IHI 2007 Institute for Healthcare Improvement 2007 Balanced Scorecard Scorecards and Performance...
38
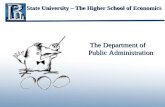
IHI 2007 Associates, L.L.C. Pugh Ettinger M cC arthy Institute for Healthcare Improvement 2007 Balanced Scorecard Scorecards and Performance Measures Sam ple B oard D ashboard PEOPLE Benchm ark FY Target FY 06 QTR 1 FY 06 QTR 2 FY 06 QTR 3 FY 06 QTR 4 Employee TurnoverRate (A nnual) .5% /month 2.50% 2.41% 2.84% 2.79% RN V acancy R ate 1.00% 8% 18.00% 10.00% 5.00% PA TIE N T SA FE TY/R IS K MANAGEMENT Benchm ark FY Target FY 06 QTR 1 FY 06 QTR 2 FY 06 QTR 3 FY 06 QTR 4 Falls with injury (Q uarterly) 0 50 111 126 111 Medication E rrors (A DEs)Category E-I .025/1000 doses 2/1000 doses 3.5 5.0 4.0 CentralLine Infections R ate (Critical Care Units) 0 1.8/100 lines 1.8 3.1 1.3 V entilatorA ssociated P neumonia 0 1 case perquarter 0 1 5 Mortality R ate Index 0.4 0.75 0.62 0.56 0.61 NumberofLives Saved /IHIM easure 150/quarter 181 219 181 C LIN IC AL QU A LITY Benchm ark FY Target FY 06 QTR 1 FY 06 QTR 2 FY 06 QTR 3 FY 06 QTR 4 EVIDENCE-BASED CARE % OF P A TIE N T S REC EIVIN G ALL REQUIRED ELEM ENTS A cute MI 100% 90-95 98% 98% 97% 95% Pneum onia 100% 80-90 89% 88% 82% 79% Congestive H eartFailure 100% 90-95 98% 93% 94% 97% S urgical Infection P revention P rotocol 100% 100 96% 98% 98% 98% B elow Target Meeting Target Exceeds Target C linicalExcellence C ustom er& S ervice Excellence C orporate Effectiveness OverallM ortality R ate OverallM orbidity O verallPatientSatisfaction PatientSatisfaction "D elighted" P hysician S atisfaction "D elighted" PhysicalS urroundings D issatisfaction EOS Leadership S cores G rowth E fficiency N etOperating Margin C om m unity P erception Atorbetterthan target W ithin 5% ofreaching target P atientS afety E vidence Based Medicine Outside of5% oftarget Funded by the Office of Rural Health and Washington’s Department of Health
-
Upload
laureen-powers -
Category
Documents
-
view
214 -
download
0
Transcript of IHI 2007 Institute for Healthcare Improvement 2007 Balanced Scorecard Scorecards and Performance...

IHI 2007Associates, L.L.C.
Pugh Ettinger McCarthy Institute for Healthcare Improvement 2007
Balanced ScorecardScorecards and Performance Measures
Sample Board Dashboard
PEOPLE Benchmark FY Target FY 06 QTR 1 FY 06 QTR 2 FY 06 QTR 3FY 06 QTR
4
Employee Turnover Rate (Annual) .5%/month 2.50% 2.41% 2.84% 2.79%
RN Vacancy Rate 1.00% 8% 18.00% 10.00% 5.00%
PATIENT SAFETY/RISK MANAGEMENT Benchmark FY Target FY 06 QTR 1 FY 06 QTR 2 FY 06 QTR 3FY 06 QTR
4
Falls with injury (Quarterly) 0 50 111 126 111
Medication Errors (ADEs) Category E-I .025/1000 doses 2/1000 doses 3.5 5.0 4.0
Central Line Infections Rate (Critical Care Units) 0 1.8/100 lines 1.8 3.1 1.3
Ventilator Associated Pneumonia 0 1 case per quarter 0 1 5
Mortality Rate Index 0.4 0.75 0.62 0.56 0.61
Number of Lives Saved / IHI Measure 150/quarter 181 219 181
CLINICAL QUALITY Benchmark FY Target FY 06 QTR 1 FY 06 QTR 2 FY 06 QTR 3FY 06 QTR
4
EVIDENCE-BASED CARE % OF PATIENTS RECEIVING ALL REQUIRED ELEMENTS
Acute MI 100% 90-95 98% 98% 97% 95%
Pneumonia 100% 80-90 89% 88% 82% 79%
Congestive Heart Failure 100% 90-95 98% 93% 94% 97%
Surgical Infection Prevention Protocol 100% 100 96% 98% 98% 98%
Below Target Meeting TargetExceedsTarget
Clinical Excellence Customer & Service Excellence
Corporate Effectiveness
Overall Mortality Rate
Overall Morbidity
Overall Patient Satisfaction
Patient Satisfaction "Delighted"
Physician Satisfaction "Delighted"
Physical Surroundings Dissatisfaction
EOS Leadership Scores
Growth
Efficiency
Net Operating Margin
Community Perception
At or better than target
Within 5% of reaching target
Patient Safety
Evidence Based Medicine
Outside of 5% of target
Funded by the Office of Rural Health and Washington’s Department of Health

