Identifying - CEConnection for Nursingnursing.ceconnection.com/ovidfiles/01244666-200809000... ·...
6
Identifying
Transcript of Identifying - CEConnection for Nursingnursing.ceconnection.com/ovidfiles/01244666-200809000... ·...

Identifying

Delineated as a blockage ofeither the small or large intes-tine, intestinal obstruction is anacute condition. Every year, atleast 1 in 1,000 patients is diag-nosed with this condition.1
Intestinal obstruction may becategorized as mechanical ornonmechanical, and can lead toperforation of the bowel, sepsis,or electrolyte imbalances.2
Moreover, a lack of sufficientblood supply to the intestinecan result in bowel infarction.2
Intestinal obstruction must beaddressed as soon as it’s diag-nosed because the conditionoften rapidly develops into anemergency situation.3
AnatomyThe digestive tract extends fromthe mouth to the anus, and isapproximately 7.6 to 9.1 meterslong.4 Included within this tract isthe gastrointestinal (GI) tract,comprised of the esophagus,stomach, and the small and largeintestine. Accessory organs ofthe GI system include the liver,pancreas, and gall bladder.
The stomach is a pouchlikestructure that serves as a tempo-rary storage area for food duringthe early stages of digestion. Thestomach breaks down food intoabsorbable components andmoves the contents to the smallintestine, where they combine
with pancreatic secretions andbile from the liver. Almost allfood nutrients are absorbed intothe bloodstream via the smallintestine. The large intestine joinsthe small intestine at the ileocecaljunction, where unabsorbedproducts from the small bowel—including water, fiber, and elec-trolytes—pass into the large intes-tine. The body receives 90% ofthe liquid from digestion fromthe large intestine, which pro-vides sodium and water to therest of the body. As this fluidis removed from the bowel, thesolid waste remains to beexpelled. (See Organs of theGI system.)
www.nursing2008criticalcare.com September l Nursing2008CriticalCare l 19
1.5ANCC/AACN
CONTACT HOURS
intestinal obstruction
Better safe than sorryBy Susan M. Goldberg, RN, CNOR, BS

Mechanical obstructions A mechanical bowel obstruction isdefined as a partial or completeblockage of the intestine. Theseobstructions can occur in eitherthe small or large bowel, arise inall ages and genders, and are trig-gered by the following:3
Adhesions. These accountfor 50% to 70% of all intestinalobstruction cases.1 Some adhe-sions are congenital, while some
are caused by prior abdominalsurgery. Composed of tough bandsof tissue, adhesions can connectintestines to each other or to adja-cent organs. In some cases, thistight, fibrous tissue drags theintestines out of place, where theycan become blocked or twisted.
Hernias. These occur whenthe muscle wall, which holdsthe internal organs in place,weakens or tears. The danger of
an untreated hernia occurs if partof the intestine protrudes throughthis weakened area. In somecases, it might be possible for thehealthcare provider to manuallypush the intestine back into theabdominal cavity, but it’s only atemporary fix. If the intestinebecomes incarcerated, the bloodsupply to the bowel is dimin-ished, leading to ischemia ornecrosis. Gangrene and bowelperforation are serious complica-tions that can lead to infectionand death.5
Volvulus. This occurs whenthe bowel becomes twisted onitself and cuts off its own bloodsupply. This leads to bowelischemia and gangrene. Theprocess can occur quickly andcan progress to gangrene within6 to 12 hours.1
Intussusception. This occursmost often in infants when theintestine telescopes and one partof the bowel slips into another.The prognosis for this condition isgood, especially if surgery is per-formed immediately upon diag-nosis. Death becomes more likelyif intussusception isn’t treatedwithin 24 hours.2 (See Causes ofintestinal obstruction.)
Crohn’s disease. This diseaseis a recurrent, granulomatous typeof inflammatory bowel disease(IBD). While medications haveproven to be effective in creatingand maintaining remission insome cases of Crohn’s disease,two-thirds to three-quarters ofpeople with the condition eventu-ally need surgery.6 As a resultof the inflammatory response,the bowel wall thickens and theintestinal lumen narrows, whichmay result in an intestinalobstruction.2,6 Patients withrecurrent symptoms or complica-
20 l Nursing2008CriticalCare l Volume 3, Number 5 www.nursing2008criticalcare.com
Identifying intestinal obstruction
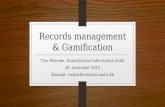
Organs of the GI systemThis illustration shows the organs of the GI tract and several accessory organs.
