Imaging vs functional assessment of left main intermediate ... · Imaging vs functional assessment...
37
Imaging vs functional assessment of Imaging vs functional assessment of left main intermediate lesion. A time for the final statement ? A time for the final statement ? Tomasz Pawłowski, MD, PhD, FESC Klinika Kardiologii Inwazyjnej CSK MSWiA Warsaw, Poland
Transcript of Imaging vs functional assessment of left main intermediate ... · Imaging vs functional assessment...

Imaging vs functional assessment ofImaging vs functional assessment ofleft main intermediate lesion.
A time for the final statement ?A time for the final statement ?
Tomasz Pawłowski, MD, PhD, FESCKlinika Kardiologii Inwazyjnej CSK MSWiA
Warsaw, Poland

□□ I have no conflict of interest related to this presentation□□ I have no conflict of interest related to this presentation□□ I have no conflict of interest related to this presentation□□ I have no conflict of interest related to this presentation

Left main stenosis
-LM disease5-7 % of all angios
- Mortality within 3 years – 50 % with medical treatment

How to assess intermediate left main ?

The question……
Limitations of angiography:
- Overlap of the catheter and LAD/Cx- Overlap of the catheter and LAD/Cx
- Spillover of contrast medium
- Mixing of blood & contrast media
- No reference segment- No reference segment
- Small LM – diffuse disease
- Bifurcation
- Calcification
- Continuity of the plaque into LAD/Cx

Contrast imaging of intermediate & ambigous lesion

Contrast imaging of intermediate & ambigous lesion
IVUS vs FFR – a selection bias ???
IVUSFFR FFR
IVUS IVUSFFR

Contrast imaging of intermediate & ambigous lesion
Misclasiffication by angio:
62/213pts = 29 %18/72 pts = 25 % (isolated LM)
Hamilos et al. Circulation 2009
The dots represent patients with isolated LMCA stenosis.
Hamilos et al. Circulation 2009

Non-invasive assessment of left main significance
Chest painIVUS ???IVUS ???
Ischemic cascade
ECG changeStress ECG
Diastolic & Systolicdysfunction
Stress Echo / MRI
Perfusionabnormalities
Nuclear imagingFFR

Case presentationCase presentation
• 78 years old man
• Hypertension history
• Dyslipidemia history
• Reffered for invasive
assessement of LM lesionassessement of LM lesion

How to assess intermediate left main ?

