INTERSTITIAL AND FIBROTIC LUNG DISEASESBecause airway disease and other lung diseases also may...
38
© 2014 Decker Intellectual Properties Inc pulm-crit Interstitial and Fibrotic Lung Diseases — 1 DOI 10.2310/7900.1054 10/08 INTERSTITIAL AND FIBROTIC LUNG DISEASES Lake D. Morrison, MD, and Paul W. Noble, MD function testing, and imaging studies are all required in the workup of a patient with DPLD. In many cases, careful interpretation of these data may obviate the need for a tissue diagnosis, as discussed below. history and physical examination The two most prominent complaints in patients with DPLD are typically cough and dyspnea on exertion. Often these symptoms develop quite insidiously, with a patient, or those close to the patient, noting on careful reflection that his or her cough or dyspnea has been present for many months to even years. Likewise, patients will admit that they had ignored their dyspnea, often believing that they were either “just getting older” or “getting out of shape.” Some DPLDs, such as acute interstitial pneumonia (AIP), acute hypersensitivity pneumonitis, eosinophilic pneu- monia, or cryptogenic organizing pneumonia (COP), may develop over weeks, and the clinician needs to recognize this feature. Chest pain, especially substernal chest pain reminiscent of angina, is unusual for most of the IIPs. Pleuritic chest pain may arise in collagen vascular diseases, such as rheumatoid arthritis when an inflammatory pleural effusion is present, or may reflect a pneumothorax, sometimes seen in cystic lung diseases such as lymphangioleiomyomatosis (LAM) or Langerhans cell histiocytosis (LCH). Wheezing in DPLD suggests airways disease. When no history of asthma or chronic obstructive pulmonary disease (COPD) is present, the clinician should consider certain diseases that might affect the smaller airways, such as hypersensitivity pneumo- nitis or respiratory bronchiolitis. Lymphangitic spread of tumor can lead to obstruction of airways, as can endobron- chial sarcoidosis. Hemoptysis is uncommon in many of the DPLDs and should prompt the clinician to consider vasculitis such as Wegener or Goodpasture syndrome, or another alveolar hemorrhage syndrome. These conditions are discussed elsewhere [search for these topics in this The patient’s past medical history, as well as a detailed review of symptoms in all major organ systems, requires special attention. DPLD seen in conjunction with conditions such as connective tissue diseases is most likely to be a man- ifestation of that disease. Asking about rashes, swallowing difficulties, muscle weakness, and joint aches can often point the careful interviewer to a more focused workup. In some cases, symptoms may be very minor when compared to the patient’s pulmonary complaints. It is also well known that pulmonary manifestations of a connective tissue disease may precede other symptoms. 2–4 A careful appraisal of the interval medical history is therefore required each and every time a patient is interviewed during his or her workup. Reviewing the social history of a patient with DPLD takes on special importance since a number of conditions are associated with exposures at home or at work. Tobacco usually plays an essential role in conditions such as LCH, Interstitial lung disease refers to any of a number of conditions in which infiltration of the alveolar walls with an inflam- matory and/or fibrotic process occurs, often leading to restriction of lung function and impairment of gas exchange. In normal lungs, the alveolar septa are thin structures. Macrophages, fibroblasts, and other cells are present in small numbers. Collagen and related extracellular proteins are not prominent. In interstitial lung diseases, proliferation of the fibroblasts and excessive collage deposition occur, pre- sumably in response to some type of injury. Depending on a number of factors yet to be fully understood, including the cause and timing of injury, as well as factors unique to certain individuals, the inflammatory component of this response may be prominent or minor, and anti- inflammatory medications may or may not be effective. Because airway disease and other lung diseases also may affect the interstitium of the lung, and interstitial lung dis- eases can affect the airways, the term diffuse parenchymal lung disease (DPLD) is often preferred. In this chapter, we adopt that general term. In approaching a patient with DPLD, the clinician seeks to establish a potential cause. As described elsewhere in this text, interstitial and fibrotic lung diseases can be seen in association with a number of conditions and exposures. When no convincing association can be made, the term idio- pathic interstitial pneumonia (IIP) should be used. As described below, IIPs may share many features with the DPLDs seen in conjunction with known clinical entities. In spite of this, the clinical course can vary significantly, and it is incumbent upon the practicing clinician to make an exhaustive search for the causes or known associations of a DPLD as the prognosis and potential therapies can vary widely. This chapter outlines an approach to the patient with DPLD and describes the salient features of the individual IIPs. DPLDs associated with other conditions or exposures, including sarcoidosis, are described elsewhere [search for these topics in this book]. The categorization suggested by the American Thoracic Society/European Respiratory Society (ATS/ERS) International Multidisciplinary Consen- sus Committee listed in Figure 1 provides a structured way of approaching patients with DPLD. 1 Approach to the Patient with DPLD The main objective in performing a detailed evaluation of the patient with DPLD is to guide treatment. Given the nature and prevalence of these diseases, this most often dis- tills to determining whether the patient has (a) idiopathic pulmonary fibrosis (IPF), a disease with limited treatment options, or (b) an interstitial pneumonia that might respond to therapy. Drawing this conclusion requires a comprehen- sive analysis of all data available as no one feature trumps all others. A detailed history, comprehensive physical examination, appropriate laboratory studies, pulmonary Scientific American Medicine ]. book
Transcript of INTERSTITIAL AND FIBROTIC LUNG DISEASESBecause airway disease and other lung diseases also may...

© 2014 Decker Intellectual Properties Inc pulm-crit Interstitial and Fibrotic Lung Diseases — 1DOI 10.2310/7900.1054
10/08
I N T E R S T I T I A L A N D F I B R O T I C L U N G D I S E A S E S
Lake D. Morrison, MD, and Paul W. Noble, MD
function testing, and imaging studies are all required in the workup of a patient with DPLD. In many cases, careful interpretation of these data may obviate the need for a tissue diagnosis, as discussed below.
history and physical examination
The two most prominent complaints in patients with DPLD are typically cough and dyspnea on exertion. Often these symptoms develop quite insidiously, with a patient, or those close to the patient, noting on careful refl ection that his or her cough or dyspnea has been present for many months to even years. Likewise, patients will admit that they had ignored their dyspnea, often believing that they were either “just getting older” or “getting out of shape.” Some DPLDs, such as acute interstitial pneumonia (AIP), acute hypersensitivity pneumonitis, eosinophilic pneu-monia, or cryptogenic organizing pneumonia (COP), may develop over weeks, and the clinician needs to recognize this feature.
Chest pain, especially substernal chest pain reminiscent of angina, is unusual for most of the IIPs. Pleuritic chest pain may arise in collagen vascular diseases, such as rheumatoid arthritis when an infl ammatory pleural effusion is present, or may refl ect a pneumothorax, sometimes seen in cystic lung diseases such as lymphangioleiomyomatosis (LAM) or Langerhans cell histiocytosis (LCH). Wheezing in DPLD suggests airways disease. When no history of asthma or chronic obstructive pulmonary disease (COPD) is present, the clinician should consider certain diseases that might affect the smaller airways, such as hypersensitivity pneumo-nitis or respiratory bronchiolitis. Lymphangitic spread of tumor can lead to obstruction of airways, as can endobron-chial sarcoidosis. Hemoptysis is uncommon in many of the DPLDs and should prompt the clinician to consider vasculitis such as Wegener or Goodpasture syndrome, or another alveolar hemorrhage syndrome. These conditions are discussed elsewhere [search for these topics in this
The patient’s past medical history, as well as a detailed review of symptoms in all major organ systems, requires special attention. DPLD seen in conjunction with conditions such as connective tissue diseases is most likely to be a man-ifestation of that disease. Asking about rashes, swallowing diffi culties, muscle weakness, and joint aches can often point the careful interviewer to a more focused workup. In some cases, symptoms may be very minor when compared to the patient’s pulmonary complaints. It is also well known that pulmonary manifestations of a connective tissue disease may precede other symptoms.2–4 A careful appraisal of the interval medical history is therefore required each and every time a patient is interviewed during his or her workup.
Reviewing the social history of a patient with DPLD takes on special importance since a number of conditions are associated with exposures at home or at work. Tobacco usually plays an essential role in conditions such as LCH,
Interstitial lung disease refers to any of a number of conditions in which infi ltration of the alveolar walls with an infl am-matory and/or fi brotic process occurs, often leading to restriction of lung function and impairment of gas exchange. In normal lungs, the alveolar septa are thin structures. Macrophages, fi broblasts, and other cells are present in small numbers. Collagen and related extracellular proteins are not prominent. In interstitial lung diseases, proliferation of the fi broblasts and excessive collage deposition occur, pre-sumably in response to some type of injury. Depending on a number of factors yet to be fully understood, including the cause and timing of injury, as well as factors unique to certain individuals, the infl ammatory component of this response may be prominent or minor, and anti-infl ammatory medications may or may not be effective. Because airway disease and other lung diseases also may affect the interstitium of the lung, and interstitial lung dis-eases can affect the airways, the term diffuse parenchymal lung disease (DPLD) is often preferred. In this chapter, we adopt that general term.
In approaching a patient with DPLD, the clinician seeks to establish a potential cause. As described elsewhere in this text, interstitial and fi brotic lung diseases can be seen in association with a number of conditions and exposures. When no convincing association can be made, the term idio-pathic interstitial pneumonia (IIP) should be used. As described below, IIPs may share many features with the DPLDs seen in conjunction with known clinical entities. In spite of this, the clinical course can vary signifi cantly, and it is incumbent upon the practicing clinician to make an exhaustive search for the causes or known associations of a DPLD as the prognosis and potential therapies can vary widely.
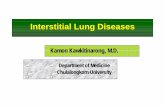
This chapter outlines an approach to the patient with DPLD and describes the salient features of the individual IIPs. DPLDs associated with other conditions or exposures, including sarcoidosis, are described elsewhere [search for these topics in this book]. The categorization suggested by the American Thoracic Society/European Respiratory Society (ATS/ERS) International Multidisciplinary Consen-sus Committee listed in Figure 1 provides a structured way of approaching patients with DPLD.1
Approach to the Patient with DPLD
The main objective in performing a detailed evaluation of the patient with DPLD is to guide treatment. Given the nature and prevalence of these diseases, this most often dis-tills to determining whether the patient has (a) idiopathic pulmonary fi brosis (IPF), a disease with limited treatment options, or (b) an interstitial pneumonia that might respond to therapy. Drawing this conclusion requires a comprehen-sive analysis of all data available as no one feature trumps all others. A detailed history, comprehensive physical examination, appropriate laboratory studies, pulmonary
Scientific American Medicine
].book

pulm-crit Interstitial and Fibrotic Lung Diseases — 2
10/08
desquamative interstitial pneumonia (DIP), and respiratory bronchiolitis–interstitial lung disease (RB-ILD) and an important role in IPF and asbestosis and might be protective in other disorders, such as hypersensitivity pneumonitis. Drugs such as amiodarone, methotrexate, gold, bleomycin, and cyclophosphamide can lead to an interstitial pneumoni-tis, and the clinician needs to review not only the patient’s current medications but also those taken in the past. Occu-pational exposure to ores and metals, dusts, fumes, gases, and chemicals can all lead to different forms of DPLD, many of which may not manifest in terms of either symptoms or physical fi ndings for years. Likewise, questions about pets such as birds or mold underneath the bathroom sink can lead to a diagnosis of chronic hypersensitivity pneumonitis in patients who might otherwise appear to have IPF. A number of medications have been associated with DPLD, as discussed elsewhere [search for these topics in this book]]Online resources can be useful in identifying possiblecausative agents (see http://www.pneumotox.com, for example).
Just as the review of systems might point to a new diagnosis of a connective tissue disorder, the physical examination must be equally thorough. A rash in a shawl pattern or a “mechanic’s hand” rash in an offi ce worker might lead to questions about muscle weakness and, ulti-mately, a diagnosis of dermatomyositis-related interstitial
lung disease. Lymph node enlargement or erythema nodo-sum might point toward sarcoidosis. Bibasilar inspiratory crackles are an important feature of many of the IIPs, espe-cially IPF. Their absence in IPF, on the other hand, should prompt considering a diagnosis other than IPF. Similarly, digital clubbing is a common feature in IPF or other advanced fi brotic diseases. On the other hand, digital clubbing in a patient with patchy alveolar infi ltrates could suggest bronchoalveolar cell carcinoma. Physical fi ndings consistent with pulmonary hypertension (PH) might lead to different treatment options, but signs of cor pulmonale might suggest end-stage disease with imminent mortality.
pulmonary function testing
Pulmonary function testing in DPLDs typically refl ects a restrictive defect, in which the forced vital capacity (FVC) and volume expired in the fi rst second (FEV1) are both reduced. Total lung capacity (TLC) and residual volume (RV) are also typically reduced. In some cases, the FEV1-to-FVC ratio is elevated. A gas exchange impairment is often present, as indicated by a reduction in the diffusing capacity of the lung for carbon monoxide (DLCO), even after adjustment for anemia (if present).
In cases of early DPLD, lung volumes may be normal.5 An isolated reduction in DLCO may be an early sign of DPLD
Figure 1 Classifi cation scheme of diffuse parenchymal lung disease from the 2001 American Thoracic Society consensus statement on idiopathic interstitial pneumonias. DPLD = diffuse parenchymal lung disease; IIP = idiopathic interstitial pneumonia; LAM = lymphangioleio-myomatosis; LCH = Langerhans cell histiocytosis.
Diffuse Parenchymal Lung Disease
Idiopathicpulmonary
fibrosis
IIP other thanidiopathic
pulmonary fibrosis
Desquamative interstitialpneumonia
Respiratory bronchiolitisinterstitial lung disease
Cryptogenicorganizing pneumonia
Acute interstitialpneumonia
Lymphocyticinterstitial pneumonia
Nonspecific interstitialpneumonia (provisional)
Idiopathicinterstitial
pneumonias
GranulomatousDPLD
(e.g., sarcoidosis)
Other forms ofDPLD
(e.g., LAM, LCH)
DPLD of known cause (e.g., drugs or association,collagen vascular disease)
].

pulm-crit Interstitial and Fibrotic Lung Diseases — 3
10/08
but might also suggest other entities, such as PH. In patients with concomitant chronic obstructive lung disease, such as in smokers who also develop DPLD, the FVC, FEV1, and TLC may all be normal.6,7 Evidence of frank airways obstruction (low FEV1-to-FVC ratio, high TLC, high RV) might suggest other forms of DPLD, including LCH, chronic hypersensitivity pneumonitis, or sarcoidosis.8
laboratory studies
In cases supported by clinical history, but also when a diagnosis is not certain, testing a battery of antibodies associated with connective tissue disease can be especially helpful. As discussed below, brain natriuretic peptide may be helpful when PH is suspected. At our institution, we typically check any patient presenting with DPLD of uncertain origin for the symptoms outlined in Table 1.
If a diagnosis of a mysotitis syndrome is clinically sus-pected and the anti-Jo1 is negative, we also evaluate other antisynthetase antibodies, including anti-Mi2, anti-PL-12, anti-PL-7, anti-EJ, anti-OJ, anti-Ku, and anti-U2snRNP.
imaging
Chest imaging is a key aspect to diagnosing DPLDs. Several different types of abnormalities can be seen, as described below. In a small subset of patients with IPF, plain chest fi lms—and sometimes even computed tomography (CT)—can be normal.9,10 More often than not, however, abnormalities on the CT will be present, even when the roentgenogram is normal.11
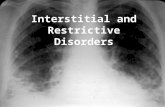
The advent of high-resolution computed tomography (HRCT) of the thorax has revolutionized the diagnostic approach to the IIPs. HRCT allows for detailed evaluation of the lung parenchyma in slices 1 to 2 mm thick [see Figure 2].12 Not only does it provide considerably clearer
images of lung anatomy than plain chest roentgenograms, it also has obviated the need for surgical lung biopsy in a number of conditions, including IPF in its classic form.6 It also has helped narrow the differential diagnosis signifi -cantly in other conditions. For example, pulmonologists will change their diagnosis more than half the time when HRCT is added to all other clinical information (other than biopsy).13 HRCT is especially helpful in diagnosing IPF, lymphangitic carcinoma, sarcoidosis, silicosis,
Figure 2 Example of differing appearance of “regular” computed tomography (CT) imaging and “high-resolution” CT. The high-resolution technique provides clearer images of the lung parenchyma.
a
b
Table 1 Studies and Symptoms Associated with Patients Presenting with DPLDStudy Association
Erythrocyte sedimentation rate (ESR)
General infl ammation
C-reactive protein (CRP) General infl ammation
Antinuclear antibody (ANA)
Several connective tissue diseases
Often mildly elevated in IPF
Rheumatoid factor (RF) Rheumatoid arthritis
Antineutrophilic cytoplasmic antibody (ANCA)
Systemic vasculitis
Anti-Jo 1 Dermatomyositis/polymyositis
Anti-SCL70 Systemic sclerosis
Anti-Ro (SSA), Anti-La (SSB)
Sjögren syndrome
Creatinine kinase, aldolase Myositis of any cause
Anti-RNP Mixed-connective tissue disease
DPLD = diffuse parenchymal lung disease.

