kindness. With a culture of caring, compassion, dignity and privacy, our integrated approach is focused on bringing world-class experts together to care for the patient and family as one.
A
THE NEWGOLD STANDARD
UCLA HEALTH

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND
BUILT FOR MIRACLES RONALD REAGAN UCLA MEDICAL CENTERLevel 1 Trauma Center: Our trauma center represents the highest level of emergency care to tackle any traumatic injury, 24 hours a day, 7 days a week, 365 days a year.
Neurosurgical Operating Rooms: We can ac-commodate more than 2,000 cases a year.
• High-definition, magnification video systems for microsurgery• Electrophysiologic equipment for brain monitoring• Intraoperative angiography• Frameless stereotactic imaging workst- ation (BrainLAB) for neuro-navigation
Stereotactic Radiosurgery: Gold-standard noninvasive, bloodless surgery instrumenta-tion, Novalis TX equipped with GPS-like image guidance system, 3D-multiplanar computer-ized models for high-resolution brain mapping.
Interventional Imaging Suite: Interventional angiography suites equipped with 3D rotational angiography for endovascular procedures.
Comprehensive Stroke Center: Our Brain Attack Team specializes in rapid stroke care response using the latest in neurosurgical interventions and neuro-intensive care at UCLA and around Southern California.
Edie Baskin Bronson & Richard “Skip” Bronson Cerebral Blood Flow Laboratory: Clinical tran-scranial Doppler evaluations and cerebral blood flow testing on patients.
Singleton Neuro-ICU 24-7• Continuous EEG monitoring• 3 Tesla MRI scanners and PET-CT Scan for acute crises • Cerebral microdialysis • Brain oximetry • Transcranial Doppler• World’s first ICU Robot• Comprehensive ICU supercomputing system for predictive medicine
96-99%96 TO 99 PERCENTILE IN PATIENT
SATISFACTION ACCORDING TO INDEPENDENT NATIONAL SURVEYS
1.5 MIL.1.5 MILLION PATIENTS ARE SEEN IN MORE
THAN 80 COMMUNITY-BASED CLINICS OF THE UCLA FACULTY PRACTICE
UCLA HEALTH: THE NEW GOLD STANDARD | 5
80,00080,000 PATIENTS ARE
TREATED ANNUALLY AT UCLA HOSPITALS
24 YR.RONALD REAGAN MEDICAL CENTER RANKED #1 HOSPITAL IN THE WEST
FOR 24 CONSECUTIVE YEARS

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND
MESSAGE FROM
THE CHAIRMAN
6 | MESSAGE FROM THE CHAIRMAN
ear colleagues and friends, As neurosurgeons and neuro-scientists, we marvel daily at the capacity of the human brain
to repair and heal itself. Yet it is our patients’ courage to triumph over the most devastat-ing conditions that inspires us to continue our exploration into the inner space of the brain and spine, as we unearth solutions to the most critical neurological problems that face millions of Americans today. The recently-launched national initiative to map the human brain feels similar to the country’s ambition to land a man on the moon. In my opinion, our team of biomedical scientists and surgeons are closer than ever to unraveling the mys-teries of some of the most puzzling diseas-es such as cancer, stroke, traumatic injury,
epilepsy, Parkinson’s disease, Alzheimer’s disease and autism.
In reporting on our innovative technology and latest research endeavors, we share the stories of how we have profoundly improved the quality of life and, in many cases, saved the lives of our patients and their families. We use a 360-degree integrative and multidis-ciplinary team approach to patient care that translates into superior clinical outcomes. Ronald Reagan UCLA Medical Center consis-tently ranks number one on the West Coast and in the top five in the nation, according to U.S. News and World Report. The UCLA De-partment of Neurosurgery also ranks year after year in the top 10 in the world accord-ing to U.S. News and World Report. Our high annual rankings are the result of our patients’
successes combined with our innovation to translate science and technology into medical breakthroughs at the bedside.
Our UCLA Brain Injury Research Center translates the biology of traumatic brain injury into real-world treatments to raise the standard of care and protect our soldiers on the battlefield, athletes on the sports field and children on the playground. Their expertise has led to advising the U.S. Military, the NFL and the recent release of the first evidence-based guidelines for sports concussions.
The UCLA Stroke Center continues to be a world leader in research and treatment of cerebrovascular disease. Certified by the Joint Commission as a Comprehensive Stroke Center and funded by a prestigious National Institutes of Health SPOTRIAS
D
UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND
(Specialized Programs of Translational Re-search in Acute Stroke) grant, it is one of just eight such centers in the country. We reach beyond our community to serve the entire Southern California region with the Telestroke unit, and hospitals across the country through our Tele-ICU network, which beams in a neurointensivist via telemedicine to treat critical patients in community hospi-tals lacking this expertise. Our endovascular devices invented at UCLA circle the globe treating patients with stroke.
The UCLA Brian Tumor Program contin-ues to shine as a beacon of hope, carrying a record of patients with brain tumors living longer than patients treated at any other hos-pital. Our personalized brain cancer vaccine, DCVax, is the first of its kind and is currently in
Phase III clinical trials in 46 centers through-out America. It is on the road to FDA approval as well as clinical trials throughout Europe. Using this vaccine, we are harnessing the pa-tient’s immune system, genetics, pathology, brain mapping and a wide database of bioin-formatics to optimize outcomes.
Through a recently-awarded NIH grant in the UCLA Spine Center, we are innovat-ing next-generation neurobionics and neu-romodulation with interventions that may enable patients with severe paralysis to stand, step, and regain voluntary muscle control once lost to injury. Additionally, our neuroscientists recently discovered that stimulating the entorhinal cortex in the brain could lead to boosting memory in patients with Alzheimer’s disease.
Looking ahead, we are on the threshold of opening the Global Neurosurgery Institute in the Edie and Lew Wasserman Building at UCLA to deploy the latest advancements in telemedicine that will surround our patients with world-class expertise. Today, we will share how we make beating impossible odds possible, by staying focused on our mission of working together as a team to provide ex-ceptional patient care and invent the future of neurosurgery.
MESSAGE FROM THE CHAIRMAN | 7
Neil A. Martin, MD, FAANS PROFESSOR & W. EUGENE STERN CHAIR IN NEUROSURGERY

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND8 | AWARDS & RECOGNITIONS
We are honored to serve our country’s veterans through our collabo-ration with the West Los Angeles Veterans Administration Hospital. We provide a full-time staff of world-class neurosurgical experts ded-icated to the men and women of the US Armed Forces. Our team is privileged to manage an average of nearly 100 cases a week referred from around Southern California and across the United States.
Our team is dedicated to excellence in patient care and advanc-ing research throughout the Greater Los Angeles community. We provide neurosurgical expertise in the Ronald Reagan UCLA Medical Center, Mattel Children’s Hospital UCLA, UCLA Medical Center (Santa Monica), UCLA Spine Center (Santa Monica), and Harbor-UCLA Medical Center.
UCLA NEUROSURGERY SERVES
WRITING THE GUIDELINES FOR THE MEDICAL COMMUNITY:
Linda M. Liau, MD, PhDEditor-in-Chief, Journal ofNeuro-Oncology
Gary W. Mathern, MDCo-Editor-in-Chief, Epilepsia
James I. Ausman, MDSurgical Neurology International
Langston T. Holly, MDServes on the Editorial Board of the Journal of Neurosurgery – Spine
David A. Hovda, PhDServes on Editorial Boards of Journal of Neurotrauma and the Journal of Cerebral Blood Flow& Metabolism
EDITORS OF LEADING NEUROSURGICAL JOURNALS
UCLA NEUROSURGERY DEPARTMENT
AWARDS &RECOGNITIONS
JOINT COMMISSION NATIONAL QUALITY APPROVAL AWARDED TO
UCLA STROKE CENTER
7 CLINICIANS IN THE UCLA NEUROSURGERY DEPARTMENT VOTED
BEST DOCTORS IN AMERICA
10 TOP SURGEONS VOTED BY THE CONSUMERS’ RESEARCH COUNCIL
OF AMERICA
THE UCLA STROKE CENTER IS A DESIGNATED CENTER OF THE NIH-FUNDED SPECIALIZED
PROGRAMS OF TRANSLATIONAL RESEARCH IN ACUTE STROKE (SPOTRIAS)
TOP 10 NEUROSURGERY DEPARTMENT ACCORDING TO
U.S. NEWS AND WORLD REPORT
NO. 5 IN THE WORLD FOR MOST RESEARCH PAPERS PUBLISHED
IN MEDICAL JOURNALS
NO. 2 IN NATIONAL INSTITUTES OF HEALTH (NIH) RESEARCH GRANTS
AT $5,943,956

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND FACULTY OVERVIEW | 9
The mission of the Department of Neurosurgery is to invent the future of neurosurgery by improving neurosurgical treatment of brain and spinal disease through innovative research and development, by providing and advancing the highest level of surgical and medical care for our patients and by training the next generation of neurosurgical pioneers.
FACULTY OVERVIEW
OUR MISSION
Neil A. Martin, MD, FAANSPROFESSOR & W. EUGENE STERN CHAIR IN NEUROSURGERY & CO-DIRECTOR OF
THE UCLA STROKE CENTER
Linda M. Liau, MD, PhD PROFESSOR & VICE CHAIR OF
ACADEMIC AFFAIRS & DIRECTOR OF THE UCLA BRAIN TUMOR PROGRAM
Langston T. Holly, MDASSOCIATE PROFESSOR & CO-VICE
CHAIR OF CLINICAL AFFAIRS FOR THE DEPARTMENT OF NEUROSURGERY &
DIRECTOR OF THE UCLA SPINE CENTER
Marvin Bergsneider, MD PROFESSOR & CO-VICE CHAIR OF CLINICAL AFFAIRS, RESIDENCY
PROGRAM DIRECTOR
David A. Hovda, PhD PROFESSOR & VICE CHAIRMAN OF
RESEARCH AFFAIRS & DIRECTOR OF THE BRAIN INJURY RESEARCH CENTER
EXECUTIVE LEADERSHIP
he faculty members of the UCLA Department of Neuro-surgery are experts in the di-agnosis, treatment and man-
agement of diseases in the brain and spine. We consistently rank in the top 10 programs in the nation according to U.S. News and World Report. The strength of the UCLA Department of Neurosurgery is the collaboration between its multidisciplinary teams of experts in every relevant field focused on a specific disease or
disorder of the brain or spine. Our patients are the beneficiaries of centralized, world-class expert care provided by specialists who have spent a lifetime dedicated to discovering the best treatments to target a disease at every level. Our clinicians, scientists and research-ers rank 5th in world for published medical journal studies that have unearthed the evi-dence to write the guidelines and standards of care for the medical community. Our team ranks 2nd in National Institutes of Health
funding. We deliver the latest translations of basic science into cutting-edge treatments at the bedside for our patients. As leaders in neurosurgery, we continue to attract and train the next generation of neuroscientists and neurosurgical pioneers, mapping new frontiers of the human brain and discovering cures for the most complex neurological dis-eases facing our families today, and our chil-dren’s families tomorrow.
T

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND
CLINICIANSJames I. Ausman, MD, PhD CLINICAL PROFESSOR
Gary W. Mathern, MD PROFESSOR IN RESIDENCE & DIRECTOR OF THE PEDIATRIC EPILEPSY SURGERY PROGRAM & PEDIATRIC NEUROSURGERY PROGRAM
Ulrich Batzdorf, MD PROFESSOR & EXECUTIVE DIRECTOR OF SPINAL NEUROSURGERY
Duncan Q. McBride, MD ASSOCIATE CLINICAL PROFESSOR & CHIEF OF NEUROSURGERY AT HARBOR-UCLA MEDICAL CENTER
Donald P. Becker, MDDISTINGUISHED PROFESSOR & CHAIRMAN EMERITUS OF NEUROSURGERY
Nancy McLaughlin,MD, PhD ASSISTANT CLINICAL PROFESSOR OF NEUROSURGERY
Manuel M. Buitrago Blanco, MD, PhDASSISTANT PROFESSOR OF NEUROSURGERY, NEUROLOGY & NEUROCRITICAL CARE
Nader Pouratian,MD, PhDASSISTANT PROFESSOR & DIRECTOR OF THE NEUROSURGICAL MOVEMENT DISORDERS PROGRAM
Antonio De Salles, MD, PhD PROFESSOR & CO-DIRECTOR OF THE STEREOTACTIC SURGERY PROGRAM, & CO-DIRECTOR OF THE RADIOSURGERY PROGRAM
Paul M. Vespa, MD, FCCM, FAAN PROFESSOR IN RESIDENCE OF NEUROSURGERY & NEUROLOGY & DIRECTOR OF THE NEUROCRITICAL CARE PROGRAM
Duc H. Duong, MDCLINICAL PROFESSOR
Isaac Yang, MDASSISTANT PROFESSOR & NEUROSURGEON
Melvin Cheatham, MDCLINICAL PROFESSOR & UCLA DEPARTMENT OF NEUROSURGERY ADVISORY BOARD
Fredric L. Edelman, MD CLINICAL PROFESSOR
John G. Frazee, MDCLINICAL PROFESSOR & DIRECTOR OF THE NEUROENDOSCOPY PROGRAM & CHIEF OF NEUROSURGERY AT WEST LOS ANGELES VA MEDICAL CENTER
Itzhak Fried, MD, PhD PROFESSOR & DIRECTOR OF THE EPILEPSY SURGERY PROGRAM.
Nestor Gonzalez, MD, FAHAASSISTANT PROFESSOR OF NEUROSURGERY & RADIOLOGICAL SCIENCES & RUTH AND RAYMOND STOTTER ENDOWED CHAIR IN NEUROSURGERY
Daniel Lu, MD, PhD ASSISTANT PROFESSOR OF NEUROSURGERY
Dennis R. Malkasian, MD, PhD ASSOCIATE CLINICAL PROFESSOR OF NEUROSURGERY
Jean-Philippe Langevin, MDASSISTANT PROFESSOR OF NEUROSURGERY
Jorge Lazareff, MDPROFESSOR OF NEUROSURGERY
Alessandra Gorgulho, MDCLINICAL INSTRUCTOR IN STEREOTACTIC SURGERY
Bob Shafa, MD ASSISTANT PROFESSOR
10 | FACULTY OVERVIEW

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND
RESEARCH SCIENTISTS
JOINT APPOINTMENTS
Valeriy I. Nenov, PhD ADJUNCT PROFESSOR & DIRECTOR OF THE BRAIN INTENSIVE MONITORING & MODELING LABORATORY
Mayumi Prins, PhD ASSOCIATE PROFESSOR IN RESIDENCE & DIRECTOR OF THE UCLA TRAUMATIC BRAIN INJURY PREVENTION & EDUCATION PROGRAM
Reza Jahan, MD ASSISTANT PROFESSOR, INTERVENTIONAL NEURORADIOLOGY & NEUROSURGERY
Robert M. Prins, PhD ASSOCIATE PROFESSOR IN RESIDENCE
Scott Krahl, PhD ASSOCIATE PROFESSOR & NEUROPHYSIOLOGIST
Richard L. Sutton, PhD ADJUNCT ASSOCIATE PROFESSOR
Tom Belle Davidson, MDDIRECTOR OF NEURO-ONCOLOGY, MATTEL CHILDREN’S HOSPITAL UCLA WITH JOINT APPOINTMENT IN NEUROSURGERY
Anthony P. Heaney, MD, PhD ASSOCIATE PROFESSOR, ENDOCRINOLOGY & NEUROSURGERY
Thomas C. Glenn, PhD ADJUNCT ASSISTANT PROFESSOR & CO-DIRECTOR OF THE CEREBRAL BLOOD FLOW LABORATORY
Fernando Gómez-Pinilla, PhD PROFESSOR & DIRECTOR OF THE NEUROTROPHIC RESEARCH LABORATORY
Grace Griesbach, PhD ASSISTANT PROFESSOR
Neil G. Harris, PhD ASSOCIATE PROFESSOR IN RESIDENCE
Nasim Afsar-manesh, MD ASSISTANT CLINICAL PROFESSOR, INTERNAL MEDICINE & NEUROSURGERY
A. Nick Shamie, MD ASSISTANT PROFESSOR OF ORTHOPAEDIC SURGERY & NEUROSURGERY
FACULTY OVERVIEW | 11
Carol A. Kruse, PhD PROFESSOR
Gary Duckwiler, MD PROFESSOR, INTERVENTIONAL NEURORADIOLOGY & NEUROSURGERY
Xiao Hu, PhD ASSOCIATE PROFESSOR IN RESIDENCE
Christopher C. Giza, MD ASSOCIATE PROFESSOR IN RESIDENCE WITH SECONDARY APPOINTMENT IN PEDIATRIC NEUROLOGY

12 | A YEAR IN REVIEW
A YEAR IN REVIEWMAPPING THE FUTURE OF NEUROSURGICAL HEALING
1.
4.
UCLA Stroke Center Awarded ‘Comprehensive Stroke Center’ Certification
Read More – Pg. 39
3.
David A. Hovda Appointed to the Defense Health Board, Advising Secretary of Defense
Read More – Pg. 50
7.
2.
6.
5.
UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND
Intraoperative CT Guided Endoscopic Surgery, Breakthrough for Brain Hemorrhage Patients
Read More – Pg. 36
New Method for Memory Strengthening Could Lead to Treatment of Alzheimer’s Disease
Read More – Pg. 42
Congress of Neurological Surgeons Grants Synthes Skull Base Surgery Award for SRT Study
American Heart Association Innovative Science Award for Stroke Prevention Research
Read More – Pg. 37
Brain Cancer Vaccine Team Celebrates Patient Living 10Years and Phase III Clinical Trial
Read More – Pg. 22

A YEAR IN REVIEW | 13
8.
9.
12.
13.
14.
11.
10.
s mankind advances its technologies in communication, medicine and other vital sciences, the world is fast de-creasing in scale. Today, the lifesaving breakthroughs that take place in our laboratories and operating rooms
can be and are exported around the world with lightening speed. This fact sheds new light on the value of the work our doctors and research scientists do every day. Our work, once limited to those in our own back-yard, now affects and improves the lives of millions around the globe.
Driven by a common spirit of exploration, the members of the UCLA Department of Neurosurgery are pushing and creating new boundar-ies in the field of neuroscience and truly mapping the future of neuro-surgical healing. Pioneering and innovation have long been ingrained into the tradition of our department and its many comprehensive programs. Thus today we are proud to celebrate yet another year of invaluable accomplishment and contribution to the world of neurosci-ence and neurosurgery.
A
UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND
NIH Grant for $6 Million to Restore Spinal Cord Function
Read More – Pg. 62
NIH Grant to Develop Predictive Monitoring System, Using IBM Big Data Software
Read More – Pg. 53
500th Deep Brain Stimulation Treatment Performed at UCLA
Read More – Pg. 56
UCLA Announces First Evidence-Based Guidelines for Sports Concussions
Read More – Pg. 50
EVA the Robo-Doc Joins the Neuro-ICU Team at UCLA
Read More – Pg. 52
UCLA Spine Center Opens in Santa Monica, CA
Mystery of Rare Pediatric Epilepsy Unlocked – Possible Key to Understanding Autism
Read More – Pg. 68

UCLA neurosurgeons pioneer the field of minimally-invasive brain and spine surgeries.
No incision, bloodless brain and spine surgery, with no anesthesia.
Microsurgical operations using tiny or no incisions lead to enhanced outcomes and shorter hospital stays.
UCLA operating suites are among the most advanced in the world.
Microcraniotomy experts in dime-size incisions beneath the eyebrow or under the hairline.
Invented the gold-standard of non-invasive brain and spine surgery.
14 | PIONEERS IN MINIMALLY-INVASIVE SURGERY
Inventing the Future of Neurosurgery
NON-INVASIVE STEREOTACTIC RADIOSURGERYOur specially trained neurosurgeons invented the gold-standard for non-invasive brain surgery using stereotactic radiosurgery. The Novalis Tx delivers shaped beams of radiation, using the BrainLab image-guidance system to maximize precision in treatment while protecting vital brain tissue.
• Skull base tumors › Meningiomas › Chordomas › Craniopharyngiomas
• Arteriovenous malformations• Metastatic brain tumors• Pituitary tumors• Primary tumors
• Primary malignant tumors• Spinal tumors• Trigeminal neuralgia
EXPANDED ENDOSCOPIC ENDONASAL APPROACH
• Craniopharyngiomas• Chrodomas• Meningiomas
• Pituitary tumors• Cerebrospinal fluid leaks• Colloid cyst
• Neurocysticercosis
The UCLA team is one of a few in the country utilizing the Expanded Endoscopic Endonasal Approach. The team of neurosurgeons and sinus, head and neck surgeons routinely use an endoscope, 4mm in diameter, with a high definition video camera on the tip and microsurgical instruments to enter the nasal passage. This eliminates the need for a facial incision or craniotomy to remove tumors.
ENDOSCOPIC-ASSISTED MICROSURGERY Endoscopic-assisted brain surgery treats trigeminal neuralgia and its accompanying severe facial pain with remarkable precision and positive outcomes. Microvascular decompression of the facial nerve draws on microsurgery to separate the blood vessel causing compression on the facial nerve. The surgery entails making a small incision about the size of a nickel behind the ear and uses neuro-navigation to enter the brain stem and move the trigeminal nerve away from the blood vessel. The pain is instanta-neously stopped and cured in up to 90 percent of patients.
• Trigeminal neuralgia • Hemifacial spasm • Vestibular nerve section
UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND
MINIMALLY–INVASIVE SURGERY
PIONEERS IN

