in this issue: Narcotic Addiction - ssmhealth.com Health... · Babies Breathe and Essential Care...
20
St. Mary’s Hospital – St. Louis Cardinal Glennon Children’s Hospital PERINATAL Times Vol. 29 | May 2016 in this issue: Narcotic Addiction in Pregnancy
Transcript of in this issue: Narcotic Addiction - ssmhealth.com Health... · Babies Breathe and Essential Care...

Vol. 29 | April 2016
St. Mary’s Hospital – St. LouisCardinal Glennon Children’s Hospital
PERINATALTimesVol. 29 | May 2016
in this issue:
Narcotic Addiction in Pregnancy

vol. 29 | may 2016
v
St. Mary’s Hospital – St. LouisCardinal Glennon Children’s Hospital
Vol. 29 | May 2016
INSIDE THIS ISSUE:
1 NRP IN THE KNOW Persistently Low Heart Rate: Indications for Compressions
3 FORMULARY FACTS Subutex & Pregnancy
5 Narcotic Addicted Pregnant Women: Treatment Alternatives
10 Neonatal Abstinence Syndrome: Evaluation & Management of the Maternal Infant Dyad
15 THE MONITOR CORNER Sinusoidal Fetal Heart Rate Pattern
The Perinatal Outreach Program
The Perinatal Outreach Program is a collaborative effort between SSM Health Maternity Care at SSM Health St. Mary’s Hospital - St. Louis, SSM Health Cardinal Glennon Children’s Hospital and St. Louis University School of Medicine.
It is designed to improve outcomes for mothers and babies through educational programs and quality improvement activities for regional perinatal care providers in eastern Missouri and southern Illinois.
SSM Health Cardinal Glennon Children’s Hospital and SSM Health St. Mary’s Hospital - St. Louis are the designated Administrative Perinatal Center for Southern Illinois.
Perinatal Times Editorial Board
Meredith Meyer, RNC, BSN, Editor
SSM Health Cardinal Glennon Children’s Hospital
SSM Health St. Mary’s Hospital – St. Louis
Mohamad Al-Hosni, MD Gilad A. Gross, MD
Ayoob Ali, MD, MPH Kathleen Klug, RN, BSN
Glenn Barber, RNC, BSN Katie Kulaitis, RN, BSN
Robyn Gude, RN, MSN Thomas Myles, MD
Mary Hope, RN, BSN Laurie Niewoehner, PharmD
Justin Josephsen, MD Pam Randazzo, RNC, BSN
William Keenan, MD Sharon Rector, RNC, MSN
Patricia Oberkirsch Judy Wilson-Griffin, RNC, PNCNS
Funding
Financial support for The Perinatal Times is provided by SSM Health – St. Louis and the Illinois Department of Public Health.
Letters
The Perinatal Times welcomes comments on any of its articles and will consider such letters for publication. Suggestions for future topics of interest or announcements are encouraged.
Please send correspondence to:
The Perinatal Times Meredith Meyer, Editor
SSM Health St. Mary’s Hospital - St. Louis 6420 Clayton Road Richmond Heights, MO 63117
To receive an electronic version of The Perinatal Times, please email Patricia Oberkirsch at [email protected]

About the Author
Glenn Barber is a Neonatal Outreach Educator in the Perinatal Outreach Department at SSM Health Cardinal Glennon Children’s Hospital. He is a Regional NRP Instructor, a Lead STABLE Instructor and a Master Trainer for the Helping Babies Breathe and Essential Care for Every Baby Programs with 25 years of clinical experience.
the PERINATAL Times | 1
v
St. Mary’s Hospital – St. LouisCardinal Glennon Children’s Hospital
A 39 2/7 week gestation infant is delivered by emer-gent caesarian section for persistent fetal bradycardia. The amniotic fluid was clear. Immediately after birth, the infant was limp and apneic. The baby was placed under a radiant warmer, dried, stimulated and posi-tioned with the airway opened. Effective positive pressure ventilation is started at a rate of 50. A second team member detects the heart at 40 beats per minute and places an oximeter probe on the right wrist. The FiO2 was increased to 100% with the pre-ductal SPO2 at 38%. The infant was then intubated with a 3.5 ETT. Placement was verified and ventilation with chest movement and breath sounds continued. Thirty seconds later, the heart rate remains less than 60.
Which of the following interventions would be appropriate for this infant?
1. Give 1 ml of Epinephrine 1:10,000 IM while IV access is being obtained.
2. Start coordinated chest compressions and ventilation using a 15:2 ratio.
3. Start coordinated chest compressions and ventilation using a 3:1 ratio.
4. Continue to only ventilate for another 2 minutes and reevaluate the heart rate.
Correct response
Start coordinated chest compressions & ventilation using a 3:1 ratio.
Discussion
Effective ventilation remains the key and most import-ant skill in neonatal resuscitation. The 6th edition NRP recommends at least 30 seconds of effective venti-lation prior to the start of chest compressions. Chest compressions will have little benefit without adequate lung ventilation. Babies with a heart rate <60 beats per minute, in spite of effective ventilations, are likely to have depressed myocardial function secondary to low blood oxygen levels and significant acidosis.1 Chest compressions are a means of mechanically pumping blood by compressing the heart against the spine. This increases the intrathoracic pressure causing blood to be pumped into the arteries. When the sternal pressure is released, the blood then fills the heart from the veins.
Chest compressions with ventilation in a newborn requires a team approach and must have at least two people. The person assisting ventilations should continuously assess for effective chest movement
Persistently Low Heart Rate:Indications for Compressionsby Glenn Barber, RNC-NIC,BSN
NRP in the Know
NRP in the Know