Esophagus
Descending thoracic aorta
Liver
Stomach
Gallbladder
Duodenum
Rugae
Pancreas
Superior mesenteric vein and artery
Transverse colon
Ascending colon
Descending colon
Small intestine
Ileocecal valve
Cecum
Vermiform appendix
Sigmoid colon
Rectum
External anal sphincter muscles
Anus

tions of Crohn’s disease, suchas abscess formation or intesti-nal obstruction, may requireadditional surgery.6
Foreign body obstruction. Aremarkable number of items areaccidentally ingested or deliber-ately inserted into the digestivetract. These items must beremoved before they perforatethe intestine, block the normaldigestive flow, or cause irritationor inflammation that can leadto infection.
Benign or cancerous tumors.Colon cancer is on the decline—deaths from colorectal cancer de-creased 5.7% from 2002 to 2004.7
Tumors resulting from colon can-cer block the intestines. Tumorsfrom other sources, such as theliver, pancreas, or pelvic organs,may also compress portions ofbowel to the point of ischemia.
Diverticular disorders.These are disorders in whichsmall pouches, called diverticula,develop inside the intestinalwall.2 When treated medicallyand with dietary adjustments,patients can sometimes preventthis condition from worsening.If the sacs become infected orinflamed, diverticulitis develops.Infection occurs when foodbecomes trapped in a diverticu-lum, creating inflammation andinfection. If a diverticulum wereto rupture under these condi-tions, emergency surgical inter-vention would become necessary.
Other causes of mechanicalobstruction include fecalimpaction, or intestinal infectionssuch as Salmonella, Shigelladysenteriae, and Escherichia coli.1
Nonmechanical causesA nonmechanical bowelobstruction is called an ileus.
This occurs when peristalsisstops. Peristalsis is the involun-tary, rhythmic contraction of themuscles of the GI tract thatforces the contents along.4
Without movement, intestinalcontents collect. This stasis ofpartially digested food or lackof motion can lead to inflamma-tion, infection, and possiblerupture. Peritonitis, sepsis,and death may rapidly follow.Nonmechanical causes include:
Medications. Opioids andsome antipsychotic drugs,antidepressants, and antihista-mines are known to slow peri-stalsis. Patients who undergochemotherapy are advised topractice good bowel habits, such as increasing fluid and
fiber intake, since chemotherapy can slow bowel function.
Abdominal injury. Blunt forcetrauma to the abdomen can leadto intra-abdominal bleeding. Thiscan harm the bowel in severalways. For instance, blood lossfrom the injury redirects normalblood flow from the intestines.If the intestines themselves areinjured, blood loss coupled withinfectious GI spillage occurs.Bowel obstruction can also bea postoperative complication ofabdominal surgery.
DiagnosisSymptoms, history, and a lackof bowel sound alert healthcareproviders to the potential of anobstructed bowel. (See Prevent-
www.nursing2008criticalcare.com September l Nursing2008CriticalCare l 21
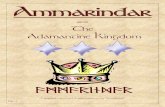
Possible causes of intestinal obstruction(A) Intussusception invagination or shortening of the colon caused by themovement of one segment of bowel into another. (B) Volvulus of the sig-moid colon; the twist is counterclockwise in most cases. Note the edem-atous bowel. (C) Hernia (inguinal). The sac of the hernia is a continuationof the peritoneum of the abdomen. The hernial contents are intestine,omentum, or other abdominal contents that pass through the hernialopening into the hernial sac.

ative measures.) If a patient hasa prior history of obstructionsor of a chronic illness, such asIBD, the index of suspicionwould be raised.
Diagnosis is confirmed with X-ray or computed tomography(CT) study. An ultrasound wouldalso indicate the existence andlocation of the intestinal block-age. A barium enema may beused in selected cases.
TreatmentWith any suspicion of intestinalobstruction, the patient shouldbe advised not to eat or drinkanything until a specific diagno-sis is made. If an obstructionexists, more food or liquidwould put additional pressureon the bowel from above.Should this patient requiresurgery, maintaining an N.P.O.status is essential.