Neuronavigation using GPS-like precision in navigating through vital control centers of the brain.
Neuroendoscopy, high-definition video cameras for optimizing visibility.
Pioneers in endovascular treatments employ coils and blood vessel routes into the brain, while avoiding surgery to repair vascular malformations.
Experts in the expanded endoscopic endonasal approach, utilizing the natural nasal passage to the brain, thus eliminating the craniotomy.
PIONEERS IN MINIMALLY-INVASIVE SURGERY | 15
EXPERTS IN MICROCRANIOTOMY EYEBROW INCISIONSUCLA neurosurgeons draw on minimally-invasive microcraniotomy surgical techniques to remove brain tumors or vascular malformations that would normally require a long scalp incision and a larger bony opening. This eyebrow incision technique conceals a facial scar and minimizes damage to healthy brain tissue. Using CT-Scan image guidance and endoscopic assistance, minimally-invasive brain surgery, called Intraoperative CT guided Endoscopic Surgery (ICES), is in clinical trials to remove blood in the event of a hemorrhagic stroke. These techniques are revolutionizing neurosurgery.
MINIMALLY-INVASIVE SPINE SURGERYNeurosurgeons specially trained in spine surgery utilize minimally-invasive keyhole incisions, ½ inch in diameter, to repair the spine and thus eliminate discomfort, lessen recovery times, reduce trauma and shorten hospital stays. UCLA is a pioneer in stereotactic radiosurgery, which uses an invisible blade of shaped beam radiation and an image-guidance system to remove spinal tumors and other abnormalities.
• Artificial disc• Kyphoplasty• Laminectomy
• Lumbar fusion• Microdisectomy• Pedicle screw placement
• Posterior cervical disectomy• Spinal mass & tumor resection• Thoracic discectomy
MINIMALLY-INVASIVE ENDOVASCULAR EXPERTS Combining our expertise in keyhole-sized incisions with CT-Scan image guidance, we use blood vessels as routes to vascular malformations, minimizing the need for a craniotomy. Guglielmi detachable coils (GDCs) invented at UCLA have transformed the treatment of intracranial aneurysms around the world. Similarly, our MERCI clot retrieval device made it possible to stop a stroke in progress. It was recently modified to become the SOLITAIRE Flow Restoration Device, for restoring blood flow after a stroke.
• Arteriovenous malformations (AVM)• Cerebral aneurysms
• Meningioma (preoperative embolization)• Stroke
UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND
ombining our spirit of inno-vation and mission for excel-lent patient care, we bring the future forward as we invent the
next generation of neurosurgery today. UCLA neurosurgeons have pioneered minimally-in-vasive, endoscopic brain and spine surgery to improve outcomes and lessen recovery times. Our highly-experienced neurosurgeons lead the field, having performed thousands of min-imally-invasive, non-invasive and endovascu-lar surgeries to repair the brain and spine.
Ronald Reagan UCLA Medical Center operat-ing suites are among the most advanced in the world. Using image guidance systems com-bined with endoscopic instruments and high-definition video cameras, we can perform brain surgery using natural nasal passage-ways to the brain or through dime-size inci-sions. These techniques replace the need for an open craniotomy and long scalp incisions. Our specially trained neurosurgeons are at the forefront of neuronavigation and neuro-endoscopy innovations. Their breakthrough
techniques and technology have led to access-ing tumors and vascular malformations in areas of the brain and spine, which were once thought inoperable 15 years ago. Though these tumors and malformations often lie deep within the brain, angled-lens endoscopes give the neurosurgeons visual access to operate around corners, thus improving their ability to completely magnify and remove the tumor while simultaneously reducing complications.
C

CLINICAL QUALITY PROGRAMUCLA NEUROSURGERY
THE PERFECT PATIENT EXPERIENCE, EVERY TIME, ANY TIME, 24-7s clinicians and leaders on the frontlines of medicine at UCLA, we have the experience, ingenuity and most im-portantly, the responsibility to reform healthcare from the inside. UCLA is one of the premier academic medical
centers that set the standards for medical care in the country and the world. In the Neurosurgery Department’s three-part mission dedicated to patient care, teaching, and research, we endeavor to develop a system to standardize quality that can be implemented throughout the Ronald Reagan UCLA Medical Center, UCLA Health, UC campuses and beyond.
We believe that by diagnosing the deficits in healthcare through our experience in the trenches, we can contribute to repairing the U.S. healthcare system with a strategic approach to quality care. For over a decade, we have ranked in the top five hospitals in the country and “Best in the West” according to U.S. News and World Report. We are in a unique
position to be an example for the rest of the medical community, while understanding that upholding the highest standards also means refining our internal systems and innovating new systems.
Neil A. Martin, MD, Professor & W. Eugene Stern Chair in Neuro-surgery, formed the UCLA Neurosurgery Clinical Quality Program to improve our patient care, enhance patient safety, increase efficiency and reduce costs for our patients.
Our program involves the specialties and combined disciplines of faculty members, nurses, care partners, therapists, pharmacists, in-fection control specialists, patient affairs liaisons and medical center finance department representatives. By working together as a team to evaluate overall performance, we have created more efficient systems in our daily operations.
A
The team has conducted an extensive three-year chart review of readmissions, categorizing preventability and common causes of re-hospitalizations. Interven-tions have been designed and are being implemented to address the most common causes of readmissions.
3: THE READMISSIONREDUCTION INITIATIVE
The Blood Pressure Control Project was designed to de-termine the safest and most effective oral blood pressure medications for Neurosurgery patients and to reduce the time required to get blood pressure to target levels.
2: BLOOD PRESSURE CONTROL PROJECT
The Neurosurgery Dashboard collects metrics for overall care, quality, safety, patient satisfaction and efficien-cy, allowing the team to continue providing the highest quality health care.
4: NEUROSURGERY QUALITYIMPROVEMENT DASHBOARD
THE NEUROSURGERY CLINICAL QUALITY PROGRAM IS FOCUSED ON THE FOLLOWING INITIATIVES:
UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND16 | CLINICAL QUALITY PROGRAM
The Infection Prevention Program works with UCLA Health’s Antimicrobial Stewardship Program to identify and correct improper antibiotic use. Surgical site infections for spinal fusions and laminectomies have been reduced to just 8 in the last 30 months. Blood stream infections have been virtu-ally eliminated, with only 1 in the last 66 months.
1: INFECTION PREVENTION
1
2009 2010
30-Day Readmissions
2011 2012
5 4 3 2 4 8 3 4 0 0 6 3 6 31

Eliminating inefficiencies that lead to late discharge will help ensure that patients can pick up their medications, settle at home in a timely manner and get answers to any questions that may arise while their primary pro-viders are available to help answer questions.
7: IMPROVING THROUGHPUT: AVERAGE LENGTH OF STAY
The Transitions of Care project was designed to evaluate the discharge process and improve care during this vulnerable time. This has involved a formal process to ensure appropriate follow-up for patients and clari-fication of discharge paperwork.
6: TRANSITIONSOF CARE PROJECT
The team is reducing waste by implementing the following programs: green IT, green office, green labs, water waste reduction, recycling of plastic and cardboard containers on the unit, discarding linens, re-stocking unused supplies, re-packaging intubation trays, and evaluation of lab utilization.
8: HEALTH CARE SUSTAINABILITY& WASTE REDUCTION
UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND
BENNY CHAN / FOTOWORKS
CLINICAL QUALITY PROGRAM | 17
The Neurosurgery PFAC is co-led by family members of pa-tients and representatives from the department with the ob-jective of creating a partnership between physicians, nurses, staff, patients and families. Members of the council provide input and feedback on patient care, services provided, new policies, and also recommend new programs and strategies.
5: PATIENT/FAMILY ADVISORY COUNCIL
4.5
2009 2010
Average Length of Stay
2011 2012
4.5 4 4.3 4.5 4.5 4 4 4 4 3.5 3.7 4 4 3.54
NEUROSURGERY ENHANCED RECOVERY, VALUE & SAFETY (NERVS)he UCLA Department of Neuro-surgery has deployed evidence-based and best-practice clini-cal protocol to aim for the ideal
surgical experience. An emerging concept in health care is the value of disease-specific, patient-oriented outcomes encompassing the total episode of care divided by the sum of total costs. The ideal surgical care episode is defined by: relief of signs and symptoms, accelerated recovery, minimal discomfort and absence of complications.
The Neurosurgery Enhanced Recovery after surgery, Value & Safety project (NERVS) led by Nancy Mclaughlin, MD, PhD, and Neil A. Martin, MD, is focused on comprehensive re-design of neurosurgical care. In two baseline case studies, we documented improved clini-cal outcomes and reduced total costs for the entire episode of surgical care. Cost assess-ment emerged as critical to contain or reduce cost of delivery of care and further improve and maximize value of care.
This redesign strategy requires a total system approach focused on three phases: pre-operative assessment and preparation, anesthetic and conduct of surgery, and post-operative management and recovery stages
T
DECREASEOVERALL COST
IMPROVE PATIENTSATISFACTION
IMPROVE DELIVERY OF PATIENT CARE
NERVS
CLINICALOUTCOMES
RISKMGMT.
PATIENT SAFETY
of care. Only by addressing all three phases of care and by encompassing all medical specialties and related services, can we ef-fectively achieve ideal surgical care. The ob-jectives are to improve patient outcome and patient satisfaction while decreasing the cost of care delivery.
We are assessing our processes through-out each phase of care and establishing benchmark outcome and cost data of four common surgical procedures encompass-ing 65% of elective cases. After completion of the redesign and measurement of its
impact, the program will be implemented throughout the UCLA Department of Neu-rosurgery and other departments across UC campuses. The NERVS project was one of 11 recipients, across the entire UC System, selected for a new grant award of $250,000 to improve the safety and quality of surgical care, jointly sponsored by the UC Center for Health Quality & Innovation and the Office of Risk Services. We believe this is the future of optimal care delivery in all specialties, of-fering patients optimal value and best out-comes delivered at the lowest cost.
WENDY TUCKER, CO-CHAIR OF THE PFAC WITH HUSBAND, MARCO FERREIRA

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND18 | BRAIN TUMOR PROGRAM
Linda M. Liau, MD, PhD

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND
inda M. Liau, MD, PhD, Vice Chair of the Department of Neurosurgery and Di-rector of the Brain Tumor Program at UCLA, leads a multidisciplinary team of
world-class neurosurgeons, neuroscientists, neuro-pathologists, neuro-oncologists, neuroradiologists, in-terventional radiologists, radiation oncologists, geneti-cists, basic scientists and clinical scientists. The team is dedicated to the diagnosis, management and treat-ment of all types of brain tumors. They meet regularly to develop coordinated care that translates to optimal clinical outcomes and patients living longer than those treated at other centers. As world leaders in the treat-ment of brain tumors, our neurosurgeons utilize the most advanced technology in intra-operative imaging, awake craniotomy, minimally-invasive endoscopic surgery and non-invasive stereotactic radiosurgery.
The UCLA Brain Tumor Program is a model for other health care institutions nationwide. Dr. Liau’s record of achievement is impeccable as a principal recipi-ent of four prestigious National Institutes of Health (NIH) grants and the Editor-in-Chief of the Journal of Neuro-Oncology. She has personally performed more than 1,000 brain tumor surgeries, and she and her col-leagues at UCLA treat over 500 brain tumor patients each year. Dr. Liau collaborates with several other neu-rosurgeons who operate on brain tumors (Dr. Neil A. Martin, Dr. Marvin Bergsneider and Dr. Isaac Yang), as well as UCLA neuro-oncologists (Dr. Timothy Clough-esy, Dr. Albert Lai and Dr. Leia Nghiemphu), neuro-pathologists (Dr. William Yong and Dr. Harry Vinters), radiation oncologists (Dr. Tania Kaprealian), and neu-roradiologists (Dr. Whitney Pope), in the hunt to better understand and treat these brain tumors.
L
My hope is to ultimately find a cure for brain cancer. I have several patients out 5 to 10 years after their original diagnosis of glioblastoma, which is a disease with a prognosis of usually less than two years. Each year we celebrate our patient survivors and
that is what makes working here at UCLA so worthwhile.—Linda M. Liau, MD, PhD, Director of the Brain Tumor Program at UCLA
“”
BRAIN TUMOR PROGRAM | 19

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND
hile completing her residency at UCLA, Dr. Linda M. Liau lost her mother to metastatic cancer. That pivotal moment changed
the course of her life and many others. As a physician-scientist, she is in a unique position to translate her pre-clinical findings in the labora-tory to the clinic. She received early recognition and seed funding from most notably the Kimmel Translational Science Award, given by the Sidney Kimmel Foundation dedicated to cancer re-search. This led to the development of the first personalized brain cancer vaccine in the UCLA laboratory. This novel immunotherapy involves surgically removing a patient’s tumor and then drawing blood to extract immune cells from the
patient’s body. In the lab, Dr. Liau isolated a spe-cific type of immune cell, called a dendritic cell, and activated it to train the patient’s immune cells to recognize, hunt down, and eliminate the tumor cells. The custom-made vaccine is devel-oped from the patient’s activated dendritic cells (DCs), which when injected back into the body, jumpstart the patient’s immune system to train “killer T cells” to seek out the tumor and strike it dead on the spot in the brain.
Today, the DCVax-L® vaccine is in Phase III, randomized, multi-center clinical trials for glio-blastoma in 46 hospitals in the United States, and has entered multiple centers internationally in Europe. The UK Health System has just adopted DCVax as a national priority trial.
Dr. Liau’s dream is to secure FDA approval for this immunotherapy as a standard treatment—in conjunction with surgery, radiation, and chemo-therapy—for patients with glioblastoma multi-forme. The hope is to work toward curing brain cancer once and for all.
W
BRAIN TUMOR BOARD MEETINGMultidisciplinary CollaborationUCLA Brain Tumor experts meet once a week at the UCLA Brain Tumor Board meeting to discuss patient cases and devise the optimal treatment plan for each individual patient, based on weighing all medical and surgical options. This relieves the patient from the need to visit multiple offices. The UCLA Brain Tumor Board is a resource for other clinics and doctors. Local, national and international physicians send in brain tumor cases to receive expert consultation on how to treat the challenging ones.
A PERSONAL QUEST TO CURE BRAIN CANCERTrue Bench to Bedside: UCLA Innovation Now in Phase III Clinical Trials
20 | BRAIN TUMOR PROGRAM
GENETIC PROFILING & PREDICTIVE MEDICINEUCLA brain cancer researchers have banked more than 5,000 brain tumor specimens. With molecular diagnostics, gene expression analy-sis, next generation genetic sequencing, and ad-vanced medical bioinformatics, we have a robust database of patient profiles to help develop pre-dictive, individualized treatment plans for new patients that increase survival.
TIM CLOUGHESY, DIR. UCLA NEURO-ONCOLOGY PROG.
DENDRITIC CELL (RED) ENGULFING A BRAIN TUMOR CELL (BLUE)
UCLA BRAIN TUMOR BOARD MEETING
ROBERT M. PRINS, PHD, ASSOCIATE PROF. IN RESIDENCE

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND
PRECISION PRE-OPERATIVE & INTRA-OPERATIVE
BRAIN MAPPING
Neil A. Martin, MD, Marvin Bergsneider, MD,Bob Shafa, MD, Isaac Yang, MD,Robert M. Prins, PhD, Carol A. Kruse, PhD,Emma Billingslea-Yoon, NPNEUROSURGERY
Whitney Pope, MDNEURORADIOLOGY
Michael Selch, MD, Tania Kaprealian, MDRADIATION ONCOLOGY
Nader Pouratian, MD, PhDSTEREOTACTIC RADIOSURGERY
Timothy F. Cloughesy, MD, Albert Lai, MD, Leia Nghiemphu, MDNEURO-ONCOLOGY
rior to the brain surgery, our patients undergo a 3D MRI in order to allow for
pre-operative and intra-operative brain mapping. For tumors near lan-guage areas, patients also undergo functional MRI (fMRI) scans, where they perform tasks such as reading, thinking, spelling and talking, which enables us to image these functional control centers of the brain. Those fMRI scans and the 3D MR images with white matter tractography are
carefully processed to be used in surgery to physically map the control centers on the brain as the neuro-surgeon removes the brain tumor. For tumors very close to functional language areas, the “asleep, awake, asleep” technique was perfected by anesthesiologists at UCLA, to allow neurosurgeons to wake patients during surgery and test vital func-tions such as talking or moving, while they remove the tumor. Patients are then put back to sleep for the non-mapping portion of the surgery.
P
INTERDISCIPLINARY TEAM
TUMORS TREATEDGliomasAstrocytomasBrainstem gliomasEpendymomasGangliogliomasGlioblastomasMedulloblastomasMixed gliomasOligodendrogliomasOptic nerve gliomas
Metastatic CancerBrain cystsBrain metastasisChoroid plexus papillomasCNS lymphomaCystic tumorsDermoid tumorsGerminomasLymphomaPineal tumors
Skull Base TumorsAcoustic neuromaAdenomasChordomasCraniopharyngiomasEpidermoid tumorsMeningiomasPituitary tumorsRathke’s cleft cyst
Spinal Cord TumorsAstrocytomasEpendymomasMeningiomasSchwannomas
3,000 5,000 30BRAIN TUMOR SURGERIES
PERFORMEDBANKED SAMPLES OF HUMAN
TUMORS, BLOOD, AND CSFDIFFERENT TYPES OF
BRAIN TUMORS TREATED
1STTO DEVELOP PERSONALIZED
BRAIN CANCER VACCINE
Jennifer Sugioka was the fifth glioblastoma patient to receive the DCVax vaccine and this year celebrates 13 years cancer free.
History of FirstsBRAIN TUMOR PROGRAM
BRAIN TUMOR PROGRAM | 21
Linda M. Liau, MD, PhD PROGRAM DIRECTORClinical Success
(L TO R): DCVAX PATIENT, JENNIFER SUGIOKA & BRAIN TUMOR PROGRAM DIRECTOR, DR. LINDA M. LIAU AT THE 2011 UCLA VISIONARY BALL.
First in-human use of a dendritic cell (DC)-based cancer vaccine for brain tumor patients [now known as DCVax].
First in-human use of a replicating retroviral vector (RRV) for gene therapy for malignant gliomas [now known as Toca-511TM].
First in-human use of combination therapy of DC vaccine with novel toll-like receptor (TLR-7) agonist, resiquimod.
First to develop cDNA microarray gene expression-based classification of glial tumors.
First to identify molecular genetic subgroup of glioblastoma that may be predictive of response to immunotherapy.
First intra-operative awake mapping of music comprehension/production areas in the brain.
First to use high-field intra-operative iMRI in the West Coast.

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND22 | BRAIN TUMOR PROGRAM
BRAD SILVER
LIVINGPROOF
BRAIN TUMOR PROGRAMPATIENT HIGHLIGHT
At 33, Brad Silver, a swimming and water polo coach, suf-fered from blinding headaches that he tried to ignore. It was
meant to be a happy time. His wife was seven months pregnant and he couldn’t wait to meet his son. As an all-American athlete, growing up surfing and lifeguarding in Huntington Beach, he knew that something was awry with his body. A visit to the hospital turned into a battery of tests that ended in devastat-ing news. “You have two months to live,” Brad recalled the doctor’s prognosis.
He was diagnosed with late stage brain cancer, a glioblastoma. Surgery was not an option.
“I needed to find something, or someone, to at the minimum keep me alive so I could be there for the birth of my son,” he said. Brad went for a second and third opinion. Then he found Dr. Liau at UCLA.
“I chose Dr. Linda M. Liau and Dr. Tim Clough-esy because they got to know me as a father
and an athlete,” he said. “At other hospitals the doctors were divided. At UCLA, they were not just a surgeon and oncologist, they worked together as my team and I trusted them to do everything they could to keep me alive.”
Dr. Liau performed his surgery on April 10, 2003. She removed a golf ball-sized tumor from his left lateral lobe. Nine days later, he witnessed the miracle of his son’s birth. He called him Brad Silver Jr. in memory of himself. Not knowing how many days, weeks or months he would have left with his family, he entered a phase I clinical trial.
Dr. Liau used a section of his tumor to create a personalized vaccine. From his drawn blood, she extracted his immune cells and trained them to recognize his brain tumor cells as an invader. These immune cells, called dendritic cells, would train killer T-cells to hunt down, attack and eliminate the brain cancer cells. She then injected this host of dendritic cells back into his body as a vaccine. With the help
of Dr. Liau, Brad experienced his son’s first breath of life, his first smile, his first laugh, his first words and his first steps.
Year after year, on April 10th, Brad sent flowers to Dr. Liau on his anniversary of life after brain cancer. Simultaneously, he cel-ebrated the birthday of his son, Brad Silver Jr.
“Initially, I thought I would only see his birth, then I no longer had to change his diapers. He was wearing undies,” Brad said with a chuckle. “He starts to walk and run, now he swims, he plays tennis, he surfs and stand-up paddles with me.”
Today, Brad and his family celebrate 10-years cancer-free and Brad Silver Jr.’s 10th birthday in Abu Dhabi, where he now lives with his family. He no longer needs to be close to UCLA. He simply sends his MRI scans into Dr. Liau via email.

