Immunity to malaria: more questions than answers Jean Langhorne, Francis M Ndungu, Anne-Marit...
29
Immunity to malaria: more questions than answers Jean Langhorne, Francis M Ndungu, Anne-Marit Sponaas & Kevin Marsh Nature Immunology, July 2008 12 th January 2009
-
Upload
debra-long -
Category
Documents
-
view
219 -
download
3
Transcript of Immunity to malaria: more questions than answers Jean Langhorne, Francis M Ndungu, Anne-Marit...

Immunity to malaria: more questions than answers
Jean Langhorne, Francis M Ndungu, Anne-Marit Sponaas & Kevin Marsh
Nature Immunology, July 2008
12th January 2009
Overview
1. Introduction to malaria
2. Immunity to malaria• mechanisms of immunity• immune response • Immune memory
2

Malaria Vector-borne infectious disease
Caused by protozoan parasites of the genus plasmodium
Human malaria P. falciparum P. vivax P. ovale P. malariae
all persons become ill on the first exposure
Causes flu-like illness anemia, fever, chills followed by control of parasitemia in severe cases coma and death
3
Center of disease control and prevention, Atlanta, USA.
common & severe
rare & mild

Malaria
Wide spread in tropical and subtropical regions 400 million cases per year 3 million death Majority 2-5 years
4
© DPDx: CDC's web site for laboratory identification of parasites
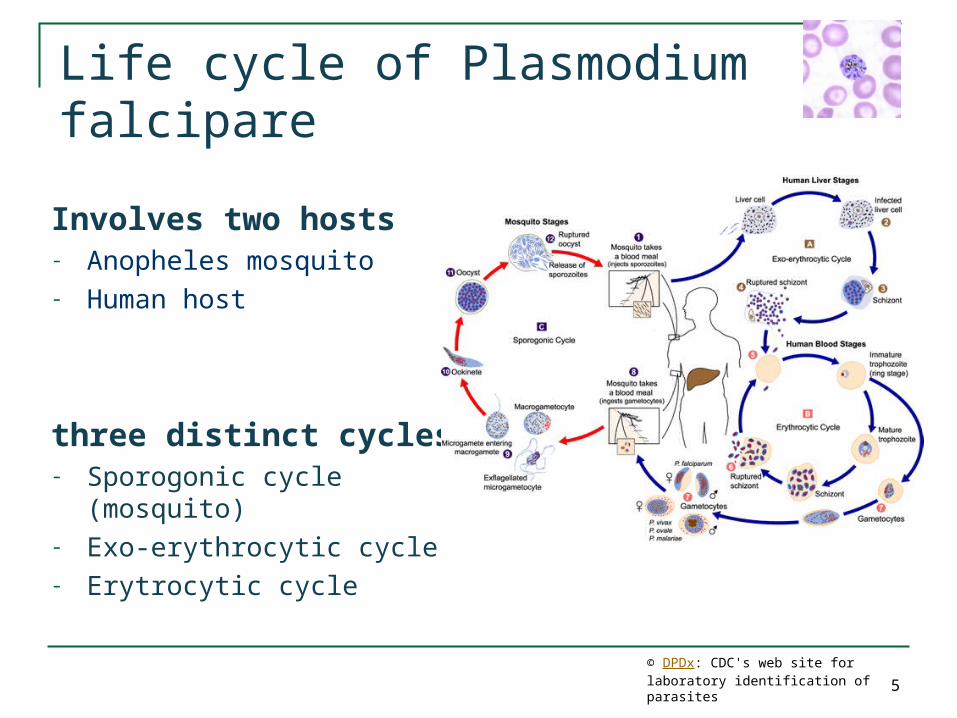
Life cycle of Plasmodium falcipare
5
Involves two hosts- Anopheles mosquito- Human host
three distinct cycles- Sporogonic cycle (mosquito)- Exo-erythrocytic cycle- Erytrocytic cycle