pulm-crit Interstitial and Fibrotic Lung Diseases — 4
10/08
hypersensitivity pneumonitis, and pulmonary alveolar proteinosis.6,8 For the most part, HRCT is indicated in every patient presenting with DPLD.1
Several patterns have been identifi ed in DPLDs, and recognition of these can help the clinician narrow the dif-ferential diagnosis. A peripheral reticular interstitial pattern is a common fi nding in many forms of DPLD, including IPF and nonspecifi c interstitial pneumonia (NSIP), as well as many connective tissue diseases and asbestosis. On plain roentgenograms viewed in a posterior-anterior plane, an “L reverse L” pattern is typically seen, in which most disease is seen just medial to the lateral edges of the ribs, extending along the diaphragms medially [see Figure 3].14 On CT images, these abnormalities are more easily identifi ed as reticular lines, traction bronchiectasis, and honeycombing. Traction bronchiectasis refers to dilated airways in areas of otherwise fi brotic lung [see Figure 4]. Honeycombing refers to destruction of the lung parenchyma resulting in cysts between thickened intralobular septae [see Figure 5].14 Honeycombing is a key feature to diagnosing IPF and should be considered present only in unequivocal cases evaluated by expert radiologists or pulmonologists. In general, radio-graphic abnormalities are most prominent in the periphery of the bases on the lungs, becoming less so near the apices.1 When predominantly upper lobe disease is seen, other diag-noses, such as hypersensitivity pneumonitis, sarcoidosis, silicosis, and drug-related diseases, should be considered [search for these topics in this book].
Volume loss is another typical feature of fi brotic lung diseases. When lung volumes are increased on radiographs, the clinician should consider other entities, such as lymphan-gioleiomyomatosis, LCH, sarcoidosis, or concomitant emphysema and pulmonary fi brosis, for example.
Ground-glass opacities are areas of increased lucencies that do not obscure the underlying vasculature [see Figure 6]. Ground-glass opacity is a nonspecifi c fi nding that can repre-sent alveolar or interstitial abnormalities, refl ecting any number of processes, such as infection, edema, infl am mation, or early fi brosis. As discussed in the sections on specifi c DPLDs below, ground-glass opacities are a common fi nding in many conditions but typically less so in IPF.
Consolidation is a common fi nding in two of the IIPs, namely AIP and COP. Nodules, especially along broncho-vascular structures, are not typical for IPF and would point toward other diagnoses, such as sarcoidosis, chronic hyper-sensitivity pneumonitis, LCH, DIP, or RB-ILD. Pleural disease is uncommon in all of the IIPs and would point toward other processes, such as lung disease associated with connective tissue diseases. Mediastinal lymphadenopathy (>1 cm in diameter) is often seen to some extent in IPF and other IIPs.15,16
One important caveat is that breadth of experience in interpreting HRCT may be very important. A number of nonspecifi c fi ndings are often present on images of patients with DPLD, and a confi dent diagnosis cannot be made on radiographic data alone in 25 to 50% of patients with histologically confi rmed usual interstitial pneumonia (UIP).17 Radiologists from academic centers, presumably with more experience in DPLDs, are more likely to agree on a radio-graphic diagnosis than are community radiologists.18 Accordingly, a radiographic “fi nal” diagnosis should be made with caution.
A summary of radiologic features in DPLDs is shown in Table 2. Integrating clinical history, physical examination, pulmonary function testing, laboratory studies, and radio-graphy often provides substantial clues to diagnosing specifi c diseases appearing as DPLD. In general, however, pathology usually provides the most information.
bronchoscopy with bronchoalveolar lavage
The role of bronchoscopy with bronchoalveolar lavage (BAL) in DPLDs has been debated. Bronchoscopy is gener-ally a safe procedure to perform and can be diagnostic in some cases of DPLD, such as eosinophilic pneumonias, infection, malignancy, and alveolar proteinosis, among other etiologies.8 In IIPs, differential cell counts can provide some information on underlying disease and prognosis but are rarely defi nitive. An absence or paucity of lymphocytes favors a diagnosis of UIP over chronic hypersensitivity pneumonitis or sarcoidosis.19 Unfortunately, BAL analysis does not appear to be useful in distinguishing UIP from fi brosing NSIP.20
tissue studies
Pathology: Historical Perspective and Current Classifi cation
Fibrotic, interstitial pneumonias have been recognized in clinical medicine for over a century. In 1892, Osler described cirrhosis of the lung as “a fi brinoid change, which may have its starting point in the tissue about the bronchi and blood-vessels, the interlobular septa, the alveolar walls or in the pleura. So diverse are the different forms and so varied the conditions under which this change occurs that a proper classifi cation is extremely diffi cult.”21 Subsequently, in 1944, Hamman and Rich described four cases of acute-onset,
Figure 3 Peripheral distribution of fi brosis seen on a roentgeno-gram of a patient with idiopathic pulmonary fi brosis. Note the “L reverse-L” appearance of the fi brotic periphery compared to the relative sparing of the central areas.

pulm-crit Interstitial and Fibrotic Lung Diseases — 5
10/08
rapidly progressive fi brotic lung disease characterized by “widespread connective tissue hyperplasia throughout the interstitial structures. The alveolar walls were tremendously thickened; in the early stages of the process crowded with fi broblasts.”22 For some time thereafter, the term Hamman-Rich syndrome was used for any diffuse, fi brotic lung dis-ease,23 even though we have subsequently learned that these cases represent a rather small portion of interstitial pneumonias (namely, AIP, described below).
In subsequent decades, the causes and associations of many interstitial pneumonias were identifi ed, including collagen vascular diseases, occupational exposures, medica-tions, and familial forms. Still, a number of conditions remained unexplained. After years of using various terms, a combined clinical and pathologic classifi cation scheme was proposed by Liebow and Carrington, in which fi ve distinct subtypes of IIP were described.24 This format was further developed and refi ned to the one described by Katzenstein and Myers in 1998.25 This classifi cation scheme has been
adopted by the ATS/ERS in their consensus statement, identifying the major histopathologic patterns and their clinical correlates.1
The major patterns described by Katzenstein and Myers, broadened somewhat by the ATS/ERS, include UIP, NSIP, DIP and the related respiratory bronchiolitis (RB), diffuse alveolar damage (DAD), lymphoid interstitial pneumonia (LIP), and bronchiolitis obliterans with organizing pneu-monia (BOOP). In many cases, the name of the pathologic pattern is the same as the name of the disease when that pathology is seen in an idiopathic entity. As such, the ATS/ERS recommends adding the term pattern to the pathology.1 For example, an NSIP pattern may be seen in NSIP, an idiopathic entity, or it may be seen in interstitial lung disease associated with collagen vascular diseases, such as rheumatoid arthritis. When the names of pathology and disease differ, each is used as appropriate. When a pattern of DAD is seen in conjunction with other processes, the diagnosis is adult respiratory distress syndrome (ARDS).
Figure 4 Traction bronchiectasis. Fibrosis peripherally causes the airways to lose their normally tapering. (a) and (b) Coronal and sagittal images from the same patient. (c) A patient with more extensive fi brosis. In all cases, the peripheral fi brosis leads to air-ways dilatation.
a b
c

pulm-crit Interstitial and Fibrotic Lung Diseases — 6
10/08
Lacking a known clinical association, the clinical diagnosis is AIP.
The major features of histopathologic patterns of inter-stitial lung diseases are discussed separately under each of the detailed discussions of the individual IIPs below. It
is important to recognize that several of these patterns of pathology will be seen in interstitial pneumonias associated with other conditions, such as various connective tissue diseases [search for these topics in this book]. Although many surrogate markers offer important information in the analysis of DPLD, histology, espe cially when UIP is found, remains the most important predictor of prognosis.26
The Role of Lung Biopsy
In many of the DPLDs, a surgical lung biopsy is needed to establish a diagnosis. Specimens obtained via transbron-chial technique are typically small, roughly the size of bread crumbs. Surgical biopsies are typically a few cubic centime-ters in size. Table 3 shows diagnoses that can be made on transbronchial biopsies.
The role of biopsy needs to be carefully considered in patients with functionally severe disease on presentation as the clinical course might not differ depending on the diag-nosis of UIP or fi brosing NSIP.27 The clinician should also note that patients with more severe disease are at increased risk for surgical lung biopsy. Mortality increases signifi -cantly as the DLCO approaches 30% or lower.28 Patients with UIP are more likely to experience a decline in FVC or an increase in radiographic ground-glass opacity in the 6 months following surgical lung biopsy than are patients with NSIP. A decrease in FVC adds to predictive value as well.29
Lettieri and colleagues reported low mortality rates in a retrospectively evaluated cohort of 83 patients undergoing surgical lung biopsy for DPLD.30 The overall mortality rate was 6.1% at 90 days, with a slightly higher rate of 9.5% in the patients ultimately diagnosed with IPF. In their cohort, the need for mechanical ventilation and being immunosup-pressed were risk factors for death. When these patients were excluded, the overall mortality rate was 1.5%. Seven (8.4%) of these patients experienced postoperative complica-tions, with only two in patients ultimately diagnosed with IPF (4.8%). In a separate cohort of 68 consecutive patients, a similar mortality rate of 4.4% was observed, but the compli-cation rate was much higher, at 19.1%, including frequent need for hospital readmission (10.7%) and the need for post-operative mechanical ventilation (5.9%).31 Finally, a series of 196 consecutive patients over 7 years in Taiwan indicated no mortality and a morbidity rate of 6.6%. This series included 43 patients with IIP, 34 with DAD, and 60 with infection disease (primarily in the setting of underlying immunosuppression).32
There have been case reports of acute exacerbations of IPF following surgical pulmonary resection for malignancy.33 The impact of this on diagnostic biopsies for DPLD is not clear,34 although 2 of 11 acute exacerbations occurring in a cohort of 147 patients occurred immediately following surgical lung biopsy.35
making a final diagnosis
Reaching a fi nal diagnosis in any patient with DPLD can be challenging. All aspects of the history, examination, imaging, laboratory data, and pulmonary function testing must be considered. An approach recommended by the ATS is presented in Figure 7. Often provisional diagnoses
Figure 5 Honeycombing, as seen in idiopathic pulmonary fi brosis. Note the areas of “stacked cysts” that refl ect advanced fi brosis.
Figure 6 Ground-glass opacifi cation. Note that normal lung archi-tecture can be seen, but the parenchyma has a diffuse “haziness” when compared with areas of complete aeration (such as the larger airways shown here). This example shows that ground-glass opacifi cation can, at times, be rather subtle.

pulm-crit Interstitial and Fibrotic Lung Diseases — 7
10/08
are made at multiple steps in the process. In some cases, a diagnosis may change months or even years after the onset of symptoms because new data have emerged, such as the clear development of a connective tissue disease.
In an important study performed by Flaherty and col-leagues, a stepwise approach in which the clinician has HRCT alone initially, progressing to full clinical details and pathology, along with the input from radiologists and
Table 2 Radiographic Features of Various Diffuse Parenchymal Lung Diseases1
Clinical Diagnosis
Histologic Pattern
Usual Radiographic Features
Typical Distribution on CT
Typical CT Findings CT Differential Diagnosis
IPF/CFA UIP Basal-predominant reticular abnormality with volume loss
Peripheral, subpleural, basal
Reticular, honeycombingTraction bronchiectasis/
bronchiolectasis; architectural distortion
Focal ground glass
AsbestosisCollagen vascular
diseaseHypersensitivity
pneumonitisSarcoidosis
NSIP, provisional
NSIP Ground-glass and reticular opacity
Peripheral, subpleural, basal, symmetric
Ground-glass attenuation
Irregular linesConsolidation
UIP, DIP, COPHypersensitivity
pneumonitis
COP OP Patchy bilateral consolidation
Subpleural/peribronchial
Patchy consolidation and/or nodules
Infection, vasculitis, sarcoidosis, alveolar carcinoma, lymphoma, eosinophilic pneumonia, NSIP
AIP DAD Progressive diffuse ground-glass density/consolidation
Diffuse Consolidation and ground-glass opacity, often with lobular sparing
Traction bronchiectasis later
Hydrostatic edema Pneumonia Acute eosinophilic pneumonia
DIP DIP Ground-glass opacity Lower zone, peripheral predominance in most
Ground-glass attenuation
Reticular lines
RB-ILD Hypersensitivity
pneumonitis SarcoidosisPCP
RB-ILD RB Bronchial wall thickening; ground-glass opacity
Diffuse Bronchial wall thickening
Centrilobular nodules Patchy ground-glass
opacity
DIP NSIP Hypersensitivity
pneumonitis
LIP LIP Reticular opacities, nodules
Diffuse Centrilobular nodules, ground-glass attenuation, septal and bronchovascular thickening, thin-walled cysts
Sarcoidosis, lymphangitic carcinoma, Langerhans cell histiocytosis
AIP = acute interstitial pneumonia; CFA = cryptogenic fi brosing alveolitis; COP = cryptogenic organizing pneumonia; DAD = diffuse alveolar damage; DIP = desquamative interstitial pneumonia; IPF = idiopathic pulmonary fi brosis; LIP = lymphoid interstitial pneumonia; NSIP = nonspecifi c interstitial pneumonia; OP = organizing pneumonia; PCP = Pneumocystis carinii pneumonia; RB-ILD = respiratory bronchiolitis–associated interstitial lung disease; UIP = usual interstitial pneumonia.
Table 3 Diseases that Can Be Diagnosed on Transbronchial Biopsy (Rather than Surgical Lung Biopsy)
Often Occasionally Rarely/Never
Sarcoidosis AIP (DAD pathology) IPF (UIP pathology)
Lymphangitic spread of tumor Vasculitis RB-ILD or DIP
Eosinophilic pneumonia Amyloidosis NSIP
Infections Langerhans cell histiocytosis LIP
Alveolar proteinosis Lymphangioleiomyomatosis COP (BOOP pathology)
AIP = acute interstitial pneumonia; BOOP = bronchiolitis obliterans with organizing pneumonia; COP = cryptogenic organizing pneumonia; DAD = diffuse alveolar damage; DIP = desquamative interstitial pneumonia; IPF = idiopathic pulmonary fi brosis; LIP = lymphocytic interstitial pneumonia; NSIP = nonspecifi c interstitial pneumonia; RB-ILD = respiratory bronchiolitis–interstitial lung disease.

pulm-crit Interstitial and Fibrotic Lung Diseases — 8
10/08
pathologists, led to the most accurate diagnosis.36 Using the histologic pattern of UIP on biopsy, the kappa value of the clinician reading the HRCT alone was 0.41 but increased to 0.86 when all pertinent data and consultation were allowed. These fi ndings argue for a multidisciplinary, consensus-reaching approach to diagnosing all challenging cases of IIP.
Idiopathic Interstitial Pneumonias
Each of the IIPs is discussed separately below. For discussion of DPLDs associated with other conditions elsewhere, see 14:VII Disorders of the Chest Wall.
idiopathic pulmonary fibrosis
Epidemiology
Surprisingly, limited data are available on the epidemiol-ogy of IPF, in part because of changes in the case defi nition over the past several decades. In addition, lack of familiarity
in the medical community with IPF and high mortality render this relatively uncommon disease diffi cult to charac-terize from a population standpoint. Estimates of annual incidence appear to be on the order of 10 per 100,000, with ranges reported from 6.8 to 16.4.3,37,38 Overall prevalence appears to be on the order of 20 per 100,000, with ranges reported from 14.0 to 42.7.3,37,38 Typically, IPF does not pres-ent until the sixth decade of life,1 and the annual incidence and prevalence increase signifi cantly in older individuals. For example, estimates of prevalence among individuals aged 75 and older may be as high as 276.9 per 100,000 men and 192.1 per 100,000 women.38 This pattern of male pre-dominance holds true in patients older than 65 years but may not be as pronounced in younger patients.38 Overall, males with IPF outnumber females by approximately 1.5 to 1.8:1.3,39 There has been a predominance of Caucasians reported in IPF, but there is no known racial predilection for the disease.3 There is no distinct geographic distribution for IPF.6
History, physical examination,chest radiograph, lung function tests
Not IIP(e.g., associated collagen vascular disease,
environmental, drug related)
Possible IIP
HRCT
Confident CT diagnosisof IPF with consistent
clinical features
Atypical clinicalor CT features
for IPF
Features diagnosticof another
DPLD (e.g., LCH)
SuspectedotherDPLD
If nondiagnosticTBBx
or BAL?
TBBx, BALor other
relevant test
Surgical lung biopsy
UIP NSIP RB DIP DAD OP LIPNon-IIP
confirmed
Figure 7 Diagnostic approach to diffuse parenchymal lung disease recommended by the American Thoracic Society. BAL = bronchoalveolar lavage; CT = computed tomography; DAD = diffuse alveolar damage; DIP = desquamative interstitial pneumonia; DPLD = diffuse parenchymal lung disease; HRCT = high-resolution computed tomography; IIP = = idiopathic interstitial pneumonia; IPF = idiopathic pulmonary fi brosis; LIP = lymphocytic interstitial pneumonia; NSIP = nonspecifi c interstitial pneumonia; OP = organizing pneumonia; LCH = Langerhans cell histiocytosis; RB = respiratory bronchiolitis; TBBx = transbronchial biopsy; UIP = usual interstitial pneumonia.

pulm-crit Interstitial and Fibrotic Lung Diseases — 9
10/08
Survival in IPF is poor. Symptoms are often present for months or even years before a diagnosis is made.1,39 Median survival following diagnosis is approximately 3 years. In one major center’s cohort, median survival following the onset of symptoms was greater than 6 years,39 suggesting that some patients may wait over 3 years before a diagnosis of IPF is made. Recent estimates suggest that mortality from IPF has increased. In this study, which analyzed data from the National Center for Health Statistics, the age-adjusted mortality rate increased 28.4% for men and 41.3% for women from 1992 to 2003 (i.e., from 40.2 to 61.0 deaths per 1,000,000 in men and from 39.0 to 55.1 deaths per 1,000,000 in women).
Risk factors for developing IPF include cigarette smoking, environmental antigens, infections, chronic aspiration, and drugs.1 Cigarette smoking has a fascinating impact on IPF as it paradoxically seems to both predispose individuals to IPF and “protect” them from disease progression.39–41 A majority of patients with IPF have a smoking history.39–41 At a major referral center in the United States, current smokers with IPF had an extended survival when compared with former smokers or never-smokers.39 In general, their disease seemed to be less severe than that of never-smokers. Interestingly, when a similar cohort at a British referral center was ana-lyzed and disease severity was considered, severity-adjusted survival was better in never-smokers than in either current or former smokers, or in those two groups combined.41 Taken together, these data suggest the possibility of a “healthy smoker” effect, in which patients quit smoking as their disease worsens. Whether smoking might both pre-dispose to fi brosis, perhaps through oxidative stress but, in turn, attenuate the fi brotic response to some degree remains to be seen.
Obesity has been associated with better survival in patients with IPF.42 In addition, nutritional depletion has been associated with poor survival in end-stage lung disease of many etiologies, including DPLD.43 Although the latter fi nding is intuitive, the former defi es easy reasoning. The study in question was retrospective and needs to be validated.
Histopathology
The usual interstitial pneumonia pattern is the most commonly seen pathology in ILD. A UIP pattern is seen in IPF (also known as cryptogenic fi brosing alveolitis in Europe) and is characterized by patchy, nonuniform, and variable distribution of interstitial changes.25 The variability in the amount of fi brosis within a biopsy is often apparent at scanning magnifi cation of the microscope: areas of dense fi brosis, interstitial infl ammation, honeycombing, and normal lung may all be present in the same section [see Figure 8]. Even within fi brotic areas, lesions of apparently different age are present, with some zones of acellular collagen deposition and areas of presumed active fi brosis (“fi broblastic foci”) [see Figure 9]. This fi nding is termed temporal heterogeneity. When present, interstitial infl amma-tion is usually mild, with lymphocytes, plasma cells, and histiocytes associated with hyperplastic type II pneumo-cytes.1 Biopsy specimens should show areas of relatively normal lung to make a pathologic diagnosis of UIP.
Otherwise, the pathologist may only be able to diagnose “severe fi brosis with honeycomb change (of uncertain etiology).”1
In addition to IPF, a UIP pattern can be seen in a number of other clinical settings, including collagen vascular dis-ease, drug toxicity, chronic hypersensitivity pneumonitis, asbsestosis, and rare disorders such as Hermansky-Pudlak syndrome.1 In some cases, further distinguishing character-istics on biopsy specimens may point to one of these diagnoses.
Pathogenesis
Because of the relentless progression of IPF in most individuals, our failure to understand the underlying patho-genesis has been particularly frustrating. Once thought to be an infl ammatory process, IPF is now considered to be a complex interaction of epithelial cells, mesenchymal cells, and various cytokines.44 The relative paucity of infl amma-tory cells seen on histopathology at most time points has led many to believe that infl ammation plays only a minor role, if any at all. This concept is supported by the fact that decades of typical anti-infl ammatory therapy have not been effective in treating IPF. An infl ammatory milieu, however, seems to be present in IPF, especially since proinfl ammatory cytokines, chemokines, antioxidants, and immunoglobulins are upregulated in patients with IPF.45 The common fi nding of mild mediastinal lymphadenopathy on CT images of patients with IPF also supports the notion that some infl ammation is present.16
At a fundamental level, most investigators agree on two aspects of IPF: (1) an initiating injury(ies) occurs, and (2) the host response is abnormal and persistent.46 Whether the injurious agent persists, whether the insult is too great to overcome, or whether the host is predisposed to abnormal recovery is uncertain.46 Any number of precipitating factors have been considered, including tobacco, gastroesophageal refl ux and aspiration, infections, and environmental expo-sures, among others.6 Although association with these factors has been seen in many studies, no clear causative roles have been established.
In IPF, epithelial cells, especially type I pneumocytes, are damaged and undergo apoptosis. Exposure of the basement membrane in the alveolus occurs, and this damage fails to be fully repaired. Type II epithelial cells become hyper-plastic, presumably in an attempt to repair the basement membrane, but they do not reestablish normal alveolar func-tion. Some have suggested that this phenomenon results from polarization of the immune response toward T helper type 2 immunity, which, in turn, stimulates the release of profi brotic cytokines, fi broblast migration, proliferation, and differentiation into myofl ibroblasts.47
In the setting of epithelial cell injury and basement membrane exposure, a number of growth factors accumu-late, including transforming growth factor–b (TGF-b), platelet-derived growth factors (PDGFs), and fi broblast growth factor-2, among others, the consequence of which may be recruitment of fi broblasts and myofi broblasts, often through tyrosine-kinase signaling pathways.48
Myofi broblasts are involved in fi brosis of virtually all tis-sues and have a phenotype between muscle and nonmuscle

