
Article 121 ofthe 1982 Law ofthe Sea Convention And The Maritime ...

Influence of the Extent of the Zone at Risk on theEffectiveness of Drugs in Reducing Infarct Size
LAIR G.T. RIBEIRO, M.D., WAI-MAN CHEUNG, M.S., AND PETER R. MAROKO, M.D.
SUMMARY The goal of this study was to examine whether the effectiveness of a drug in protectingischemic myocardium depends on the size of the hypoperfused zone (the area at risk) measured immediatelyafter coronary artery occlusion (CAO). Methoxy-verapamil (D600), a potent calcium antagonist, was usedto test this hypothesis. In 68 dogs, 1 minute after CAO, 8 mCi of technetium-99m-labeled albuminmicrospheres were injected into the left atrium for later assessment of the hypoperfused zone by autoradiog-raphy. Eighteen dogs were treated with D600 (0.8 mg/kg as a bolus 15 minutes after CAO and 0.2 mg/kg/hour as a continuous infusion for 6 hours). After 6 hours, the hearts were excised and the left ventricles cutinto 3-mm-thick slices and stained with triphenyltetrazolium chloride. The extent of myocardial damagewas measured by planimetry of the unstained areas. Thereafter, the same slices were autoradiographed andthe extent of the hypoperfused zones measured by planimetry of the "cold spots."Both the treated and control dogs were classified according to the amount of the left ventricle that was
hypoperfused: small (< 25%), medium (25-30%), and large (> 30%). In control dogs with small, mediumand large hypoperfused zones, the percentages of the hypoperfused zone that evolved to infarction were 95.9+ 3.5% (mean ± SEM), 90.8 3.5%, and 93.1 ± 2.6%, respectively; in the D600-treated dogs, 31.9 ±
8.3%, 53.8 ± 3.0%, and 61.3 9.2%, respectively. Thus, the dogs with the smallest areas at risk had themost extensive reduction in damage (67%); the effectiveness of treatment was intermediate in those withmedium areas at risk (41%) and treatment had the least effect in those with the largest area at risk (34%).Thus, the size of the area at risk, determined in vivo immediately after CAO, is an important factor indetermining the effectiveness of a drug in reducing myocardial damage.
NUMEROUS INTERVENTIONS are effective in re-ducing the extent of myocardial damage after experi-mental coronary artery occlusion. '-5 However, it is notknown whether, besides the beneficial properties ofthe intervention, the degree of effectiveness dependsupon the initial size of the area at risk of infarction,i.e., the hypoperfused zone (HZ). The goal of thisinvestigation was to determine whether methoxy-vera-pamil (D600), a potent calcium antagonist,6"'reducesmyocardial damage to the same extent in areas of hy-poperfusion of different magnitudes. The area of hypo-perfusion was determined by a recently developedtechnique that has the advantage of assessing the extentof the HZ immediately after coronary artery occlusion,in vivo,8 permitting evaluation of the extent of the HZbefore intervention and under the actual conditions ofcollateral blood flow.9
MethodsSixty-eight mongrel dogs that weighed 17-22 kg
were anesthetized with sodium thiamylal, endotra-cheally intubated, and ventilated with room air using aHarvard respirator. ECGs (lead aVF) and systemic ar-terial pressures through a polyethylene cannula in theleft carotid artery (Statham P23Db pressure trans-ducer) were recorded continuously throughout the ex-periments (Gould Instruments). The chest was openedin the fifth left intercostal space and the heart wassuspended in a pericardial cradle. A polyethylene cath-eter was placed in the left atrium through its appendageto inject radiolabeled microspheres. The left anteriordescending coronary artery was dissected free from the
From the Deborah Cardiovascular Research Institute, Browns Mills,New Jersey.
Address for correspondence: Peter R. Maroko, M.D., Deborah Car-diovascular Research Institute, Browns Mills, New Jersey 08015.
Received July 27, 1981; revision accepted September 1, 1981.Circulation 66, No. 1, 1982.
adjacent tissue and occluded permanently with a silksuture.
To assess the zone of hypoperfusion, 2 x 106 highlyradioactive (8 mCi) albumin microspheres, 20 u indiameter (3M Company), were injected into the leftatrium 1 minute after coronary artery occlusion.8 9
Fifteen minutes after occlusion, the dogs were ran-domized into two groups, 50 to a control group and 18to a D600-treated group. In the latter, D600 was ad-ministered intravenously: 0.8 mg/kg as a bolus, fol-lowed by a continuous infusion of 0.2 mg/kg/hour until6 hours after coronary artery occlusion.
Six hours after coronary artery occlusion, the dogswere killed and the left ventricle (LV) was dissectedfree from all other structures (i.e., the free wall of theright ventricle, atria, aorta and valves). The LV wasfrozen at - 70°C for 30 minutes and was then cut into20-25 3-mm-thick slices from apex to base. The sliceswere incubated in a 1% solution of triphenyltetrazo-lium chloride (TTC, Sigma Chemicals) for 10 minutesat 37°C. The normal tissue stained dark red and thedamaged tissue pale yellow. A transparent plasticsheet was placed over the slices, and their contours andthose of the yellow and red areas were traced onto theplastic. The total areas of the slices and the areas ofdamaged myocardium were calculated by planimetry(Apple IL computer). Thereafter, the extent of the HZwas determined on the same slices. The slices wereplaced on a sheet of high-speed x-ray film (Cronex 4,E.I. DuPont) and image contrast was obtained withsensitive, medium-contrast enhancing screens. Thefilm was exposed for 13 hours and developed (X-omatautomatic processor). To identify the border, the sameslices were exposed to a "soft" x-ray (25kVp-100mA) and superimposed on the autoradiographs. TheHZs (cold spots) were white, and the perfused areas(hot spots) were black (fig. 1). The contours of theseimages were transferred to a plastic overlay, and the
181
by guest on April 27, 2018
http://circ.ahajournals.org/D
ownloaded from

VOL 66, No 1, JULY 1982
FIGURE 1. (left) Autoradiograph of a representative myocardial slice. The black area (hot spot) indicates the perjhUsed myocardiumand the white area (cold spot), which is not well defined, indicates the hvpoperfused myocardium. (right) The same autoradiography,but with 'soft x-ray" of the slice superimposed. The cold spot can be easily delineated.