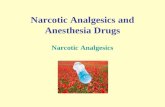
HR below 60 BPM
Consider intubation chest compressions
Coordinate with PPV
HR below 60 BPM
Take ventilation corrective steps
HR below 100 BPM
Yes
No
No
Yes
Yes
Indications for Compressions (continued)
2 | vol. 29 | may 2016
with ventilation while the second person preforms chest compressions ensuring correct placement, depth, tempo, and coordinated ratio of compressions/ventilations. Other team members may be needed for management of oxygen/oximetry or vascular assess.
The thumb technique is the preferred method of chest compressions suggested by the NRP. The two thumbs are used to compress the sternum, while the hands encircle the chest and the fingers support the back or spine. Studies have shown that the thumb technique produces higher blood pressure, can sustain a consis-tent quality of compressions for a longer time, and is perceived as easier and less tiring for the provider. The two finger technique is achieved by using the middle finger and either the index or ring finger to compress the sternum. It is important to remember to support the back with the other hand during this method. Regardless of technique, the thumbs or fingers should remain in contact with the chest at all times during the compression and release. If the thumbs or fingers are
lifted off the sternum after compression, there is an increased risk of injury or malposition. Chest compres-sions should be performed on the lower third of the sternum avoiding the xiphoid process.
Chest compressions must always be a coordinated effort with positive pressure ventilations. The recom-mended cycle is 3 compressions plus 1 ventilation and should be performed at a tempo to accomplish 90 compressions and 30 breaths every minute. The team should avoid giving a compression and ventilation simultaneously, whereas one will decrease the efficacy of the other. The person performing chest compression should count aloud “One-and-Two-and-Three-and- Breathe” which will help develop a well-coordinated rhythm among the team.
The 6th edition NRP recognized that it may take longer than 30 seconds of compressions to see changes in the heart rate. It may take 45 seconds or longer after the initiation of chest compression before the coronary perfusion pressure returns. Therefore, it is now recommended to wait at least 45 – 60 seconds, after establishing effective compression and ventilation, before pausing the resuscitation effort to evaluate the heart rate. Chest compressions can be discontinued when the heart rate increases above 60 beats per minute. The focus then shifts back to pro-viding effective ventilations at a higher rate of 40 – 60 breaths per minute. Along with chest compressions and ventilations, additional interventions such as umbilical catheter placement or Epinephrine should be considered if the heart rate remains below 60 beats per minute.
Along with optimizing teamwork, other key elements of neonatal resuscitation are preparation, anticipation of problems, prompt recognition, and early intervention. The sooner one more skillfully intervenes the more likely a positive response. ❧
References
1. Kattwinkel J, McGowan JE, Zaichkin J. Textbook of Neonatal Resuscitation. 6th ed. Elk Grove Village: American Academy of Pediatrics; 2011.
2. Perlman JM, Wyllie J, Kattwinkel J, et al. Special Report—Neonatal Resuscitation: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Pediatrics. 2010; 126:e1318-1345.
Source: Kattwinkel J, McGowan JE, Zaichkin J. Textbook of Neonatal Resuscitation. 6th ed. Elk Grove Village: American Academy of Pediatrics; 2011.

Formulary Facts
the PERINATAL Times | 3
Subutex & Pregnancyby Laurie Niewoehner, Pharm D
About the Author
Laurie Niewoehner is a Clinical Pharmacy Specialist at SSM Health St. Mary’s Hospital – St. Louis. She attended the University of Minnesota and com-pleted a specialty residency program in Pediatrics at Children’s Mercy Hospital and the University of Missouri-Kansas City School of Pharmacy in Kansas City. Laurie is also a preceptor for Neonatology and Women’s Health pharmacy students.
M ethadone has been the standard of care for opioid dependency during pregnancy for the past
40 years. It has enhanced the opioid dependent woman’s chances of having a trouble-free pregnancy and healthy baby compared to continued narcotic abuse. Continued abuse can lead to an increased risk of developing infectious diseases, Hepatitis, HIV, and pregnancy complications such as miscarriage, low birth weight, and neurobehavioral issues.
The National Institute on Drug Abuse (NIDA) supported a clinical trial where buprenorphine was found to be a safe and effective alternative to methadone for opioid dependence during pregnancy. Unlike methadone, buprenorphine is a partial rather than full opioid agonist so it causes less severe fetal opioid dependence than methadone therapy. It also produces a lower level of physical dependence so patients who might suddenly stop the medication would have fewer withdrawal symptoms. There were similar rates of pregnancy complications and they gave birth
Formulary Facts

4 | vol. 29 | may 2016
Subutex & Pregnancy (continued)Subutex & Pregnancy (continued)
References
1. Jones, H., Johnson, R, et al. 2005. Buprenorphine versus methadone in the treatment of pregnant opioid-dependent patients: effects on the Neonatal Abstinence Syndrome. Alcohol and Drug Dependence 79, 1-10
2. www.nih.gov “Buprenorphine treatment in preg-nancy: less distress to babies”, NIH News. 2010
3. www.drugabuse.gov Whitten Lori. “Buprenorphine During Pregnancy Reduces Neonate Distress” NIH : National Institute on Drug Abuse.2012.
to infants that were comparable on key indicators of neonatal health. Infants who were born to women who received buprenorphine had milder neonatal opioid withdrawal than those whose moms received metha-done. These babies required less medication (1.1 mg vs 10.4 mg) and spent less time in the hospital (10 vs 17.5 days). This data suggests that buprenorphine treatment is a good option for pregnant women who are new to treatment. However, if a patient is pregnant and stable on methadone maintenance, they should remain on this therapy for the pregnancy. The goal is to induce treat-ment smoothly and suppress withdrawal as completely and rapidly as possible. ❧
DRUG FACTS
Subutex® Buprenorphine• Semi-synthetic CIII opioid
• Partial mu-opioid agonist
• Supplied as 0.4 mg, 2 mg, 8 mg
• Starting dose: 4 mg PO BID and maintenance is between 16-24 mg daily. Dose gradually decreased.
• Medication therapy usually initiated when early withdrawal symptoms are beginning to show
• Must be dissolved under the tongue as chewing or swallowing will not have effect
• Onset of effects: 20-40 minutes
• Half-life- 31-35 hours
• Side Effects: headaches, depression, insomnia, nausea, vomiting, constipation, and low blood pressure. Be sure to monitor any other medications patient may be on such as antidepressants and sleep aids.
• Patients should not drink alcohol while on the medication
• Patients should not suddenly stop taking the medications as they may experience withdrawal symptoms
• Injecting or “shooting up” medication can cause life-threatening infections or cause serious withdrawal symptoms
• Limited to prescribing physicians who have met specific criteria listed in DATA 2000
Suboxone® (buprenorphine and naloxone) is currently avoided in pregnancy due to the potential risk of withdrawal if not taken properly.

