Maximizing Utilization of PAs & NPs: Rules, Realities, and ... · 1 Maximizing Utilization of PAs &...
29
Maximizing Utilization of PAs & NPs: Rules, Realities, and Reimbursement Session Code: TU15 Date: Tuesday, September 20, 2016 Time: 2:30pm - 4:00pm Total CE Credits: 1.5 Presenter(s): Tricia Marriott, PA-C, MPAS, MJ Health Law, CHC
-
Upload
truongtram -
Category
Documents
-
view
216 -
download
0
Transcript of Maximizing Utilization of PAs & NPs: Rules, Realities, and ... · 1 Maximizing Utilization of PAs &...
Maximizing Utilization of PAs & NPs: Rules,
Realities, and Reimbursement
Session Code: TU15
Date: Tuesday, September 20, 2016
Time: 2:30pm - 4:00pm
Total CE Credits: 1.5
Presenter(s): Tricia Marriott, PA-C, MPAS, MJ Health Law,
CHC
1
Maximizing Utilization of PAs & NPs
Rules, Realities, and Reimbursement
NAMSS 2016 Boston/TU15
Speaker
Tricia Marriott, PA-C, MPAS, MJ Health Law, CHC®
Senior Director, Regulatory & Professional Advocacy; Principal Advisor, AAPA Center for Healthcare Leadership &Management; Staff Liaison to the Joint Commission
American Academy of PAs (AAPA)
www.chlm.org
Disclosure
Tricia Marriott is an employee of the AAPA. She has no other financial or industry disclosures to report.
She is also currently licensed in the State of Connecticut, NCCPA certified, and is employed part-time by the Yale Medical Group in the Department of Orthopaedics.
2
Disclaimer
This presentation is provided for informational purposes only and does not constitute legal or payment advice.
• The ultimate responsibility for statutory and regulatory compliance, as well as the proper submission of claims, rests entirely upon the provider of services.
• Medicare policy changes frequently, so be sure to keep current by going to www.cms.gov and to your Medicare Administrative Contractor’s website.
• The American Medical Association has copyright and trademark protection of CPT ®.
Myths & Misunderstandings
5
APNs and PAs like being called ‘mid-levels’ or ‘physician extenders’
NPs and PAs are ‘mid-levels’, ‘physician extenders’,
or “allied health”…
NPs and PAs are
NPs and PAs1
6
3
APNs and PAs cannot see new patients
NPs and PAs cannot see new Medicare patients
NPs and PAs CAN see new Medicare patients. 2
[When they do, the claim must be submitted under their own NPI, resulting in reimbursement at 85%.]
7
Physicians must see every patientand/or be on site.
§190 Physician Assistant(PA) Services
“The physician supervisor (or physician designee) need not be physically present with the PA when a service is being furnished to a patient and may be contacted by telephone, if necessary, unless State law or regulations require otherwise.”
There is no Medicare rule that requires a physician to see every patient. 3
§200 Nurse Practitioner (NP) Services
“The collaborating physician does not need to be present with the NP when the services are furnished or to make an independent evaluation of each patient who is seen by the NP.”
8
We lose money on APN/PA services because
Medicare only reimburses 85%
The practice loses money on services provided by an NP/PA because
Medicare only reimburses 85%.
Many organizations recoup NP/PA expenses and generate positive margin when PAs and NPs are utilized appropriately.
9
4
Myths
• PAs/NPs cannot see new patients• Physician must be present in the office or clinic
when a PA/NP sees patients.• Physician must see every patient.• A physician co-signature on a note means the claim
may be submitted under the physician.• Reimbursement for services provided by PAs/NPs
“leaves 15% on the table”.• Commercial payers won’t pay.• Patients won’t be happy: What about the “brand”?
10
Read all of the results at advisory.com/mplc/pcsurvey 4
FOUNDATIONAL PILLARS
12
5
Foundation
PAs and NPs are not clinical support staff.
PAs and NPs provide professional services at a medical level of care that a physician would otherwise have to provide.
13
PA/NP ServicesDefined by Medicare:
“They are the type that are considered
physician’s services if furnished by a doctor
of medicine or osteopathy (MD/DO).”5
PAs/NPs as Providers
What are the business implications?
What are the regulatory and compliance issues?
What are the cultural implications?
Situational analysis:
�What are we doing now?
�What needs to happen?
�How do we get it done?
15
6
Interdependent Concepts
Regulatory Compliance and Scope of Practice
Credentialing & Privileging
Maximizing PA/NP Utilization
Reimbursement & Billing Policy
CULTURE
16
RECOGNIZED BY MEDICARE
PART B SINCE 1998
PAS & NPS
17
Balanced Budget Act of 1997
• Removed the restriction on settings and services furnished by PAs/NPs: payments allowed for services furnished by PAs/NPs in all settings.
• Effective for services furnished on or after January 1, 1998
• Prior to 1998, very little opportunity to bill for PAs/NPs other than via “incident-to” provision, and reimbursement rate in rural/healthcare provider shortage areas was 65%.
• Payment … 85 percent of the physician fee schedule.
18
7
PAs/NPs are no longerclinical support staff:
No longer included in Medicare Part A Cost Report 6
42CFR Subpart B—Inpatient Hospital Services and InpatientCritical Access Hospital Services§ 409.10 Included services.
(b) Inpatient hospital services does not include the following types of services:
(4) Physician assistant services, as defined in section 1861(s)(2)(K)(i) of the Act.
(5) Nurse practitioner and clinical nurse specialist services, as defined in section 1861(s)(2)(K)(ii) of the Act.
19
Medicare Benefit Policy Manual
§190: Physician Assistant Services7
****************************************************
20
PA/NP recognized by Medicare
• PAs and NPs are recognized as enrolled “non-physician providers”, “ordering/referring” providers, and “eligible providers” in the Medicare program.
• Must be enrolled in Medicare (PECOS) if ordering, referring and/or billing. 8 (Rule in effect since January 1, 2014)
• Reimbursement for services provided by PAs and NPs are reimbursed at 85% of the physician fee schedule.
• There are provisions for 100%, such as the “Incident-to” provision in the office & Shared/Split Visits in the hospital setting; specific rules apply.
21
8
PAs/NPs can bill all levels of E/M: Medicare
“PAs may furnish services billed under all levels of CPT evaluation and management codes, and diagnostic tests if furnished under the general supervision of a physician.” 9
“NPs may furnish services billed under all levels of evaluation and management codes and diagnostic tests if furnished in collaboration with a physician.” 10
22
CPT® Code Utilization
“A “physician or other qualified health care professional” is an individual who is qualified by education, training, licensure/regulation (when applicable), and facility privileging(when applicable)who performs a professional service within his/her scope of practice and independently reports that professional service.”