total areas of the slices and the HZs were calculated byplanimetry (Apple II computer).The following measurements were calculated: (1)
The percentage of the LV that showed myocardialdamage by TTC staining. This zone is called infarctsize (IS) and is expressed as a percentage of the LV. (2)The percentage of the LV that was initially hypoper-fused as determined by autoradiography. This zone,the HZ, is expressed as a percentage of LV. (3) Thepercentage of the HZ that evolved to infarction. Thiswas calculated by dividing IS by HZ and multiplyingby 100. This represents the percentage of the area thatwas at risk because of reduced blood flow that actuallyevolved to myocardial tissue injury.The weights of the IS and HZ were also calculated
ponderally, using the weight of the LV and multiplyingit by the IS and HZ, respectively.The dogs were then classified according to the ex-
tent of the HZ: those with initial small, medium andlarge HZs (< 25, 25-30% and > 30% of the LV). Thepercentage of the HZ that evolved to infarction wasanalyzed in each of the three classes both in the controland the D600-treated dogs. Thereafter, this index (IS/HZ x 100) was compared between the treated andcontrols of each class; thus, the effectiveness of treat-ment could be assessed by calculating the ratio IS/HZx 100 for the treated dogs and dividing it by the sameratio for the corresponding class of control dogs:
(IS treated IS control
HZ treated HZ controlx 100
The resulting number is the percent reduction of the ex-tent of damage (as normalized by the zone at risk) result-ing from treatment in each class. The percent of reductionin IS was examined also as a continuous function of theHZ.
Comparisons between values obtained in the samedogs were made using a paired t test, and between treatedand control dogs by t test for group observations. Analy-sis of variance was used to compare values among differ-ent subgroups.10 The Fisher exact test was used forevaluation of mortality. I The results are presented asmean ± SEM.
ResultsThe HZs created by coronary artery occlusions in
both treated and control animals were similar in magni-tude. The HZ 1 minute after coronary artery occlusionwas 26.2 ± 1.3% of the LV in the controls and 26.7 ±2.3% of the LV in the treated dogs, showing thatocclusion resulted in comparable areas at risk. Heartrate and mean systemic arterial pressure were similarin both groups 15 minutes after coronary artery occlu-sion and just before administration of D600 in thetreated group (table 1). Therefore, before treatmentstarted, the two groups were similar by the size of area atrisk and by the measured hemodynamic variables.
In the control group, mean systemic arterial pressuredid not change, while heart rate increased 6 hours afterocclusion, by an average of 21 beats/min. In contrast,in the D600-treated group, mean arterial pressure fellby an average of about 16 mm Hg and heart rateslightly decreased (NS). Thus, in the treated dogs,both mean arterial pressure and heart rate were signifi-cantly lower than in the control dogs (table 1).The incidence of death from ventricular fibrillation
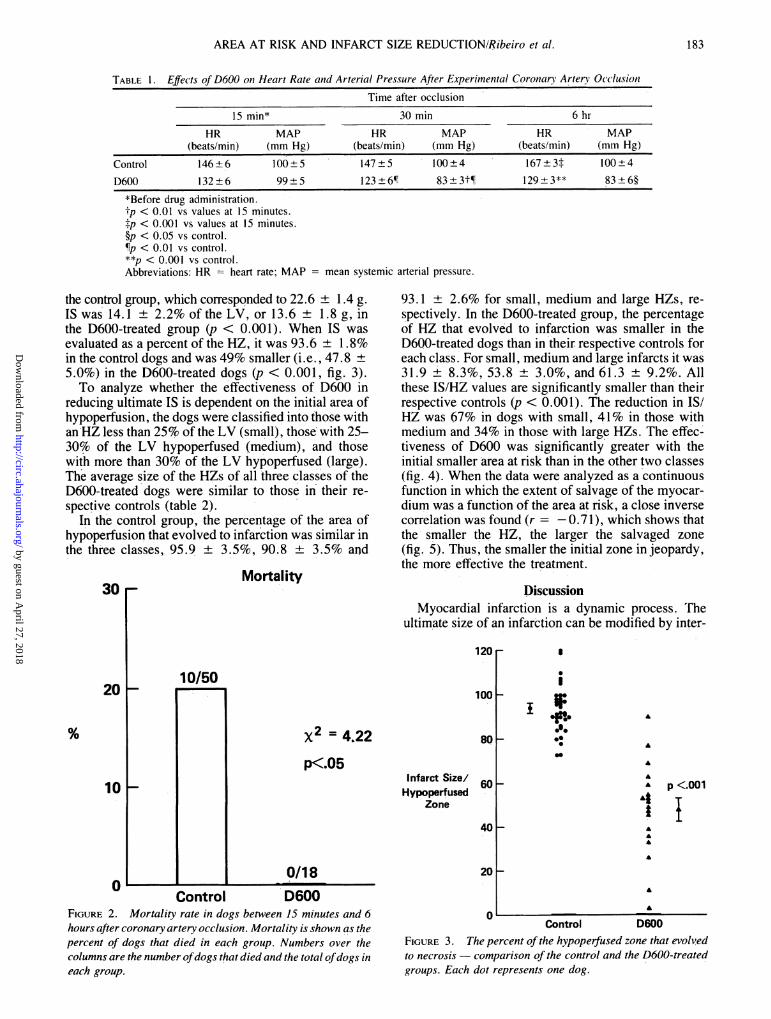
from 15 minutes to 6 hours after coronary artery occlu-sion was 20% (10 of 50 dogs) in the control group and0% in the D600-treated group (X2 = 4.22, p K 0.05)(fig. 2).