pulm-crit Interstitial and Fibrotic Lung Diseases — 10
10/08
Figure 8 Usual interstitial pneumonia histopathologic pattern seen in idiopathic pulmonary fi brosis. Note the variegation seen in the amount of fi brosis at scanning magnifi cation. Dense fi brosis is seen adjacent to the pleura on the right of the image. On the left side of the image, areas of unaffected lung are present (hematoxylin-eosin stain; X20 original magnifi cation).
cells, with contractile and collagen-secreting properties.49 They express smooth muscle actin, a feature that distin-guishes them from other fi broblasts.50 Their contractility is stimulated by a number of cytokines, including endothelin-1 and TGF-b.49 They appear to be a key player in the fi brosis of IPF. The origin of these cells is not certain, and there is debate as to whether they are resident cells in the lung, whether they result from epithelial cells transitioning to mesenchymal cells in response to injury, or whether they are circulating cells derived from the bone marrow.47 Regardless of their origin, stimulated myofi broblasts appear to organize into clusters of cells known as fi broblastic foci. These clusters are typically adjacent to damaged epithelial cells and may often be at the “leading edge” of fi brosis, near normal-appearing lung.25 Fibroblastic foci are a characteris-tic feature of UIP pathology, distinguishing it from the other pathologies seen in DPLD.6
In conjunction with epithelial cell derangement and per-sistent fi brosis, a number of other potentially pathogenic aspects of IPF have been uncovered. Vascular remodeling in IPF includes very aberrant connections that may account for right-to-left shunting seen in IPF.47 Factors promoting
angiogenesis, such as basic fi broblast growth factor and vascular endothelial growth factor (VEGF), as well as certain CXC chemokines and interferon gamma, which inhibit anigogenesis, have been implicated in IPF.51 In addition, an imbalance of extracellular matrix production and degrada-tion may stem from increased production of tissue inhibitor of metalloproteinases (TIMPs), which inhibit breakdown of the matrix.
Given familial clustering of IPF (discussed below), several attempts have been made to identify gene polymorphisms that might be associated with sporadic IPF. At least 12 pub-lications to date have failed to identify polymorphisms in genes associated with IPF, including genes associated with infl ammation, surfactant proteins, the coagulation cascade, and fi broblast pathways.52 Ongoing studies of familial cohorts are focusing on identifying new genetic loci that might be associated with familial pulmonary fi brosis (FPF). If these studies are fruitful, genetic associations in sporadic IPF might also be unveiled.
In short, the pathogenesis of IPF is complex and poorly understood. Epithelial injury, damage to the basement membrane, and ineffective repair with features of exuberant

pulm-crit Interstitial and Fibrotic Lung Diseases — 11
10/08
fi brosis leading to the development of fi broblastic foci characterize progression of the disease. As summarized in Figure 10, important signaling molecules, including TGF-b, PDGF, VEGF, interferon gamma, endothelin-1, TIMPs, and CXC chemokines, among many others, come together in full orchestration to play out the relentless and unremitting loss of lung function seen in this devastating disease.
Clinical Features
History and physical examination The insidious onset of nonproductive cough and dyspnea characterizes IPF. Usually, these symptoms are present for more than 6 months.6 Dry, end-inspiratory, “Velcro-like” crackles are present in 80% of patients, typically originating in the bases bilaterally.1 Digital clubbing is noted in up to half of patients.1 Signs of PH and cor pulmonale may develop as disease progresses. Cyanosis also suggests more advanced disease.6
Imaging A confi dent diagnosis of IPF in the appropriate clinical setting can be made radiographically based on the presence of bilateral, predominantly subpleural, and basilar reticulations, with radiographic honeycombing present and absence of small nodules or extensive ground-glass opacities [see Figures 5 and 6].6,16,53 Of these fi ndings, lower lung
honeycombing [see Figure 5] and upper lung irregular lines may be the most important features; using these two factors alone gives positive predictive value for UIP pathology of 85%.16 When trained radiologists are confi dent of the diagnosis of IPF, they are accurate 95% of the time.53 The differential diagnosis of a radiographic UIP pattern includes collagen vascular disease, chronic hypersensitivity pneumonitis, and asbestosis.54
In terms of differentiating IPF from the other IIPs, the extent of honeycombing is perhaps the most important feature to distinguish UIP from fi brotic NSIP.55 Not sur-prisingly, the extent of radiographic fi brosis (reticulation and honeycombing) is an important predictor of mortality and has been shown to correlate well with impairments in gas exchange.12 Subpleural sparing is a feature more commonly associated with NSIP than UIP [see Figure 11]. UIP pathology can be distinguished from RB-ILD or DIP by less ground glass, lack of bronchovascular thickening, and greater extent of traction bronchiectasis.55 Parenchymal bands, mosaic perfusion, and subpleural branching opaci-ties and curvilinear lines appear to help distinguish asbestosis from UIP [see Figure 12].56
As discussed below, rapid deterioration during an acceler-ated phase of IPF is common. Radiographic fi ndings during these acute exacerbations include multifocal and diffuse
Figure 9 Fibroblastic focus adjacent to an airway within an area of active fi brosis in a patient with idiopathic pulmonary fi brosis (hematoxylin-eosin stain; X100 original magnifi cation).

pulm-crit Interstitial and Fibrotic Lung Diseases — 12
10/08
opacifi cations, often with a ground-glass appearance.35,57 It is important to recognize these, as well as to recognize other potentially treatable or signifi cant fi ndings on HRCT, includ-ing malignancy and atypical infections such as atypical mycobacteria, Pneumocystis, and mycetomas attributable to Aspergillus and other organisms [see Figure 13].58
Diagnosis
Diagnosing IPF with certainty requires the fi nding of UIP on pathology in the appropriate clinical setting, namely
the exclusion of other causes of UIP, such as drug toxicities, exposures, and collagen vascular diseases. Except in very early disease, restriction on pulmonary function testing with gas exchange impairments, as well as typical imaging abnormalities mentioned above, are usually seen.6 In the absence of a surgical biopsy, the ATS/ERS, in its consensus statement of 2000, outlined major and minor criteria in diag-nosing IPF. In this schema, all major criteria and at least three of the four minor criteria should be present to make a confi dent diagnosis of IPF in an immunocompetent host1:
Figure 10 Pathogenesis of idiopathic pulmonary fi brosis.

pulm-crit Interstitial and Fibrotic Lung Diseases — 13
10/08
Major criteria (all):• exclusion of other known causes of DPLD• abnormal pulmonary function with evidence of
restriction and impaired gas exchange• bibasilar reticular abnormalities with minimal ground-
glass opacities on HRCT• transbronchial lung biopsy or BAL showing no features
to support an alternative diagnosis
Minor criteria (at least three):• age > 50 years• insidious onset of otherwise unexplained dyspnea on
exertion• duration of illness > 3 months
• bibasilar, inspiratory crackles (dry or “Velcro”-like in quality)
Although most of these criteria are typically employed, we believe that many practitioners do not perform bronchosco-pies unless they are otherwise indicated (such as to assess for infection if clinically suspected). One group has reported the potential role of transbronchial biopsies in diagnosing UIP pathology.59 These data have not been validated yet, and traditional recommendations of surgical lung biopsy should apply for the time being.
Comorbid Clinical Conditions
Pulmonary hypertension PH has long been known to be a complicating feature of ILD associated with certain collagen vascular diseases, such as systemic sclerosis [search for these topics in this book]. The role of PH in IPF is starting to be better understood. The prevalence of PH in IPF is not precisely known and has been reported to range from 32 to 85% in different populations.60–63 The reasons for this wide discrepancy in rates are probably multifold, including the notion that the prevalence of PH progresses with disease. In a retrospective analysis of patients awaiting lung transplantion, the prevalence of PH increased from 33 to 85% in a retrospective analysis of one center’s patients awaiting lung transplantation.64
Right-heart catheterization remains the gold standard for diagnosing PH, and, unfortunately, no one surrogate test seems to replace it reliably. Echocardiography is relatively sensitive but overestimated PH in half of the patients undergoing lung transplantation evaluation in a retrospec-tive cohort study.65 Measuring brain natriuretic peptide might be useful in identifying patients with PH.66,67 Radio-graphic evidence of PH on plain fi lms (i.e., pulmonary artery enlargement) [see Figure 14] has been associated with increased mortality and should prompt further evaluation when present.39 In contrast, however, an enlarged pulmo-nary artery on HRCT did not correlate with PH in another study.68
Although mean pulmonary pressures seem to correlate with mortality,62,69 changes in mean pressures do not corre-late with FVC, suggesting that the mechanisms for PH in IPF extend beyond merely fi brosis and subsequent obliteration of the vasculature. A better marker for PH might be exercise
Figure 11 “Subpleural sparing” seen in nonspecifi c interstitial pneumonia but not typically seen in idiopathic pulmonary fi brosis.
Figure 12 Asbestosis. Findings favoring asbestosis over idiopathic pulmonary fi brosis include subpleural line (large black arrow), dotlike projections (red rarrows), and mosaic perfusion throughout. None of these fi ndings, however, are pathognomonic for asbestosis. Pleural plaques are also present in this image (small black arrows).

pulm-crit Interstitial and Fibrotic Lung Diseases — 14
10/08
capacity as both exercise capacity and PH affected survival on transplant waiting lists (although the two measures were not directly compared).70 The survival impairment attributable to PH may be more signifi cant than just refl ect-ing advanced disease as patients with PH who receive lung transplants fare worse following surgery than patients with no PH pretransplantation.71
Emphysema Smoking is associated with both IPF and emphysema. Not surprisingly, some patients develop both conditions [see Figure 15], and some experts feel that this should be considered a separate entity.72 A retrospective
study identifying patients’ radiographic evidence of both emphysema and pulmonary fi brosis suggests that this cohort is characterized by preserved lung volumes, signifi -cant impairments in gas exchange, hypoxemia with exer-tion, and concomitant PH in about half of the patients.72 The vast majority of patients in this study were males with a current or former history of smoking.72 The signifi cance of the male predominance needs to be assessed in further studies. All dyspneic patients presenting with normal lung volumes and an isolated reduction in gas exchange should be assessed for PH and combined emphysema and pulmonary fi brosis.73
Figure 13 Example of concomitant development of Aspergillus mycetoma and atypical mycobacterial infection in a patient with idiopathic pulmonary fi brosis. (a) Patient baseline 14 months earlier. (b) Cavity harboring a mycetoma that had formed. (c) Adjacent consolidation that was fl uorodeoxyglucose avid on positron emission tomography. Cultures from bronchoalveolar lavage grew both Aspergillus fumigatus and Mycobacterium avium complex.
a b
c

pulm-crit Interstitial and Fibrotic Lung Diseases — 15
10/08
Gastroesophageal refl ux disease Aspiration of gastric contents can lead to pulmonary fi brosis. In animal models, aspiration-induced lung injury occurs, and fi brosis has been reported in a pig model.74 Several small series indicate that aspiration is common in patients with IPF.75,76 One small retrospective case series suggests that treating aspiration was associated with stabilization of lung function in patients with IPF.77 Whether these results refl ect a promising avenue of therapy for IPF needs to be evaluated on a larger scale.
Other conditions Data from a limited number of small studies suggest that some other conditions may coexist with IPF at a higher rate than in the general population, as summarized below:
• In a cohort of patients awaiting lung transplantation at a single university center, a group with fi brotic lung disease had a higher prevalence of coronary artery dis-ease than a group with nonfi brotic lung disease (COPD,
Figure 15 Concomitant centrilobular emphysema and pulmonary fi brosis. Peripheral honeycombing, (a) (thick arrow) can be diffi cult to distinguish from paraseptal emphysema (b) (thin arrow).
a b
Figure 14 Enlargement of pulmonary artery on plain fi lms (a) and chest computed tomographic scan (b) in patient with idiopathic pulmonary fi brosis, emphysema, and pulmonary hypertension. In the setting of signifi cant fi brotic lung disease, it can be diffi cult to identify the pulmonary artery on plain chest roentgenograms.
a b

pulm-crit Interstitial and Fibrotic Lung Diseases — 16
10/08
PH primarily), after adjusting for coronary artery disease risk factors.78
• Patients with DPLD may have high rates of osteoporosis and osteopenia when compared with the general popula-tion, even after adjustment for current or previous use of corticosteroids and/or bisphosphonates.79
• Patients with IPF who receive lung transplants may be at increased risk for pulmonary embolism.80 Whether this refl ects a risk inherent to IPF remains to be determined.
The data from these studies need to be confi rmed in follow-up analyses. Clinicians should be aware of these potential associations in managing all patients with IPF.
Course of Disease and Predicting Outcomes
A number of investigators have attempted to identify which clinical variables are most important in predicting the course of disease in IPF. Virtually all reasonable clinical parameters have been explored, including the use of composite tools. At times, the results have been confl icting. Nonetheless, it is important to understand and identify useful studies, especially considering that lung transplanta-tion offers the most successful potential therapy. Given that lung transplantation requires a minimum threshold level of fi tness and functional capacity, IPF patients who decline too rapidly may miss the window in which transplantation will be considered.
The importance of baseline characteristics has been diffi -cult to determine. One simple reason for this relates to the combined effect of restrictive lung disease with concomitant obstructive lung disease and its impact on pulmonary function testing and imaging. Another confounding factor relates to the changes in diagnostic criteria for IPF and the other IIPs, rendering interpretation of older studies more challenging. In spite of these diffi culties, some simple func-tional assessments, such as desaturation on a 6-minute walk test to less than 88%, correspond to an increased risk of death.81 The amount of fi brosis seen on biopsy might also predict mortality.82–84 For patients awaiting lung transplanta-tion, the distance walked in 6 minutes may be more useful than other functional assessments.85 The 6-minute walk, a relatively straightforward study, seems to have superior predictive abilities and reproducibility than more elaborate exercise testing.86 Unfortunately, the utility of the 6-minute walk distance has not been borne out in all studies.87 Still, of all data from a single point in time, exercise capacity is probably the most useful.62,70,81,87,88
In a large, multicenter trial of patients with mild to moderate IPF, the extent of fi brosis seen on HRCT was associated with increased mortality.12 Interestingly, the extent of radiographic fi brosis in patients with NSIP also predicts mortality, perhaps even more accurately than the underlying pathologic diagnosis when compared with IPF.89
King and colleagues and Watters and colleagues proposed two models incorporating clinical, radiographic, and patho-logic (“CRP”) data at presentation to predict survival in patients with IPF.39,90 Their revised model from 2001—which incorporates age, smoking history, clubbing, extent of interstitial opacities, presence of PH on plain fi lm, TLC, and arterial oxygen tension (PaO2) at maximal exercise—offers
a prospectively validated survival model. Unfortunately, their data have not been confi rmed in follow-up studies, and the model might be cumbersome for the practicing clinician to use routinely. One interesting phenomenon that was once again shown to be present in this study related to the “protective” effect of active tobacco use, in which current smokers fare better than never-smokers, who, in turn, fare better than former smokers.39 Although smoking may retard the progression of disease, a more likely explanation is that the current smokers had less advanced disease.
Recognizing that many patients with IPF also have con-comitant emphysema, a scoring system that accounts for this was devised by UK physicians. This Composite Physiologic Index (CPI) makes an adjustment for the extent of emphy-sema. Using radiographic criteria, the authors developed a formula based on the extent of fi brosis and emphysema on CT scans. They then developed the CPI formula based on spirometry and gas exchange measurements to refl ect or predict the extent of fi brosis on imaging. This formula was then assessed in longitudinal follow-up and found to be predictive of mortality more closely than any of the isolated clinical parameters alone.91 This test may be most useful in making predictions about patients with both IPF and concomitant emphysema.91 Some investigators actually contend that IPF with emphysema should be considered a separate disease entity, often with a very poor prognosis.72
Although these indices may some day prove valuable, they are not widely used in clinical practice today. Further-more, changes in clinical parameters over time may be more useful in predicting clinical deterioration. A number of studies have now pointed to change in FVC, often set at 10%, as being clinically predictive of further disease progression.
As mentioned before, IPF, like the other IIPs, is a hetero-geneous disease. Ostensibly, similar patients may behave quite differently over time, and our ability to distinguish this on initial assessment is relatively poor. Several authors have investigated the predictive power of trends in clinical progression to predict mortality. Of the many variables investigated, a few stand out as predictive in a variety of settings, including a decline in FVC of 10% or more as early as 6 months.29,92–94 Other measures of disease progression, such as measures of oxygenation (A-a gradient, DLCO, amount of desaturation on a 6-minute walk test), and a decrease in six-minute walk distance may have prognostic signifi cance.29 Of all of these, a change in FVC of 10% may be the most reliable end point.95 Unfortunately, however, a number of patients appear to decline rapidly in an acute time frame without any previously documented 10% decre-ment. In a large, multinational study evaluating the use of interferon gamma (see below), 43% of those who died during the observation period did not have FVC decrements of 10%.95 In general, acute exacerbations of IPF, as well as admission to an intensive care unit (ICU) for any cause, portend a very poor prognosis.93,96
Acute Exacerbations
A poorly understood and often ominous feature of IPF is what is typically referred to as an acute exacerbation. A recent consensus statement has been proposed by the Idiopathic Pulmonary Fibrosis Clinical Research Network (IPFnet) in

