I -O R A 1D, L T M...Ms. Lauren Villemaire, for training me on the software and techniques required...
21
INTRA-OBSERVER REPRODUCIBILITY AND ACCURACY OF 1D, 2D, AND 3D LUNG TUMOUR MEASUREMENTS 6 WEEK PROJECT REPORT Laura Close Medical Biophysics 3970Z The University of Western Ontario April 1, 2011
Transcript of I -O R A 1D, L T M...Ms. Lauren Villemaire, for training me on the software and techniques required...

INTRA-OBSERVER REPRODUCIBILITY AND ACCURACY OF
1D, 2D, AND 3D LUNG TUMOUR MEASUREMENTS
6 WEEK PROJECT REPORT
Laura Close
Medical Biophysics 3970Z
The University of Western Ontario
April 1, 2011

1
ACKNOWLEDGEMENTS
Dr. Grace Parraga, for welcoming me into her lab group with the opportunity to perform
an educational six-week research project.
Mr. Amir Owrangi, for all of his help and guidance in terms of answering questions and
offering suggestions that best lead to a successful project.
Ms. Lauren Villemaire, for training me on the software and techniques required to
complete this project, with additional help and guidance throughout.
Mr. Andrew Wheatley, for organizing all requirements in setting me up at Robarts
Research Institute, as well as technical support.

2
ABSTRACT
Development and assessment of lung cancer treatments depend on several factors,
including tumour measurement techniques. With use of X-ray computed tomography images,
1D, 2D, and 3D lung tumour measurement methods are compared. Intra-observer
reproducibility of each method is assessed on two patient tumours at nine time points and three
phantom tumours at four slice thicknesses. Accuracy of each method is additionally assessed on
the phantom tumours. 3D measurements display high intra-observer reproducibility and the
highest potential for accurate ground truth measurement reproduction. This provides insight into
the appropriateness of introduction of 3D measurement methods into clinical settings.
INTRODUCTION
It is known that cancer has become the leading cause of death in Canada, and more
specifically, lung cancer is the leading cause of cancer-related death (1). With such a vast
number of people affected, the importance of research in this area is highly stressed. There are
countless variables contributing to the effectiveness of patient treatment that must be recognized.
Such variables include choice of treatment (e.g. chemotherapy, radiation therapy), the length of
time for which the treatment is administered, and how that treatment is monitored longitudinally.
Imaging can play a very important role both in initial tumour assessment and monitoring changes
over time. In order to best utilize cross-sectional tumour images in obtaining useful data,
appropriate tumour measurement techniques are essential. Measurements have great
implications, as the ability to successfully quantify tumour size can directly impact and improve
upon decisions involving treatment requirements and effectiveness. Although two-dimensional
and one-dimensional measurements have been implemented into clinical settings thus far, three-
dimensional measurements have the greatest potential in terms of accurately incorporating
tumour size properties from all planes. Despite the more apparent benefits of volume
measurements, there are other criteria that must be met in order to ensure three-dimensional
methods are reliable. The main objectives of this project are to:

3
1) Determine the intra-observer reproducibility of one-dimensional, two-dimensional, and
three-dimensional measurement methods.
2) Determine the accuracy of one-dimensional, two-dimensional, and three-dimensional
measurements in relation to ground truth measurements.
3) Use these factors to gain insight into whether three-dimensional measurements are
appropriate for use in clinical settings.
THEORY
Methods of Tumour Measurements
Tumour measurement methods have undergone a number of revisions since initial
implementation of such techniques into clinical settings. The most fundamental changes relate to
the number of dimensions incorporated into the measurements. In 1979, the World Health
Organization introduced a 2D measurement defined as the longest diameter of the tumour
multiplied by the longest perpendicular bisector (2). However, there were apparent limitations
with this technique, including the lack of an established minimum lesion size deeming the
technique appropriate, as well as the possibility of longest diameters existing out-of-plane from
the cross-sections being observed (2). This challenged the reproducibility of such measurements
(2). In 2000, Response Evaluation Criteria in Solid Tumours came about, introducing 1D
tumour measurements (2). This overcame certain limitations present with the 2D measurement
technique, including the fact that a minimum lesion size was defined, and higher reproducibility
was exhibited. However, the longest diameter may still exist out-of-plane from the image slices
being observed, and general tumour sphericity is also assumed (2). In order to best overcome the
limitations of 1D and 2D measurements, 3D measurements are ultimately required. An example
of software that has been developed in order to obtain such measurements is 3D Quantify,
created at Robarts Research Institute in London, Ontario. Another software program called
ClearCanvas (ClearCanvas, Inc., Toronto, Canada) is an open-source picture archiving and
communication system (2). As opposed to software such as ClearCanvas, which is capable of
basic 1D and 2D measurements, 3D Quantify contains an algorithm enabling a volume to be
calculated from triangular three-dimensional mesh models of contoured images (2). Three-