IS, determined by planimetry of slices stained withTTC, as a percentage of the LV, was 24.4 ± 0.8% in
12 CIRCULATION
by guest on April 27, 2018
http://circ.ahajournals.org/D
ownloaded from
AREA AT RISK AND INFARCT SIZE REDUCTIONIRibeiro et al.
TABIE 1. Effects of D600 on Heart Rate and Arterial Pressure After Experimental Coroncarv Artery Occlusion
Time after occlusion
15 min* 30 min 6 hr
HR MAP HR MAP HR MAP(beats/min) (mm Hg) (beats/min) (mm Hg) (beats/min) (mm Hg)
Control 146±6 100±5 147±5 100±4 167 3t 100±4
D600 132±6 99±5 123±611 83±3t¶ 129±3** 83±6§
*Before drug administration.tp < 0.01 vs values at 15 minutes.tp < 0.001 vs values at 15 minutes.§p < 0.05 vs control.¶p < 0.01 vs control.**p < 0.001 vs control.Abbreviations: HR = heart rate; MAP = mean systemic arterial pressure.
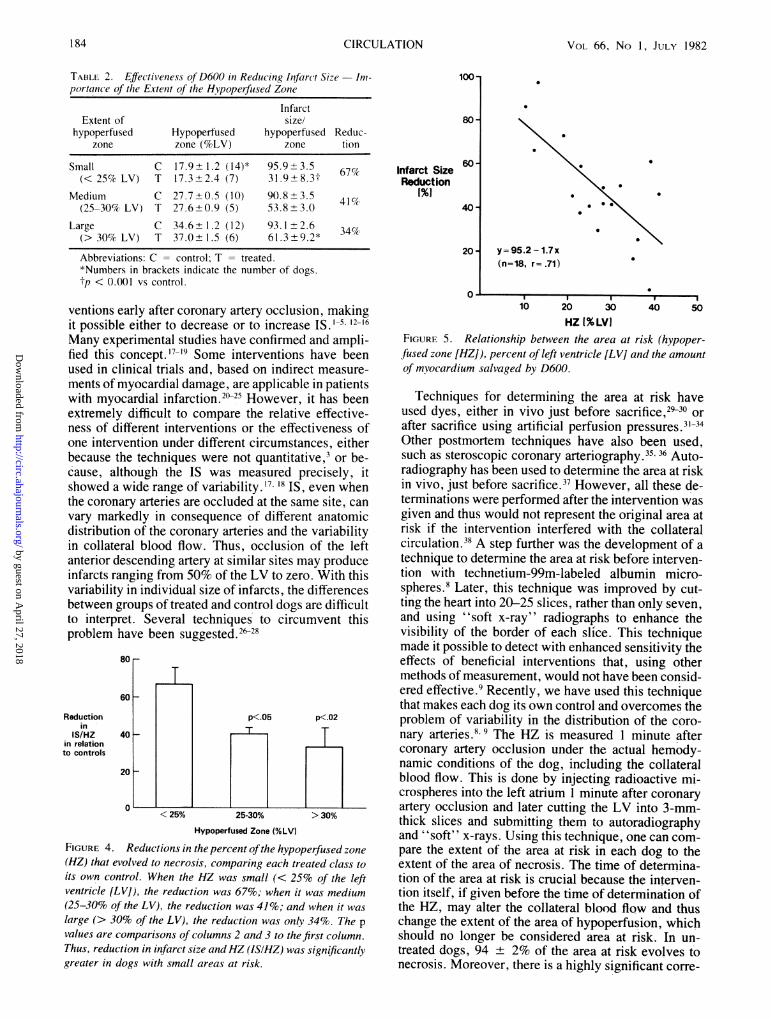
the control group, which corresponded to 22.6 + 1.4 g.IS was 14.1 + 2.2% of the LV, or 13.6 + 1.8 g, inthe D600-treated group (p < 0.001). When IS wasevaluated as a percent of the HZ, it was 93.6 ± 1.8%in the control dogs and was 49% smaller (i.e., 47.8 ±5.0%) in the D600-treated dogs (p < 0.001, fig. 3).To analyze whether the effectiveness of D600 in
reducing ultimate IS is dependent on the initial area ofhypoperfusion, the dogs were classified into those withan'HZ less than 25% of the LV (small), those' with 25-30% of the LV hypoperfused (medium), and thosewith more than 30% of the LV hypoperfused (large).The average size of the HZs of all three classes of theD600-treated dogs were similar to those in their re-spective controls (table 2).