pulm-crit Interstitial and Fibrotic Lung Diseases — 17
10/08
conjunction with several other internationally known inves-tigators.97 In this statement, proposed diagnostic criteria included the following:
• Previous or concurrent diagnosis of IPF• Unexplained worsening or development of dyspnea
within 30 days• HRCT with new bilateral ground-glass abnormality and/
or consolidation superimposed on a background reticular or honeycomb pattern consistent with a UIP pattern
• No evidence of pulmonary infection by endotracheal aspirate or BAL
• Exclusion of alternative causes, including the following: • Left heart failure • Pulmonary embolism
• Identifi able causes of acute lung injury
The incidence of acute exacerbations has been diffi cult to determine. Several retrospective studies have shown a wide range of incidence, ranging from 5% in 9 months to 57% in 3 years.97 Death is common during an acute exacerbation, with several studies reporting rates approaching 80 to 100%.97 Even in patients with early disease, rapid progres-sion of IPF occurs frequently. In a retrospective analysis of the control arm of a placebo-controlled clinical trial of patients with mild to moderate IPF, 21% died during the 76-week observation period, over half of whom experienced acute or subacute progression of disease, consistent with acute exacerbations [see Figure 16].93
No recognizable risk factors have been identifi ed, other than, potentially, surgical lung biopsy, as mentioned above. The risk does not seem to be related to the level of lung impairment.97 Typical clinical features include worsening of dyspnea and cough over the previous month.97 Fever and fl ulike symptoms have also been reported, complicating the notion of excluding infection in defi ning this entity.35,98 Lung biopsy specimens typically reveal DAD, with or without hyaline membranes, on a background of UIP.99 Other pathologic features, such as organizing pneumonia, may sometimes be seen.98,100
Treatment is generally supportive. If ventilated, patients should be treated with the same lung-protective strategies used to treat patients with ARDS [search for these topics in
]. In terms of pharmacologic therapy, high-dose glucocorticoids are typically used, but there are no data from controlled trials to prove their effi cacy.97 In a trial evaluating the use of anticoagulation in IPF, 32 of 56 patients
were hospitalized for acute exacerbation (53% of whom died).101 Interestingly, mortality was lower in the treated group than in those who did not receive anticoagulation (18% versus 71%), although signifi cant concerns about these data exist.102 Limited data suggest that pirfenidone, a novel antifi brotic agent, might protect against acute exacerba-tions.103
The etiology of acute exacerbations is unknown. Whether they refl ect a process intrinsic to the underlying pathology or an undiagnosed acute insult, such as a viral infection or gastroesophageal refl ux with aspiration, for example, remains to be determined.97
Treatment Considerations
Unfortunately, there is no proven therapy for the treat-ment of IPF. Clinical research has been marred by changing case defi nitions, a lack of placebo-controlled study arms, small numbers of patients, and a relatively short period between diagnosis and death. In spite of these limitations, pulmonologists and internists continue to prescribe medica-tions without proven benefi t in the hope that an individual patient might respond. Fortunately, more placebo-controlled trials are in progress or planned for the near future.
Anti-infl ammatory medications Based on the erroneous belief that IPF was driven primarily by infl ammation, corticosteroids have been used in treating IPF for decades, although there have never been any placebo-controlled clini-cal trials evaluating its use as monotherapy in treating IPF.104 Earlier studies have suggested that 10 to 30% of patients with IPF may respond to corticosteroids, but these were performed prior to the current classifi cation scheme and case defi nition of IPF and may therefore refl ect misdiagnosis.105,106 Based on several careful reviews, there is no evidence of suffi cient quality to justify routine use of corticosteroids alone in the treatment of IPF.106,107 As discussed below, there is marginal evidence to justify its use in conjunction with other agents.106–110 Steroids used in the treatment of IPF are associated with signifi cant morbidity.111
Cytotoxic and immunosuppressive agents Azathio-prine blocks DNA synthesis and thereby impairs pro-liferation of many cell lines, including neutrophils and lymphocytes. Like corticosteroids, azathioprine has been used to modulate the immune response thought to play a role in IPF. The best clinical trial conducted to date
Lu
ng
Fu
nct
ion
Time
a b
Time
Lu
ng
Fu
nct
ion Figure 16 Change in view of progression of idio-
pathic pulmonary fi brosis. Patients were once thought to decline steadily over time. Emerging evidence sug-gests that the decline occurs in more of a stepwise fashion, with sudden, unpredictable deteriorations occurring during the course of disease.
this book

pulm-crit Interstitial and Fibrotic Lung Diseases — 18
10/08
compared 13 patients receiving high-dose prednisone plus placebo with 14 patients treated with high-dose prednisone and azathioprine.108 In this study, a small survival benefi t was seen in the azathioprine arm after adjusting for age differences. In spite of the small size of this trial, therapy with azathioprine and prednisone has become common-place, especially in Europe, where a trial of N-acetylcysteine (NAc) was designed such that prednisone and azathioprine were given to the control group (discussed below).109
Cyclophosphamide is an alkylating agent that suppresses lymphocyte function. It is used in a number of autoimmune conditions, including many associated with DPLD [search for these topics in this book]. To date, no trial has shown a statistically signifi cant improvement associated with IPF.106,110 Given signifi cant side effects, including increased risk of myelosuppression, hepatoxicity, bladder toxicity, and several forms of malignancy, as well as the risk of DPLD 112
attributable to cyclophosphamide,113 its use cannot be recommended in the treatment of IPF.
Cyclosporine, mycophenolate mofetil, and methotrexate have not been shown to be effective in treating IPF.114 Although not directly comparable, progression of native lung fi brosis in IPF patients receiving a single lung transplant suggests that calcineurin inhibitor–based immu-nosuppression regimens are unlikely to be useful in treating IPF.115,116
Immunomodulatory and antifi brotic agents Interferon gamma-1b is a cytokine shown to have a number of inhi-bitory effects on fi broblasts. Based on a small preliminary study showing promising results,117 a large, randomized, placebo-controlled trial was conducted worldwide evaluat-ing its use versus placebo in 330 IPF patients who had not responded to a trial of corticosteroids.118 Although no differ-ence was seen between these two groups, a trend was seen toward better survival, and subgroup analyses indicated that patients with mild to moderate disease did have lower mortality. A follow-up trial focusing on these patients was recently terminated by the sponsor for increased mortality in the treatment group (http://www.clinicaltrials.gov; #NCT00075998; Press release; InterMune, March 6, 2007). As of the date of this publication, there appears to be no role for the use of interferon gamma-1b in the treatment of IPF.
Endothelin-1, a potent vasoconstrictor implicated in the pathogenesis of PH, has also been shown to have profi brot-ic properties. Bosentan, an endothelin-1 receptor antagonist, was evaluated in a randomized, placebo-controlled trial in the treatment of IPF (BUILD-1).119 This trial did not show a difference in the primary end point of increase in exercise capacity but did show trends toward delayed time to death or disease progression, especially in patients with early, radiographically mild, biopsy-proven disease.119 Based on subgroup analyses, the BUILD 3 trial is currently enrolling to determine if IPF patients with mild to moderate disease respond to treatment with bosentan (http://www.clinicaltrials.gov, #NCT00391443).
Pirfenidone is a novel agent with anti-infl ammatory, antioxidant, and antifi brotic properties. A randomized, double-blind, placebo-controlled trial conducted in Japan to evaluate the effects of this medication on oxygenation in patients with IPF was terminated by the data safety
monitoring board because the control group was experienc-ing acute exacerbations at a signifi cantly higher rate than the treatment group.103 Based on these fi ndings, as well as trends toward a benefi t in pulmonary function, a random-ized, double-blinded, placebo-controlled trial has completed enrolment of 400 patients worldwide, evaluating patients with both low-dose and high-dose pirfenidone (http://www.clinicaltrials.gov, #NCT00287716). This trial is expected to be completed by 2009.
Colchicine inhibits collagen synthesis and a number of other elements important in fi broblast proliferation. It has been evaluated in retrospective studies and one randomized controlled trial. To date, there is no compelling evidence arguing for its use in IPF.106,114 d-Penicillamine, another agent that interrupts collagen formation, has been used exten sively in the past, but no controlled trials have been performed, and its side effects may very well outweigh any potential benefi t it might have in treating IPF.114
Antioxidants NAc is an antioxidant compound used in the treatment of acetaminophen overdose. It is a precursor to glutathione and was shown to restore depleted glutathi-one levels in the lungs of patients with pulmonary fi brosis.120 A large, multinational trial tested use of high-dose NAc in conjunction with prednisone and azathioprine versus pred-nisone and azathioprine in the treatment of IPF.109 In this trial (the IFIGENIA study), patients in both groups experi-enced a decline in pulmonary function (FVC and DLCO) after a year of therapy, but the group that received NAc had less severe declines in these parameters. There was no mortality difference between the groups.
The results of the IFIGENIA trial are somewhat hard to interpret. Given that there was no placebo arm, it is impos-sible to tell whether prednisone/azathioprine/NAc offered a better outcome than no therapy at all. Some have postu-lated that NAc may have mitigated some of the possible harmful effects of azathioprine, including hepatotoxicity and myelotoxicity.106 A clinical trial conducted by the IPFnet evaluating prednisone/azathioprine/NAc versus NAc alone versus placebo is slated to begin enrolment in the near future (“PANTHER”; http://www.ipfnet.org). It is hoped that the results of the PANTHER trial will help clarify the role of NAc alone, as well as NAc used in conjunction with prednisone and azathioprine.
Anticoagulation Vascular injury and a tendency toward thrombosis may play a role in the pathogenesis of IPF. A study was performed in Japan evaluating the use of prednisolone or prednisolone plus anticoagulation in hospi-talized IPF patients.101 In this study, a survival benefi t—especially in patients experiencing acute exacerbations—was seen. Unfortunately, a number of methodologic fl aws in study design have rendered this small study diffi cult to interpret.106 Whether a benefi t to anticoagulation is shown in larger trials remains to be seen, but these results are encour-aging. Given a lack of effective therapy for acute exacerba-tions of IPF, one might want to weigh the benefi ts of empiric anticoagulation in these often terminal events.
Agents to treat PH As mentioned elsewhere, PH is being increasingly recognized as a comorbid condition in

pulm-crit Interstitial and Fibrotic Lung Diseases — 19
10/08
patients with IPF. One particular concern with treating PH in IPF patients is that many agents affect the entire pulmo-nary vascular bed indiscriminantly, potentially mitigating the protective effects of hypoxic vasoconstriction within particularly fi brotic areas of the lung. In some cases, how-ever, the magnitude of PH appears to be out of proportion to the severity of lung parenchymal disease, and several investigators have postulated that treating PH might be benefi cial.
Intravenous epoprostenol, well established in the treat-ment of idiopathic pulmonary arterial hypertension, does not appear to be effective in treating PH associated with IPF. It has been shown to decrease pulmonary vascular resis-tance and increase cardiac output, but at the expense of worsening shunting.51,121 Inhaled iloprost looked promising in pilot data121 and has been studied in a multicenter phase II trial, the results of which have not yet been published (http://clinicaltrials.gov, #NCT00109681).
Open-label use of sildenafi l for 3 months was associated with improvements in distance walked in 6 minutes.122 Two studies are currently under way evaluating the effect of sildenafi l on exercise capacity in patients with IPF. One is a multicenter trial being conducted by the IPFnet (http://www.ipfnet.org; http://clinicaltrials.gov, #NCT00517933); the other is a single-center study sponsored by the Veterans Administration (http://clinicaltrials.gov, #NCT00359737).
Calcium channel blockers are effective in a subgroup of patients with idiopathic pulmonary arterial hypertension but have not been shown to have a role in other forms of PH.123 Whether the potential role for anticoagulation in IPF discussed above actually refl ects treatment of the in situ thrombosis seen in PH is not clear.101
Lung transplantation Lung transplantation remains the only therapy for IPF with proven survival benefi t.124 Under the previous organ allocation system used in the United States for lung transplantation, time on the waiting list was paramount in being offered a transplant. Under this system, the median time on the waiting list was roughly 2 years. As of May 2006, the allocation system was revised such that a complex, iterative formula comparing antici-pated benefi t from transplantation with anticipated clinical course in the absence of transplantation now determines the priority of organ allocation. As a result, the waiting time for patients with IPF has decreased considerably.
As mentioned above, it is diffi cult to predict the course of disease in patients with IPF. Once any meaningful predictor of poor outcome has been reached, appropriate patients should be referred for transplantation. The need to refer patients at the time of initial diagnosis appears to have been obviated by the new allocation system.
Agents under investigation At the time of this publica-tion, results from a number of completed trials were pending. Agents under evaluation include etanercept, ima-tinib, zileuton, and rapamycin, among other agents. Thus far, studies on angiotensin-converting enzyme inhibitors and statins have not been promising.
nonspecific interstitial pneumonia
The concept of NSIP has evolved over time from describ-ing a “waste basket” of pathology not otherwise classifi able,
to a group of interstitial lung diseases with a favorable pro-gnosis when compared with IPF, to, more recently, a more specifi c clinical entity. NSIP has been described in conjunc-tion with a number of conditions, including collagen vascu-lar disease, chronic hypersensitivity pneumonitis, various other exposures, and, since the 1980s, HIV disease.1 The concept of NSIP as an idiopathic entity is more challenging for the clinician, especially given the notion that diseases associated with NSIP may not manifest until well after pulmonary disease occurs. In fact, some have contended that “idiopathic” NSIP is merely NSIP associated with undifferentiated connective tissue disease, presenting primarily in the lung.4
Histopathology
In contrast to UIP, NSIP is a temporally homogeneous process [see Figure 17].125 Although areas of spared lung and areas of dense infl ammation or fi brosis may be present, all of the lesions appear to be roughly the same age.125 This tem-poral uniformity distinguishes NSIP from UIP. Fibroblastic foci may be present in NSIP, but they are not prominent, nor is honeycombing, both of which would argue for a diagnosis of UIP [see Figure 9].
Today, there is a focus on classifying NSIP based on spe-cifi c features rather than a lack of specifi c features (as might be suggested by its name). Katzenstein and Fiorelli origi-nally described three patterns of NSIP histopathology: one with primarily cellular infl ammation, one with primarily fi brosis and a relative paucity of infl ammation, and a third with a mixed pattern.125 In the cellular NSIP pattern, mild to moderate interstitial infl ammation is seen in conjunction with type II pneumocyte hyperplasia.126 Interstitial fi brosis is absent, and there is a lack of alveolar septal thickening.126 In the fi brotic NSIP pattern, dense or loose fi brosis is seen, but not in the temporally heterogeneous pattern of UIP.126 The lung architecture is generally not lost (special staining may be required), and chronic infl ammation may be present [see Figure 18].1,126
Clinical Features
Because so many conditions can lead to NSIP, it is diffi cult to describe specifi c features of idiopathic NSIP as there are likely to be several subsets of patients captured under this classifi cation, many of whom may be manifesting aspects of an undiagnosed or undifferentiated connective tissue disease. In general, patients seem to present at a younger age than do patients with IPF, often in their late 40s or 50s, with a very wide range in age.127 No gender predominance is seen. The role of tobacco is not clear and does not seem to play the pivotal role in the development of disease that it does in other diseases, such as DIP or RB-ILD (see below). As in UIP, familial cohorts of NSIP have been identifi ed, some with association to specifi c genetic mutations, such as surfactant protein C.128,129
As with other forms of DPLD, patients with NSIP present with cough and dyspnea, typically present for more than a year.127 Bronchorrhea, fevers, chest paint, weight loss, and malaise have all been observed in NSIP.2,127 Crackles are common on examination, often in a basilar or sometimes widespread distribution.1,2,127 Inspiratory squeaks may be heard, and digital clubbing is seen as much as half the

pulm-crit Interstitial and Fibrotic Lung Diseases — 20
10/08
time.127 Given the strong association with connective tissue diseases, the physical examination of any patient with suspected or biopsy-proven NSIP needs to be particularly thorough.
Pulmonary function testing resembles that seen with IPF, with restriction and impairment in DLCO. Two-thirds of patients with NSIP will develop hypoxemia with exertion.1 Bronchoscopy differs from UIP with the fi nding of increased numbers on BAL of lymphocytes and neutrophils and eosinophils to a lesser degree.1
Imaging
Chest radiographs are typically abnormal in NSIP, with patchy alveolar opacities as well as interstitial changes [see Figure 19]. They are typically not helpful in the diagnosis, unlike HRCT scans.1 Several investigators have attempted to identify salient features of NSIP radiographically.130–135 The most common fi ndings in NSIP on HRCT are areas of ground-glass opacity and fi ne reticular opacities [see Figure 20]. Reticulation can lead to traction bronchiectasis and bronchiolectasis but not to the extent of frank honey-combing. In fact, it is common to observe an absence of
reticulation or any other signifi cant radiographic abnormal-ities at the periphery of lungs in patients with NSIP (so-called “peripheral sparing”) [see Figure 11].133,136 When honeycombing is seen, it seems to occur in cases of fi brotic NSIP exclusively.130 Examples of cellular and fi brotic NSIP are shown in Figure 20.
In many ways, the HRCT scan in NSIP is not as helpful in suggesting the pathologic diagnosis as it is in refl ecting the progress or resolution of disease. Ground-glass opacifi ca-tions are often present on early CT in this disease. Over time, decreased ground-glass opacity without the development or progression of reticulation has been associated with func-tional improvement, as is seen with successful treatment of cellular NSIP.132 Conversely, decreased ground-glass opacity in conjunction with increased reticulation on imaging corresponds to increased amounts of fi brosis and less infl ammation.130,133
Diagnosis
Making a confi dent diagnosis of idiopathic NSIP requires a surgical lung biopsy.1 Although NSIP is often presumed as the underlying pathology in DPLDs associated with con-
Figure 17 Histopathology of nonspecifi c interstitial pneumonia. The process is generally described as “temporally homogeneous,” meaning that the damage in all areas of injury appears to be the same age (hematoxylin-eosin stain; X40 original magnifi cation).