About the Author
Jaye Shyken, M.D. is an associate professor in the Department of Obstetrics, Gynecology, and Women’s Health, Division of Maternal-Fetal Medicine, at Saint Louis University School of Medicine. Dr. Shyken is a Maternal-Fetal Medicine specialist in the Maternal-Fetal Medicine Division at SSM Health St. Mary’s Hospital - St. Louis with areas of specialty including alcohol and substance abuse in pregnancy, smoking cessation, and high-risk pregnancy.
Treatment Alternatives
the PERINATAL Times | 5
M aternal opioid abuse is a growing public health concern with impact on both maternal and newborn health. Drug use and abuse
generally precedes conception, and those who use only casually can often stay abstinent for pregnancy. However, for those who are dependent, cessation can be extremely difficult if not impossible. The stigma associated with narcotic dependence in pregnancy along with a paucity of resources to address her addiction make identification and referral problematic.
This decade has seen a huge increase in the number of people who abuse and become dependent on narcot-ics. There is an increasing trend towards emergency department visits, overdoses, and overdose deaths, of which pregnant women have not been spared. According to the National Survey on Drug Use and Health, between 2004 and 2010 the number of people who abused or were dependent on pain medications increased from 1.4 million to 1.9 million. Over this time period, the percentage of these individuals using heroin doubled, with an increase in heroin users from 70,000 in 2004 to 266,000 in 2010.¹ U.S. overdose deaths involving prescription opioid analgesics increased to about 17,000 deaths in 2010, almost double the number in 2001.² This increase coincided with a nearly fourfold increase in the use of prescribed opioids for the treatment of pain.³ This trend is mirrored in the obstetric population. From 2000 to 2007 the trend in prescription opioid use in pregnancy among a population of over 1.1 million Medicaid-enrolled women increased from 18.5% to 22.8%. This trend was seen for each trimester of pregnancy.⁴
Of even greater concern is the rise in the incidence of neonatal abstinence syndrome (NAS). NAS occurs in 55-94% of newborns whose mothers are opioid dependent.⁵ NAS is discussed in further detail elsewhere in this publication.
The American College of Obstetricians and Gynecologists (ACOG) recommends universal screen-ing for drug use in all women prior to and in early
pregnancy. Women should be queried about their use of tobacco, alcohol, prescription, and non-pre-scription medications in a non-judgmental manner.⁶ Identification of substance use by enhanced patient self-report allows the opportunity for brief intervention and referral for treatment. Once identified, the obstet-ric provider should educate the patient regarding the potential effects of opioids and opioid dependence on her and her fetus/newborn. Brief interventions include counseling to become abstinent if they can, engag-ing her in self-help strategies including Alcoholics Anonymous and Narcotic Anonymous meetings, or referring for substance abuse counseling and treat-ment. Chemical screening in the way of analysis of urine, blood, hair, saliva, and sweat are possible, but these tests are fraught with limitations. Since narcotic metabolites are present in the urine for 2 to 3 days, a negative test does not rule out more remote use or a test result that is below the threshold of identification. A positive test does not provide information about the duration, frequency and quantity of drug ingested. The ACOG does not recommend routine biochemical testing as the sole means of detection of substance use in women (ACOG, 2012).
Opioid abuse is associated with medical complications and adverse pregnancy outcomes. These women are additionally at risk from activities related to seeking and using narcotics such as needle-related infectious
Narcotic Addicted Pregnant Women:
Treatment Alternativesby Jaye Shyken, M.D.

The WISH Center (Women and Infants Substance Abuse Help)
Located at SSM Health St. Mary’s Hospital – St. Louis, the WISH Center utilizes a multidisciplinary approach in the care and treatment of narcotic addicted preg-nant women. Maternal Fetal Medicine Specialists from Saint Louis University provide the innovative care for these high acuity mothers and babies.
The program includes medical addiction treatment with buprenorphine, coordination for chemical
6 | vol. 29 | may 2016
morbidity, trading sex for drugs, accidents and trauma, and involvement with law enforcement. Concomitant use of other drugs of abuse such as methamphet-amines, cocaine, tobacco, and benzodiazepines carry their own profile of potential morbidity. Frequently, women have additional psychiatric diagnoses. Even in the absence of current narcotic injection, they are at risk for carrying infection with hepatitis B, hepatitis C, or HIV.
First trimester narcotic use has recently been recog-nized in two case-control studies to be associated with doubling the risk for open neural tube defects, conoventricular septal defects, atrioventricular septal defects, and hypoplastic left heart syndrome.7,8
It should be noted that the absolute risk for these conditions, however, remains low. Chronic use of heroin in pregnancy is associated with risk of fetal growth restriction, abruptio placenta, fetal death, preterm labor, and meconium staining.⁹ It is unclear whether risks are attributable to placental dysfunction due to repeated intoxication and withdrawal and to what extent life-style related conditions are contributory.
Treatment options
Currently available treatment alternatives for women who are narcotic-dependant are detoxification, either with or without medication assistance, or chemical dependence treatment with narcotic replacement therapy. Narcotic addiction is very difficult to treat and relapse is frequent. Sustained sobriety after non-med-ication maintained rehabilitation treatment is low. Seventy-one percent of users relapse within 6 weeks when rehabilitation is not accompanied by narcotic maintenance therapy.¹⁰ Case reports from the 1970s suggested a high risk for miscarriage and fetal death¹¹ as well as rising levels of intrauterine epinephrine and norepinephrine levels¹² leading to the widespread reluctance to offer detoxification as a treatment strategy for pregnant women. In fact, detoxification through methadone taper in a medically and obstet-rically supervised setting does not appear to have obvious adverse maternal and fetal effects. However, the success rate is relatively low at 50-59% even in the short term, and it requires prolonged hospitalization on the order of 21 to 39 days.13,14,15 Currently, the role for opioid detoxification in pregnancy is minimal given the likelihood of failure and the intensive resources demanded to achieve success.
Methadone maintenance therapy (MMT) in pregnancy is considered the standard of care in the United States
and methadone remains the only FDA approved medication for narcotic replacement for pregnant women. The benefits of methadone maintenance are many including the prevention of withdrawal with its attendant drug seeking behavior and the elimination of needle-associated morbidity. The result is decreased use of illegal opiates and other drugs, prevention of fluctuation of maternal drug levels over the course of a day, reduction in the spread of HIV and other sexually transmitted diseases, decrease in crime, reduction in maternal mortality and severe morbidity, and improvement in maternal nutrition. There is overall improvement in general health. On the fetal side, there is a decrease in the risk of neonatal hypoxia due to a more stable intrauterine environment and a reduction in obstetrical complications. Stabilized mothers are more likely to attend prenatal visits, participate in chemical dependency treatment, maintain employ-ment, and retain custody of their children.
Methadone is a full mu-opioid agonist and a weak N-methyl-D-apartate (NMDA) receptor antagonist. Methadone has the advantage of a high bioavailability and long half-life, such that once daily dosing is generally possible. It is of low cost, taken orally, and exhibits a slow onset to withdrawal after discontinua-tion. Methadone is metabolized by the cytochrome p 450 system (CYP), but it also inhibits CYP. Therefore, there is a long list of drug interactions, many of which are clinically significant. Adverse effects include QTc prolongation, respiratory depression, and hypotension. Due to the potential for QT interval prolongation, other medications that can prolong the QTc in susceptible individuals should be avoided or used with great caution.¹⁶ Frequently, dose increases are necessary as pregnancy progresses due to the increased volume of distribution, increased renal clearance, and increased
Treatment Alternatives (continued)

