ImmunoPET with Anti-Mesothelin Antibody in Patients with ... · of the target and internalization...
12
Personalized Medicine and Imaging ImmunoPET with Anti-Mesothelin Antibody in Patients with Pancreatic and Ovarian Cancer before Anti-Mesothelin Antibody–Drug Conjugate Treatment Laetitia E. Lamberts 1 , Catharina W. Menke-van der Houven van Oordt 2 , Eva J. ter Weele 1,3 , Frederike Bensch 1 , Michiel M. Smeenk 1 , Johannes Voortman 2 , Otto S. Hoekstra 4 , Simon P. Williams 5 , Bernard M. Fine 6 , Daniel Maslyar 6 , Johan R. de Jong 7 , Jourik A. Gietema 1 , Carolien P. Schr € oder 1 , Alphons H.H. Bongaerts 8 , Marjolijn N. Lub-de Hooge 3,7 , Henk M.W. Verheul 2 , Sandra M. Sanabria Bohorquez 6 , Andor W.J.M. Glaudemans 7 , and Elisabeth G.E. de Vries 1 Abstract Purpose: Mesothelin (MSLN) is frequently overexpressed in pancreatic and ovarian cancers, making it a potential drug target. We performed an 89 Zr-PET imaging study with MMOT0530A, a MSLN antibody, in conjunction with a phase I study with the antibody–drug conjugate DMOT4039A, containing MMOT0530A bound to MMAE. The aim was to study antibody tumor uptake, whole-body distribution, and relation between uptake, response to treatment, and MSLN expression. Experimental Design: Before DMOT4039A treatment, pati- ents received 37 MBq 89 Zr-MMOT0530A followed by PET/CT imaging 2, 4, and 7 days postinjection. Tracer uptake was expressed as standardized uptake value (SUV). MSLN expression was deter- mined with immunohistochemistry (IHC) on archival tumor tissue. Results: Eleven patients were included, 7 with pancreatic and 4 with ovarian cancer. IHC MSLN expression varied from absent to strong. Suitable tracer antibody dose was 10 mg MMOT0530A and optimal imaging time was 4 and 7 days postinjection. Tumor tracer uptake occurred in 37 lesions with mean SUV max of 13.1 (7.5) on PET 4 days postinjection, with 11.5 (7.5) in (N ¼ 17) pancreatic and 14.5 (8.7) in (N ¼ 20) ovarian cancer lesions. Within patients, a mean 2.4-fold (1.10) difference in uptake between tumor lesions existed. Uptake in blood, liver, kidneys, spleen, and intestine reflected normal antibody distribution. Tracer tumor uptake was correlated to IHC. Best response to DMOT4039A was partial response in one patient. Conclusions: With 89 Zr-MMOT0530A-PET, pancreatic and ovarian cancer lesions as well as antibody biodistribution could be visualized. This technique can potentially guide individu- alized antibody-based treatment. Clin Cancer Res; 22(7); 1642–52. Ó2015 AACR. Introduction Recognition of tumor-specific molecular characteristics involved in all hallmarks of cancer has led to the development of many targeted cancer drugs (1). Despite the success of targeted cancer drugs, regretfully, for several tumor types, such as pancreatic and ovarian cancer, no important "drugable" targets are available. A promising approach is to use tumor- specific membrane proteins (even those with no known role in tumorigenesis) as targets for toxin delivery by several innova- tive drug types such as immunotoxins and antibody–drug conjugates (ADC; ref. 2). An interesting target molecule in this respect is the membrane-bound surface glycoprotein mesothe- lin (MSLN; ref. 3). The biologic function of MSLN is still largely unknown. It is expressed minimally by normal mesothelial cells lining pleural, pericardial, and peritoneal surfaces (4). Interestingly, besides in mesotheliomas, MSLN is also highly overexpressed in 80% to 100% of pancreatic and ovarian cancers (5–8) and to a lesser extent in several other human cancers (3, 8–10). 1 Department of Medical Oncology, University of Groningen, University Medical Center Groningen, Groningen, the Netherlands. 2 Department of Medical Oncology,VU University Medical Center, Amsterdam, the Netherlands. 3 Department of Clinical Pharmacy and Pharmacology, University of Groningen, University Medical Center Groningen, Gro- ningen, the Netherlands. 4 Department of Radiology and Nuclear Med- icine, VU University Medical Center, Amsterdam, the Netherlands. 5 Department of Early Clinical Development, Genentech, Inc. South San Francisco, California. 6 Department of Biomedical Imaging, Gen- entech, Inc. South San Francisco, California. 7 Department of Nuclear Medicine and Molecular Imaging, University of Groningen, University Medical Center Groningen, Groningen, the Netherlands. 8 Department of Radiology, University of Groningen, University Medical Center Gro- ningen, Groningen, the Netherlands. Note: Supplementary data for this article are available at Clinical Cancer Research Online (http://clincancerres.aacrjournals.org/). Corresponding Author: Elisabeth G.E. de Vries, Department of Medical Oncol- ogy, University Medical Center Groningen, PO Box 30.001, Groningen 9700 RB, the Netherlands. Phone: 0031-50-3612821; Fax: 0031-50-3614862; E-mail: [email protected] doi: 10.1158/1078-0432.CCR-15-1272 Ó2015 American Association for Cancer Research. Clinical Cancer Research Clin Cancer Res; 22(7) April 1, 2016 1642 on February 10, 2021. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from Published OnlineFirst November 20, 2015; DOI: 10.1158/1078-0432.CCR-15-1272
Transcript of ImmunoPET with Anti-Mesothelin Antibody in Patients with ... · of the target and internalization...

Personalized Medicine and Imaging
ImmunoPET with Anti-Mesothelin Antibody inPatients with Pancreatic and Ovarian Cancerbefore Anti-Mesothelin Antibody–DrugConjugate TreatmentLaetitia E. Lamberts1, CatharinaW. Menke-van der Houven van Oordt2, Eva J. terWeele1,3,Frederike Bensch1, Michiel M. Smeenk1, Johannes Voortman2, Otto S. Hoekstra4,Simon P.Williams5, Bernard M. Fine6, Daniel Maslyar6, Johan R. de Jong7,Jourik A. Gietema1, Carolien P. Schr€oder1, Alphons H.H. Bongaerts8,Marjolijn N. Lub-de Hooge3,7, Henk M.W.Verheul2, Sandra M. Sanabria Bohorquez6,Andor W.J.M. Glaudemans7, and Elisabeth G.E. de Vries1
Abstract
Purpose: Mesothelin (MSLN) is frequently overexpressed inpancreatic and ovarian cancers, making it a potential drug target.We performed an 89Zr-PET imaging study with MMOT0530A, aMSLN antibody, in conjunction with a phase I study with theantibody–drug conjugate DMOT4039A, containing MMOT0530Abound to MMAE. The aim was to study antibody tumor uptake,whole-body distribution, and relation between uptake, response totreatment, and MSLN expression.
Experimental Design: Before DMOT4039A treatment, pati-ents received 37 MBq 89Zr-MMOT0530A followed by PET/CTimaging 2, 4, and 7 days postinjection. Tracer uptake was expressedas standardized uptake value (SUV). MSLN expression was deter-mined with immunohistochemistry (IHC) on archival tumor tissue.
Results: Eleven patients were included, 7 with pancreatic and 4with ovarian cancer. IHCMSLN expression varied from absent to
strong. Suitable tracer antibody dose was 10 mg MMOT0530Aand optimal imaging time was 4 and 7 days postinjection. Tumortracer uptake occurred in 37 lesions with mean SUVmax of 13.1(�7.5) on PET 4 days postinjection, with 11.5 (�7.5) in (N¼ 17)pancreatic and 14.5 (�8.7) in (N ¼ 20) ovarian cancer lesions.Within patients, a mean 2.4-fold (�1.10) difference in uptakebetween tumor lesions existed. Uptake in blood, liver, kidneys,spleen, and intestine reflected normal antibody distribution.Tracer tumor uptake was correlated to IHC. Best response toDMOT4039A was partial response in one patient.
Conclusions: With 89Zr-MMOT0530A-PET, pancreatic andovarian cancer lesions as well as antibody biodistribution couldbe visualized. This technique can potentially guide individu-alized antibody-based treatment. Clin Cancer Res; 22(7); 1642–52.�2015 AACR.
