Hospital utilization and reimbursement method in Brazil
13
INTERNATIONAL JOURNAL OF HEALTH PLANNING AND MANAGEMENT, VOL. 4, 3-15 (1989) HOSPITAL UTILIZATION AND REIMBURSEMENT METHOD IN BRAZIL JOSE RODRIGUES Department of Business Administration, Federal University, Paraiba, Brazil SUMMARY Urban private hospital discharges in Brazil increased enormously during the last decade. Several measures were taken in an effort to slow the rate of increase in hospital admissions and the escalation of hospital costs, which were out of control by the end of the last decade. The introduction of a new case-based reimbursement method, late in 1983, not only contributed to increased hospitalizations, but to changed hospital case mix, as private hospitals shifted from more costly to less costly patients. This occurred especially in the most developed areas of the country, where the concentration of profit-making hospitals is very high. The case-based prospective payment method can be seen as a good managerial tool for use in comparing hospital performance. However, it seems not to be a good mechanism for controlling health care expenditures, especially when profit-making hospitals dominate the provision of hospital care. Any decrease in hospitalization by private hospitals in Brazil has been caused by the severe economic recession, which hit the Brazilian economy hard, and by the shift in hospital admissions from private to public hospitals, not by the introduction of the new reimbursement method which has changed the unit of payment from ‘patient day’ to case or procedure. KEY WORDS: Hospital utilization; Brazil; Reimbursement method; Case mix; Cost INTRODUCTION Because hospital services account for the major share of health care spending, utilization of acute hospital care has been the subject of considerable research for a long time, at least in developed countries, Increased utilization of medical care may sometimes be the result of an increase in government financing of medical services to the population rather than a response to change in the population’s health status. In the case of Brazil where expenditures in the hospital sector have increased enormously, not much research has been done to identify the factors that have contributed to increased use of hospital services. Increases in hospital costs and variations in hospital utilization have prompted a search for explanation. The number of hospital discharges and the rate of discharges from urban hospitals in Brazil have traditionally been on the rise. In 1971, 2.9 million inpatients were discharged from hospitals which provide hospital care for the urban population under the national social security scheme; in 1981 there 0749-6753/89/0 1OOO3-13$06.50 @ 1989 by John Wiley & Sons, Ltd.
-
Upload
jose-rodrigues -
Category
Documents
-
view
213 -
download
0
Transcript of Hospital utilization and reimbursement method in Brazil

INTERNATIONAL JOURNAL OF HEALTH PLANNING AND MANAGEMENT, VOL. 4, 3-15 (1989)
HOSPITAL UTILIZATION AND REIMBURSEMENT METHOD IN BRAZIL
JOSE RODRIGUES Department of Business Administration, Federal University, Paraiba, Brazil
SUMMARY Urban private hospital discharges in Brazil increased enormously during the last decade. Several measures were taken in an effort to slow the rate of increase in hospital admissions and the escalation of hospital costs, which were out of control by the end of the last decade. The introduction of a new case-based reimbursement method, late in 1983, not only contributed to increased hospitalizations, but to changed hospital case mix, as private hospitals shifted from more costly to less costly patients. This occurred especially in the most developed areas of the country, where the concentration of profit-making hospitals is very high. The case-based prospective payment method can be seen as a good managerial tool for use in comparing hospital performance. However, it seems not to be a good mechanism for controlling health care expenditures, especially when profit-making hospitals dominate the provision of hospital care. Any decrease in hospitalization by private hospitals in Brazil has been caused by the severe economic recession, which hit the Brazilian economy hard, and by the shift in hospital admissions from private to public hospitals, not by the introduction of the new reimbursement method which has changed the unit of payment from ‘patient day’ to case or procedure.
KEY WORDS: Hospital utilization; Brazil; Reimbursement method; Case mix; Cost
INTRODUCTION
Because hospital services account for the major share of health care spending, utilization of acute hospital care has been the subject of considerable research for a long time, at least in developed countries, Increased utilization of medical care may sometimes be the result of an increase in government financing of medical services to the population rather than a response to change in the population’s health status.