© DPDx: CDC's web site for laboratory identification of parasites
6
Life cycle of Plasmodium falcipare
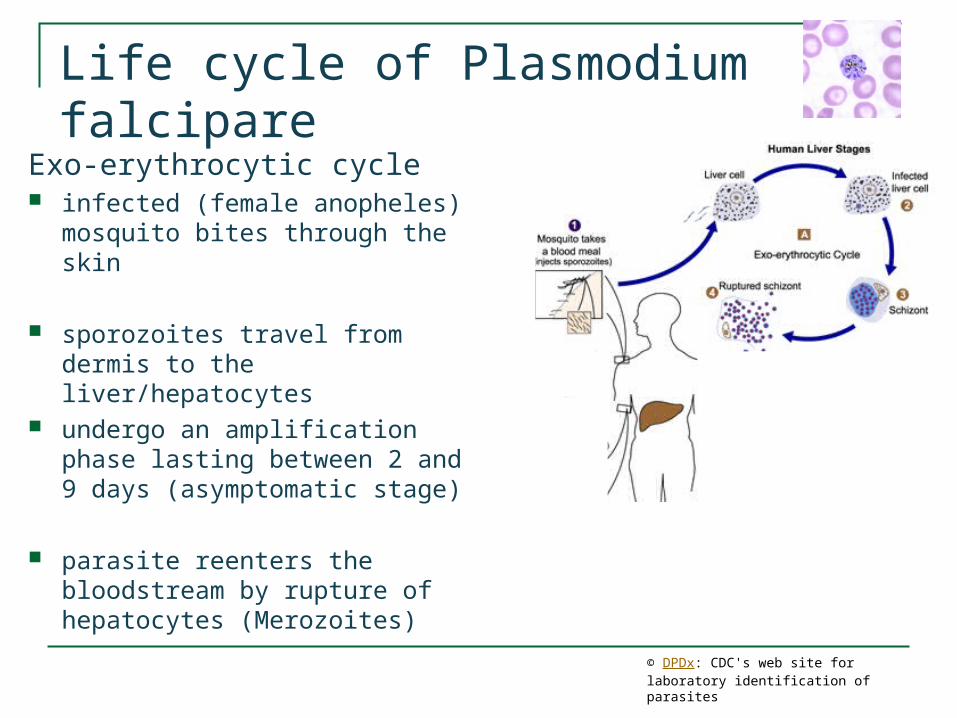
Exo-erythrocytic cycle infected (female anopheles)
mosquito bites through the skin
sporozoites travel from dermis to the liver/hepatocytes
undergo an amplification phase lasting between 2 and 9 days (asymptomatic stage)
parasite reenters the bloodstream by rupture of hepatocytes (Merozoites)
© DPDx: CDC's web site for laboratory identification of parasites
Life cycle of Plasmodium falcipare
7
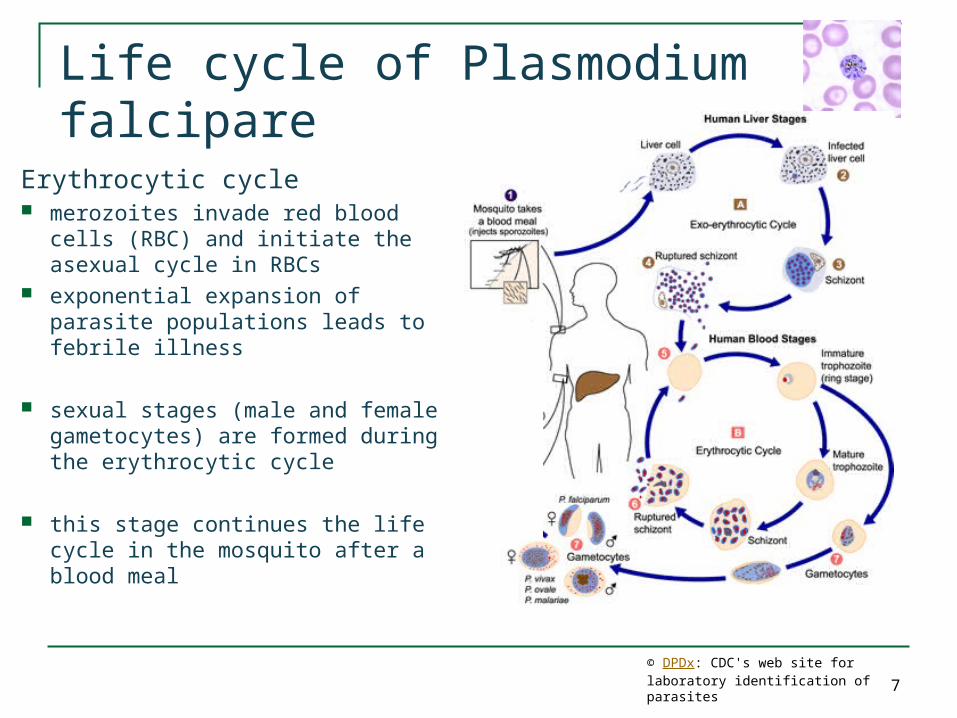
Erythrocytic cycle merozoites invade red blood cells
(RBC) and initiate the asexual cycle in RBCs
exponential expansion of parasite populations leads to febrile illness
sexual stages (male and female gametocytes) are formed during the erythrocytic cycle
this stage continues the life cycle in the mosquito after a blood meal
© DPDx: CDC's web site for laboratory identification of parasites
Life cycle of Plasmodium falcipare
8
© DPDx: CDC's web site for laboratory identification of parasites
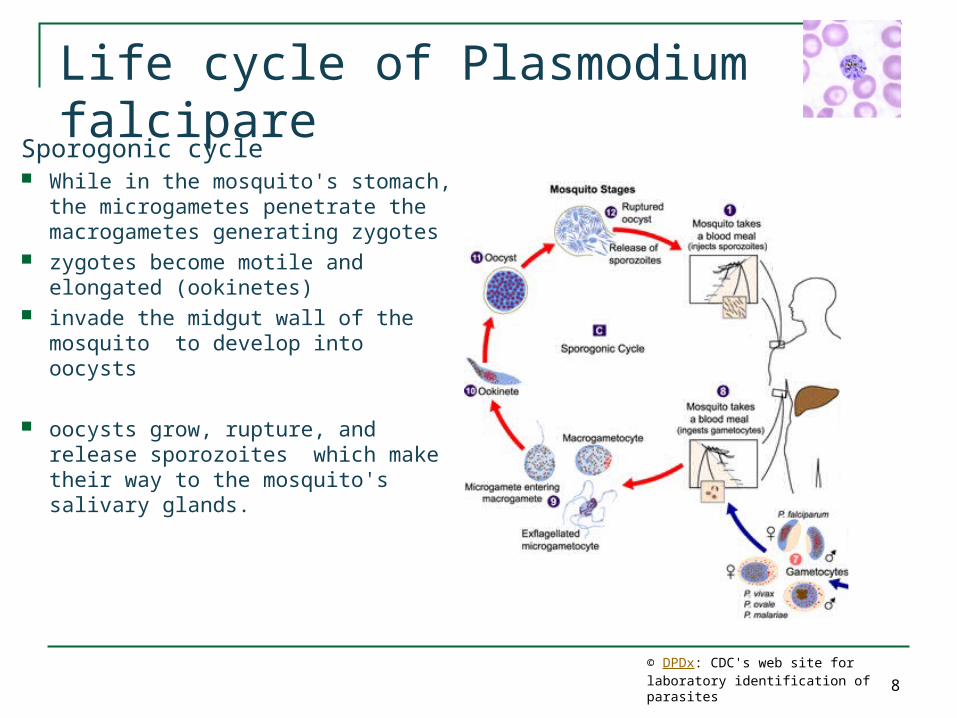
Sporogonic cycle While in the mosquito's stomach,
the microgametes penetrate the macrogametes generating zygotes
zygotes become motile and elongated (ookinetes)
invade the midgut wall of the mosquito to develop into oocysts
oocysts grow, rupture, and release
sporozoites which make their way to the mosquito's salivary glands.