IntroductionRecognition of tumor-specific molecular characteristics
involved in all hallmarks of cancer has led to the developmentof many targeted cancer drugs (1). Despite the success oftargeted cancer drugs, regretfully, for several tumor types, suchas pancreatic and ovarian cancer, no important "drugable"targets are available. A promising approach is to use tumor-specific membrane proteins (even those with no known role intumorigenesis) as targets for toxin delivery by several innova-tive drug types such as immunotoxins and antibody–drugconjugates (ADC; ref. 2). An interesting target molecule in thisrespect is the membrane-bound surface glycoprotein mesothe-lin (MSLN; ref. 3). The biologic function of MSLN is still largelyunknown. It is expressed minimally by normal mesothelialcells lining pleural, pericardial, and peritoneal surfaces (4).Interestingly, besides in mesotheliomas, MSLN is also highlyoverexpressed in 80% to 100% of pancreatic and ovariancancers (5–8) and to a lesser extent in several other humancancers (3, 8–10).
1Department ofMedical Oncology, University ofGroningen, UniversityMedical Center Groningen, Groningen, the Netherlands. 2Departmentof Medical Oncology, VU University Medical Center, Amsterdam, theNetherlands. 3Department of Clinical Pharmacy and Pharmacology,University of Groningen, University Medical Center Groningen, Gro-ningen, theNetherlands. 4Department of Radiology andNuclear Med-icine, VU University Medical Center, Amsterdam, the Netherlands.5Department of Early Clinical Development, Genentech, Inc. SouthSan Francisco, California. 6Department of Biomedical Imaging, Gen-entech, Inc. South San Francisco, California. 7Department of NuclearMedicine and Molecular Imaging, University of Groningen, UniversityMedical Center Groningen, Groningen, the Netherlands. 8Departmentof Radiology, University of Groningen, University Medical Center Gro-ningen, Groningen, the Netherlands.
Note: Supplementary data for this article are available at Clinical CancerResearch Online (http://clincancerres.aacrjournals.org/).
Corresponding Author: Elisabeth G.E. de Vries, Department of Medical Oncol-ogy, University Medical Center Groningen, PO Box 30.001, Groningen 9700 RB,the Netherlands. Phone: 0031-50-3612821; Fax: 0031-50-3614862; E-mail:[email protected]
doi: 10.1158/1078-0432.CCR-15-1272
�2015 American Association for Cancer Research.
ClinicalCancerResearch
Clin Cancer Res; 22(7) April 1, 20161642
on February 10, 2021. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst November 20, 2015; DOI: 10.1158/1078-0432.CCR-15-1272

MSLN has been recognized as a potential drug target for morethan 10 years. Several approaches to target MSLN have beeninvestigated in clinical trials, such as inducing antibody-depen-dent cellular toxicity and applying adoptive T-cell immunother-apy (11, 12). An immunotoxin was also developed, with antitu-mor activity shown in phase I/II studies (13–16). Moreover, apreliminary report about MSLN for drug delivery by an ADCwithamaytansinoid cytotoxin showed a partial response (PR) in 1 andstable disease (SD) in 2 mesothelioma patients (17).
Currently, ADCs hold a lot of interest in oncology. Adotrastu-zumab emtansine (T-DM1), recently registered by FDA andEuropean Medicines Agency, prolongs progression-free survival(PFS) and overall survival with less toxicity in human epidermalgrowth factor receptor 2 (HER2)-positive metastatic breast cancerpatients compared with the combination of lapatinib with cape-citabine (18). Moreover, a dozen ADCs for different antigens arein different phases of development. It would be helpful to safelyand accurately predict the behavior of the ADCs in early drugdevelopment (19, 20).
Noninvasive antibody imaging using single photon emissioncomputed tomography (SPECT) and PET, that is, immunoPET,can serve this goal. In general, PET provides better spatial andtemporal resolution than SPECT based on its physical principle ofdetecting coincident gamma pairs instead of single gamma rays.ImmunoPET canbeused to determine target antigen expression atwhole-body level and to provide information about antibodybiodistribution and organ pharmacokinetics, information that isusually lacking from phase I study designs (21). Zirconium-89(89Zr) is the preferred radioisotope for PET imaging of internal-izing targets such as MSLN, as it residualizes in the target tissueafter cellular internalization, causing increasing tumor-to-normaltissue ratios over time (22). Several studieswith 89Zr-immunoPETin cancer patients have shown that after administration of 37MBq(1 mCi) 89Zr-labeled antibody, quantitative assessment of tumoruptake and whole-body biodistribution is feasible (23–28).Labeling a complete ADC with a radioisotope could lead toinstability of the molecule (29, 30). Using the "naked" antibodyfor PET imaging of the target will, however, also provide insight
into drug distribution, because the process that drives traceruptake (i.e., tissue exposure and penetration, and also expressionof the target and internalization of the antibody) is similarand therefore PET with the "naked" antibody of an ADC seemsrational.
In human MSLN–expressing tumor-bearing mice, 89Zr-labeledanti-MSLN antibody MMOT0530A showed progressive and anti-gen-specific tumor uptake on microPET at 1, 3, and 6 days aftertracer injection (31). Therefore, we performed a clinical PET imag-ing study with the "naked" 89Zr-labeled MMOT0530A in conjunc-tion with the phase I study of ADC DMOT4039A, composed ofhumanized IgG1 monoclonal antibody (mAb) MMOT0530A andthe potent mitotic agent monomethyl auristatin MMAE. The aimwas to determine and quantify tumor antibody uptake, whole-body distribution, and organ pharmacokinetics in patients withunresectable pancreatic or platinum-resistant ovarian cancer. Inaddition, the relation between tracer uptake and MSLN expressionand response to DMOT4039A treatment was explored.
Patients and MethodsPatient population
Patients with histologically confirmed, unresectable, and/ormetastatic pancreatic or platinum-resistant ovarian cancer andmeasurable disease according to RECIST 1.1, who were includedin the phase I study with DMOT4039A (ClinicalTrials.gov iden-tifier NCT01469793) in the UniversityMedical Center Groningen(UMCG, Groningen, the Netherlands) or the VU UniversityMedical Center (VUMC, Amsterdam, the Netherlands), wereeligible for this imaging study (ClinicalTrials.gov identifierNCT01832116). Other inclusion criteria were Eastern Coopera-tiveOncologyGroup (ECOG) performance score 0 or 1, adequatebone marrow (absolute neutrophil count � 1.5 � 109/L, hemo-globin � 9 g/dL, and platelet count � 100 � 109/L), liver [totalbilirubin � 1.5 � upper limit of normal (ULN) and aspartateaminotransferase and alanine aminotransferase � 2.5 � ULN],and renal function (serum creatinine � 1.5 � ULN). Majorexclusion criteria were history of severe allergic reactions toantibody therapies and prior treatment with MSLN-targeted ther-apy. This trial was approved by the Medical Ethical Committee ofthe UMCG and the Central Committee on Research InvolvingHuman Subjects, a competent authority in the Netherlands. Allpatients provided written informed consent.
Study designPatients received 37MBq (1mCi) 89Zr-MMOT0530A (effective
radiation dose of approximately 18–22 mSv, based on radiationdosimetry studies of other 89Zr-labeled antibodies with compa-rable characteristics; refs. 32, 33) intravenously andwere observedfor 1 hour to detect any infusion-related adverse events. Todetermine the suitable tracer dose, the first cohort of two patientsreceived 89Zr-labeled MMOT0530A (�1 mg) without any addi-tional unlabeled antibody. In the second cohort, the radiolabeledantibody was complemented with unlabeled antibody to a totalamount of 10 mg MMOT0530A. The unlabeled antibody wascoinfused with the 89Zr-labeled antibody. To determine theoptimal antibody tracer dose, the distribution of the tracer in thebody as a whole was analyzed. From other antibody tracers, weknow that an additional dose of unlabeled antibody is oftenneeded for imaging.When the amount of tracer still present at day7 postinjection is high enough to visualize the circulation clearly,
Translational Relevance
Mesothelin (MSLN) has been recognized as an interestingtarget for immunotoxins and antibody–drug conjugates(ADC). DMOT4039A, composed of anti-MSLN antibodyMMOT0530A and cytotoxic agent MMAE, is evaluated inpatients with pancreatic and ovarian cancer. In early drugdevelopment, information regarding target presence, organdistribution at the whole-body level, as well as binding of theantibody to the target could be extremely helpful to guide andindividualize drug dosing. This study shows that immunoPETwith the 89Zr-labeled MMOT0530A is able to visualize whole-body distribution and quantify uptake in pancreatic andovarian tumor lesions. Whole-body organ-level uptake of thetracer was highest in liver. Tumor lesion uptake betweenpatients and within patients varied. These data support furtherdevelopment of more immunoPET tracers consisting of the"naked" antibody of an ADC to determine whole-body targetexpression and organs at risk for toxicity, to ultimately guidedosing and confirm delivery of the ADC.
