Hope in sight for retinoblastoma
2
NEWS AND VIEWS receptor–related protein 1 (LRP1/CD91), used by DC as a scavenger receptor, and this binding may theoretically contribute to the engulfment of anthracyclin-treated tumor cells—although recent studies in CD91-deficient cells argue against this possibility 8 . It will be intriguing to determine whether other CD91 ligands play a role in the uptake of anthracyclin-treated tumor cells, DC maturation or DC cross-priming. One such ligand is heat-shock protein gp96—another KDEL-containing protein localized to the endoplasmic reticulum that can escape that compartment and be exposed on the cell surface 9 . Regardless of which phagocytosis paradigm is key for this process, one is compelled to ask what it is that makes anthracyclins unique among apoptotic agents in promoting CRT translocation and initiating the immuno- genic tumor death program. This difference seems to lie with the ability of anthracyclins to enforce the early phosphorylation of eIF2α (ref. 2), a process normally observed in the endoplasmic reticulum under conditions of cellular stress, as a prelude to CRT emergence on the cell surface. This finding raises the possibility that useful therapies may derived from promoting eIF2α function—perhaps by antagonizing the function of the GADD34/ PP1 complex, which normally dephosphory- lates peIF2α (ref. 2). Such approaches may trigger the transloca- tion of intracellular CRT to the plasma mem- brane of the tumor cell in order to, as Obeid et al. put it, “confer immunogenicity to other- wise nonimmunogenic death.” Recombinant CRT could also be contemplated for co- administration into tumors treated with radio- or chemotherapy as a means to aug- ment DC-mediated cross-presentation in vivo—although it is not clear whether other agent-specific alterations would be required for immunogenicity. Additional factors would need to be seriously considered, also partly because of the range of biologic effects attributable to CRT. For instance, whereas an N-terminal fragment of CRT (vasostatin) has potent antiangiogenic effects 10 , topical appli- cation of full-length recombinant CRT may promote tumor angiogenesis 11 . Another cautionary note is that CRT may also prevent perforin- and complement- mediated cytolysis of tumor targets 12 , poten- tially debilitating the therapeutic efficacy of tumor-specific cytotoxic T cells in patients treated with such CRT-based approaches. Future studies should help resolve these outstanding issues. Meanwhile, the new findings support the notion that agents that encourage tumor cells to ‘die a good death’ hold considerable promise for the develop- ment of adjuvant immunotherapies designed to prolong life. 1. Klebanoff, C.A., Gattinoni, L. & Restifo, N.P. Immunol. Rev. 211, 214–224 (2006). 2. Obeid, M. et al. Nat. Med. 13, 52–59 (2006). 3. Ip, W.K. & Lau, Y.L. J. Immunol. 173, 189–196 (2004). 4. Albert, M.L. et al. J. Exp. Med. 188, 1359–1368 (1998). 5. Ackerman, A.L., Giodini, A. & Cresswell, P. Immunity 25, 607–617 (2006). 6. Ostwald, J.T. & MacLennan, D.H. J. Biol. Chem. 249, 974–979 (1974). 7. Johnson, S., Michalak, M., Opas, M. & Eggleton, P. Trends Cell Biol. 11, 122–129 (2001). 8. Walters, J.J. & Berwin, B. Traffic 6, 1173–1182 (2005). 9. Robert, J., Menoret, A. & Cohen, N. J. Immunol. 163, 4133–4139 (1999). 10. Pike, S.E. et al. J. Exp. Med. 188, 2349–2356 (1998). 11. Gold, L.I. et al. J. Investig. Dermatol. Symp. Proc. 11, 57–65 (2006). 12. Fraser, S.A., Karimi, R., Michalak, M. & Hudig, D. J. Immunol. 164, 4150–4155 (2000). Hope in sight for retinoblastoma Julien Sage The retinoblastoma gene (RB) was the first tumor suppressor gene cloned. But, until recently, little clinical progress had been made to target human tumors deficient in RB function. A new approach emerges from studying retinoblastoma tumors. The author is in the Departments of Pediatrics and Genetics, Stanford University, Stanford, California 94305, USA. e-mail: [email protected] Most, if not all, human tumor cells have muta- tions in the RB pathway, which acts as a check- point at the G1/S transition of the cell cycle. Thus, therapeutic approaches against cells with altered function of the pRB protein would benefit a large number of cancer patients 1 . However, limited progress has been made in identifying drugs that specifically recognize tumor cells with loss of pRB function. For instance, retinoblastoma, the pediatric retinal tumor that is the archetypal RB-mutant tumor, is still often treated by enucleation, radiation and systemic chemotherapy, resulting in blind- ness and increased risk of secondary tumors 2 . More than 20 years—and 20,000 references in PubMed—after its original discovery, tar- geted strategies against RB-mutant tumors are finally beginning to emerge, as shown in a recent report in Nature. Laurie et al. attack RB-mutant cancer cells not by focusing on RB itself, but by targeting molecules related to the RB pathway (ref. 3 and Fig. 1). The authors noticed that inactivation of