Intravascular ultrasound (IVUS)
• Tomographic view of left main as well as proximal parts
of LAD & Cxof LAD & Cx
• Plaque burden & composition, vessel size & remodelling
• Proved clinical value for LM PCI optimalisation
• Variability in sizes & lengths & plaque distribution
• Variability in amount of supplied myocardium
• Two separate pullbacks are needed
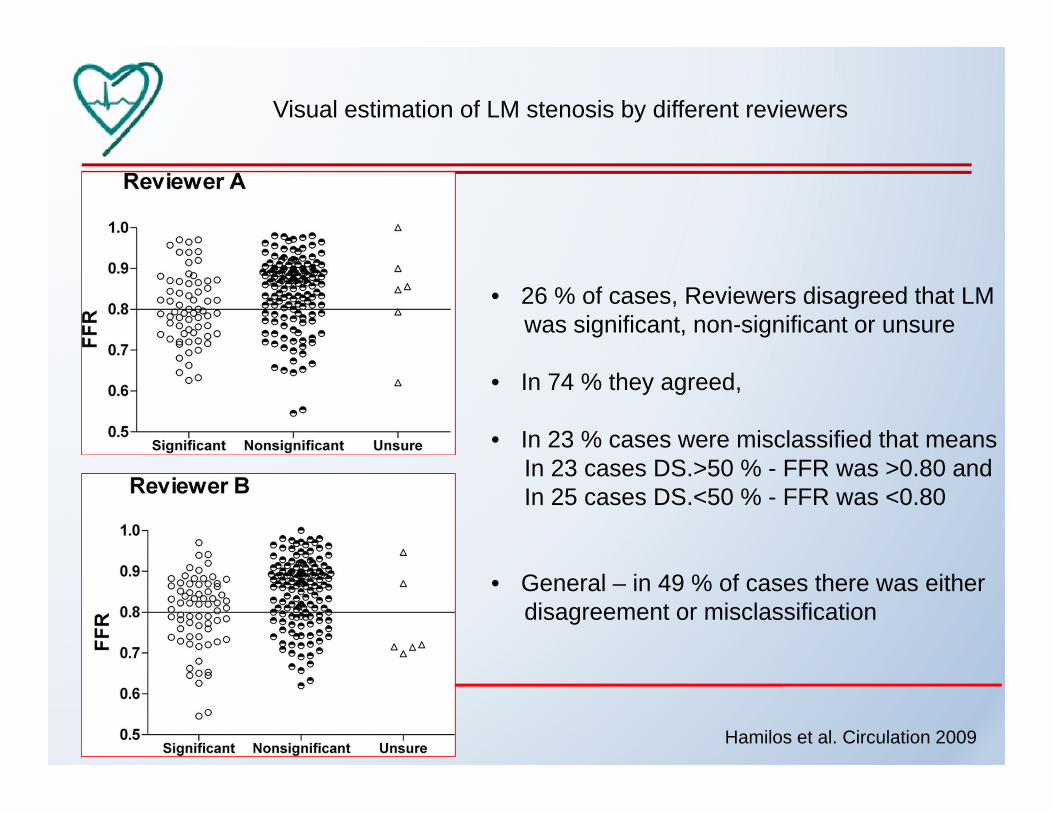
Visual estimation of LM stenosis by different reviewers
• 26 % of cases, Reviewers disagreed that LMwas significant, non-significant or unsure
• In 74 % they agreed,
• In 23 % cases were misclassified that meansIn 23 cases DS.>50 % - FFR was >0.80 andIn 23 cases DS.>50 % - FFR was >0.80 andIn 25 cases DS.<50 % - FFR was <0.80
• General – in 49 % of cases there was eitherdisagreement or misclassification
Hamilos et al. Circulation 2009

Plaque distribution in LM & proximal LAD & Cx
Oviedo et al. Circ Cardiovasc Interv 2010