“Throughout the CPT code set the use of terms such as “physician”, ‘qualified health care professional”, or “individual” is not intended to indicate that other entities may not report the service.”
CPT ® 2016, Professional Edition, p. xii
23
PAs and NPs: One DifferenceDirect Billing/Payment
PAs
Medicare does allow PAs to submit claims under their own NPI.
Medicare does not allow PAs to direct bill/receive direct payment; while the claim is submitted under the PA’s NPI, the payment field is to the PA’s employer. 11, 12
NPs
Nurse practitioners may direct bill under their NPI and receivedirect payment from Medicare.13
• Nurse practitioners may reassign their payment to their employer.
• Most NPs reassign payment as a condition of their
employment.
24

9
COLLABORATION/ SUPERVISION
25
Supervision/Collaboration:Medicare
Medicare policy for supervision/collaboration essentially same for PAs14 and NPs15;
– Access to reliable electronic communication
– Personal presence of the physician is generally not required
– Medicare policies will not override state law guidelines or facility policies
26
NP Collaboration: Medicare
Medicare Benefit Policy Manual: Chapter 15§200 Nurse Practitioner (NP) Services
D. Collaboration Collaboration is a process in which an NP works with one or more physicians (MD/DO) to deliver health care services, with medical direction and appropriate supervision as required by the law of the State in which the services are furnished.
In the absence of State law governing collaboration, collaboration is to be evidenced by NPs documenting their scope of practice and indicating the relationships that they have with physicians to deal with issues outside their scope of practice.16
27
10
• Medicare Conditions of Payment require that PAs/NPs are supervised by 17/collaborate with18 an MD/DO.
• Medicare’s Conditions of Participation (CoP) for Hospitals require that each patient is under the care of an MD/DO.19
• There are no provisions for any other type of physician under Medicare payment rules. (DPM, Chiropractor, DDS, etc.)
Medicare:Supervision by an MD/DO
28
SCOPE OF PRACTICE
Scope of Practice
State Law, Rules and Regs Physician(s)
Payer Policy
Employer
Federal Law
Hospital/SNF/
NF/FQHC/RHC/LTCH/CAH/IRF
• Medicare• Dept. of Transportation• EMTALA• Dept. of Labor
– Federal Workers’ Comp– Federal Employee Health
Benefit Plan
• Medical Staff bylaws, rules/regs
• Joint Commission standards• Medicare CoPs
(Conditions of Participation)
• Employment Contract• Employer policies• Payer policy/contract
with employer
• Practice Act
• Insurance law
• Corporate law
• Ionizing radiation law
• Laser laws
• DMV laws
• Death Certificate laws
• Disaster law
• Camp/Sports/School
Physicals laws
• Impaired practitioner laws
• Public Health Code
• Medicaid law/Rules and Regs
• Workers’ Comp law/Policies
• State Medical Board
• Delegation/Collaboration/Written Agreement• Experience working with PAs/NPs
• MACs (Medicare Administrative Contractors)
• Private Payers• Worker’s Comp
(state and federal)• State Medicaid
30
11
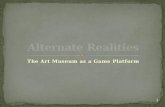
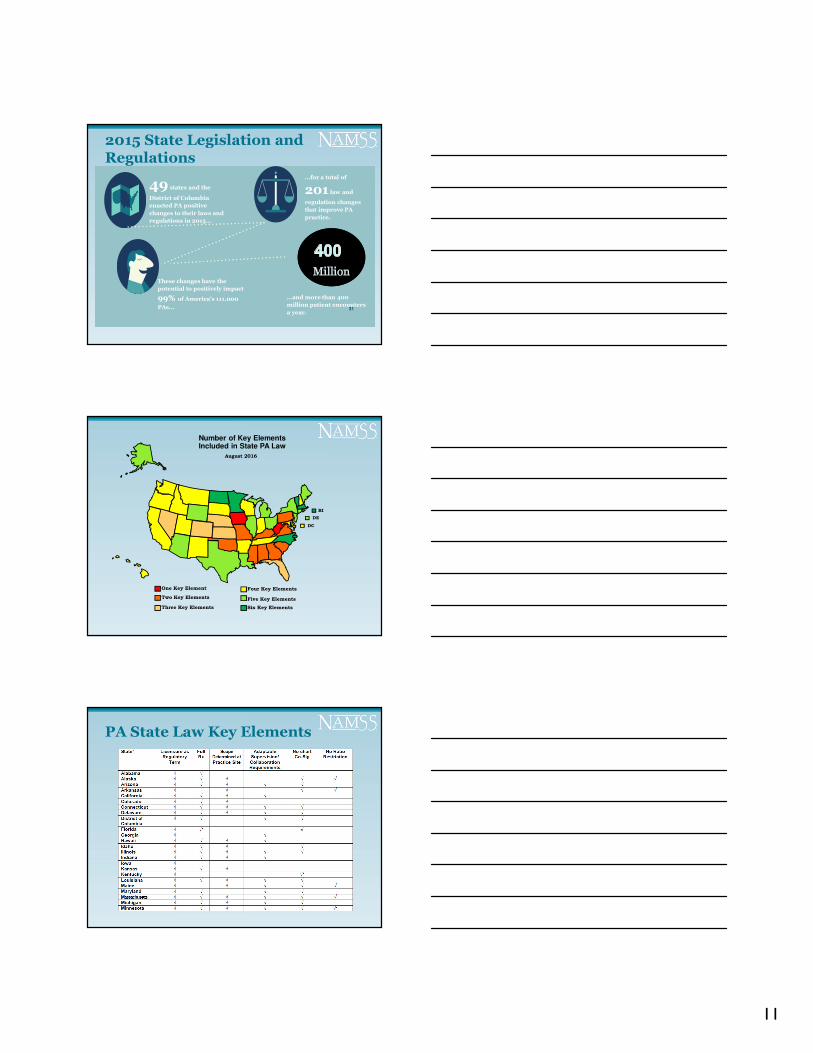
2015 State Legislation and Regulations
31
49 states and the
District of Columbia
enacted PA positive
changes to their laws and
regulations in 2015…
…for a total of
201 law and
regulation changes
that improve PA
practice.
These changes have the
potential to positively impact
99% of America's 111.000
PAs…
…and more than 400
million patient encounters
a year.