In the case of Brazil where expenditures in the hospital sector have increased enormously, not much research has been done to identify the factors that have contributed to increased use of hospital services. Increases in hospital costs and variations in hospital utilization have prompted a search for explanation.
The number of hospital discharges and the rate of discharges from urban hospitals in Brazil have traditionally been on the rise. In 1971, 2.9 million inpatients were discharged from hospitals which provide hospital care for the urban population under the national social security scheme; in 1981 there
0749-675 3/89/0 1OOO3-13$06.50 @ 1989 by John Wiley & Sons, Ltd.

4 JOSE RODRIGUES
were 10.8 million inpatients. This increase in a ten year period was quite significant, considering that the United States took more than 30 years to double its number of patients admitted in hospitals (Abernethy and Pearson, 1979). The urban population growth in Brazil was only about 50 percent during this period (1971-1981).
Several measures have been taken in Brazil in an effort to slow the rate of increase in hospital admissions and the escalation of hospital costs which were out of control by the end of the last decade. The introduction of a new case- based prospective payment late in 1983 was one of the measures in this direction. However, no study has been done to show the effect of this new method of payment on utilization.
In the United States, Diagnosis Related Groups (DRGs) have been widely used as the base for a prospective payment system by grouping cases into categories that seem to consume equivalent amount of resources. Hospital- ization rates in the United States started going down since 1983. However the relationship between the shift in payment and the decline in hospital utilization is unclear (Smith and Pickard, 1986). The overall effect on aggregate costs using any of these units of payment (case, day et aZ.) cannot be predicted, since these measures ‘motivate hospitals 1) to increase the quantity of that output; and 2) to contain the amenity level, quality level, intensity and scope of service provided per unit of output‘ (Dowling, 1974).
In a country where a large proportion of the population is still lacking basic needs, it is essential, first of all, to know how the hospital sector operates and, second, to identify areas where changes in practice will lead towards more effective utilization of allocated hospital services. It has been found that Roemer’s law which states that ‘hospital beds that are built tend to be used’ (Shain and Roemer, 1959) is working perfectly well for the Brazilian hospital sector, and the maldistribution of health care resources in the country is a matter of concern (Rodrigues, 1987). This paper documents the increase in hospitalization in Brazil during the last fifteen years and evaluates the impact of a new case-based prospective payment, introduced late in 1983, on hospital utilization.
THE BRAZILIAN HOSPITAL SYSTEM AND PAYMENT METHOD
The Brazilian Social Security Program, which is financed in large part by the working population through compulsory contributions, has contributed to the inception of the largest organization in the country, whose budget is the largest after the federal government. The Ministry of Social Insurance and Assistance, created in 1974, encompasses several entitites, including the National Social Insurance Institute for Medical Care (Instituto Nacional de Assistencia MCdica de Previdencia Social-INAMPS) . Today medical care under the Social Security Program covers almost the whole population and INAMPS, which is part of the Ministry of Social Insurance and Assistance, is the major financer of hospital care in the country.
With the expansion of insurance coverage since the late 1960s, the hospital

HOSPITAL UTILIZATION AND REIMBURSEMENT METHOD IN BRAZIL 5
industry in Brazil grew faster than the rest of the economy during the last decade. During that period, the number of private hospital beds, both profit and non-profit, increased by more than 40 percent, and the number of hospital beds increased to approximately 4 beds per 1,OOO population. However, the inequality in the distribution of these beds is quite significant. While there are some states with more than 6 beds per 1,OOO population, there are others with less than 2 beds per 1,OOO population.
In 1980, private hospital beds, both profit and non-profit, accounted for approximately 70 percent of the total number of beds. About 30 percent were owned by the federal, state and local governments. In view of this, approximately 80 percent of urban patients were treated in private hospitals, both profit and non-profit (contratados). A small proportion (about 2 percent) are treated in federal hospitals, which are administered by INAMPS itself, and the remaining number of patients were treated in state, university, and municipal hospitals. Most of these hospitals (conveniados) are reim- bursed differently than private hospitals and their beds are used by INAMPS and indigent patients.