dependency treatment and methadone maintenance, comprehensive high-risk prenatal care and delivery, maternal-fetal medicine subspecialty care, pharmacy services, social services case management, behavioral medicine support, neonatal consultation, lactation consultation and Medicaid/insurance financial counseling.
An appointment for evaluation can be scheduled by contacting 314-768-8726 or through the Perinatal Access line: 1-888-636-7642
Treatment Alternatives
the PERINATAL Times | 7
CYP enzyme activity. Rarely, split twice-daily dosing is necessary.¹⁷ Overall, the benefit of providing this medication to pregnant women outweighs the risk.
When used for the management of addiction, methadone is administered only in federally licensed methadone maintenance facilities. In general, women are maintained on 60-150 mg of methadone daily, but dosing is titrated to achieve the least amount of drug that eliminates craving and prevents withdrawal. Clients are required to visit the center daily for meth-adone administration. These facilities also provide drug testing and chemical dependency counseling. Unfortunately, the number of these facilities is limited. Distance from a federally licensed methadone clinic and need for daily visits may not make this an option for some women.
In 2008 a consensus panel from SAMHSA concluded that buprenorphine, a partial mu agonist, may be a good option for narcotic-addicted pregnant women. This was confirmed by ACOG in 2012⁶ specifically for women who cannot tolerate methadone, refuse to take it, find compliance with daily dosing difficult, or for those who do not have a treatment facility available. Unlike methadone, buprenorphine (Subutex) is a partial agonist at the mu receptor as well as an antagonist at the kappa receptor in the central nervous system. It strongly binds to these receptors without activating them and is highly protein-bound, decreasing, but not eliminating some of the negative effects and the potential for overdose and abuse. It is available as a 2 mg and 8 mg sublingual tablet as it has very poor bioavailability when given orally. It has a long half-life of 24 to 60 hours and demonstrates a “ceiling effect”. In essence, when given over a certain dose, generally 16-20 mg, no additional benefit is accrued. It is slowly released from its receptor and is not easily displaced
by competing opioids. Buprenorphine is available by prescription from a credentialed provider who has a SAMHSA waiver (DATA 2000 waiver ID#). Potential benefits of buprenorphine over methadone include its availability in an office-based setting, less overdose potential, fewer drug interactions, and less placental transfer. After a sustained demonstration of sobriety, women can be granted prescriptions for as long as 30 days at a time.
There are some disadvantages to buprenorphine. The decision whether to begin methadone or buprenor-phine requires careful evaluation taking into account elements of the social, psychiatric, medical and sub-stance abuse history. Buprenorphine is likely associated with a greater risk for treatment failure compared to methadone for pregnant women.¹⁸ Other factors that may preclude the use of buprenorphine include depen-dence on high doses of benzodiazepines or other CNS depressants, such as alcohol, significant untreated psychiatric conditions, suicidal or homicidal ideation, multiple previous treatment failures with frequent relapses, poor response to well-conducted buprenor-phine maintenance previously, significant medical complications, high baseline need for opiates (1 to 1.5 grams/day or more), chaotic social situation or other high risk factors for relapse, and need for certain medi-cations that would pose a dangerous interaction. Those who would benefit from daily supervision and are not in residential treatment may benefit from methadone as their treatment modality. Another disadvantage to buprenorphine is that it requires that the patient be in mild to moderate withdrawal prior to initiation, so that the addition of buprenorphine, a partial agonist does not result in precipitated withdrawal.
Buprenorphine is available as monotherapy, which is preferred in pregnancy. It is also available in combina-tion with the narcotic antagonist naloxone in a 4:1 ratio (Suboxone). Naloxone has poor bioavailability orally or sublingually. It is presented in this combination solely to deter injection or inhalation use which results in precipitated withdrawal. Therefore, there is a lower potential for diversion and abuse.¹⁹ Buprenorphine monotherapy is preferred over the combination agent due to a greater experience and demonstration of safety in the literature.
There are still relatively few trials in the literature com-paring buprenorphine to methadone in a systematic way. Yet information is accumulating. In the Cochrane Database18, four trials were identified, three of which were double- blinded, involving 271 pregnant women.

8 | vol. 29 | may 2016
The findings from these pooled data suggested that the risk of dropout from treatment was less with methadone in three studies involving 233 women. Birth weights were higher in the buprenorphine group in the two trials that could be pooled (mean difference of 365 grams) and the third study found no significant differ-ence. The number of newborns who required treatment for NAS was not significantly different between the groups, but the quality of evidence was low. Only one study evaluated side effects which were not found to be different for the mothers.18 However, the largest study to date, which was included in the Cochrane Review, involved 175 women and was a double-blinded, multi-center, randomized trial. Buprenorphine was associated with significantly lower doses of morphine used to treat neonatal withdrawal, shorter duration of hospitalization of the newborn by a mean 7 days, and shorter duration of treatment days for NAS.²⁰ A recent cohort analysis of 62 women, 31 treated with methadone and 31 treated with buprenorphine and naloxone was published. There was a significantly lower risk of NAS in the buprenorphine-naloxone group compared to the methadone group (51.6% v 25.1%), lower peak NAS scores and shorter neonatal hospital-izations.²¹ Although limited in number, this suggests that buprenorphine-naloxone is a viable alternative to buprenorphine monotherapy.
Antepartum Management
Whether buprenorphine or methadone is chosen as the agent for narcotic replacement in pregnancy, it must be accompanied by rigorous chemical depen-dency treatment. Neither addiction treatment nor prenatal care can be managed optimally without communication and cross-consultation. In addition to routine elements of prenatal care, fetal morphology investigation and surveillance for growth restriction are necessary. Testing for HIV and hepatitis A, B and C is indicated. If serology is negative, vaccination for hepatitis A and B should be accomplished. Educational efforts are directed towards lactation, preterm labor identification, and relapse prevention. Women are counseled that NAS is expected, but that treatment is possible and necessary to make the baby com-fortable. Neonatology and anesthesia consultations should be offered. Anesthesia consultation prior to 36 weeks is mandatory if cesarean delivery is anticipated or neuraxial analgesia is contraindicated. Relapse identification and management is accomplished by building rapport and having frank and non-judgmental
conversations. In some instances, relapse prevention is achieved by increasing methadone or buprenorphine doses. Urine drug screens are necessary to ensure compliance and if positive, provide an opportunity to investigate obstacles for sobriety. The antepartum care requires a multi-disciplinary team of obstetric provider, nursing, chemical dependency provider, social services, lactation consultant, neonatologist and sometimes psychiatrist. Prior to prescribing medications for a pregnant woman on methadone or buprenorphine, care should be taken to identify possibly dangerous drug interactions and provide safer alternatives.
Intrapartum Issues
It is important to note that buprenorphine or meth-adone is not sufficient medication for labor pain. Women who are on opioid-agonist medications are significantly tolerant to opioids and cross-tolerant to other classes of potentiating medications such as the sedative-hypnotics. In addition, they experience increased pain sensitivity. Partial agonists such as nalbuphine (Nubain) and butorphanol (Stadol) are contraindicated as they can precipitate withdrawal in methadone maintained women and are also contraindi-cated for buprenorphine maintained women. Consider the use of early epidural analgesia in labor which can generally be discontinued after perineal repair.
Cesarean delivery is only necessary in this population for obstetric indications. For women who do require cesarean delivery, very high doses of narcotic med-ication may be necessary to control pain and ICU admission may become indicated. Since buprenorphine is a partial mu agonist with low intrinsic activity, high receptor affinity and slow dissociation, lower doses of full agonists for pain will be ineffective. Patient con-trolled epidural analgesia or combined spinal-epidural analgesia are appropriate options as well as prolonged epidural placement in the post-operative period. Either methadone or buprenorphine is continued to prevent withdrawal throughout the hospitalization.22,23 An exception to this might be in buprenorphine treated women who need high doses of a pure narcotic ago-nist, such as fentanyl, for pain control. These women would therefore take narcotics for the duration of their acute pain which would prevent their withdrawal. However, prior to restarting buprenorphine they must be abstinent from narcotics and be in mild to moderate withdrawal. This management is best accomplished by their buprenorphine provider generally as an outpa-tient in the postpartum period.
Treatment Alternatives (continued)