When a patient presentswith an intestinal obstructionthat requires immediate atten-tion, a nasogastric tube is insert-ed to clear the stomach andintestines above the blockage.This helps reduce some of thepressure inside the bowel andhopefully prevent a rupture.The tube is left in place andconnected to suction to preventthe persistent vomiting of gas-tric secretions common with abowel obstruction.
Because the digestive processis disrupted, the patient is indanger of dehydration and elec-trolyte imbalance. Water, plusessential nutrients and miner-als, are trapped in the bowel,excluding them from generalcirculation. This may cause apotassium im-balance that canaffect the function of the heart.In these cases, I.V. fluid and
electrolyte replacement mustquickly be addressed.
Whether or not a rupture ofthe intestine has occurred, antibi-otic therapy is recommended. Anonruptured, inflamed bowel iscategorized by the Centers forDisease Control and Preventionas a class II: clean-contaminatedsurgical site.8 There’s an increasedrisk of infection because thesurgery is performed on aninflamed part of the body. If theintestine ruptures with grossspillage of bowel contents, therisk of infection rises to class III:contaminated. Antibiotic therapyis prudent at this juncture.However, caution must be takento prevent the overuse of antibi-otics that may destroy essentialintestinal bacteria.
Not all bowel resections occurunder urgent circumstances. Forinstance, there are cases when apotential intestinal obstructioncould be caused by increasingtumor size. Waiting to operateuntil a preoperative course ofradiation shrinks the tumor mayimprove the surgical outcome.Patients with a hernia or IBDmay schedule their surgery undermore controlled circumstances.
Surgical interventionWhen a patient is able to elec-tively schedule her intestinalresection, a bowel preparationis often prescribed. This may
include a low residue or liquiddiet for a day or two prior tosurgery, and mechanicalcleansing of the colon witheither a laxative, an enema,or both.
It was thought that emptyingthe colon of solid waste reducesthe amount of bacteria presentwhen the resection is performed.However, the necessity of thepreoperative bowel preparationhas recently been questioned.In a recent study, patients whoperformed mechanical bowelpreparation had a higher rateof wound infection, pulmonarycomplications, and morecomplications overall.9
Intraoperative medicationadministration may depend onthe preoperative diagnosis.Antibiotics are routinely used,due to the infection risk classifi-cation of clean-contaminatedor contaminated.
Perioperative precautionsSince these cases pose such a
22 l Nursing2008CriticalCare l Volume 3, Number 5 www.nursing2008criticalcare.com
Identifying intestinal obstruction
Preventative measures Overall, there isn’t any one thing that prevents intestinal obstructions. It’sworthwhile to maintain good bowel health and prevent fecal impaction withgood health habits, such as a high fiber diet, drinking enough water, andusing stool softeners if necessary.3
Since bowel obstructions can’t always be prevented, recognizing thesigns and symptoms and acting on them before the situation becomes life-threatening is crucial. The following should be addressed by a healthcareprovider if they persist or cause a change in overall status:3
• abdominal pain or cramping• abdominal distention• nausea and vomiting• fever with a temperature above 101°F (38.3°C)• dehydration • diarrhea (may be early sign of obstruction)• constipation or no flatus.

high risk of infection, additionalmeasures are taken in the OR.
Many surgeons irrigate theperitoneal cavity with warm0.9% sodium chloride solutionor an antibiotic irrigation solu-tion before closing to furtherdecrease contamination.
Intraoperatively, the patientis monitored for fluid and elec-trolyte balance by the anesthe-sia care provider. If an indwellingcatheter is in place, care mustbe taken to monitor output andobserve the color of the urine. Ifthe patient experienced traumawith extensive internal damage,kidney and bladder function mustbe closely observed. Dependingon the patient’s condition, thesurgeon’s preference, and thelocation of the blockage, surgerymay be performed through anopen incision or via laparoscopy.