Fractional flow reserve (FFR)
• Easy and accurate procedure protocol
• Proved clinical cut-off value for lesion deferral
• Proximal LAD & Cx disease affects FFR results in LM
• Adenosine infusion needed
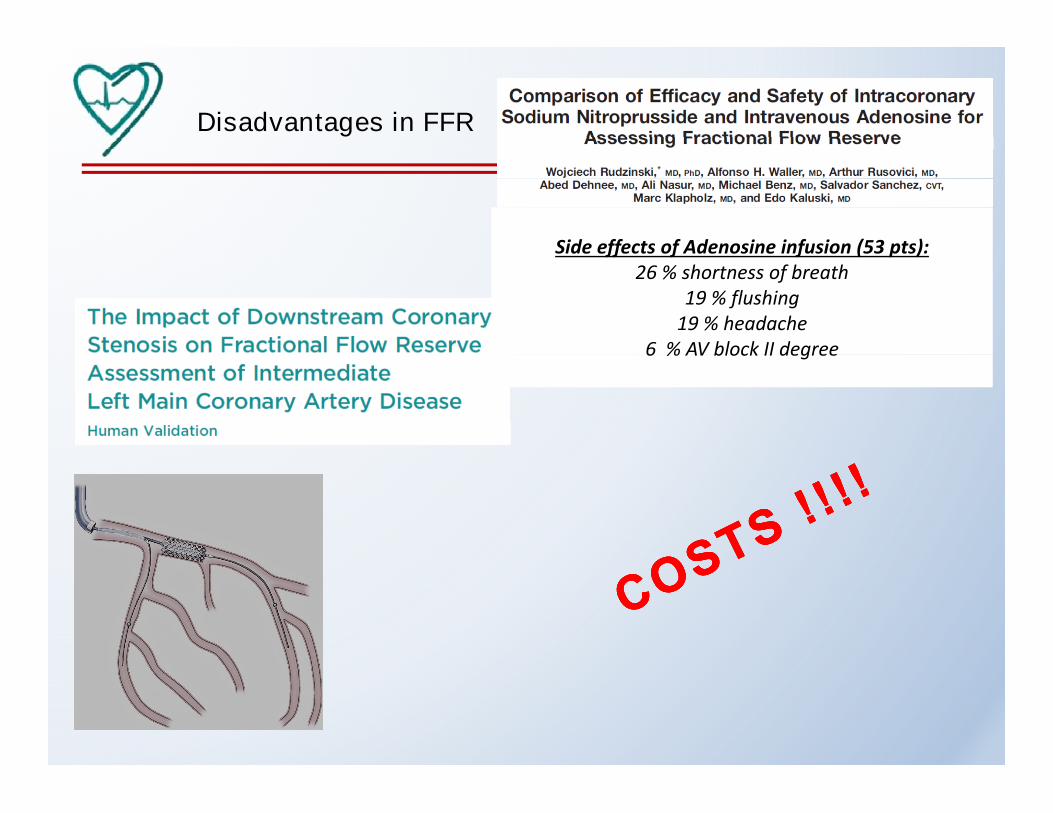
Disadvantages in FFR
Side effects of Adenosine infusion (53 pts):Side effects of Adenosine infusion (53 pts):26 % shortness of breath
19 % flushing19 % headache
6 % AV block II degree6 % AV block II degree
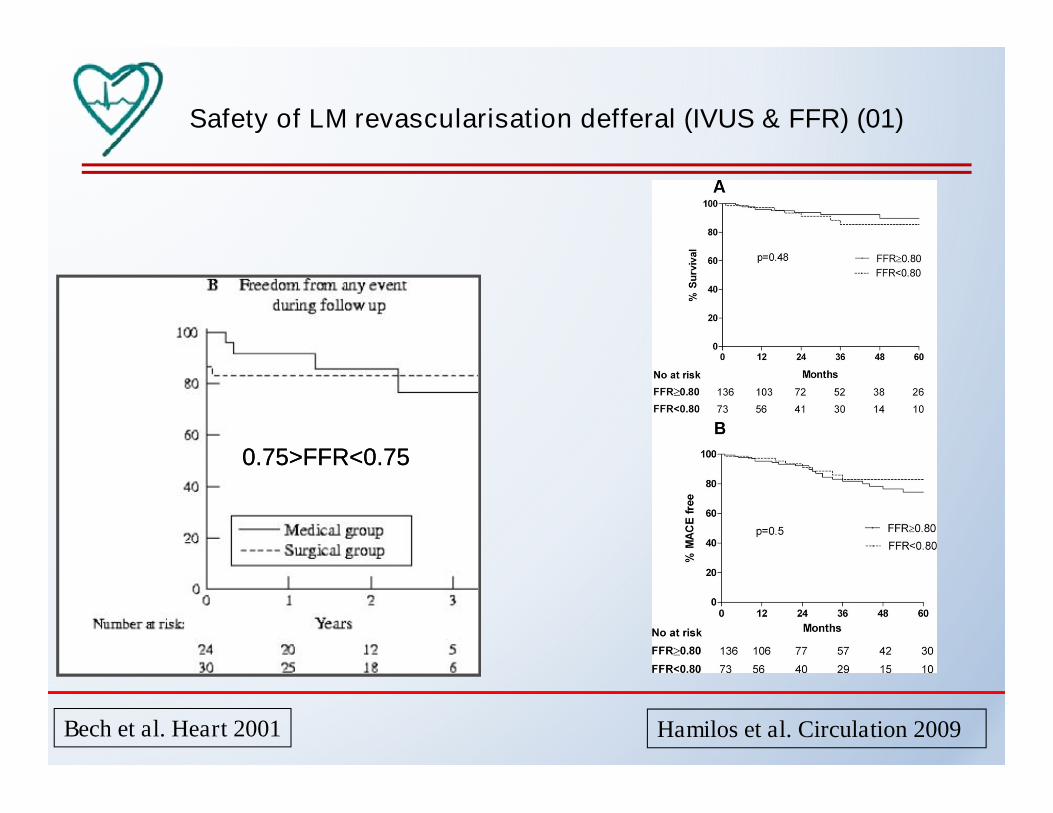
Safety of LM revascularisation defferal (IVUS & FFR) (01)