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND BRAIN TUMOR PROGRAM | 23
Linda M. Liau, MD, PhDDr. Liau’s clinical expertise is in intra-operative functional brain mapping and use of intra-operative imaging for resection of brain tumors. Her research efforts are focused on the molecular biology of brain tumors, gene therapy, immunotherapy, and brain cancer vaccines.
Linda M. Liau, MD, PhD, Robert M. Prins, PhD,Emma Billingslea-Yoon, NPNEUROSURGERY
Judith Ford, MDRADIATION ONCOLOGY
Timothy Cloughesy, MD, Whitney Pope, MD,John Bentson, MDNEURO-ONCOLOGY & NEURORADIOLOGY
Harry Vinters, MD, William Yong, MDNEUROPATHOLOGY
BRAD’S TEAM
90 percent of patients with GBM die in the first year, the other five percent within two years, and hardly anyone is around after five. I’m not a statistic. They don’t have statistics for survivors. I have lived 10 years and I continue to soak in life as a father, a husband, a teacher, a surfer. I’m 100 percent back to being me because of Dr. Liau and the vaccine.
“”
Total NIH Funding
$4,141,837TOTAL NIH/NON-NIH GRANTS, INCLUDING DIRECT & INDIRECT COSTS, FOR THE DURATION OF THE RESEARCH PERIOD
NIH GrantsBRAIN TUMOR PROGRAMBRAD’S TIMELINE
APRIL Brad celebrates his son’s first birthday, sends Dr. Liau flowers to mark one year living cancer-free.
2004
APRIL Brad celebrates his son’s third birthday and he realizes, “I don’t have to be a cancer patient anymore, now I get to just be me.”
2006
2003FEBRUARYBrad’s headaches lead to an MRI that reveals brain cancer.
APRIL 10 Dr. Liau removes the golf ball sized tumor from Brad’s brain. Brad begins radiation and chemotherapy.
APRIL 19Nine days later Brad witnesses the birth of his son.
MAYDr. Liau creates and administers the personalized brain cancer vaccine.
MARCH 17Biopsy reveals stage IV glioblastoma. He is told by outside doctors that surgery is not an option.
2005 APRIL Brad celebrates his son’s second birthday. He marks two years cancer-free. Brad completes two years of chemotherapy.
APRIL Brad cuts the cake for his son’s 10th birthday. He celebrates the 10-year milestone of living beyond cancer. “My life is back to what it was 11 years ago.”
2013
—Brad Silver
National Cancer Institute
Phase I study of dendritic cell immunotherapy for malignant gliomas.
Gene expression-based classification of glial tumors.
Dendritic cell-based vaccine targeting MAA in malignant gliomas.
PACAP modulation of SHH signaling in human medulloblastoma.
Adoptive transfer of alloCTL for immunotherapy of recurrent gliomas.
CNS anti-tumor immunity induced by dendritic cell vaccination and TLR agonists.
Cell invasion, motility, and proliferation level estimate mapsin glioma imaging.
Office of the NIH Director
Cellular quiescence and braintumor stem cells.
National Institute of Neurological Disorders and Stroke
Translational development of replication-competent retrovirus vectors.
UCLA Neurosurgery Research Training & Education Program.

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND24 | PITUITARY TUMOR PROGRAM
Marvin Bergsneider, MD

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND
An intriguing movie when I was growing up was the Fantastic Voyage—watching a surgeon become miniaturized to go inside
the body to operate on a patient. Today, we have transformed that fantasy into reality at UCLA by using video to give us ultra-high magnification and resolution from an endoscope projected on
high-definition screens in our operating theater.
—Marvin Bergsneider, MD, Co-Director of the Pituitary Tumor Program at UCLA
“
”he UCLA Pituitary Tumor Program brings together an experienced inter-disciplinary team of world-class spe-cialists in the diagnosis, treatment
and management of pituitary tumors. Our team has performed more than 500 endoscopic surgeries with techniques pioneered and perfected at UCLA. We treat a high volume of cases every year, making our team one of the most experienced in the nation. We work together to provide patients with the most optimal plan of care that optimizes quality of life and meets their individual needs.
The combined neurosurgery-endocrine clinic is one of a few in the country that provides patients with a joint-consult to weigh the options of surgery and medications with Marvin Bergsnieder, MD, Co-Direc-tor of the UCLA Pituitary Tumor Program specializing in minimally invasive and endoscopic surgery, and Anthony P. Heaney, MD, PhD, Co-Director of UCLA Pi-tuitary Tumor Program specializing in endocrinology. As leaders in the management of pituitary tumors, we bring together the experts once a month for the UCLA Pituitary Tumor Board to discuss the pathology, diag-nosis and treatment of a patient.
T
PITUITARY TUMOR PROGRAM | 25

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND26 | PITUITARY TUMOR PROGRAM
JENGI MARTINEZ
SAVINGHER WINGS
PITUITARY PROGRAMPATIENT HIGHLIGHT
fter returning from a mission in 2006, Jengi Martinez, a pilot in the Air Force, visited a military doctor at Camp Pendleton in San Diego.
Something was not right.Jengi had been flying since high school. She
pilots a C-17, one of the largest aircrafts in the military, flying in and out of war zones to transport troops—wounded soldiers in medical evacuations from the battlefields and fallen comrades home to their families.
“It’s a very humbling experience to bring them home so they can be with their families,” Jengi said. “I’m proud every day.”
The magnitude of her missions easily out-weighed the unusual symptoms that Jengi was experiencing. It wasn’t difficult to ignore the ir-regular periods and unusual weight gain, until the doctor announced that Jengi had a brain tumor.
At 31, the diagnosis came on the tails of a near-decade-long investigation that led her to multiple specialists and many misdiagnoses. More tests revealed the tumor was just outside her brain in the pituitary gland, which is about the size of
a pea, yet it controls hormones and a multitude of functions in the body. The military is very strict about pilots using any medications.
“I knew this tumor wouldn’t kill me, but it could kill my career and that is so much a part of who I am,” Jengi said.
In despair, she sought a second opinion outside the military. She visited the Pituitary Tumor Program clinic at UCLA to meet with Dr. Marvin Bergsneider, renowned neurosurgeon and Dr. Anthony P. Heaney, expert endocrinologist. In her first consult with the doctors, she was impressed that they had already read her pathology, medical records, examined her images and presented her with realistic options. She explained meds were not an option for her. Together, they discussed the minimally-invasive, endoscopic endonasal surgery that would not require a craniotomy or incisions to remove the tumor.
“After meeting my doctors, I felt confident I could beat this tumor,” Jengi said.
The doctors then graciously consulted with the military doctors so that Jengi had a chance to return to the cockpit.
Dr. Bergsneider and Dr. Heaney suggested she attend their patient support group. The pa-tients and their families really helped her, and her mother understand what to expect for the surgery and recovery. For the first time since her diagnosis, she sat in a room full of people on the same journey. Each person was at a different stage of treatment and recovery, but each gave her great comfort and confidence in Dr. Bergs-neider and Dr. Heaney. In 2012, she underwent the endoscopic endonasal procedure to remove the pituitary tumor. The recovery was quick, and within four weeks, she was back in the cockpit, executing her duties and serving her country. To celebrate her restored health and weight loss, Jengi competed in her first triathlon.
“I’m so thankful to Dr. Bergsneider, Dr. Heaney and Dr. Wang for being an advocate for me,” Jengi said from the cockpit of her airplane at March Air Force Base, just weeks after the surgery. “I feel like I’m starting fresh. Not only do I get to serve my country, but I get to do a job that I love.”
A

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND PITUITARY TUMOR PROGRAM | 27
Neil A. Martin, MD,Nancy McLaughlin, MD, PhDNEUROSURGERY
Nader Pouratian, MD, PhDSTEREOTACTIC RADIOSURGERY
Noriko Salamon, MDNEURORADIOLOGY
Michael Selch, MD,Tania Kaprealian, MDRADIATION ONCOLOGY
Marilene Wang, MD,Jeffrey Suh, MDENDOSCOPIC SINUS SURGERY
CONDITIONS TREATEDAcromegaly Craniopharyngioma Cushing’s disease
Nelson’s syndrome Parasellar meningioma Pituitary insufficiency
Pituitary tumors Prolactinomas Rathke’s cleft cyst
Thyrotropinomas
2.3100 2,171REDUCED LENGTH OF HOSPITAL STAY TO 2.3
DAYS FROM 4.1 IN 2010
AVERAGE NUMBER OF PITUITARY TUMORS
TREATED EACH YEAR
REDUCED AVERAGE COST PER PITUITARY CASE BY
$2,171
500MORE THAN 500 CASES
TREATED BY THE PITUITARY PROGRAM AT UCLA
Experience with more than 500 endoscopic surgeries to remove pituitary tumors.
Joint neurosurgery-neuroendocrine clinic is one of just a few in the nation.
Minimally-invasive surgical options for the removal of pituitary tumors using endoscopic techniques pioneered and perfected at UCLA.
Non-invasive treatments: Stereotactic radiosurgery utilizes the Gold Standard NovalisTx shaped-beam radiation to eliminate the tumor with GPS-like precision without surgery.
INTERDISCIPLINARY TEAM
HighlightsPITUITARY PROGRAM
r. Bergsneider oper-ates side by side with the top UCLA head and neck surgeons
specializing in skull base surgery and rhinology. He harnesses endo-scopic instruments with high-defi-nition magnification, resolution and
video to project on plasma screens in one of the most advanced en-doscopic operating theaters in the country. He specializes in the fol-lowing treatments: endoscopic endonasal surgery, microscopic endonasal surgery and minimally-invasive keyhole craniotomy.
D
HIGH-DEFINITIONADVANCED ENDOSCOPIC SURGERY OPERATING THEATER
DR. MARVIN BERGSNEIDER COLLABORATES WITH UCLA HEAD AND NECK SURGEON DR. MARLIENE WANG
www.pituitary.ucla.edu
Joint Neurosurgery-Endocrine Clinic
The combined neurosurgery-endocrine clinic is one of a few in the country that provides patients with a joint-consult to weigh the options of surgery and medications with an interdisciplinary team, led by neurosurgeon Dr. Marvin Bergsnieder and endocrinologistDr. Anthony P. Heaney.
As leaders in the management of pituitary tumors, we bring together the experts once a month for the UCLA Pituitary Tumor Board Meeting to discuss the pathology, diagnosis and treatment of a patient.
Comprehensive Care Clinic
(L TO R): DR. MARVIN BERGSNIEDERAND DR. ANTHONY P. HEANEY
PROGRAM CO-DIRECTORSMarvin Bergsneider, MD & Anthony P. Heaney, MD, PhD

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND28 | UCLA SKULL BASE TUMOR PROGRAM
ENDOSCOPIC, MINIMALLY-INVASIVE TECH-NIQUES REVOLUTIONIZE SKULL BASE SURGERY Advanced endoscopic endonasal surgery and keyhole craniotomy use the endoscope, which has revolutionized the removal of these skull base tumors. UCLA neurosurgeons are specially trained in team-approach operating room techniques and minimially-inva-sive endoscopic surgery. Microsurgical instruments used with the endoscope increase the surgeon’s ability to remove the complete tumor in most cases, therefore decreasing the chance for reoccurrence while setting the stage for optimum recovery.
• Use of the natural passageway or the keyhole ½ inch-diameter incision to enter the brain• The endoscope tube, 4mm in diameter and equipped with a video camera, projects high-visibility deep in the brain• Keyhole incision procedures or a micro-craniotomy begins with an incision hidden in the eyebrow or beneath the hairline • High-definition video cameras project unsurpassed illumination, magnification and optical resolution of the surgical field• High visibility equals complete tumor removal• Fewer side effects than craniofacial surgery• Eliminates a long scalp incision craniotomy and skull bone removal• No visible scars• Reduces recovery times and shortens hospital stays
UCLA SKULL BASETUMOR PROGRAM
he UCLA Skull Base Tumor and Acoustic Neuroma Program unite 10 different specialties in a mul-tidisciplinary team to provide ex-
ceptional treatments and optimize quality of life for patients battling skull base tumors such as meningiomas, epidermoids and acoustic neuro-mas. There are multiple approaches for treat-ing these tumors that are classified as benign. However, when tumors of this type develop near vital control centers of the brain, they can be life
threatening or debilitating, often causing a loss of neurological function such as hearing and balance for patients.
Our neurosurgeons, Isaac Yang, MD, Marvin Bergsneider, MD, and Neil A. Martin, MD, spe-cialize in skull base tumors, minimally-invasive surgical techniques and non-invasive stereo-tactic radiosurgery. Dr. Yang works side by side with ENT otolaryngologists, to deliver a compre-hensive approach to these complex disorders. They collaborate with interventional radiologists,
stereotactic radiosurgery specialists, radiolo-gists, head and neck surgeons, facial plastic surgeons, pathologists and basic scientists for evaluation and diagnostic testing that ultimately results in a personalized approach to treatment.
A variety of factors including patient age, health, tumor location/size and tumor growth rate are weighed in evaluating the best treatment options. At UCLA, the specialists join together to determine the most effective personalized treat-ment strategy for each individual patient.
T
ISAAC YANG, MD, ASSISTANT PROF. & NEUROSURGEON
MINIMALLY-INVASIVE ENDOSCOPIC SURGERY

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND UCLA SKULL BASE TUMOR PROGRAM | 29
DIAGNOSIS &SURVEILLANCE
INTRAOPERATIVEBRAIN MAPPING
PRECISION TREATMENT
In the diagnostic or surveillance phase, pa-tients with small, asymptomatic acoustic neu-romas are evaluated through regular intervals of MRI scans, audiograms and radiographic tests combined with CT scans. This provides the team with a more in-depth understanding of the tumor’s effects on the patient’s brain and hearing nerves.
With our highest priority to preserve neurologi-cal function while ensuring we remove as much of the tumor as possible, we conduct intraopera-tive brain and nerve monitoring to assess motor functions and neurophysiological functions during the surgery. This allows us the ability to go as deep and far as possible without disrupting facial nerves, balance and cognitive functions.
In the case of a tumor requiring surgery, the goal is to completely remove the tumor while preserving hearing and balance. At UCLA, the neurosurgeon works in tandem with the head-and-neck surgeon to perform these delicate surgeries. With larger tumors, surgeons may operate for up to 20 hours as they work tirelessly to ensure preservation of neurological function while accessing and removing the tumors.
COMPREHENSIVE TREATMENT:ACOUSTIC NEUROMAS
UCLA SKULL BASETUMOR PROGRAM
SKULL BASE PROGRAM
Highlights
UCLA neurosurgeons routinely use minimally-invasive techniques:
In non-invasive radiosurgery, the Novalis Tx is used with the BrainLab neuronavigation system, in which focused beams of radiation strike the tumor with GPS-like precision while preserving vital control centers.
In the translabyrinthine approach, the surgeon makes a “C” shaped incision behind the ear and enters through the ear’s mastoid and semicircular canals to reveal the most lateral aspect of the tumor.
In the retro-sigmoid approach, also known as keyhole craniotomy, the surgeon makes a small incision behind the ear, which provides the neurosurgeon access to the cer-ebellum and brainstem.
In the middle fossa approach, an incision is made in front of the ear. Bone covering the top of the inter-nal auditory canal is removed to expose the tumor.
In the Endoscopic Endonasal Ap-proach (EEA), an endoscope is used to enter the brain via the nasal passage and remove the tumor, eliminating the need for incision and shortening recovery time.
Pituitary tumors: 328
Rathke’s cleft cyst: 39
Craniopharyngioma: 12
Meningioma: 13
Chordoma: 10
Spontaneous CSF leak: 16
Misc: 75
February 2008–June 2013
TOTAL: 493
UCLA EEA Cases
WHO WE ARE
coustic neuroma, also known as neu-rinoma or vestibu-lar schwannoma, is
a benign (non-cancerous) fibrous tissue growth arising from the ves-tibulocochlear nerve. Located in the inner ear, the vestibulocochlear nerve (eighth cranial nerve) controls hearing and balance. Acoustic neu-romas slowly grow over many years,
but do not metastasize to other areas. However, these tumors are located deep within the skull near centers of the brain that control vital functions. Pressure resulting from tumor growth can press against these sensitive structures. Symp-toms can range from mild to severe and can include loss of hearing in one ear, ringing of the ear (tinnitus), loss of balance, and dizziness.
A
TUMORS WE TREATAcoustic neuromas (vestibular schwannomas)Chordomas
Petroclival and cavernous sinus meningiomaSkull base tumors (meningiomas and epidermoids)
Isaac Yang, MD, Marvin Bergsneider, MD,Neil A. Martin MD, Nancy McLaughlin, MD, PhDNEUROSURGERY
Nader Pouratian, MD, PhDSTEREOTACTIC RADIOSURGERY
Akira Ishiyama, MD, Quinton Gopen, MD,Vishad Nabili, MDHEAD AND NECK SURGERY
Michael Selch, MD, Tania Kaprealian, MDRADIATION ONCOLOGY
NEURO-NAVIGATION IMAGING

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND30 | STEREOTACTIC RADIOSURGERY PROGRAM
A COMPREHENSIVE APPROACH TO DELIVER THE HIGHEST QUALITY OF CARE
ur doctors and research scientists here at UCLA have pioneered stereo-tactic radiosurgery and the led the nation in developing next generation
technologies that have made this procedure a non-invasive, safe and targeted treatment for malignant and benign tumors, arteriovenous malformations and intractable pain of the brain and spine. The UCLA team of radiosurgery specialists has treated more than 10,000 patients and is among the most experienced in the world.
Radiosurgery is surgery without the incision or anes-thesia. The outpatient procedure is under an hour. The focused beams of radiation have GPS-like precision
in targeting and eliminating the tumor or malforma-tion while leaving vital brain tissue unharmed. This requires advanced 3D imaging that allows for the neu-rosurgeon and physicist to plan in virtual reality a 360-degree, revolving focused beam strike to all sides.
Patients receive a comprehensive approach to treatment planned by our team of neurosurgeons, radiation oncologists, radiologists, dosimetrists and medical physicists who meet weekly to deliver the highest quality of care and optimal outcomes. The team has consistently reported safe and effective outcomes for patients at UCLA, and has set the gold standard for radiosurgery to benefit patients across the nation and around the globe.
O
WHO WE ARENader Pouratian, MD, PhD, Antonio De Salles, MD, PhD,Daniel Lu, MD, PhD, Nancy McLaughlin, MD, PhD,Bob Shafa, MD, Isaac Yang, MD, Nestor Gonzalez, MDNEUROSURGERY
Tania Kaprealian, MD, Pat Kupelian, MD, Phil Beron, MD,Michael Selch, MDRADIATION ONCOLOGY

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND
or tumors that do not respond to either medical or surgical treatment, UCLA offers state-of-the-art, focused-beam radiation
therapy. The Novalis Shaped-Beam Stereo-tactic Radiotherapy system was developed at UCLA, and is the most technologically advanced system of its kind. This non-invasive treatment is safe and very effective. In a bloodless, blade-less elimination of the tumor, the neurosurgeon collaborates with a physicist and radiation on-cologist to map the brain and target the tumor with GPS-like precision using focused beams of radiation, while protecting vital brain tissue. This
outpatient procedure takes up to 40 minutes and can be an alternative to open brain surgery for some types of tumors. F
STEREOTACTIC RADIOSURGERY PROGRAM | 31
SRS PROGRAM
10,000
1st
1980
MORE THAN 10,000 PATIENTS TREATED SINCE THE PROGRAM DEBUTED
FIRST TO INTRODUCE RADIOSURGERY IN THE UNITED STATES
YEAR OUR PROGRAM WAS FOUNDED, PIONEERING RADIOSURGERY FOR 33 YEARS
Facts & Figures
Gold Standard
Malignant & Benign Brain Lesions
Primary Brain Tumors
Brain Metastasis
Arteriovascular Malformations
Trigeminal Neuralgia
Spine & Organ Disorders
Parkinson’s Disease
Essential Tremor
Dystona
Spine Tumors
CONDITIONS TREATED
UCLA’s Novalis Shaped-Beam Surgery system now considered the Gold Standard for image-guided, shaped-beam radiosurgery—uses stereotactic technology as well as highly specialized computer software for radiation therapy planning.
Enables treatment of intracranial lesions once considered inoperable due to proximity to eloquent or critical structures.
Avoids many of the co-morbidities common to invasive surgery, such as infections, hemorrhage and other complications.
NON-INVASIVESTEREOTACTIC RADIOSURGERY
STEREOTACTIC RADIOSURGERY, FOCUSED-BEAM RADIATION, USING A FRAMELESS IMAGE-GUIDANCE SYSTEM ON THE SPINE