4
dimensional measurements account for irregular tumour shapes, and asymmetrical growth rates
or shrinkage rates due to treatment, demonstrating superiority in comparison to 1D and 2D
methods.
Imaging Modality
The details of the imaging process performed impact lung tumour images, and thus, the
measurements performed on these images. X-ray computed tomography is of principle use in
tumour measurements (3). It is able to adequately display the contrasted lung tumour boundary
in relation to background lung tissues (2), and advantageously compares to alternate imaging
modalities. For instance, X-ray radiograph displays flat plane limitations and merging of lung
structures from above or under the region of interest (2). X-ray CT addresses such interference
with slice selection. Additionally, a volume of information is available with the addition of a z-
plane, allowing for 3D representations (2). With availability of thinner slice thicknesses relating
to finer resolution in the z-plane, data within the overall volume of information can be rearranged
in order to generate constructed images in several plane orientations. X-ray CT remains to be the
favourable approach in comparison to other advanced imaging techniques as well, such as
magnetic resonance imaging, which demonstrates disadvantages including limited spatial
resolution and cardiac/respiratory motion, hindering detection of smaller lesions (2). Increasing
availability of X-ray CT scanners, in addition to improvements in resolution, have correlated
with increased detection of smaller lesions (4), which exemplifies one of the many important
implications of this imaging modality.
Lung Tumour Properties
Utilizing the best measurement and imaging techniques are important in terms of
grasping all characteristics of the tumours. Lung tumours, in particular, rarely possess a compact
shape, but are often spiculated with spikes or points on the surface (3). Additionally, tumours
may form against the chest wall or other structures, and differing numbers of blood vessels may
surround or grow within them (3). Over a course of treatment, tumour position may be altered
relative to surrounding blood vessels, and the tumour’s ability to attenuate x-rays may change
(3). Phantom tumours, which are artificially-constructed tumours available for imaging in
artificial lungs, are important in mimicking possible patient tumour geometries for research

5
purposes. In particular, phantom tumours can be useful in applications in which known tumour
dimensions are needed, such as assessing accuracy of software from which tumour
measurements are calculated.
Reproducibility and Accuracy Analysis
With the introduction of new tumour measurement methods, two important statistical
criteria that must be satisfied include reproducibility and accuracy of the measurements.
Reliability, or reproducibility, refers to how reproducible a measurement is when it is randomly
repeated under the same conditions, often in order to assess performance of human observers (5).
The best method for determining reproducibility is by use of the intra-class correlation
coefficient (ICC) (5). Two types of ICC values exist. If systematic variability due to raters is
considered relevant, this rater variability contributes to the ICC calculation, producing an
absolute agreement ICC value (ICC(A)) (6). If rater variability is considered irrelevant, a
consistency ICC value (ICC(C)) is produced (6). Measurement accuracy can be assessed
through comparison of measured values with a set of ground truth measurements. Presence or
absence of statistical differences in data sets can be detected through two-sample, two-tailed t-
tests, with equal/unequal variances defined by preceding f-tests. ICC values ≥ 0.9 are
recommended for clinical measurements (7), and t-test p-values < 0.05 demonstrate evidence to
reject the notion that the means of the two data sets are equal, with a 5% chance of mistaken
rejection.
APPROACH/METHODS
Conditions
X-ray computed tomography images of lung tumours are acquired. Images at nine time
points of a patient undergoing a course of treatment over roughly two years are obtained, in
which two tumours of differing sizes exist in each image. Additionally, images of three irregular
phantom tumours of differing shapes and sizes at four slice thicknesses are acquired. 1D, 2D,
and 3D measurements of each individual tumour under each condition are performed in two
software programs. 1D and 2D measurements are made in ClearCanvas, while 3D

6
measurements are obtained using 3D Quantify. A total of five rounds of measurements are made
for each image, and in order to ensure non-bias, all images are provided completely randomized.
Furthermore, known ground truth measurements of phantom tumours remain secretive at the
time that the measurements are performed, while the patient tumours, due to their nature, have no
such attainable ground truth measurements. One round of measurements per day is not
exceeded. Consistent conditions are also ensured in that images are displayed using the same
display monitor, in a room with consistent low-lighting.
1D Measurements
In order to perform 1D measurements, cross-sectional image slices are manually scrolled
through until the slice with the best potential for containing the longest diameter is visually
depicted. A line measuring this longest diameter is then drawn in ClearCanvas, as displayed in
Figure 1, and a length in centimetres is acquired on the pre-calibrated images.
(a) (b) (c) (d) (e)
Figure 1. 1-Dimensional Measurements. RECIST measurement examples for (a) large patient tumour at time
point 1, (b) small patient tumour at time point 1, (c) large phantom tumour at 0.5mm slice thickness, (d) medium
phantom tumour at 0.5mm slice thickness, and (e) small phantom tumour at 0.5mm slice thickness are displayed.
2D Measurements
2D measurements are also performed in ClearCanvas, in which the initial step in
acquiring the longest diameter measurement is completed in a similar fashion to obtaining the
RECIST measurement. Additionally, a ninety degree angle is measured and the longest
perpendicular diameter is visually depicted and measured, as displayed in Figure 2. The product
of the two diameters results in the WHO measurement.