Mesothelin Imaging in Pancreatic or Ovarian Cancer Patients
www.aacrjournals.org Clin Cancer Res; 22(7) April 1, 2016 1643
on February 10, 2021. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst November 20, 2015; DOI: 10.1158/1078-0432.CCR-15-1272

we consider this to be the consequence of an adequate proteindose in the tracer. To determine the optimal day for PET scanning,we analyzed all lesions and all organs at all 3 PET scans for eachpatient. The PET moment on which an adequate tracer amountwas present in the circulation and most tumor lesions in mostpatients hadmaximumtracer uptakewas considered tobe thebestPET scan.
Clinical grade 89Zr-MMOT0530A was produced in the UMCGessentially as was described previously (31, 34). PET scans wereacquired from the top of the skull to mid-thigh with a 64-slicePET/CT camera (Biograph mCT, Siemens in the UMCG andGemini TF or Ingenuity TF, Philips in the VUMC), for 5 minutesper bed position at day 2 and 4, and 10 minutes per bed positionat day 7 after tracer injection. For attenuation and scatter correc-tion, immediately after the PET scan, a low-dose CT scan wasacquired with the same PET/CT camera, as part of the sameprocedure.
Diagnostic CT scans were performed within 21 days beforetracer injection and after every 2 cycles of DMOT4039A. CT scanswere evaluated centrally at UMCG for measurable lesions accord-ing to RECIST 1.1 (35). After the last PET scan (either on the sameday or within a week thereafter), patients continued in the phase Istudy and received treatment with DMOT4039A (36). Archivaltumor tissue (both primary andmetastatic tissue, if available) wastested for MSLN expression with an immunohistochemical assayusing 19C3 mouse anti-human antibody (37). Immunohisto-chemical scoringwas based on at least 10%of tumor cells stainingpositive, scoring 3þ for strong, 2þ formoderate, 1þ forweak, and0 for <10% cells staining.
89Zr-MMOT0530A PET analysisAll PET scans were reconstructed similarly (256 matrix, 3
iterations, 21 subsets, and 8-mm filters) and visually analyzedby an experienced nuclear medicine physician. All regions withhigh tracer uptake, compared with normal organs, were furtheranalyzed using diagnostic CT and the number and locations ofvisible tumor lesions on the PET scan were determined. Quan-tification of radioactivity concentration in tumor lesions andnormal organs was performed using A Medical Image DataExaminer (AMIDE) software (version 0.9.3, Stanford Universi-ty, Stanford, CA; ref. 38). In addition to the amount of injectedactivity and bodyweight, the amount of radioactivity within alesion or organ served to determine the standardized uptakevalues (SUV). To assess the present radioactivity, three-dimen-sional spherical volumes of interest (VOI) were manuallydrawn around tumor lesions. To assess the biodistribution ofthe tracer background, VOIs were drawn in the circulation(measured in the left ventricle), liver, spleen, kidney, intestine,lung, brain, bone marrow, femur head, and thigh muscle. Toassess the radioactivity concentration in tumor lesions andorgans, SUVmax (the maximum voxel intensity in the VOI) wascalculated. Tumor-to-blood ratios (TBR) were determinedusing SUVmax in tumor lesions and SUVmax in blood pool. Inaddition, to calculate the percentage of the tracer in the liver, inall PET scans of all patients, the liver was three-dimensionallydelineated and the volume of the liver with the correspondingradioactivity concentration present in the liver at that PETmoment was calculated. Subsequently, the total liver traceruptake was expressed as percentage of radioactivity still presentin the whole body at that PET scan (hereby correcting for89Zr-decay and excretion both).
Pharmacokinetic assessmentsBlood samples for pharmacokinetic analyses of 89Zr were
collected at 5 time points: before and 15 minutes postinjection,as well as at day 2, 4, and 7 postinjection (same days as the PETscans). Radioactivity wasmeasured in 1mLwhole blood samplesper time point by use of a calibrated well-type gamma-counter(LKB Instruments). Thereafter, radioactivity (determined in activ-ity permL) was converted to SUV equivalent values, using weight,injected amount of radioactivity, andmoment of blood sampling(thereby correcting for 89Zr decay). The SUV uptake in the circu-lation determined by PET was correlated to the calculated SUVvalue in the blood samples at the corresponding days.
In addition, the apparent clearance (Cl), volume of distri-bution (Vd), and elimination half-life (t1/2) of 89Zr-labeledMMOT0530A were calculated using a noncompartmental phar-macokinetic model in the "KINFIT module" of the softwarepackage MWPharm v 3.81 (Mediware).
Statistical analysesData are presented as mean � SD. Associations between para-
meters were calculated using the Pearson correlation test (CP) fortwo continuous variables and the Spearman correlation test (CS)for one continuous andone categorical variable. An independent ttest was performed to compare tumor uptake between pancreaticand ovarian cancer lesions. P values < 0.05 were consideredsignificant.
ResultsPatient characteristics
Between March 2013 and February 2014, a total of 11 patients(7 patients with pancreatic and 4 patients with ovarian cancer)eligible for participation in the phase I study with DMOT4039A,were consecutively enrolled in this study; 2 men and 9 womenwith a median age of 62 years (range 44–70) (Table 1). Threeprimary pancreatic tumors and two primary ovarian tumors werestill in situ at the moment of trial participation.
89Zr-MMOT0530A PETThe first 2 patients received only 89Zr-labeled MMOT0530A
(�1 mg protein dose) without additional unlabeled antibody,the 9 patients thereafter were administered 89Zr-labeledMMOT0530A and unlabeled MMOT0530A antibody in a totalamountof 10mg (range9.4–10.4). Themean radioactivity at timeof injection was 36.78 MBq (�1.26). No infusion-related reac-tions or adverse events were observed in this imaging study.
Tracer dose and organ distribution. In the first 2 patients, whoreceived approximately 1mg 89Zr-MMOT0530A,mean SUVmax inthe circulation (measured in the left ventricle on PET scans)decreased fast from 9.2 (�1.6) on day 2 to 6.0 (�2.0) on day4 to 3.6 (�0.2) on day 7 postinjection. In the next 9 patients, inwhom approximately 10 mg additional cold MMOT0530A wasadministered, more labeled antibody remained in the circulationwith amean SUVmax of 10.2 (�3.2), 8.3 (�2.1), and6.8 (�2.9) onday 2, 4, and 7 postinjection, respectively (Supplementary Fig.S1A). With a mean SUVmax of 6.8 (�2.9) at day 7 postinjection,sufficient tracer was available for ongoing tumor uptake until day7 postinjection. Moreover, visibility of tracer present in thecirculation improved using 10 mg of unlabeled antibody addedto the labeled MMOT0530A (Fig. 2A–C). Therefore, a suitable
Lamberts et al.
Clin Cancer Res; 22(7) April 1, 2016 Clinical Cancer Research1644
on February 10, 2021. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst November 20, 2015; DOI: 10.1158/1078-0432.CCR-15-1272

tracer dose was determined to be a total of 10 mg MMOT0530A(of which �1 mg was 89Zr-labeled).
The 89Zr-MMOT0530A organ distribution showed (based onthePET scan4days postinjection) ahigh SUVmax in the circulation(7.9� 2.2), aswell as in the liver (13.2� 4.1), kidneys (9.1� 4.5),and the spleen (8.0 � 3.4). The high intestinal mean SUVmax atday 4 of 8.0 (� 2.7) reflected excretion with highest uptake inpatients with habitual constipation. Low uptake was observed inmuscle (2.4� 1.3), lung (2.4� 1.0), bone (1.5� 0.6), and braintissue (1.1 � 0.3).