pulm-crit Interstitial and Fibrotic Lung Diseases — 21
10/08
Figure 18 Cellular (a) and fi brosing (b) variants of nonspecifi c interstitial pneumonia (hematoxylin-eosin stain; X100 original magnifi cation).
a
b

pulm-crit Interstitial and Fibrotic Lung Diseases — 22
10/08
nective tissue diseases, there are no radiographic or other features that would allow the clinician to make a confi dent diagnosis in lieu of tissue samples. A predominance of ground glass suggests a diagnosis of NSIP, but the ability of radiologists to make an accurate diagnosis ranges from 41 to 73%.89,130,135,137
Results from bronchoscopy are of some utility in NSIP but cannot be used to make a confi dent diagnosis. Given that BAL shows more lymphocytes in NSIP, it can be helpful
to distinguish NSIP from UIP.1 Unfortunately, many of the other conditions considered in the differential diagnosis may have a lymphocytic predominance on BAL as well. Transbronchial biopsies may be consistent with NSIP, but the amount of tissue obtained is generally inadequate.1
Even with surgical lung biopsies, the diagnosis may remain diffi cult. All surgical lung biopsy specimens need to be thoroughly reviewed as different pathology patterns may be present in the same patient. In general, the predominant pattern is thought be the most important, except in cases in which features of UIP are present with other patterns, such as NSIP. In these cases, the disease course generally mirrors that of patients with UIP alone.138,139
Another problem associated with interpreting surgical lung biopsy specimens relates to signifi cant interobserver disagreement in the diagnosis of specifi c DPLDs among expert pathologists,36,138,140 most of which centers around diagnosing NSIP. Given these uncertainties, it is essential to have an experienced surgeon biopsy three areas of the lung, ideally at the interface between normal and affected tissue, to optimize the chance of making the correct diagnosis.1
Once the pathology of NSIP is identifi ed, it is essential to redouble efforts to search for features suggestive of the many conditions associated with NSIP as treatment and prognosis vary widely among these different entities.
Treatment and Clinical Course
Treating idiopathic NSIP has generally included glucocor-ticoid and immunosuppression (azathioprine and cyclo-phosphamide most commonly), although no prospective, randomized, controlled trials have been performed.127 Retrospective data indicate that cellular NSIP responds
Figure 19 Plain roentgenogram of a patient with nonspecifi c interstitial pneumonia.
Figure 20 Cellular (a) and fi brosing (b) variants of nonspecifi c interstitial pneumonia (NSIP) radiographically. Note the similarities in the extent of ground-glass opacifi cations and lack of radiographic honeycombing (which would suggest usual interstitial pneumonia pathology). Cellular and fi brosing NSIP cannot be distinguished radiographically.
a b

pulm-crit Interstitial and Fibrotic Lung Diseases — 23
10/08
better to therapy than does fi brotic NSIP; in either case, however, relapses are common.127
The overall prognosis in NSIP is better than that in IPF or UIP from other causes. The clinical course is more variable, with some patients improving, many stabilizing, and some progressing to death.1 In some cases, the clinical course of NSIP is relentlessly progressive, such as that seen in IPF.133 Uncommonly, acute exacerbations of NSIP—with features similar to those seen in IPF—have been reported.141
The notion that NSIP in some cases actually becomes UIP has been debated for years. When both NSIP and UIP are seen in different biopsy sites done at the same time, the clinical course more closely follows that of IPF than of idio-pathic NSIP.138 In gene expression analyses, sporadic NSIP and UIP appear to be quite similar, whereas sporadic and familial IIPs differ considerably.142 Nonetheless, gene expression profi les have been successfully used to distin-guish UIP from NSIP,143 suggesting that some important differences do exist. For the time being, it is probably pru-dent to advise patients that IPF and NSIP are truly different entities, but NSIP may, on occasion, progress in a fashion very similar to that of IPF.
acute interstitial pneumonia
AIP is a rare form of fulminant DPLD that rapidly pro-gresses to respiratory failure and often death. In retrospect, we now know that it was the lung disease originally described by Hamman and Rich and for years was referred to as Hamman-Rich syndrome.22 AIP is perhaps best thought of as idiopathic ARDS. This histopathology of AIP—namely, DAD—is also seen in a number of other conditions, includ-ing ARDS of known cause, collagen vascular diseases, hematopoietic stem cell or solid-organ transplantation, drug reactions, radiation pneumonitis, hypersensitivity pneumo-nitis, viral and bacterial infection, acute eosinophilic pneu-monia, and acute exacerbations of IPF (discussed above).1,144 When one of these is present, a diagnosis of AIP is not appropriate.
Histopathology
DAD is an injury pattern that characteristically progresses from an acute pattern to one of organization and sometimes to one of end-stage fi brosis [see Figure 21]. At any stage, the lesions appear to be of the same age, suggesting a single insult, typically occurring weeks prior to biopsy (“temporal homogeneity”).25 Initially, epithelial cell injury leads to denuding of the alveolar wall, capillary leak, edema, and formation of hyaline membranes. Interstitial infl ammation may be prominent.1 In the subsequent organizing phase, active proliferation of fi broblasts and myofi broblasts occurs, with ensuing collagen deposition.145 Thrombi in small to medium-sized pulmonary arterioles may also be seen.145 If this process continues for a suffi cient period, a honey-comb-like appearance may result, with progressive and severe fi brosis.25 On other occasions, complete recovery may occur.1
Clinical Features
There is no gender predilection in AIP, and no relation-ship to smoking has been discerned.1 The age at onset varies widely, with a mean near 49 years (range 7–83 years).146
The onset of AIP is typically abrupt, with several days of a fl ulike illness with headaches, myalgias, malaise, sore throat, and productive cough.146,147 Exertional dyspnea ensues, often becoming severe.1 Patients typically present within 3 weeks of the onset of their symptoms appearing quite ill. Fever is present in half of patients at presentation, but all investiga-tions for infectious etiologies are, by defi nition, negative.146 Examination may show evidence of widespread consolida-tion or diffuse crackles. Digital clubbing is typically absent in AIP, and its presence might suggest a diagnosis of acute exacerbation of (undiagnosed) IPF.144
Pulmonary function testing, when done, shows a restric-tive pattern with gas exchange impairments, which are often severe.148 Hypoxemia is present, and patients commonly require mechanical ventilation.1 By clinical criteria, patients meet the defi nition of ARDS, namely, an acute onset, a ratio of PaO2 to fraction of inspired oxygen of less than 200, dif-fuse bilateral opacities on chest imaging, and a pulmonary arterial occlusion pressure of less than 18 cm H2O.1,148
Imaging
Chest radiographs often show bilateral, patchy opaci-fi cations, with sparing of the costophrenic angles [see Figure 22].149 As disease progresses, diffuse consolidation occurs. In the organizing phase, less consolidation is present, and irregular linear opacities are seen.1
CT shows areas of ground-glass attenuation, bronchial dilation, and architectural distortion, in different patterns at different points of disease progression [see Figure 23].149,150 Consolidation and ground-glass opacifi cations may be pres-ent at various times in the course of the disease. Traction bronchiectasis, along with interlobular septal thickening, typically signifi es the proliferative and fi brotic stages of DAD and has been associated with higher mortality.151,152
Treatment and Clinical Course
Unfortunately, proven therapies for AIP are lacking, and the standard of care takes clues from the treatment of ARDS. Supplemental oxygen therapy is almost always required. If disease progresses to necessitate mechanical ventilation, lung-protective strategies, as suggested by the ARDSnet trial,153 are appropriate.154 Use of positive end-expiratory pressure to limit potential oxygen toxicity, sedation to syn-chronize breathing with the ventilator, supplement nutri-tion, and all other typical aspects of respiratory care for the ICU patient are indicated.
Regarding medications, high-dose parenteral corticoste-roids are often recommended, in part based on beliefs that this therapy is benefi cial in improving survival in fi bro-proliferative ARDS.155 A recent follow-up trial suggests that moderate-dose corticosteroid therapy may be benefi cial in improving pulmonary function in early, severe ARDS.156 Whether these results can be translated to AIP remains to be seen. A recent retrospective case series reports lower mortality rates in association with steroid therapy lung-protective ventilation techniques.154 Another study suggests that patients with AIP fare better than those with ARDS associated with other conditions.157 Whether the results of these small case series will impact the care of patients affl icted by AIP remains to be seen.

pulm-crit Interstitial and Fibrotic Lung Diseases — 24
10/08
Mortality rates for AIP were historically high, with an overall case-fatality ratio of approximately 70%, but the range in these studies varied from 12.5 to over 90%.147 Unfortunately, reporting biases and other fl aws in case series analyses signifi cantly obscure any conclusions that can be drawn from these data. For those who survive, however, four general patterns of recovery have occurred: (1) complete recovery of lung function; (2) stable but persistent abnormalities in lung function; (3) progressive pulmonary fi brosis; and (4) recurrent AIP.147
RB-ILD and DIP
Although often classifi ed separately, the entities of RB-ILD and DIP are primarily smoking-related DPLDs perhaps best thought of as representing ends of a spectrum.1 Some confusion surrounding these diseases undoubtedly relates to the terminology used. Respiratory bronchiolitis is a patho-logic lesion found in cigarette smokers in which pigmented intraluminal macrophages are found within fi rst- and second-order respiratory bronchioles [see Figure 24]. Usually, these lesions are asymptomatic,158 but in rare cases, they are associated with signifi cant symptoms, impairments in
Figure 21 Diffuse alveolar damage seen in acute interstitial pneumonia. Hyaline membranes (arrows) are present in alveolar spaces. The interstitium contains a mixed cellular and fi brotic infi ltrate (hematoxylin-eosin stain; X100 original magnifi cation).
Figure 22 Chest roentgenogram in patient with acute interstitial pneumonia. Patchy alveolar opacities are radiographically indistin-guishable from those seen in adult respiratory distress syndrome.

pulm-crit Interstitial and Fibrotic Lung Diseases — 25
10/08
pulmonary function, and imaging abnormalities.1 In these instances, the term RB-ILD is used.
On the other end of this spectrum of smoking-related IIPs, pigmented macrophages fi ll alveolar spaces more diffusely and in more widespread areas of the lung in DIP. In addi-tion, infl ammation is often seen in the alveolar septae, and mild to moderate fi brosis may be present [see Figure 25].126 The term desquamative was originally used because it was thought that epithelial cells lining the alveolar spaces were sloughing off into the lumen.159 Although it was soon recog-nized that these cells were indeed macrophages, the termi-nology has persisted in spite of a recent international group considered changing the name to alveolar macrophage pneumonia.1 Further complicating this nomenclature is the fact that “DIP-like” lesions can be seen many other DPLDs, especially in current and former smokers.
Clinical Features
Case series describing features of RB-ILD and DIP indicate that roughly 90% of affl icted patients are current or former smokers.160,161 Other associations include drug exposures, connective tissue diseases, exposures, genetic mutations associated with DPLDs, and other conditions, such as hepatitis C infection.162–165 Although studies describ-ing these diseases are limited to cohorts of relatively few
Figure 24 Respiratory bronchiolitis–interstitial lung disease histopathology. Pigmented intraluminal macrophages are found within infl amed fi rst- and second-order bronchioles (hematoxylin-eosin stain; X40 original magnifi cation).
Figure 23 Computed tomographic image of early acute interstitial pneumonia. Ground-glass opacifi cation is the predominant feature radiographically.

pulm-crit Interstitial and Fibrotic Lung Diseases — 26
10/08
patients, RB-ILD and DIP both appear to occur in men about twice as often as in women, typically arising in the fourth to fi fth decades of life.1 Smoking histories on average of 30 pack-years or more are common.1,166
As with other IIPs, patients with RB-ILD or DIP often describe the insidious onset of gradual dyspnea and a dry cough.1 Inspiratory crackles may be found on examination, and digital clubbing has been reported in as many as half of patients with DIP160–162,167 and up to a quarter of patients with RB-ILD.161,166 Pulmonary function testing shows restriction, obstruction, a reduction in gas exchange, or a combination of all three.161,165,166,168
Imaging
Radiographs in RB-ILD/DIP emphasize the importance of using CT over roentgenograms in the evaluation of DPLDs as chest x-rays may show thickening of the bronchial walls or faint interstitial opacifi cations but in many cases may be normal.1,159,161,169 Common CT abnormalities seen include centrilobular nodules, ground-glass attenuation, and some-times fi brosis [see Figure 26].55 In keeping with the notion
that these diseases occupy different ends of a spectrum of disease, more ground-glass opacities and more fi brosis have been observed in DIP than in RB-ILD.169
Treatment and Clinical Course
Unfortunately, since RB-ILD and DIP are relatively rare diseases, the number of patients described in case series thus far does not allow for a reliable understanding of the natural history of these diseases. Nonetheless, certain observations can be made:
1. Many patients, especially after smoking cessation, seem to have a relatively stable course.
2. In spite of the above, radiographic and pulmonary function abnormalities may persist for years.161,170
3. Mortality rates for DIP appear to be much better than for IPF, with reports of around 30% in 9 years of follow-up.160,162
4. RB-ILD may respond to smoking cessation alone,162 although a recent report suggests that disease progression occurs in spite of avoiding tobacco.166
Figure 25 Desquamative interstitial pneumonia (DIP). Like respiratory bronchiolitis–interstitial lung disease, pigmented macrophages are present in airways. The infl ammation in DIP is more diffuse, and evidence of collagen deposition (fi brosis) is also present (hematoxylin-eosin stain; X20 original magnifi cation).

pulm-crit Interstitial and Fibrotic Lung Diseases — 27
10/08
5. The role of and response to corticosteroid therapy are much harder to determine because of a lack of controlled trials. Many patients with DIP have reported sympto-matic improvement after the initiation of corticosteroid therapy,160,162 and resolution of ground-glass infi ltrates following corticosteroid therapy has been reported.171
cryptogenic organizing pneumonia
As an idiopathic entity, COP was fi rst described by Davison and colleagues in 1983172 and then by Epler and col-leagues in 1985.173 Epler used the term bronchiolitis obliterans organizing pneumonia (BOOP) to describe the clinical disease and the pathology. The joint ATS/ERS commission has recommended using COP for the disease that would be con-sidered “idiopathic BOOP”1 primarily because it conveys the essential features of the entity and avoids confusion with other clinical entities, such as constrictive bronchiolitis obliterans.1
Organizing pneumonia is a pathologic pattern seen in a number of infl ammatory conditions. In many cases, simulta-neous involvement of the alveoli and terminal bronchioles leads to a pattern described as BOOP. Features of BOOP have been described in association with a large number of other conditions, including postinfection, use of prescrip-tion and recreational drugs, rheumatologic conditions, immunodefi ciencies, environmental exposures, and miscel-laneous other diseases, such as infl ammatory bowel disease, thyroiditis, and primary biliary cirrhosis [see Table 4].174
Histopathology
The hallmarks of organizing pneumonia include excessive proliferation of granulation tissue in small airways and
alveolar ducts with chronic infl ammation in the surround-ing tissue [see Figure 27].175,176 These buds of granulation tissue may extend from one alveolar duct to another, leading to a “butterfl y” pattern of fi brinous pneumonia. These lesions occupy airspaces predominantly, often in a patchy ditribution along bronchovascular bundles. The appearance of the lesions suggests that they are of approximately the same age (“temporal homogeneity”) Foamy macrophages are often seen in the alveolar spaces. Giant cells, granulo-mas, and vasculitic lesions are not present. Advanced fi brosis and microscopic honeycombing are not present at the time of diagnosis.
Clinical Features
On average, COP typically arises in the sixth decade of life, but the range has been reported as 21 to 80 years.177 Men and women seem to be affected equally, and nonsmokers and ex-smokers are affected approximately twice as often as current smokers.178 Unlike those affl icted with IPF, patients with COP can often describe with certainty when they fi rst developed symptoms, which often include a fl ulike illness with fevers, cough, malaise, anorexia with weight loss, and progressive dyspnea.177,178
On physical examination, patients with COP will often have dry, inspiratory crackles, although up to a quarter of patients may have a normal respiratory examination.178 Digital clubbing is rare.177–179
Laboratory studies are nonspecifi c and can mimic infec-tion. Elevated white blood cell counts, as well as markedly elevated C-reactive protein and erythrocyte sedimentation rates (often exceeding >100 mm/hour), have been report-ed.178,179 Neutrophils in the peripheral blood count may be elevated; increases in eosinophils are not typical178
Figure 26 Computed tomographic features of respiratory bronchiolitis–interstitial lung disease may include subtle foci of ground-glass opacifi cation (a). In desquamative interstitial pneumonia (b), more extensive ground-glass opacifi cation may be present.
a b