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND
AUSTIN WELCH
OVERCOMINGADVERSITY
SRS PROGRAMPATIENT HIGHLIGHT
32 | STEREOTACTIC RADIOSURGERY PROGRAM
t the Chadwick High School junior class retreat, Austin Welch stands up with a bald head among a crowd of peers
to make a bold case for becoming junior class president. He resembles a young Bill Clinton when talking about the importance of helping people and perseverance.
Shortly after his 15th birthday while surfing in Hawaii, Austin felt pins and needles in his left hand. He paddled in. A headache fol-lowed. His speech slurred. He struggled to tell his parents what was happening to him. They rushed him to the emergency room. The scans revealed an arteriovenous malforma-tion (AVM), a tangled web of abnormal veins and arteries in his brain, which arrests blood flow and can produce devastating bleeding.
“It came out of the blue. It didn’t seem that bad at first, then I started to see doctors and receive really bad news. That was tough. It’s not easy to face your own mortality at 15,” Austin said.
When he returned home to Palos Verdes, he visited specialist after specialist who offered little hope. The location of the AVM presented serious risks. The physicians suggested that he would be paralyzed and have speech defi-cits even with a surgery. Austin was the star of the basketball team and president of his soph-omore class. He was not about to give that up, so he continued the search.
His parents eventually received a referral through a friend to see Dr. Nestor Gonzalez, renowned neurosurgeon and neurointer-ventionalist at UCLA. Austin connected with Dr. Gonzalez instantly because he spoke to him like an adult, while other physicians ad-dressed his parents, not him. Since the risks of surgery were high, Dr. Gonzalez recom-mended that Austin have endovascular em-bolization to treat some dangerous portions of the AVM, followed by stereotactic radiosur-gery that would target the AVM with focused beams of radiation. The Novalis Tx protects
the healthy brain tissue while zeroing in to remove the AVM without open brain surgery.
Austin had an angiogram that revealed three aneurysms on the walls of the blood vessels that fill up like a balloon with blood and carry a high risk of bleeding. Dr. Gonzalez sealed off the aneurysms with ONYX, a liquid agent that solidifies the aneurysm, therefore restoring blood flow in the brain. Austin then had a 30-minute stereotactic radiosurgery treatment planned and executed by Dr. Gon-zalez and his team at UCLA.
Austin became president of his junior class at Chadwick High School. He recently received his acceptance to go to Dartmouth College. Today, as he nears graduation, Austin is proud to serve as president of Chad-wick High School and his dream is to one day say, “Vote for me for President of the United States of America.”
A

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND STEREOTACTIC RADIOSURGERY PROGRAM | 33
Nestor Gonzalez, MDNEUROSURGERY
Antoinette AndersonCLINICAL & RESEARCH COORDINATOR
Antonio De Salles, MD, PhDRADIOSURGERY
Viktor Szeder, MD, Radoslav Raychiev, MD, Amit Balgude, MD, Angelos Konstas, MDINTERVENTIONAL NEURORADIOLOGY
UCLA SRS CLINICAL OUTCOMES
Nestor Gonzalez, MDDr. Nestor Gonzalez is a Ruth & Raymond Stotter Professor in neu-rosurgery and interventional neuroradiology who has unique training, having completed two separate and distinct residency training pro-grams in both radiology and neurosurgery as well as a fellowship in interventional neuroradiology.
AUSTIN’S TEAM
When I thanked Dr. Gonzalez for saving my life, he said to me, ‘the world needs better politicians—
intelligent, generous, strong, good people just like you.’ He cares about me, not just as a patient, but
as a person. It’s incredible to be where I am.
“”
SRS PROGRAM
History of Firsts
Highlights
We advanced stereotactic radiosurgery from a minimally-invasive procedure to completely non-invasive.
Highly-effective way of treating the most difficult tumors in the brain, spine and in other areas of the body.
The UCLA Stereotactic Radiosur-gery Program was formed in 1980 when the Karolinska Institute of Stockholm, Sweden donated one of two “Gamma Knife” units in ex-istence at the time for the purpose of collaborative research. Since that time, the UCLA radiosurgery team has innovated treatments with the Gamma Knife, LINAC Scalpel, XKnife and, more recently, with Novalis Tx, to now deliver the most advanced, safest and effec-tive radiosurgery in the world.
Frameless Novalis Tx is the most advanced radiosurgery developed with the expertise of UCLA radio-surgeons. The system does not require a halo treatment frame to be fastened to the patient’s head, making the outpatient procedure comfortable, painless, safer and more effective.
First radiosurgery for trigeminal neuralgia with linear accelerators in the world.
First Gamma Knife radiosurgery in America.
First Novalis radiosurgery in America.
First endoscopic clipage of aneurysm.
29+71+X71.5%VOL. REDUCTION
AFTER SRT
—Austin Welch
In recent years, neurosurgeons have turned to ste-reotactic radiosurgery to treat inoperable brain tumors, arteriovenous malformations (AVM) and other abnormalities that can cause debilitating pain such as trigeminal neuralgia. The clinical outcomes have been promising and continue to improve with our innovations to BrainLab, our neu-ro-imaging guidance system, and the Novalis Tx. As a result, our patients are experiencing less invasive and more effective radiosurgery that ultimately im-proves their quality of life.
STEREOTACTIC RADIOSURGERY USING FOCUSED-BEAM RADIATION & IMAGE GUIDANCE TO TREAT AN AVM
BRAINSTEM METASTASIS 90% 1 YR. CONTROL
GIANT AVM 71.5% VOL. REDUCTION
TRIGEMINAL NEURALGIA 79.3% PAIN RELIEF
MENINGIOMA 90-97% CONTROL RATE
PITUITARY TUMOR APPROACHING 100%
RADIOGRAPHIC CONTROL AT 32 MONTHS
5210=151151111110=
5210=15115111110=
5210=1511511500=
5210=151151111110=
5210=151151111110

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND34 | UCLA STROKE CENTER
Neil A. Martin, MD

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND UCLA STROKE CENTER | 35
Every day, we touch and save the lives of patients struck by stroke, not just here at UCLA, but also in hospitals across California through our Telestroke Network,
and around the world through our endovascular treatments invented by our clinicians. We are mapping the next frontier of stroke care. In the past, when a patient suffered a stroke, the goal was to stabilize the brain for rehabilitation.
Today at UCLA, we snare the clot, reverse the stroke and restore the brain. As a result, we witness medical miracles and resilience in our patients.
—Neil A. Martin, MD, Professor & W. Eugene Stern Chair in Neurosurgery & Co-Director, UCLA Stroke Center
“
”he UCLA Stroke Center is a national and international leader in the diag-nosis, treatment and management of cerebrovascular diseases. More than
15,000 patients have been cared for at the UCLA Stroke Center that has been certified as a Compre-hensive Stroke Center by the Joint Commission and the American Heart Association. We are one of only five centers nationwide with a specialized transla-tional research grant from the National Institutes of Health to study promising new surgical interven-tions and therapies for stroke.
Our clinicians and scientists are among the world’s
foremost leaders and pioneers in the treatment of ischemic and hemorrhagic stroke, having developed the first FDA-approved MERCI device—a mechanical device that uses a micro-wire to remove the blood clot and stop a stroke in progress. This year, the team supplanted the MERCI device with the FDA-approved SOLITAIRE Flow Restoration Device. The Guglielmi detachable coils (GDCs) invented at UCLA have trans-formed the treatment of intracranial aneurysms and are now used around the world. Endovascular thera-pies innovated and pioneered by interventional radi-ologists and neurosurgeons at UCLA have now been adopted in medical centers across the globe.
T

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND36 | UCLA STROKE CENTER
UCLA STUDY SHOWS PROMISE & HOPE FOR HEMORRHAGIC STROKE PATIENTSMinimally-Invasive Intraoperative CT Guided Endoscopic Surgery (ICES)
At the 2013 International Stroke Conference, UCLA neurosurgeons announced the potentially groundbreaking results of the randomized, con-trolled phase II clinical trial, which determined
that minimally-invasive endoscopic surgery appears to have safer and more effective outcomes as compared with the standard medical treatment for brain hemorrhage. In the past, open surgery that involved a large incision further trau-matized the brain in an effort to remove the blood. The pro-cedure failed to improve the outcome of the patient’s quality of life in the aftermath of a hemorrhagic stroke. This devas-tating, critical condition has a mortality rate of more than 75 percent. If the patient manages to survive, he or she faces a life of long-term severe disability.
The UCLA-originated clinical trial led by Dr. Paul M. Vespa and Dr. Neil A. Martin, in conjunction with Johns Hopkins University, set out to determine the safety and effectiveness of removing blood using a “keyhole” incision—smaller than the size of a dime—with Intraoperative CT guided Endoscopic Surgery (ICES). The endoscope, a tiny probe with a camera on the tip, was used to navigate with GPS-like precision. This
image-guided system displays CT scans of the brain on moni-tors that allows surgeons to pinpoint the bleeding. A catheter was then placed in the tiny bur hole, and the blood was im-mediately removed.
As a result, the procedure was safe with no further bleeding or harm to the patient. On average, 71 percent of the blood was immediately removed. This procedure was performed at seven major medical centers with 24 enrolled patients. Eigh-teen of the patients had the endoscopic surgery and six had standard medical treatment.
After six months, post-op, the neurological outcomes for pa-tients were better and mortality was lower with the endoscopic surgery patients as compared to standard medical treatment patients. Endoscopic surgery has the key advantage to get the blood out all at once, immediately alleviating the pressure on the brain and setting the stage for ultimate recovery.
The UCLA Stroke Center is in the National In-stitutes of Health (NIH)-funded Specialized Programs of Translational Research in Acute Stroke (SPOTRIAS) network conducting early phase clinical trials, sharing data and driving new therapies for acute stroke patients.
NIH-FUNDED SPOTRIAS NETWORK
BEFORE AND AFTER IMAGES OF HEMORRHAGIC STROKE PATIENT TREATED WITH ICES
Nestor Gonzalez, MD

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND UCLA STROKE CENTER | 37
INTRODUCING ANEW PARADIGM
RESEARCH TRANSLATES TO MEDICAL BREAKTHROUGHS
estor Gonzalez, MD, an interna-tionally-recognized neurosur-geon and interventional neu-roradiologist at UCLA, received
the prestigious American Heart Association (AHA) Science Innovation Award in recog-nition of “introducing a new paradigm into medicine.” He is studying the mechanisms that lead to the formation of new conduits to supply blood to the brain in patients with nar-rowing cerebral arteries (the structures that bring blood to the brain). By targeting these natural mechanisms to improve blood flow to the brain through medical and surgical treat-ments, new paths can be created to treat pa-tients with symptoms of TIA or stroke.
Dr. Gonzalez is leading the application of Encephalo-duro-arterio-synangiosis (EDAS) surgery, an indirect bypass for the treatment of narrowing arteries in the brain. In the surgery, he opens a window into the surface of brain and “borrows” an artery from the scalp, placing it in contact with the brain at which point new blood vessels begin to grow in response to natural molecules produced by the body when the brain is deprived of oxygen. EDAS is deemed safe and effective because the procedure does not disrupt the native brain arteries.
The National Institutes of Health (NIH) and the National Institute of Neurological Disor-ders (NINDS) sponsor this research conduct-ed by Dr. Gonzalez.
N
CONDITIONS TREATEDAneurysmsArterial dissectionArteriovenous malformations Carotid and intracerebral arterial stenosis
Cavernous angiomas HematomasHemifacial spasmIntracranial and spinal AVMs
Moyamoya diseaseStrokeTrigeminal neuralgia
1 of 5 1,200 1stUS HOSPITALS CONDUCTING
GOVERNMENT-FUNDED STROKE RESEARCH
SURGERIESPERFORMEDEACH YEAR
MOST COMPREHENSIVE STROKE CENTER IN THE
WORLD
15,000PATIENTS TREATED
SINCE THE PROGRAM BEGAN IN 2001
First mechanical device therapy for acute ischemic stroke:
• MERCI Retriever• Invented at UCLA
Leading device therapies for cerebral aneurysms:
• Guglielmi detachable coil, Matrix coil.
• Invented at UCLA
Leading catheter therapy for intracranial arteriovenous malformations and fistulae:
• ONYX as liquid embolic agent for intracranial arteriovenous malformations and fistulae
• Invented at UCLA
First clinical cellphone PACS system for remote review of CT and MRI scans in acute stroke developed at UCLA.
First US multicenter trial of endoscopic treatment for acute intracerebral hemorrhage.
First routine use of intraoperative digital subtraction angiography for evaluation after surgical aneurysm and AVM treatment.
First Neuro ICU-adjacent comprehensive stroke imaging center with CT, PET, 3T MRI.
First cerebral blood flow laboratory to use bedside xenon CBF studies and TCD for stroke critical care and research.
UCLA STROKE CENTER
History of Firsts
John G. Frazee, MDVASCULAR NEUROSURGERY
Latisha Ali, MD, Doojin Kim, MD,David S. Liebeskind, MD STROKE NEUROLOGY
Paul M. Vespa, MD, Manuel M. Buitrago Blanco, MDNEUROCRITICAL CARE
Lucas Restrepo, MDNEUROHOSPITALIST NEUROLOGY
Nestor Gonzalez, MD, Gary Duckwiler, MD,Reza Jahan, MD, Sachin Rastogi, MD,Satoshi Tateshima, MD, Viktor Szeder, MDINTERVENTIONAL NEURORADIOLOGY
WHO WE ARECO-DIRECTORSNeil A. Martin, MD, Bruce Dobkin, MD,Jeffrey L. Saver, MD, Sidney Starkman, MD
Doctor HighlightJEFFREY L. SAVER MD,IS PROFESSOR OF NEUROLOGY, CO-DIRECTOR OF THE UCLA STROKE CENTER, AND MEDICAL DIRECTOR OF THE STROKE UNIT.

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND
JON GALVAN
BEATING THEIMPOSSIBLE
38 | UCLA STROKE CENTER
UCLA STROKE CENTERPATIENT HIGHLIGHT
earing a deadline, Jon Galvan, a senior producer for a video game company, arrived at the studio early to finalize a project for ship-
ment. Jon plays and makes video games for a living. Yet that July morning in 2008, the rising pressure felt more palpable than the play. While testing the game, he chewed on sunflower seeds. The crackling ceased when he heard a loud jarring pop in his brain that felt like an ex-plosion striking him down.
“I did a header into the drywall,” Jon recalled barreling toward the wall as he lost conscious-ness that morning in the production studio. He shouted out for help but his words sounded jumbled and slurred.
“Before, I went down, I thought to myself, I’m not going out like this.”
At 38 years old, Jon and his wife, Nicole, had just celebrated their son’s second birthday. His career was on the rise after producing the video game Medal of Honor at Electronic Arts, among others. In the virtual reality gaming world, Jon
could calculate the odds to continue to play or yield to game over. In reality, he faced tough odds for survival. The pop was a severe hemorrhagic stroke in the basal ganglia brought on by undiag-nosed hypertension. He had less than 25 percent chance of survival. If he survived, the deficits could be immeasurable. A friend arranged for Jon to be transferred to the UCLA Stroke Center. That move increased his odds.
The ambulance arrived at UCLA. Dr. Neil A. Martin, Professor & W. Eugene Stern Chair in Neurosurgery and renowned stroke expert, met Nicole, Jon’s wife, to explain his condition. The standard treatment of open brain surgery often resulted in poor outcomes. Dr. Martin introduced the possibility of performing an experimental procedure called ICES, Intraoperative CT guided Endoscopic Surgery, which could potentially remove all of the blood and alleviate deadly in-tracranial pressure. Both could set the stage for an ultimate recovery. Nicole agreed.
Jon was wheeled into the endoscopic oper-ating theater at UCLA. Dr. Martin made a tiny
incision about the size of a dime above Jon’s eyebrow and then a bur hole to insert an endo-scope that navigated his brain. The CT scans pointed him to the area that was bleeding. He gently inserted a catheter and removed all the blood. After the surgery, Jon spent weeks in the neuro-ICU.
At first he could not walk or talk. Eventually, he emerged from the ICU and entered extensive rehabilitation that entailed training his brain to rewire itself. He gradually regained function—walking, talking and even telling jokes again. He returned to playing video games, and began volunteering at the studio. Today, he is working part-time and is set to begin on a UCLA clinical trial to stimulate his spinal cord and further rehabilitate his motor function.
“At one point, I realized that I wasn’t suppose to be here and I said thank you to Dr. Martin,” Jon said. “Whatever he did to me was unique, special, a one-shot deal that saved my life. I not only recovered, I’m thriving.”
N

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND
Neil A. Martin, MD
Neil A. Martin, MDNEUROSURGERY
Paul M. Vespa, MD, Alex Nee, MD,Benjamin Emanuel, MDNEUROCRITICAL CARE TEAM
Areti Tillou, MDGENERAL SURGERY
Patrick Pezeshkian, MD, Justin Dye, MDColin Buchanan, MDNEUROSURGERY RESIDENTS
Jonathan Cotliar, MDDERMATOLOGY
Saleh Salehmoghaddam, MD NEPHROLOGY
Professor & W. Eugene Stern Chair in Neurosurgery, Dr. Neil A. Martin is Co-Director of the UCLA Stroke Center and Director of the Aneurysm and AVM Program. Dr. Martin specializes in the research and treatment of neurovascular disorders, including arteriovenous malformation, aneurysm and stroke.
JON’S TEAM
UCLA STROKE CENTER | 39
The UCLA Stroke Center has been certified as a comprehensive stroke center by the Joint Com-mission and the American Heart Association/American Stroke Association. It is one of the first 10 stroke centers in the nation to receive the prestigious designation. The UCLA Stroke Center has also received the two highest American Heart Association awards recognizing excellence in stroke treatment: Gold Plus Stroke Award and Target: Stroke Honor Roll hospital.
LOS ANGELES COUNTY
The UCLA Stroke Center innovated the Telestroke Network Partner Program (red lines), which gives community hospitals across California direct, immediate, around-the-clock video consultations with UCLA stroke experts. Through two-way video conferencing, our neu-rologists can beam into a local hospital to give a stroke-specific neurologic exam while reviewing local diagnostic images for rapid response to stroke, when minutes can mean the difference between brain damage and full recovery. The UCLA Tele-ICU Network (blue lines) provides around-the-clock neurocritical care specialists to assist patients with brain and spine trauma emergencies in hospitals without this expertise throughout California and across the country in Atlantic City, New Jersey.
American Heart AssociationAmerican Stroke AssociationCERTIFICATIONMeets Standards forComprehensive Stroke Center
Joint Commission National Quality Approval(Awarded to UCLA Stroke Center)
AWARD-WINNING CARE
TELEMEDICINECONNECTING TO OUR COMMUNITY & SHARING OUR EXPERTISE

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND
JAMIE MORISHITA
HOLDINGOUT HOPE
40 | UCLA STROKE CENTER
UCLA STROKE CENTERPATIENT HIGHLIGHT
t first her right hand tingled. The numbness crawled onto her face and crept down her leg, para-lyzing her. Frightened, Jaime
Morishita visited doctor after doctor. At 30 years old, she appeared healthy, with her only problem being high blood pressure. The medi-cations failed to stop these bouts of paralysis. As a mother of three, she grew more fearful. She and her husband had planned to have another baby, but her health would not permit it. The episodes and headaches increased.
“As long as I don’t breathe too hard,” Jaime would say to herself, “I can control it.”
What Jaime didn’t realize was these epi-sodes were strokes, transient ischemic attacks on her brain. The blood flow would just stop, causing the brain to lose oxygen.
“Even just blowing bubbles for my children at the park would trigger the numbness to strike me and disconnect my entire right side from my body,” Jaime said. She stopped exercising
and going places where she may exert too much energy, for fear of the episodes.
By her 32nd birthday, a neurologist di-agnosed her with Moyamoya, a cerebrovas-cular disorder that causes narrowing of the carotid arteries and, as a result, tiny blood vessels that form to compensate for the lack of blood flow in the brain. The tangle of tiny blood vessels on the MRI scans looks like a “puff of smoke,” translated to Moyamoya in Japanese. These tiny blood vessels could break at any time causing hemorrhage— essentially a major stroke.
Her neurologist referred her to Dr. Nestor Gonzalez, a pioneer and expert in the treat-ment of cerebrovascular disorders. Dr. Gonza-lez specializes in the most minimally-invasive approach to treat Moyamoya. On May 7, 2012, Jaime underwent EDAS (Encephalo-Duro-Ar-terio-Synangiosis), an indirect bypass that in-volves Dr. Gonzalez carefully removing a native artery from her scalp and implanting it in her
brain. As a result, the brain gives off a chemi-cal to grow blood vessels from the artery, thus revascularizing the brain. Within weeks, on June 27, 2012, she went in for her first an-giogram and the blood vessels were sturdily growing, already increasing blood flow in her brain. The mini-strokes stopped. Jaime began to feel normal again.
At six months, she received her second an-giogram post-op and the vessels continue to grow and flow.
Shortly after, Jaime discovered her womb was also growing. An ultrasound confirmed a healthy baby on the way.
“I can’t believe that I’m pregnant. I actually didn’t think we would be able to have another child. I was so scared that I was going to have to live with those episodes. Dr. Gonzalez was right to do EDAS. He is amazing. Now I have my miracle baby,” Jaime says, rubbing her six-month bump.
A

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND
Dr. Nestor Gonzalez is an Assistant Professor in Neurosurgery and Interventional Neuroradiology who has unique training, having completed two separate and distinct residency training programs in both radiology and neurosurgery, as well as a fellowship in interventional neuroradiology.
Nestor Gonzalez, MD
Nestor Gonzalez, MD, Brandon Evans, MD,Justin Dye, MD, Collin Buchanan, MD,NEUROSURGERY
Jeffrey L. Saver, MD, David Liebeskind, MDSTROKE NEUROLOGISTS
Viktor Szeder, MD, Radoslav Raychiev, MD, Amit Balgude, MD, Angelos Konstas, MDINTERVENTIONAL NEURORADIOLOGY
JAMIE’S TEAM
I can’t believe that I’m pregnant. I actually didn’t think we would be able to have another child. I was so scared that I was going to have to live with those episodes. Dr. Gonzalez was right to do EDAS. He is
amazing. Now I have my miracle baby.
“”
UCLA STROKE CENTER
Highlights
Total NIH Funding
$1,557,164TOTAL NIH/NON-NIH GRANTS, INCLUDING DIRECT & INDIRECT COSTS, FOR THE DURATION OF THE RESEARCH PERIOD
NIH Grants
EDAS Outcomes
—Jamie Morishita
Functional outcome: 95% (mRs≤2)Post-operative stroke rate: 0Long-term stroke rate: 3%Cerebral hemorrhage: 0Reoperations: 3%
National Institute of Neurological Disorders & Stroke
Cerebral lactate metabolism following human traumaticbrain injury.
Surgical indirect revascularization for symptomatic intracranial arterial stenosis.
UCLA STROKE CENTER | 41
UCLA EDAS REVASCULARIZATIONS(ENCEPHALO-DURO-ARTERIO-SYNANGIOSIS)
29+71+X32SYMPTOMATIC INTRA-
CRANIAL ARTERIAL STENOSIS
70MOYAMOYA DISEASE
TOTAL NUMBER OF EDAS PROCEDURES: 102
MOYAMOYA DISEASE EDAS REVASCULARZATION
Average age: 30 (Range 4-57)
Female/male: 47/23
Clinical follow-up average: 14 months
Angiographic follow up average: 13 months
The donor artery is placed in close proximity to the superficial brain arteries. A network of collaterals forms between the donor artery and the adjacent brain vessels without a sur-gical anastomosis.
World’s Leading Stroke Center.
More than 15,000 patients treated at the UCLA Stroke Center.
NIH-funded center among five in the nation conducting translational research for stroke.
Telestroke Network services the entire Southern California region.
Certified Comprehensive Stroke Center by the Joint Commission.
Endovascular and surgical treatments developed at UCLA are now circling the globe.