0.75>FFR<0.750.75>FFR<0.750.75>FFR<0.750.75>FFR<0.75
Bech et al. Heart 2001 Hamilos et al. Circulation 2009
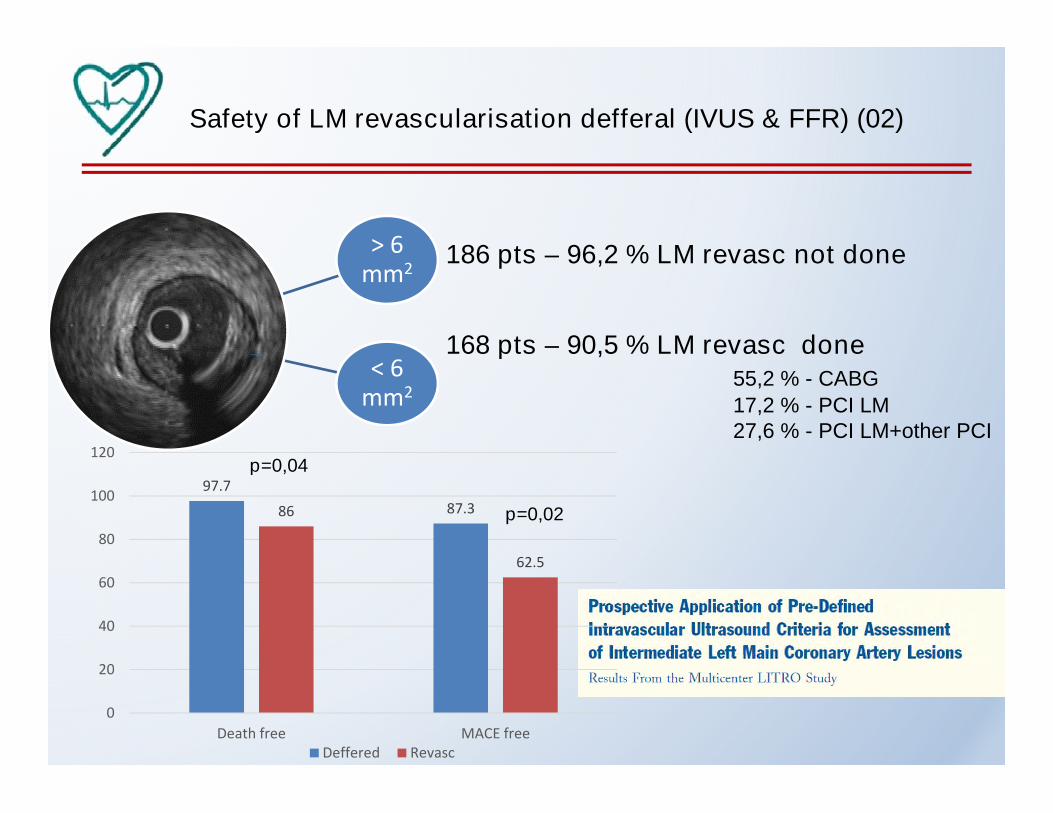
Safety of LM revascularisation defferal (IVUS & FFR) (02)
> 6 186 pts – 96,2 % LM revasc not done> 6mm2
< 6
186 pts – 96,2 % LM revasc not done
168 pts – 90,5 % LM revasc done< 6
mm2
168 pts – 90,5 % LM revasc done55,2 % - CABG
17,2 % - PCI LM27,6 % - PCI LM+other PCI
120p=0,04
97.7
87.386
62.5
80
100
120p=0,04
p=0,02
62.5
20
40
60
0
20
Death free MACE freeDeffered Revasc

