ICF short course (elementary) on clinical use of ICF
60
Interprofessional Collaborative Practice: In the desert or on the mountain… Stefanus Snyman
-
Upload
stefanus-snyman -
Category
Health & Medicine
-
view
49 -
download
3
Transcript of ICF short course (elementary) on clinical use of ICF

Interprofessional Collaborative Practice:
In the desert or on the mountain…
Stefanus Snyman

International Classification of Functioning, Disability & Health
--- Interprofessional Care Framework for the biopsychosocialspiritual
approach to patients, communities and systems ---
DAY 1: The ICF? What is it?

What on earth are you doing here?
• Name
• What do you do?
• Expectations of the ICF course?

Outcomes of ICF series of workshops
• Apply the WHO’s ICF as a framework for
interprofessional collaborative practice to
improve patient outcomes and strengthen
health systems.
• Argue why the ICF framework may be a
catalyst to improve patient-centred and
community-centred care, as well as the
morale and motivation of staff.

CPD
• If everything is attended and all assignments
done on time:
• 14 General
• 3 Ethics

Overview of ICF series (1)
• Day 1: (2h)
• Introduction to Health Professions Education for
21st century:
• Overview of the ICF framework in the context of
ethics and human
• Interprofessional teams case study
• After Day 1
• Structured reflection (½h) (within 1 week)
• Each interprofessional team prepare 1 case study
to present at next workshop (3h)

Overview of ICF series (2)
• Day 2 (2h)
• Presentation by interprofessional teams on their
real case study (Summative and formative
assessment by peers (including ethics / human
rights)
• Sit in with student case discussions / assessments
• After Day 2
• Structured reflection on interprofessional case study
that your team presented (1hour)
• Prepare a draft document to submit to the
Department of Health motivating the ICF framework
as an approach to encourage patient-centred and
community-centred care (4 hours)

Overview of ICF series (3)
• Day 3:
• Interprofessional teams conduct a ward round in
hospital (1 patient for a group) based on the ICF
framework, including team discussion, management
plan and feedback to patient
OR
ICF coding for quality improvement purposes
• Feedback by interprofessional teams regarding their
proposed approach to present to the Department of
Health a motivation to promote the use of the ICF
framework to improve patient- and community-
centred care
• Summative and formative assessment of
presentation
• After Day 3:
• Evaluation of course

Learning Resources
• Taking notes during this contact session
• ICF Practical Guide
• ICF and ICF-CY Books
• ICF online: http://www.who.int/classifications/icf/en/
• ICF eLearning tooI:
Your common sense !!!

The future of HPE in 1910
• Introduction of basic sciences in medical curricula
• Doubling of human lifespan1910

November 2010

Lancet December 2010
Health professionals have made huge contributions to
health and socio-ecomonic development over the past
century, but we cannot carry out 21st century health
reforms with outdated or inadequate competencies….
That is why we call for a new round of more agile and
rapid adaption of core competencies based on
transnational, multi-professional, and long-term
perspectives to serve the needs of individuals and
populations
What we need, more than just disciplinary knowledge and
skills, is a well-rounded health professional acting as
change agent to address the health needs of the 21st
century

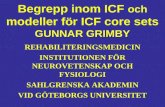
Transformative
Learning
Interdependence
in
Education
Health Equity
Patient-centred Population-
based
Locally responsive
Globally connected
Open educational resources
Competency-based
Responsive to rapidly
changing needs
Creative use of IT
VISION
Adapted from: J
Frenk, L Chen, ZA
Bhutta et al: Health
Professionals for a
new century:
transforming
education to
strengthen health
systems in an
inderdependent
world.
www.thelancet.com,
2010;376:1923-1958
The Lancet et al. challenge


Adapted with the permission of CanMEDS © 2005


In search of an Interprofessional Care/Collaboration
Framework: a common language and approach
A statistical, research,
clinical, social policy
and educational tool to:
• Provide scientific basis
• Interprofessional
teamwork
• Common language
• Permit comparison
• Systematic coding
scheme


The pilot study: ICF – catalyst for IPECP

Interdependence
• Appreciate community workers
role
• Commit to teamwork
Transformative learning
• Ownership for holistic
patient care
• Question biomedical model
used in tertiary hospitals
• Integrate ethics and
human rights in patient
care
• Initiate IPE community
projects in response to
gaps indentified using ICF
Health system strengthening
• Preceptors apply ICF in
teaching and practice
• Adopt ICF as approach to
patient care in PHC and district
hospital settings
• Service providers request
capacity building in ICF
• Influence patient outcomes
Assessment drives
practice
Results from study

International importance
• Play role to write WHO’s ICF Practical Guide
• WHO book on CBE just published
• 1 of 4 projects worldwide selected by Institute of
Medicine’s Global Forum of Innovation in Health
professions Education


The qualifiers
Individual / Community
Functioning & Disability
Body function & structure
Change in body function
Change in body structure
Activities & Participation
Capacity Performance
Contextual factors
Environmental factors
Barriers / Facilitators
Personal Factors