2
Associates, L.L.C.
Pugh Ettinger McCarthy
IHI 2007
On the phone…
20 Years CEO experience in hospitals, health systems and managed care
CEO of United General Hospital, Sedro Woolley, WA 1979-1984
Senior Faculty Member IHI
Consulting work focuses on improving quality and performance
Michael Pugh

3
Associates, L.L.C.
Pugh Ettinger McCarthy
IHI 2007
How Does Your Board Answer the Questions…
How good is our hospital?
Are we achieving what we need to achieve?
How do we know?

4
Associates, L.L.C.
Pugh Ettinger McCarthy
IHI 2007
Another Way to Think About How Good…
What are you willing to promise patients about medication safety at your hospital?
What are you willing to promise patients about the use of evidence-based medicine in your hospital and clinics?
What are you willing to promise patients about the level of care and service that will be provided?
What are you willing to promise the community about access and cost?

5
Associates, L.L.C.
Pugh Ettinger McCarthy
IHI 2007
How Good?
What level of medication error is acceptable if you are the patient?
How do you pick the patient that is not to receive evidence-based treatment?
How do you decide which patient should have a surgical site infection?
How do you explain to your mother that it is perfectly acceptable to wait in the ER for 8 hours and receive a bill for $3500.00?

6
Associates, L.L.C.
Pugh Ettinger McCarthy
IHI 2007
1. Prevent Harm from High-Alert Medications... starting with a focus on anticoagulants, sedatives,
narcotics, and insulin
2. Reduce Surgical Complications by reliably implementing all of the changes in care
recommended by SCIP, the Surgical Care Improvement Project (www.medqic.org/scip)
3. Prevent Pressure Ulcers... by reliably using science-based guidelines for their
prevention

7
Associates, L.L.C.
Pugh Ettinger McCarthy
IHI 2007
4. Reduce Methicillin-Resistant Staphylococcus Aureus (MRSA) infection by reliably implementing scientifically proven infection control
practices
5. Deliver Reliable, Evidence-Based Care for Congestive Heart Failure to avoid readmissions
6. Get Boards on Board … by defining and spreading the best-known leveraged
processes for hospital Boards of Directors, so that they can become far more effective in accelerating organizational progress toward safe care

8
Associates, L.L.C.
Pugh Ettinger McCarthy
IHI 2007
Building Stronger Health Care Boards
Basic Governance Functions– Keeper of the Mission– Set Direction and Expectations– Monitor Progress – Hire and Evaluate the CEO– Represent the interests of the
community

9
Associates, L.L.C.
Pugh Ettinger McCarthy
IHI 2007
Scorecards are Tools for Monitoring Progress and Setting Expectations Financial
Operating Budgets and Targets
Cash Capital Expenditures Financial Integrity--
Audits Compliance
Legal and Regulatory Board Policy Risk Management
Strategic Progress on
implementation of key strategies
Results Quality
Patient Satisfaction Clinical Care
Performance Indicators Patient and Employee
Safety

10
Associates, L.L.C.
Pugh Ettinger McCarthy
IHI 2007
Why Use Scorecards and Performance Measures? You should be able to look at what the
leadership of an organization measures and determine the organization’s priorities and strategy
In God we Trust, all else bring data….