the PERINATAL Times | 9
References
¹ National Survey on Drug Use and Health (NSUH)2004-2010, SAMHSA 2012.
² Centers for Disease Control and Prevention (CDC), National Center for Health Statistics. CDC WONDER Online Database, 2012.
³ Harvard Medical School, Painkillers fuel growth in drug addiction: Opioid overdoses now kill moer people than cocaine or heroin. Harvard Ment Hlth Let. 2011;27(7);4-5.
⁴ Desai RJ, et al. Obstet Gyneco.l 2014;123;997-1002.
⁵ Hudak ML, Tan RC, The Committee on Drugs, and the Committee on Fetus and Newborn. Neonatal drug withdrawal. Pediatrics 2012;129;e540-60.
⁶ American College of Obstetricians and Gynecologists. Opioid abuse, dependence, and addiction in preg-nancy. Committee Opion No. 524, American College of Obstetricians and Gynecologists. Obstet Gynecol 2012;119:1070-6., reaffirmed 2014.
⁷ Yazdy MM, et al. Obstet Gynecol 2013;122:838-44.
⁸ Broussard CS, Rasmussen SA, Reefhuis J, et al al. Maternal treatment with opioid analgesics and risk for birth defects. National Birth Defects Prevention Study. Am J Obstet Gynecol 2011;2014:314.e1-11
⁹ Center for Substance Abuse Treatment. Medication-assisted treatment for opioid addiction during pregnancy. SAMHSA/CSAT treatment improvement protocols. Rockville, MD; Substance Abuse and mental Health Services Administration, 2012.
¹⁰ Gossop M, Green L, Phillips G, et al. Lapse, relapse and survival among opiate addict after treatment. A prospective follow-up study. Br J Psychiatry. 198;154;348-53.
¹¹ Rementeria JL, Nunag NN. Narcotic withdrawal in pregnancy: stillbirth incidence with a case report. Am J Obstet gynecol. 1973;116;1152-6.
¹² Zuspan FP, Gumpel JA, Mejia-Zelaya A, et al. Fetal stress from methadone withdrawal. Am J Obstet Gynecol 1975;122:43-6.
¹³ Stewart RD, Nelson DB, Adhikari EH, et al. The obstetrical and neonatal impact of maternal opioid detoxification in pregnancy. Am J Obstet Gynecol 2013;209;267.e1-5.
¹⁴ Luty J, Nikolaou V, Bearn J. Is opiate detoxifica-tion unsafe in pregnancy? J Subst Abuse Treat 2003;24:363-7.
¹⁵ Dashe JS, Jackson GL, Olscher DA, et al. Opioid detoxi-fication in pregnancy. Obstet Gynecol 1998;92:854-8.
¹⁶ Trescot AM, Datta S, Lee M, et al. Opioid pharmacology. Pain Physician 2008;11:S133-53.
¹⁷ Young JL, Martin PR. Treatment of opioid dependence in the setting of pregnancy. Psychiatr Clin N Am 2012;35:441-60.
¹⁸ Minozzi S, et al. Maintenance agonist treatments for opiate-dependent pregnant women. Cochrane Database Syst Rev 2013;12:cD006318
¹⁹ Johnson RE, McCagh JC. Buprenorphine and nal-oxone for heroin dependence. Curr Psychiatry Rep 2000;2:519-26.
²⁰ Jones HE, Kaltenbach K, Heil SH, et al. Neonatal absti-nence syndrome after methadone or buprenorphine exposure. N Engl J Med 2010;363;2320-31.
²¹ Wiegand SL, Stringer EM, Stuebe AM, et al. Burepnorphine and naloxone compared with meth-adone treatment in pregnancy. Obstet Gynecol 2015;125;363-8.
²² Meyer M, Parnya G, Keefer A, et al. Intrapartum and postpartum analgesia for women maintained on buprenorphine during pregnancy. Eur J Pain 2010;14:939-43.
²³ Meyer M, Wagner K, Benvenuto A, et al. Intrapartum and postpartum analgesia for women maintained on methadone during pregnancy. Obstet Gynecol 2007;110:261-6.
Postpartum Period
The postpartum period is an important time to screen for depression and offer services that aim to promote family unity and contribute to long-term maternal health. Home health visits may be beneficial. It is essential that social services are involved in coordi-nation in the postpartum period, particularly if the Division of Family Services is also involved.
In conclusion, for opioid addicted pregnant women, opioid discontinuation would rarely, if ever, be indi-cated. Methadone is still considered the first line, only FDA approved medication for narcotic replacement in pregnancy. Buprenorphine is a reasonable alternative, even as a first line agent in some women. We are in need of trials regarding new strategies to address the issues of polysubstance abuse, co-morbid psychiatric conditions, and possible medication interactions. ❧
Treatment Alternatives