In the control group, the percentage of the area ofhypoperfusion that evolved to infarction was similar inthe three classes, 95.9 + 3.5%, 90.8 ± 3.5% and
Mortality30 -
20H
10 F-
0
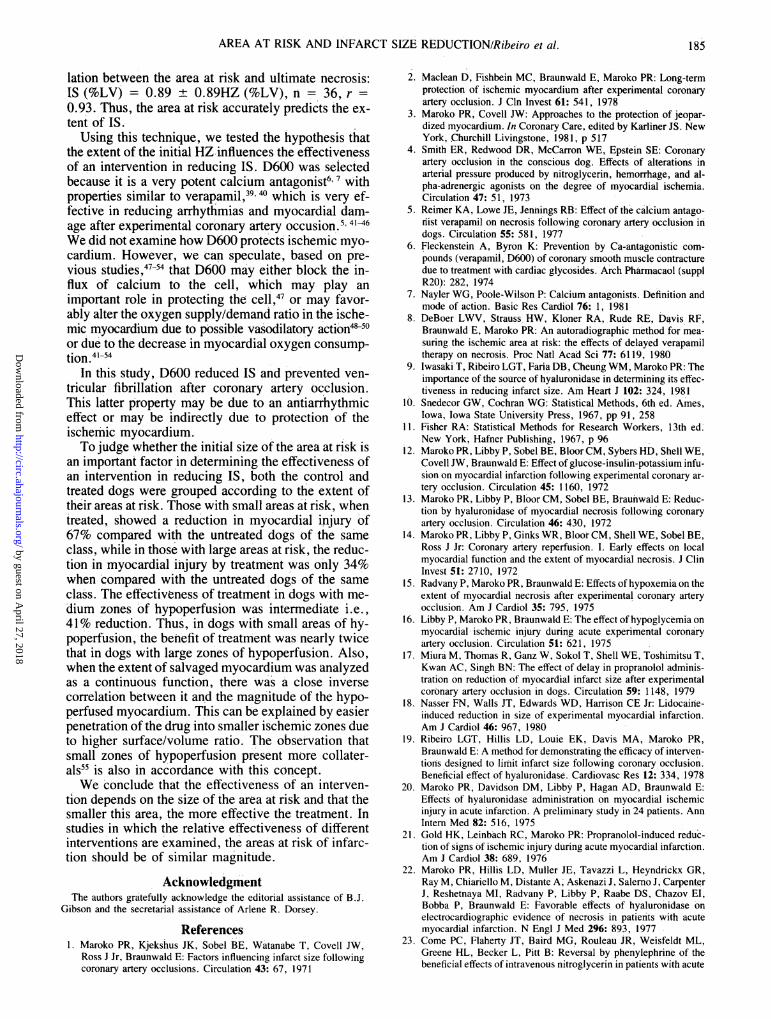
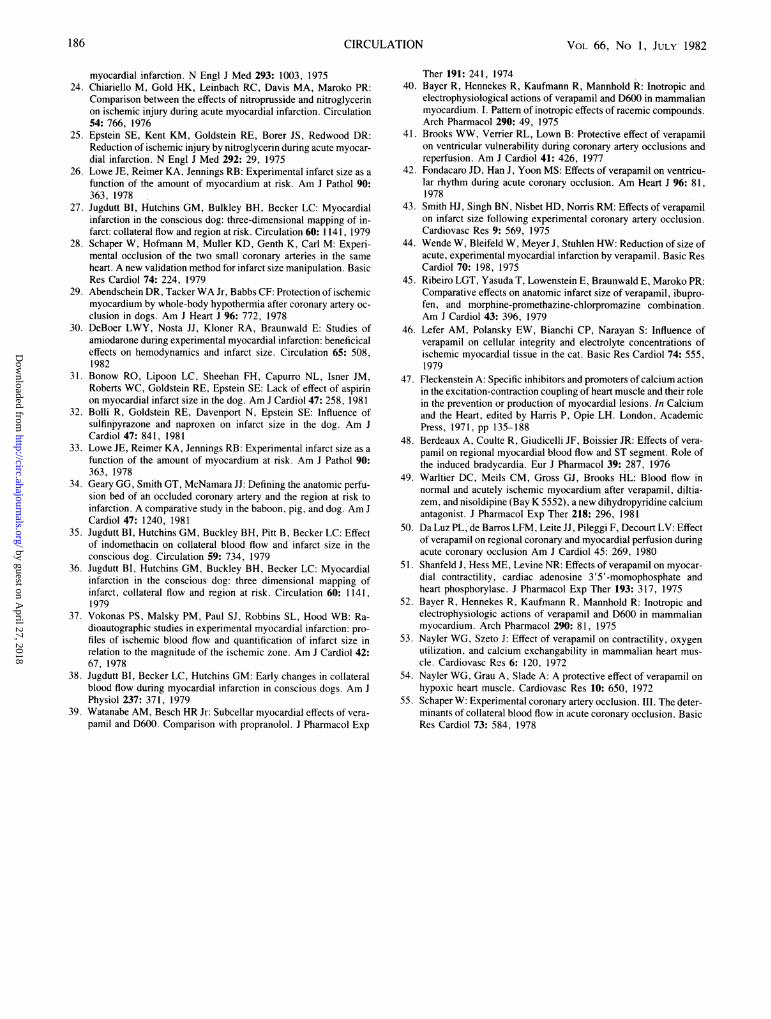
93.1 ± 2.6% for small, medium and large HZs, re-spectively. In the D600-treated group, the percentageof HZ that evolved to infarction was smaller in theD600-treated dogs than in their respective controls foreach class. For small, medium and large infarcts it was31.9 ± 8.3%, 53.8 + 3.0%, and 61.3 ± 9.2%. Allthese IS/HZ values are significantly smaller than theirrespective controls (p < 0.001). The reduction in IS/HZ was 67% in dogs with small, 41% in those withmedium and 34% in those with large HZs. The effec-tiveness of D600 was significantly greater with theinitial smaller area at risk than in the other two classes(fig. 4). When the data were analyzed as a continuousfunction in which the extent of salvage of the myocar-dium was a function-of the area at risk, a close inversecorrelation was found (r = -0.71), which shows thatthe smaller the HZ, the larger the salvaged zone(fig. 5). Thus, the smaller the initial zone in jeopardy,the more effective the treatment.