11
Associates, L.L.C.
Pugh Ettinger McCarthy
IHI 2007
Balanced Scorecards Drive Operating Strategies
Strategic Feedback/Learning
•articulating vision•strategic feedback
•review and learning
Balanced Scorecard
Adapted fromThe Balanced ScorecardKaplan & Norton
Adapted fromThe Balanced ScorecardKaplan & Norton
Clarify/TranslateVision and Strategy
•consensus
Communicating andLinking
•goals•performance measures
Planning and TargetSetting
•align w/ strategy•allocate resources

12
Associates, L.L.C.
Pugh Ettinger McCarthy
IHI 2007
Seven Leadership Leverage Points for Driving Great Performance*
1. Set measured system-level aims and oversee their achievement at the Board level
2. Align aims, measures and strategies in a leadership learning system
3. Channel leadership attention to aims4. Engage an effective and committed executive
team5. Engage the CFO in this work6. Engage with physicians7. Build deep improvement capability
*www.ihi.orgReinertsen, Pugh, Bisognano 2006

13
Associates, L.L.C.
Pugh Ettinger McCarthy
IHI 2007
Leverage Point 1: Establish system level measures
Set measured system-level aims and oversee their achievement at the Board level Owned by the governing board Collectively, the measures answer the
question: How good are we? Transparent—everyone in the organization
should know the Key Measures

14
Associates, L.L.C.
Pugh Ettinger McCarthy
IHI 2007
What Should Be On the Hospital Board’s Performance Scorecard?
Mortality Readmission Rates Patient Experience % of Patients
Receiving Care According to the Evidence
Employee Satisfaction or Engagement
Cost per Discharge Days Cash on Hand Patient Safety Access
Board performance measures should at minimum include expected aims and results for:

15
Associates, L.L.C.
Pugh Ettinger McCarthy
IHI 2007
IHI Proposed System Level Measures
IOM Dimension System MetricSafe ADEs/1000 doses
Effective & Equitable HSMRFunctional Outcomes (SF-6 for Chronic disease)
Patient-Centered Inpatient Satisfaction% patients dying in hospital
Timely Days to 3rd next available appointment
Efficient Health care costs per capitaHospital costs per discharge
Other Staff voluntary turnoverInvestment per capita

Critical Questions For Creating Alignment Between Desired Results and Quality Projects
Organizational Performance
Measures
Drivers(Core Strategies and
Theories)
Quality Projects(Operating Plan)
1. What are your system level aims and aspirations?
2. What are the system-level measures of those aims? (Big Dots)
3. How good must you be, and by when?
1. What are your key organizational strategies for moving your dots?
2. What really has to be changed, or put in place, in order to achieve each of these goals?
1. What set of projects will move the Drivers far enough, fast enough, to achieve your aims?
IHI 2007

Aligned Operating Strategies and Quality Projects Drive Desired Results
Organizational
AimsWhat by When
Drivers(Core Operating Strategies
and Theories)
Quality Projects(Operating Plan)
Cost per Discharge decrease by 2% in 2007
HSMR Mortality Rate less than 70 in 2007
Patient Satisfaction 75% rate top box in 2007
Decrease Nosocomial Infections
Improve Flow
Remove Waste
Surgical Site Infection Project
Ventilator Project Evidence-based Care
Project Clean Hands Project ER to Bed Project
IHI 2007

An Organization’s Measurement System Should Be Linked to Drive Desired Results
0
20
40
60
80
100
1stQtr
2ndQtr
3rdQtr
4thQtr
East
West
North
0
20
40
60
80
100
120
1st Qtr 2nd Qtr 3rd Qtr 4th Qtr
0
20
40
60
80
100
120
1st Qtr 2nd Qtr 3rd Qtr 4th Qtr
0
20
40
60
80
100
120
1st Qtr 2nd Qtr 3rd Qtr 4th Qtr
0
20
40
60
80
100
120
1st Qtr 2nd Qtr 3rd Qtr 4th Qtr
0
20
40
60
80
100
120
1st Qtr 2nd Qtr 3rd Qtr 4th Qtr
0
20
40
60
80
100
120
1st Qtr 2nd Qtr 3rd Qtr 4th Qtr
0
20
40
60
80
100
120
1st Qtr 2nd Qtr 3rd Qtr 4th Qtr
0
20
40
60
80
100
120
1st Qtr 2nd Qtr 3rd Qtr 4th Qtr
0
20
40
60
80
100
120
1st Qtr 2nd Qtr 3rd Qtr 4th Qtr
0
20
40
60
80
100
120
1st Qtr 2nd Qtr 3rd Qtr 4th Qtr
0
20
40
60
80
100
120
1st Qtr 2nd Qtr 3rd Qtr 4th Qtr
Organizational Performance Measures
Strategic Measures/Drivers
Process & OperationalMeasures
IHI 2007