The growth of profit-making hospitals, which account for the highest number of hospital beds in the country, was higher than non-profit hospitals in the last decade. Although some of the non-profit hospitals were church- sponsored, they no longer exercise the same charitable function because all patients treated by them are paid by INAMPS in the same way that payment is made to profit-making hospitals. All non-profit hospitals however still have a philanthropic denomination and are exempt from federal taxation.
The federal government contracts for more than 80 percent of all private hospital beds, through INAMPS to provide medical services for the population. Because the upper middle class is treated privately and pays for its treatment directly (even if entitled to free medical care under INAMPS), all private hospitals keep some beds for this privileged category of patients that does not want to follow bureaucratic procedures and does not want to be treated in beds located in common hospital wards. Therefore, private hospitals always keep a small proportion of highly comfortable beds for these patients carrying private insurance. Partly due to the predominance of the private interests, most of the country’s health care resources are allocated to the curative subsystem controlled by INAMPS, and an insignificant propor- tion is devoted to the preventive subsystem, controlled by the Ministry of Health.
Hospitals in Brazil have always been reimbursed on a prospective basis. For many years INAMPS used to reimburse hospitals on a per diem basis. In addition, another unit of payment was adopted for specific services such as laboratory and radiology procedures. The per diem reimbursement as used by INAMPS has not been based on determined costs, because hospital information in Brazil is very poor. As in many other countries, a deficiency in information available for rate-setting was causing risks to the providers, payers and patients. Nothing is known about how INAMPS used to determine its per diem reimbursement formula, but it was probably done in a

6 JOSE RODRIGUES
quite primitive way. As is well known, the use of the patient day as the unit of payment induces the hospital to increase the number of admissions and length of stay.
A dramatic change occurred in the method of hospital payment by the end of 1983, when INAMPS introduced the case-based prospective payment. Again, not much is known about how INAMPS arrived at its diagnostic or case classification. According to INAMPS, the case-based prospective payment was obtained by the average values of all cases or procedures from all patient bills all over the country.
It has been stated that for ‘the purpose of paying the hospital, the accuracy of a classification system is measured by its ability to classify a case with other cases which have similar costs for necessary care’ (Jencks et al., 1984). Although the ‘selection of an appropriate measure of case mix requires careful delineation of the steps in the measurement process’ (Hornbrook, 1982), the implementation of a case-based prospective pricing system seems to be a move in the right direction and in terms of hospital financing it represents a quite radical change.
The new method of payment was introduced in an effort to slow the rate of increase in hospital admissions and expenditures which were out of control by the end of the last decade. The escalation of hospital costs had in part contributed to the bankruptcy of the whole social security system in 1981. The federal government, against the will of the country’s population, increased individual contributions in order to solve the financial crisis of the system (at a time when INAMPS was always documenting fraud, abuse and poor quality of care given to the patients by some hospitals).
DATA AND METHOD
The primary source of hospital inpatient data in Brazil is the Instituto Nacional de AssistCncia MCdica da PravidCncia Social-INAMPS. Data on hospital admissions and discharges from patients under INAMPS scheme are published yearly. Urban hospital admissions are classified by the major specialties of general medicine, general surgery, obstetrics, psychiatric and tuberculosis treatment. No information is given about patient and hospital characteristics. The data are aggregated at the state level and have been published during the last 15 years. No classification exists for rural hospital admissions, and INAMPS has published just the total number of rural admissions at the state level.
The basic information, which is necessary for planning purposes, such as hospital occupancy, average length of stay, patient days, patient age and sex, and number of hospital beds, is not provided, despite the fact that INAMPS has (relatively) large computer facilities. For the purpose of this work, data on urban hospital discharges from all private hospitals, both profit and non- profit, contracted by INAMPS for the provision of hospital care for the urban population were assembled for the years of the present and last decade, based on INAMPS data publication (MPAS, 1977/1986).