Number of Key Elements Included in State PA Law
August 2016
DC
DE
One Key Element
Two Key Elements
Three Key Elements
Four Key Elements
Five Key Elements
Six Key Elements
RI
PA State Law Key Elements
12
PA State laws update
PA Profession Regulatory Changes
35
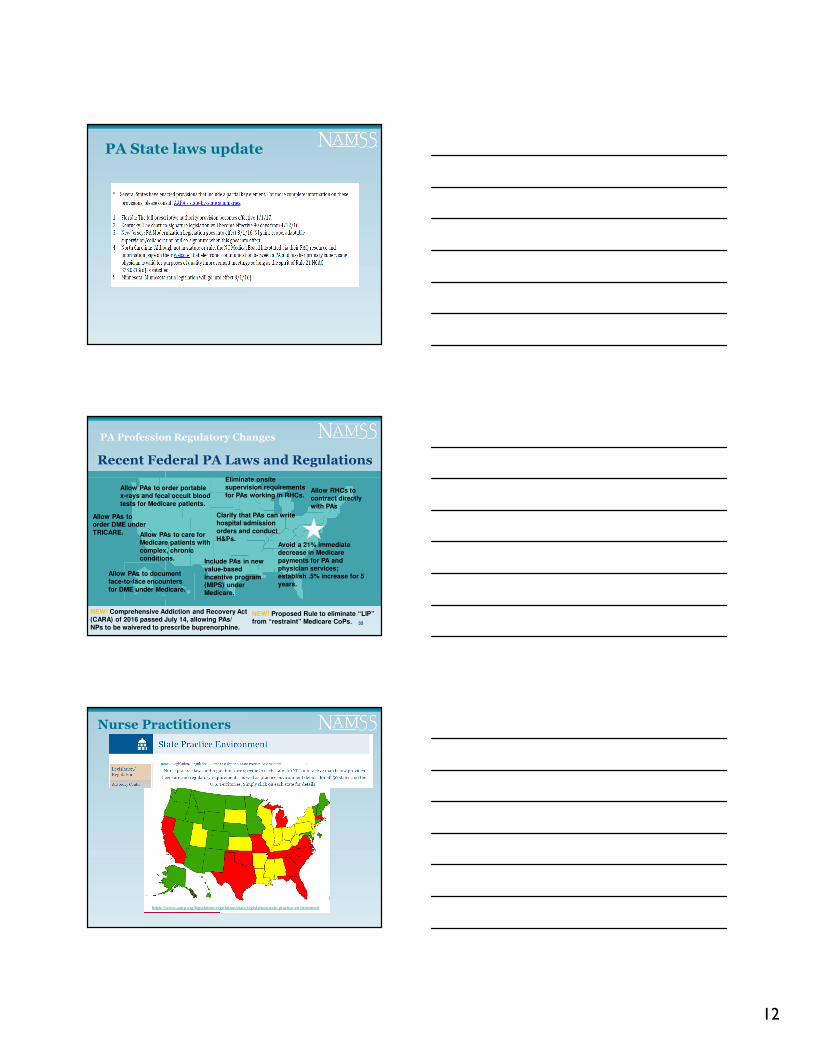
Recent Federal PA Laws and Regulations
Allow PAs to order portable x-rays and fecal occult blood
tests for Medicare patients.
Clarify that PAs can write hospital admission
orders and conduct H&Ps.
Eliminate onsite supervision requirements
for PAs working in RHCs.Allow RHCs to contract directly
with PAs
Allow PAs to order DME under
TRICARE.
Avoid a 21% immediate decrease in Medicare
payments for PA and physician services; establish .5% increase for 5
years.
Include PAs in new value-based
incentive program (MIPS) under Medicare.
Allow PAs to care for Medicare patients with
complex, chronic conditions.
Allow PAs to document face-to-face encounters
for DME under Medicare.
NEW! Proposed Rule to eliminate “LIP”from “restraint” Medicare CoPs.
NEW! Comprehensive Addiction and Recovery Act (CARA) of 2016 passed July 14, allowing PAs/
NPs to be waivered to prescribe buprenorphine.
https://www.aanp.org/legislation-regulation/state-legislation/state-practice-environment
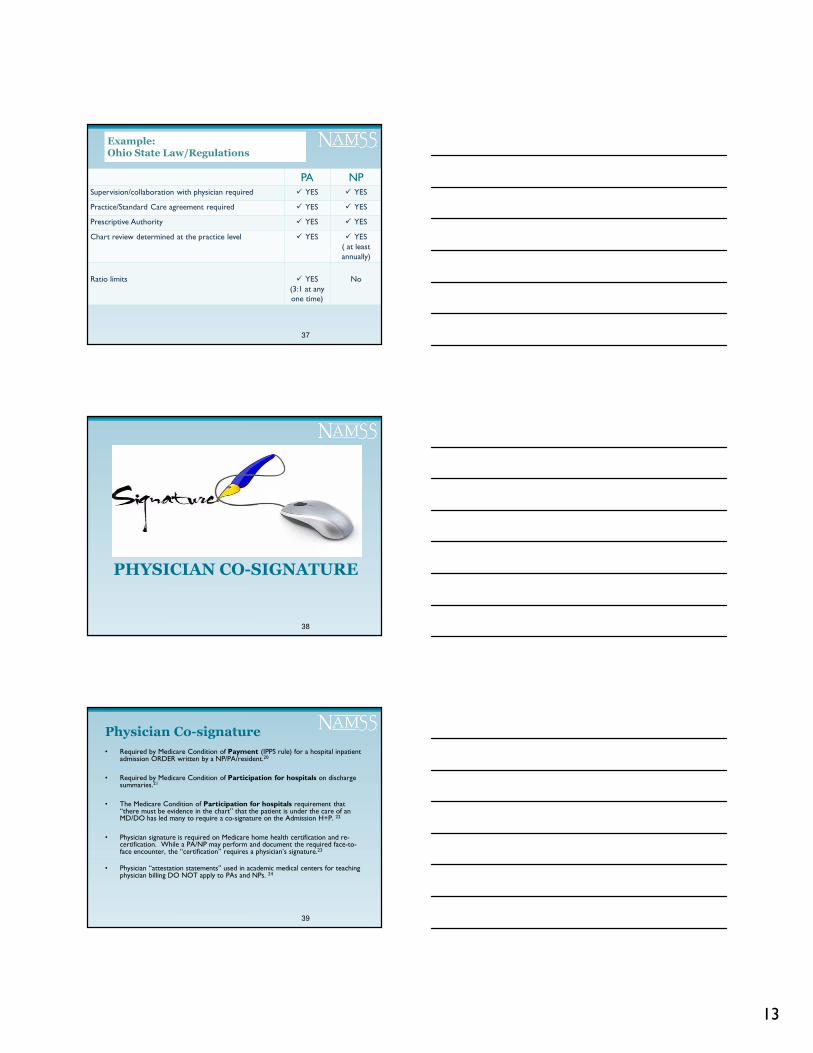
Nurse Practitioners
13
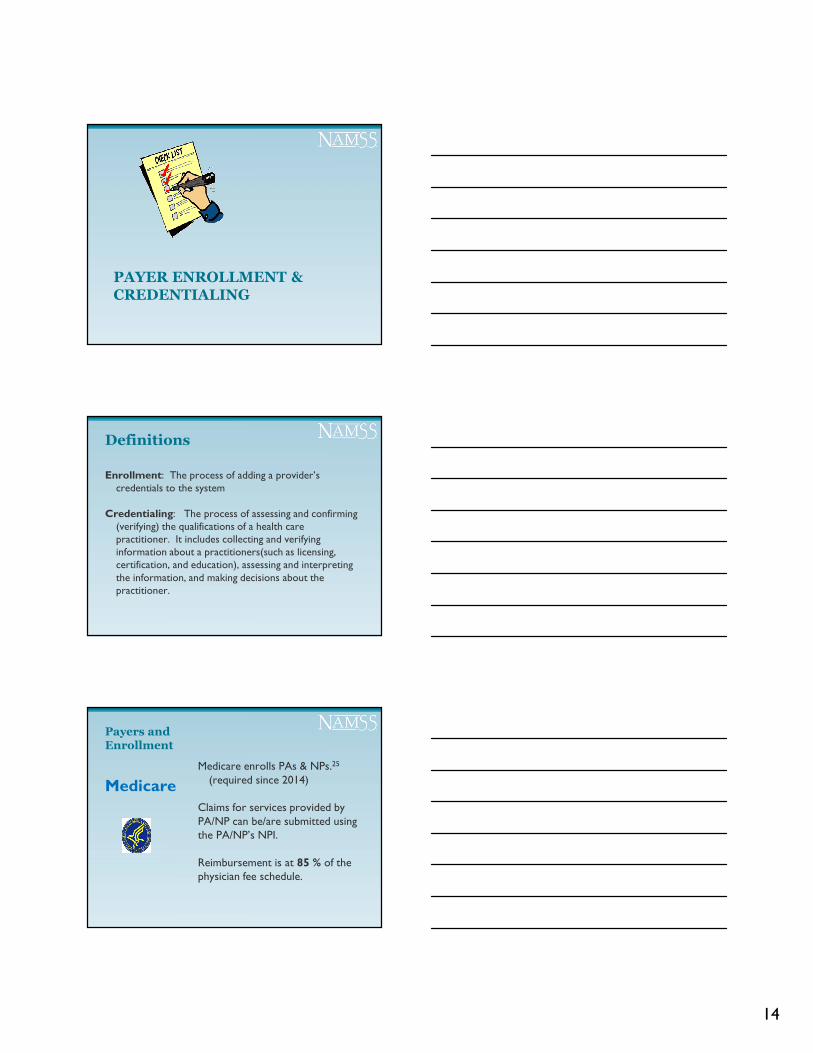
Example:Ohio State Law/Regulations
PA NPSupervision/collaboration with physician required � YES � YES
Practice/Standard Care agreement required � YES � YES
Prescriptive Authority � YES � YES
Chart review determined at the practice level � YES � YES( at least annually)
Ratio limits � YES(3:1 at any one time)
No
37
PHYSICIAN CO-SIGNATURE
38
• Required by Medicare Condition of Payment (IPPS rule) for a hospital inpatient admission ORDER written by a NP/PA/resident.20
• Required by Medicare Condition of Participation for hospitals on discharge summaries.21
• The Medicare Condition of Participation for hospitals requirement that “there must be evidence in the chart” that the patient is under the care of an MD/DO has led many to require a co-signature on the Admission H+P. 22
• Physician signature is required on Medicare home health certification and re-certification. While a PA/NP may perform and document the required face-to-face encounter, the “certification” requires a physician’s signature.23
• Physician “attestation statements” used in academic medical centers for teaching physician billing DO NOT apply to PAs and NPs. 24
Physician Co-signature
39
14
PAYER ENROLLMENT &CREDENTIALING
Definitions
Enrollment: The process of adding a provider’s credentials to the system