19
Associates, L.L.C.
Pugh Ettinger McCarthy
IHI 2007
Simple Rules for Board Level Scorecards and Dashboards Measure what is
important Review every meeting Use topic specific
scorecards to drill down at committee level (finance, strategy & planning, quality, safety, etc.)
Use Simple Formats
Set all-or-none target levels for clinical care and safety measures (100% or 0%)
Avoid using averages; use percentiles measured against standards
Avoid color coding to low expectations
Data graphed over time is the most powerful format

20
Associates, L.L.C.
Pugh Ettinger McCarthy
IHI 2007
Color Coded DashboardsOnly As Good As Your Targets
Simple, and sometimes too simple
Color coding without numbers can mislead
Tendency is to assume that only the “red” blocks need attention
If used, boards need to frequently ask how the targets are set

21
Associates, L.L.C.
Pugh Ettinger McCarthy
IHI 2007
The Case For All-or-None Measurement
Report to the Board Quality Committee
“Our MI Core Indicators were greatly improved last quarter. Only one EBC requires corrective action.”
Evidence-Based Care
Measure
EBC Compliance
%EBC 1 80% At or Above Target
EBC 2 100% Needs Work
EBC 3 100% Corrective Action
EBC 4 60%EBC 5 80%EBC 6 90%
Governance Question: “What % of Patients Got the Right Care?”

22
Associates, L.L.C.
Pugh Ettinger McCarthy
IHI 2007
The Case For All-or-None MeasuresOnly 30% of Patients Received the Right Care*
Patient 1
Patient 2
Patient 3
Patient 4
Patient 5
Patient 6
Patient 7
Patient 8
Patient 9
Patient 10 Total
EBC Compliance
%EBC 1 1 1 0 1 1 1 1 0 1 1 8 80%EBC 2 1 1 1 1 1 1 1 1 1 1 10 100%EBC 3 1 1 1 1 1 1 1 1 1 1 10 100%EBC 4 0 1 0 1 1 1 1 0 1 0 6 60%EBC 5 1 1 1 0 1 0 1 1 1 1 8 80%EBC 6 1 1 1 1 0 1 1 1 1 1 9 90%
Per Patient Totals
5 6 4 5 5 5 6 4 6 5
% of Care Elements
Received by Patient
83% 100% 67% 83% 83% 83% 100% 67% 100% 83%
% of Patients Receiving Perfect
Care
30%
*Right Care defined as receiving all of the required EBC elements that the patient was eligible for

23
Associates, L.L.C.
Pugh Ettinger McCarthy
IHI 2007
The Case for Measuring Against Standards/Expectations
Door to Intervention time proven to be critical to Heart Attack outcomes
Standard=30 minutes from presentation to (Thrombolytics or 90 minutes to Angioplasty)
Quality Committee Report “Our data indicates that
we are exceeding the national standard. Our average time for thrombolytics is 29.5 minutes.”
Great Report or Not?

24
Associates, L.L.C.
Pugh Ettinger McCarthy
IHI 2007
Not. What about the 25% of patients with delayed care?
0
10
20
30
40
50
%
0 10 20 30 40 50 60 70 80 90
Minutes
Door to Therapy-MI
25% of All PatientsBeyond the Standard
Average = 29.5 Minutes
30 Minute Standard

25
Associates, L.L.C.
Pugh Ettinger McCarthy
IHI 2007
Anywhere HospitalHeart Surgery Program Board Report
5.9%
1.1%
Jan 05
Jan 06
Monthly Mortality
Should this be a cause for celebration?
“Compared to January of last year, our heart surgery mortality has decreased from 5.9% to 1.1%