HOSPITAL UTILIZATION AND REIMBURSEMENT METHOD IN BRAZIL 7
TRENDS IN HOSPITALIZATION RATE
Utilization is defined here by the number of patients discharged in the hospital. Due to lack of informstion, other important measures of hospital utilization such as length of stay and occupancy rate are not mentioned in the present work.
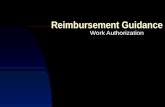
As is shown in Table 1, the rate of urban hospital discharges increased significantly in the country from 54 in 1971 to 126 discharges per 1,OOO population in 1981. It started dropping after 1982, but it is still over 100 discharges per 1,000 population (Figure 1). The highest increment in hospital admissions occurred between 1974 and 1975, with the creation of the Ministry of Social Security which passed legislation giving access to health services in
Table 1. Rates of urban patient discharges by regions in Brazil: 1971, 1974, 1975, 1980/1986
Rate of Discharges per 1,OOO popuation Region 1971 1974 1975 1980 1981 1982 1983 1984 1985 1986 Brazil 54 66 84 119 126 118 105 110 102 102 North 39 48 62 81 114 113 110 110 105 90 Northeast 35 44 55 80 93 91 79 91 95 96 Southeast 56 66 85 118 122 117 10.5 109 101 93 South 80 107 131 177 176 154 139 145 120 150 West Central 54 64 84 134 154 143 112 106 100 101
140
120
100
80 0
960 Q)
c 0 IY 40
20
0 71 72 73 74 75 76 77 78 79 80 81 82 83 84 85 86
Year
Figure 1. Urban patient discharge ratel1000 population, Brazil, 1971-1986

8 JOSE RODRIGUES
hospital to any person. It can also be seen in Table 1 and Figure 2 that there is a wide regional variation in hospital utilization in Brazil. For all the years presented, discharge rates in the South Region were highest, with 177 discharges per 1,OOO population in 1980. For most of the years discharge rates in the South Region, which is the richest in the country, were twice as high as the rate in the Northeast Region, which is the poorest Region in the country. Excluding the two poorest regions (North and Northeast) the rate of hospital discharges in the other regions is presently as high as the rate in developed countries (Groenewegen and Van Der Zee, 1988; Brewer and Freedman, 1982; Haupt, 1982; Pasley et al., 1987).
. . 71 72 73 74 75 76 77 78 79 80 81 82 83 84 85 86
Year ~ = North Rote/1000 N Eost R o t e A 0 0 0 Southeost Rote/ l000
South Rote/1000 0 W.Centrol Rote/1000
Figure 2. Urban patient discharge rate/1000 population, by regions in Brazil, 1971- 1986
Table 2 shows the number of urban private hospital discharges. In 1979, private hospitals accounted for 90 percent of the total of all urban hospital discharges. In 1986, this percentage dropped to 67. From 1971 to 1981, hospital discharges were increasing at a high rate, but in 1982 they dropped for the first time. All the factors that have influenced the decline in hospitalization since 1982 are not known. However, financial crisis that has affected the social security system since then must have been the most influential factor explaining the decrease of hospitalization. By delaying the payment of hospital patient bills monthly, INAMPS may have made it difficult for some hospitals to fill all of their beds. It was expected that the introduction of the new reimbursement method late in 1983 was to decreae hospitalization. Moreover, the dramatic increase of approximately 8 percent in hospital discharges in private hospitals between 1983 and 1984 may lead one to conclude that the new reimbursement method has contributed to an

HOSPITAL UTILIZATION AND REIMBURSEMENT METHOD IN BRAZIL 9
Table 2. Number of urban hospital discharges from short-stay private hospitals by regions in Brazil (1979-1986)
Year Region 1979 1980 1981 1982 1983 1984 1985 1986
Brazil 7645
North 172 Northeast 1194 Southeast 3937 South 1771 West Central 571
% of private hospital discharges 90
(In thousands) 8427 9202 8775 7778 8427 7596 7637
178 192 187 176 177 143 113 1244 1421 1337 1100 1259 1246 1184 4319 4692 4620 4211 4541 4127 3805 2036 2172 1915 1723 1890 1565 2012 651 724 716 568 560 514 523
88 85 84 80 80 71 67
increase, and not to a decrease in hospital admissions. Consequently, it seems that the case-based reimbursement method failed to control the increase of hospitalization.