2. Immunity to malaria• mechanisms of immunity• immune response • Immune memory
9
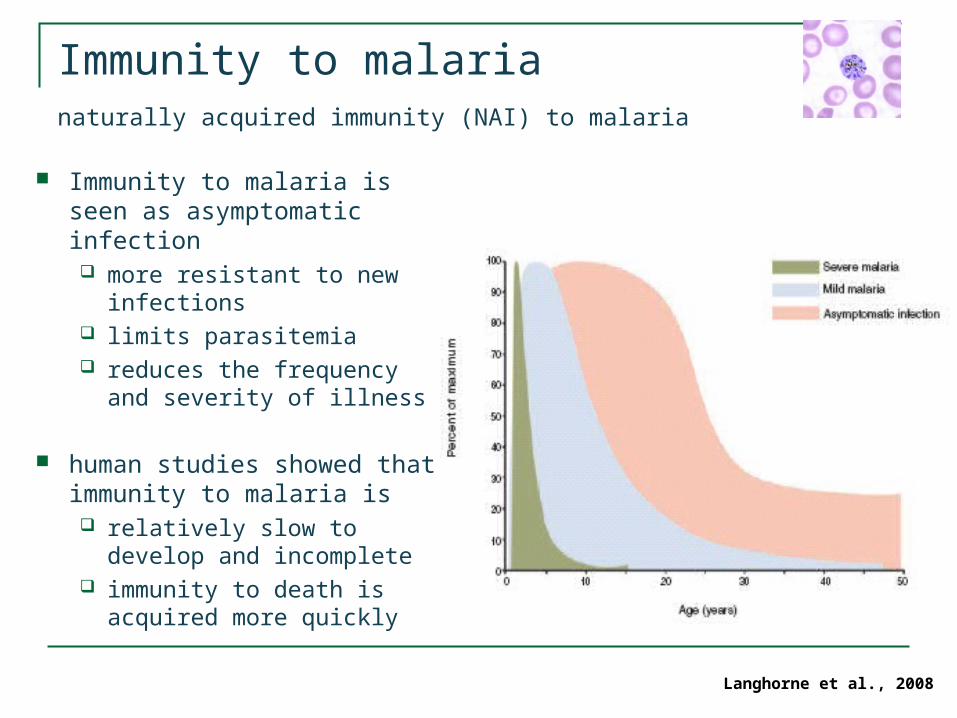
Immunity to malarianaturally acquired immunity (NAI) to malaria
Immunity to malaria is seen as asymptomatic infection more resistant to new
infections limits parasitemia reduces the frequency
and severity of illness
human studies showed that immunity to malaria is relatively slow to develop
and incomplete immunity to death is
acquired more quicklyLanghorne et al., 2008