26
Associates, L.L.C.
Pugh Ettinger McCarthy
IHI 2007
When do you want to have your Heart Surgery?
0
1
2
3
4
5
6
7
Jan
-05
Feb
Mar
Ap
r
May
Ju
n
Ju
l
Au
g
Sep
Oct
Nov
Dec
Jan
-06
St. Elsewhere Monthly Heart SurgeryMortality
AVG = 3.5%
5.9%
1.1%

27
Associates, L.L.C.
Pugh Ettinger McCarthy
IHI 2007
An Oregon Hospital’s Proposed Governance Scorecard (example)
Quality Dimension Measure Dashboard Metric
Access to Care ER Waiting Time% of Patients treated and discharged in less than 2 hours
Effectiveness30 Day Hospital Readmissions
% of Total Discharges Readmitted within 30 days
Effectiveness Mortality% of in hospital deaths/total monthly discharges
SafetyNumber of Adverse
EventsTotal Number of Patient Injuries During the Month (Falls, ADEs, Infections)
SafetyNosocomial Infections
% of Patients with hospital acquired infection as percentage of monthly discharges
Financial Effectiveness Cost/Discharge
Total Monthly Inpatient Operating Cost/Total Number of Discharges

28 In Partnership with the
American Hospital Association
Clinical Excellence Customer & Service Excellence
Corporate Effectiveness
Overall Mortality Rate
Overall Morbidity
Overall Patient Satisfaction
Patient Satisfaction "Delighted"
Physician Satisfaction "Delighted"
Physical Surroundings Dissatisfaction
EOS Leadership Scores
Growth
Efficiency
Net Operating Margin
Community Perception
At or better than target
Within 5% of reaching target
Patient Safety
Evidence Based Medicine
Outside of 5% of target
Bronson 2004 Scorecard

2005 Jan-06 Goal Grade Trendf
NQF
MeasuresInitiatives
100KSAVEDLIVES
CAMPAIGN
# of Falls With Injury/1000 Patient Days7
% of Pneumonia Patients With Antibiotic Within 4 Hrs.4
AMI Mortality4
Reduce Falls
% of Patients With Central Line Bundle6
ATB Within 4 Hrs. for Pneumonia
Prevention of Central Line Infections
Prevention of Ventilator-Associated Pneumonia
DVT Screening/ProphylaxisPerioperative Beta Blockade
Prevention of Surgical Site Infections
# of Falls/1000 Patient Days7
% of ICU Vent Patients With Bundle2
# of VAP Cases in ICU/1000 Ventilator Days6
# of Central Line Related Primary BSI6
Rate of Infection in Clean Surgical Patients6
Appropriate Prophylactic Antibiotic Selected4
Prophylactic Antibiotic Discontinued Within 24 Hrs.4
% of Patients With Appropriate DVT Prophylaxis8
% of Patients With Appropriate Prophylactic Beta Blocker8
Prophylactic Antibiotic Started Within 1 Hour4
% of Code Blues Occurring Outside ICU2,2a
Beta-Blocker at Arrival4
Medication Errors5
# of Unreconciled Medications/100 Admissions5
Smoking Cessation Counseling4
Beta-Blocker at Discharge4
ACE1 or ARB at Discharge for Patients with LVSD4
PCI Door to Dilation < 120 Minutes4
% of Unreconciled Medications5
Patient Safety and Quality Scorecard
Prepared by: M.Mullesch and J.Lovrien. Updated: 2/22/06. Sources 1: Preliminary Data, 2: AMH Critical Care PI, 2a: HPF Code Blue Que, 3: TSI, 4: Delta, 5: AMH Pharm., 6: AMH Infection Control, 7: AMH QI Dept., 8: Random Sample AMH IP Records a: Institute of Healthcare Improvement, b: AMH Target, c: Hospital Quality Alliance, d: IHS Target, e: National Quality Forum, f: + Better, - Worse, = No Change
Adverse Drug Events
Deploy RapidResponse Team
Evidence-Based Care for AMI
ASA at Discharge4
# of Calls to the Rapid Response Team2
ASA at Arrival4# of Code Blues/1000 Inpatient Discharges2,2a,3
GRADES: = Worse Than Target = At Target = Better Than Target
AMH Mortality4
1
11
2
1
Pe
rce
nta
ge
Actual Expected