It can be seen, however, that hospital discharges declined in 1985 and 1986 in relation to 1984. This drop was in part caused by a kind of admission control mechanism when INAMPS decided to establish a quota of the number of patients for each hospital. In addition to that, there was a significant shift in hospitalization from private to public hospitals since 1985. Private hospitals which were accountable for more than 80 percent of the total of hospital discharges over the years, in 1985 were accountable for just about 70 pecent. This may have been another important factor explaining the decline in private hospital discharges from 1985 onwards.
There have always been complaints that INAMPS used to discriminate against public hospitals, despite the federal recommendation that priority should be given first to public hospitals in terms of patient referrals. (It has in some quarters been assumed that there is a difference between recommend- ation and practice in INAMPS’ policy.)
Table 3 shows the distribution of private hospital discharges by the major specialties of general medicine, general surgery, and obstetric treatment. There have been changes over the years in patient discharges by specialty. In 1971, for instance, general medicine accounted for 43 percent of all hospital discharges; in 1986 it accounted for 62 percent. In the same period, the percentage of general surgery discharges in relation to the total number of discharges dropped from 24 to 15 percent. Obstetric care also dropped from 33 to 23 percent. As will be shown, the increase in the proportion of cases treated in general medicine and the decrease in the proportion of the other two specialties means a dramatic change in hospital behavior in relation to hospitalization and, consequently, a change in hospital case mix. Both the increase and the decrease in hospitalization have increased the percentage of cases treated in the spcialty of general medicine and decreased the percentages in the other two specialties.

10 JOSE RODRIGUES
Table 3. Percentage of urban Private Short-Stay Hospital discharges by major specialties in Brazil (1971-1986)
Percentage
Medicine Surgery Care Year General General Obstetric
1971 1972 1973 1974 1975 1976 1977 1978 1979 1980 1981 1982 1983 1984 1985 1986
43 45 48 48 52 53 52 54 54 57 58 58 58 61 60 62
24 23 22 21 21 22 20 19 19 19 18 17 17 17 17 15
33 32 30 31 27 25 28 27 27 24 24 25 25 22 23 23
If general surgery means treatment of more complicated cases, it is evident that by increasing the percentage of cases treated in the specialty of general medicine and by decreasing the percentage in the specialty of general surgery, hospitals are treating a higherproportion of less complex cases, even when the number of hospitalization inceases. The same is true if hospitalization decreases.
In order to observe the effect of the new reimbursement method on hospital utilization and hospital behavior, three periods of time should be considered for the analysis of Table 3. The first period is from 1971 to 1981, when the number of hospital discharges was increasing in Brazil. As hospital discharges increased in this period, the percentage of cases treated in the specialty of general medicine increased from 43 to 58 percent. On the other hand, the percentage of general surgery decreaed from 24 in 1971 to 18 percent in 1981. As hospitalizations increased in this period, hospitals were treating a higher proportion of less complicated cases. The second period of time to be considered is when hospital discharges started decreasing, but before the introduction of the new reimbursement method (1982-1983). It was observed that hospital discharges decreased in 1982 and in 1983, but no change has been registered in the percentage of patients treated in the major specialties in relation to 1981 (the year of the highest number of hospital discharges in Brazil) (Table 2). Finally, the period from 1984 to 1986 after the introduction of the new reimbursement method. The increase in hospital discharges in 1984 culminated in a significant change in the percentage of patients treated in general medicine; from 58 in 1983 to 61 percent in 1984. This has happened at the expense of a decrease in the percentage of obstetric

HOSPITAL UTILIZATION AND REIMBURSEMENT METHOD IN BRAZIL 11
care from 25 to 22 percent. By looking at Tables 2 and 3, it can be seen that the number of hospital discharges in 1984 was the same as in 1980, but hospital case mix was different in terms of the proportion of patients treated in each specialty.