Credentialing: The process of assessing and confirming (verifying) the qualifications of a health care practitioner. It includes collecting and verifying information about a practitioners(such as licensing, certification, and education), assessing and interpreting the information, and making decisions about the practitioner.
Payers and Enrollment
Medicare enrolls PAs & NPs.25
(required since 2014)
Claims for services provided by PA/NP can be/are submitted using the PA/NP’s NPI.
Reimbursement is at 85 % of the physician fee schedule.
Medicare
15
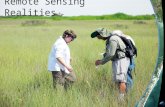
Payers and Enrollment:
• Medicaid programs in all states & DC pay for services provided by PAs and NPs.
• Medicaid enrolls or identifies the PA on the claim in 40 states; most states enroll NPs.
• 10 states and DC do not recognize PAs on the claim; claims are submitted under the physician.
• Some state Medicaid programs do not cover services provided in hospitals.
• Reimbursement rates vary widely.
– CT 90% for PAs and NPs
– TX 92% for PAs and NPs
– VA 100% for PAs and 75% for NPs
Medicaid
States that enroll PAs
State Medicaid Program Enrollment for PAs
RI
DE
DC
AAPA April 2016
States that do not enroll PAs
States scheduled to beginenrolling in 2016
44
Example-Illinois Medicaid: PAs
A-202.1 Charges Exception: A physician may submit a bill for services provided by a non-enrolled Advanced Practice Nurse (APN), a Physician Assistant (PA) or a Genetic Counselor, as long as such practice is in accordance with the policy outlined in this handbook or not in conflict with the following rules and regulations: Nurse Practice Act (225 ILCS 65) Physician Assistant Practice Act (225 ILCS 95) Genetic Counselor Licensing Act (225 ILCS 135) Department of Professional Regulations rules for administration of Physician
Assistant Practice Act (68 Ill. Adm. Code 1350) ….
Source: Handbook for Practitioners Rendering Medical Services, p.21 http://www2.illinois.gov/hfs/SiteCollectionDocuments/a200.pdf
16
Example-Illinois Medicaid: APNs
“All Certified Nurse Practitioners (CNP) and Clinical Nurse Specialists (CNS), may enroll with the department. With the exception of psychiatric services (CPT code range 90801 through 90899), which must be rendered by a physician, all services rendered by an APN are reimbursed at 100 percent of the physician’s rate. In addition, APNs may enroll as a primary care provider under the Maternal and Child Health (MCH) program.” http://www2.illinois.gov/hfs/MedicalProvider/MedicaidReimbursement/Pages/IndividualPractitioner.aspx
For enrollment information:Handbook for Practitioners Rendering Medical ServicesSection A-201.2 Advanced Practice Nurse Enrollment p.15 http://www2.illinois.gov/hfs/SiteCollectionDocuments/a200.pdf
Payers and Enrollment
Commercial Payers
• Private payers may promulgate their own rules.