pulm-crit Interstitial and Fibrotic Lung Diseases — 28
10/08
and would point toward other diagnoses, such as chronic eosinophilic pneumonia.
Imaging
Three main chest radiographic patterns have been described in COP: “typical COP” with multiple alveolar infi ltrates, “focal COP” with a solitary opacity, and “infi ltra-tive COP” with infi ltrative opacities.178,180,181 Infi ltrates may be migratory.182 On CT, there is often a bronchocentric pattern in which areas of consolidation, ground glass, nodules, and nonseptal linear or reticular opacities may follow the
bronchovascular bundles [see Figure 28].178,181,183,184 Honey-combing is typically present only in late-stage, progressive disease.184 Pleural thickening, pleural effusions, hyperinfl a-tion, and cavitary lesions have been reported.177,185
Pulmonary Function
Lung function testing typically shows a restrictive ventila-tory defect with evidence of a gas exchange impairment.178 Obstruction is seen in those with a history of smoking and underlying COPD.177,178 Hypoxemia is common, especially with exertion.177 Severe cases of hypoxemia with evidence of intra-alveolar shunting have also been reported.178
BAL samples in patients with COP are similar to those seen with hypersensitivity pneumonitis, namely, an increase in neutrophils and lymphocytes and a low CD4-to-CD8 T cell ratio.177,186 Detection of eosinophils is uncommon and would suggest an eosinophilic pneumonia as an alternative diagnosis.177
Diagnosis
Diagnosing COP requires a high degree of clinical sus-picion. Many patients are initially misdiagnosed as having a bacterial pneumonia, often receiving one or two courses of antibiotics before COP is considered, leading to delays in diagnosis of 1 to 3 months.178 The differential diagnosis is broad and includes, in addition to bacterial pneumonia, hypersensitivity pneumonitis, ARDS/AIP, chronic eosino-philic pneumonia, and aspiration pneumonia, among several other entities.
Radiographically, bronchial dilatation and nonseptal linear or reticular opacities appear to be more common in COP than in chronic eosinophilic pneumonia, but this dis-tinction is diffi cult to make with confi dence.181 Generally, radiographs alone are not useful in distinguishing COP from its many mimics.
When tissue is obtained, surgical lung biopsy via thorac-tomy or through video-assisted thoracoscopy is recom-mended. An algorithm for using the combination of BAL and transbronchial biopsies186 has been suggested, but the inadequate amount of tissue obtained via a fl exible broncho-scope limits this approach.3 A pathologist experienced in examining lung tissue should be advised of the clinical and radiographic fi ndings as the fi nding of organizing pneumo-nia should prompt a search for related conditions mentioned above [see Table 5]. Only when all other conditions associat-ed with organizing pneumonia are ruled out clinically and by histopathology should a diagnosis of COP be made.
Treatment and Clinical Course
Unlike many of the IIPs, COP can often be treated effectively, at least initially. Corticosteroids are the mainstay of initial therapy, typically at moderate to high doses over several months to a year. No standardized consensus has been reached: a typical regimen includes once-daily doses of 1 mg/kg (60 mg/day) for 1 to 3 months followed by 40 mg/day for 3 months, then tapering for a total duration of 1 year,174,177,178 whereas others have suggested shorter courses initially.3 Although shorter courses may be effective in certain individuals, relapses are common, often within 1 to 3 months of discontinuing or even tapering corticosteroids.173,177,187 Parenteral methylprednisolone at doses of 500 to 1,000 mg/day (“pulse dosing”) has been
Table 4 Various Medical Conditions Associated with Bronchiolitis Obliterans
Organizing Pneumonia (BOOP) on Pulmonary Histopathology118
Idiopathic BOOPRapidly progressive BOOPFocal nodular BOOPPostinfection BOOP Chlamydia, Legionella, and Mycoplasma Adenovirus, cytomegalovirus, and infl uenza virus Malaria and Pneumocystis CryptococcusDrug-related BOOP Antibiotics: amphotericin B, cephalosporins, minocycline,
nitrofurantoin, sulfasalazine, and sulfamethoxypyridazine Bleomycin sulfate and methotrexate Gold Amiodarone Illicit use of cocaine l-Tryptophan Phenytoin Carbamazepine Ticlopidine hydrochlorideRheumatologic or connective tissue BOOP Lupus erythematosus Rheumatoid arthritis Sjögren syndrome and Sweet syndrome Polymyositis-dermatomyositis Scleroderma-progressive systemic sclerosis Ankylosing spondylitis Polymyalgia rheumatica Behçet syndromeImmunologic disorder BOOP Common variable immunodefi ciency syndrome Essential mixed cryoglobulinemiaOrgan transplantation BOOP Bone marrow, lung, and renalRadiotherapy BOOPEnvironmental exposures Textile printing dye Penicillium mold dust House fi reMiscellaneous BOOP Infl ammatory bowel disease Lymphoma and cancer T cell chronic lymphocytic leukemia HIV infection Myelodysplastic syndrome Hunner interstitial cystitis Chronic thyroiditis and alcoholic cirrhosis Seasonal syndrome with cholestasis Primary biliary cirrhosis Coronary artery bypass graft surgery

pulm-crit Interstitial and Fibrotic Lung Diseases — 29
10/08
Figure 27 Bronchiolitis obliterans with organizing pneumonia histopathology seen in cryptogenic organizing pneumonia. Granulation tissue is present in small airways, whereas chronic infl ammation is present in surrounding lung tissue (hematoxylin-eosin stain; X40 original magnifi cation).
recom mended for particularly rapidly progressing forms of COP,3 and cytotoxic therapy with cyclophosphamide and azathioprine has been used.
In some series, relapses occur in over half the cases.187 In spite of this, most patients respond to retreatment with cor-ticosteroids, although some may require long-term therapy. In spite of this, data do not suggest long-term morbidity and mortality as a consequence of recurrence.187 Because of their anti-infl ammatory effects, macrolides have been associated with effective maintenance therapy in treating a few patients with COP as well as BOOP relating to radiation injury.188,189
lymphoid interstitial pneumonia
Like other terms used to describe DPLDs, LIP has under-gone some changes in its defi nition since fi rst introduced by Liebow and Carrington in 1969.24 Once thought to be a
Figure 28 Chest computed tomography in cryptogenic organizing pneumonia mimics the appearance of multifocal pneumonia. Bron-chocentric consolidation with scattered nodules and ground-glass opacifi cations is present in this image.

pulm-crit Interstitial and Fibrotic Lung Diseases — 30
10/08
Epidemiology and Clinical Features
Idiopathic LIP is uncommon. For example, searching the clinical database of patients seen in the Interstitial Lung Disease Clinic at the National Jewish Medical and Research Center in Denver, Colorado, from 1985 to 1999 revealed only 15 cases of histopathologically confi rmed LIP out of 1,167 patients biopsied.192 Only three of these were believed to have idiopathic LIP. LIP occurs more frequently in women, often diagnosed in the fi fth decade of life.1,192 As in other IIPs, symptoms progress gradually, with cough and breath-lessness being most prominent, in addition to fever, weight loss, chest pain, and arthralgias in some cases.1
preneoplastic disorder, it has since been suggested that many putative cases of LIP were actually low-grade lym-phomas from the outset1 and that malignant transformation of LIP is a rare event.190,191 The histopathology of LIP is seen in conjunction with a number of conditions, and fi nding it on surgical lung biopsy warrants a thorough investigation for these conditions, which include rheumatoid arthritis, Sjögren syndrome, Hashimoto thyroiditis, pernicious ane-mia, hepatitis, systemic lupus erythematosus, autoimmune hemolytic anemia, primary biliary cirrhosis, myasthenia gravis, hypogammaglobulinemia, and immunodefi ciency states, including HIV.1
Table 5 Summary of Key Features of the Idiopathic Interstitial Pneumonias*Clinical-
Radiographic-Pathologic Diagnosis
IPF NSIP COP AIP DIP, RB-ILD LIP
Duration of illness
Chronic (> 12 mo) Subacute to chronic (months to years)
Subacute (< 3 mo)
Abrupt (1–2 wk) Subacute (weeks to months), smoker
Chronic (> 12 mo), women
Frequency of diagnosis
47–64% 14–36% 4–12% Rare (< 2%) 10–17% Rare
HRCT Peripheral, subpleural, basal predominance
Peripheral, subpleural, basal, symmetric
Subpleural or peribronchial
Diffuse, bilateral DIP: diffuse ground-glass opacity in the middle and lower lung zones
Diffuse
Reticular opacities Ground-glass attenuation
Patchy consolidation
Ground-glass opacities, often with lobular sparing
RB-ILD: bronchial wall thickening, centrilobular nodules, patchy ground-glass opacity
Centrilobular nodules
Honeycombing Consolidation (uncommon)
Nodules Ground-glass attenuation
Traction bronchiectasis/bronchiolectasis
Lower lobe volume loss
Septal and bronchovascular thickening
Architectural distortion
Subpleural sparing may be seen
Thin-walled cysts
Focal ground glass (rare)
Histologic patterns
Usual interstitial pneumonia
NSIP Organizing pneumonia
Diffuse alveolar damage
DIP, RB-ILD LIP
Treatment Poor response to corticosteroid or cytotoxic agents
Corticosteroid responsiveness
Corticosteroid responsiveness
Effectiveness of corticosteroid unknown
Smoking cessation Corticosteroid responsiveness
Corticosteroid responsiveness
Prognosis 50–80% mortality in 5 yr
Unclear, < 10% mortality in 5 yr
Deaths rare 60% mortality in < 6 mo
5% mortality in 5 yr
Not well defi ned
Adapted from King TE Jr. Clinical advances in the diagnosis and therapy of the interstitial lung diseases. Am J Respir Crit Care Med 2005;172:268–79.AIP = acute interstitial pneumonia; COP = cryptogenic organizing pneumonia; DIP = desquamative interstitial pneumonia; HRCT = high-resolution computed tomography; IPF = idiopathic pulmonary fi brosis; LIP = lymphocytic interstitial pneumonia; NSIP = nonspecifi c interstitial pneumonia; RB-ILD = respiratory bronchiolitis–associated interstitial lung disease.

pulm-crit Interstitial and Fibrotic Lung Diseases — 31
10/08
Imaging
CT generally reveals ground-glass opacities, ill-defi ned centrilobular nodules, and sometimes frank consolidation [see Figure 29].193 Thin-walled cysts, bronchovascular thick-ening, and interlobular septal thickening have also been described.55,194,195
Pathology
The histology of LIP is characterized by dense infi ltration within the alveolar septae with lymphocytes, plasma cells, and histiocytes, as well as type II pneumocyte hyper-plasia and lymphoid follicles along the distribution of the lymphatics.1 Architectural distortion, to the point of honeycombing occasionally, nonnecrotizing granulomas, and intra-alveolar macrophages, may also be present [see Figure 30].1
Treatment and Clinical Course
There are no standards for treating LIP. Schwarz and King recommend treating in a fashion similar to that for COP: prednisone at 1 mg/kg/day for 8 to 12 weeks tapered to 0.25 mg/kg/day over the next 1.5 to 3 months.3 Long-term resolution or stability following corticosteroids alone has been reported in as many as 50% of patients.196 A number of other immunosuppressive and cytotoxic agents have been used, including cyclophosphamide, azathioprine, and cyclo-sporine, and lung transplantation has also been performed.192 Median survival in one cohort of LIP patients was 11.5 years.192 Unfortunately, few of these reports are limited to idiopathic LIP, and new molecular techniques now allow for better detection of lymphoproliferative disorders that might signifi cantly affect mortality statistics. Such data, therefore, should be interpreted with caution.
familial pulmonary fibrosis
DPLD was fi rst described in families over 50 years ago.197 FPF is generally defi ned as two or more members of the same family with idiopathic DPLD. Several lines of evidence point to a genetic component of FPF, including clustering in family members in distinct environments; autosomal dominant inheritance (with variable penetrance); pulmo-nary fi brosis in known genetic disorders, such as Herman-sky-Pudlak syndrome, neurofi bromatosis, and dyskeratosis congenita; differential responses to known fi brogenic dusts, such as asbestos; and variable expression of pulmonary fi brosis among different mice strains exposed to bleomycin.198
Understanding the genetics of FPF has been challenging. Several candidate genes have been explored,52 but only the genes encoding for two proteins have been implicated in larger familial cohorts of FPF.128,163,199 A case report of a muta-tion in SFTPC,163 the gene encoding for surfactant protein C, arising in a mother and daughter with IIPs led to fi nding a separate mutation of the same gene in several generations of a large kindred.128 Mutations in SFTPC can lead to accumu-lation of abnormal surfactant proteins in type II cells of the lung, leading to fi brotic changes in cellular models.129,200–202 Thus far, at least 12 additional mutations in surfactant protein C have been associated with DPLD.202 To date, these mutations have rarely been observed in sporadically occurring DPLD.203–205
A similar series approach was taken in evaluating a cohort for mutations in telomerase, an enzyme that contributes to DNA and RNA stability and that is abnormal in dyskera-tosis congenita. Dyskeratosis congenital is a rare hereditary disease with a number of clinical features, including skin hyperpigmentation, oral leukoplakia, nail dystrophy, and, in one-fi fth of patients, pulmonary fi brosis.206 Heterozygous mutations in hTERT and hTR, two genes that encode for telomerase, have been identifi ed in a registry of families with pulmonary fi brosis.199 Screening in another group of patients with FPF revealed additional mutations in hTERT as well as another in hTERC, which encodes for the RNA component of telomerase.207 Given that smoking causes telomere shortening that would be repaired by telomerase,208 and smoking is a risk factor for developing FPF,198 a mechanistic explanation for smoking and FPF seems plausible.
Clinically, FPF appears to have characteristics similar to those of the various forms of IIPs described above. Most pedigrees are heterogeneous, with different manifestations of IIPs occurring within the same family.198 Smoking is strongly associated with development of disease,198 and the risk of mortality increases as more family members are affected.209
Studying the details of FPF may provide signifi cant insight into its causes and the causes of sporadic IIPs.
advanced fibrotic lung disease
In some cases, radiographs and surgical lung biopsy demonstrate such severe fi brosis that no underlying diagnosis can be made. Even in these cases, attempts should be made to understand the precipitating causes and disease course to hone in on a likely diagnosis as the outcome may differ substantially. Patients with asbestosis or end-stage
Figure 29 Lymphoid interstitial pneumonia. Ground-glass opacifi -cations, nodules, and cystic lucencies (or some combination thereof) may be seen on high-resolution computed tomography.

pulm-crit Interstitial and Fibrotic Lung Diseases — 32
10/08
Figure 30 Histopathology of lymphoid interstitial pneumonia. Dense infi ltration of lymphocytes leads to architectural distortion (hematoxylin-eosin stain; X20 original magnifi cation).
sarcoidosis may have a better prognosis than those with IPF.
Conclusions
DPLD can be particularly challenging to characterize and treat. Over the past several decades, this fi eld of medicine has been encumbered by changing classifi cation schemes, a poor understanding of disease progression, and empiric use of a number of medications in spite of a lack of supporting evidence. Fortunately, consensus panels of experts have met and decided on broadly accepted classifi cation schemes. A better understanding of the complex pathophysiology has allowed for consideration of a number of new therapies. The medical community has a better understanding and recognition of these diseases, and the advent of HRCT has led to earlier diagnosis.
Any patient with DPLD needs a thorough investigation, including a detailed history and physical examination, laboratory analyses, pulmonary function testing, HRCT of the chest, and other ancillary studies. Based on careful
review of these data, the clinician determines if a surgical lung biopsy will be necessary. Diagnostic options need to be evaluated in the context of determining whether the patient has IPF, a disease with limited treatment options, or a DPLD that might be responsive to therapy. Our ability to predict the clinical course of disease is generally quite limited. As such, appropriate patients with progressive fi brotic diseases should be referred early for lung transplantation evaluation.
In recent years, several randomized, placebo-controlled, investigational trials have been completed or are in progress. Although clear and compelling treatment has not emerged, a number of agents appear to be promising, at least in some settings. Earlier recognition of disease and enrolment of patients in clinical trials will likely play critical roles in ultimately achieving effective therapies. The advent of two important consortia, the IPFnet in the United States and the European IPF Network (EurIPFnet), will undoubt-edly lead to important studies in the coming years. Clinical data, along with a better understanding of the underlying pathophysiology, will someday lead to effective therapies for these devastating diseases.

pulm-crit Interstitial and Fibrotic Lung Diseases — 33
10/08
Lake D. Morrison, MD, has received grants for clinical research from Actelion, maker of bosentan, and from InterMune Pharma-ceuticals, maker of pirfenidone, as well as from the National Institutes of Health.
Paul W. Noble, MD, has served as a consultant for InterMune Pharmaceuticals and Actelion.
References
1. American Thoracic Society/European Respiratory Society International Multidisciplinary Consensus Classifi cation of the Idiopathic Interstitial Pneumonias, June 2001. Am J Respir Crit Care Med 2002;165:277–304.
2. Cottin V, Donsbeck AV, Revel D, et al. Nonspecifi c inter-stitial pneumonia. Individualization of a clinicopathologic entity in a series of 12 patients. Am J Respir Crit Care Med 1998;158:1286–93.
3. Schwarz MI, King TE Jr. Interstitial lung disease. 4th ed. Hamilton (ON): BC Decker; 2003.
4. Kinder BW, Collard HR, Koth L, et al. Idiopathic nonspe-cifi c interstitial pneumonia: lung manifestation of undif-ferentiated connective tissue disease? Am J Respir Crit Care Med 2007;176:691–7.
5. Doherty MJ, Pearson MG, O’Grady EA, et al. Cryptogenic fi brosing alveolitis with preserved lung volumes. Thorax 1997;52:998–1002.
6. American Thoracic Society. Idiopathic pulmonary fi brosis: diagnosis and treatment. International consensus state-ment. American Thoracic Society (ATS), and the European Respiratory Society (ERS). Am J Respir Crit Care Med 2000;161:646–64.
7. Hanley ME, King TE Jr, Schwarz MI, et al. The impact of smoking on mechanical properties of the lungs in idio-pathic pulmonary fi brosis and sarcoidosis. Am Rev Respir Dis 1991;144:1102–6.
8. The diagnosis, assessment and treatment of diffuse parenchymal lung disease in adults. Introduction. Thorax 1999;54 Suppl 1:S1–14.
9. Epler GR, McLoud TC, Gaensler EA, et al. Normal chest roentgenograms in chronic diffuse infi ltrative lung disease. N Engl J Med 1978;298:934–9.
10. Orens JB, Kazerooni EA, Martinez FJ, et al. The sensitivity of high-resolution CT in detecting idiopathic pulmonary fi brosis proved by open lung biopsy. A prospective study. Chest 1995;108:109–15.
11. Wells A. Clinical usefulness of high resolution computed tomography in cryptogenic fi brosing alveolitis. Thorax 1998;53:1080–7.
12. Lynch DA, David Godwin J, Safrin S, et al. High-resolution computed tomography in idiopathic pulmonary fi brosis: diagnosis and prognosis. Am J Respir Crit Care Med 2005;172:488–93.
13. Aziz ZA, Wells AU, Bateman ED, et al. Interstitial lung disease: effects of thin-section CT on clinical decision making. Radiology 2006;238:725–33.
14. Miller J, Wallace T. Diagnostic thoracic imaging. New York: McGraw-Hill Companies; 2006.
15. Souza CA, Muller NL, Lee KS, et al. Idiopathic interstitial pneumonias: prevalence of mediastinal lymph node enlargement in 206 patients. AJR Am J Roentgenol 2006;186:995–9.
16. Hunninghake GW, Lynch DA, Galvin JR, et al. Radiologic fi ndings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia. Chest 2003;124:1215–23.
17. Noth I, Martinez FJ. Recent advances in idiopathic pulmonary fi brosis. Chest 2007;132:637–50.
18. Flaherty KR, Andrei AC, King TE Jr, et al. Idiopathic interstitial pneumonia: do community and academic phy-sicians agree on diagnosis? Am J Respir Crit Care Med 2007;175:1054–60.
19. Welker L, Jorres RA, Costabel U, Magnussen H. Predictive value of BAL cell differentials in the diagnosis of interstitial lung diseases. Eur Respir J 2004;24:1000–6.
20. Veeraraghavan S, Latsi PI, Wells AU, et al. BAL fi ndings in idiopathic nonspecifi c interstitial pneumonia and usual interstitial pneumonia. Eur Respir J 2003;22:239–44.
21. Osler W. The principles and practice of medicine. New York: Appleton & Co.; 1892.
22. Hamman L, Rich A. Acute diffuse interstitial fi brosis of the lungs. Bull Johns Hopkins Hosp 1944;74:177–212.
23. Collard HR, King TE Jr. Demystifying idiopathic interstitial pneumonia. Arch Intern Med 2003;163:17–29.
24. Liebow A, Carrington C. The interstitial pneumonias, frontiers of pulmonary radiology. New York: Grune and Stratton; 1969.
25. Katzenstein AL, Myers JL. Idiopathic pulmonary fi brosis: clinical relevance of pathologic classifi cation. Am J Respir Crit Care Med 1998;157:1301–15.
26. Flaherty KR, Toews GB, Travis WD, et al. Clinical signifi -cance of histological classifi cation of idiopathic interstitial pneumonia. Eur Respir J 2002;19:275–83.
27. Latsi PI, du Bois RM, Nicholson AG, et al. Fibrotic idiopathic interstitial pneumonia: the prognostic value of longitudinal functional trends. Am J Respir Crit Care Med 2003;168:531–7.
28. Utz JP, Ryu JH, Douglas WW, et al. High short-term mortality following lung biopsy for usual interstitial pneumonia. Eur Respir J 2001;17:175–9.
29. Flaherty KR, Mumford JA, Murray S, et al. Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia. Am J Respir Crit Care Med 2003;168:543–8.
30. Lettieri CJ, Veerappan GR, Helman DL, et al. Outcomes and safety of surgical lung biopsy for interstitial lung disease. Chest 2005;127:1600–5.
31. Kreider ME, Hansen-Flaschen J, Ahmad NN, et al. Complications of video-assisted thoracoscopic lung biopsy in patients with interstitial lung disease. Ann Thorac Surg 2007;83:1140–4.
32. Lee YC, Wu CT, Hsu HH, et al. Surgical lung biopsy for diffuse pulmonary disease: experience of 196 patients. J Thorac Cardiovasc Surg 2005;129:984–90.
33. Hoshikawa Y, Kondo T. [Perioperative lung injury: acute exacerbation of idiopathic pulmonary fi brosis and acute interstitial pneumonia after pulmonary resection]. Nippon Geka Gakkai Zasshi 2004;105:757–62.
34. Yuksel M, Ozyurtkan MO, Bostanci K, et al. Acute exacer-bation of interstitial fi brosis after pulmonary resection. Ann Thorac Surg 2006;82:336–8.
35. Kim DS, Park JH, Park BK, et al. Acute exacerbation of idiopathic pulmonary fi brosis: frequency and clinical features. Eur Respir J 2006;27:143–50.