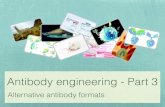
The tracer distribution on the three consecutive PET scans wascomparable between patients. The widest ranges were observedfor the liver (Supplementary Fig. S1B) and kidneys (Supplemen-tary Fig. S1C) and to a lesser extent also for the blood pool, spleen,and intestine. Mean SUVmax in the liver was 11.1 (�3.3), 13.2(�4.1), and 14.7 (�5.8) and in the kidney 8.3 (�2.6), 9.1 (�4.5),and 9.0 (�3.7) on PET 2, 4, and 7 days post injection, respectively.Mean SUV on PET scan series showed a decline in tracer in theblood pool as expected. The other organs showed stable traceruptake over time. Figure 1 shows the organ distribution for thePET scans 2, 4, and 7 days postinjection for all patients.
On the PET scans, we determined amean liver volume of 1.60 L(�0.26 L). The absolute liver uptake was decreasing over timewith a radioactivity level of 3.68MBq (�7.38), 2.58MBq (�3.57),and 1.39 MBq (�2.76) on PET at days 2, 4, and 7, respectively.However, the percentage injected dose of radioactivity per gramofliver tissue (assuming a tissue density of 1 g/mL; %ID/g) wasincreasing over time, with a mean %ID/g of 0.82 (�0.30), 1.00(�0.29), and 1.07 (�0.31) on PET at 2, 4, and 7 days postinjec-tion, respectively. The mean liver uptake at PET 4 days postinjec-tion was in the first cohort 22.5% (22.6% and 22.47%) and in thesecond cohort 18.2% (�2.4).
The pharmacokinetic variables shown in Table 2 are presentedfor both cohorts. The 89Zr-MMOT0530A clearance measured in
whole blood in cohort 1was2-fold faster as comparedwith cohort2; with 0.066 L/hour in cohort 1 compared with 0.033 L/hour incohort 2. Consequently, t1/2 was also shorter in cohort 1 (70hours) than in cohort 2 (105 hours).
Tracer uptake in tumor lesions. 89Zr-MMOT0530A uptake wasobserved in at least one tumor lesion in all patients (range 1–8per patient). Representative PET/CT scans from one pancreaticcancer patient are shown in Fig. 2.Weused the PET scanof day 4 topresent the tumor uptake analyses, as on this PET scanmost tumorlesions had maximum uptake and an adequate amount of tracerwas available in the circulation (Fig. 3). Because of the decay of89Zr, the PET scans at day 7 weremore difficult to analyze visuallyand at day 2 tumor uptake did not yet reach its maximum. MeanSUVmax of all lesionswas 13.1 (�7.5) onPET 4days postinjection.A total of 37quantifiable tumor lesionswere detected, ofwhich36were also visible on the diagnostic CT scan. One lesion, a lymphnode in the neck, was positioned outside the field-of-view of theCT scan. Eleven of the 37 lesions were not measurable accordingto RECIST 1.1 due to being cystic (n ¼ 3), peritoneal localization(n¼4), or adiameter of<15mmon the short axis in case of lymphnodes (n ¼ 4).
Heterogeneity was present between and within patients as89Zr-MMOT0530A tumor uptake varied greatly. No clear patternwas found to explain the heterogeneity in tumor uptake. MeanSUVmax onPET 4days postinjection onpatient-based analysiswas13.4 (�6.9) with a 5.3-fold difference in mean tumor uptakebetween patients. The lowest mean SUVmax was 5.1 in a patientwith pancreatic cancer and the highest was 27.2 in a patient withovarian cancer. Also, a large intrapatient variation of the tumorSUVmax values was found within 8 patients with more thanone lesion, with a mean difference of 2.4-fold (�1.1). MeanSUVmax on day 4 postinjection was 14.4 (�13.7) for primarytumor lesions (n ¼ 5), and 12.9 (�6.4) for metastatic
Brain
Mea
n SU
V max
0
5
10
15
20
Abdcavity
Bone Muscle Lung Bonemarrow
Intestine Spleen Blood pool Kidney Liver
Figure 1.89Zr-MMOT0530A tracer uptake innormal organs of all patients on PETon 2, 4, and 7 days postinjection inblue, green, and yellow bars (n ¼ 11),respectively. Error bars display SD.Abd cavity, abdominal cavity.
Mesothelin Imaging in Pancreatic or Ovarian Cancer Patients
www.aacrjournals.org Clin Cancer Res; 22(7) April 1, 2016 1645
on February 10, 2021. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst November 20, 2015; DOI: 10.1158/1078-0432.CCR-15-1272

lesions. Figure 4 shows tumor uptake for all tumor lesions perpatient and per disease.
Tracer uptake differed between lesions of patients with pan-creatic and ovarian cancer (Fig. 5). Mean SUVmax on day 4postinjection in lesions of pancreatic cancer (n ¼ 17) was 11.5(�5.6), while in those of ovarian cancer (n ¼ 20) this was 14.5(�8.7; P ¼ 0.221). Five patients had primary tumors in situ. Thetwo primary ovarian cancers had a SUVmax of 8.4 and 38.91,respectively. In the primary pancreatic tumors (n ¼ 3), meanSUVmax was 8.2 (�0.9). Metastatic tumor lesions of pancreaticorigin (n ¼ 14) had a mean SUVmax of 12.1 (�6.0), whereas formetastatic lesions of ovarian cancer origin (n ¼ 18) this was 13.5(�6.9). TBR was rising over time for all except one patient; meanTBR for all patients was 0.9 (�0.4) at PET 2 days postinjection, 1.7(�0.8) and 2.3 (�1.2) at PET 4 and 7 days postinjection, respec-
tively. In patients with pancreatic cancer, the TBR [0.9 (�0.4), 1.5(�0.8), and 1.9 (�1.1)] was lower than in patients with ovariancancer [1.0 (�0.4), 1.9 (�0.8), and 2.6 (�1.3)]. Primary pancre-atic lesions had a TBR of 0.70, 1.1, and 1.28 at PET 2, 4, and 7 dayspostinjection, respectively.
Six measurable lesions on diagnostic CT, according to RECIST1.1, were not visible on PET. This was the case for one abdominaltumor mass (maximum diameter 30 mm) in a patient withovarian cancer, for a retroperitoneal lymph node (15 � 16 mm)in a patient with pancreatic cancer and for 2 lung lesions (�10mm) in a patient with pancreatic cancer, and 2 liver lesions(maximum diameters 16 and 11 mm) in a pancreatic cancerpatient in whom other liver metastases were visible (uptake didnot correspond with metastases on CT). Furthermore, cysticlesions, some peritoneal lesions, and 9 small lymph nodes
Figure 2.89Zr-MMOT0530A PET in a pancreaticcancer patient day 2 (A), day 4 (B), andday 7 (C) after tracer injection, showingwhole-body distribution with highestuptake in circulation (heart), liver,kidneys, and primary tumor (red circle).A fusion with diagnostic CT shows theprimary pancreatic tumor (red circle)and the high liver uptake in healthyliver (D).
Lamberts et al.
Clin Cancer Res; 22(7) April 1, 2016 Clinical Cancer Research1646
on February 10, 2021. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst November 20, 2015; DOI: 10.1158/1078-0432.CCR-15-1272

(<15mm short axis on diagnostic CT)were not visualized on PET.Interestingly, in one patient with pancreatic cancer, high uptakewas observed in both adrenal glands (SUVmax on day 4 postin-jection were 21.6 in the right and 19.9 in the left adrenal gland),while on diagnostic CT, the adrenal glands were classified as fattyadenoma.
Correlation 89Zr-MMOT0530A blood pool activity on PETversus 89Zr activity in blood samples
In 8 patients, whole blood samples for 89Zr activity measure-ments were available. The SUV equivalents from ex vivo mea-surements of blood samples at 2, 4, and 7 days postinjectioncorrelated well with image-derived SUV values of the bloodpool measured by PET (Pearson correlation 0.765, P ¼ 0.000;Fig. 6).