About the Author
Dr. Kimberly Spence is a Neonatal-Perinatal Medicine and Pediatrics Specialist at SSM Health Cardinal Glennon Children’s Hospital. She specializes in quality improvement initiatives and neonatal abstinence syndrome. Dr. Spence is an assistant professor in the Department of Pediatrics, Division of Neonatology, at Saint Louis University School of Medicine.
10 | vol. 29 | may 2016
Neonatal abstinence syndrome (NAS) is the medical term used to describe the process of neonatal drug withdrawal. In utero drug exposure has been on the rise for the past 10 years. The number of patients with the diagnosis of NAS requiring treatment has increased by two-three times over the past decade. Approximately 6-8% of pregnant women use selective serotonin reuptake inhibitors (SSRIs)1 and illicit drug use is ~16% among pregnant teens and 7.4% among pregnant women aged 18-25 years old.2 The increased prevalence of both SSRI and illicit drug use has led to the growing problem of neonatal abstinence syndrome in nurseries across the United States. The prevalence rates of NAS in 2009 was ~ 4.4 per 1000 live births according to ICD-9 codes, a 10 fold increase over the prior 10 years.3
One of the biggest struggles with NAS is accurately identifying infants at risk for withdrawal. It is often difficult as the history may not be a completely honest one. In addition, many withdrawal symptoms are also symptoms of other common and potentially life-threat-ening neonatal conditions such as sepsis (fever, not eating well and breathing fast), hypoglycemia (jitter-iness and irritability, poor feeding), or a head bleed (hypertonia, irritability). Also complicating the picture is the high rate of polysubstance abuse. The clinician must then try to differentiate among the many overlap-ping symptoms of withdrawal from nicotine vs opioids vs SSRIs (see Table 1).
Organization of a Multidisciplinary Task Force and Policy Development
In order to provide the most comprehensive care to both mom and baby, nurseries must develop a policy to address the screening and evaluation for NAS, as well as its management. This requires organizing a multidisciplinary committee and utilizing their expertise and experience to develop an approach to
the families and infants affected by NAS. This multi-disciplinary committee would likely include bedside nurses who care for moms and babies, a pediatrician, an obstetrician, social worker, pharmacist, and other nursing managers involved in nursery and/or obstetric services. Some committees are also including parents affected by NAS.
This group should develop a policy to address:
1. Screening criteria for both moms and babies (see Table 1)
2. Referral criteria for social work or involvement of child protective services
3. Diagnostic Testing (urine, meconium and/or umbilical cord)
4. Choice of NAS scoring tools such as Finnegan, Modified Finnegan or Neonatal Narcotic Withdrawal Index, etc4
5. Duration of infant observation
6. Standardized non-pharmacologic manage-ment of infants with NAS
7. Standardized pharmacologic management of infants with NAS
8. Identification of discharge and follow-up needs of individual families
Neonatal Abstinence Syndrome:
Evaluation & Management of the Maternal Infant Dyadby Kimberly Spence, M.D.

Table 1 Triggers for Drug Screening Infant
Maternal History Infant
Absent, late, or inadequate prenatal care
SGA neonate (<10%) or IUGR (intrauterine growth restriction) with an unknown etiology
Previously documented/admitted history of drug
abuse or history of positive drug screen
Perinatal depression, unexplained.
Teen pregnancy Neonate clinical signs and symptoms concerning for withdrawal. See Table 2.
Previous unexplained late fetal demise
NA
Repeated spontaneous abortions
Preterm labor, preterm delivery, and/or premature
rupture of membranes
Precipitous labor
Abruptio placentae
Hypertensive episodes
Unexplained maternal behavior- e.g. severe mood swings, anxiety, psychosis,
hallucinations, panic
Cerebrovascular accidents
Myocardial infarctions
STD’s (sexually transmitted diseases) or hepatitis
Gum or periodontal disease- e.g. broken teeth,
severe decay, infections
Significant weight loss, malnourished, low BMI
(body mass index)
Neonatal Abstinence Syndrome
Diagnostic Testing
The choice of diagnostic testing continues to grow. The most common sources for drug testing currently are urine, meconium, and umbilical cord. Urine offers the benefit of a quick screen prior to discharge but is limited by its lack of sensitivity, which is approximately 37%.5 Meconium is another widely available test but is limited by the delay in results by 1-2 weeks. However, its specificity is ~94%.4 We have decided to send both urine and meconium to improve capture rates of drug use while preserving the rapid identification of infants at risk prior to the 48 hour discharge window.
Scoring Tools
SSM Health St. Louis facilities are currently using the Modified Finnegan Scoring Tool.6 Different tools have different advantages. The important thing is to stick with what the nursing staff knows and perform inter-observer reliability testing. Inter-observer reli-ability testing assesses the degree to which different observers (nurses, doctors and therapists) give con-sistent scores of the same observed infant NAS exam. Consistent scoring techniques are critical to optimal medical management of the infant suffering with NAS.
Duration of infant observation
Infants with in utero exposure to short-acting opioids such as heroin should be observed for at least 48 hours prior to discharge to determine if infant will suffer from withdrawal necessitating pharmacologic management. However, infants with in utero drug exposure to narcotics with longer half-lives such as methadone or buprenorphine need to be observed in the hospital for at least 4-5 days to observe for withdrawal. Withdrawl may not take place for up to 7-10 days with buprenor-phine and may be even longer for some infants exposed to methadone depending on the infant’s individual drug metabolism. Close follow-up after dis-charge is necessary to provide ongoing observation for possible signs and symptoms of delayed withdrawal.
Pharmacologic Management
Once scoring techniques are standardized and more consistent, it is important to address standardization of the pharmacologic treatment of NAS. The primary pharmacologic treatment of opioid withdrawal is another opioid such as morphine or methadone. Table 3 addresses the differences between methadone and morphine.4 SSM Health St. Louis hospitals have chosen to begin treatment with morphine sulfate. There are
the PERINATAL Times | 11