PrognosisThe outcome of an intestinal
obstruction depends on an earlydiagnosis and prompt treatment.Complications of untreatedobstruction include strangula-tion, perforation, sepsis, anddeath.1
Remember that the patientmay be compromised by infec-tion, dehydration, electrolyteimbalance, or any preexistingconditions he might have beyondthe current emergency. By care-fully managing all aspects of theperioperative experience, we canhelp provide the best outcome forour patients. �
REFERENCES
1. Gale Encyclopedia of Children’s Health.Intestinal obstructions health article. Avail-able at: http://www.healthline.com/galecontent/intestinal-obstructions. Accessed January24, 2008.
2. Porth CM. Essentials of PathophysiologyConcepts of Altered Health States. 2nd ed.Philadelphia, PA: Lippincott Williams &Wilkins; 2007.
3. Griffith HW. Complete Guide to Symp-toms, Illness, and Surgery. 5th ed. The
Berkley Publishing Group; 2006.
4. Chang A, Hawley HB, Katz LM, Pi-otrowski NA, Rizzo C. Magill’s MedicalGuide. 3rd ed. Hackensack, NJ: SalemPress; 2005:1430-1433.
5. Homan WP. The Hernia Book: SoundAdvice on Symptoms and Treatment. NewYork, NY: Consumers Union of UnitedStates; 1993.
6. Crohn’s and Colitis Foundation of Amer-ica. Surgery for Crohn’s disease. Availableat: http://www.ccfa.org/printview?pageUrl=/info/surgery/surgerycd. Accessed January24, 2008.
7. American Cancer Society. ColorectalCancer: Early Detection. Available at:http://www.cancer.org/docroot/CRI/content/CRI_2_6X_Colorectal_Cancer_Early_Detection_10.asp. Accessed February 8,2008.
8. Surgical Wound Classification accordingto the CDC. Available at: http://www.qi.org.tw/pms/wounds/wound.asp. Accessed January24, 2008.
9. Allen G. Evidence for practice: bowelpreparation. AORN J. 2005;83(3).
Susan M. Goldberg is a perioperative educator,Frederick Memorial Hospital, Frederick, Md.
Adapted from: Goldberg SM. Identifying intestinalobstruction: better safe than sorry. OR Nurse.2008;2(3):21-27.
The author has disclosed that he has no signifi-cant relationship with or financial interest in anycommercial companies that pertain to this educa-tional activity.
www.nursing2008criticalcare.com September l Nursing2008CriticalCare l 23
INSTRUCTIONSIdentifying intestinal obstruction: Better safe than sorry
Earn CE credit online:Go to http://www.nursingcenter.com/NCC and
receive a certificate within minutes.
DISCOUNTS and CUSTOMER SERVICE
• Send two or more tests in any nursing journal published by LippincottWilliiams and Wilkins together and deduct $0.95 from the price of each test.• We also offer CE accounts for hospitals and other health care facilities onnursingcenter.com. Call 1-800-787-8985 for details.
PROVIDER ACCREDITATION
Lippincot Williams & Wilkins, publisher of Nursing2008 Critical Care, willaward 1.5 contact hours for this continuing nursing education activity.
LWW is accredited as a provider of continuing nursing education by theAmerican Nurses Credentialing Center’s Commission on Accreditation.
LWW is also an approved provider of continuing nursing education by theAmerican Association of Critical-Care Nurses #00012278 (CERP Category A),District of Columbia, Florida #FBN2454, and Iowa #75. LWW home studyactivities are classified for Texas nursing continuing education requirementsas Type 1. This activity is also provider approved by the California Board ofRegistered Nursing, Provider Number CEP 11749, for 1.5 contact hours.Your certificate is valid in all states.
TEST INSTRUCTIONS
• To take the test online, go to our secure Web site athttp://www.nursingcenter.com/NCC.• On the print form, record your answers in the testanswer section of the CE enrollment form on page 24.Each question has only one correct answer. You maymake copies of these forms.• Complete the registration information and courseevaluation. Mail the completed form and registrationfee of $17.95 to: Lippincott Williams & Wilkins, CE Group,2710 Yorktowne Blvd., Brick, NJ 08723. We will mail yourcertificate in 4 to 6 weeks. For faster service, include a faxnumber and we will fax your certificate within 2 busi-ness days of receiving your enrollment form.• You will receive your CE certificate of earned contacthours and an answer key to review your results. Thereis no minimum passing grade.• Registration deadline is October 31, 2010.