Mechanisms of Immunity
Picture of human immunity to malaria has been provided by two main sources: Deliberately induced malaria in non immune persons Natural history studies in endemic populations
Immune attack could be directed at any point in the life cycle of plasmodium
Pre-erythrocytic cycle (asymptomatic stage) Probably has limited involvement
Erythrocytic cycle
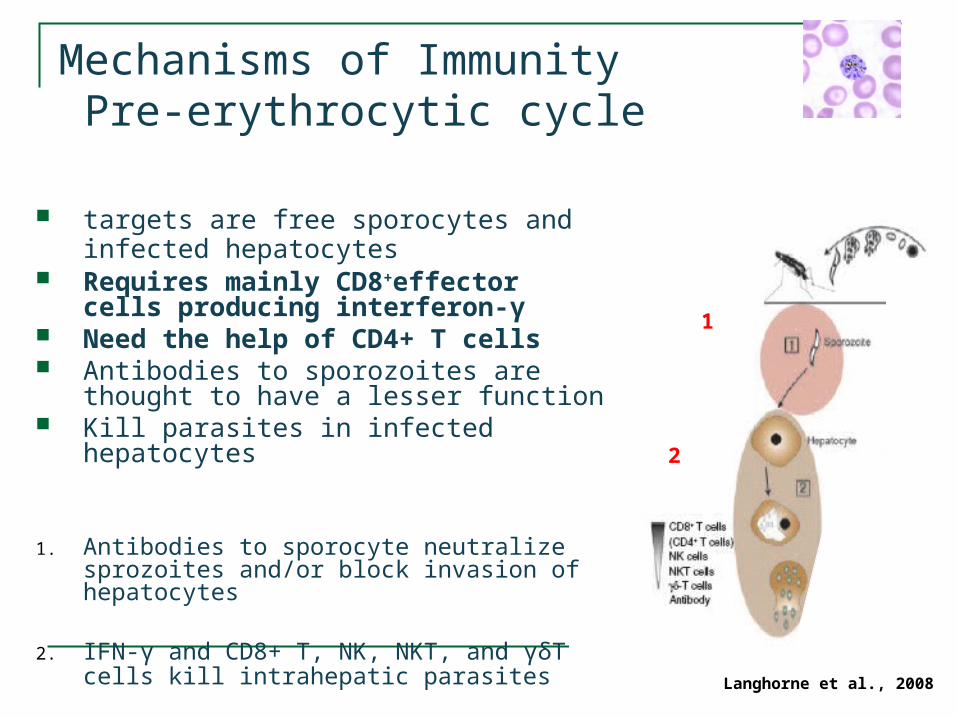
Mechanisms of Immunity Pre-erythrocytic cycle
targets are free sporocytes and infected hepatocytes
Requires mainly CD8+effector cells producing interferon-γ
Need the help of CD4+ T cells Antibodies to sporozoites are thought
to have a lesser function Kill parasites in infected hepatocytes
1. Antibodies to sporocyte neutralize sprozoites and/or block invasion of hepatocytes
2. IFN-γ and CD8+ T, NK, NKT, and γδT cells kill intrahepatic parasites
1
2
Langhorne et al., 2008