Table 2 Drug Class and Withdrawal Signs and Symptoms
Drug class Withdrawal Signs and Symptoms
Opioids Irritability, hypertonia, excessive crying, vomiting, poor weight gain, poor sleeping, uncoordinated sucking reflex with resultant poor feeding, elevated temperature, loose stools, seizures, sneezing, yawning, tremors
Nicotine Irritability, tremors, sleep disturbances8
Cocaine Irritability, hyperactivity, tremors, high-pitched cry and excessive sucking3
SSRIs Crying, irritability, hypertonia, poor suck, feeding difficulty, tachypnea, sleeping disturbance, seizures, tremors3
Neonatal Abstinence Syndrome (continued)
12 | vol. 29 | may 2016
two current approaches to dosing regimens: weight based or score-based protocols. SSM Health has chosen a weight-based approach as that is consistent with how all medications are dosed to neonates. See Table 4 for current dosing guidelines. It is important to note the practicalities of dosing such a small volume; the dosing is linked with the volume that can be measured in a syringe (0.05 ml).
Dose can be titrated according to NAS scores. Dose could be increased by 0.02 mg/kg q3hr, for continued NAS scores >8. There is not a maximum dose of mor-phine per se; dose should be titrated up according to continuing NAS scores >8. However, if infant symptoms are still not controlled on 1 mg/kg/d of morphine and/or there are complications/unacceptable side effects of morphine use, consider changing to methadone or adding clonidine. The infant should be in a level 2 nursery on a cardiorespiratory monitor during dose titration.
Once infant scores have stabilized for 48 hours, wean-ing may be considered. Once a decision is made to wean the drug, this weaning should be done no faster than every 24-48 hours. Weaning should be done only with the NAS scores consistently less than 8 and in the
presence of adequate weight gain. It is recommended to wean the dose by 0.02 mg/kg in increments of 0.05 ml until the starting dose is reached. Once the starting dose has been reached, the frequency of the medica-tion can be adjusted. Recommended interval changes are every 4 hours, to every 6 hours, and then to every 8 hours. If the baby had difficulty on a q 8 hour interval, consider weaning to q12 hours. Once tolerating q8-12 hours for 24-48 hours, stop the morphine and observe for at least 24-48 hours prior to discharge.
Non-pharmacologic management
Non-pharmacologic techniques remain an underutilized and under-valued approach to caring for the infant and family affected by NAS. Non-pharmacologic techniques are critical to delaying and potentially reducing the overall dose of morphine needed to treat infants with NAS (anecdotal evidence). Nursing must learn the accepted techniques and consistently apply them in order to model the behavior and teach parents. Parental education regarding useful techniques for con-soling their infants offers an empowerment opportunity for these mothers and fathers. Non-pharmacologic techniques should start immediately after birth for the at-risk infant.
Treatments include, but are not limited to:
1) swaddling, 2) quiet and dim room, 3) reducing visitors, 4) ensuring rooming in opportunities for parents, 5) skin to skin contact with parent, 6) breast-feeding if eligible, 7) swinging or swaying motion, 8) provide pacifier for non-nutritive sucking, 9) use of light weight (such as muslin) swaddling blankets to reduce chance of elevated temperatures, 10) infant massage, 11) frequent diaper changes, 12) frequent small volume feeds, 13) occupational and physical therapy, and 14) minimal stimulation in general.
Breastfeeding deserves its own mention. Breastfeeding has been shown to reduce treatment duration for infants with NAS on average from 47 to 29 days.7 The amount of actual drug excreted into breast milk is very small.3 Therefore it is more likely the bonding and skin to skin contact that breastfeeding facilitates are responsible for the decreased severity of NAS. Not all moms are eligible to breastfeed. Some contraindi-cations to breast feeding include HIV positive status, polysubstance abuse, and not being enrolled in a drug rehab program. It is important to consider any other relative contraindications as well such as duration of sobriety and psychiatric health of the mother.

Table 3 Morphine versus Methadone4
Morphine Methadone
½ life ~ 4.5-13.3 hrs
Requires more frequent dosing q3-4 vs q6-12hr
½ life ~ 4-62 hrs
Higher risk of drug accumulation and resultant toxicity
Dosage: 0.02-0.05 mg/kg per
dose q3-4hrs
Dosage 0.05-0.1 mg/kg per dose q6 hrs initially. May wean to q12.
Ethanol content: Zero Ethanol content: 8%
Bioavailability: variable but <40%
Bioavailability: 36-100%
Shorter half-life leads to more ups and downs
until steady state is reached.
Longer half-life leads to less ups and downs in drug levels so less chance for withdrawal symptoms at end of dosing interval.
Table 4 Starting doses of morphine based on weight
Weight (kg)
Total morphine dose (volume ) Morphine mg/kg
2.0-2.5 0.04 mg (0.1 ml) ~0.02 mg/kg
2.6-3.5 0.06 mg (0.15 ml) ~0.02 mg/kg
3.6-4.5 0.08 mg (0.2 ml) ~0.02 mg/kg
Neonatal Abstinence Syndrome
the PERINATAL Times | 13
Critical to the management of these infants is parental education and involvement. One big change in the approach to caring for infants and families affected by NAS is the new emphasis on education, empower-ment, and expectations. An educational packet given to families outlines the course of infants with NAS, discusses both pharmacologic and non-pharmacologic treatment, and recommends how to assist in the care of their baby. The packet also contains the scoring tool. The educational packet is reviewed by the bedside nurse so questions can be answered and issues clar-ified. Some nurseries have also developed a contract with families outlining the medical team’s expectations of the family, specifically detailing how long and/or often families are expected to visit (at least daily and stay for several feedings if possible).
In summary
A standardized approach to these families is critical to the safe and successful discharge of infants with NAS. However, as important as policy development is, more important is the dialogue such meetings engender. Integral to the success of this program is having all
services on the same page with regards to the goals for the family as a whole. These meetings provide opportunities to share information on local resources or new barriers identified. Development of a policy does not mean an end to these meetings. NAS is an ongoing problem and requires an ongoing dedicated task force to continue to address the evolving needs of these families affected by NAS. ❧

14 | vol. 29 | may 2016
Neonatal Abstinence Syndrome (continued)
References1 Ornoy A and Koren G. Selective serotonin reuptake inhibitors in human pregnancy: On the way to resolving the controversy. Seminars in Fetal and Neonatal Medicine. 2014; 19: 188-194.
2 Patrick SW et al. Neonatal Abstinence Syndrome and Associated Health Care Expenditures: United States, 2000-2009. JAMA. 2012; 307:1934-40.
3 Hudak ML, Tan RC and the Committee on Drugs and The Committee on Fetus and Newborn. Clinical Report: Neonatal Drug Withdrawal. Pediatrics. 2012; 129: e540-560.
4 Bio L, Siu A and Poon CY. Update on the pharmacologic management of neonatal abstinence syndrome. Journal of Perinatology. 2011; 31: 692–701.
5 Ostrea EM, Brady MJ, Parks PM, Asensio DC, Naluz A. Drug screening of meconium in infants of drug depen-dent mothers. An alternative to urine testing. J Ped. 1989; 115:474-477.
6 D’Apolito, K, and Finnegan, L. Assessing Signs and Symptoms of Neonatal Abstinence Using the Finnegan Scoring Tool. An inter-observer reliability program. NeoAdvances. 2010.
7 Welle-Strand G, Skurtveit S, Jansson LM, Bakstad B, Bjarko L and Ravndal E. Breastfeeding reduces the need for withdrawal treatment in opioid–exposed infants. Acta Paedeatrica. 2013; 102:1060-1066.
8 Pichini S and Garcia-algar O. In utero exsposure to smoking and newborn neurobehavior; how to assess neonatal withdrawal syndrome? Ther Drug Monit. 2006; 28:288-90.