pulm-crit Interstitial and Fibrotic Lung Diseases — 34
10/08
36. Flaherty KR, King TE Jr, Raghu G, et al. Idiopathic inter-stitial pneumonia: what is the effect of a multidisciplinary approach to diagnosis? Am J Respir Crit Care Med 2004;170:904–10.
37. Coultas DB, Zumwalt RE, Black WC, Sobonya RE. The epidemiology of interstitial lung diseases. Am J Respir Crit Care Med 1994;150:967–72.
38. Raghu G, Weycker D, Edelsberg J, et al. Incidence and prevalence of idiopathic pulmonary fi brosis. Am J Respir Crit Care Med 2006;174:810–6.
39. King TE Jr, Tooze JA, Schwarz MI, et al. Predicting survival in idiopathic pulmonary fi brosis: scoring system and survival model. Am J Respir Crit Care Med 2001;164:1171–81.
40. Baumgartner KB, Samet JM, Stidley CA, et al. Cigarette smoking: a risk factor for idiopathic pulmonary fi brosis. Am J Respir Crit Care Med 1997;155:242–8.
41. Antoniou KM, Hansell DM, Rubens MB, et al. Idiopathic pulmonary fi brosis: outcome in relation to smoking status. Am J Respir Crit Care Med 2008;177:190–4.
42. Alakhras M, Decker PA, Nadrous HF, et al. Body mass index and mortality in patients with idiopathic pulmonary fi brosis. Chest 2007;131:1448–53.
43. Cano NJ, Pichard C, Roth H, et al. C-reactive protein and body mass index predict outcome in end-stage respiratory failure. Chest 2004;126:540–6.
44. Selman M, King TE, Pardo A. Idiopathic pulmonary fi brosis: prevailing and evolving hypotheses about its pathogenesis and implications for therapy. Ann Intern Med 2001;134:136–51.
45. Zuo F, Kaminski N, Eugui E, et al. Gene expression analy-sis reveals matrilysin as a key regulator of pulmonary fi brosis in mice and humans. Proc Natl Acad Sci U S A 2002;99:6292–7.
46. Hunninghake GW, Schwarz MI. Does current knowledge explain the pathogenesis of idiopathic pulmonary fi brosis? A perspective. Proc Am Thorac Soc 2007;4:449–52.
47. Strieter RM. Pathogenesis and natural history of usual interstitial pneumonia: the whole story or the last chapter of a long novel. Chest 2005;128:526S–32S.
48. Noble PW, Homer RJ. Idiopathic pulmonary fi brosis: new insights into pathogenesis. Clin Chest Med 2004;25:749–58, vii.
49. Crystal RG, Bitterman PB, Mossman B, et al. Future research directions in idiopathic pulmonary fi brosis: summary of a National Heart, Lung, and Blood Institute working group. Am J Respir Crit Care Med 2002;166:236–46.
50. Roy SG, Nozaki Y, Phan SH. Regulation of alpha-smooth muscle actin gene expression in myofi broblast differen-tiation from rat lung fi broblasts. Int J Biochem Cell Biol 2001;33:723–34.
51. Ghofrani HA, Wiedemann R, Rose F, et al. Sildenafi l for treatment of lung fi brosis and pulmonary hypertension: a randomised controlled trial. Lancet 2002;360:895–900.
52. Grutters JC, du Bois RM. Genetics of fi brosing lung diseases. Eur Respir J 2005;25:915–27.
53. Hunninghake GW, Zimmerman MB, Schwartz DA, et al. Utility of a lung biopsy for the diagnosis of idiopathic pulmonary fi brosis. Am J Respir Crit Care Med 2001;164:193–6.
54. Lynch DA, Travis WD, Muller NL, et al. Idiopathic interstitial pneumonias: CT features. Radiology 2005;236:10–21.
55. Sumikawa H, Johkoh T, Ichikado K, et al. Usual interstitial pneumonia and chronic idiopathic interstitial pneumonia: analysis of CT appearance in 92 patients. Radiology 2006;241:258–66.
56. Akira M, Yamamoto S, Inoue Y, Sakatani M. High-resolution CT of asbestosis and idiopathic pulmonary fi brosis. AJR Am J Roentgenol 2003;181:163–9.
57. Akira M, Hamada H, Sakatani M, et al. CT fi ndings during phase of accelerated deterioration in patients with idiopathic pulmonary fi brosis. AJR Am J Roentgenol 1997;168:79–83.
58. Panos RJ, Mortenson RL, Niccoli SA, King TE Jr. Clinical deterioration in patients with idiopathic pulmonary fi brosis: causes and assessment. Am J Med 1990;88:396–404.
59. Berbescu EA, Katzenstein AL, Snow JL, Zisman DA. Transbronchial biopsy in usual interstitial pneumonia. Chest 2006;129:1126–31.
60. Agarwal R, Gupta D, Verma JS, et al. Noninvasive estima-tion of clinically asymptomatic pulmonary hypertension in idiopathic pulmonary fi brosis. Indian J Chest Dis Allied Sci 2005;47:267–71.
61. Nadrous HF, Pellikka PA, Krowka MJ, et al. Pulmonary hypertension in patients with idiopathic pulmonary fi brosis. Chest 2005;128:2393–9.
62. Lettieri CJ, Nathan SD, Barnett SD, et al. Prevalence and outcomes of pulmonary arterial hypertension in advanced idiopathic pulmonary fi brosis. Chest 2006;129:746–52.
63. Hamada K, Nagai S, Tanaka S, et al. Signifi cance of pulmo-nary arterial pressure and diffusion capacity of the lung as prognosticator in patients with idiopathic pulmonary fi brosis. Chest 2007;131:650–6.
64. Nathan SD, Shlobin OA, Ahmad S, et al. Serial develop-ment of pulmonary hypertension in patients with idio-pathic pulmonary fi brosis. Respiration 2008;76:288–94.
65. Arcasoy SM, Christie JD, Ferrari VA, et al. Echocardio-graphic assessment of pulmonary hypertension in patients with advanced lung disease. Am J Respir Crit Care Med 2003;167:735–40.
66. Leuchte HH, Neurohr C, Baumgartner R, et al. Brain natriuretic peptide and exercise capacity in lung fi brosis and pulmonary hypertension. Am J Respir Crit Care Med 2004;170:360–5.
67. Leuchte HH, Baumgartner RA, Nounou ME, et al. Brain natriuretic peptide is a prognostic parameter in chronic lung disease. Am J Respir Crit Care Med 2006;173:744–50.
68. Zisman DA, Karlamangla AS, Ross DJ, et al. High-resolution chest CT fi ndings do not predict the presence of pulmonary hypertension in advanced idiopathic pulmonary fi brosis. Chest 2007;132:773–9.
69. Patel NM, Lederer DJ, Borczuk AC, Kawut SM. Pulmo-nary hypertension in idiopathic pulmonary fi brosis. Chest 2007;132:998–1006.
70. Kawut SM, O’Shea MK, Bartels MN, et al. Exercise testing determines survival in patients with diffuse parenchymal lung disease evaluated for lung transplantation. Respir Med 2005;99:1431–9.

pulm-crit Interstitial and Fibrotic Lung Diseases — 35
10/08
71. Whelan TP, Dunitz JM, Kelly RF, et al. Effect of preo-perative pulmonary artery pressure on early survival after lung transplantation for idiopathic pulmonary fi brosis. J Heart Lung Transplant 2005;24:1269–74.
72. Cottin V, Nunes H, Brillet PY, et al. Combined pulmonary fi brosis and emphysema: a distinct underrecognised entity. Eur Respir J 2005;26:586–93.
73. Aduen JF, Zisman DA, Mobin SI, et al. Retrospective study of pulmonary function tests in patients presenting with isolated reduction in single-breath diffusion capacity: implications for the diagnosis of combined obstructive and restrictive lung disease. Mayo Clin Proc 2007;82:48–54.
74. Raghu G. The role of gastroesophageal refl ux in idiopathic pulmonary fi brosis. Am J Med 2003;115 Suppl 3A:60S–4S.
75. Sweet MP, Patti MG, Leard LE, et al. Gastroesophageal refl ux in patients with idiopathic pulmonary fi brosis referred for lung transplantation. J Thorac Cardiovasc Surg 2007;133:1078–84.
76. Tobin RW, Pope CE 2nd, Pellegrini CA, et al. Increased prevalence of gastroesophageal refl ux in patients with idiopathic pulmonary fi brosis. Am J Respir Crit Care Med 1998;158:1804–8.
77. Raghu G, Yang ST, Spada C, et al. Sole treatment of acid gastroesophageal refl ux in idiopathic pulmonary fi brosis: a case series. Chest 2006;129:794–800.
78. Kizer JR, Zisman DA, Blumenthal NP, et al. Association between pulmonary fi brosis and coronary artery disease. Arch Intern Med 2004;164:551–6.
79. Caplan-Shaw CE, Arcasoy SM, Shane E, et al. Osteoporosis in diffuse parenchymal lung disease. Chest 2006;129:140–6.
80. Nathan SD, Barnett SD, Urban BA, et al. Pulmonary embo-lism in idiopathic pulmonary fi brosis transplant recipients. Chest 2003;123:1758–63.
81. Lama VN, Flaherty KR, Toews GB, et al. Prognostic value of desaturation during a 6-minute walk test in idiopathic interstitial pneumonia. Am J Respir Crit Care Med 2003;168:1084–90.
82. Gay SE, Kazerooni EA, Toews GB, et al. Idiopathic pulmo-nary fi brosis: predicting response to therapy and survival. Am J Respir Crit Care Med 1998;157:1063–72.
83. Nicholson AG, Fulford LG, Colby TV, et al. The relation-ship between individual histologic features and disease progression in idiopathic pulmonary fi brosis. Am J Respir Crit Care Med 2002;166:173–7.
84. Enomoto N, Suda T, Kato M, et al. Quantitative analysis of fi broblastic foci in usual interstitial pneumonia. Chest 2006;130:22–9.
85. Lederer DJ, Arcasoy SM, Wilt JS, et al. Six-minute-walk distance predicts waiting list survival in idiopathic pulmonary fi brosis. Am J Respir Crit Care Med 2006;174:659–64.
86. Eaton T, Young P, Milne D, Wells AU. Six-minute walk, maximal exercise tests: reproducibility in fi brotic inter-stitial pneumonia. Am J Respir Crit Care Med 2005;171:1150–7.
87. Flaherty KR, Andrei AC, Murray S, et al. Idiopathic pulmonary fi brosis: prognostic value of changes in physi-ology and six-minute-walk test. Am J Respir Crit Care Med 2006;174:803–9.
88. Hallstrand TS, Boitano LJ, Johnson WC, et al. The timed walk test as a measure of severity and survival in
idiopathic pulmonary fi brosis. Eur Respir J 2005;25:96–103.
89. Flaherty KR, Thwaite EL, Kazerooni EA, et al. Radiological versus histological diagnosis in UIP and NSIP: survival implications. Thorax 2003;58:143–8.
90. Watters LC, King TE, Schwarz MI, et al. A clinical, radio-graphic, and physiologic scoring system for the longitudi-nal assessment of patients with idiopathic pulmonary fi brosis. Am Rev Respir Dis 1986;133:97–103.
91. Wells AU, Desai SR, Rubens MB, et al. Idiopathic pulmo-nary fi brosis: a composite physiologic index derived from disease extent observed by computed tomography. Am J Respir Crit Care Med 2003;167:962–9.
92. Collard HR, King TE Jr, Bartelson BB, et al. Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fi brosis. Am J Respir Crit Care Med 2003;168:538–42.
93. Martinez FJ, Safrin S, Weycker D, et al. The clinical course of patients with idiopathic pulmonary fi brosis. Ann Intern Med 2005;142:963–7.
94. Jegal Y, Kim DS, Shim TS, et al. Physiology is a stronger predictor of survival than pathology in fi brotic interstitial pneumonia. Am J Respir Crit Care Med 2005;171:639–44.
95. King TE Jr, Safrin S, Starko KM, et al. Analyses of effi cacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fi brosis. Chest 2005;127:171–7.
96. Saydain G, Islam A, Afessa B, et al. Outcome of patients with idiopathic pulmonary fi brosis admitted to the inten-sive care unit. Am J Respir Crit Care Med 2002;166:839–42.
97. Collard HR, Moore BB, Flaherty KR, et al. Acute exacerba-tions of idiopathic pulmonary fi brosis. Am J Respir Crit Care Med 2007;176:636–43.
98. Parambil JG, Myers JL, Ryu JH. Histopathologic features and outcome of patients with acute exacerbation of idiopathic pulmonary fi brosis undergoing surgical lung biopsy. Chest 2005;128:3310–5.
99. Kondoh Y, Taniguchi H, Kawabata Y, et al. Acute exacer-bation in idiopathic pulmonary fi brosis. Analysis of clinical and pathologic fi ndings in three cases. Chest 1993;103:1808–12.
100. Churg A, Muller NL, Silva CI, Wright JL. Acute exacerba-tion (acute lung injury of unknown cause) in UIP and other forms of fi brotic interstitial pneumonias. Am J Surg Pathol 2007;31:277–84.
101. Kubo H, Nakayama K, Yanai M, et al. Anticoagulant therapy for idiopathic pulmonary fi brosis. Chest 2005;128:1475–82.
102. Kinder BW, Collard HR, King TE Jr. Anticoagulant therapy and idiopathic pulmonary fi brosis. Chest 2006;130:302–3.
103. Azuma A, Nukiwa T, Tsuboi E, et al. Double-blind, placebo-controlled trial of pirfenidone in patients with idiopathic pulmonary fi brosis. Am J Respir Crit Care Med 2005;171:1040–7.
104. Richeldi L, Davies HR, Ferrara G, Franco F. Corticoste-roids for idiopathic pulmonary fi brosis. Cochrane Database Syst Rev 2003;CD002880.
105. Turner-Warwick M, Burrows B, Johnson A. Cryptogenic fi brosing alveolitis: response to corticosteroid treatment and its effect on survival. Thorax 1980;35:593–9.