Mechanisms of Immunity Erythrocytic cycle
targets are free merozoites or intraerythrocytic parasites (Schizont)
Humoral responses are the key to blood stage immunity (protective antibody response)
3. Antibodies to merozoites opsonize merozites for uptake and/or inhibit invasion of RBCs
4. Antibodies to • block infection of RBCs by merozoites• Antibody-dependent cellular killing
mediated by cytophilic antibodies• Block adhesion of infected RBCs to
endothelium• Neutralize parasite toxins and prevent
the induction of excessive inflammationLanghorne et al., 2008
3
4

Mechanisms of Immunity Erythrocytic cycle
targets are free gametocytes Humoral responses are the key to
blood stage immunity (protective antibody response)
5. Antibodies prevent sequestration and maturation of gametocytes
6. Antibody and complement mediate lysis of gametocytes and prevent further development
Langhorne et al., 2008
5
6

Immune response to plasmodium
Many features are similar to those of sepsis, over-vigorous or disordered immune responses are central
CD4+ and CD8+ T cells are chief participants in acute pathology
Enhanced amounts of cytokine responses TNF IL-1 β, IL-6, IL-10 IFN-γ CCL3 (MIP-1α), CCL4 (MIP-1β)
Immune response to plasmodium
Specific cytokine profiles associated with different syndromes Relatively low IL-10 in severe malaria anaemia Large amounts of IL-10 in respiratory distress Low amounts of CCL5 in severe disease and
mortality
Polymorphism in host genes is associated with susceptibility IFN-γ Interferon regulatory factors TNF IL-10, IL-4
Balance in the regulation of pro- and anti-inflammatory cytokines may be critical in determining the extent of pathology

Trigger for cytokine production
Depends on interaction of host cells and parasite via pattern-recognition receptors (PRR)
Can be induced by infected RBCs or parasite products with several Toll-like receptors (erythrocytic cycle)
Plasmodium falciparum erythrocyte membrane protein 1 (PfEMP1)
Glycosylphosphatidylinositol anchors (GPI) Hemazoin Ds DNA

Trigger for cytokine production

Trigger for cytokine production
MyD88 Intracellular adaptor for several TLRs Important for the induction of some but not all of
the pathology Also required for controlling acute-stage parasitemia
Immune response via several PRR Quantity of inflammatory cytokines? Qualitiy of a person’s response to a particular
clone?
Difficult to distinguish pathological from protective responses

Immune memory in malaria
Immunity to malaria develops Relatively slow Is not sterile
Continued exposure to malarial antigens is needed for Generation of memory and effector cells Persistence or memory and effector cells Maintenance of immunity
It is still unclear what components of immunity is lost without exposure Short lived immunity Longlived immunity

Immune memory in malaria
Rapid boosting of antibody responses indicate the presence of memory B cells
Accumulation of memory B cell specific for malaria indicates the presence of memory B cells
anti-P. falciparum memory B cells present in adults for over 8 years without evident re-
exposure
a subsequent study in children in contrast presence of anti-P. falciparum serum antibody only very low frequencies of malaria-specific memory B
cells
Immune memory in malaria
Pre-Erythrocytic cycle
To be protective specific CD4+ and CD8+ T cells must be maintained as effector cells to differentiate
very rapidly into effector-killer cells
Population shift between mostly protective effector phenotype to the less protective memory phenotype
This could explain why immunological memory is not always correlated with immunity
Immune memory in malaria
Erythrocytic cycle
CD4+ T cells are induced by natural infection Frequencies of responding cells and the prevalence of
exposed people with measurable malaria-specific CD4+ T cells are often low
lower concentrations of malaria-specific antibodies in malaria-infected people positive for HIV
suggests that CD4+ T cell help is necessary for the induction and also for the maintenance of protective antibody
Requirment for memory CD4+ T cells in immunity has still to be elucidated