MSLN IHC expression versus PET uptakeMSLN expression levels determined in primary (n ¼ 7) and
metastatic (n¼ 7) archival tumor samples varied from 0 to 3þ in10 patients (Table 1). Primary tissue was available in 3 of the 4patients with ovarian cancer, and metastatic tumor tissue wasavailable in only 1 patient. Archival tissue was available in 6 of7 patients with pancreatic cancer, only metastatic tissue in2 patients, and both primary and metastatic tissue in 4 patients.IHC score was 0 in both primary and metastatic tissue in onepatient, while in one patient, the IHC score was higher in primarycompared with metastatic tissue (IHC score 3þ vs. 2þ). In allothers, the immunohistochemical scores were consistent.
On a patient-based analysis, the immunohistochemical scorecorrelated with the mean SUVmax per patient on PET day 4(Spearman correlation 0.689, P ¼ 0.027). However, no correla-tion was found when the two tumor types were analyzed sepa-rately. In ovarian cancer, the correlation coefficientwas 0.775 (P¼0.225). For pancreatic cancer tissue, the correlation coefficientwas0.676 (P ¼ 0.14).
Response to DMOT4039A and PET uptakeFive patients received the weekly schedule (dose 0.8–1.2
mg/kg) and 6 patients the every-3-week schedule (dose 2.4–2.8mg/kg) ofDMOT4039A. In 9of 11patients, best responsewas SD,one patient experienced immediate progressive disease (PD), andone patient had a confirmed PR ongoing for 311þ days. Ninepatients with stable disease and one with PR had a mean PFS of121 days (range 28–311þ, from start of treatment to PD; ref. 35).PET uptake on a per-patient basis (mean PET uptake over alllesions in one patient) did not correlate with PFS (CP�0.101, P¼0.768). On a per-lesion analysis of 26 lesions that were measur-able according to RECIST 1.1, there was no correlation betweenPET uptake and best response onCT in percentage compared withbaseline (CP �0.06, P ¼ 0.786). The patient with ongoing PRshowed PET tracer uptake in 2 liver metastases and in the primarypancreatic tumor (Fig. 7), with SUVmax values on PET 4 dayspostinjection of 21.0, 12.0, and 7.4, respectively.
DiscussionThis is the first-in-human study evaluating anti-MSLN anti-
body tumor uptake and whole-body distribution, using thenaked antibody of an ADC with 89Zr-MMOT0530A PET forwhole-body antibody distribution. In addition to primarypancreatic and ovarian cancers, metastatic lesions were alsovisualized.
A relatively small amount of 10mgMMOT0530Awas found tobe a suitable protein dose for PET imaging. With a lower proteindose, presence of the tracer in the circulation was too low at day 7tobeoptimally visualized and consequentlywould likely prohibitoptimal tumor uptake. The optimal moment for PET scanningwas 4 days after tracer injection, because most tumor lesions hadmaximum uptake at that moment. Although tumor-to-back-ground ratios were lower at day 4 than day 7 they were easierto analyze given the ongoing decay of 89Zr.
Invasive determination of 89Zr in whole blood was completelyin line with the PET findings. In patients who received 1 mgantibody (cohort 1), the 89Zr-labeled MMOT0530A half-life wasshorter than the patients receiving 10 mg antibody (cohort 2).This is most likely due to faster antibody clearance in the firstcohort with the lower antibody dose. For certain antibody-based
40
30
SUV m
ax p
er le
sion
20
10
02 4 7
Figure 3.89Zr-MMOT0530A PET uptake expressed in SUVmax (on y-axis) on 2, 4, and 7days, respectively, on x-axis for all 37 tumor lesions.
40
30
20
10
01 2 4 5 6
Patient number
SUV m
ax P
ET 4
day
s pi
7 8 9 10 113
Figure 4.SUVmax values at PET 4 days postinjection of all quantifiable tumor lesions(n ¼ 37) plotted per patient on the x-axis (7 pancreatic cancer patientswith 17 lesions in open dots and 4 ovarian cancer patients with 20 lesions inblack filled dots). Squares, primary tumor lesions; circles, metastatic lesions.pi, postinjection.
Mesothelin Imaging in Pancreatic or Ovarian Cancer Patients
www.aacrjournals.org Clin Cancer Res; 22(7) April 1, 2016 1647
on February 10, 2021. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst November 20, 2015; DOI: 10.1158/1078-0432.CCR-15-1272

tracers with dose-dependent antibody kinetics, higher doses ofunlabeled antibody are needed to counteract the rapid clearanceat lower doses (39, 40).
89Zr-MMOT0530A uptake in liver is relatively high and risesover time in contrast to other uptake in other organs. Thismight be due to hepatic catabolism of MMOT0530A asopposed to target antigen expressed, as MSLN is not normallyexpressed in normal liver. Hepatic catabolism might be pro-moted by the antibody complexing with MSLN antigen shedinto the circulation. Shedding of antigen into the tumor inter-stitium is a well-known process for cell-surface proteins includ-ing MSLN, which can also influence tumor uptake of MSLNtargeting agents in preclinical models (41, 42). However, liveruptake levels of this antibody are comparable with that of otherantibodies, such as trastuzumab and huJ591 (26, 43). The highuptake in the liver suggests that it is appropriate to monitor theliver as a potential site of toxicity with the ADC DMOT4039A.In the phase I study, the dose-limiting toxicities were hypopho-sphatemia and hyperglycemia and clinically significant livertoxicity, expressed as liver function abnormalities, occurred inless than 10% of the patients (36).
89Zr-MMOT0530A tumor uptake was heterogeneous betweenand within patients. We observed a mean 5.3-fold differencebetween, and 2.4-fold difference within patients. Inter- and intra-patient heterogeneity is a widely acknowledged phenomenon inoncology, especially since the multiregion sequencing of tumorsamples from primary renal carcinomas and their metastatic sitesshowed in 4 patients that target heterogeneity was not onlypresent between different lesions within one patient, but evenwithin one lesion (44). By recognizing the existence and extent ofheterogeneity, PET imaging of a tumor-specific target adds valu-able information for individualized treatment decisions.
MSLN-specific tracers have been developed (from differentantibodies) for SPECT, as well as PET. A Copper-64 (64Cu)-antiMSLN Fab fragment visualized MSLN-expressing xenograftedtumors, as did several Indium-111(111In)-labeled anti-MSLNantibodies (45–48). Moreover, an antibody targeting MSLN wasrecently conjugated to quantum dots encapsulated in micelles todetect human tumor xenografts in mice (49).
In the preclinical study preceding this clinical trial, 89Zr-MMOT0530A was used for PET imaging of MSLN-expressinghuman pancreatic tumor xenografts (31). Antigen-specific tracer
Figure 5.PET images 4 days postinjection froma patient with pancreatic cancer withthe primary tumor (SUVmax ¼ 9.17)encircled in red and SUVmax of 9.55 inthe healthy liver (A); a patient withovarian cancerwith ametastasis in theligamentum falciparum encircled withSUVmax of 16.6. SUVmax in the healthyliver is 12.9 (B).
12
10
8
6
4
2
05 10
SUVmax on PET
SUV
in 1
mL
who
le b
lood
15
Figure 6.Correlation between SUV in 1 mL whole blood samples at day 2, 4, and 7 after89Zr-MMOT0530A injection and SUVmax of blood pool as measured in the leftventricle on corresponding PET scans (n ¼ 8 patients). Blue, day 2postinjection; green, day 4 postinjection; gray, day 7 postinjection. Pearsoncorrelation 0.765, P ¼ 0.000.
Table 1. Patient characteristics at baseline
Characteristics All patients, n ¼ 11
Pancreatic cancer (n) 7Ovarian cancer (n) 4Gender, male/female (n) 2/9Age (median in years, range) 62, 44–70Primary tumor in situPancreatic cancer (n) 3Ovarian cancer (n) 2
Tumor lesions on PET scann, range per patient 37, 1–8
IHC MSLN expression on primary tumorn (disease type)0 1 (pancreatic cancer)1þ 02þ 4 (2 ovarian cancer, 2 pancreatic cancer)3þ 2 (1 ovarian cancer, 1 pancreatic cancer)Unknown 4 (1 ovarian cancer, 3 pancreatic cancer)
IHC MSLN expression on metastatic tumorn (disease type)0 1 (pancreatic cancer)1þ 02þ 6 (1 ovarian cancer, 5 pancreatic cancer)3þ 0Unknown 4 (3 ovarian cancer, 1 pancreatic cancer)
Lamberts et al.