The decrease in discharges in 1985 and 1986 in relation to 1984 contributed to increase further more the percentage of cases treated in general medicine and to decrease the percentage in general surgery. The data suggest that as hospitalization decreased after the introduction of the new reimbursement method, hospitals were changing case mix, by admitting a higher proportion of less complex cases and a lower proportion of more complicated cases. Consequently, the new reimbursement method not only contributed to increased hospitalization in the first year after its introduction, but also contributed to change hospital case mix in favour of less complicated cases.
The percentage of cases treated in the specialty of general medicine in private hospitals is high in Brazil. The concept of need in cases classified as general medicine is less definable operationally than in surgical services. In consequence, high admission rates in the specialty of general medicine, especially in for-profit hospitals, must be seen with suspicion. There are claims that a large percentage of all cases treated in the Brazilian hospitals could be treated on a primary care basis without requiring the services of specialized physicians.
It may be difficult to have comparable data on inpatient care between countries due to the differences in the classification of diagnostic. However, while surgical procedures in the United States have been on the rise and comprise more than 40 percent of total discharges (McCarthy and Finkel, 1980; AHA, 1986), it is observed that in Brazil surgical procedures have been going down to a low of 15 percent of the total number of discharges. This is not the case in the Brazilian public hospitals where the percentage of surgical procedures is above 40 percent of total discharges.
The decrease in the percentage of cases treated in obstetric care may not mean a decrease in utilization. The number of patients under obstetric treatment in private hospitals may have decreased, but length of stay may have increased taking into consideration that the Caesarian section rate has been increasing over the year. It has been claimed that Brazil has the highest Caesarian section rate in the world: financial incentives seem to be influencing this medical procedure (Rodrigues, 1988; Barros et al., 1986; Lins and Fortney, 1981).
Table 4 shows the variations in inpatient care from 1980 to 1986 across the three most populated regions in Brazil, which have accounted for approxi- mately 90 percent of all hospitalizations. It is interesting to observe that hospitalization in general medicine is-relative to other specialties-higher in the richest regions of the country like the South and Southeast. On the other hand, the percentage of surgical discharges in the South is lower than in the other two regions. It is known that the South region has the highest concentration of profit-making hospitals. Between 1983 and 1984, one year after the introduction of the case-based prospective payment, hospitalizations

12 JOSE RODRIGUES
Table 4. Percentage of urban Private Short-Stay Hospital discharges by regions and major specialties in Brazil (1980-1986)
Specialtyand Region 1980 1981 1982 1983 1984 1985 1986 Year
General Medicine Northeast Southeast South
General Surgery Northeast Southeast South
Obstetric Care Northeast Southeast South
55 54 62
18 20 17
27 26 21
55 56 52 55 55 58 55 57 57 60 6 0 6 0 63 61 62 66 65 67
18 16 18 19 20 19 19 17 17 18 17 16 16 16 15 13 13 11
27 28 30 26 24 23 26 26 26 22 23 24 21 23 23 21 22 22
in general medicine in the South jumped from 62, in 1983, to 66 percent in 1986.
DISCUSSION
The findings suggest the need for further analysis of the Brazilian hospital sector despite data limitations. In a country where private, profit-making hospitals dominate the provision of health services and most of the scarce resources are allocated to curative medical care, there is a need to explain whether the process of resource allocation is based on the needs of the population or on the pressure of health service providers. Although less than 2 percent of the Gross National Product-GNP-is spent on curative care by the federal government, the proportion spent in preventive medicine is insignificant compared to that figure. Increaed utilization of hospital services in Brazil, especially in more developed regions, may have had negligible impact on the population’s health status. It is important to investigate further the claim that most of the health needs of the Brazilian population are of a simple nature and can be treated out of hospital.