pulm-crit Interstitial and Fibrotic Lung Diseases — 36
10/08
106. Walter N, Collard HR, King TE Jr. Current perspectives on the treatment of idiopathic pulmonary fi brosis. Proc Am Thorac Soc 2006;3:330–8.
107. Shah NR, Noble P, Jackson RM, et al. A critical assessment of treatment options for idiopathic pulmonary fi brosis. Sarcoidosis Vasc Diffuse Lung Dis 2005;22:167–74.
108. Raghu G, Depaso WJ, Cain K, et al. Azathioprine combined with prednisone in the treatment of idiopathic pulmonary fi brosis: a prospective double-blind, random-ized, placebo-controlled clinical trial. Am Rev Respir Dis 1991;144:291–6.
109. Demedts M, Behr J, Buhl R, et al. High-dose acetylcysteine in idiopathic pulmonary fi brosis. N Engl J Med 2005;353:2229–42.
110. Davies HR, Richeldi L, Walters EH. Immunomodulatory agents for idiopathic pulmonary fi brosis. Cochrane Database Syst Rev 2003;CD003134.
111. Flaherty KR, Toews GB, Lynch JP 3rd, et al. Steroids in idiopathic pulmonary fi brosis: a prospective assessment of adverse reactions, response to therapy, and survival. Am J Med 2001;110:278–82.
112. Lynch JP 3rd, McCune WJ. Immunosuppressive and cytotoxic pharmacotherapy for pulmonary disorders. Am J Respir Crit Care Med 1997;155:395–420.
113. Malik SW, Myers JL, DeRemee RA, Specks U. Lung toxic-ity associated with cyclophosphamide use. Two distinct patterns. Am J Respir Crit Care Med 1996;154:1851–6.
114. Bouros D, Antoniou KM. Current and future therapeutic approaches in idiopathic pulmonary fi brosis. Eur Respir J 2005;26:693–702.
115. Grgic A, Lausberg H, Heinrich M, et al. Progression of fi brosis in usual interstitial pneumonia: serial evaluation of the native lung after single lung transplantation. Respiration 2008;76:139–45.
116. Wahidi MM, Ravenel J, Palmer SM, McAdams HP. Pro-gression of idiopathic pulmonary fi brosis in native lungs after single lung transplantation. Chest 2002;121:2072–6.
117. Ziesche R, Hofbauer E, Wittmann K, et al. A preliminary study of long-term treatment with interferon gamma-1b and low-dose prednisolone in patients with idiopathic pulmonary fi brosis. N Engl J Med 1999;341:1264–9.
118. Raghu G, Brown KK, Bradford WZ, et al. A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fi brosis. N Engl J Med 2004;350:125–33.
119. King TE Jr, Behr J, Brown KK, et al. BUILD-1: a random-ized placebo-controlled trial of bosentan in idiopathic pulmonary fi brosis. Am J Respir Crit Care Med 2008;177:75–81.
120. Behr J, Maier K, Degenkolb B, et al. Antioxidative and clinical effects of high-dose N-acetylcysteine in fi brosing alveolitis. Adjunctive therapy to maintenance immuno-suppression. Am J Respir Crit Care Med 1997;156:1897–901.
121. Olschewski H, Ghofrani HA, Walmrath D, et al. Inhaled prostacyclin and iloprost in severe pulmonary hyperten-sion secondary to lung fi brosis. Am J Respir Crit Care Med 1999;160:600–7.
122. Collard HR, Anstrom KJ, Schwarz MI, Zisman DA. Silde-nafi l improves walk distance in idiopathic pulmonary fi brosis. Chest 2007;131:897–9.
123. Sitbon O, Humbert M, Jais X, et al. Long-term response to calcium channel blockers in idiopathic pulmonary arterial hypertension. Circulation 2005;111:3105–11.
124. Thabut G, Mal H, Castier Y, et al. Survival benefi t of lung transplantation for patients with idiopathic pulmonary fi brosis. J Thorac Cardiovasc Surg 2003;126:469–75.
125. Katzenstein AL, Fiorelli RF. Nonspecifi c interstitial pneumonia/fi brosis. Histologic features and clinical signifi cance. Am J Surg Pathol 1994;18:136–47.
126. Travis WD, Matsui K, Moss J, Ferrans VJ. Idiopathic non-specifi c interstitial pneumonia: prognostic signifi cance of cellular and fi brosing patterns: survival comparison with usual interstitial pneumonia and desquamative interstitial pneumonia. Am J Surg Pathol 2000;24:19–33.
127. Martinez FJ. Idiopathic interstitial pneumonias: usual interstitial pneumonia versus nonspecifi c interstitial pneumonia. Proc Am Thorac Soc 2006;3:81–95.
128. Thomas AQ, Lane K, Phillips J 3rd, et al. Heterozygosity for a surfactant protein C gene mutation associated with usual interstitial pneumonitis and cellular nonspecifi c interstitial pneumonitis in one kindred. Am J Respir Crit Care Med 2002;165:1322–8.
129. Stevens PA, Pettenazzo A, Brasch F, et al. Nonspecifi c interstitial pneumonia, alveolar proteinosis, and abnormal proprotein traffi cking resulting from a spontaneous muta-tion in the surfactant protein C gene. Pediatr Res 2005;57:89–98.
130. Johkoh T, Muller NL, Colby TV, et al. Nonspecifi c intersti-tial pneumonia: correlation between thin-section CT fi nd-ings and pathologic subgroups in 55 patients. Radiology 2002;225:199–204.
131. Hartman TE, Swensen SJ, Hansell DM, et al. Nonspecifi c interstitial pneumonia: variable appearance at high-resolution chest CT. Radiology 2000;217:701–5.
132. Kim EY, Lee KS, Chung MP, et al. Nonspecifi c interstitial pneumonia with fi brosis: serial high-resolution CT fi nd-ings with functional correlation. AJR Am J Roentgenol 1999;173:949–53.
133. Silva CI, Muller NL, Hansell DM, et al. Nonspecifi c interstitial pneumonia and idiopathic pulmonary fi brosis: changes in pattern and distribution of disease over time. Radiology 2008 Apr;247:251–9.
134. Screaton NJ, Hiorns MP, Lee KS, et al. Serial high resolu-tion CT in non-specifi c interstitial pneumonia: prognostic value of the initial pattern. Clin Radiol 2005;60:96–104.
135. Elliot TL, Lynch DA, Newell JD Jr, et al. High-resolution computed tomography features of nonspecifi c interstitial pneumonia and usual interstitial pneumonia. J Comput Assist Tomogr 2005;29:339–45.
136. Kim DS, Collard HR, King TE Jr. Classifi cation and natural history of the idiopathic interstitial pneumonias. Proc Am Thorac Soc 2006;3:285–92.
137. MacDonald SL, Rubens MB, Hansell DM, et al. Nonspe-cifi c interstitial pneumonia and usual interstitial pneumo-nia: comparative appearances at and diagnostic accuracy of thin-section CT. Radiology 2001;221:600–5.
138. Flaherty KR, Travis WD, Colby TV, et al. Histopathologic variability in usual and nonspecifi c interstitial pneumo-nias. Am J Respir Crit Care Med 2001;164:1722–7.
139. Monaghan H, Wells AU, Colby TV, et al. Prognostic implications of histologic patterns in multiple surgical

pulm-crit Interstitial and Fibrotic Lung Diseases — 37
10/08
lung biopsies from patients with idiopathic interstitial pneumonias. Chest 2004;125:522–6.
140. Nicholson AG, Addis BJ, Bharucha H, et al. Inter-observer variation between pathologists in diffuse parenchymal lung disease. Thorax 2004;59:500–5.
141. Park IN, Kim DS, Shim TS, et al. Acute exacerbation of interstitial pneumonia other than idiopathic pulmonary fi brosis. Chest 2007;132:214–20.
142. Yang IV, Burch LH, Steele MP, et al. Gene expression profi ling of familial and sporadic interstitial pneumonia. Am J Respir Crit Care Med 2007;175:45–54.
143. Selman M, Pardo A, Barrera L, et al. Gene expression profi les distinguish idiopathic pulmonary fi brosis from hypersensitivity pneumonitis. Am J Respir Crit Care Med 2006;173:188–98.
144. Parambil JG, Myers JL, Aubry MC, Ryu JH. Causes and prognosis of diffuse alveolar damage diagnosed on surgical lung biopsy. Chest 2007;132:50–7.
145. Katzenstein AL, Myers JL, Mazur MT. Acute interstitial pneumonia. A clinicopathologic, ultrastructural, and cell kinetic study. Am J Surg Pathol 1986;10:256–67.
146. Bouros D, Nicholson AC, Polychronopoulos V, du Bois RM. Acute interstitial pneumonia. Eur Respir J 2000;15:412–8.
147. Vourlekis JS. Acute interstitial pneumonia. Clin Chest Med 2004;25:739–47, vii.
148. Olson J, Colby TV, Elliott CG. Hamman-Rich syndrome revisited. Mayo Clin Proc 1990;65:1538–48.
149. Primack SL, Hartman TE, Ikezoe J, et al. Acute interstitial pneumonia: radiographic and CT fi ndings in nine patients. Radiology 1993;188:817–20.
150. Johkoh T, Muller NL, Taniguchi H, et al. Acute interstitial pneumonia: thin-section CT fi ndings in 36 patients. Radiology 1999;211:859–63.
151. Ichikado K, Johkoh T, Ikezoe J, et al. Acute interstitial pneumonia: high-resolution CT fi ndings correlated with pathology. AJR Am J Roentgenol 1997;168:333–8.
152. Ichikado K, Suga M, Muller NL, et al. Acute interstitial pneumonia: comparison of high-resolution computed tomography fi ndings between survivors and nonsurvi-vors. Am J Respir Crit Care Med 2002;165:1551–6.
153. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. The Acute Respiratory Distress Syndrome Network. N Engl J Med 2000;342:1301–8.
154. Suh GY, Kang EH, Chung MP, et al. Early intervention can improve clinical outcome of acute interstitial pneumonia. Chest 2006;129:753–61.
155. Meduri GU, Headley AS, Golden E, et al. Effect of pro-longed methylprednisolone therapy in unresolving acute respiratory distress syndrome: a randomized controlled trial. JAMA 1998;280:159–65.
156. Meduri GU, Golden E, Freire AX, et al. Methylpred nisolone infusion in early severe ARDS: results of a randomized controlled trial. Chest 2007;131:954–63.
157. Quefatieh A, Stone CH, DiGiovine B, et al. Low hospital mortality in patients with acute interstitial pneumonia. Chest 2003;124:554–9.
158. Niewoehner DE, Kleinerman J, Rice DB. Pathologic changes in the peripheral airways of young cigarette smokers. N Engl J Med 1974;291:755–8.
159. Liebow AA, Steer A, Billingsley JG. Desquamative interstitial pneumonia. Am J Med 1965;39:369–404.
160. Carrington CB, Gaensler EA, Coutu RE, et al. Natural history and treated course of usual and desquamative interstitial pneumonia. N Engl J Med 1978;298:801–9.
161. Ryu JH, Myers JL, Capizzi SA, et al. Desquamative inter-stitial pneumonia and respiratory bronchiolitis-associated interstitial lung disease. Chest 2005;127:178–84.
162. Yousem SA, Colby TV, Gaensler EA. Respiratory bronchi-olitis-associated interstitial lung disease and its relation-ship to desquamative interstitial pneumonia. Mayo Clin Proc 1989;64:1373–80.
163. Nogee LM, Dunbar AE 3rd, Wert SE, et al. A mutation in the surfactant protein C gene associated with familial interstitial lung disease. N Engl J Med 2001;344:573–9.
164. Iskandar SB, McKinney LA, Shah L, et al. Desquamative interstitial pneumonia and hepatitis C virus infection: a rare association. South Med J 2004;97:890–3.
165. Moon J, du Bois RM, Colby TV, et al. Clinical signifi cance of respiratory bronchiolitis on open lung biopsy and its relationship to smoking related interstitial lung disease. Thorax 1999;54:1009–14.
166. Portnoy J, Veraldi KL, Schwarz MI, et al. Respiratory bronchiolitis-interstitial lung disease: long-term outcome. Chest 2007;131:664–71.
167. Park JS, Brown KK, Tuder RM, et al. Respiratory bronchiolitis-associated interstitial lung disease: radiologic features with clinical and pathologic correlation. J Comput Assist Tomogr 2002;26:13–20.
168. Myers JL, Veal CF Jr, Shin MS, Katzenstein AL. Respira-tory bronchiolitis causing interstitial lung disease. A clinicopathologic study of six cases. Am Rev Respir Dis 1987;135:880–4.
169. Heyneman LE, Ward S, Lynch DA, et al. Respiratory bron-chiolitis, respiratory bronchiolitis-associated interstitial lung disease, and desquamative interstitial pneumonia: different entities or part of the spectrum of the same disease process? AJR Am J Roentgenol 1999;173:1617–22.
170. Fraig M, Shreesha U, Savici D, Katzenstein AL. Respira-tory bronchiolitis: a clinicopathologic study in current smokers, ex-smokers, and never-smokers. Am J Surg Pathol 2002;26:647–53.
171. Akira M, Yamamoto S, Hara H, et al. Serial computed tomographic evaluation in desquamative interstitial pneumonia. Thorax 1997;52:333–7.
172. Davison AG, Heard BE, McAllister WA, Turner-Warwick ME. Cryptogenic organizing pneumonitis. Q J Med 1983;52:382–94.
173. Epler GR, Colby TV, McLoud TC, et al. Bronchiolitis obliterans organizing pneumonia. N Engl J Med 1985;312:152–8.
174. Epler GR. Bronchiolitis obliterans organizing pneumonia. Arch Intern Med 2001;161:158–64.
175. Colby TV. Pathologic aspects of bronchiolitis obliterans organizing pneumonia. Chest 1992;102:38S–43S.
176. Katzenstein AL. Katzenstein and Askin’s surgical pathol-ogy of non-neoplastic lung disease. 3rd ed. Philadelphia: WB Saunders; 1997.
177. King TE Jr, Mortenson RL. Cryptogenic organizing pneumonitis. The North American experience. Chest 1992;102:8S–13S.

pulm-crit Interstitial and Fibrotic Lung Diseases — 38
10/08
178. Cordier JF. Cryptogenic organising pneumonia. Eur Respir J 2006;28:422–46.
179. Cordier JF, Loire R, Brune J. Idiopathic bronchiolitis oblit-erans organizing pneumonia. Defi nition of characteristic clinical profi les in a series of 16 patients. Chest 1989;96:999–1004.
180. Muller NL, Staples CA, Miller RR. Bronchiolitis obliterans organizing pneumonia: CT features in 14 patients. AJR Am J Roentgenol 1990;154:983–7.
181. Arakawa H, Kurihara Y, Niimi H, et al. Bronchiolitis obliterans with organizing pneumonia versus chronic eosinophilic pneumonia: high-resolution CT fi ndings in 81 patients. AJR Am J Roentgenol 2001;176:1053–8.
182. Epstein DM, Bennett MR. Bronchiolitis obliterans organiz-ing pneumonia with migratory pulmonary infi ltrates. AJR Am J Roentgenol 1992;158:515–7.
183. Lee KS, Kullnig P, Hartman TE, Muller NL. Cryptogenic organizing pneumonia: CT fi ndings in 43 patients. AJR Am J Roentgenol 1994;162:543–6.
184. Ujita M, Renzoni EA, Veeraraghavan S, et al. Organizing pneumonia: perilobular pattern at thin-section CT. Radiology 2004;232:757–61.
185. Heller I, Biner S, Isakov A, et al. TB or not TB: cavitary bronchiolitis obliterans organizing pneumonia mimicking pulmonary tuberculosis. Chest 2001;120:674–8.
186. Poletti V, Cazzato S, Minicuci N, et al. The diagnostic value of bronchoalveolar lavage and transbronchial lung biopsy in cryptogenic organizing pneumonia. Eur Respir J 1996;9:2513–6.
187. Lazor R, Vandevenne A, Pelletier A, et al. Cryptogenic organizing pneumonia. Characteristics of relapses in a series of 48 patients. The Groupe d’Etudes et de Recherche sur les Maladles « Orphelines » Pulmonaires (GERM« O »P). Am J Respir Crit Care Med 2000;162:571–7.
188. Stover DE, Mangino D. Macrolides: a treatment alternative for bronchiolitis obliterans organizing pneumonia? Chest 2005;128:3611–7.
189. Ichikawa Y, Ninomiya H, Katsuki M, et al. Low-dose/long-term erythromycin for treatment of bronchiolitis obliterans organizing pneumonia (BOOP). Kurume Med J 1993;40:65–7.
190. Kradin RL, Young RH, Kradin LA, Mark EJ. Immunoblas-tic lymphoma arising in chronic lymphoid hyperplasia of the pulmonary interstitium. Cancer 1982;50:1339–43.
191. Teruya-Feldstein J, Temeck BK, Sloas MM, et al. Pulmo-nary malignant lymphoma of mucosa-associated lymphoid tissue (MALT) arising in a pediatric HIV-positive patient. Am J Surg Pathol 1995;19:357–63.
192. Cha SI, Fessler MB, Cool CD, et al. Lymphoid interstitial pneumonia: clinical features, associations and prognosis. Eur Respir J 2006;28:364–9.
193. Johkoh T, Muller NL, Pickford HA, et al. Lymphocytic interstitial pneumonia: thin-section CT fi ndings in 22 patients. Radiology 1999;212:567–72.
194. Silva CI, Flint JD, Levy RD, Muller NL. Diffuse lung cysts in lymphoid interstitial pneumonia: high-resolution CT and pathologic fi ndings. J Thorac Imaging 2006;21:241–4.
195. Ichikawa Y, Kinoshita M, Koga T, et al. Lung cyst forma-tion in lymphocytic interstitial pneumonia: CT features. J Comput Assist Tomogr 1994;18:745–8.
196. Koss MN, Hochholzer L, Langloss JM, et al. Lymphoid interstitial pneumonia: clinicopathological and immuno-pathological fi ndings in 18 cases. Pathology 1987;19:178–85.
197. Peabody JW, Peabody JW Jr, Hayes EW, Hayes EW Jr. Idiopathic pulmonary fi brosis; its occurrence in identical twin sisters. Dis Chest 1950;18:330–44.
198. Steele MP, Speer MC, Loyd JE, et al. Clinical and pathologic features of familial interstitial pneumonia. Am J Respir Crit Care Med 2005;172:1146–52.
199. Armanios MY, Chen JJ, Cogan JD, et al. Telomerase mutations in families with idiopathic pulmonary fi brosis. N Engl J Med 2007;356:1317–26.
200. Hamvas A, Nogee LM, White FV, et al. Progressive lung disease and surfactant dysfunction with a deletion in surfactant protein C gene. Am J Respir Cell Mol Biol 2004;30:771–6.
201. Chibbar R, Shih F, Baga M, et al. Nonspecifi c interstitial pneumonia and usual interstitial pneumonia with muta-tion in surfactant protein C in familial pulmonary fi brosis. Mod Pathol 2004;17:973–80.
202. Mulugeta S, Nguyen V, Russo SJ, et al. A surfactant protein C precursor protein BRICHOS domain mutation causes endoplasmic reticulum stress, proteasome dysfunc-tion, and caspase 3 activation. Am J Respir Cell Mol Biol 2005;32:521–30.
203. Selman M, Lin HM, Montano M, et al. Surfactant protein A and B genetic variants predispose to idiopathic pulmonary fi brosis. Hum Genet 2003;113:542–50.
204. Lawson WE, Grant SW, Ambrosini V, et al. Genetic muta-tions in surfactant protein C are a rare cause of sporadic cases of IPF. Thorax 2004;59:977–80.
205. Markart P, Ruppert C, Wygrecka M, et al. Surfactant pro-tein C mutations in sporadic forms of idiopathic interstitial pneumonias. Eur Respir J 2007;29:134–7.
206. Dokal I. Dyskeratosis congenita in all its forms. Br J Haematol 2000;110:768–79.
207. Tsakiri KD, Cronkhite JT, Kuan PJ, et al. Adult-onset pulmonary fi brosis caused by mutations in telomerase. Proc Natl Acad Sci U S A 2007;104:7552–7.
208. Morla M, Busquets X, Pons J, et al. Telomere shortening in smokers with and without COPD. Eur Respir J 2006;27:525–8.
209. Lee HL, Ryu JH, Wittmer MH, et al. Familial idiopathic pulmonary fi brosis: clinical features and outcome. Chest 2005;127:2034–41.
Acknowledgments
The authors gratefully acknowledge the contributions of Drs. Thomas Sporn and Santiago Martinez for providing pathology and radiology fi gures, respectively.