Immune memory in malaria
1. Inhibition of DC maturation
2. Hemozoin can inhibit macrophage monoyte function
3. IL-10 from DCs and macrophages modulated by infect RBCs inhibit CD4+ T cell activation
4. CD4+ T cells produce IL-10 and transforming growth factor-β, which inhibts the generation of central and memory-effector cells
Immune memory in malaria
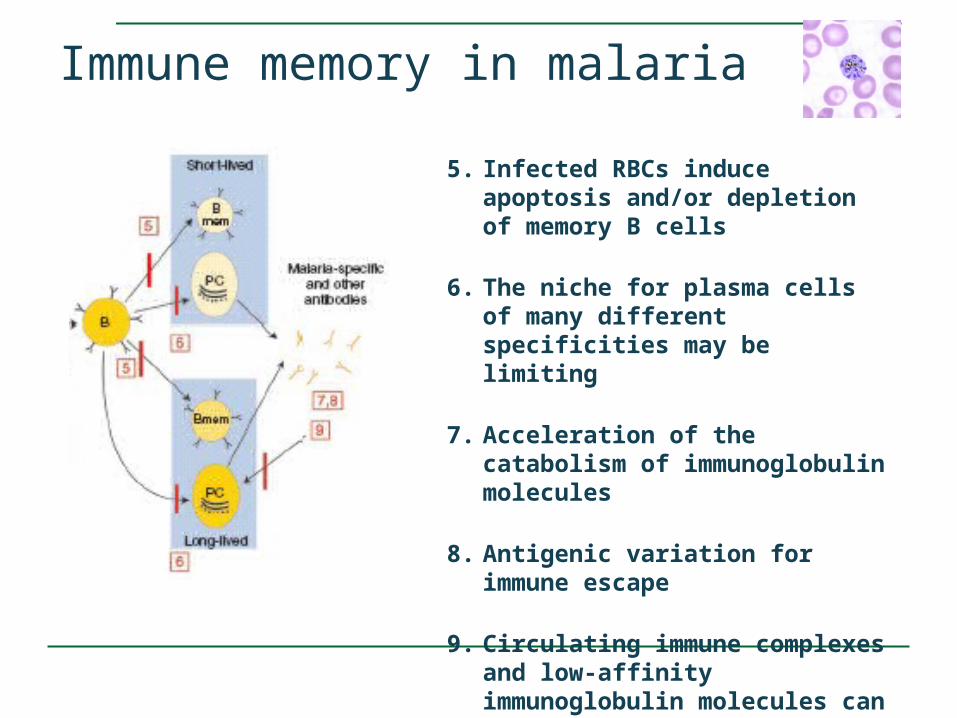
5. Infected RBCs induce apoptosis and/or depletion of memory B cells
6. The niche for plasma cells of many different specificities may be limiting
7. Acceleration of the catabolism of immunoglobulin molecules
8. Antigenic variation for immune escape
9. Circulating immune complexes and low-affinity immunoglobulin molecules can trigger apoptosis of long-lived plasma cells
Conclusions - more questions than answers
Advanced understanding the host response to plasmodium
But many questions remain: What to measure as a correlate for immunity? What mechanisms regulate immune pathology in
semi-immune people? What defects contribute to the relatively
ineffective immunity in children? Why immunity to plasmodium infection can be
short-lived?

Thank you for your attention!

Complete life cycle
Trigger for cytokine production
Plasmodium falciparum erythrocyte membrane protein 1 (PfEMP1) Adhesive molecules sequestration in the post-capillary venules
Glycosylphosphatidylinositol anchors (GPI) Anchor on many plamodium membrane proteins induction of proinflammatory responses
Hemazoin disposal product formed from the digestion of
erythrocytes