The Monitor Corner
the PERINATAL Times | 15
T he sinusoidal fetal heart rate pattern is a visually apparent smooth sine wave pattern in the fetal heart rate (FHR) baseline with a cycle frequency
of three to five per minute, which persists for at least 20 minutes (Macones et al., 2008). A true sinusoidal FHR pattern is a rare but ominous sign of fetal jeopardy that requires immediate investigation and intervention. It is strongly associated with severe fetal anemia and/or significant fetal acidosis. Fetal anemia can occur as a result of placental abruption or previa, Rh isoimmuni-zation, massive fetomaternal hemorrhage, twin-to-twin transfusion syndrome, ruptured vasa previa, traumatic fetal bleeding, fetal intracranial hemorrhage and certain viral infections (Lyndon, O’Brien-Abel, & Simpson, 2014).
The pathophysiology of the sinusoidal pattern has been debated, but Murata and colleagues (1985) correlated the pattern with elevated levels of arginine vasopressin as seen with post hemorrhagic anemia or acidosis. The hormone has a direct effect on the fetal heart, and the sinusoidal pattern results.
A non-persistent or intermittent, irregular sinusoidal pattern is commonly seen after narcotic administration and/or with fetal sleep cycles, fetal thumb-sucking or rhythmic movements of the fetal mouth (Lyndon, O’Brien-Abel, & Simpson, 2014). This pseudo pattern is
preceded or followed by periods of normal variability and reactivity. In this situation fetal compromise is unlikely, and no intervention is required.
Since these two patterns might easily be confused, Modanlou and colleagues (1982) established six criteria that have been found helpful in accurately defining and interpreting the true sinusoidal FHR pattern. The criteria include the following:
1. Stable baseline FHR of 120-160 bpm with a regular undulating wave form
2. Amplitude of 5-15 bpm
3. Frequency of 2 to 5 cycles per minute
4. Absent variability
5. Oscillation of the sine wave above and below the baseline
6. Absence of acceleration
About the Author
Sharon Rector is an Education Consultant specializing in perinatal nursing at SSM Health - St. Louis.
The Monitor Corner
Sinusoidal Fetal Heart Rate Pattern
by Sharon Rector, MSN, RNC-OB, C-EFM

The Monitor Corner (continued)
16 | vol. 29 | may 2016
When a sinusoidal FHR pattern is suspected, further evaluation of fetal wellbeing might include a fetal stimulation test (scalp or acoustic), contraction stress test or biophysical profile (Nageotte & Gilstrap III, 2009). A positive Kleihauer-Betke test for fetal cells in the maternal blood would also suggest the presence of fetal hemorrhage. A true sinusoidal pattern is a Category III (abnormal) tracing that requires prompt evaluation and intervention that usually includes delivery or intrauterine transfusion.
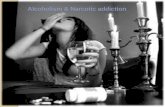
Case Study
The following fetal monitor tracings are from a 32 y/o, G4P2103 admitted at 33 weeks gestation for evaluation of irregular contractions. The nurse’s initial assessment included a FHR baseline of 145 bpm with moderate variability, fetal movement was present and no con-tractions were noted. The nurse was suspicious about the possibility of a sinusoidal pattern. The physician concurred and performed a biophysical profile that resulted in a score of 2 out of 10 with a normal AFI. Betamethasone 12 mg was given IM to accelerate fetal lung maturity. This pattern was observed for about 4 hours. The patient became more uncomfortable with irregular contractions, and no fetal movement was observed. A Maternal-Fetal Medicine consult was obtained, and the specialist was concerned about the sinusoidal pattern. A Kleihauer-Betke test was ordered and the results were positive demonstrating 3.65% fetal cells. The plan was to proceed with delivery.
A baby girl weighing 1950 grams was delivered via cesarean section. Apgar scores were 2 at 1 minute and 7 at 5 minutes. The infant received positive pressure ventilation and was intubated. Her initial hemoglobin
was 2.8 g/dl (normal newborn level is 13.5-18.4 g/dl). She received 2 units of PRBCs, and her condition quickly stabilized. Venous cord blood gases included a pH of 7.07, PCO2 of 49, HCO3 of 14 and base excess of -14.1. Arterial cord blood gases included a pH of 7.04, PCO2 of 52, HCO3 of 14 and base excess of -14.5. The infant did well and was discharged at 1 month of age weighing 2750 grams. ❧
References1 Lyndon, A., O’Brien-Abel, N., & Simpson, K.R. (2014). Fetal assessment during labor. In K.R. Simpson & P.A. Creehan (Eds.), Perinatal Nursing (4th ed., pp. 445-492). Philadelphia: Lippincott Williams & Wilkins.
2 Macones, G.A., Hankins, G.D., Spong, C.Y., Hauth, J., & Moore, T. (2008). The 2008 National Institute of Child Health and Human Development workshop report on electronic fetal monitoring: Update on definitions, interpretation and research guidelines. Journal of Obstetric, Gynecologic, and Neonatal Nursing, 37(5), 510-515.
3 Modanlou, H.D., & Freeman, R.K. (1982). Sinusoidal fetal heart rate pattern: Its definition and clinical significance. American Journal of Obstetrics and Gynecology, 142(8), 1033-1038.
4 Murata, Y., et al. (1985). Experimentally produced sinusoidal fetal heart rate patterns in the chron-ically instrumented fetal lamb. American Journal of Obstetrics and Gynecology, 153(6), 693-702.
5 Nageotte, M.P., & Gilstrap, L.C. (2009). Intrapartum fetal surveillance. In R.K. Creasy & R. Resnick (Eds.), Maternal-Fetal Medicine (6th ed., pp. 397-417). Philadelphia: Saunders Elsevier.

The Monitor Corner
the PERINATAL Times | 17
EFM Strip 1
EFM Strip 2

St. Mary’s Hospital – St. LouisCardinal Glennon Children’s Hospital
SSM Health Cardinal Glennon Children’s Hospital1465 S. Grand Blvd.St. Louis, MO 63104
ADDRESS SERVICE REQUESTED
Continuing Education OpportunitiesMany continuing education opportunities, including traditional lectures, hands-on practice, as well as online presentations, are available for perinatal professionals in eastern Missouri and southern Illinois. These are offered through SSM Health St. Mary’s Hospital – St. Louis, SSM Health Cardinal Glennon Children’s Hospital, Saint Louis University School of Medicine, and the Perinatal Outreach Program. Most programs offer nursing contact hours and/or CMEs.
For course calendars or more specific information on programs, please go to www.cardinalglennon.com and click on the “For Professionals” tab or call the Perinatal Outreach Program at 314-577-5317.
©2016 SSM Health. All rights reserved. SM-STL-16-172723 5/16