7
(a) (b) (c) (d) (e)
Figure 2. 2-Dimensional Measurements. WHO measurement examples for (a) large patient tumour at time point
1, (b) small patient tumour at time point 1, (c) large phantom tumour at 0.5mm slice thickness, (d) medium phantom
tumour at 0.5mm slice thickness, and (e) small phantom tumour at 0.5mm slice thickness are displayed.
3D Measurements
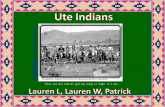
3D volume measurements are obtained using 3D Quantify. Once a cross-sectional image
slice best depicting the tumour is selected, a user-defined rotational axis is drawn across the
tumour. Next, the boundary of the tumour is traced using a sensor pad and pen. The tumour
image is then rotated eighteen degrees about the previously defined rotational axis, and tracing is
repeated. A total of ten tracings are completed with eighteen degrees of rotation between each
displayed cross-section, as illustrated in Figure 3. A resulting set of contours and corresponding
3D triangular mesh are created, and a volumetric measurement and model are displayed, as
shown in Figure 4.
Figure 3. Generation of a Mesh Model. An example of the
generation of a 3D mesh model for the medium phantom at 0.5mm
slice thickness is displayed. Ten required tumour tracings are shown,
beginning at the top left image, with eighteen degrees of rotation
between each tracing. The final model is indicated in the red circle.

8
(a) (b) (c) (d) (e)
Figure 4. 3-Dimensional Measurements. Volumetric measurement examples for (a) large patient tumour at time
point 1, (b) small patient tumour at time point 1, (c) large phantom tumour at 0.5mm slice thickness, (d) medium
phantom tumour at 0.5mm slice thickness, and (e) small phantom tumour at 0.5mm slice thickness are displayed.
RESULTS
Measured Tumour Size under Varying Conditions
Results obtained are based on a total of 450 measurements consisting of five rounds of
measurements of each tumour (patient/phantom) in each condition (time point/slice thickness).
Figures 5-7 act as visual representations of change in large and small patient tumour size over the
course of treatment lasting almost two years, as seen using RESIST, WHO, and volume
measurements, respectively. Each data point represents an average of five rounds of
measurements, with each error bar representing the corresponding standard deviation. General
decreasing tumour size trends are visually apparent with each measurement technique, with
greatest fluctuations existing in the case of 3D measurements.
(a) (b)
Figure 5. RECIST Measurements over Elapsed Treatment Time. Relationships between mean measured
patient tumour size and time in years using 1-dimensional measurements for (a) large and (b) small tumours are
displayed.
0
1
2
3
4
5
6
0.00 0.50 1.00 1.50 2.00
Mea
n R
EC
IST
Dia
met
er (
cm)
Time (years)
0
0.5
1
1.5
2
2.5
3
0.00 0.50 1.00 1.50 2.00
Mea
n R
EC
IST
Dia
met
er (
cm)
Time (years)

9
(a) (b)
Figure 6. WHO Measurements over Elapsed Treatment Time. Relationships between mean measured patient
tumour size and time in years using 2-dimensional measurements for (a) large and (b) small tumours are displayed.
(a) (b)
Figure 7. Volume Measurements over Elapsed Treatment Time. Relationships between mean measured patient
tumour size and time in years using 3-dimensional measurements for (a) large and (b) small tumours are displayed.
Visually descriptive plots are shown for phantom tumours in Figures 8-9, incorporating
large, medium, and small tumour measurements at four slice thicknesses for 1D, 2D, and 3D
measurement techniques. Again, data points represent averages of five measurement rounds
with corresponding standard deviations represented as error bars. Figure 8 displays RECIST and
WHO measurements, in which no obvious trends can be visually observed in relation to
0
2
4
6
8
10
12
14
16
18
20
0.00 0.50 1.00 1.50 2.00
Mea
n W
HO
(cm
^2
)
Time (years)
0
1
2
3
4
5
6
0.00 0.50 1.00 1.50 2.00
Mea
n W
HO
(cm
^2
)
Time (years)
0
20
40
60
80
100
120
140
160
0.00 0.50 1.00 1.50 2.00
Mea
n V
olu
me
(cm
^3
)
Time (years)
0
5
10
15
20
25
30
0.00 0.50 1.00 1.50 2.00
Mea
n V
olu
me
(cm
^3
)
Time (years)

10
increasing slice thickness. Figure 9 displays volume measurements in which positive linear
trends are displayed for each phantom tumour with corresponding coefficients of determination.
In this case, increasing slice thickness correlates with increases in acquired measurements.
(a) (b)
Figure 8. RECIST and WHO Measurements over Increases in Slice Thickness. Relationship between mean
measured phantom tumour size and slice thickness for large, medium, and small phantom sizes using (a) 1-
dimensional measurements and (b) 2-dimensional measurements.
Figure 9. Volume Measurements over Increases in Slice Thickness. Relationship
between mean measured phantom tumour size and slice thickness for large, medium, and
small phantom sizes using 3-dimensional measurements is displayed.
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
0 2 4 6
Mea
n R
EC
IST
Dia
met
er (
cm)
Slice Thickness (mm)
0
2
4
6
8
10
12
14
0 2 4 6
Mea
n A
rea (
cm^
2)
Slice Thickness (mm)
Phantom 1
Phantom 2
Phantom 3
R² = 0.9939
R² = 1
R² = 0.69550
5
10
15
20
25
0 1 2 3 4 5 6
Mea
n V
olu
me
(cm
^3
)
Slice Thickness (mm)
Phantom 1
Phantom 2
Phantom 3