DiscussionMyocardial infarction is a dynamic process. The
ultimate size of an infarction can be modified by inter-
120 r
10/50
I
Control
ioo0
x2 = 4X22p<.05
80t~-
Infarct Size/Hypoperfused
Zone
I
i
090I
so.
60 F-
401-
0/18D600
FIGURE 2. Mortality rate in dogs between 15 minutes and 6hours after coronary artery occlusion. Mortality is shown as thepercent of dogs that died in each group. Numbers over thecolumns are the number ofdogs that died and the total ofdogs ineach group.
A
A
AA p <.001
I iA
A
20ka
nControl D600
FIGURE 3. The percent of the hypoperfused zone that evolvedto necrosis - comparison of the control and the D600-treatedgroups. Each dot represents one dog.
183
by guest on April 27, 2018
http://circ.ahajournals.org/D
ownloaded from
VOL 66, No 1, JULY 1982
TABLE 2. Effectiveness of D600 in Reducing Infarct Size -Im-portance of the Extenit of the Hypoperfused Zone
InfarctExtent of size/
hypoperfused Hypoperfused hypoperfused Reduc-zone zone (%LV) zone tion
Small C 17.9+ 1.2 (14)* 95.9 3.5 67%(< 25% LV) T 17.3+2.4 (7) 31.9 8.3t 6
Medium C 27.7+0.5 (10) 90.8+3.5 4157(25-30% LV) T 27.6+0.9 (5) 53.8+3.0
Large C 34.6+1.2 (12) 93.1+2.6 34%(> 30% LV) T 37.0+1.5 (6) 61.3+9.2*
Abbreviations: C = control: T = treated.*Numbers in brackets indicate the number of dogs.tp < 0.001 vs control.
ventions early after coronary artery occlusion, makingit possible either to decrease or to increase IS. -5. 12-16Many experimental studies have confirmed and ampli-fied this concept.'7-'9 Some interventions have beenused in clinical trials and, based on indirect measure-ments of myocardial damage, are applicable in patientswith myocardial infarction.2(25 However, it has beenextremely difficult to compare the relative effective-ness of different interventions or the effectiveness ofone intervention under different circumstances, eitherbecause the techniques were not quantitative,3 or be-cause, although the IS was measured precisely, itshowed a wide range of variability. 17 18 IS, even whenthe coronary arteries are occluded at the same site, canvary markedly in consequence of different anatomicdistribution of the coronary arteries and the variabilityin collateral blood flow. Thus, occlusion of the leftanterior descending artery at similar sites may produceinfarcts ranging from 50% of the LV to zero. With thisvariability in individual size of infarcts, the differencesbetween groups of treated and control dogs are difficultto interpret. Several techniques to circumvent thisproblem have been suggested.2$28
80 r
60 F
Reductionin
IS/HZin relationto controls
40 1-
20k
0
1I
<25%
p<.05 p<.02
25-30% > 30%
Hypoperfused Zone (%LV)
FIGURE 4. Reductions in the percent ofthe hypoperfused zone(HZ) that evolved to necrosis, comparing each treated class toits own control. When the HZ was small (< 25% of the leftventricle [LV]), the reduction was 67%; when it was medium(25-30% of the LV), the reduction was 41%; and when it waslarge (> 30% of the LV), the reduction was only 34%. The p
values are comparisons of columns 2 and 3 to the first column.Thus, reduction in infarct size andHZ (ISIHZ) was significantlygreater in dogs with small areas at risk.
100
80
Infarct SizeReduction
1%1
60'
40
20' y = 95.2 - 1.7 x
(n=18, r= .71)
u . . .I I 1:10 20 30
HZ 1% LVI40 50
FIGURE 5. Relationship between the area at risk (hypoper-fused zone [HZ]), percent of left ventricle [LV] and the amountof mvocardium salvaged by D600.
Techniques for determining the area at risk haveused dyes, either in vivo just before sacrifice,2930 orafter sacrifice using artificial perfusion pressures.31-34Other postmortem techniques have also been used,such as steroscopic coronary arteriography.35 36 Auto-radiography has been used to determine the area at riskin vivo, just before sacrifice.37 However, all these de-terminations were performed after the intervention wasgiven and thus would not represent the original area atrisk if the intervention interfered with the collateralcirculation.38 A step further was the development of atechnique to determine the area at risk before interven-tion with technetium-99m-labeled albumin micro-spheres.8 Later, this technique was improved by cut-ting the heart into 20-25 slices, rather than only seven,and using "soft x-ray" radiographs to enhance thevisibility of the border of each slice. This techniquemade it possible to detect with enhanced sensitivity theeffects of beneficial interventions that, using othermethods of measurement, would not have been consid-ered effective.9 Recently, we have used this techniquethat makes each dog its own control and overcomes theprobzlem of variability in the distribution of the coro-nary arteries.', 9 The HZ is measured 1 minute aftercoronary artery occlusion under the actual hemody-namic conditions of the dog, including the collateralblood flow. This is done by injecting radioactive mi-crospheres into the left atrium 1 minute after coronaryartery occlusion and later cutting the LV into 3-mm-thick slices and submitting them to autoradiographyand "soft" x-rays. Using this technique, one can com-pare the extent of the area at risk in each dog to theextent of the area of necrosis. The time of determina-tion of the area at risk is crucial because the interven-tion itself, if given before the time of determination ofthe HZ, may alter the collateral blood flow and thuschange the extent of the area of hypoperfusion, whichshould no longer be considered area at risk. In un-treated dogs, 94 + 2% of the area at risk evolves tonecrosis. Moreover, there is a highly significant corre-
I Iw
184 CIRCULATION
* 0
.