The escalation of hospital costs led the health authorities to take concrete measures in an attempt to curb hospital expenditures. One of these measures, the introduction of a case-based prospective payment, seems to have failed to stop hospital admissions. It is known that, when hospitals receive a preestablished amount for providing medical care based on a patient’s procedure or diagnosis, the incentives are to increase admissions, shift from more costly to less costly patients, and to manipulate data to maximize profitability (Dowling, 1974; Hellinger, 1985; Wennenberg et al., 1984). The results presented here show that there have been significant changes in

HOSPITAL UTILIZATION AND REIMBURSEMENT METHOD IN BRAZIL 13
private hospital case mix, based on the major medical specialties. The increase in the percentage of cases treated in the specialty of general medicine has increased substantially, while the percentages in the specialties of general surgery and obstetric care have decreased over the years. This has happened when hospitalizations were either increasing or decreasing.
The new method of payment not only contributed to increase hospitaliza- tions but to changed hospital case-mix, leading private hospitals to shift from more costly to less costly patients, especially in the most developed areas of the country where the concentration of profit-making hospitals is very high. The decrease in hospitalizations in private hospitals in 1985 was not caused by the new reimbursement method, but by the severe economic recession that hit the Brazilian economy hard and by the shift in hospital admissions from private to public hospitals (based on the reorientation of INAMPS policy to the use of existing and underutilized public health services facilities). It has been shown that public hospitals in Brazil always operated at a lower occupancy rate than private hospitals. To maintain private hospitals with higher occupancy rates at the expense of public hospitals is to discriminate against these institutions which represent the consumers’ investment out of taxation. Due to the high fixed cost of public hospitals, an unfilled bed represents a significant loss. When INAMPS keeps an empty bed in public hospitals and, at the same time, pays to fill a bed in private hospital, the Brazilian society is paying twice for a patient treatment-by paying to keep an empty bed while also paying for the use of another bed (Rodrigues, 1983).
The introduction of a case-based prospective payment can be seen as a good managerial tool that can be used to compare hospitals’ performance. However, it seems not to be a good mechanism to control health care expenditures, especially when profit-making hospitals dominate the provision of hospital care.
More research has to be developed in order to know how health care resources are allocated in the country and what factors have contributed to the present pattern of health care utilization. The answers to these questions are helpful in determining the amount of financial resources that should be spent in health care in the country.
The Brazilian health care system is going through another change. In 1987, the National Commission for Health Reform proposed a new health care system for the country. Despite the positive aspects of the proposed health reform, there seem to be some contradictory statements. The Commision seemed to expect that more than 10 percent of the Gross National Product - GNP-should be spent in the health care sector (CNRS, 1987). This exaggerated and unrealistic proposal has to be viewed with suspicion. It has been said already that those who advocate too much resources for health care ‘are either mistaken or have in mind objectives other than the improvement of the health of the population’ (Fuchs, 1979). By spending more than 10 percent of the GNP in health services, as it is proposed, Brazil will be moving to create one of the most sophisticated industrial health complexes in Latin America that may not have too much effect on the population’s health status.

14 JOSE RODRIGUES
Reform should seek to have a positive impact on the population’s health status, by changing the chaotic and inefficient structure of the present system which seems to have contributed to the accumulation of benefits in the hands of few at the expense of contributions from an exploited working population.
ACKNOWLEDGEMENTS
This study was carried out as a Post-Doctoral Fellow at the Johns Hopkins University, Department of Health Policy and Management. I would like to thank the Universidade Federal da Paraiba, Conselho Nacional de Desen- volvimento Cientifico e Tecnologico and the Johns Hopkins University for their financial help.
REFERENCES
Abernethy, D.S., Pearson, D.A., (1979). Regulating hospital costs: The development of public policy. Washington, D.C.: AUPHA Press. Ann Arbor p. 30.
American Hospital Association (1986). Hospital Statistics, 1985. Chicago. Barros, F.C., Vaughan, J.P., Victora, C.G. (1986). Why so many cesarean section?