Sample Board Dashboard Format
CULTURE Benchmark FY Target FY 06 QTR 1 FY 06 QTR 2 FY 06 QTR 3FY 06 QTR
4
Employee Turnover Rate (Annual) .5%/month 2.50% 2.41% 2.84% 2.79% 3.00%
RN Vacancy Rate 1.00% 8% 18.00% 10.00% 5.00% 7.00%
PREVENTING HARM (Safety) Benchmark FY Target
Falls with injury (Quarterly) 0 5 TO 10 15 18 10 3
Medication Errors (ADEs) Category E-I .025/1000 doses 2/1000 doses 3.5 5.0 4.0 1
Central Line Infections Rate (Critical Care Units) 0 3 TO 5 2 6 0 0
Ventilator Associated Pneumonia 0 1 case per quarter 0 1 5 1
Pressure Ulcers 0 10 to 15 40 30 15 12
CLINICAL QUALITY Benchmark FY Target
EVIDENCE-BASED CARE % OF PATIENTS RECEIVING ALL REQUIRED ELEMENTS
Acute MI 100% 90-95 98% 98% 97% 95%
Pneumonia 100% 80-90 89% 88% 82% 79%
Congestive Heart Failure 100% 90-95 98% 93% 94% 97%
Surgical Infection Prevention Protocol 100% 100 96% 98% 98% 98%
Mortality Rate (HSMR) 40 80 to 85 101 84 84 60
FINANCIAL HEALTH Benchmark FY Target
Cost/discharge $4,200 $5,500 $4,900 $5,100 $7,000 $6,000
Days Cash On Hand 180 days 80-90 91 80 67 82
Sample Board Dashboard Below Target Meeting TargetExceedsTarget

31
Associates, L.L.C.
Pugh Ettinger McCarthy
IHI 2007
Summary Every hospital board should adopt a set of high
level performance measures and targets used to define expectations and track performance
Content and systematic review is more important than format
Use All-or-None Targets for Key Clinical Measures
Asking good questions the key to successful governance

32
Associates, L.L.C.
Pugh Ettinger McCarthy
IHI 2007
For More Information
Michael Pugh
Pugh Ettinger McCarthy Associates, LLC
P.O. Box 8298
Pueblo, Colorado 81008
719 542-2433 Direct
719 542-2564 Fax
Institute for Healthcare Improvement www.ihi.org
Center for Healthcare Governance
www.americangovernance.com
These slides may be used by others only in their existing format with proper attribution/service marks of Pugh Ettinger McCarthy Associates, IHI and the Center for Healthcare Governance

IHI 2007Associates, L.L.C.
Pugh Ettinger McCarthy Institute for Healthcare Improvement 2007
Questions/Comments?

34
Associates, L.L.C.
Pugh Ettinger McCarthy
IHI 2007
Future WSHA & AWPHD Programs
Governing Board Orientation & Education
May 1, 2007
12-1 PM

35
Associates, L.L.C.
Pugh Ettinger McCarthy
IHI 2007
Future WSHA & AWPHD Programs
CEO & Trustee Quality Summit
SeaTac Hilton
May 31, 2007
8 AM-5 PM Facilitated by Dr. James Reinertsen

36
Associates, L.L.C.
Pugh Ettinger McCarthy
IHI 2007
Future WSHA & AWPHD Programs
Rural Hospital Summer Workshop
Campbell’s Resort
Chelan, WA
June 25-27, 2007 Dennis Stillman: Board Self-Evaluation Brad Berg: Compliance Planning Jan Jennings: Building Better Boards and
Managing a Hospital in the 21st Century

37
Associates, L.L.C.
Pugh Ettinger McCarthy
IHI 2007
Future WSHA & AWPHD Programs
WSHA 75th Annual Meeting
Bell Harbor International Conference Center
Seattle, WA
October 11, 2007
1:00-3:00 PM Mock Board Meeting – Relationships,
Learning, Decision-making, and Behavior: Larry Walker, playwright

IHI 2007Associates, L.L.C.
Pugh Ettinger McCarthy Institute for Healthcare Improvement 2007
Thank you for participating!
Please fill out the evaluation.