42 | ITZHAK FRIED: THE DISCOVERY OF STIMULATING MEMORY IN THE HUMAN BRAIN UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND

THE DISCOVERY OF STIMULATING MEMORY IN THE HUMAN BRAIN
ITZHAK FRIED
ITZHAK FRIED: THE DISCOVERY OF STIMULATING MEMORY IN THE HUMAN BRAIN | 43
t the intersection of the brain and the mind exists the lifework of Itzhak Fried, MD, PhD, Profes-sor of Neurosurgery, Psychiatry
and Bio-Behavioral Sciences at UCLA. His operations have led to hundreds of patients living seizure-free lives, while his explorations have unearthed a groundbreaking discovery of stimulating memory in a critical junction of the brain. This finding, reported in the New England Journal of Medicine by Dr. Fried and his UCLA colleagues, could lead to treatments for boosting memory in patients with early de-mentia and Alzheimer’s disease. Reaching this point is just one milestone in a series of mara-thons probing the inner space of the human brain for more than 25 years.
Dr. Fried is one of the top 10 finalists for the Global B.R.A.I.N (Breakthrough Research and Innovation for Neurotechnology) Prize com-petition inspired by Israeli President Shimon Peres and Israel Brain Technologies. Each neuroscientist in the finalists has demonstrat-ed “breakthrough achievements that have sig-nificant impact on humanity.”
Since his early days as a neuroscientist, he aspired to unlock the fundamentals of brain functions that are uniquely human. Yet, he re-alized that only one kind of doctor could truly interact with the living human brain. Dr. Fried set out to become a neurosurgeon. He com-pleted medical school at Stanford University and moved on to Yale University for his neu-rosurgical residency training with a focus on treating patients with epilepsy. After a year on the faculty at Yale, UCLA recruited Dr. Fried to take over the Adult Epilepsy Surgery Program.
“There was a fantastic team at UCLA and an infrastructure with a great tradition for epilep-sy surgery set by Paul Crandall,” Dr. Fried said. “He developed the technology to go precisely into the brain to gain the location of the group of cells responsible for the seizures and later remove them with surgery. We furthered the clinical research when we listened in to indi-vidual cells. We could cure our patients, while at the same time we were able to bring these recordings to the level of a single neuron, which provided insight into how human memory works and how other functions of the brain are carried out at the neuronal level.”
Early on at UCLA, he implanted intracra-nial subdural electrodes to localize the area of the brain producing the seizures for his pa-tients. While monitoring the chronic seizures of a 16-year-old girl, he and his team con-ducted cognitive tasks. As they applied elec-trical stimulation at a particular site in the left frontal lobe, she laughed when shown a picture of a horse. “That horse is funny,” she said. The laughter escalated on the next task when she read a sentence about a rainbow. This time the rainbow was funny.
“Then this charming girl looked at all of us and upon electrical stimulation of the area, she laughed hysterically and said, ‘you guys are so funny,’” Dr. Fried said, recalling the moment of discovering this phenomenon in the supple-mentary motor area of the brain where laugh-ter occurred. The finding was later published in Nature in February of 1998.
In recording single brain cells, or neurons, to determine and group the brain networks causing the seizures, he listened in on cells and/or groups of cells that responded to specific individuals such as a particular celebrity. The first single cell recording of this type was of a cell, which responded uniquely to Bill Clinton. In another patient a neuron responded to Jennifer Aniston, firing each time any photo of her was shown to the patient, whether it was in color, in black and white, or the actress in profile. It was as if the neuron knew the identity or the concept of Jennifer Aniston and did not really care about the particular way the actress was displayed.
In fact such a neuron would respond even to the written name of the person or to the sound of her name.
“The Jennifer Aniston cell gave us profound insight on how the brain codes concepts and shapes our memories,” he said. It showed an uncanny code of explicit representation of con-cepts in individual neurons. Dr. Fried published these insights with his colleagues in the 2013 February issue of Scientific American.
Dr. Fried’s laboratory has contributed sig-nificantly towards understanding cognition through direct recordings from brain cells in humans. His team was the first to record in-dividual brain cells in the act of summoning a spontaneous memory. This study published in Science magazine revealed not only where a
remembered experience is registered but also, in part, how the brain is able to recreate it. Fur-thermore, in a different set of studies he has shown that cells in another area of the brain, the supplementary motor area, signal the for-mation of human will, even before it is recog-nized by self. For these achievements he has been named Fellow of The American Associa-tion for the Advancement of Science.
“I’m always learning,” Dr. Fried said. “The con-summate physician is always learning.”
Recently, his sons challenged him to run a marathon not realizing that he had spent his life running marathon after marathon. They bet him that he could not cross the finish line. He quietly trained for a few months and then invited his family to Paris in spring 2009 to watch him cross the marathon finish line. Yes, his sons lost the bet. Today, he has completed marathons in other parts of the globe. Likewise, he has forged collaborations with physicians and scientists around the globe. Dr. Fried brought the field of epilepsy surgery to Israel. He modeled the coun-try’s first program after UCLA.
His most recent discovery of a critical area in the brain, where stimulation enhances memory, gained recognition around the world. Being in the top 10 finalists for the Global B.R.A.I.N. prize really translates to being one of the top neuroscientists in the world. He has spent many years studying the hippocampus, the memory’s mainframe. The stimulation, electrical currents, applied through the elec-trodes implanted in the brain, turned out to be most effective in the entorhinal cortex, the golden gateway of the hippocampus.
The next challenge is to determine if a brain pacemaker, electrodes implanted in the brain, which are currently used to treat movement disorders such as Parkinson’s disease and es-sential tremor, could be used for patients with memory disorders such as dementia, stroke, epilepsy or brain injury.
“This kind of clinical research and patient care is a lifelong marathon, not for sprinters,” Dr. Fried said. “There is still much work to be done. Looking back does capture some amazing moments. It is a great source of satisfaction to change a person’s life for the better through brain surgery, and at the same time learn the fundamentals of the human condition.”
A
UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND44 | ADULT EPILEPSY SURGERY PROGRAM

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND ADULT EPILEPSY SURGERY PROGRAM | 45
Every patient is unique and special. We direct our efforts to remove brain networks responsible for
seizures while preserving those networks responsible for the function and well-being of the individual.
—Itzhak Fried, MD, PhD, Director of the Adult Epilepsy Surgery Program
“”
or more than 50 years, UCLA has led the world in the diagnosis, manage-ment and surgical treatment of in-tractable epilepsy for children and
adults. Our Seizure Disorder Center performs between 40 and 50 surgeries annually. UCLA’s neurosurgeons pioneered many of the innova-tions in the evaluation and surgical treatment of seizure disorders since its inception.
The UCLA team has performed more than 1,000 surgeries to stop seizures in children and adults suffering from epilepsy. UCLA has a long history of treating epilepsy, having pioneered surgical
procedures for the treatment of epilepsy since 1961. Itzhak Fried, MD, PhD, Director of the Adult Epilepsy Surgery Program in the Department of Neurosurgery at UCLA and Co-Director of the UCLA Seizure Disorder Center, and his team, are world-class experts, specializing in the advanced diagnosis, treatment and management of epilepsy. We intersect a wide range of specialties including: neurosurgery, neurology, clinical neurophysiology, electrophysiology, neuropsychology, occupational therapy, psychiatry, neuroradiology, specialized nurses in epilepsy, EEG technologists skilled in epi-lepsy, epileptology and physiology.
F

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND46 | ADULT EPILEPSY SURGERY PROGRAM
ur outcomes for epilepsy surgery lead the world because we use an advanced, three-pronged pro-tocol developed at UCLA, which
is the standard for neurosurgeons worldwide. In the first phase, we evaluate patients in our te-lemetry unit, which is equipped with video and non-invasive scalp electroencephalograph elec-trodes, to document and characterize seizures. As part of the evaluation, patients undergo ex-tensive brain imaging, including advanced MRI protocols such as T1- and T2- weighted inversion
recovery, FLAIR, 3D reconstruction, diffusion tensor imaging (DTI) and positron emission to-mography (PET) scans. In some cases a special technique probing magnetic dipoles in the brain (magnetic source imaging) is used.
The findings are then presented to the epilepsy surgery team, a panel consisting of neurologists, neurosurgeons, electrophysiologists, radiolo-gists, psychologists and our coordinating clini-cal nurse specialist. If the source of the seizures cannot be localized or if it is near a language or movement center of the brain, we will perform
stimulation mapping using subdural (over the surface of the brain) or depth electrodes implant-ed in the brain. The patient will then undergo another round of observation and recording of the seizures in the telemetry unit. In the final phase, our team uses imaging technology, including electrocorticography (ECoG), functional brain mapping and intra-operative image guidance to map the route to the region of the brain, while protecting vital control centers. Finally, the neu-rosurgeon removes the abnormality in the brain and as result eliminates the seizures.
O
SETTING THE GOLD STANDARDNeurosurgical Protocol for Epilepsy Developed at UCLA
Surgery for epilepsy was once seen as a last resort for patients and was only performed when anti-seizure medications failed to stop the seizures. A recent, evidence-based, multi-center study led by UCLA set the guidelines that if a patient continues to ex-perience seizures after two anti-seizure medications have failed, then an evaluation for surgery from a comprehensive epilepsy center should not be delayed.
The recent controlled, randomized UCLA study published in the Journal of the American Medical Association in March 2012, ex-amined 38 patients who failed to have seizures controlled after trying two anti-seizure drugs. The team randomly assigned 15 to brain surgery and 23 to continued medical treatment, all patients were similar in age and diagnosis. During the second year follow ups, the 23 patients on anti-seizure medications still suffered from seizures. Eleven of the brain surgery patients were seizure free.
Evidence-based research now shows that surgery should be considered as soon as possible. Epilepsy will strike one in a hundred Americans at some point in their life. Seizure disorders are rising in people after the age of 60 and will continue to in-crease as the baby boomers age. Research has shown patients
UCLA STUDY SHOWS THAT SURGERY CAN LEAD TO A SEIZURE-FREE LIFEResearch Shows Surgery Should Not Be Delayed
live an average of 22 years with uncontrolled seizures before con-sidering surgery. On average, patients living with uncontrolled seizures are at increased risk for drowning and other fatal ac-cidents. Depression, progressive memory loss and other cognitive disorders debilitate these patients’ quality of life. Children are at risk for slow-to-no development of vocational and social skills. Our evidence now shows patients should consider evaluation for surgery early, before the harmful consequences become irrevers-ible. With 50 years dedicated to the surgical treatment of epilepsy, we are world leaders in helping hundreds of patients go on to live productive, seizure-free lives.

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND ADULT EPILEPSY SURGERY PROGRAM | 47
1ST1960 18CHRONIC MICROELECTRODE
RECORDINGS FROM PATIENTS WITH EPILEPSY
YEAR THE EPILEPSY SURGERY PROGRAM WAS
ESTABLISHED AT UCLA
SURGICAL TREATMENT OF 18 DIFFERENT TYPES
OF EPILEPSY
1,000MORE THAN 1,000
SURGERIES PERFORMED TO TREAT SEIZURES
CONDITIONS TREATEDAicardi syndrome Cortical dysplasia Epilepsy caused by small tumors of blood vessel malformations Epilepsy where resection is not an option
Epilepsy where seizure focus is near functional area of brain Extratemporal lobe epilepsy hemimegalencephaly Hippocampal sclerosis Lennox-Gestaut syndrome
and other epilepsies with drop attacks Mesial frontal lobe epilepsy Mesial temporal lobe epilepsy Perinatal strokes Rasmussen encephalitis
Sturge-Weber syndrome Trauma Tuberous sclerosis complex Tumors, especially DNET and low grade gliomas Unilateral polymicrogyria
ADULT EPILEPSY PROGRAM
History of Firsts
Gary W. Mathern, MD, PhDDIRECTOR, PEDIATRIC EPILEPSY SURGERY PROGRAM
Jerome Engel, Jr., MD, PhDDIRECTOR, SEIZURE DISORDER CENTER
Sandra Dewar, RN, MSCLINICAL DIRECTOR, SIEZURE DISORDER CENTER
WHO WE ARE
Itzhak Fried, MD, PhD PROGRAM DIRECTOR
First chronic depth electrode recordings for epilepsy.
First EEG telemetry for epilepsy.
First chronic microelectrode recordings from patients with epilepsy.
First correlation of electrophysiological characteristics of epileptic hippocampus with tissue pathology obtained from en bloc anterior temporal resections.
First laboratory to establish parallel human/animal research protocols for epilepsy
First PET scans for epilepsy diagnosis.
First long-term EEG monitoring with sphenoidal and scalp electrodes
First to established multidisciplinary Phase I and Phase II protocols for surgery.
First to hold a comprehensive international conference on epilepsy surgery (First Palm Desert Conference, 1986).
First to establish an internationally-accepted classification of surgical outcome (the Engel Classification).
First to identify pathological high frequency oscillations (pHFOs) as biomarkers of the epileptogenic region.
Among the first to demonstrate widespread neocortical thinning as characteristic of classical mesial temporal lobe epilepsy with hippocampal sclerosis.
First to establish an epilepsy surgery program in Israel.
tzhak Fried, MD, PhD, Director of the Adult Epilepsy Surgery Program at UCLA, uses depth electrodes implanted in patients with epilepsy to localize seizures in the brain for diagnosis and surgery. Simultaneously, he studies the fundamental functions of the neurons in an effort to develop applications to restore lost neurological function due to epilepsy, memory disorders such as Alzheimer’s disease or stroke. Recently
published in the 2013 February issue of the Scientific American, he and his UCLA team reported on recording a single brain cell, the Jennifer Aniston neuron, which revealed how neurons code and shape human memories. In his latest research published in the September 2013 issue of Nature Neuroscience, he and a team of neuroscientists discovered the grid cells, like GPS in the brain, which help people keep track of their location while moving in an unfamiliar environment.
I
A RECORD OFDISCOVERY & INNOVATION

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND48 | ADULT EPILEPSY SURGERY PROGRAM
RICK SMITH
ROCKETSURGERY
ADULT EPILEPSY SURGERY PROGRAMPATIENT HIGHLIGHT
e felt a bolt of lightening strike his head and body. A blackout fol-lowed. Rick Smith, an aerospace engineer, slipped out of his office
chair and onto the floor at Wyle Laboratories. He had just celebrated his big 4-0. Until that first grand mal seizure, he was healthy.
Another engineer entered his office to see Rick convulsing on the floor. He dialed 9-1-1. When Rick came to, an ambulance crew was surrounding him. After that initial seizure, his driving privileges were restricted. Fortunately, his wife, Karen, worked at the laboratory, so he was able to continue working. Even with antiseizure medications, Rick endured un-expected seizures, most commonly complex partial seizures, or “stare-offs”, for more than nine years. Everywhere he went, he had to think about the impact a seizure would have on him and those around him.
In search of a life beyond his seizures, he met with Sandra Dewar, RN, MS, Jerome Engel, Jr.,
MD, PhD, Itzhak Fried, MD, PhD, and a large team of doctors at the UCLA Seizure Disorder Center to determine if he was a surgical can-didate. He discovered all of the potential cat-alysts to his adult onset epilepsy. They asked him a series of questions. He answered yes to each one, from having experienced blows to the head and exposure to chemicals, to experienc-ing high levels of stress.
The team of clinicians explained that Rick would need to check into the hospital for a set of studies, which included 24-hour supervised video EEG monitoring so the medical team could pinpoint the start of the seizures. The clinicians found the scar tissue in his brain where the overactive cells misfired during an epileptic seizure. They were confident they had isolated the problem area. Next, the Wada test was done. This required a portion of his brain to be anesthetized while they tested his neurological, motor, and verbal functions. He passed with flying colors. He recalls one of the
happiest days of his life was when Dr. Fried emerged from a huddle with his research team and said to Rick, “We believe you’re a candi-date for surgery.”
Rick underwent brain surgery by Dr. Fried to have the scar tissue removed and, in return, got his old life back. Today, at age 60, 12 years after surgery, Rick is seizure-free. He is a grandfather with two grandsons. His son now works at the laboratory with him.
Rick continues to pursue his work at NTS Technical Systems in Santa Clarita, CA, with a passion. He is so grateful to enter his golden years without having to rely on medications to control his seizures.
“I cannot believe they cured my epilepsy. It’s a medical miracle. My only regret is not undergoing surgery sooner. I could have saved myself from suffering from nine years of sei-zures. I want to blast it out to anyone suffer-ing from epilepsy to go to UCLA. You can live seizure-free.”
H

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND ADULT EPILEPSY SURGERY PROGRAM | 49
Itzhak Fried, MD, PhD
Itzhak Fried, MD, PhDNEUROSURGERY
Jerome Engel, Jr., MD, PhDNEUROLOGY
Susan Bookheimer, PhDNEUROPSYCHOLOGY
Sandra Dewar, RN, MSCLINICAL NURSE SPECIALIST
RICK’S TEAM
Professor in Residence and Director of the Epilepsy Surgery Program, Dr. Fried’s research and clinical work is dedicated to the treatment of intractable seizure disorders and epilepsy.
I cannot believe they cured my epilepsy. It’s a medical
miracle. My only regret is not undergoing surgery sooner. I could have saved myself from suffering from nine years of seizures. I want to blast it
out to anyone suffering from epilepsy to go to UCLA. You
can live seizure-free.—Rick Smith
“
”
A TRIBUTE TOPAUL H. CRANDALL A PIONEER IN THE SURGICAL TREATMENT OF EPILEPSY
n remembrance, we honor Paul H. Crandall, the father of the Epilepsy Surgery Program at UCLA and pioneer in the
surgical treatment of epilepsy. He was one of the founding members of the neurosurgery division, which became a department in 2008. Dr. Crandall cared for patients, conducted clinical research and taught for 32 years. He retired in 1988 as a professor emeritus and passed away in 2012.
Dr. Crandall started UCLA’s first research
program in the surgical treatment of epilepsy in 1960. He also led one of UCLA’s longest running NIH grants and was responsible for developing the first seizure-monitoring unit.
During NASA’s early Gemini orbital mission, Dr. Crandall heard mission control reporting an astronaut’s heart rate. Intrigued, he contacted NASA to find out how they were able to remote-ly monitor heart rate and transmit multiple channels of data back to earth. He obtained the FM telemetry device from NASA and con-nected it to electrodes implanted in the brain
to record signals on a reel-to-reel recorder. This led to 24-hour monitoring of the patient and the recording of the first seizure at UCLA in 1968. Soon after, he simultaneously video re-corded the patient to compare external behav-ior with brain activity. Using these recordings, Dr. Crandall honed in on the brain cells causing the seizures. He would then remove those cells in surgery and thus put an end to the seizures. Today, EEG telemetry protocols that Dr. Cran-dall developed are the standard used in hospi-tals worldwide.
DR. ALFONSINA Q. DAVIES ENDOWED CHAIR IN HONOR OF PAUL CRANDALL, MDThomas and Nadia Davies invested more than a decade in search of a solution for the epileptic seizures that debilitated their daughter, Alfonsina, “Nina”, since her birth. In 1977, Dr. Crandall performed an experi-mental brain surgery on their 17-year-old daughter to end her seizures. She went on to earn her doctoral degree in education and become the Assistant Superintendent of the Santa Ana School District. Nina helped many children with disabilities get a second chance at life, just as she had received.
Decades later, in 2011, Nina passed away
I
due to SUDEP (Sudden Unexpected Death in Epilepsy). In memory of their daughter and in honor of Dr. Crandall, the Davies established an endowed chair in their names to continue to support UCLA as a world-leader in the surgical treatment of epilepsy for generations to come. Dr. Crandall’s spirit will live on in the Chair awarded to a preeminent physician-scientist with a history of creativity, innovation and willingness to view old problems in new ways with new technology. With the support this endowment provides, thou-sands more patients suffering from epilepsy will live in a future without seizures.
(TOP L-R) NADIA & THOMAS DAVIES(BOTTOM L-R) DR. PAUL CRANDALL & ALFONSINA DAVIES