11
Intra-Observer Reproducibility
Statistics relating to intra-observer reproducibility are displayed in Tables 1-2, in which
absolute and consistency intra-class correlation coefficients are shown. In Table 1, ICC values
are displayed for the pair of patient tumours at each time point and each measurement method.
In Table 2, ICC values are displayed for the set of phantom tumours at each slice thickness and
each measurement method. In both tables, the values that are ≥ 0.9, as indicated by the lightest
background colour, demonstrate recommended reliability for clinical measurements (7). For
patient tumours in Table 1, all values are clinically acceptable except for those corresponding to
select time points in the case of the 3D measurements. For phantom tumours in Table 2, all
values displayed are clinically acceptable.
1D 2D 3D
ICC(A) ICC (C) ICC(A) ICC (C) ICC(A) ICC (C)
1 0.983 0.983 0.982 0.977 0.98 0.974
2 0.966 0.96 0.999 0.999 0.839 0.888
3 0.971 0.966 0.977 0.996 0.993 0.991
4 0.995 0.996 0.986 0.989 0.992 0.993
5 0.975 0.979 0.991 0.993 0.847 0.849
6 0.975 0.972 0.948 0.958 0.891 0.897
7 0.982 0.982 0.973 0.973 0.718 0.712
8 0.982 0.99 0.972 0.978 0.923 0.925
9 0.987 0.99 0.957 0.957 0.858 0.843
Table 1. Intra-Observer Reproducibility Statistics for Patient Tumours. Absolute and consistent ICC values
for the set of two patient tumours at each time point are displayed.
1D 2D 3D
ICC(A) ICC (C) ICC(A) ICC (C) ICC(A) ICC (C)
0.5mm 0.996 0.997 0.995 0.993 0.997 0.997
1.0mm 0.997 0.998 0.995 0.998 0.997 0.997
2.0mm 1 1 0.991 0.995 0.996 0.997
5.0mm 0.995 0.995 0.993 0.995 0.984 0.997
Table 2 . Intra-Observer Reproducibility Statistics for Phantom Tumours. Absolute and consistent ICC values
for the set of three phantom tumours at each slice thickness are displayed.
Accuracy
Measurement accuracy is depicted in Table 3, in which performed measurements are
compared to the known sets of ground truth measurements for phantom tumours. P-values from
two-tailed t-tests, assuming unequal variance (as all F-test p-values are less than 0.05) are shown
for each phantom tumour at each slice thickness and measurement technique. Using an alpha
ICC Values
≥0.9
≥0.8
≥0.7
ICC Values
≥0.9
≥0.8
≥0.7

12
value of 0.05, values with the lightest background colour demonstrate situations for which the
performed measurements are not statistically different from the ground truth measurements.
Such values are only apparent in the case of the 3D measurements.
Slice Thickness Tumour 1D 2D 3D
0.5mm
Large 0.000 0.000 0.008
Medium 0.000 0.000 0.038
Small 0.019 0.000 0.540
1.0mm
Large 0.000 0.000 0.291
Medium 0.000 0.000 0.002
Small 0.001 0.001 0.001
2.0mm
Large 0.000 0.000 0.957
Medium 0.000 0.000 0.008
Small 0.000 0.001 0.010
5.0mm
Large 0.000 0.000 0.020
Medium 0.000 0.000 0.001
Small 0.003 0.000 0.001
Table 3. Accuracy Statistics for Phantom Tumours. P-values obtained by 2-sample, 2-tailed
t-tests assuming unequal variance, comparing each phantom tumour at each slice thickness
against corresponding ground truth measurements are displayed.
DISCUSSION
The results that have been obtained incorporate any error or variation due to every step in
the process of obtaining final measurements including the imaging process, software capabilities,
measurement technique, and performance of the individual. The choice between 1D, 2D, and 3D
measurements methods, however, is shown to be a large factor in influencing tumour size
estimates. In the case of measured tumour size at various time points over a course of treatment,
all methods display general decreasing tumour size trends over time. It is noted, however, that
the volume measurements display the largest fluctuations, or the least consistent decreasing
trends, in comparison to the 1D and 2D measurements. Taking ten dimensions into account, as
opposed to only one, appears to provide a higher likelihood of such fluctuations. Furthermore,
data points displayed with large error bars (standard deviations), likely correspond to less clearly
defined tumour images due to factors such as poor contrast in relation to background structures.
For poorer images, ten boundary estimations likely provide even more room for error in
comparison to straight-forward linear measurements. Though relatively large error bars are
present with the first, and especially the second, time points in the 3D measurements (Figure 7),
p<0.001
0.001<p<0.01
0.01<p<0.05
p>0.05