IVUS in LM revascularisation

7.4 7.7
13
10
12
14
IVUS No IVUS
*7.4
3.3 3.5
7.7
6
4.5
6.3
2.22
4
6
8
*
11.9
13.6
16
12
14
16
18IVUS
*
0.6
0
2
Death Cardiac death MI TLR ST
*
64.7
7.1
8.89.6
4
6
8
10
12
*
0
2
4
Death TVR Death TVR
Overall Drug eluting stents 14.4
22.2
16
19
15
20
25Pts – distal LM lesion
** *
Park et al. Circ Cardiovasc Interv 2009
Overall Drug eluting stents 14.411.7 11
0
5
10
15 * *
*p<0.050
Death-MI-TLR Cardiac death-MI-TLR
Cardiac death-MI-TLR
IVUS No IVUSHernandez et al. JACC Interv 2014
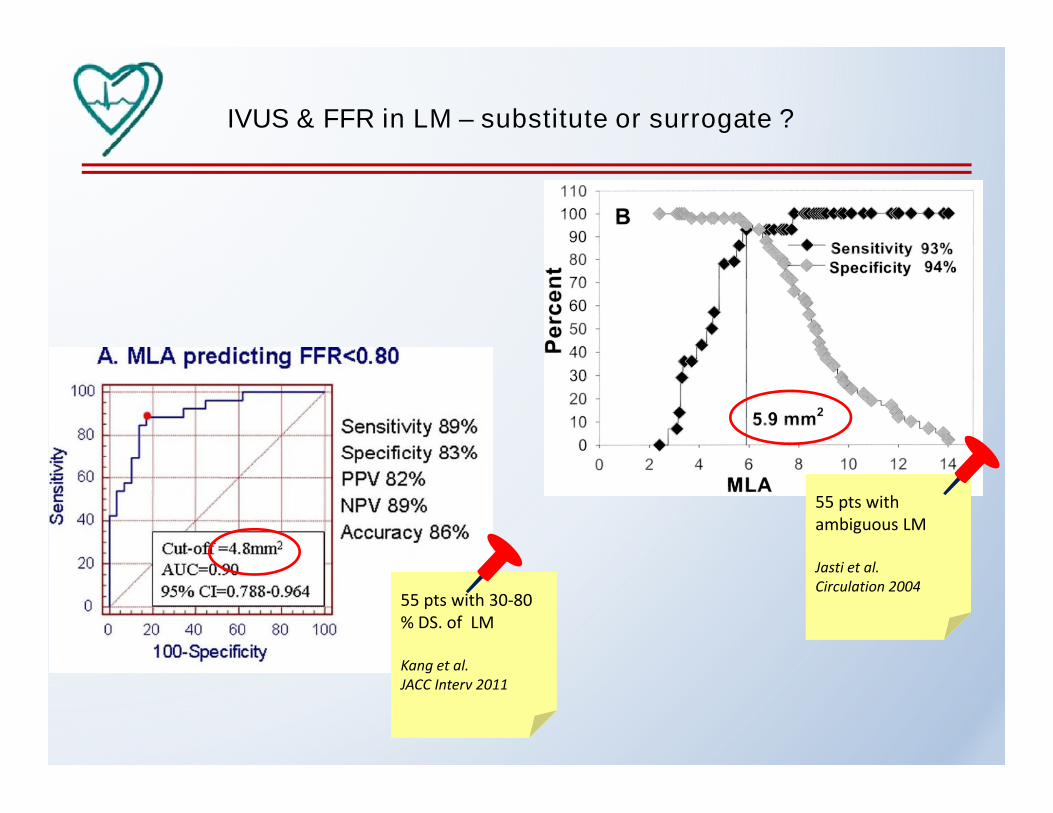