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND50 | UCLA BRAIN INJURY RESEARCH CENTER
RAISING AWARENESS ON SPORTS CONCUSSIONS IN THE NATIONAL FOOTBALL LEAGUEDr. Hovda has been an internationally-recognized expert on concussion awareness for over two decades. He helped the National Football League in the 1990s recognize the po-tentially detrimental side effects of multiple concussions on the football field. His research and education have helped the NFL set practices to diagnose the symptoms of an initial concussion and remove players from action while the brain shuts down to repair itself.
BRAIN INJURY RESEARCH CENTER
avid A. Hovda, PhD, is the found-ing and current Director of the Brain Injury Research Center and the Vice Chair for Research
for the Department of Neurosurgery at UCLA. His early discoveries of the detrimental effects concussions have on the brain led to the mili-tary and the National Football League recog-nizing traumatic brain injury (TBI). In 2011, the White House appointed Dr. Hovda to the Defense Health Board, a team of 14 experts from across the country to advise the Secretary of Defense on matters dealing with the health and care of
service members. The appointment came as a result of Dr. Hovda receiving the highest civil-ian honor in 2011, the Strength of the Nation award, for his efforts to save troops suffering from multiple concussions on the battlefield, as well as his research that led to a standardized recovery protocol for warriors wounded from brain trauma. He was a key expert in establish-ing the National Intrepid Center of Excellence in Bethesda, Maryland which focuses on diag-nosing, treating, managing and studying service members with TBI, and educating families on the long-term effects of concussions.
D
THE UCLA SPORTSCONCUSSION CLINIC & BRAIN SPORT PROGRAMChristopher C. Giza, MD, opened the UCLA Sports Concussions Clinic to diagnose, treat and manage concussions for both young and profes-sional athletes. Dr. Giza’s team also educates parents, coaches and leagues about preventing multiple concussions. His Brain Sport Program works with high schools and colleges to obtain baseline neurological exams pre-season so that, if a head injury is sustained during the season, physicians can properly diagnose the concussion.
This year, Dr. Giza announced the first evi-dence-based guidelines for the management of sports-related concussions at the American Academy of Neurology meeting in San Diego. If a concussion is suspected, players must be im-mediately removed from the game followed by an evaluation by a licensed health care professional.
DR. HOVDA RECEIVING THE STRENGTH OF THE NATION AWARD

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND UCLA BRAIN INJURY RESEARCH CENTER | 51
BIRC UCLA IS AN OFFICIAL ADVISOR TO:California Athletic Commission
US Department of Defense
National Football League
World Boxing Council
Major League Baseball
Medical Research Council
NATO
NCAA
PROTECTING OUR TROOPS FROM TRAUMATIC BRAIN INJURY
BRAIN INJURY RESEARCH CENTER
BIRC PROGRAM
History of Firsts
Total NIH Funding
$15,597,410TOTAL NIH/NON-NIH GRANTS, INCLUDING DIRECT & INDIRECT COSTS, FOR THE DURATION OF THE RESEARCH PERIOD
NIH Grants
WHO WE AREDavid A. Hovda, PhD DIRECTOR
he UCLA Brain Injury Research Center (BIRC) experts have extended their ex-
pertise to protect our soldiers from traumatic brain injuries (TBI) and multiple concussions—the signa-ture wounds of the Afghanistan and Iraq wars. At the request of the Joint Chiefs of Staff U.S. Army, David A. Hovda, PhD, formed a team to visit Afghanistan to set up concussion care centers, concussion units and the installation of three MRI scan-ners. His research inspired the mili-tary’s protocols for the diagnosis, treatment and management of TBI as well as increased awareness of
concussions among the troops. IED blasts have made TBI, which gradu-ally erodes the nervous system, the silent killer of these wars.
Christopher C. Giza, MD, an as-sociate professor of neurosurgery at UCLA, travelled to the frontlines of Afghanistan to oversee the estab-lishment of these programs. Con-cussion units were built to provide protective environments for soldiers in the vulnerable recovery stage. In addition, concussion care centers were put in place, complete with MRI scanners and experts trained in protocols that will decrease the vast numbers of soldiers carrying these invisible wounds home from war.
T
Christopher C. Giza, MD, Paul M. Vespa, MD,Neil A. Martin, MD, Tom C. Glenn, PhD, Fernando Gomez-Pinilla, PhD,
Neil G. Harris, PhD, Grace Griesbach, PhD, David McArthur, PhD, Mayumi Prins, PhD, Richard L. Sutton, PhD
DR. GIZA (2ND FROM LEFT) WITH TROOPS AT THE KANDAHAR AIRFIELD
First to describe a metabolic cascade following TBI.
First to describe the cost of mild TBI in the capacity for plasticity during development.
First to redefine the role of the fuel glucose after TBI.
First to use quantitative positron emission tomography after TBI.
First to combine cerebral micro-dialysis, positron emission to-mography along with monitoring in ICU.
First to be recognized by the US Army and Marine Corps for help in mild TBI.
First to establish a University of California annual meeting on TBI.
First to describe the neuroscience between TBI, PTSD and Parkin-son’s Disease.
First to map the regional brain volumetric changes and connec-tions across time after TBI.
First to describe the neuroscience of diet and exercise on recovery after TBI.

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND
Neuro ICU
52 | NEUROCRITICAL CARE PROGRAM
Paul M. Vespa, MDPaul M. Vespa, MD

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND NEUROCRITICAL CARE PROGRAM | 53
RONI (Robot of the Neuro-ICU) was the world’s first ICU robot and was pioneered right here at UCLA in 2005. In the case of a stroke, when minutes mean the difference between preserving or losing brain function, RONI enables the neurocritical care specialist to beam into the neuro-ICU and be virtually bedside with the patient in minutes. Under the control of the physician at a computer away from the ICU, the 5’6 robot has a head that is a flat screen projecting the physician’s face allowing for real-time, two-way, face-to-face commu-nication with the nursing staff, patients and families in the ICU. The telepresence is remarkably human in nature enabling the physician to conduct a neurologi-cal exam on a patient. Studies have demonstrated that RONI can decrease morbidity, mortality and length of patient’s stay. The concept of a robot-doctor is now be-coming a new standard of care across the United States.
Based on our experience with RONI, we have just launched the next generation of telerobotics, the iRo-bot-Doc EVA, Executive Virtual Attending physician. EVA represents a big step forward since it can drive itself around the ICU using autonavigation and can be operated via iPad by the push of a button. EVA saves time by moving to the bed of a patient in distress while the doctor checks the electronic medical record for critical information. EVA’s high-resolution optics and real-time data displays enable a full evaluation of the patient by the remote doctor. UCLA is using this technology to bring our expertise to our community hospitals so that neurocritical specialists can save lives through remote consultations. In this way, we hope to deliver the best care anywhere, anytime.
Changing outcomes requires changing our treatments. At UCLA, we pioneered continuous EEG in the Neuro-ICU to detect silent seizures that occur in 24 percent of brain trauma patients and can result in elevated in-tracranial pressure. This innovation is becoming a new standard of care internationally. Dr. Vespa and UCLA bioengineers have received an NIH grant to develop
and test a bedside monitor/alarm system to detect rising intracranial pressure. The team is using big data software by IBM to analyze in real-time streams of physiological signals coming from the bedside monitor to predict the elevation of intracranial pressure. This takes our care in the ICU from responsive to a predic-tive and preventative approach.
INVENTING A NEW PREDICTIVE MODEL
INVENTING THE FUTURE: 24/7 ROBOTICS & TELEMEDICINE
IROBOT-DOC:REVOLUTIONIZING ACCESS
We invent the future of critical care toenable the future for our patients.
—Paul M. Vespa, MD, Director of the Neurocritical Care Program”“
ur neurosurgical/neurological ICU is a world-leader in providing patients with minute-to-minute, 24-7 critical care. In the 24-bed, state-of-the-art
ICU, Paul M. Vespa, MD, a renowned neurocritical care specialist, leads an elite team of neurosurgi-cal and neurological residents, respiratory tech-nologists, electroencephalography (EEG) technolo-gists and specialized neuroscience nurses. Each patient is continuously monitored with EEG, cerebral
microdialysis, brain oximetry, the world’s first ICU Robot—built by InTouch Health—and a comprehen-sive ICU Supercomputing System. Additionally, the Edie Baskin Bronson and Richard “Skip” Bronson Cerebral Blood Flow laboratory provides advanced diagnostics of cerebral circulation using transcra-nial Doppler and XENON-133 CBF measurement. Adjacent to the ICU are CT, MRI and PET scanners to ensure rapid response to any critical event.
O

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND54 | UCLA CENTER FOR NEUROMODULATION & NEUROBIONICS
Nader Pouratian, MD, PhD

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND UCLA CENTER FOR NEUROMODULATION & NEUROBIONICS | 55
he UCLA Neuromodulation and Neu-robionics Program brings together a world-class team of neurosurgeons, neurologists, psychiatrics, pediatric
neurologists and psychiatrists, electrophysiolo-gists, bioengineers, computer scientists and neuro-scientists specialized in deep brain stimulation for movement disorders such as Parkinson’s disease, essential tremor and dystonia and other neurologic and psychiatric diseases.
Our team is a national leader, having treated more than 500 patients with brain pacemakers since the program’s inception. Each week, we treat one to two
patients. We are pioneers in the use of stereotaxis in deep brain stimulation with a vast experience in computer-assisted image guidance that allows us to implant the brain pacemakers with precision.
Our team of experts in brain pacemaker implants are improving and extending quality of life for patients who have reached a stage where medications are no longer reliable. In advancing deep brain stimulation, the team is launching early clinical trials, implanting electrodes deep in the brain to stimulate neuronal ac-tivity in patients suffering from severe depression and obsessive compulsive disorder.
T
The brain is a complex electrical circuit. Neurobionics is the electronic interface with the human brain. We implant electrodes to stimulate or, in
essence, reset the electrical activity for people debilitated by their disease.
—Nader Pouratian, MD, PhD, Director of the Neuromodulation & Neurobionics Program
“”

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND56 | UCLA CENTER FOR NEUROMODULATION & NEUROBIONICS
500TH PATIENT IMPLANTED WITH A BRAIN PACEMAKER AT UCLA
r. Nader Pouratian, MD, PhD, has been conducting research using imaging techniques to map the human brain and elec-
trical recording techniques to decode the signals that neurons use to communicate with each other. Essentially, he is translating
neuronal language. The first generation of this brain-computer interface uses an elec-trode cap on the patient’s head that translates thoughts or brain signals into letters that can be spelled out on a computer screen. The goal is also to reconstruct sounds into language using the brain-computer interface known as
the translator—using electrodes connected to the brain and a computer that interprets what you are trying to say. Next-generation nano-electrodes implanted in the brain will trans-late thoughts or intended activities connected to a brain-computer interface embedded in a prosthetic arm or leg.
Celebrating the 500th patient implanted with a brain pacemaker at UCLA, Dr. Nader Pou-ratian performed the surgery and shared the experience with 40 million viewers from around the world on Twitter.
It was the first awake brain surgery to be publicly shared using Twitter and vid-eo-based social media platform Vine. The patient, Brad Carter, a 39-year-old actor and musician from Los Angeles, played a guitar in the operating room while Dr. Pouratian tested the electrical impulses to stimulate his brain and slow his benign es-sential tremor.
In the summer of 2006, the tremors began in his hands and eyes. Medications failed to stop the tremors that gradually deteriorated his career as musician and song writer.
“Little by little, it steals you,” Brad said about the uncontrollable tremors. “I felt my creative life vanishing. I wanted to prolong my creative life, my life.”
In a medical miracle moment caught on Vine and posted on Twitter, Brad’s tremors slowed and he played the guitar live in the OR. “And he was really good,” Dr. Pouratian said.
Once the videos posted, they rapidly circled the globe like a grapevine. Millions of folks watched in awe, including William Shatner who shared the Vines with fans, friends and followers. Brad is no stranger to cameras. He has acted on shows such as CSI,
D
NEXT GENERATIONTranslating Brain Signals into Language and Movement
First Live-Tweeted Brain Surgery in the World
Dexter and the Mentalist. Brad brought his guitar into the operating room with hopes of
fine-tuning the stimulation, so he could return to his passion and perform live again. After his second surgery to have the battery placed and his pacemaker programmed, Brad appeared on stage at UCLA to play guitar live, captivating the world once again.
“There’s nothing like losing a skill that you were really good at to make you want to have that skill back,” Brad said. “I can’t wait to be creative again and I can’t wait to play guitar again. I’m very excited to record an album as this gets better.”

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND UCLA CENTER FOR NEUROMODULATION & NEUROBIONICS | 57
NEUROMODULATORSRAISING THE BAR FOR DEEP BRAIN STIMULATION
OUR THERAPIES Deep brain stimulation (DBS) Intrathecal infusion pumps Microvascular decompression
Motor cortex stimulation Radiofrequency ablation Spinal & peripheral nerve stimulation
Stereotactic radiosurgery
710 1STINVESTIGATING USE
OF DBS IN 7 NEW APPLICATIONS
OUR WORLD-CLASS EXPERTS INTERSECT 10 MEDICAL SPECIALTIES
TO UTILIZE STEREOTAXIS IN DEEP BRAIN STIMULATION
500MORE THAN 500 DEEP BRAIN STIMULATIONS
PERFORMED
NEUROMODULATION& NEUROBIONICS
ader Pouratian, MD, PhD, Director of the UCLA Center for Neu-romodulation and Neurobionics, and his team is currently de-veloping and testing a sensing generator that will continuously record signals
in the brain and automatically program the frequency of the stimulation to deliver the therapy in real time without the physician and patient needing to fine-tune. This will improve the current method to implant electrodes and later fine-tune the stimula-tion. The sensing generator will automate and personalize deep brain stimulation.
N
Yvette Bordelon, MD, PhD,Allan Wu, MDNEUROLOGY
Antonio De Salles, MD, PhDDIRECTOR OF FUNCTIONAL NEUROSURGERY
Tania Kaprealian, MDRADIATION ONCOLOGY
Susan Y. Bookheimier, PhD,Alexander Bystritsky, MD, PhDPatricia Walshaw, PhDDEPARTMENT OF PSYCHIATRY AND BIOBEHAVIORAL SCIENCES
Jeff Bronstein, MD, PhDNEUROLOGY, DIRECTOR OF UCLA MOVEMENT DISORDER PROGRAM
INTERDISCIPLINARY TEAM
Nader Pouratian, MD, PhD PROGRAM DIRECTOR
Future Therapy
Doctor Highlight
We are investigatingdeep brain stimulation for:
Tourette’s syndrome Post-traumatic Stress Syndrome Dementia Depression Addiction Morbid obesity Tinnitus
YVETTE BORDELON, MD, PHD, IS ASSISTANT PROFESSOR OF NEUROLOGY SPECIALIZING IN MOVEMENT DISORDERS.
BRAIN PACEMAKER IMPLANTED TO TREAT PARKINSON’S
A wide range of neurological diseases cause tremors, spasticity, muscle rigidity, pain and other movement disorders. These symptoms are produced by irregular activity in the brain. Neuromodulation can be effective for patients who have not responded sufficiently to other less-invasive treatment options for conditions such as the following:
Movement Disorders: Parkinson’s disease, essential tremor,dystonia (including cervical dystonia).
Spasticity: Multiple Sclerosis, cerebral palsy, stroke, spinal cordinjury, head injury.
Pain: Trigeminal neuralgia, occipital neuralgia, cluster headaches,migraines.
Psychiatric Disease: Obsessive Compulsive Disorder.
Conditions Treated

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND58 | UCLA CENTER FOR NEUROMODULATION & NEUROBIONICS
NEUROMODULATION & NEUROBIONICSPATIENT HIGHLIGHT
RICHARD ROTHENBERG
THE BIONICMAN
ichard Rothenberg walked on Main Street with his family at Disneyland. It was turning out to be a memorable day, though
not exactly the kind of memory for the family photo album. Pain racing like wildfire through his knees, elbows and hips became devastat-ingly clear to him. He recalls the moment as the line of demarcation splitting his life into two distinct halves.
While threading through the crowd, his cousins, both doctors, listened to Richard describe the radiating pain that his orthope-dist and acupuncturist failed to control. His cousins detected a neurological problem, the type they see in the elderly, not a 37-year-old man in the prime of his life.
Richard went to UCLA to see Jeff Bronstein, MD, PhD, a renowned neurologist. The neu-rological test and MRI scans confirmed his cousins’ suspicions of Parkinson’s disease.
“I started to deteriorate,” Richard said.
“It came in peaks and valleys. At my worst I would become completely paralyzed unable to move for 45 minutes to an hour, for 4 to 5 times a day. All I could do was lie down and hope being frozen would pass. It was a terrifying ex-perience. Even though I knew it would pass, I felt like I was never going to move again.”
The medications worked initially, but then ceased. In denial, he refused to consider Dr. Bronstein’s recommendation for surgery. Gradually, his work and family slipped away. He moved in with his parents because he could no longer take care of himself. His ex-wife took care of his children. The days turned into years.
Then a wake-up call came in the form of a lung infection that exacerbated the Parkin-son’s symptoms. He visited Dr. Nader Poura-tian to explore a brain pacemaker.
“On my first visit with Dr. Pouratian, I imme-diately had a good feeling about him,” Richard said. “He had very steady hands and a firm
handshake. He also made me feel confident and was very tolerant of all my family asking him a million questions. With this procedure, bedside manner is important, as you’re awake for part of the surgery.”
Six years after his initial diagnosis, Richard began an awake craniotomy for deep brain stimulation.
“The effect of the procedure was instanta-neous. When they switched me on, my nerves felt smooth—for the first time in a long time. It was truly magical. I’m the envy of all my non-bionic friends. The affect this has had on my life with my kids—I can now be a physically active father.”
Richard returned to work as a banker and enjoys being able to participate in physical ac-tivities with his kids.
“My daughter really only knew me with Parkinson’s disease,” Richard said. “It’s a new life for us now. Miracles can happen.” This year, Richard fell in love, married, and is now the father of twins.
R

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND UCLA CENTER FOR NEUROMODULATION & NEUROBIONICS | 59
Nader Pouratian, MD, PhD
Nader Pouratian, MD, PhDNEUROSURGERY
Arik Johnson, MDNEUROLOGY/PSYCHOLOGY
Eric BehnkeCLINICAL SPECIALIST IN OR
Susan Bookheimer, MDNEUROPSYCHOLOGIST
Yvette Bordelon, MD,Jeff Bronstein, MDNEUROLOGY
RICHARD’S TEAM
The effect of the procedure was instantaneous. When they switched me on, my nerves felt smooth—for the first time in a long time. It was truly magical. I’m the envy of all my non-bionic friends. The affect this has had on my life with my kids—I can now be a physically active father.
“”
Dr. Pouratian’s primary neurosurgical interest is in surgeries that preserve and restore function to patients, including movement disorder surgeries, surgeries for psychiatric conditions and surgeries for peripheral nerve injuries and tumors.
First to provide image guidance of deep brain stimulation surgery.
First to provide comprehensive surgical management of peripheral nerve disease.
NEUROMODULATION& NEUROBIONICS
History of Firsts
Total NIH Funding
$968,996TOTAL NIH/NON-NIH GRANTS, INCLUDING DIRECT & INDIRECT COSTS, FOR THE DURATION OF THE RESEARCH PERIOD
NIH Grants
—Richard Rothenberg
RICHARD’S TIMELINE
2005 Richard is diagnosed with Parkinson’s at UCLA.
Medications temporarily control the disease. 2006
His life deteriorates. Richard can no longer work, take care of himself or be a father to his children.
2010
2007-09 Medications cease to be effective and the disease gradually takes over his body.
Brain pacemaker is implanted, giving Richard a new lease on life. He returns to work and finds joy in once again becoming an active father.2011
Richard gets married and fathers twins.
2012
We have performed more than 500 deep brain stimulation surgeries, more than any other center in Southern California.
We have pioneered the use of stereotaxis in deep brain stimulation.
Our extensive experience in computer-assisted image guidance allows us to implant brain pacemakers with precision.
We perform the DBS procedure using an “asleep-awake-asleep” craniotomy ensuring patient comfort and in-depth testing to optimize outcomes.
Besides deep brain stimulation, we perform spinal cord stimulation, peripheral nerve stimulation, and other innovative procedures almost daily.
Highlights