13
this pattern is not consistent, as relatively negligible error bars exist for time points in which
more properly defined images are likely present.
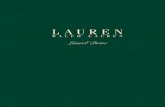
The measured phantom tumours at varying slice thicknesses also display interesting
results. There does not appear to be an obvious effect of slice thickness on 1D and 2D
measurements, while, based on the results, 3D measurements appear to increase as slice
thickness increases. Reasoning behind this perceived increase is somewhat visually apparent in
Figure 10. Increased slice thickness corresponds to blurrier, less defined boundaries. In
performing linear measurements, only a limited portion of the boundary is incorporated into
these measurements, and an increase in blurring does not seem to have a significant effect.
However, while performing 3D measurements, the entire tumour boundary comes into play ten
times, and a blurred boundary may cause a broader outline to be drawn, resulting in possible
overestimation of tumour volume. Other studies support the notion of increases in error with
increases in slice thickness, in which such error is found to be statistically significant (8).
(a) (b) (c)
Figure 10. Slice Thickness Effects on Tumour Appearance. Differences in
tumour appearance between 0.5mm slice thickness (top row) and 5.0mm slice
thickness (bottom row) are indicated for (a) large (b) medium and (c) small phantom
tumours.
High intra-observer reproducibility is an important requirement for any measurement
technique in order to demonstrate reliability required for practical use. Intra-class correlation
coefficients (Table 1) demonstrate that, in the case of the patient tumour measurements, all 1D
and 2D measurements, and four out of the nine 3D measurements display required

14
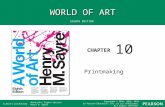
reproducibility for clinical settings. As mentioned earlier, poorly contrasted tumour images can
correspond to increased variability, especially in the case of 3D measurements. Figure 11
demonstrates a time point at which the ICC values fall below the required magnitude.
Boundaries are not clearly defined in these images, as the larger tumour displays similar
attenuation to the surrounding structure, and the smaller tumour displays an unclear boundary
portion along the pleural surface.
(a) (b)
Figure 11. Images from which 3D Reproducibility is
Below Requirement. (a) Large and (b) small patient
tumours at time point 9 are displayed.
Alternatively, ICC values (Table 2) for 1D, 2D, and 3D measurements at all slice
thicknesses for the phantom tumours all demonstrate the required reproducibility for clinical
settings. The phantom tumours have more clearly defined boundaries and act as better
representations of true 3D measurement capabilities in terms of intra-observer reproducibility.
These results are based on less ambiguous measurements.
Accuracy of measurements, as displayed through the ability to recreate ground truth
measurements, is another important requirement that measurement methods in clinical settings
should satisfy. Using an alpha value of 0.05, the only cases in which performed measurements
are not statistically different from ground truth measurements occur under use of the 3D
measurement method (Table 3). If a lower alpha value is hypothetically allowable, an even
larger number of 3D measurements demonstrate accuracy, while the number of measurements
displaying 1D and 2D accuracy remain rather low. Based on these results, 3D measurements
display the greatest potential in terms of accurately defining true tumour size. It is quite likely
that 1D and 2D measurements display poor accuracy due to loss of the longest dimensions in
alternate planes from the cross-sections observed. Furthermore, it is interesting to note that
although only some measurements display accuracy, all phantom tumour measurements

15
demonstrate high reproducibility. This indicates that measurements may have been consistent,
but consistently wrong. 1D and 2D measurements likely consist of repeated measurements of
only the longest dimensions that are actually displayed in the cross-sectional images, as opposed
to the true longest dimensions. All tumour measurements may have additionally been affected
by interference of other structures. For instance, airways or blood vessels of similar attenuation
may blend with the tumours and become incorporated into the measurements, causing
misjudgement of true boundaries. Perhaps a more highly trained individual, such as a
radiologist, would better be able to distinguish between such features, and potentially
demonstrate higher accuracy.
That fact that 3D measurements are shown to demonstrate adequate intra-observer
reproducibility and, additionally, display the greatest potential in terms of accurately recreating
ground truth measurements, leads to favouritism of this method. Aside from these factors, 3D
measurements logically have the potential to be favoured as only volume can incorporate all size
characteristics of a tumour, rendering it the truest measurement. The fact that the results
demonstrate accurate measurements of irregularly-shaped phantom tumours is promising, as
patient tumours tend to be of simpler geometries (2).
Tumour measurements have very important implications, as perceived changes in tumour
size can influence treatment plans and development of new therapies, thereby affecting lives.
With the apparent advantages of three-dimensional methods, the question may arise as to why
one-dimensional methods are in current use in clinical settings. One roadblock is overcome with
imaging advances relating to the third dimension. Through availability of thinner slice thickness
in X-ray CT, adequate spatial resolution for volume measurements can be displayed (3).
Another roadblock that is still present, however, is the issue of time-consumption (2). Manual
3D segmentations require much more time than simple linear measurements, which is an
obstacle that had been acknowledged for translation into clinical settings (2). If the advantages
of 3D measurements are stressed, perhaps increased time investment in measurements can be
deemed worthwhile. More realistically, however, mastered development of automated, yet
accurate techniques would be the best candidate for clinical use. This would additionally be
expected to further reduce both intra- and inter-observer variability (2). Regardless, three-
dimensional methods exhibit several advantages.