by guest on April 27, 2018
http://circ.ahajournals.org/D
ownloaded from
AREA AT RISK AND INFARCT SIZE REDUCTION/Ribeiro et al.
lation between the area at risk and ultimate necrosis:IS (%LV) = 0.89 + 0.89HZ (%LV), n = 36, r0.93. Thus, the area at risk accurately predicts the ex-tent of IS.
Using this technique, we tested the hypothesis thatthe extent of the initial HZ influences the effectivenessof an intervention in reducing IS. D600 was selectedbecause it is a very potent calcium antagonist6 7 withproperties similar to verapamil,394 which is very ef-fective in reducing arrhythmias and myocardial dam-age after experimental coronary artery occusion.46We did not examine how D600 protects ischemic myo-cardium. However, we can speculate, based on pre-vious studies,47-5 that D600 may either block the in-flux of calcium to the cell, which may play animportant role in protecting the cell,47 or may favor-ably alter the oxygen supply/demand ratio in the ische-mic myocardium due to possible vasodilatory action450or due to the decrease in myocardial oxygen consump-tion.41 9
In this study, D600 reduced IS and prevented ven-tricular fibrillation after coronary artery occlusion.This latter property may be due to an antiarrhythmiceffect or may be indirectly due to protection of theischemic myocardium.To judge whether the initial size of the area at risk is
an important factor in determining the effectiveness ofan intervention in reducing IS, both the control andtreated dogs were grouped according to the extent oftheir areas at risk. Those with small areas at risk, whentreated, showed a reduction in myocardial injury of67% compared with the untreated dogs of the sameclass, while in those with large areas at risk, the reduc-tion in myocardial injury by treatment was only 34%when compared with the untreated dogs of the sameclass. The effectiveness of treatment in dogs with me-dium zones of hypoperfusion was intermediate i.e.,41% reduction. Thus, in dogs with small areas of hy-poperfusion, the benefit of treatment was nearly twicethat in dogs with large zones of hypoperfusion. Also,when the extent of salvaged myocardium was analyzedas a continuous function, there was a close inversecorrelation between it and the magnitude of the hypo-perfused myocardium. This can be explained by easierpenetration of the drug into smaller ischemic zones dueto higher surface/volume ratio. The observation thatsmall zones of hypoperfusion present more collater-als55 is also in accordance with this concept.We conclude that the effectiveness of an interven-
tion depends on the size of the area at risk and that thesmaller this area, the more effective the treatment. Instudies in which the relative effectiveness of differentinterventions are examined, the areas at risk of infarc-tion should be of similar magnitude.
AcknowledgmentThe authors gratefully acknowledge the editorial assistance of B.J.
Gibson and the secretarial assistance of Arlene R. Dorsey.
References1. Maroko PR, Kjekshus JK, Sobel BE, Watanabe T, Covell JW,
Ross J Jr, Braunwald E: Factors influencing infarct size followingcoronary artery occlusions. Circulation 43: 67, 1971
2. Maclean D, Fishbein MC, Braunwald E, Maroko PR: Long-termprotection of ischemic myocardium after experimental coronaryartery occlusion. J Cln Invest 61: 541, 1978
3. Maroko PR, Covell JW: Approaches to the protection of jeopar-dized myocardium. In Coronary Care, edited by Karliner JS. NewYork, Churchill Livingstone, 1981, p 517
4. Smith ER, Redwood DR, McCarron WE, Epstein SE: Coronaryartery occlusion in the conscious dog. Effects of alterations inarterial pressure produced by nitroglycerin, hemorrhage, and al-pha-adrenergic agonists on the degree of myocardial ischemia.Circulation 47: 51, 1973
5. Reimer KA, Lowe JE, Jennings RB: Effect of the calcium antago-nist verapamil on necrosis following coronary artery occlusion indogs. Circulation 55: 581, 1977
6. Fleckenstein A, Byron K: Prevention by Ca-antagonistic com-pounds (verapamil, D600) of coronary smooth muscle contracturedue to treatment with cardiac glycosides. Arch Pharmacaol (supplR20): 282, 1974
7. Nayler WG, Poole-Wilson P: Calcium antagonists. Definition andmode of action. Basic Res Cardiol 76: 1, 1981
8. DeBoer LWV, Strauss HW, Kloner RA, Rude RE, Davis RF,Braunwald E, Maroko PR: An autoradiographic method for mea-suring the ischemic area at risk: the effects of delayed verapamiltherapy on necrosis. Proc Natl Acad Sci 77: 6119, 1980
9. Iwasaki T, Ribeiro LGT, Faria DB, Cheung WM, Maroko PR: Theimportance of the source of hyaluronidase in determining its effec-tiveness in reducing infarct size. AmlHeart J 102: 324, 1981