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND60 | UCLA SPINE CENTER
Langston T. Holly, MD

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND UCLA SPINE CENTER | 61
Our Spine Center gives patients access to a team of experts working together to evolve the optimal treatment plan. We weigh the options
of non-invasive and minimally-invasive approaches to eliminate chronic pain and get them back to normal daily living. We take the
journey with our patients from surgery through rehabilitation.
—Langston T. Holly, MD, Director of the UCLA Spine Center
“”
he UCLA Spine Center is one of the only academic spine programs in the country with a completely integrated practice that incorporates neurosurgeons, or-
thopaedic surgeons, physiatrists and clinical scientists in one seamless unit. Langston T. Holly, MD, Director of the UCLA Spine Center, specializes in neurosurgery and collaborates with specialists in orthopedic care to lead a world-class spine team in the diagnosis, man-agement and treatment of spinal disorders, spinal in-juries, chronic spinal pain and degenerative spinal dis-eases. Our experienced surgeons performed more than 900 surgeries last year.
The UCLA Spine Center leads the nation in National Institute of Health (NIH) spine research funding. Active research programs include basic and clinical science for spinal cord injury research as well as advanced imaging techniques for the evaluation of degenera-tive spine disease. It is also one of the very few centers in the world with the ability to readily translate basic science breakthroughs discovered in the laboratory
to the treatment of spinal disorders in patients. We are leaders in the bench-to-bedside approach, which translates to our patients receiving unique cutting-edge treatments and innovative surgical techniques that op-timize outcomes and improve recovery and function.
Additionally, UCLA has a tradition of treating pa-tients with Chiari malformation and with syringomy-elia, going back over 30 years. We have treated more than 350 patients with Chiari malformation and more than 150 patients with syringomyelia. Chiari malfor-mation and syrinomyelia are complex entities, which are frequently missed in diagnosis. Our panel of spe-cialists who constitute a center for the treatment of these disorders is also involved in disseminating infor-mation among the medical community, patients and their families.
The human spine is the strength and nerve center of the human body, for this reason, our neurosurgeons are committed to the full recovery of our patients every step of the way from the evaluation through surgery and rehabilitation.
T

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND62 | UCLA SPINE CENTER
aniel Lu, MD, PhD, Assistant Pro-fessor of Neurosurgery and Direc-tor of the Neuromotor Recovery and Rehabilitation Center, and
Reggie Edgerton, PhD, Distinguished Pro-fessor of Integrative Biology, are conducting groundbreaking translational bench-to-bed-side research to stimulate lost motor function in six patients inflicted with a spinal cord injury that has resulted in paralysis of the extremities. The clinical trials are modulating the excitabil-ity of the neural circuits that control the spinal cord. We stimulate these circuits with epidural electrodes placed over the lumbosacral spinal cord. When this stimulation is combined with motor training, the neural circuits become re-markably effective at basic movements, such as standing and stepping and even maintaining balance. The research team is demonstrating that the spinal cord neurons are intelligent and have a memory of these movements to stand
and step with minimal input from the brain. The National Institutes of Health awarded a
significant grant of $6 million to Dr. Lu and Dr. Edgerton to conduct these clinical trials that could have applications for patients with paral-ysis. More than 5 million Americans live with paralysis that results in an inability to move the upper and lower extremities. An estimated 1.3 million suffer from spinal cord injury. Christo-pher Reeve was afflicted with this injury that paralyzed him from the neck down.
New hope for patients with spinal cord injury came when Rob Sommers, 25, para-lyzed for four years as the result of a car ac-cident, stood for 30 minutes and took steps on a treadmill with assistance. This break-through study was published in the presti-gious medical journal, The Lancet in 2011, by Dr. Edgerton and a team of scientists from University of Louisville, the California Insti-tute of Technology and the Pavlov Institute
of Physiology in St. Petersburg, Russia. The stimulation transmited signals that mimiced the brain to initiate motor function. The reha-bilitation retrained the spinal cord network to produce movements to stand and take steps. In addition, after weeks and months of daily stimulation, significant improvement occurred in bladder function, blood pressure control, temperature control and sexual function.
Dr. Lu and Dr. Edgerton are focused on further improving patients’ ability to recover greater levels of motor and autonomic function through the synergistic effects of pharmacological neu-romodulation combined with epidural stimula-tion and locomotor training. The time has finally come when we can tell patients that through novel therapies, they may return to a normal life after their injury, and that here at UCLA, we will be with them every step of the way.
D
RE-ENABLING MOTOR FUNCTIONRestoring Spinal Cord Function by Modulating Spinal Cord Circuitry
At the UCLA Spine Center, we are at the forefront of innovation and technology to improve the treatment of spinal disorders and develop new strategies to increase functional recovery after spinal cord injury. The Neuromotor Recovery and Rehabilitation Center (NRRC) directed by Dr. Daniel Lu, utilizes cutting-edge tools, such as the upper extremity robot, to assess function and test regimens that can improve spinal cord function.
Our researchers utilize advanced molecular techniques and mul-tiple approaches to increase the capacity of nerve cells to establish circuits and process information. The research is also focused on the application of the intrinsic power of nutrients serving as food for the central nervous system, which can help damaged spinal cord circuits improve function and foster rehabilitative strategies.
INNOVATION, DISCOVERY & ADVANCING OF TRANSLATIONAL SCIENCE
THE UPPER EXTREMITY ROBOT IS USED TO ASSESS MOTOR FUNCTION

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND UCLA SPINE CENTER | 63
he University Health-system Consortium (UHC) reviews na-tional academic
medical centers to determine excellence in clinical outcomes, reviewing quality, safety and cost effectiveness. Based on studies concluded in March of 2013, the UHC ranked the UCLA Spine Center at Ronald Reagan UCLA
Medical Center #4 in the nation for spine surgery. The UHC quality and accountability study takes into account and evaluates all 62 aca-demic spine centers in the nation.
T
0%RATE OF REOPERATION FOR
RECURRENT DISC HERNIATION ON101 MINIMALLY INVASIVE LUMBAR
MICRODISCECTOMIES
5,955TOTAL NUMBER OF
SPINE SURGERY CASES SINCE 2005
CONDITIONS TREATEDChiari malformationCongenital abnormalitiesDegenerative disc disease
Disc herniationOsteomyelitisRheumatoid arthritis
ScoliosisSpinal cord tumorsSpinal injury
StenosisSyringomyelia
Ulrich Batzdorf, MD, Daniel Lu, MD, PhD,Duncan Q. McBride, MDNEUROLOGICAL SURGERY
A. Nick Shamie, MDORTHOPAEDIC SURGERY
David Fish, MD, Jae Jung, MDPHYSICAL MEDICINE & REHABILITATION
V. Reggie Edgerton, PhD,Fernando Gomez-Pinilla, PhDRESEARCH SCIENTISTS
INTERDISCIPLINARY TEAM
SPINE CENTER
Coordinated care—neurosurgery and orthopaedic specialists collaborate to evolve the best plan of care to meet the individual needs and lifestyle of our patients.
NIH-funded translational research for spinal cord injury, one of an elite few in the country.
Pioneers in minimally-invasivespine surgery.
Non-invasive spine surgery—the Novalis Tx stereotactic radiosurgery is a focused beam of radiation to treat tumors and abnormalities without spine surgery.
Non-surgical solutions for degenerative spinal conditions include radiofrequency ablation, spinal cord stimulation, spinal injections, trigger point injections, physical therapy, rehabilitation and pain management.
The Spine Center’s educational program is one of the first to integrate orthopaedic and neurosurgical fellows, residents and other international trainees in an active, collegial spine center.
National leader among Spine Centers in NIH funded research.
Langston T. Holly, MD DIRECTOR
HighlightsTOP 5 IN THE NATIONUHC RANKS UCLA AMONG TOP SPINE CENTERS
0%0% RATE OF CEREBROSPINAL
FLUID LEAK ON 101 MINIMALLY-INVASIVE LUMBAR
MICRODISCECTOMIES
#4RANKED #4 IN THE NATION FOR SPINE
SURGERY BY THE UHC
Cases
1,170
874
649
592
406
LOS
1.04
0.71
0.75
1.07
0.81
Readmit Rate
4.44%
4.46%
3.24%
3.38%
5.28%
Spine Center
PENN HOSP
DUHS DUKERALEIGH
URMC HIGHLAND
UCLA SANTA MONICA
NEWTOWN

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND64 | UCLA SPINE CENTER
CODY WILLIAMS
YOUTHFULDETERMINATION
SPINE CENTERPATIENT HIGHLIGHT
n a Friday night in 2009, the first football game of the season at Santa Monica High School, Cody Williams, a junior playing varsity,
tackled the quarterback as he entered the end zone. Cody’s facemask caught on the quarter-back’s knee. Snap. Cody’s head jerked back at a velocity that injured his neck and spine. Cody blacked out. He crashed onto the field. His mother, Stacy, dressed in his jersey embla-zoned with “14” waited for him to get up. “Get up,” she silently repeated over and over as he lay motionless on the field.
The ambulance rushed him to Santa Monica UCLA Hospital. Dr. Langston T. Holly had just emerged from a surgery when he received word of the football player with a spinal cord injury. He was paralyzed from the neck down, essentially a quadriplegic. Dr. Holly saw Cody’s mom wearing his football jersey and he re-membered his own mom wearing his jersey to his football games. He then flashed forward to his own sons playing football.
“I performed the surgery in the same way I
would do it if it was my own son laying there on the operating table,” Dr. Holly said, reflecting on the more than nine hour surgery that it took to stabilize Cody’s neck and spine.
When Cody awoke from surgery, he could move his left arm, which filled his mother with hope. Cody was still quadriplegic, but Dr. Holly set the stage for rehabilitation of his spine to begin.
“To me, I feel like Dr. Holly is an angel sent to the hospital because he did a perfect surgery on me,” Cody said. “If I didn’t have him, I don’t know where I would be today.”
Dr. Holly referred Cody to his colleague Daniel Lu, MD, PhD, the principal investigator on a NIH-funded clinical trial to restore func-tion to spinal cord injury patients. With novel rehabilitation and spinal cord stimulation that harnesses the circuitry of the spinal cord, Cody is seeing meaningful gains in his hands and even his legs.
“Right after the surgery, I couldn’t even sit up,” Cody said. “But now I can sit up, I can swim. I can stand and take steps in physical
therapy. I will walk again.”In June 2011, Cody graduated from Santa
Monica High School and received a stand-ing ovation from the crowd as he accepted his diploma. For him and his Mom, this was a glo-rious, crowning moment in their journey from that night on the football field.
Three months later, Cody was invited to speak on stage at the famous TedX Youth Con-ference in Santa Monica. He took the stage, holding a microphone (a miraculous feat for someone with his injury).
“I came here to talk about staying positive through bad times,” Cody said into the mi-crophone with a bold confidence. “I got hurt a couple years ago, and people always ask me, ‘Why are you so happy?’ I tell them there is really no point in getting down and upset. Getting down will just make you feel worse about it. Staying positive will help you get through it...Today, I can walk 40 steps with a walker.” The audience burst into applause and cheers.
Today, Cody feels stronger than ever.
O
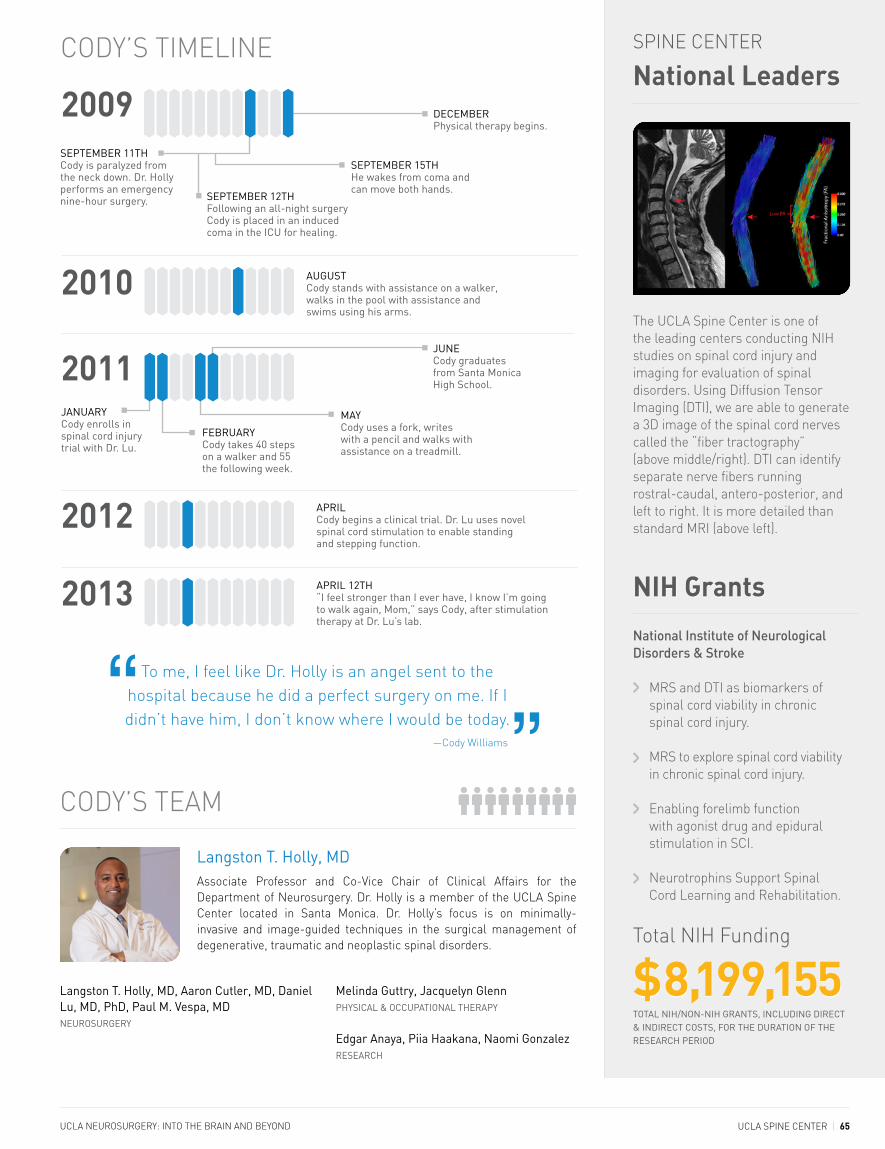
UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND UCLA SPINE CENTER | 65
Langston T. Holly, MD
Langston T. Holly, MD, Aaron Cutler, MD, Daniel Lu, MD, PhD, Paul M. Vespa, MDNEUROSURGERY
Melinda Guttry, Jacquelyn GlennPHYSICAL & OCCUPATIONAL THERAPY
Edgar Anaya, Piia Haakana, Naomi GonzalezRESEARCH
CODY’S TEAM
To me, I feel like Dr. Holly is an angel sent to the hospital because he did a perfect surgery on me. If I didn’t have him, I don’t know where I would be today.“
”Associate Professor and Co-Vice Chair of Clinical Affairs for the Department of Neurosurgery. Dr. Holly is a member of the UCLA Spine Center located in Santa Monica. Dr. Holly’s focus is on minimally-invasive and image-guided techniques in the surgical management of degenerative, traumatic and neoplastic spinal disorders.
—Cody Williams
Total NIH Funding
$8,199,155TOTAL NIH/NON-NIH GRANTS, INCLUDING DIRECT & INDIRECT COSTS, FOR THE DURATION OF THE RESEARCH PERIOD
National Institute of Neurological Disorders & Stroke
National Leaders
NIH Grants
MRS and DTI as biomarkers of spinal cord viability in chronic spinal cord injury.
MRS to explore spinal cord viability in chronic spinal cord injury.
Enabling forelimb function with agonist drug and epidural stimulation in SCI.
Neurotrophins Support Spinal Cord Learning and Rehabilitation.
SPINE CENTER
The UCLA Spine Center is one of the leading centers conducting NIH studies on spinal cord injury and imaging for evaluation of spinal disorders. Using Diffusion Tensor Imaging (DTI), we are able to generate a 3D image of the spinal cord nerves called the “fiber tractography” (above middle/right). DTI can identify separate nerve fibers running rostral-caudal, antero-posterior, and left to right. It is more detailed than standard MRI (above left).
JANUARY Cody enrolls in spinal cord injury trial with Dr. Lu.
CODY’S TIMELINE
AUGUSTCody stands with assistance on a walker, walks in the pool with assistance and swims using his arms.
2010
APRILCody begins a clinical trial. Dr. Lu uses novel spinal cord stimulation to enable standing and stepping function.
2012
2009 DECEMBERPhysical therapy begins.
2011
SEPTEMBER 15TH He wakes from coma and can move both hands.
SEPTEMBER 12TH Following an all-night surgery Cody is placed in an induced coma in the ICU for healing.
FEBRUARY Cody takes 40 steps on a walker and 55 the following week.
MAY Cody uses a fork, writes with a pencil and walks with assistance on a treadmill.
JUNE Cody graduates from Santa Monica High School.
APRIL 12TH“I feel stronger than I ever have, I know I’m going to walk again, Mom,” says Cody, after stimulation therapy at Dr. Lu’s lab.
2013
SEPTEMBER 11TH Cody is paralyzed from the neck down. Dr. Holly performs an emergency nine-hour surgery.

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND66 | PEDIATRIC EPILEPSY SURGERY PROGRAM
Gary W. Mathern, MD, with patient Dylan Catania

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND PEDIATRIC EPILEPSY SURGERY PROGRAM | 67
This is about changing kids’ lives for the better.Even with half of your brain removed, you can do a lot.
Our patients go on to thrive, walk, talk, play, read, drive and graduate from high school and college.
—Gary W. Mathern, MD, Director of the Pediatric Epilepsy Surgery Program
“”
he UCLA Pediatric Epilepsy Surgery Program is a world leader in the diagno-sis, treatment and management of rare childhood diseases that cause intractable
epilepsy. Our interdisciplinary team has performed more than 750 surgeries on infants and children with intrac-table epilepsy. More than 225 of those patients received hemispherectomies since the center’s inception in 1986. We were the first to operate on infantile spasms and are one of the few centers in the world that offers surgery to children with intractable epilepsy. Our team consults with pediatricians around the world, and children come to UCLA from across the country. The majority of chil-dren who receive surgery go on to live seizure-free lives.
One reason children have such good outcomes is that we conduct highly detailed and accurate evalu-ations prior to surgery. Our team is sensitive to the emotional, developmental, psychological, educational, social, economic and familial challenges facing the families of children undergoing surgery. We collabo-rate seamlessly with the child’s physician before and after to ensure the best outcomes. Our team includes talented and compassionate specialists in pediatric neurosurgery, pediatric neurology, child psychiatry, pediatric neuroradiology, pediatric neuropsychology, developmental linguistics and neuropathology, clinical nurse specialist and social workers.
T

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND68 | PEDIATRIC EPILEPSY SURGERY PROGRAM
or more than a decade, Gary W. Mathern, MD, Director of the Pediatric Epilepsy Surgery Program at UCLA, has slowly
and methodically collected brain tissue and DNA from children with a very rare disease called hemimegalencephaly. This debilitating disease causes severe epilepsy. Currently, Dr. Mathern performs hemispherectomy proce-dures to remove the dysfunctional hemisphere of the brain and eliminate the occurrence of seizures, which damage the entire brain. Dr. Mathern knew the answer to what was going on with these children lay in their tissue and
DNA. He was the only one in the world who stored these vital tissue samples, waiting until technology caught up. Today, the answer can be found in a recent edition of Nature Genet-ics. Dr. Mathern’s study has uncovered a trio of genes, called de novo somatic mutations, which control cell size and proliferation and are the catalyst of hemimegalencephaly. The study suggests that drugs already in exis-tence to stop or lower the signals from these mutated genes could be designed to reduce or eliminate the need for radical surgery that entails removing half of the child’s brain. This could be the tip of the iceberg and lead to the
genetic mutations that may cause other child-hood diseases like autism.
Dr. Mathern is the Co-Editor in Chief of Epilepsia, a renowned medical journal sup-ported by the International League Against Epilepsy. He received the Ambassador for Epilepsy Award of the International Bureau for Epilepsy and the International League Against Epilepsy to recognize his outstanding international contributions to advancing the cause of epilepsy.
Recently, he awed a wide audience at TEDxConejo with his presentation What Can You Do With Half a Brain?
Gary W. Mathern, MD, is a Professor and Director of the Pediatric Epilepsy Surgery Program and Pediatric Neurosurgery Program in the Department of Neurosur-gery at UCLA. He is a pioneer in the sur-gical treatment of children with epilepsy. He is highly pursued for his expertise in treating pediatric epilepsy with the cere-bral hemispherectomy that entails remov-ing half of the dysfunctional brain causing seizures in infants and children.
He modified an intricate surgical tech-nique, a lateral hemispherecotomy, to perform this procedure on infants that was published in the Journal of Neurosurgery in 2004 and is now used worldwide. After the hemispherectomy, the brain miracu-lously rewires functions using only one side of the brain. For this reason, he advocates this procedure to be performed as early as
possible because the brain is more plastic in early development. The later the surgery, the longer the infant or child suffers mul-tiple seizures that can cause debilitating and irreparable brain damage.
He recommends that a child be evalu-ated for surgery if two anti-seizure medi-cations have failed to stop the seizures. Families have described their children pre-surgery as trapped inside their bodies and post-surgery as alive, thriving, walking and talking. This is a true marvel of neu-rosurgery and a gift of life Dr. Mathern has given to families stuck in an endless cycle of thirty to fifty seizures a day that rob their children of life and normal develop-ment. Without the surgery, these children would have been headed to an IQ of 50, not being able to recognize mom or dad by age one, not likely to talk or engage in social
activity. The radical neurosurgical interven-tion frees the child’s brain to develop.
Dr. Mathern has performed hundreds of these surgeries and his patients go on to miraculous recoveries, learning how to talk, read and go to school, obtain their driver’s licenses and graduate from high school and college.
F
PIONEER IN GIVING SEIZURE-FREE LIFE TO CHILDREN
BANKING ON THE FUTURE OF DNA TECHNOLOGYA Decade of Brain Tissue Sampling Helps Unlock Mystery of Rare Pediatric Epilepsy
DR. GARY W. MATHERN WITH DYLAN CATANIA IN 2010