Defining concepts (1): Body function and
structure
• Body functions
Physiological functions of body systems
• Body structures
Anatomical parts of the body

Body function and structure: Impairment
• Any loss of, or abnormality to body
structures/functions
• Anatomical, physical or psychological
• Manifestations of underlying pathology
• Temporary / permanent
• Progressive / regressive / static
• Intermittent / continuous / fluctuant
• Vary in severity

Body function and structure: Impairment
• Mental status
• Sensory functions (vision, hearing, vestibular,
pain)
• Voice and speech
• Vascular and circulatory system
• Respiratory system
• Endocrine, digestive and metabolic
• Genito-urinary and reproductive systems
• Skin and related structures


Defining concepts:
Activity and participation
• ActivityTasks or actions
• Activity limitationInability / difficulty to perform an activity in the manner
or range considered normal for all individuals of a
similar group
• ParticipationLife roles
• Participation restriction
Problems related to social roles

Activity / Participation domains (1)
• Learning and applying knowledge
• General tasks and demands
• Organising and planning tasks
• Multiple tasks
• Using money and finance
• Communication
• Verbal (understanding and producing)
• Nonverbal (understanding and producing)

Activity / Participation domains(2)
• Mobility
• Indoors (home)
• Outdoors
• Transportation


Activity / Participation domains(3)
• Self care
• Personal care
• Health care
• Domestic life
• Domestic management
and tasks

Activity / Participation domains(4)
• Interpersonal interactions
• Family
• Intimate
• Informal
• Major life
• Education
• Employment

Activity / Participation domains (5)
• Community, social
and civic life
• Community
• Recreation and
leisure
• Religion and
spirituality


Defining concepts (4): Contextual factors
• Environmental
• Personal
Represent the specific context and background
of an individuals life

Environmental factors
Barriers or facilitators
2 levels – individual /
social
• Products and
technology
• Natural environment
and man made
changes
• Support &
relationships
• Attitudes
• Services, systems &
policies

Environmental factors

Personal factors
Positive / negative
• Age
• Gender
• Race
• Education
• Experiences
• Personality
• Aptitude
• Coping styles
• Lifestyle
• Fitness, etc.

The ICF
• Function & Disability is…• Result of a complex relationship between
health condition, participation and contextual factors
• Contextual factors
• May hinder / cause barriers
• May facilitate
• No linear relationship between impairment /
activity / contextual factors – demonstrating
the complexity of health

Examples: Disabilities that may be associated
with the 3 levels of functioning linked to a health
condition.

Different levels of disability are linked to three
different levels of intervention.


Example of patient presentation

Rumours
• Time
• Complex
• Impossible

Barriers
• Professional tribalism
• Biomedical model
• Tradition
• Individual stars
• Against transformative learning – a threat


BATHO PELE
Access
Openness and Transparency
Consultation
Redress
Courtesy
Service standards
Information
Value for Money
PATIENT CHARTER
Healthy and Safe environment
Participation in Decision-Making
Access to Health Care
Knowledge of one’s health insurance/medical aid scheme
Choices in health services
Treated by a named health care provider
Confidentiality and privacy
Informed consent
Refusal of treatment
A second opinion
Continuity of care
Complaints about health services
Better patient outcomes and Improvement of health
system

ICF within ethical, human rights and legal
framework
• Ethics:
• Autonomy
• Benevolence
• Non- malevolence
• Justice
• Human rights
• Legal framework

Questions

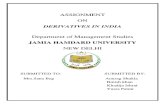
Let’s apply it…
Health condition / disorder /
disease
Body
function &
structure
(Impairment)
Activities
(Limitations)Participation
(Restriction)
Personal
factorsEnvironmenta
l factorsContextual
factors
In context of ethics, human rights and legal
framework

Peter’s story (See handout and video)
PETER
Peter is a 76-year-old male who was diagnosed with Parkinson’s disease approximately 5 years ago. He has been referred by his
neurologist for a PT and OT consult. He lives in a two story row home in South Philadelphia with his wife, Mary. Peter reports that he
had a good understanding of his disease initially, but now feels confused. He has tried to stay active in order to maintain his level of
function. He is very involved in the community and has many long time friends. He has been taking medication, Sinemet, for about 3
years and it has “helped tremendously.”
Peter states that his condition has been steadily worsening, especially over the last 6 months. When he was diagnosed 5 years ago,
his right arm and leg seemed stiff and he had trouble moving them. Now he has more difficulty initiating his movements, especially in
the morning and after he gets to the bottom or top of the stairs. He says, “I get stuck, and I just can’t move.” He also states that it has
been taking him longer and longer to get to where he is going and he is often late for his community activities, such as attending church,
meeting friends for breakfast, and playing cards. He reported falling twice within a week about 2 months ago, both times tripping over
uneven sidewalks. Since then Mary suggested he carry a cane that she used after her hip replacement surgery ten years ago. He
reports that he is “embarrassed” to use it.
He is experiencing increased shaking, and more recently has had some difficulty eating, holding cards, and keeping his buttons on the
bingo cards. Two weeks ago when he was calling numbers for bingo, he pushed the wrong numbers several times and was very upset
and embarrassed. His wife reports that he has always carried the bags for their grocery shopping, but recently he has had difficulty
because he is “too tired.” Mary also reports that he has been getting extremely frustrated with his condition, and wonders if he is
depressed, as he has been leaving the house less frequently.
PMH: BPH, GERD, dyslipidemia, hypertension, Parkinson’s disease (PD)