10. Snedecor GW, Cochran WG: Statistical Methods, 6th ed. Ames,Iowa, Iowa State University Press, 1967, pp 91, 258
11. Fisher RA: Statistical Methods for Research Workers, 13th ed.New York, Hafner Publishing, 1967, p 96
12. Maroko PR, Libby P, Sobel BE, Bloor CM, Sybers HD, Shell WE,Covell JW, Braunwald E: Effect of glucose-insulin-potassium infu-sion on myocardial infarction following experimental coronary ar-tery occlusion. Circulation 45: 1160, 1972
13. Maroko PR, Libby P, Bloor CM, Sobel BE, Braunwald E: Reduc-tion by hyaluronidase of myocardial necrosis following coronaryartery occlusion. Circulation 46: 430, 1972
14. Maroko PR, Libby P, Ginks WR, Bloor CM, Shell WE, Sobel BE,Ross J Jr: Coronary artery reperfusion. I. Early effects on localmyocardial function and the extent of myocardial necrosis. J ClinInvest 51: 2710, 1972
15. Radvany P, Maroko PR, Braunwald E: Effects of hypoxemia on theextent of myocardial necrosis after experimental coronary arteryocclusion. Am J Cardiol 35: 795, 1975
16. Libby P, Maroko PR, Braunwald E: The effect of hypoglycemia onmyocardial ischemic injury during acute experimental coronaryartery occlusion. Circulation 51: 621, 1975
17. Miura M, Thomas R, Ganz W, Sokol T, Shell WE, Toshimitsu T,Kwan AC, Singh BN: The effect of delay in propranolol adminis-tration on reduction of myocardial infarct size after experimentalcoronary artery occlusion in dogs. Circulation 59: 1148, 1979
18. Nasser FN, Walls JT, Edwards WD, Harrison CE Jr: Lidocaine-induced reduction in size of experimental myocardial infarction.Am J Cardiol 46: 967, 1980
19. Ribeiro LGT, Hillis LD, Louie EK, Davis MA, Maroko PR,Braunwald E: A method for demonstrating the efficacy of interven-tions designed to limit infarct size following coronary occlusion.Beneficial effect of hyaluronidase. Cardiovasc Res 12: 334, 1978
20. Maroko PR, Davidson DM, Libby P, Hagan AD, Braunwald E:Effects of hyaluronidase administration on myocardial ischemicinjury in acute infarction. A preliminary study in 24 patients. AnnIntern Med 82: 516, 1975
21. Gold HK, Leinbach RC, Maroko PR: Propranolol-induced reduc-tion of signs of ischemic injury during acute myocardial infarction.Am J Cardiol 38: 689, 1976
22. Maroko PR, Hillis LD, Muller JE, Tavazzi L, Heyndrickx GR,Ray M, Chiariello M, Distante A, Askenazi J, Salerno J, CarpenterJ, Reshetnaya MI, Radvany P, Libby P, Raabe DS, Chazov El,Bobba P, Braunwald E: Favorable effects of hyaluronidase onelectrocardiographic evidence of necrosis in patients with acutemyocardial infarction. N Engl J Med 296: 893, 1977
23. Come PC, Flaherty JT, Baird MG, Rouleau JR, Weisfeldt ML,Greene HL, Becker L, Pitt B: Reversal by phenylephrine of thebeneficial effects of intravenous nitroglycerin in patients with acute
185
by guest on April 27, 2018
http://circ.ahajournals.org/D
ownloaded from
VOL 66, No 1, JULY 1982
myocardial infarction. N Engi J Med 293: 1003, 197524. Chiariello M, Gold HK, Leinbach RC, Davis MA, Maroko PR:
Comparison between the effects of nitroprusside and nitroglycerinon ischemic injury during acute myocardial infarction. Circulation54: 766, 1976
25. Epstein SE, Kent KM, Goldstein RE, Borer JS, Redwood DR:Reduction of ischemic injury by nitroglycerin during acute myocar-dial infarction. N Engl J Med 292: 29, 1975
26. Lowe JE, Reimer KA, Jennings RB: Experimental infarct size as afunction of the amount of myocardium at risk. Am J Pathol 90:363, 1978
27. Jugdutt BI, Hutchins GM, Bulkley BH, Becker LC: Myocardialinfarction in the conscious dog: three-dimensional mapping of in-farct: collateral flow and region at risk. Circulation 60: 1141, 1979
28. Schaper W, Hofmann M, Muller KD, Genth K, Carl M: Experi-mental occlusion of the two small coronary arteries in the sameheart. A new validation method for infarct size manipulation. BasicRes Cardiol 74: 224, 1979
29. Abendschein DR, Tacker WA Jr, Babbs CF: Protection of ischemicmyocardium by whole-body hypothermia after coronary artery oc-clusion in dogs. Am J Heart J 96: 772, 1978
30. DeBoer LWY, Nosta JJ, Kloner RA, Braunwald E: Studies ofamiodarone during experimental myocardial infarction: beneficicaleffects on hemodynamics and infarct size. Circulation 65: 508,1982
31. Bonow RO, Lipoon LC, Sheehan FH, Capurro NL, Isner JM,Roberts WC, Goldstein RE, Epstein SE: Lack of effect of aspirinon myocardial infarct size in the dog. Am J Cardiol 47: 258, 1981
32. Bolli R, Goldstein RE, Davenport N, Epstein SE: Influence ofsulfinpyrazone and naproxen on infarct size in the dog. Am JCardiol 47: 841, 1981
33. Lowe JE, Reimer KA, Jennings RB: Experimental infarct size as afunction of the amount of myocardium at risk. Am J Pathol 90:363, 1978