• Many choose not to enroll PA/NPs. They DO however pay for services provided by PA/NPs.
• Claim is submitted under the physician’s number.
• Many do not discount; payment is at the physician rate.
• The organization billing must ascertain claims methodology and payment rate for each payer with whom they contract.
Example: Aetna
• Aetna enrolls PAs & NPs (since June 2010) except in Alaska, Kansas, Maine, Michigan and Missouri.
• Discounts PA/NP services to 85%.• Aetna’s policy manual states that it follows Medicare’s
“Incident-to” policy, allowing for 100% reimbursement if all rules are met.
• It remains the responsibility of the practice to ascertain the payment policy and claims instructions for each payer with whom they contract.
17
BILLING & REIMBURSEMENT
49
Medicare Payment Policy:“Incident to Billing”
“””We bill everything under the physician…”…”
“Incident-to Billing”26
“Incident to” is a Medicare billing provision that allows
reimbursement for services delivered by PAs/NPs at 100 percent of the physician fee schedule, provided that all “incident to” criteria are met.
“Incident to” billing only applies in a non-facility setting such as the physician’s office or physician’s clinic/POS 11.
DOES NOT apply in outpatient hospital clinic (provider based) or any facility setting such as inpatient hospital, skilled nursing facility/NF/IRF/LTCH, emergency department, and POS 22.
18
What’s Hot?
In the News
http://www.jdsupra.com/legalnews/mintz-levin-health-care-qui-tam-update-57076
In the News:Medicaid Billing under the physician NPI for services provided by NPs and PAs
From AHLA today:Audit: Northgate, Asaker Overbilled MassHealth, Medicaid, CHIP For Services Provided By Nurse Practitioners, PAs.The Springfield (MA) Republican (2/25, Berry) reports a state audit revealed Northgate Medical PC, of Springfield, Massachusetts, “substantially overbilled MassHealth for services that cost more than the actual services provided.” Over three years, the provider overbilled MassHealth by more than $191,000. In addition, AsakerMedical Associates, based in Brockton, “improperly billed MassHealth for over $24,000 in doctor-provided services that were actually performed by nurse practitioners.” State Auditor Suzanne M. Bump said “both Northgate and Asakerreceived overpayments from MassHealth, the state’s combined Medicaid and Children’s Health Insurance Program, for services ostensibly provided by doctors,” when in reality, nurse practitioners or physicians’ assistants (sic) provided the services.
19
What’s Hot?
06-20-2016After it self-disclosed conduct to OIG, Medical Plaza Family and Geriatric Physician, P.A. (Medical Plaza), North
Carolina, agreed to pay $109,975.24 for allegedly violating the Civil Monetary Penalties Law. OIG alleged that Medical Plaza submitted claims to Medicare for payment under two physicians' National Provider Identification numbers for incident-to services provided to patients at Medical Plaza when the services had been provided by Medical Plaza's nurse practitioners.
06-17-2016After it self-disclosed conduct to OIG, Radiology Alliance, PC (Radiology Alliance), Tennessee, agreed to pay
$355,461.34 for allegedly violating the Civil Monetary Penalties Law. OIG alleged that Radiology Alliance submitted claims to Federal health care programs that were false or fraudulent in the following ways: (1) services were performed by two radiology practitioner assistants that were supervised by Radiology Alliance's physicians as if they were personally provided by the physicians; (2) in certain instances Radiology Alliance billed for nursing practitioner and physician assistant services using the supervising physician's billing number at the supervising physician's billing rate; and (2) billed for the insertion of peripherally inserted central catheter lines by hospital nurses and radiology technicians that were supervised by Radiology Alliance's physicians as if those services were directly provided by the physicians.
https://oig.hhs.gov/fraud/enforcement/cmp/psds.asp
Medicare “Incident-to” Rules
• The physician must have personally treated the patient on his or her initial visit for the particular medical problem and established the diagnosis and treatment plan. (This is not a shared visit.)
• A physician (does not need to be the same physician) is within the suite of offices when the PA/NP renders the service upon
the patient’s return for follow-up for the same problem.
Medicare “Incident-to” Rules
• The physician must have some ongoing participation in the patient’s care.
• This must be reflected in the medical record somehow, in the event of an audit.
• If all requirements are met, encounter can be billed under physician’s NPI for 100% reimbursement.
• If ALL are not met, bill under the PA/NP’s NPI; reimbursement will be at 85%.
Be sure to check you MAC websites for guidance!!! 27
20
What about the 15% left on the table?!
Billing and Reimbursement
58
59
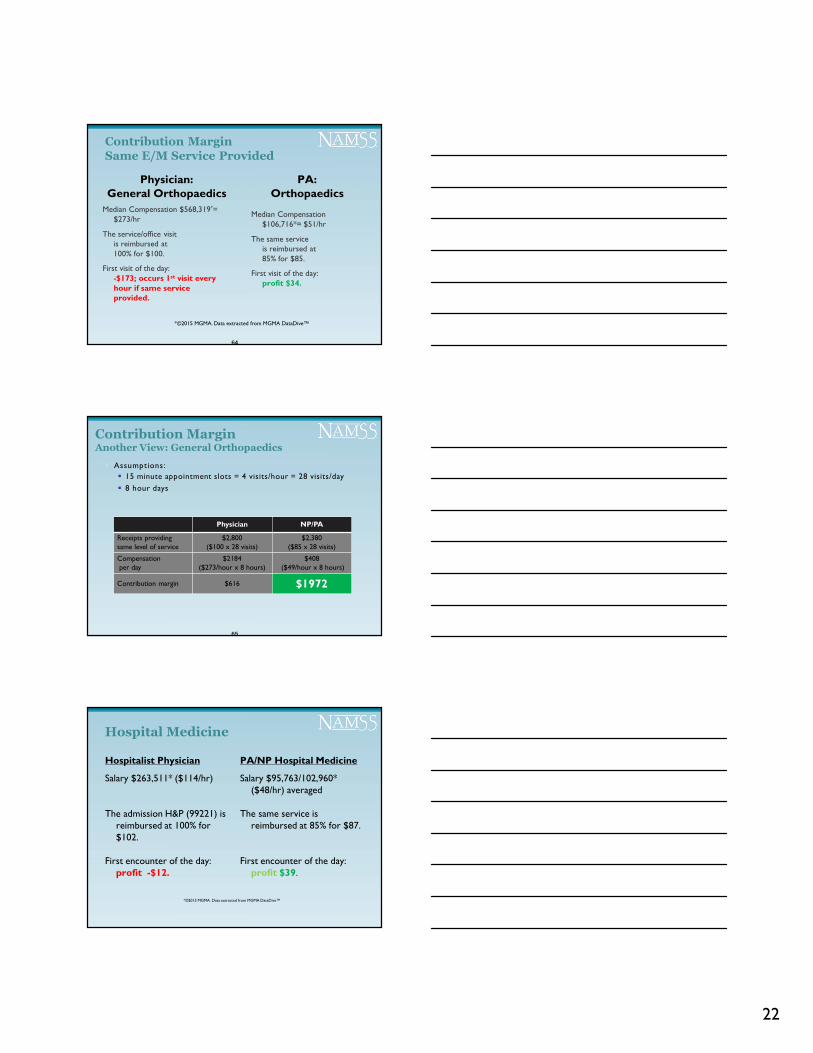
Office/Outpatient Visit: Established Patient
CPT Code Work RVU Non-facilityPrice*
Physician
Non-facilityPrice*PA/NP
99213 0.97 $73.40 $62.39
Source: CMS Physician Fee ScheduleAccessed March 25, 2016
*National Payment Amount: actual practice amount will vary by geographic index
60
15%= $11.01
21
• NPs/PAs are paid approximately 1/2 to 1/3 the salary of their physician counterpart.(This is a broad generalization, but supported by MGMA data.)