IVUS & FFR in LM – substitute or surrogate ?
55 pts withambiguous LM
Jasti et al.Jasti et al.Circulation 2004
55 pts with 30-80% DS. of LM
Kang et al.Kang et al.JACC Interv 2011
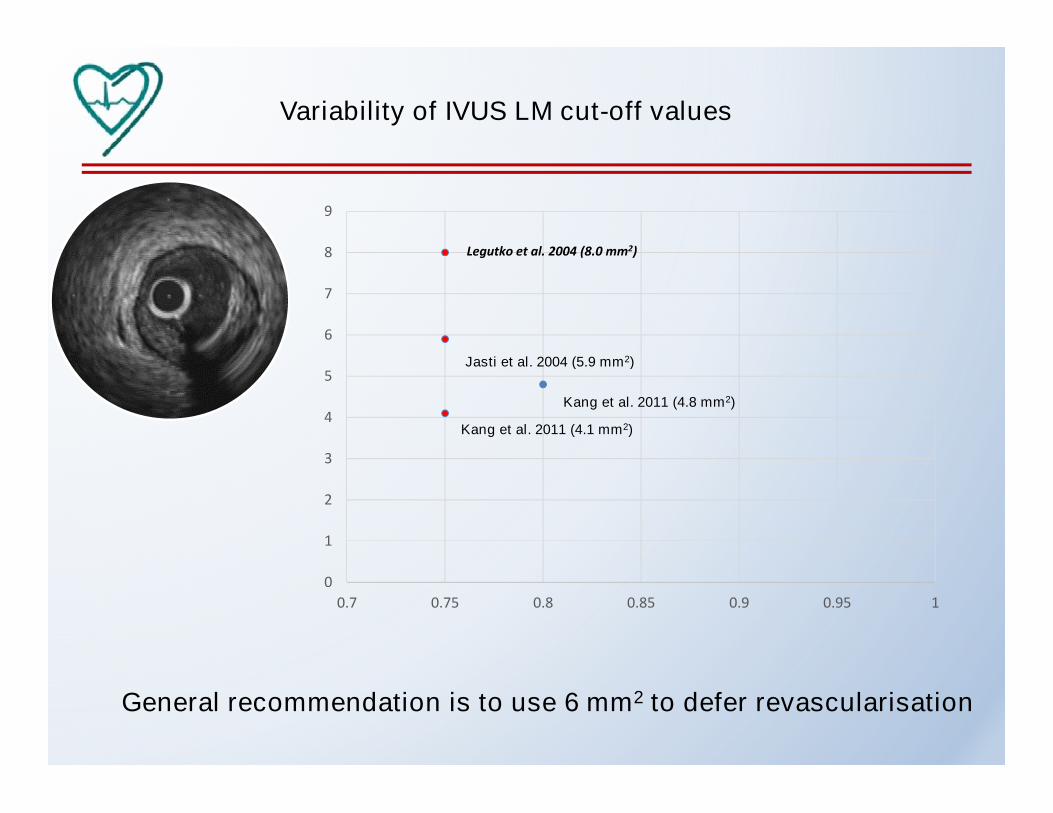
Variability of IVUS LM cut-off values
8
9
Legutko et al. 2004 (8.0 mm2)
6
7
8
Jasti et al. 2004 (5.9 mm2)
Legutko et al. 2004 (8.0 mm2)
3
4
5Jasti et al. 2004 (5.9 mm2)
Kang et al. 2011 (4.8 mm2)
Kang et al. 2011 (4.1 mm2)
1
2
3
0
0.7 0.75 0.8 0.85 0.9 0.95 1
General recommendation is to use 6 mm2 to defer revascularisation