Clin Cancer Res; 22(7) April 1, 2016 Clinical Cancer Research1648
on February 10, 2021. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst November 20, 2015; DOI: 10.1158/1078-0432.CCR-15-1272

uptake occurred with increasing uptake over time; mean TBRincreased from 0.5 via 1.3 to 2.4 at 24, 72, and 144 hourspostinjection, respectively.
In general, radionuclide-labeled antibody uptake is higher intumor lesions of patients than in xenografted animal models.However, in the current clinical study, TBRs in primary pancre-atic cancer lesions were relatively low and lower than in the
subcutaneously implanted human pancreatic tumors in thepreclinical study. This difference may be explained by the higherinjected dose of about 1 MBq with 0.5 mg/kg MMOT0530A permice than the dose administered in humans. In pancreaticcancer, there is a known discrepancy between results in preclin-ical assays and clinical findings of new drugs. A possible causemight be the influence of the microenvironment in humanpancreatic cancer. It has been suggested that the pancreaticstromal tissue diminishes tumor perfusion and thereby tumorpenetration and delivery of therapeutics in adequate doses (50).In the preceding preclinical assessment of this tracer, the pan-creatic tumors in mice did not contain the same relative amountof stromal tissue as human pancreatic tissue, which may explainthe difference in TBR between the preclinical and the currentclinical study. Interestingly, primary tumor lesions in pancreaticcancer patients could be visualized, indicating that the antibodydid reach these lesions. This was also the case in a recent small
Table 2. 89Zr pharmacokinetics in whole blood samples
Mean (�SD) Mean (�SD)Parameter Cohort 1 (n ¼ 2) Cohort 2 (n ¼ 6)
Cl (L/h) 0.066 (0.014) 0.033 (0.004)Vd (L) 6.66 (1.433) 4.90 (0.876)t1/2 (h) 70.36 (0.297) 105.17 (22.131)
NOTE: Cohort 1,�1 mg 89Zr-labeled MMOT0530A; Cohort 2,�1 mg 89Zr-labeledMMOT0530A supplemented with unlabeled MMOT0530A to a total of 10 mgMMOT0530A.
Figure 7.Images from the patient with pancreaticcancer with liver metastases who has anongoing partial response according toRECIST 1.1 during the writing of thisarticle. A, maximum intensity projection(MIP) image; B, overlay with CT of the89Zr-MMOT0530A PET scan performed4 days postinjection; C, baseline CT scanwith liver metastases; D, CT scan after 8cycles of DMOT4039A treatment,without measurable or visible livermetastases.
Mesothelin Imaging in Pancreatic or Ovarian Cancer Patients
www.aacrjournals.org Clin Cancer Res; 22(7) April 1, 2016 1649
on February 10, 2021. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst November 20, 2015; DOI: 10.1158/1078-0432.CCR-15-1272

study, in 4 patients with mesothelioma and 2 patients withpancreatic cancer. Here, 4 mCi 111In-labeled MSLN antibodyamatuximab was administered and subsequent SPECT showeduptake in pancreatic cancer lesions but a higher uptake inmesothelioma lesions (51).
Although not statistically significant, we saw in our study asimilar pattern as 89Zr-MMOT0530A PET showed a higher uptakein ovarian cancer lesions compared with pancreatic cancer lesions(mean SUVmax of ovarian versus pancreatic lesions were 14.5versus 11.5, respectively). This might indicate that pancreatictumor tissue is more difficult to be reached by antibodies thanmesothelioma or ovarian cancer lesions, possibly due to extensivestromal tissue in pancreatic cancer.
Moreover, in twopatientswith pancreatic cancer, themetastaticlesions showed higher tracer uptake than the primary lesions (1.9and 2.9 fold, respectively). For one of these two patients, bothprimary andmetastatic tissues (a biopsy from lymph nodes) wereavailable for MSLN expression analysis: the primary tumorshowed a higher expression (3þ) than the metastatic tissue(2þ). This again suggests heterogeneity between primary andmetastatic lesions, which might explain the differential antibodyPET uptake. Overall, immunohistochemical score correlated wellto the mean PET uptake in all lesions in a patient.
MSLN expression determined by IHC did not correlate withPET uptake in this study. IHC was performed on archival tumortissue obtained during surgery or frombiopsies.MSLN expressionmay have changed over time, and intrapatient heterogeneity willlikely play a role as well. For a better understanding about therelation between target expression based on IHC and targetexpression based on PET uptake, fresh tumor biopsies would bemost informative. However, this will still provide informationabout a small part of a tumor lesion, whereas with PET, the wholelesion is being assessed. In addition, other factors such as differ-ences in perfusion can also affect antibody uptake by tumorlesions.
Recently, two ADCs in development for prostate cancer,STEAP1 and TEN2B, have been radiolabeled with 89Zr for PETimaging inmice (52). Tumor tracer uptakewas rising in parallel tothe efficacy of the ADC treatment, suggesting resemblingmechan-isms for uptake. As the stability of the ADC is uncertainwhenboththe cytotoxin and the radionuclide are attached to the antibody,we chose to label the naked antibody for PET imaging.
Apart from providing information for early drug developmenton tracer–antibody organ distribution (and potential organs atrisk of toxicity) and tracer–antibody accumulation in the differenttumor lesions, this imaging approach might also be of interest inlater stages of drug development to select patients that are mostlikely to benefit from the treatment. As an example, the ZEPHIRstudy (ClinicalTrials.gov identifier NCT01565200) assesses thepredictive value of pretreatment 89Zr-trastuzumab PET in meta-static breast cancer patients before treatment with the ADC T-DM1. In an exploratory patient-based analysis, the combination
of 89Zr-trastuzumab PET and an early 18-Fluorine (18F) fluoro-deoxyglucose (FDG) PET showed a negative predictive valuefor RECIST response of 100%, indicating the combined techni-ques to be promising in identifying patients unlikely to respondto T-DM1. Interestingly, this imaging study also showed highlyheterogeneous 89Zr-trastuzumab uptake between and withinpatients (53).
Given our findings, 89Zr-MMOT0530A PET may be of interestto be used in future trials with DMOT4039A as a complementarytool to select patients with the highest chance of benefit fromtreatment with DMOT4039A.
Disclosure of Potential Conflicts of InterestB.M. Fine and D. Maslyar have ownership interest (including patents) in
Roche. No potential conflicts of interest were disclosed by the other authors.
Authors' ContributionsConception and design: L.E. Lamberts, S.P. Williams, B.M. Fine, D. Maslyar,E.G.E. de VriesDevelopment of methodology: L.E. Lamberts, S.P. Williams, J.R. de Jong,C.P. Schr€oder, M.N. Lub-de Hooge, E.G.E. de VriesAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): L.E. Lamberts, C.W. Menke-van der Houven vanOordt, F. Bensch, M.M. Smeenk, J. Voortman, O.S. Hoekstra, D. Maslyar,C.P. Schr€oder, A.H.H. Bongaerts, M.N. Lub-de Hooge, A.W.J.M. Glaudemans,E.G.E. de VriesAnalysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis): L.E. Lamberts, C.W. Menke-van der Houven vanOordt, E.J. ter Weele, F. Bensch, M.M. Smeenk, J. Voortman, B.M. Fine,D. Maslyar, J.R. de Jong, J.A. Gietema, C.P. Schr€oder, S.M. Sanabria Bohorquez,A.W.J.M. Glaudemans, E.G.E. de VriesWriting, review, and/or revision of the manuscript: L.E. Lamberts,C.W.Menke-van derHouven vanOordt, E.J. terWeele, F. Bensch,M.M. Smeenk,J. Voortman, O.S. Hoekstra, S.P. Williams, B.M. Fine, D. Maslyar, J.R. de Jong,J.A. Gietema, C.P. Schr€oder, M.N. Lub-de Hooge, H.M.W. Verheul, S.M.Sanabria Bohorquez, A.W.J.M. Glaudemans, E.G.E. de VriesAdministrative, technical, or material support (i.e., reporting or organizingdata, constructing databases): L.E. Lamberts, F. Bensch, M.M. Smeenk,D. Maslyar, C.P. Schr€oder, A.W.J.M. Glaudemans, E.G.E. de VriesStudy supervision: C.W. Menke-van der Houven van Oordt, H.M.W. Verheul
AcknowledgmentsThe authors thank Linda Pot, Rianne Bakker, and Annelies Jorritsma for the
labeling procedures and Paul van Snick, Cemile Karga, and Marc Huisman fortheir assistance with PET data transfer.