• The profit/contribution margin is higher when the NP/PA provides the service, even at the 85% reimbursement rate.
Contribution Margin:Provider Compensation
61
61
Median Salary $215,306*
($104/hr)
The service/office visit is reimbursed at 100% for $100.
First visit of the day: profit $4.
Same Service Provided
62
Physician: Family Medicine NP/PA: Family Medicine
Median Salary $95,118/$96,026* ($46/hr)
The same service is reimbursed at 85% for $85.
First visit of the day: profit $39.
62
*©2015 MGMA. Data extracted from MGMA DataDive™
Physician NP/PA
Receipts providing same level of service
$2,800($100 x 28 visits)
$2,380($85 x 28 visits)
Wage per day$832
($104/hour x 8 hours)$368
($46/hour x 8 hours)
Contribution margin $1,968 $2012
Another View: Family Medicine
63
� Assumptions:
� 15 minute appointment slots = 4 visits per hour = 28 visits/day
� 8 hour days
63
22
Median Compensation $568,319*= $273/hr
The service/office visit is reimbursed at 100% for $100.
First visit of the day: -$173; occurs 1st visit every hour if same service provided.
Contribution Margin
Same E/M Service Provided
Physician: General Orthopaedics
PA: Orthopaedics
Median Compensation $106,716*= $51/hr
The same service is reimbursed at 85% for $85.
First visit of the day: profit $34.
64
*©2015 MGMA. Data extracted from MGMA DataDive™
Physician NP/PA
Receipts providing same level of service
$2,800($100 x 28 visits)
$2,380($85 x 28 visits)
Compensationper day
$2184($273/hour x 8 hours)
$408($49/hour x 8 hours)
Contribution margin $616 $1972
Contribution MarginAnother View: General Orthopaedics
� Assumptions:
� 15 minute appointment slots = 4 visits/hour = 28 visits/day
� 8 hour days
65
Hospital Medicine
Hospitalist Physician
Salary $263,511* ($114/hr)
The admission H&P (99221) is reimbursed at 100% for $102.
First encounter of the day: profit -$12.
PA/NP Hospital Medicine
Salary $95,763/102,960* ($48/hr) averaged
The same service is reimbursed at 85% for $87.
First encounter of the day: profit $39.
*©2015 MGMA. Data extracted from MGMA DataDive™
23
MEDICARE PAYMENT POLICY:HOSPITAL SHARED VISITS
Split/Shared Visit 28 Hospital
• Can be billed for a new patient, admission, or subsequent hospital visit; the service performed was an evaluation and management (E/M) service, not a procedure nor a critical care service.
• PA/NP and physician must be employed by same entity (same hospital, same medical group).
• Physician must perform some element of history, exam, medical decision making and document on same calendar day.
• *If physician documentation not adequate, bill under PA/NP’s NPI.29
“Unacceptable” Shared Visit Documentation30
• "I have personally seen and examined the patient independently, reviewed the PA/NP's Hx, exam and MDM and agree with the assessment and plan as written“, signed by the physician
• "Patient seen“, signed by the physician
• "Seen and examined“, signed by the physician
• "Seen and examined and agree with above (or agree with plan)“, signed by the physician.
24
Shared Visit-Office
In the office/clinic, a shared visit only applies to an established patient. A new patient visit may not be performed as a shared visit under Medicare rules, and must be billed under the PA/NP’s NPI.
“When an E/M service is a shared/split encounter between a physician and a nonphysician practitioner (NP, PA, CNS or CNM), the service is considered to have been performed “incident to” if the requirements for “incident to” are met and the patient is an established patient.” 31
Shared visits /schedulesin the office are inefficient and poor utilization of PAs and NPs!
TEAM DEPLOYMENT DECISIONS
71
What are we doing now?
72
Evaluate current roles, responsibilities and costs associated with current team players. Opportunities? Challenges?
25
Slide used with permission.
SURVEY/ ACCREDITATIONCONSIDERATIONS
Hot Topics Reported from the Field
• Restraints and Seclusion
• EMTALA32
Medical Screening ExamCertification of False LaborOn-Call CoverageTransfers
• Conscious Sedation
• FPPE/OPPE
26
PA ResourcesAAPA Policy: Guidelines for Updating Medical Staff Bylaws: Credentialing and Privileging PAs. See page 102https://www.aapa.org/workarea/downloadasset.aspx?id=2147486552
EMTALA and PAshttp://www.aapa.org/WorkArea/DownloadAsset.aspx?id=2175
Competencies for the PA Professionhttp://www.aapa.org/WorkArea/DownloadAsset.aspx?id=2178
PAs: Assessing Clinical Competence/A Guide for regulators, hospitals, employers & third-party payershttp://www.aapa.org/WorkArea/DownloadAsset.aspx?id=2179
FPPE and OPPE are more than Just Acronyms (article)http://www.aapa.org/WorkArea/DownloadAsset.aspx?id=2180
Sample Competency Assessment Toolhttp://www.aapa.org/WorkArea/DownloadAsset.aspx?id=2181
Issue Brief, PA Scope of Practice http://www.aapa.org/WorkArea/DownloadAsset.aspx?id=583
Questions?