The need for a further policy change in Brazil. Health Policy Planning 1, 19-29. Brewer, W.R., Freedman, M.A. (1982). Causes and Implications of Variation in
Hospital Utilization. J. Public Health Policy 3, 445-454. ComissPo Nacional da Reforma Sanitaria (CNRS) (1987). Documentos ZZ. Rio de
Janeiro. Dowling, W.L. (1974). Prospective reimbursement of hospitals. Inquiry, 11, 163-180. Fuchs, J. (1979). The economics of health in a post-industrial society. The Public
Interest 56, 3-20. Groenewegen, P.P., Van Der Zee (1988). The comparison of health care systems
through regional analysis: The case of hospital admissions in Belgium and the Netherlands. SOC. Sci. Med. 26, 91-100.
Haupt, B.J. (1982). Utilization of short-stay hospitals: An annual summary for the United States, 1980. In Vital and Health Statistics. Washington D.C., HHS, National Center for Health Statistics, Series 13, No. 64.
Hellinger, F.J. (1985). Recent evidence on case-based systems for setting hospital rates Inquiry, 22, 78-91.
Hornbrook, M.C. (1982). Hospital case mix: Its definition, measurement and use: Part 11. Review of alternative measures. Medical Care Review 30, 73-123.
Jencks, S.F., Dabson, A., Willis, P., Feinstein, P.H. (1984). Evaluating and improving the measurement of hospital case mix. Health Care Financing Review (Annual Supplement): 1-1 1.
Lins, F.E., Fortney, J.A. (1981). Caesarian section in four Rio de Janeiro hospitals. Int J Gynaecol Obstet 19, 27-31.
McCarthy, E.G., Finkel, M.L. (1980). Surgical Utilization in the U.S.A. Medical Care 18, 883-891.
MinistCrio da Previdencia e Assistencia Social (MPAS) (1977). INPS. Mensdrio Estahktico 1977, Nos 2981300. Rio de Janeiro.
Ministbrio da PrevidCncia e Assistencia Social (MPAS) (1979). Instituto National de AssistCncia Medics da PrevidCncia Social. ZNAMPS EM DADOS (N6mero EspeciaY78). Rio de Janeiro.

HOSPITAL UTILIZATION AND REIMBURSEMENT METHOD IN BRAZIL 15
MinistCrio da Previdsncia e AssistCncia Social (MPAS) (198G1986). (Instituto Nacional de AssitCncia Medica da PrevidCncia Social. ZNAMPS EM DADOS (No 2, 1979. Rio de Janeiro; No 3, 1980. Rio de Janeiro; No 4, 1981. Rio de Janeiro; No 5,1982. Rio de Janeiro; No 6,1983. Rio de Janeiro; No 7,1984. Rio de Janeiro; No 8, 1985. Rio de Janeiro; No. 9, 1986. Rio de Janeiro.
Pasley, B., Vernon, P., Gibson, G., McCauley, M., Andoh, J. (1987). Geographic variations in elderly hospital and surgical discharge rates, New York State. A m J Public Health 77, 679-684.
Rodrigues, J. (1987). A distribuieo dos recurws de saude no Brasil-A administraeo da desigualdade. Revista de Administrapio de Emprtsas 27, 52-57.
Rodrigues, J. (1983). 0 INAMPS e a ‘eficisncia’ dos hospitais privados lucrativos. Revista de Administrapio 18, 93-97.
Rodrigues, J. (1988). Urban Hospital Caesarian Section Delivery Rates in Paraiba State, Brazil, 1977-1981. A m J Public Health 78 (6), 704-705.
Shain, M., Roemer, M.I. (1959). Hospital Costs relate to the supply of beds. The Modern Hospital 92(4), 71.
Smith, D.B., Pickard, R. (1986). Evaluation of the impact of Medicare and Medicaid Prospective Payment on utilization of Philadelphia area hospitals. Health Service Research, 21, 529-546.
Wennenberg, J.E., McPherson, K., Caper, P. (1984). Will payment based on diagnosis-related groups control hospital costs? N Eng J Med 311, 295-300.