16
CONCLUSION
The main objectives of this project relate to reproducibility and accuracy of lung tumour
measurements, and the implications of these findings. 1D, 2D, 3D measurements all display
high intra-observer reproducibility for use in clinical settings. 3D measurements, however,
display the greatest potential in accurate reproduction of ground truth measurements. These
findings, coupled with the fact that a measurement of volume best represents true tumour
geometry, prove to be very advantageous. Once the drawback of time-consumption is overcome
for reliable, accurate three-dimensional lung tumour measurements, it is hopeful that transition
into clinical settings can be achieved.
REFERENCES
1. The future of cancer control in Canada. (2011). Canadian Partnership Against Cancer.
2. Wilson, L.C.R. (2010). Development of multi-dimensional x-ray computed tomography
measurements of lung tumours (Master’s thesis).
3. Zhao, B., Schwartz, L.H., Moskowitz, C.S., Ginsberg, M.S., Rizvi, N.A., & Kris, M.G.
(2006). Lung cancer: computerized quantification of tumor response. Radiology, 241(3),
892-898.
4. Yankelevitz, D.F., Reeves, A.P., Kostis, W.J., Zhao, B., & Henschke, C.I. (2000). Small
pulmonary nodules: volumetrically determined growth rates based on CT evaluation.
Radiology, 217(1), 251-256.
5. Lu, L., & Shara, N. (2007). Reliability analysis: calculate and compare intra-class
correlation coefficients (ICC) in SAS. Statistics and Data Analysis, 1-4.
6. Nichols, D.P. (1998). Spss library: choosing an intraclass correlation coefficient. UCLA
Academic Technology Services, (67).
7. Portney LG, Watkins MP. Foundations of clinical research: applications to practice.
Norwalk, CT: Appleton & Lange 1993; 505-528.
8. Prionas, N.D., Ray, S., & Boone, J.M. (2010). Volume assessment accuracy in computed
tomography: a phantom study. Journal of Applied Clinical Medical Physics, 11(2), 168-
180.

17
APPENDIX
Table A. Patient Tumour Data. Raw measurement data for large and small tumours are displayed with
corresponding means, standards deviations, and coefficients of variation. Patient Tumour (Large) Patient Tumour (Small)
Time
point Round
RECIS
T (cm)
Perpen
dicular
Axis
(cm)
WHO
(cm^2)
Volume
(cm^3)
Time
point Round
RECIS
T (cm)
Perpen
dicular
axis
(cm)
WHO
(cm^2)
Volume
(cm^3)
1 1 5.3 3.4 18.0 99.6 1 1 2.4 2.0 4.8 27.2
2 5.0 3.2 16.0 120.5 2 2.4 2.1 5.0 20.3
3 4.5 3.3 14.9 116.7 3 2.4 2.2 5.3 26.0
4 4.6 3.1 14.3 136.9 4 2.4 2.2 5.3 21.9
5 4.8 3.4 16.3 120.6 5 2.4 2.1 5.0 22.7
Mean 4.8 3.3 15.9 118.9 Mean 2.4 2.1 5.1 23.6
SD 0.3 0.1 1.5 13.3 SD 0.0 0.1 0.2 2.9
CV 0.1 0.0 0.1 0.1 CV 0.0 0.0 0.0 0.1
2 1 5.5 3.4 18.7 125.7 2 1 2.4 2.1 5.0 25.0
2 4.7 4.0 18.8 48.3 2 2.5 2.0 5.0 3.5
3 4.5 4.2 18.9 127.0 3 2.5 2.0 5.0 22.8
4 4.5 4.0 18.0 163.8 4 2.5 2.1 5.3 21.8
5 4.6 4.0 18.4 132.7 5 2.5 2.1 5.3 20.3
Mean 4.8 3.9 18.6 119.5 Mean 2.5 2.1 5.1 18.7
SD 0.4 0.3 0.4 42.7 SD 0.0 0.1 0.1 8.7
CV 0.1 0.1 0.0 0.4 CV 0.0 0.0 0.0 0.5
3 1 3.8 3.4 12.9 26.6 3 1 2.1 1.7 3.6 6.9
2 4.1 3.1 12.7 26.0 2 2.1 1.8 3.8 6.4
3 3.8 3.2 12.2 29.4 3 2.0 1.7 3.4 6.1
4 4.5 3.0 13.5 29.9 4 2.0 1.7 3.4 5.7
5 3.7 3.4 12.6 27.1 5 2.1 1.8 3.8 5.8
Mean 4.0 3.2 12.8 27.8 Mean 2.1 1.7 3.6 6.2
SD 0.3 0.2 0.5 1.7 SD 0.1 0.1 0.2 0.5
CV 0.1 0.1 0.0 0.1 CV 0.0 0.0 0.1 0.1
4 1 4.3 3.0 12.9 65.8 4 1 1.9 1.6 3.0 14.6
2 4.0 2.6 10.4 70.7 2 1.9 1.4 2.7 12.9
3 4.0 2.7 10.8 77.7 3 1.8 1.6 2.9 15.2
4 3.9 2.8 10.9 68.2 4 1.8 1.6 2.9 14.7
5 4.0 2.8 11.2 75.9 5 1.9 1.6 3.0 14.1
Mean 4.0 2.8 11.2 71.6 Mean 1.9 1.6 2.9 14.3
SD 0.2 0.1 1.0 5.0 SD 0.1 0.1 0.2 0.9
CV 0.0 0.1 0.1 0.1 CV 0.0 0.1 0.1 0.1
5 1 3.7 2.1 7.8 11.4 5 1 1.7 1.4 2.4 3.3
2 3.1 2.3 7.1 29.6 2 1.6 1.3 2.1 3.3
3 3.1 2.3 7.1 20.9 3 1.6 1.4 2.2 3.0
4 3.5 2.2 7.7 17.1 4 1.6 1.4 2.2 3.0
5 3.6 2.3 8.3 17.0 5 1.6 1.4 2.2 2.9
Mean 3.4 2.2 7.6 19.2 Mean 1.6 1.4 2.2 3.1
SD 0.3 0.1 0.5 6.7 SD 0.0 0.0 0.1 0.2
CV 0.1 0.0 0.1 0.4 CV 0.0 0.0 0.0 0.1

