Transcript of Hossein Moravej Epidemiology The prevalence of congenital hypothyroidism is 1/4,000 infants...
Slide 1
Slide 2
Hossein Moravej
Slide 3
Slide 4
Epidemiology The prevalence of congenital hypothyroidism is
1/4,000 infants worldwide. Twice as many girls as boys are
affected.
Slide 5
Etiology Thyroid dysgenesis (aplasia, hypoplasia, or an ectopic
gland) is the most common cause of congenital hypothyroidism,
accounting for 85% of cases; Inborn error of thyroxine synthesis
(10%) Transplacental maternal thyrotropin-receptor blocking
antibody (5%).
Slide 6
Thyroid dysgenesis of cases of thyroid dysgenesis are aplasia,
however, In the other of infants, rudiments of thyroid tissue are
found in an ectopic location(hypoplasia).
Slide 7
Thyroid dysgenesis Most cases of hypoplasia are detected by
newborn screening, but in some children ectopic thyroid tissue
(lingual, sublingual, subhyoid) may provide adequate amounts of
thyroid hormone for many years, or it may eventually fail in early
childhood.
Slide 8
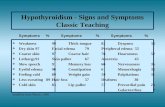
Defective Synthesis of Thyroxine (Dyshormonogenesis) Goiter is
almost always present. When the defect is incomplete, compensation
occurs, and onset of hypothyroidism may be delayed for years.
Slide 9
Dyshormonogenesis Defect of Iodide Transport Thyroid peroxidase
defects of organification and coupling: After iodide is trapped by
the thyroid, it is rapidly oxidized to reactive iodine, which is
then incorporated into tyrosine units on thyroglobulin. This
process requires generation of H 2 O 2, thyroid peroxidase, and
hematin
Slide 10
Dyshormonogenesis Defects of Thyroglobulin Synthesis Defects in
Deiodination: Monoiodotyrosine and diiodotyrosine released from
thyroglobulin are normally deiodinated within the thyroid or in
peripheral tissues by a deiodinase
Slide 11
Defects in Thyroid Hormone Transport: Passage of thyroid
hormone into the cell is facilitated by plasma membrane
transporters
Slide 12
Maternal thyrotropin receptor-blocking antibody An unusual
cause of transitory congenital hypothyroidism. Transplacental
passage of maternal TRBAb inhibits binding of TSH to its receptor
in the neonate. It should be suspected whenever : history of
maternal autoimmune thyroid disease, including Hashimoto
thyroiditis or Graves disease, maternal hypothyroidism on
replacement therapy, or recurrent congenital hypothyroidism of a
transient nature in subsequent siblings.
Slide 13
Maternal thyrotropin receptor-blocking antibody The half-life
of the antibody is 21 days, and remission of the hypothyroidism
occurs in about 3-6 mo
Slide 14
Radioiodine administration Hypothyroidism can occur as a result
of inadvertent administration of radioiodine during pregnancy for
treatment of Graves disease or cancer of the thyroid.
Slide 15
Thyrotropin and Thyrotropin-Releasing Hormone Deficiency
Deficiency of TSH can occur in developmental defects of the
pituitary or hypothalamus. More often, the deficiency of TSH is
secondary to a deficiency of TRH.
Slide 16
Slide 17
Most infants with congenital hypothyroidism are asymptomatic at
birth, even if there is complete agenesis of the thyroid gland. It
is due to the transplacental passage of moderate amounts of
maternal T 4, which provides fetal levels that are approximately
33% of normal at birth.
Slide 18
The clinician depends on neonatal screening tests for the
diagnosis of congenital hypothyroidism. Laboratory errors occur,
and awareness of early symptoms and signs must be maintained.
Slide 19
Birthweight and length are normal, but head size may be
slightly increased because of myxedema of the brain. Prolongation
of physiologic jaundice, may be the earliest sign. Feeding
difficulties, especially sluggishness, somnolence, and choking
spells during nursing, are often present during the 1st mo of life.
Respiratory difficulties, due in part to the large tongue, include
apneic episodes, noisy respirations, and nasal obstruction.
Slide 20
Cry little, sleep much, have poor appetites, and are generally
sluggish. constipation that does not usually respond to treatment.
Umbilical hernia Hypothermia