Grant SupportE.G.E. de Vries received an ERC advanced grant OnQview. Financial support
for the study was provided by Genentech to the UMCG.The costs of publication of this articlewere defrayed inpart by the payment of
page charges. This article must therefore be hereby marked advertisement inaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
ReceivedMay29, 2015; revisedOctober 16, 2015; acceptedOctober 20, 2015;published OnlineFirst November 20, 2015.
References1. Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation. Cell
2011;144:646–74.2. Teicher BA, Chari RV. Antibody conjugate therapeutics: challenges and
potential. Clin Cancer Res 2011;17:6389–97.3. Hassan R, Bera T, Pastan I. Mesothelin: a new target for immunotherapy.
Clin Cancer Res 2004;10:3937–42.
4. Chang K, Pastan I. Molecular cloning of mesothelin, a differentiationantigen present on mesothelium, mesotheliomas, and ovarian cancers.Proc Natl Acad Sci U S A 1996;93:136–40.
5. Argani P, Iacobuzio-Donahue C, Ryu B, Rosty C, Goggins M, Wilentz RE,et al. Mesothelin is overexpressed in the vast majority of ductal adeno-carcinomas of the pancreas: identification of a new pancreatic cancer
Clin Cancer Res; 22(7) April 1, 2016 Clinical Cancer Research1650
Lamberts et al.
on February 10, 2021. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst November 20, 2015; DOI: 10.1158/1078-0432.CCR-15-1272

marker by serial analysis of gene expression (SAGE). Clin Cancer Res 2001;7:3862–8.
6. Ordonez NG. Application of mesothelin immunostaining in tumor diag-nosis. Am J Surg Pathol 2003;27:1418–28.
7. Hassan R, Laszik ZG, LernerM, RaffeldM, Postier R, Brackett D.Mesothelinis overexpressed in pancreaticobiliary adenocarcinomas but not in normalpancreas and chronic pancreatitis. Am J Clin Pathol 2005;124:838–45.
8. Frierson HF Jr, Moskaluk CA, Powell SM, Zhang H, Cerilli LA, Stoler MH,et al. Large-scale molecular and tissue microarray analysis of mesothelinexpression in common human carcinomas. Hum Pathol 2003;34:605–9.
9. Kachala SS, BogradAJ, Villena-Vargas J, Suzuki K, Servais EL, Kadota K, et al.Mesothelin overexpression is a marker of tumor aggressiveness and isassociated with reduced recurrence-free and overall survival in early-stagelung adenocarcinoma. Clin Cancer Res 2014;20:1020–8.
10. Tchou J, Wang LC, Selven B, Zhang H, Conejo-Garcia J, Borghaei H, et al.Mesothelin, a novel immunotherapy target for triple negative breast cancer.Breast Cancer Res Treat 2012;133:799–804.
11. Hassan R, Cohen SJ, Phillips M, Pastan I, Sharon E, Kelly RJ, et al. Phase Iclinical trial of the chimeric anti-mesothelin monoclonal antibodyMORAb-009 in patients with mesothelin-expressing cancers. Clin CancerRes 2010;16:6132–8.
12. Beatty GL, Haas AR, Maus MV, Torigian DA, Soulen MC, Plesa G, et al.Mesothelin-specific chimeric antigen receptor mRNA-engineered T cellsinduce antitumor activity in solid malignancies. Cancer Immunol Res2014;2:112.
13. Hassan R, Bullock S, Premkumar A, Kreitman RJ, Kindler H, WillinghamMC, et al. Phase I study of SS1P, a recombinant anti-mesothelin immu-notoxin given as a bolus I.V. infusion to patients with mesothelin-expres-sing mesothelioma, ovarian, and pancreatic cancers. Clin Cancer Res2007;13:5144–9.
14. Kreitman RJ, Hassan R, Fitzgerald DJ, Pastan I. Phase I trial of continuousinfusion anti-mesothelin recombinant immunotoxin SS1P. Clin CancerRes 2009;15:5274–9.
15. Hassan R, Miller AC, Sharon E, Thomas A, Reynolds JC, Ling A, et al. Majorcancer regressions in mesothelioma after treatment with an anti-mesothe-lin immunotoxin and immune suppression. Sci Transl Med 2013;5:208ra147.
16. Hassan R, Sharon E, Thomas A, Zhang J, Ling A, MiettinenM, et al. Phase 1study of the antimesothelin immunotoxin SS1P in combination withpemetrexed and cisplatin for front-line therapy of pleural mesotheliomaand correlation of tumor response with serummesothelin, megakaryocytepotentiating factor, and cancer antigen 125. Cancer 2014;120:3311–9.
17. Bendell J, Blumenschein G, Zinner R, HongD, Jones S, Infante J, et al. First-in-human phase I dose escalation study of a novel anti-mesothelin anti-body drug conjugate (ADC), BAY 94-9343, in patients with advanced solidtumors [abstract]. In: Proceedings of the 104th Annual Meeting of theAmerican Association for Cancer Research; 2013 Apr 6–10; Washington,DC. Philadelphia (PA): AACR; 2013. Abstract nr LB-291.
18. Verma S, Miles D, Gianni L, Krop IE, Welslau M, Baselga J, et al. Trastu-zumab emtansine for HER2-positive advanced breast cancer. N Engl J Med2012;19:1783–91.
19. Tan DS, Thomas GV, Garrett MD, Banerji U, de Bono JS, Kaye SB, et al.Biomarker-driven early clinical trials in oncology: a paradigm shift in drugdevelopment. Cancer J 2009;15:406–20.
20. de Vries EG, Oude Munnink TH, van Vugt MA, Nagengast WB. Towardmolecular imaging-driven drug development in oncology. Cancer Discov2011;1:25–8.
21. Lamberts LE, Williams SP, Terwisscha van Scheltinga AG, Lub-de HoogeMN, Schroder CP, Gietema JA, et al. Antibody positron emission tomog-raphy imaging in anticancer drug development. J Clin Oncol 2015;33:1491–504.
22. Wu AM, Olafsen T. Antibodies for molecular imaging of cancer. Cancer J2008;14:191–7.
23. van Dongen GA, Poot AJ, Vugts DJ. PET imaging with radiolabeledantibodies and tyrosine kinase inhibitors: Immuno-PET and TKI-PET.Tumour Biol 2012;33:607–15.
24. Borjesson PK, Jauw YW, Boellaard R, de Bree R, Comans EF, Roos JC, et al.Performance of immuno-positron emission tomography with zirconium-89-labeled chimeric monoclonal antibody U36 in the detection of lymphnode metastases in head and neck cancer patients. Clin Cancer Res 2006;12:2133–40.
25. Gaykema SB, Brouwers AH, Lub-de Hooge MN, Pleijhuis RG, Timmer-Bosscha H, Pot L, et al. 89Zr-bevacizumab PET imaging in primary breastcancer. J Nucl Med 2013;54:1014–8.
26. Dijkers EC, Oude Munnink TH, Kosterink JG, Brouwers AH, Jager PL, deJong JR, et al. Biodistribution of 89Zr-trastuzumab and PET imaging ofHER2-positive lesions in patients with metastatic breast cancer. ClinPharmacol Ther 2010;87:586–92.
27. Oosting SF, Brouwers AH, van Es SC, Nagengast WB, Oude MunninkTH, Lub-de Hooge MN, et al. 89Zr-bevacizumab PET visualizes hetero-geneous tracer accumulation in tumor lesions of renal cell carcinomapatients and differential effects of antiangiogenic treatment. J Nucl Med2015;56:63–9.
28. Rizvi SN, Visser OJ, VosjanMJ, van Lingen A, Hoekstra OS, Zijlstra JM, et al.Biodistribution, radiation dosimetry and scouting of 90Y-ibritumomabtiuxetan therapy in patients with relapsed B-cell non-hodgkin's lymphomausing 89Zr-ibritumomab tiuxetan and PET. Eur J Nucl Med Mol Imaging2012;39:512–20.