18
Table A. Patient Tumour Data (Cont.)
Patient Tumour (Large) Patient Tumour (Small)
Time
point Round
RECIS
T (cm)
Perpen
dicular
Axis
(cm)
WHO
(cm^2)
Volume
(cm^3)
Time
point Round
RECIS
T (cm)
Perpen
dicular
axis
(cm)
WHO
(cm^2)
Volume
(cm^3)
6 1 3.3 2.2 7.3 8.8 6 1 1.6 1.1 1.8 2.5
2 3.0 2.2 6.6 16.7 2 1.6 1.3 2.1 2.7
3 2.7 1.7 4.6 12.4 3 1.6 1.0 1.6 2.2
4 3.2 1.9 6.1 10.7 4 1.5 1.3 2.0 2.1
5 3.0 2.1 6.3 9.3 5 1.5 1.3 2.0 2.3
Mean 3.0 2.0 6.2 11.6 Mean 1.6 1.2 1.9 2.4
SD 0.2 0.2 1.0 3.2 SD 0.1 0.1 0.2 0.3
CV 0.1 0.1 0.2 0.3 CV 0.0 0.1 0.1 0.1
7 1 3.5 2.0 7.0 11.6 7 1 1.4 1.2 1.7 2.3
2 3.2 1.8 5.8 5.6 2 1.4 1.2 1.7 2.0
3 2.9 1.8 5.2 3.4 3 1.4 1.2 1.7 2.1
4 3.0 1.9 5.7 12.3 4 1.4 1.2 1.7 1.6
5 3.3 2.0 6.6 12.6 5 1.4 1.2 1.7 2.0
Mean 3.2 1.9 6.1 9.1 Mean 1.4 1.2 1.7 2.0
SD 0.2 0.1 0.7 4.3 SD 0.0 0.0 0.0 0.3
CV 0.1 0.1 0.1 0.5 CV 0.0 0.0 0.0 0.1
8 1 2.8 2.0 5.6 28.4 8 1 1.4 1.1 1.5 7.2
2 2.5 2.3 5.8 55.7 2 1.4 1.1 1.5 7.4
3 2.4 1.8 4.3 41.8 3 1.3 1.1 1.4 7.1
4 2.5 1.9 4.8 45.8 4 1.3 1.1 1.4 5.4
5 2.6 2.1 5.5 37.5 5 1.4 1.2 1.7 5.4
Mean 2.6 2.0 5.2 41.8 Mean 1.4 1.1 1.5 6.5
SD 0.2 0.2 0.6 10.1 SD 0.1 0.0 0.1 1.0
CV 0.1 0.1 0.1 0.2 CV 0.0 0.0 0.1 0.2
9 1 2.8 2.2 6.2 3.8 9 1 1.4 1.1 1.5 2.2
2 2.6 1.8 4.7 8.8 2 1.5 1.1 1.7 2.0
3 2.8 2.3 6.4 6.4 3 1.4 1.1 1.5 2.1
4 2.5 1.9 4.8 8.4 4 1.3 1.1 1.4 1.7
5 2.7 2.3 6.2 7.4 5 1.4 1.1 1.5 1.9
Mean 2.7 2.1 5.6 7.0 Mean 1.4 1.1 1.5 2.0
SD 0.1 0.2 0.9 2.0 SD 0.1 0.0 0.1 0.2
CV 0.0 0.1 0.2 0.3 CV 0.1 0.0 0.1 0.1