Contact: Tricia Marriotthttp://www.chlm.org/contact-us/
Endnotes
1 The clarity and transparency to patients and co-workers as they try to define their role and scope makes calling people who they are, as defined
by licensure important. FYI, in California, the acronym “APP” was just passed in law as “advanced practice pharmacist”. In many states, there is some statutory language to be considered as well. For example in CT:
APRN/CT Statutes, Chapter 378, Sec. 20-94a. Licensure as advanced practice registered nurse. (d) A person who has received a license pursuant to this section shall be known as an “Advanced Practice Registered Nurse” and no other person shall assume such title or use the letters or figures which indicate that the person using the same is a licensed advanced practice registered nurse. https://www.cga.ct.gov/current/pub/chap_378.htm#sec_20-94c
PA/CT Statutes Chapter 370, Sec. 20-12d (c)(4) …The physician assistant shall be clearly identified by appropriate identification as a physician assistant…https://www.cga.ct.gov/current/pub/chap_370.htm#sec_20-12a
2 Medicare Benefit Policy Manual, Chapter 15: http://www.cms.gov/manuals/Downloads/bp102c15.pdf
§190 “PAs may furnish services billed under all levels of CPT evaluation and management codes, and diagnostic tests if furnished under the general supervision of a physician.”
§200 “NPs may furnish services billed under all levels of evaluation and management codes and diagnostic tests if furnished in collaboration with a physician.”
3 Medicare Benefit Policy Manual: Chapter 15, http://www.cms.gov/manuals/Downloads/bp102c15.pdf
4 The Advisory Board Company: “What do consumers want?” accessed on the internet June 29, 2016 at https://www.advisory.com/-/media/Advisory-com/Research/MPLC/Resources/2015/30502_MPLC_Consumer_Survery_IG_web.pdf
5 Medicare Benefit Policy Manual, Chapter 15, §190 PA Services & §200 NP Services; https://www.cms.gov/Regulations-and-
Guidance/Guidance/Manuals/downloads/bp102c15.pdf
27
Endnotes
6 See 42CFR Subpart B—Inpatient Hospital Services and Inpatient Critical Access Hospital Services § 409.10 Included services. Available at http://ecfr.gpoaccess.gov/cgi/t/text/text-idx?c=ecfr;sid=2c2bea9c63d63947bf1840356b00ee8e;rgn=div5;view=text;node=42%3A2.0.1.2.9;idno=42;cc=ecfr#42:2.0.1.2.9.1.35.4; and
Department of Health & Human Services (DHHS) , Centers for Medicare & Medicaid Services (CMS), Pub 100-04 Medicare Claims Processing, Transmittal 1168 Date: JANUARY 26, 2007; https://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/downloads/R1168CP.pdf
MLN Matters Article #MM521 “Direct Billing and Payment for Non-Physician Practitioner (NPP) Services Furnished to Hospital Inpatients and Outpatients” https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNMattersArticles/downloads/MM5221.pdf
See also: “OIG FY2015 Work Plan” which includes review of Medicare cost reporting: http://oig.hhs.gov/reports-and-publications/archives/workplan/2015/WP15-2%20Medicare%20AB.pdf
7 Medicare Benefit Policy Manual, Chapter 15: http://www.cms.gov/manuals/Downloads/bp102c15.pdf
8 Medicare Enrollment Guidelines for Ordering and Referring Providers , December 2015, ICN 906223, available at https://www.cms.gov/outreach-and-education/medicare-learning-network-mln/mlnproducts/downloads/medenroll_orderreferprov_factsheet_icn906223.pdf ; See also MLN Matters® Number: SE1305https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNMattersArticles/Downloads/se1305.pdf
Endnotes
9 Medicare Benefit Policy Manual: Chapter 15, §190 Physician Assistant(PA) Services http://www.cms.gov/manuals/Downloads/bp102c15.pdf
10 Medicare Benefit Policy Manual: Chapter 15, §200 Nurse Practitioner (NP) Services http://www.cms.gov/manuals/Downloads/bp102c15.pdf
11 Medicare Benefit Policy Manual, Chapter 15 – Covered Medical and Other Health Services §190 - Physician Assistant (PA) Services
D. Employment Relationship
Payment for the services of a PA may be made only to the actual qualified employer of the PA that is eligible to enroll in the Medicare program under existing Medicare provider/supplier categories…. http://www.cms.gov/manuals/Downloads/bp102c15.pdf
12 Medicare Program Integrity Manual, Pub 100-08, Chapter 10, §2.4.11Payment for the PA’s services may only be made to the PA’s employer, not to the PA himself/herself. In other words, the PA cannot individually enroll in Medicare and receive direct payment for his or her services. This also means that the PA does not reassign his or her benefits to the employer, since the employer must receive direct payment anyway. The PA’s employer can be either an individual or an organization.” http://www.cms.gov/manuals/downloads/pim83c10.pdf
13 Medicare Benefit Policy Manual, Chapter 15 – Covered Medical and Other Health Services §200 Nurse Practitioner E. Direct Billing and Payment Direct billing and payment for NP services may be made to the NP. https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/bp102c15.pdf
14Medicare Benefit Policy Manual: Chapter 15, §190 Physician Assistant(PA) Services states:“The physician supervisor (or physician designee) need not be physically present with the PA when a service is being furnished to a patient and may be contacted by telephone, if necessary, unless State law or regulations require otherwise.” https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/bp102c15.pdf
15 Medicare Benefit Policy Manual: Chapter 15, §200 Nurse Practitioner (NP) Services states:“The collaborating physician does not need to be present with the NP when the services are furnished or to make an independent evaluation of each patient who is seen by the NP.” https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/bp102c15.pdf
Endnotes16 Medicare Benefit Policy Manual: Chapter 15, §200 Nurse Practitioner (NP) Services https://www.cms.gov/Regulations-and-
Guidance/Guidance/Manuals/downloads/bp102c15.pdf
17 Medicare Benefit Policy Manual: Chapter 15, §190 Physician Assistant(PA) Services, B. Covered Services Coverage is limited to the services a PA is legally authorized to perform in accordance with State law (or State regulatory mechanism provided by State law). 1. GeneralThe services of a PA may be covered under Part B, if all of the following requirements are met:• They are the type that are considered physician’s services if furnished by a doctor of medicine or osteopathy (MD/DO); • They are performed by a person who meets all the PA qualifications, • They are performed under the general supervision of an MD/DO;… http://www.cms.gov/manuals/Downloads/bp102c15.pdf
18 Medicare Benefit Policy Manual: Chapter 15, §200 Nurse Practitioner (NP) Services, B. Covered ServicesCoverage is limited to the services an NP is legally authorized to perform in accordance with State law (or State regulatory mechanism established by State law). 1. General The services of an NP may be covered under Part B if all of the following conditions are met:• They are the type that are considered physician’s services if furnished by a doctor of medicine or osteopathy (MD/DO);• They are performed by a person who meets the definition of an NP (see subsection A); • The NP is legally authorized to perform the services in the State in which they are performed; • They are performed in collaboration with an MD/DO (see subsection D); and…
19 Medicare Conditions of P{articiaption/ §482.12(c)(2) /TAG A-0066[…the governing body must ensure that the following requirements are met:]§482.12(c)(2) (continued) If a Medicare patient is admitted by a practitioner not specified in paragraph(c)(1) of this section, that patient is under the care of a doctor of medicine or osteopathy. Interpretive Guidelines §482.12(c)(2) CMS hospital regulations do permit licensed practitioners (e.g., nurse practitioners, midwives, etc), as allowed by the State, to admit patients to a hospital, and CMS does not require these practitioners be employed by a MD/DO. However, CMS regulations do require that Medicare and Medicaid patients admitted by these practitioners be under the care of an MD/DO. Evidence of being under the care of an MD/DO must be in the patient’s medical record. If a hospital allows these practitioners to admit and care for patients, as allowed by State law, the governing body and medical staff would have to establish policies and bylaws to ensure that the requirements of 42 CFR §482 are met. https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/som107ap_a_hospitals.pdf
28
Endnotes20 IPPS Rule January 30, 2014 “Additional Clarification of Guidance”
http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/Downloads/IP-Certification-and-Order-01-30-14.pdf.