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND PEDIATRIC EPILEPSY SURGERY PROGRAM | 69
hortly after his daughter Grace’s 10th birthday, Seth Wohlberg witnessed
the tragic attack of Rasmussen’s Encephalitis (RE) on her brain. In an instant, uncontrollable seizures ensued. This rare disease began to paralyze one side of her body. The only treatment was to remove half of her brain and rely on plasticity —the brain’s ability to rewire itself—to return many of her neu-rological functions. In 2010, Dr. Gary W. Mathern performed a hemispherectomy freeing Grace of the seizures.
Mr. Wohlberg started the RE Children’s Project, a non-profit organization, to support scientific
research toward a cure for RE. Mr. Wohlberg has become the leading voice, steward, and advocate for this rare disease in America and across the globe. The RE Children’s Project supports UCLA research in collecting the brain tissue of patients with RE and studying the brain and immunologic cells along with genetics to unlock the cause in order to develop novel treatments and ultimately a cure.
S
WHO WE ARE
80%225 1stOF HEMISPHERECTOMY
PATIENTS ARE NOW LIVING SEIZURE-FREE
HEMISPHERECTOMIES PERFORMED ON INFANTS
& CHILDREN
HOSPITAL TO OPERATE ON INFANTILE SPASMS
750SURGERIES ON INFANTS
AND CHILDREN WITH INTRACTABLE EPILEPSY
PEDIATRIC EPILEPSYPROGRAM
CONDITIONS TREATEDBrain traumaCavernomasCortical dysplasiahemimegalencephaly
Hippocampal sclerosisHypothalamic hamartomaHypothalamic hamartomas infarctions
InfectionsRasmussen encephalitisSturge-Weber syndromeTuberous sclerosis complex
tumorsOther rare conditions associated with intractable epilepsy
QUEST FOR A CUREOne of the first extensive pediatric epilepsy surgery centers in the world.
First to apply FDG-PET in clinical decision-making for pediatric epilepsy.
First to apply FDG-PET/ MRI co-registration for pediatric patients, and magnetoencephalography MEG in tuberous sclerosis complex.
First to invent and perform lateralhemispherectomy procedurefor young children.
First comprehensive tuberous sclerosis complex clinic in North America for children with epilepsy.
First to operate on infantile spasms.
Cortical plasticity after hemispherectomy.
Mechanisms altering electrical conductivity & DTI in epilepsy patients.
Pathophysiology of developing dysplastic human cortex.
Molecular characterization of hemimegalencephaly.
History of Firsts
$4,002,612TOTAL NIH/NON-NIH GRANTS, INCLUDING DIRECT & INDIRECT COSTS, FOR THE DURATION OF THE RESEARCH PERIOD
NIH Grants
Total NIH Funding
Raman Sankar, MD, PhDPEDIATRIC NEUROLOGY
Jason Lerner, MDPEDIATRIC EEG LABORATORY
Harry V. Vinters, MDNEUROPATHOLOGY
Joyce Wu, MD, Joyce Matsumoto, MD,Lakha Rao, MD, Shaun Hussain, MD,Noriko Salamon, MDPEDIATRIC NEURORADIOLOGY
Gary W. Mathern, MD PROGRAM DIRECTOR
Doctor HighlightRAMAN SANKAR, MD, PHD, IS PROFESSOR OF NEUROLOGY & PEDIATRICS AND CHIEF OF PEDIATRIC NEUROLOGY.
SETH WOHLBERG WITH DAUGHTER GRACE

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND70 | PEDIATRIC EPILEPSY SURGERY PROGRAM
DYLAN CATANIA
SMALLWONDER
PEDIATRIC EPILEPSY SURGERY PROGRAMPATIENT HIGHLIGHT
The Catanias rang in the 2010 New Year with the birth of their healthy baby boy, Dylan. He was born 6 pounds, 5 ounces and measured
19 inches. Ellen was swaddling her newborn to go home from the hospital when the first seizure struck. His eyes rolled and rhythmically twitched. His body shuddered. Ellen pressed the nurse button and then ran into the hall, yelling for help as her baby looked vacant.
Dylan was rushed into neonatal intensive care. Tests revealed that Dylan had hemi-megalencephaly, a rare congenital disease that causes one side of the brain to grow larger than the other. Dylan’s parents and their 9-year-old daughter, Bella, waited for answers that finally came that afternoon, when Dr. Gary W. Mathern, an expert in hemi-megalencephaly and the Director of the Pe-diatric Epilepsy Program at UCLA, entered their lives. The only treatment to stop the sei-zures was to surgically remove the enlarged half of his brain.
“‘I’m going to take care of this, don’t you worry,’ Dr. Mathern said to us on our first meeting, and we hung on to his words through every seizure that followed,” Ellen said.
The hemispherectomy would give the left side of his brain a chance at neuroplasticity, the brain’s natural ability to rewire itself, to enable development. Without the treatment, the sei-zures on the right side would eventually move to the left and hijack his brain in such a way that by his second birthday he would be mentally re-tarded, unable to talk or recognize his parents, and never reach an IQ of more than 50. With the surgery, he had a chance to develop, walk and talk. The physical set back would affect the left side of his body, Dylan would be weak, his left hand would be paralyzed and he would have a blind spot in his left eye. He would need to be at least three months to undergo this radical procedure. Until then, he suffered fifty to sixty seizures a day.
More than one thousand seizures later, Dylan entered operating room number 7 at Mattel
Children’s Hospital at UCLA. Within minutes, the anesthesiologist relaxed him to sleep. Dr. Mathern slipped on his magnified glasses. He raised his scalpel and said to the nurse, “Call Mom and Dad. Tell them we’re beginning.” The clock read 9:15 a.m. The surgery meant navigating through the tiny folds of the brain to arrive at the corpus callosum at the base that connected the two hemispheres. He delicately disconnected the right hemisphere of the brain, being careful not to leave any tissue connected that would lead to seizures.
By 3:55 p.m., he and his team stitched up Dylan. At 4:20 p.m., Dr. Mathern went down to see Ellen and Jeff to report a successful surgery. Today, Dylan is three years old. He has remained seizure-free since the surgery, in April 2010. Each developmental milestone is a victory for the family and they have cele-brated many. Dylan knows his parents and big sister, Bella. The toddler talks, walks, laughs, dances, claps and brings his family utter joy each and every day.

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND PEDIATRIC EPILEPSY SURGERY PROGRAM | 71
ACCESSING DYLAN’S BRAIN
Cuts in skullHoles
A t-shaped cut in the scalp was peeled back into two flaps.
1.
2.
Holes were drilled in the exposed skull and cuts joined the holes.
The flap of Dylan’s skull was opened, using his temporalis jaw muscle as a hinge. The bone section continued to receive blood supply.
The disconnected part of Dylan’s brain is still alive and seizing but is harmless. His skull was closed using titanium screws and his scalp stapled shut.
Illustrations by Paul Duginski Los Angeles Times
3.
4.
Cuts in scalp
Exposed brain
Bone �ap
Staples in ScalpGary W. Mathern, MD
Gary W. Mathern, MD,PEDIATRIC NEUROSURGERY
Raman Sankar, MD, PhDPEDIATRIC NEUROLOGY
Harry Vinters, MDNEUROPATHOLOGY
Noriko Salamon, MDPEDIATRIC NEURORADIOLOGY
Conrad Szeliga, Andrea Duran, Jimmy NguyenEEF SPECIALISTS
Barbara Van De Wiele, MDANESTHESIA
Judith Brill, MDPEDIATRIC ICU
DYLAN’S TEAM
Professor in Residence and Director of the Pediatric Epilepsy Surgery Program and Pediatric Neurosurgery Program. Dr. Mathern works in conjunction with the Epilepsy Surgery Program to provide surgical treatment for children with epilepsy.
Corpus callosum
Internal capsule
Thalamus
BrainstemBrainstem
Frontal lobe
Temporal lobe
Sylvian �ssure
Cross-section (shown at right) Cross-section
Inter-hemispheric �ssure
Inter-hemispheric �ssure Left
hemisphereRight hemisphere
Left hemisphere
Right hemisphere
Lateral ventricles
BrainstemBrainstem
Frontal lobe
Temporal lobe
Sylvian �ssure
Cross-section (shown at right) Cross-section
Inter-hemispheric �ssure
Inter-hemispheric �ssure Left
hemisphereRight hemisphere
Left hemisphere
Right hemisphere
Lateral ventricles
Lateral ventricles
Temporal horn
ThalamusThalamus
Cortex
Brainstem
Corpus callosum
Lateral ventricles
Temporal horn
ThalamusThalamus
Cortex
Brainstem
Corpus callosum
The brain is divided into two hemispheres by a fissure and is connected to the rest of the body
through the brainstem.
BRAIN FUNCTION & THE PROBLEM
The affected hemisphere of Dylan’s brain was disconnected from the other hemisphere and brainstem. Most of the disconnected hemisphere was allowed to remain in place, where it will continue to receive blood and help with normal growth and skull formation.
DYLAN’S SURGERY
The major connection through which the two
hemispheres communicate is the corpus callosum.
A section of the cortex was removed, creating a “doughnut
hole” through which internal brain structures could be accessed.
Once the skull was penetrated and the brain exposed, an incision was made that followed the shape of
the ventricle.
The hemispheres of the brain contain fluid-filled, irregular-
shaped cavities called ventricles.
The hemispheres also communicate with the brainstem
and spinal cord through the thalamus and internal capsule.
—Jeff Catania (Dylan’s Father)
There are no words to describe him. Dr. Mathern is outstanding. He saved our son’s life. He saved our lives.
Dylan is now the baby boy we had been waiting for.“
”

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND
Advancing our spirit of collaboration across disciplines to provide our patients with the most cutting-edge treatments and care is expanding beyond our walls to network with experts across the nation and around the world in the Global Neurosurgery Institute at UCLA. Accumulated global knowledge on confronting neurological diseases and disorders of the brain and spine such as stroke, cancer, Parkinson’s, Alzheimer’s and autism, will be in our hands. The latest in treatments and fundamental understanding of these diseases from the physical, to the mental, to the genetic level will provide us with boundless opportunities to solve neuro-logical problems and fully restore the brain so our patients will no longer by paralyzed by disease, but instead move beyond to live healthy, produc-tive and worthwhile lives.
We are building a patient care center where world-class experts who are dedicated to solving the mysteries of your disease collaborate to optimize the most advanced treatment plan available, all accessible in one place. Video conferencing will provide truly global patient-doctor interactions. With the goal to improve survival and quality of life, we will devise a per-sonalized plan of care for our patients. Experts in neurosurgery, neurology, psychology, brain mapping, cardiology, diet, nutrition and physical therapy from UCLA, and around the world, will interact in a dynamic atmosphere to weigh the risks and benefits of treatments, to enhance optimal out-comes for our patients. This coordinated team will reform health care from the inside to set a new gold standard focused on collaboration, the secret weapon to beating these diseases of the brain and spine.
72 | GLOBAL NEUROSURGERY INSTITUTE
COLLABORATION. DISCOVERY. EXCELLENCE. The Edie & Lew Wasserman Building
GLOBAL NEUROSURGERY INSTITUTE
INVENTING THE FUTURE OF HEALTH CARE Global Neurosurgery Institute
EXPERT KNOWLEDGE, GLOBAL EXCHANGEClinical Pavilion, One Place, Team Care
e are on the verge of opening the first-of-its-kind Global Neurosurgery Institute in the Edie and Lew Wasserman Building at UCLA in 2014. The top two floors of this state-of-the art facility will become the headquarters for the
UCLA Department of Neurosurgery, uniting our world-class expert neu-rosurgeons and neuroscientists in one place, to ignite a truly unique at-mosphere of collaboration that will transform the way we practice medi-cine and perform our translational bench-to-bedside research at UCLA.
As one of the world’s top 10 neurosurgery departments, we are leading the world in research, patient care and training of the next generation of neurosurgical pioneers. The Global Neurosurgery Institute will house the most advanced patient clinic, faculty center, training pavilion and comprehensive neurosurgery campus, poised to invent the future of neurosurgery. This institute, and all that it stands to accomplish for the global future of neurosurgery, was realized and made possible by the vision and support of private donors.
W

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND GLOBAL NEUROSURGERY INSTITUTE | 73
Our mission at UCLA is laser-focused on innovation, from the latest technologies to cutting edge patient treatments. Our vision is to help hundreds, thousands and even millions of patients through innovation. With the same dedication, we train our neurosurgical residents with the latest tech-niques and treatments, as they take our methods of life-saving care beyond our walls. The Neurosurgery Training Pavilion will have the latest technology for mock surgery practice using image-guidance systems to perfect neuro-surgical skills in the most lifelike simulated experiences. Using our high-definition video and telemedicine, our neurosurgical residents can virtually beam into operating rooms in leading medical facilities across the country, while residents around the world can observe our world-class neurosurgeons perform surgeries.
On the top floor of our headquarters will be the Neurosur-gery Scholars Pavilion, home to our international network connecting our doctors and scientists to medical centers and research facilities across the United States, Latin America, Israel, Asia, Europe, Africa and the Middle East. By fostering global possibilities for advancing research, neurosurgical techniques, collaborations and clinical trials, this pavilion will ultimately lead to medical breakthroughs and cures for neurological disease and disorders.
TRAINING THE NEUROSURGICAL PIONEERS OF TOMORROWNeurosurgery Training Pavilion:Advancing Lifesaving Care
OUR VISION FOR THE FUTURE OF NEUROSURGICAL CARE Neurosurgery Scholars Pavilion:Global Possibilities
We envision the Global Neurosurgery Institute to be a global brain, or mission control center, for neurosurgery and neuroscience that will centralize medical knowledge using supercomputers, telemedicine and global confer-encing, transforming the way we practice medicine. We are moving from responsive toward predictive medicine for our patients at UCLA and beyond. Our development of the 70-seat Global Conference Pavilion will be wired with the most advanced technology, internationally connected for collaborative opportunities across international time zones and geographical borders. We will be setting the international stage for physicians and scientists to work together to provide next-generation medicine and direct access to experts for the betterment of patient care. The possibilities are endless.
Our patients will be the legacy of combined global ex-perience and lifetimes dedicated to unearthing the solu-tions and treatments for tomorrow. Our power to conquer neurological disorders and disease is within reach as we connect our global knowledge, expertise and resources. United, we care for our patients, across America, and every continent and population around the world.
A GLOBAL CENTER OFRESOURCES & EXPERTISE Global Conference Pavilion: Convergenceof Technology & Unparalleled Reach
THE NEUROSURGERY TRAINING PAVILION WILL BE EQUIPPED WITH THE LATEST TECHNOLOGY FOR MOCK SURGERY TO PERFECT THE SKILLS OF TOMORROW’S NEUROSURGEONS
THE 70-SEAT GLOBAL CONFERENCE PAVILION WILL ACT AS A HUB FOR CONNECTING PHYSICIANS AND SCIENTISTS FROM AROUND THE GLOBE

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND
Top 10 Neurosurgery Department in the nation according to U.S. News and World Report for more than 20 years.
No. 1 Best Hospital in Southern Cali-fornia, Los Angeles, and Top 5 Hos-pitals in America according to U.S. News and World Report for more than 20 years.
No. 2 in National Institutes of Health (NIH) Research Grants at $5,943,956 for 2012.
No. 5 in the world for most published research papers in medical journals.
Authors of evidence-based guidelines for brain and spinal disorders.
Advisors to the NFL, MLB, U.S. Mili-tary and White House Appointee on the Defense Health Board, for traumatic brain injury and concussion treatment.
UCLA Brain Injury Research Center leads the nation and the world.
Voted “Best Doctors in America” by medical professionals across the nation.
Voted “Top Surgeons” by Consumers’ Research Council of America.
Voted “Super Doctors” by physicians and peers across the nation.
Pioneers in minimally-invasive endo-vascular therapies for stroke.
World’s leading stroke center—NIH-SPOTRIAS network designation and certified by the Joint Commission as a Comprehensive Stroke Center.
UCLA Brain Tumor Program leading the world in next-generation medicine.
Developed the first personalized brain cancer vaccine, DCVax.
Global B.R.A.I.N. Prize top 10 finalist for discovering memory boosting.
Pioneers in minimally-invasive, endo-scopic and non-invasive brain surgery.
First Neuro-ICU in the world to use ro-botics and telemedicine.
GLOBAL LEADERSur mission to heal humankind one patient at a time is the tie that binds our cross-collaborations with a variety of other specialties at UCLA Health. Together we deliver unrivaled, centralized, world-class care and the latest translations of basic research into
medical breakthroughs at the bedside for our patients. We continue to attract and train the next generation of neuroscientists and neurosurgical pioneers mapping new frontiers of the human brain and discovering cures for the most complex neurological diseases facing our families today, and our children’s families tomorrow.
CONTACT THE UCLA DEPARTMENT OF NEUROSURGERYJames I. Ausman, MD, PhDTel: 310-825-5482Fax: 310-206-6242
Ulrich Batzdorf, MDUCLA Spine CenterTel: 310-825-5079Fax: 310-825-7245
Donald P. Becker, MDProfessor EmeritusTel: 310-794-1222Fax: 310-825-7245
Marvin Bergsneider, MDPituitary Tumor ProgramTel: 310-206-4100Fax: 310-825-9385
Fredric L. Edelman, MDTel: 818-781-3350Fax: 818-781-7237
Itzhak Fried, MD, PhDAdult Epilepsy SurgeryTel: 310-825-8409Fax: 310-794-2147
Nestor Gonzalez, MDUCLA Stroke CenterTel: 310-825-5154Fax: 310-206-6242
Langston T. Holly, MD UCLA Spine CenterTel: 310-267-5580 Fax: 310-206-1857
Linda M. Liau, MD, PhD Brain Tumor ProgramTel: 310-267-2621 Fax: 310-825-9385
Daniel Lu, MD, PhDUCLA Spine CenterTel: 310-267-2975Fax: 310-825-7245
Neil A. Martin, MD, FAANS UCLA Stroke CenterTel: 310-825-5482 Fax: 310-206-6242
Gary W. Mathern, MD Pediatric Epilepsy SurgeryTel: 310-825-7961Fax: 310-825-0922
Duncan Q. McBride, MD Harbor-UCLA Medical CenterTel: 310-319-3475Fax: 310-319-4575
Nader Pouratian, MD, PhDNeuromodulation &Neurobionics ProgramTel: 310-206-2189Fax: 310-794-1848
Bob Shafa, MD Brain Tumor ProgramTel: 310-825-1988Fax: 310-825-9385
Paul M. Vespa, MD, FAANSNeurocritical Care Tel: 310-267-9448Fax: 310-267-3841
Isaac Yang, MDSkull Base Tumor ProgramTel: 310-267-2621Fax: 310-825-9385
UCLA NEUROSURGERY:OUR DEPARTMENT IN SUMMARY
O

UCLA NEUROSURGERY: INTO THE BRAIN AND BEYOND
Nancy McLaughlin, MD, PhDTel: 310-825-5482Fax: 310-206-6242
Jean-Philippe Langevin, MDTel: 310-825-5482Fax: 310-206-6242
UCLA DEPARTMENT OF NEUROSURGERY757 Westwood Plaza, Suite 6236Los Angeles, CA 90095-7436www.neurosurgery.ucla.edu
Copyright 2013 UCLA Health, Department of Neurosurgery
Developed by Cunningham & Associates in conjunction with Studio III Marketing
REFERRING PHYSICIANS310-825-5111www.uclahealth.org/refer

nonprofitorganizationu.s. postage
PAIDu c l a
405 Hilgard AvenueBox 956923, Wilshire Center, Suite 1850Los Angeles, CA 90095-6923
















![Beyond the Blood-Brain Barrier - UCLA CTSI · Beyond the Blood-Brain Barrier: ... Circumventing the blood-brain barrier ... K30 presentation final clean.ppt [Read-Only] Author:](https://static.fdocuments.us/doc/165x107/5b0543887f8b9a0a548e9fa1/beyond-the-blood-brain-barrier-ucla-ctsi-the-blood-brain-barrier-circumventing.jpg)