Variability of IVUS LM cut-off values
6 mm2 is enough ?FFR=0.85
6 mm2 is too small ?FFR=0.72
Kang et al.Fassa et al.

Variability of IVUS LM cut-off values
Murray law for LM = 5-6 mm2
4.2
4.0Briguori (4.0)
Murray law for LM = 5-6 mm
are
a(m
m2) 3.8
3.6
3.4
Min
imu
mlu
me
na
rea
3.2
3.0
2.8
Dor (3.2)
Takagi (3.0)
Koo(prox LAD) (3.0)
Koo(mid LAD) (2.75)
Waksman (3.07)
Historic IVUS/FFR data
Min
imu
mlu
me
n
2.8
2.6
2.4
Kang (2.4)
(mid LAD) (2.75)
Historic IVUS/FFR data
Current IVUS/FFR data
Current OCT/FFR data
Reference lumen area (mm2)
2.2
2.0
1.8
5 6 7 8 9 10 11
Pawłowski (2.05)
Gonzalo (1.95)

FFR vs IVUS in intermediate LM
Cardiac deaths & survival
Mallidi et al. Cather Cardiovasc Interv 2015 De la Torre Hernandez et al. JACC 2011

Invasive assessment of intermediate left main stenosisby intravascular ultrasound & fractional flow reserveby intravascular ultrasound & fractional flow reserve
Long term clinical outcome of defferal & revascularisation
T. Pawłowski, S. Gołębiewski, J. Bil, P. Modzelewski, R.J. Gil
Central Clinical Hospital of the Ministry of the Interior and AdministrationCentral Clinical Hospital of the Ministry of the Interior and AdministrationWarsaw, Poland

Direct comparison- IVUS vs FFR
Total 120 pts with angiointermediate LM lesion assesed
invasively in 2009-2014invasively in 2009-2014
Matched pairs according to demographics, risk factors, isolated LM stenosis
60 pts with assesed by FFR 60 pts with assesed by IVUS60 pts with assesed by FFR(140 ug/kg/min, Adenosine
infution, FFR<0,80 for defferal)
60 pts with assesed by IVUS(cut-off value >6 mm2 forrevascularisation defferal)
2 year follow-up with MACE(Death, infarction, TVR)(Death, infarction, TVR)

Direct comparison- IVUS vs FFR
Demographics
Group 1 (FFR) Group 2 (IVUS) p
Demographics
Age (years) 68.5±9.2 69.8±7.8 NS
Hypertension (%) 46.6 46.6 NS
Diabetes (%) 15.0 15.0 NS
Smoking (%) 35.0 35.0 NS
Distal LM lesion (%) 36.6 38.3 NS
Previuos MI (%) 16.6 18.3 NS

Direct comparison- IVUS vs FFR
Results of LM assessment
80 70
71.3
50
60
70
80 70
28.3
IVUS10
20
30
40
30
FFR0
10
OMT
Revasc
FFR IVUS

Direct comparison- IVUS vs FFR
Operator & heart team decisionsRevascularisationRevascularisation
83.3
93.7
90
100
83.3
60
70
80
16.4
30
40
50
16.4
6.3
0
10
20
PCI CABGPCI CABG
FFR IVUS

Direct comparison- IVUS vs FFR
2 year follow-up – all patients
25
25
*
15
20
15
8.3 10
*
5
10
1.65
8.36.6
* *
FFR
IVUS0
MACEDeath
InfarctionTVRTVR
FFR IVUS

Direct comparison- IVUS vs FFR
2 year follow-up – deffered pts
15.8
14
16
18
9.110
12
14
*
7.1
4.7
9.1
4.56
8
0
2.4
4.7
2.2
4.5
0
2
4 *
00
MACE Death Infarction TVR
FFR IVUS

Direct comparison- IVUS vs FFR
2 year follow-up – revascularized pts
5050
60
33.331.2
40
*
16.620
30
*
5.5
11.1
6.2
12.5
0
10
*
0
MACE Death Infarction TVR
FFR IVUS

Direct comparison- IVUS vs FFR
2 year follow-up – mortality in subgroups
8.3
9.1
8
9
10
5.5
6.2
6
7
8
3
4
5
**
1.6
00
1
2
3 *
00
All Deffered Revasc
FFR IVUS
Conclusions (01)
• FFR in comparison to IVUS provides a better log term clinical outcome,
especially in terms of mortality in deffered from revascularisation ptsespecially in terms of mortality in deffered from revascularisation pts
• There is a trend to higher number of infarction in IVUS revascularized
subgroup
• The number of target vessel failure is lower in this subgroup that is probably
related with IVUS optimasition technique
• Using IVUS when assessing intermediate LM lesion, provides a larger number
of LM coronary angioplasty
Conclusions (02)
• The general recommendation (cardiologist’s feeling) was to use
FFR or IVUS to defer revascularisation but with tendency for IVUS forFFR or IVUS to defer revascularisation but with tendency for IVUS for
subsequent optimalisation of LM stenting
• Many data, similarly to native arteries, have showed that there is no single
cut-off value for intermediate LM lesion deffering.
Of note, huge variability in sizes & lengths of LM may play a role
• Fractional flow reserve provides a simple protocol, clear cut-off value &
good clinical outcomes and very important – is not related to variability of
LM sizes and myocardial area supplied