21 State Operations Manual, Appendix A - Survey Protocol, Regulations and Interpretive Guidelines for Hospitals https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/som107ap_a_hospitals.pdf:
A-0468
§482.24(c)(2)(vii) Discharge summary with outcome of hospitalization, disposition of case, and provisions for follow-up care.
Interpretive Guidelines §482.24(c)(2)(vii)
In accordance with hospital policy, and 42 CFR part 482.12(c)(1)(i) the MD/DO may delegate writing the discharge summary to other qualified health care personnel such as nurse practitioners and MD/DO assistants to the extent recognized under State law or a State’s regulatory mechanism. Whether delegated or non-delegated, we would expect the person who writes the discharge summary to authenticate, date, and time their entry and additionally, for delegated discharge summaries, we would expect the MD/DO responsible for the patient during his/her hospital stay to co-authenticate and date the discharge summary to verify its content.
The discharge summary requirement would include outpatient records.
For example:
• The outcome of the treatment, procedures, or surgery;
• The disposition of the case;
• Provisions for follow-up care for an outpatient surgery patient or an emergency department patient who was not admitted or transferred to another hospital…
22 State Operations Manual, Appendix A - Survey Protocol, Regulations and Interpretive Guidelines for Hospitals accessed March 11, 2016 on the internet at https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/som107ap_a_hospitals.pdf:
A-0066 (Rev. 37, Issued: 10-17-08; Effective/Implementation Date: 10-17-08)
[…the governing body must ensure that the following requirements are met:]
§482.12(c)(2) (continued) If a Medicare patient is admitted by a practitioner not specified in paragraph(c)(1) of this section, that patient is under the care of a doctor of medicine or osteopathy.
Interpretive Guidelines §482.12(c)(2)
CMS hospital regulations do permit licensed practitioners (e.g., nurse practitioners, midwives, etc), as allowed by the State, to admit patients to a hospital, and CMS does not require these practitioners be employed by a MD/DO. However, CMS regulations do require that Medicare and Medicaid patients admitted by these practitioners be under the care of an MD/DO. Evidence of being under the care of an MD/DO must be in the patient’s medical record. If a hospital allows these practitioners to admit and care for patients, as allowed by State law, the governing body and medical staff would have to establish policies and bylaws to ensure that the requirements of 42 CFR §482 are met.
Endnotes23 Home Health: https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNMattersArticles/downloads/SE1038.pdf andhttps://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNMattersArticles/downloads/MM8441.pdf
24 DEPARTMENT OF HEALTH AND HUMAN SERVICES, Centers for Medicare & Medicaid Services, Guidelines for Teaching Physicians, Interns, and Residents, Medicare Learning Network ICN 006347 February 2015, available at https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/Downloads/Teaching-Physicians-Fact-Sheet-ICN006437.pdf. There are no provisions for PAs and NPs under the CMS teaching billing rules.
25 Medicare Enrollment Guidelines for Ordering and Referring Providers , December 2015, ICN 906223, available at https://www.cms.gov/outreach-and-education/medicare-learning-network-mln/mlnproducts/downloads/medenroll_orderreferprov_factsheet_icn906223.pdf ; See also MLN Matters® Number: SE1305https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNMattersArticles/Downloads/se1305.pdf
26 Medicare Benefit Policy Manual, Chapter 15, Section 60, https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/bp102c15.pdf See also “Incident-to” Billing, MLN Matters article SE0441, https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNMattersArticles/downloads/SE0441.pdf
27 Noridian https://med.noridianmedicare.com/web/jeb/topics/incident-to-services : WPS Medicare http://www.wpsmedicare.com/j8macpartb/training/on_demand/_files/2013-0723-incident-to-services-handout.pdf ; Palmetto http://www.palmettogba.com/palmetto/incident.nsf/front?OpenForm
28 Medicare Claims Processing Manual, Chapter 12, Section 30.6.1 (B), https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf; See also CMS Transmittal https://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/downloads/R178CP.pdf
29 See Contractor Guidance:Noridian: https://med.noridianmedicare.com/web/jfb/education/event-materials/incident-to-and-locum-tenens-qa#split-shared-billingWPS http://www.wpsmedicare.com/j8macpartb/resources/provider_types/inpatientsplitem.shtmlFirst Coast (Florida) https://medicare.fcso.com/FAQs/Answers/157200.aspCGS Medicare (KY and Ohio) : http://www.cgsmedicare.com/partb/pubs/news/2013/1113/cope23908.html
30 WPS http://www.wpsmedicare.com/j8macpartb/resources/provider_types/inpatientsplitem.shtml
Endnotes
31 Medicare Claims Processing Manual, Chapter 12, Section 30.6.1 (B), https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf
32 EMTALA and PAs http://www.aapa.org/WorkArea/DownloadAsset.aspx?id=2175