19
Table B. Phantom Tumour Data. Raw measurement data for large, medium and small tumours are displayed
with corresponding means, standards deviations, and coefficients of variation.
Slice Thickness = 0.5 mm Slice Thickness = 1.0 mm
Phanto
m Round
RECIS
T (cm)
Perpen
dicular
axis
(cm)
WHO
(cm^2)
Volume
(cm^3)
Phanto
m Round
RECIS
T (cm)
Perpen
dicular
axis
(cm)
WHO
(cm^2)
Volume
(cm^3)
1 1 4.2 2.8 11.8 15.3 1 1 4.2 3.1 13.0 14.5
(large) 2 4.1 2.9 11.9 14.6 (large) 2 4.1 2.9 11.9 16.6
3 4.3 3.1 13.3 16.4 3 4.3 3.1 13.3 17.5
4 4.2 3.0 12.6 15.6 4 4.2 3.1 13.0 16.8
5 4.2 2.9 12.2 15.4 5 4.3 3.1 13.3 15.4
Mean 4.2 2.9 12.4 15.5 Mean 4.2 3.1 12.9 16.2
SD 0.1 0.1 0.6 0.6
SD 0.1 0.1 0.6 1.2
CV 0.0 0.0 0.1 0.0
CV 0.0 0.0 0.0 0.1
2 1 2.6 1.7 4.4 2.8 2 1 2.6 1.7 4.4 3.4
(mediu
m) 2 2.6 1.7 4.4 3.1 (mediu
m) 2 2.5 1.6 4.0 3.2
3 2.6 1.6 4.2 3.7 3 2.6 1.7 4.4 3.6
4 2.5 1.7 4.3 2.9 4 2.6 1.7 4.4 3.3
5 2.6 1.8 4.7 3.3 5 2.7 1.8 4.9 3.0
Mean 2.6 1.7 4.4 3.1 Mean 2.6 1.7 4.4 3.3
SD 0.0 0.1 0.2 0.4 SD 0.1 0.1 0.3 0.2
CV 0.0 0.0 0.0 0.1 CV 0.0 0.0 0.1 0.1
3 1 2.0 1.2 2.4 0.9 3 1 1.9 1.4 2.7 1.8
(small) 2 1.8 1.4 2.5 1.6 (small) 2 1.9 1.2 2.3 1.9
3 2.0 1.2 2.4 1.2 3 1.9 1.5 2.9 1.9
4 2.0 1.2 2.4 1.4 4 2.0 1.3 2.6 2.2
5 2.0 1.2 2.4 1.4 5 1.9 1.3 2.5 2.2
Mean 2.0 1.2 2.4 1.3 Mean 1.9 1.3 2.6 2.0
SD 0.1 0.1 0.1 0.3 SD 0.0 0.1 0.2 0.2
CV 0.0 0.1 0.0 0.2 CV 0.0 0.1 0.1 0.1

20
Table B. Phantom Tumour Data (Cont.)
Slice Thickness = 2.0 mm Slice Thickness = 5.0 mm
Phanto
m Round
RECIS
T (cm)
Perpen
dicular
axis
(cm)
WHO
(cm^2)
Volume
(cm^3)
Phanto
m Round
RECIS
T (cm)
Perpen
dicular
axis
(cm)
WHO
(cm^2)
Volume
(cm^3)
1 1 4.2 3.1 13.0 16.5 1 1 4.2 3.1 13.0 20.5
(large) 2 4.2 2.8 11.8 17.6 (large) 2 4.2 3.0 12.6 21.5
3 4.2 3.0 12.6 17.6 3 4.0 2.9 11.6 23.1
4 4.2 3.1 13.0 16.0 4 4.1 3.0 12.3 17.8
5 4.2 2.7 11.3 16.6 5 4.2 3.2 13.4 18.9
Mean 4.2 2.9 12.3 16.8 Mean 4.1 3.0 12.6 20.4
SD 0.0 0.2 0.8 0.7 SD 0.1 0.1 0.7 2.1
CV 0.0 0.1 0.1 0.0 CV 0.0 0.0 0.1 0.1
2 1 2.6 1.9 4.9 3.3 2 1 2.7 1.8 4.9 5.0
(mediu
m) 2 2.5 1.7 4.3 3.3 (mediu
m) 2 2.5 1.7 4.3 4.3
3 2.6 1.8 4.7 4.3 3 2.6 1.7 4.4 4.9
4 2.6 2.0 5.2 3.8 4 2.7 1.7 4.6 4.8
5 2.6 1.8 4.7 3.4 5 2.7 1.8 4.9 4.0
Mean 2.6 1.8 4.8 3.6 Mean 2.6 1.7 4.6 4.6
SD 0.0 0.1 0.4 0.4 SD 0.1 0.1 0.3 0.4
CV 0.0 0.1 0.1 0.1 CV 0.0 0.0 0.1 0.1
3 1 1.9 1.5 2.9 2.2 3 1 2.0 1.2 2.4 2.0
(small) 2 1.9 1.2 2.3 1.6 (small) 2 1.9 1.2 2.3 3.0
3 1.9 1.4 2.7 2.4 3 2.0 1.2 2.4 2.4
4 1.9 1.3 2.5 1.7 4 1.9 1.2 2.3 2.4
5 1.9 1.3 2.5 2.6 5 2.0 1.2 2.4 2.6
Mean 1.9 1.3 2.5 2.1 Mean 2.0 1.2 2.4 2.5
SD 0.0 0.1 0.2 0.4 SD 0.1 0.0 0.1 0.4
CV 0.0 0.1 0.1 0.2 CV 0.0 0.0 0.0 0.1