Peter’s story (See handout and video) 2
Current medications:
terazosin 4mg PO daily
omeprazole 20mg PO daily
atorvastatin 10mg PO daily
hydrochlorothiazide 25mg PO daily
Sinemet (carbidopa/levodopa) 50/200 ER PO at 8am, noon, 3pm, and 7 pm
Sinemet 25/100 IR at 8am, 10am and 5pm
Azilect (rasagaline) 0.5mg PO daily
Comtan (entacapone) 200mg PO four times daily
At Peter’s appointment:
VS: BP 100/68; HR 82; RR 25, T 37°C, Ht 5’11”, Wt 180 lbs
On physical examination, Peter demonstrated decreased passive and active range of motion in bilateral knee extension as well as bilateral shoulder
flexion and abduction, the right being worse than the left. He shows a slight thoracic kyphosis in both sitting and standing posture which can be
minimally corrected with cues, and almost completely corrected with manual assist. He shows decreased active and passive range of motion in trunk
extension, rotation and side bending.
There is limited shoulder ROM in BUE with greater limitations in R vs L (flexion, abduction, rotation), limitations in elbow extension bilaterally,
decreased flexion in fingers leading to decreased dexterity and coordination and in hand manipulation skills, problems with fine motor tasks such as
grasping utensils, manipulating fasteners, and handling small items such as money/coins, and cards.
While walking throughout his home, he had some “freezing” episodes. He also displays some intermittent resting tremors. Mild cogwheel rigidity is
evident in all four extremities. Sensation appears intact throughout.

Peter’s story (See handout and video) 3
Equilibrium reactions appear delayed as evidenced when challenged in standing on a flat surface. He is afraid to stand on a balance beam. He can
stand on right leg for 20 seconds with eyes open, on left for 5 seconds. He starts to fall when he closes his eyes. When walking, there is diminished
arm swing and no trunk rotation. He also has a decreased step length and a slightly narrowed base of support. Walking is worse when he is tired.
Peter manages his medications now with his wife’s help. He has a regimen of taking all his medications at 8AM every morning with his breakfast that
typically consists of eggs and bacon. He used to be very good at remembering to take the other Sinemet doses at the scheduled times, but lately is
forgetting.
His activities include: playing cards and bingo 3 days a week at the local senior center a few blocks from his home, meeting at a breakfast club 3 days
a week at the local diner, attending Sunday and Wednesday Mass, and walking his dog, Paul, at least twice a day.
Peter likes the current lifestyle that he and Mary have established, especially assisting her in household duties of shopping, carrying laundry, and
chopping/prepping for meals. He is looking for ways to decrease his symptoms.
(Acknowledgement: George Washington University

Rest of the day
1• Map your case study's information on the ICF
framework.
2• What additional information do you believe your
team need to adequately address the issues in the
case study? Ask facilitators for information.
• Indicated gaps in the information with "?" on the ICF
framework (or in another colour).
• Does this case raise any specific ethical or human
rights conflicts? Map it on your ICF framework with
"E" (or in another colour).

3• Looking at your completed ICF framework,
determine the management priorities.
• What are the interventions in the case study that the
various professions are qualified to address?
• Compile an interprofessional management plan
(tasks) using the completed ICF chart.
• Motivate who will be doing what.
• What other professions would need to be involved
in this case? Why?
• Ask facilitators for information.

What now?
• Structured reflection • Max 500 words (1-1½ pages). Email to ??
• Prepare your real case study to present on ?? 201?• Each interprofessional team prepare 1 case study to
present at next workshop on ???
• Compile your teams now! Give names to??
• Pitch on ?? 201?: The ICF - it works!
• Diarise the last workshop: ?? The ICF -
what are we waiting for?

Instructions for structured reflection
• Introduce yourself (name, family, occupation,
position)
[2 paragraphs]
• What was your understanding of the ICF before
today? (Refer to the notes you made during the
introductions)
[1 paragraph]
• What on earth were you doing here today? What
was your expectations of this series of
workshops? (Refer to the notes you made during
the introductions) [1 paragraph]
• Identify and critically analyse your positive and
negative feeling about the ICF after the first
session in the context of (1) health professions
education and (2) patient-centred care. [½ -1
page]

Thank you