34. Geary GG, Smith GT, McNamara JJ: Defining the anatomic perfu-sion bed of an occluded coronary artery and the region at risk toinfarction. A comparative study in the baboon, pig, and dog. Am JCardiol 47: 1240, 1981
35. Jugdutt BI, Hutchins GM, Buckley BH, Pitt B, Becker LC: Effectof indomethacin on collateral blood flow and infarct size in theconscious dog. Circulation 59: 734, 1979
36. Jugdutt BI, Hutchins GM, Buckley BH, Becker LC: Myocardialinfarction in the conscious dog: three dimensional mapping ofinfarct, collateral flow and region at risk. Circulation 60: 1141,1979
37. Vokonas PS, Malsky PM, Paul SJ, Robbins SL, Hood WB: Ra-dioautographic studies in experimental myocardial infarction: pro-files of ischemic blood flow and quantification of infarct size inrelation to the magnitude of the ischemic zone. Am J Cardiol 42:67, 1978
38. Jugdutt BI, Becker LC, Hutchins GM: Early changes in collateralblood flow during myocardial infarction in conscious dogs. Am JPhysiol 237: 371, 1979
39. Watanabe AM, Besch HR Jr: Subcellar myocardial effects of vera-pamil and D600. Comparison with propranolol. J Pharmacol Exp
Ther 191: 241, 197440. Bayer R, Hennekes R, Kaufmann R, Mannhold R: Inotropic and
electrophysiological actions of verapamil and D600 in mammalianmyocardium. I. Pattern of inotropic effects of racemic compounds.Arch Pharmacol 290: 49, 1975
41. Brooks WW, Verrier RL, Lown B: Protective effect of verapamilon ventricular vulnerability during coronary artery occlusions andreperfusion. Am J Cardiol 41: 426, 1977
42. Fondacaro JD, Han J, Yoon MS: Effects of verapamil on ventricu-lar rhythm during acute coronary occlusion. Am Heart J 96: 81,1978
43. Smith HJ, Singh BN, Nisbet HD, Norris RM: Effects of verapamilon infarct size following experimental coronary artery occlusion.Cardiovasc Res 9: 569, 1975
44. Wende W, Bleifeld W, Meyer J, Stuhlen HW: Reduction of size ofacute, experimental myocardial infarction by verapamil. Basic ResCardiol 70: 198, 1975
45. Ribeiro LGT, Yasuda T, Lowenstein E, Braunwald E, Maroko PR:Comparative effects on anatomic infarct size of verapamil, ibupro-fen, and morphine-promethazine-chlorpromazine combination.Am J Cardiol 43: 396, 1979
46. Lefer AM, Polansky EW, Bianchi CP, Narayan S: Influence ofverapamil on cellular integrity and electrolyte concentrations ofischemic myocardial tissue in the cat. Basic Res Cardiol 74: 555,1979
47. Fleckenstein A: Specific inhibitors and promoters of calcium actionin the excitation-contraction coupling of heart muscle and their rolein the prevention or production of myocardial lesions. In Calciumand the Heart, edited by Harris P, Opie LH. London, AcademicPress, 1971, pp 135-188
48. Berdeaux A, Coulte R, Giudicelli JF, Boissier JR: Effects of vera-pamil on regional myocardial blood flow and ST segment. Role ofthe induced bradycardia. Eur J Pharmacol 39: 287, 1976
49. Warltier DC, Meils CM, Gross GJ, Brooks HL: Blood flow innormal and acutely ischemic myocardium after verapamil, diltia-zem, and nisoldipine (Bay K 5552), a new dihydropyridine calciumantagonist. J Pharmacol Exp Ther 218: 296, 1981
50. Da Luz PL, de Barros LFM, Leite JJ, Pileggi F, Decourt LV: Effectof verapamil on regional coronary and myocardial perfusion duringacute coronary occlusion Am J Cardiol 45: 269, 1980
51. Shanfeld J, Hess ME, Levine NR: Effects of verapamil on myocar-dial contractility, cardiac adenosine 3'5'-momophosphate andheart phosphorylase. J Pharmacol Exp Ther 193: 317, 1975
52. Bayer R, Hennekes R, Kaufmann R, Mannhold R: Inotropic andelectrophysiologic actions of verapamil and D600 in mammalianmyocardium. Arch Pharmacol 290: 81, 1975
53. Nayler WG, Szeto J: Effect of verapamil on contractility, oxygenutilization, and calcium exchangability in mammalian heart mus-cle. Cardiovasc Res 6: 120, 1972
54. Nayler WG, Grau A, Slade A: A protective effect of verapamil onhypoxic heart muscle. Cardiovasc Res 10: 650, 1972
55. Schaper W: Experimental coronary artery occlusion. III. The deter-minants of collateral blood flow in acute coronary occlusion. BasicRes Cardiol 73: 584, 1978
186 CIRCULATION
by guest on April 27, 2018
http://circ.ahajournals.org/D
ownloaded from

L G Ribeiro, W Cheung and P R Marokosize.
Influence of the extent of the zone at risk on the effectiveness of drugs in reducing infarct
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1982 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.66.1.181
1982;66:181-186Circulation.
http://circ.ahajournals.org/content/66/1/181.citationthe World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on April 27, 2018
http://circ.ahajournals.org/D
ownloaded from


