29. Wu AM, Senter PD. Arming antibodies: prospects and challenges forimmunoconjugates. Nat Biotechnol 2005;23:1137–46.
30. Ducry L, Stump B. Antibody-drug conjugates: linking cytotoxic payloads tomonoclonal antibodies. Bioconjug Chem 2010;21:5–13.
31. Ter Weele EJ, Lub-de Hooge MN, Maslyar D, Terwisscha van ScheltingaAGT, Kosterink JG, de Vries EGE, et al. Imaging human pancreatic tumorxenografts with 89Zr-labeled anti-mesothelin antibody [abstract]. In: Pro-ceedings of the 104th Annual Meeting of the American Association forCancer Research; 2013 Apr 6–10; Washington, DC. Philadelphia (PA):AACR; 2013. Abstract nr 2659.
32. Borjesson PK, JauwYW, de Bree R, Roos JC, Castelijns JA, LeemansCR, et al.Radiationdosimetry of 89Zr-labeled chimericmonoclonal antibodyU36asused for immuno-PET in head and neck cancer patients. J Nucl Med2009;50:1828–36.
33. Makris NE, Boellaard R, van Lingen A, Lammertsma AA, van Dongern GA,VerheulHM, et al. PET/CTderiveswhole body andbonemarrowdosimetryof 89Zr-cetuximab. J Nucl Med 2015;56:249–54.
34. Verel I, Visser GW, Boellaard R, Stigter-van Walsum M, Snow GB, vanDongen GA. 89Zr immuno-PET: comprehensive procedures for the pro-duction of 89Zr-labeled monoclonal antibodies. J Nucl Med 2003;44:1271–81.
35. Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, et al.New response evaluation criteria in solid tumours: revised RECIST guide-line (version 1.1). Eur J Cancer 2009;45:228–47.
36. Weekes C, Lamberts LE, Borad MJ, Voortman J, McWilliams RR, RobinsonDiamond J, et al. A phase I study of DMOT4039A, an antibody-drugconjugate (ADC) targeting mesothelin (MSLN), in patients (pts) withunresectable pancreatic (PC) or platinum resistant ovarian cancer (OC).J Clin Oncol 32:5s, 2014 (suppl; abstr 2529).
37. Scales SJ, GuptaN, PachecoG, Firestein R, FrenchDM, KoeppenH, et al. Anantimesothelin-monomethyl auristatin e conjugate with potent antitumoractivity in ovarian, pancreatic, andmesotheliomamodels.MolCancer Ther2014;13:2630–40.
38. Loening AM, Gambhir SS. AMIDE: a free software tool for multimodalitymedical image analysis. Mol Imaging 2003;2:131–7.
39. Oude Munnink TH, Dijkers EC, Netters SJ, Lub-de Hooge MN, BrouwersAH, Haasjes JG, et al. Trastuzumab pharmacokinetics influenced by extenthuman epidermal growth factor receptor 2-positive tumor load. J ClinOncol 2010;28:355–7.
40. Bruno R, Washington CB, Lu JF, Lieberman G, Banken L, Klein P. Popu-lation pharmacokinetics of trastuzumab in patients with HER2þ meta-static breast cancer. Cancer Chemother Pharmacol 2005;56:361–9.
41. Zhang Y, Pastan I. High shed antigen levels within tumors: an additionalbarrier to immunoconjugate therapy. Clin Cancer Res 2008;14:7981–6.
42. Zhang Y, Xiang L, Hassan R, Pastan I. Immunotoxin and taxol synergyresults from a decrease in shed mesothelin levels in the extracellular spaceof tumors. Proc Natl Acad Sci U S A 2007;104:17099–104.
43. Pandit-Taskar N, O'Donoghue JA, Beylergil V, Lyashchenko S, Ruan S,Solomon SB, et al. 89Zr-huJ591 immuno-PET imaging in patients withadvancedmetastatic prostate cancer. Eur JNuclMedMol Imaging 2014;41:2093–105.
44. Gerlinger M, Rowan AJ, Horswell S, Larkin J, Endesfelder D, Gronroos E,et al. Intratumor heterogeneity and branched evolution revealed by multi-region sequencing. N Engl J Med 2012;366:883–92.
Mesothelin Imaging in Pancreatic or Ovarian Cancer Patients
www.aacrjournals.org Clin Cancer Res; 22(7) April 1, 2016 1651
on February 10, 2021. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst November 20, 2015; DOI: 10.1158/1078-0432.CCR-15-1272

45. Hassan R, Wu C, Brechbiel MW, Margulies I, Kreitman RJ, Pastan I.111Indium-labeled monoclonal antibody K1: biodistribution study innude mice bearing a human carcinoma xenograft expressing mesothelin.Int J Cancer 1999;80:559–63.
46. Shin IS, Lee SM, Kim HS, Yao Z, Regino C, Sato N, et al. Effect of chelatorconjugation level and injection dose on tumor and organ uptake of 111In-labeled MORAb-009, an anti-mesothelin antibody. Nucl Med Biol2011;38:1119–27.
47. Misri R, Saatchi K, Ng SS, Kumar U, Hafeli UO. Evaluation of 111In labeledantibodies for SPECT imaging of mesothelin expressing tumors. Nucl MedBiol 2011;38:885–96.
48. Yoshida C, Sogawa C, Tsuji AB, Sudo H, Sugyo A, Uehara T, et al.Development of positron emission tomography imaging by 64Cu-labeledfab for detecting ERC/mesothelin in a mesothelioma mouse model. NuclMed Commun 2010;31:380–8.
49. Ding H, Yong KT, Law WC, Roy I, Hu R, Wu F, et al. Non-invasivetumor detection in small animals using novel functional pluronic
nanomicelles conjugated with anti-mesothelin antibody. Nanoscale2011;3:1813–22.
50. Feig C, Gopinathan A, Neesse A, Chan DS, Cook N, Tuveson DA. Thepancreas cancer microenvironment. Clin Cancer Res 2012;18:4266–76.
51. Lindenberg L, Thomas A, Adler S, Mena E, Kurdziel K, Maltzman J, et al.Safety and biodistribution of 111In-amatuximab in patients with mesothe-lin expressing cancers using single photon emission computed tomogra-phy-computed tomography (SPECT-CT) imaging. Oncotarget 2015;6:4496–504.
52. Ogasawara A, Flores F, Vanderbilt A, Tinianow JN, Gill H, Kan D, et al.Tumor uptake and efficacy of antibody drug conjugates using 89ZirconiumImmunoPET. World Molecular Imaging Congress; 2011 Sept 7–10; SanDiego, California: Abstract nr. P822.
53. Gebhart G, Lamberts LE, Garcia C, Ameye L, Stroobants S, HuizingM, et al.PET/CT with 89Zr-trastuzumab and 18F-FDG to individualize treatmentwith trastuzumab emtansine (T-DM1) in metastatic HER2 positive breastcancer (mBC). J Clin Oncol 32:5s, 2014 (suppl; abstr 11001).
Clin Cancer Res; 22(7) April 1, 2016 Clinical Cancer Research1652
Lamberts et al.
on February 10, 2021. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst November 20, 2015; DOI: 10.1158/1078-0432.CCR-15-1272

2016;22:1642-1652. Published OnlineFirst November 20, 2015.Clin Cancer Res Laetitia E. Lamberts, Catharina W. Menke-van der Houven van Oordt, Eva J. ter Weele, et al. Drug Conjugate Treatment
−Pancreatic and Ovarian Cancer before Anti-Mesothelin Antibody ImmunoPET with Anti-Mesothelin Antibody in Patients with
Updated version
10.1158/1078-0432.CCR-15-1272doi:
Access the most recent version of this article at:
Material
Supplementary
http://clincancerres.aacrjournals.org/content/suppl/2015/11/20/1078-0432.CCR-15-1272.DC1
Access the most recent supplemental material at:
Cited articles
http://clincancerres.aacrjournals.org/content/22/7/1642.full#ref-list-1
This article cites 48 articles, 22 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/22/7/1642.full#related-urls
This article has been cited by 12 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/22/7/1642To request permission to re-use all or part of this article, use this link
on February 10, 2021. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst November 20, 2015; DOI: 10.1158/1078-0432.CCR-15-1272