pRB usually leads to the compensatory acti- vation of p53, a tumor suppressor that acts as a potent inducer of cell cycle arrest and cell death and is mutated in more than half of human tumors 4 . Retinoblastomas are part of the group of human tumors with intact p53 molecules, leading the authors to reason that these tumors may harbor alterations in other members of the p53 pathway. Indeed, they found that MDMX, a negative regulator of p53, was amplified in more than 60% of retinoblastomas, resulting in dampened p53 function. This observation led to the idea that increas- ing p53 activity by inhibiting MDMX with nutlin-3—a small molecule that inhibits the degradation of p53 by MDM2, a protein related to MDMX—may stop the proliferation of reti- noblastoma cells. Indeed, in culture and in a mouse xenograft model, nutlin-3 promoted cell cycle arrest and cell death in retinoblas- toma cells. In addition, nutlin-3 cooperated potently with topotecan, a chemotherapeutic agent used in patients, to stop the growth of retinoblastomas 3 . A note of caution is raised by another recent report indicating that altering the interactions between MDMX/MDM2 and p53 may produce detrimental effects 5 . Nevertheless, the new findings by Laurie et al. are a major advance in the development of new approaches against 30 VOLUME 13 | NUMBER 1 | JANUARY 2007 NATURE MEDICINE © 2007 Nature Publishing Group http://www.nature.com/naturemedicine
Transcript of Hope in sight for retinoblastoma

N E W S A N D V I E W S
receptor–related protein 1 (LRP1/CD91), used by DC as a scavenger receptor, and this binding may theoretically contribute to the engulfment of anthracyclin-treated tumor cells—although recent studies in CD91-deficient cells argue against this possibility8.
It will be intriguing to determine whether other CD91 ligands play a role in the uptake of anthracyclin-treated tumor cells, DC maturation or DC cross-priming. One such ligand is heat-shock protein gp96—another KDEL-containing protein localized to the endoplasmic reticulum that can escape that compartment and be exposed on the cell surface9.
Regardless of which phagocytosis paradigm is key for this process, one is compelled to ask what it is that makes anthracyclins unique among apoptotic agents in promoting CRT translocation and initiating the immuno-genic tumor death program. This difference seems to lie with the ability of anthracyclins to enforce the early phosphorylation of eIF2α (ref. 2), a process normally observed in the endoplasmic reticulum under conditions of cellular stress, as a prelude to CRT emergence on the cell surface. This finding raises the
possibility that useful therapies may derived from promoting eIF2α function—perhaps by antagonizing the function of the GADD34/PP1 complex, which normally dephosphory-lates peIF2α (ref. 2).
Such approaches may trigger the transloca-tion of intracellular CRT to the plasma mem-brane of the tumor cell in order to, as Obeid et al. put it, “confer immunogenicity to other-wise nonimmunogenic death.” Recombinant CRT could also be contemplated for co-administration into tumors treated with radio- or chemotherapy as a means to aug-ment DC-mediated cross-presentation in vivo—although it is not clear whether other agent-specific alterations would be required for immunogenicity. Additional factors would need to be seriously considered, also partly because of the range of biologic effects attributable to CRT. For instance, whereas an N-terminal fragment of CRT (vasostatin) has potent antiangiogenic effects10, topical appli-cation of full-length recombinant CRT may promote tumor angiogenesis11.
Another cautionary note is that CRT may also prevent perforin- and complement-mediated cytolysis of tumor targets12, poten-
tially debilitating the therapeutic efficacy of tumor-specific cytotoxic T cells in patients treated with such CRT-based approaches.
Future studies should help resolve these outstanding issues. Meanwhile, the new findings support the notion that agents that encourage tumor cells to ‘die a good death’ hold considerable promise for the develop-ment of adjuvant immunotherapies designed to prolong life.
1. Klebanoff, C.A., Gattinoni, L. & Restifo, N.P. Immunol. Rev. 211, 214–224 (2006).
2. Obeid, M. et al. Nat. Med. 13, 52–59 (2006). 3. Ip, W.K. & Lau, Y.L. J. Immunol. 173, 189–196
(2004).4. Albert, M.L. et al. J. Exp. Med. 188, 1359–1368
(1998).5. Ackerman, A.L., Giodini, A. & Cresswell, P. Immunity
25, 607–617 (2006).6. Ostwald, J.T. & MacLennan, D.H. J. Biol. Chem. 249,
974–979 (1974).7. Johnson, S., Michalak, M., Opas, M. & Eggleton, P.
Trends Cell Biol. 11, 122–129 (2001).8. Walters, J.J. & Berwin, B. Traffic 6, 1173–1182
(2005).9. Robert, J., Menoret, A. & Cohen, N. J. Immunol. 163,
4133–4139 (1999).10. Pike, S.E. et al. J. Exp. Med. 188, 2349–2356
(1998).11. Gold, L.I. et al. J. Investig. Dermatol. Symp. Proc.
11, 57–65 (2006).12. Fraser, S.A., Karimi, R., Michalak, M. & Hudig, D. J.
Immunol. 164, 4150–4155 (2000).
Hope in sight for retinoblastomaJulien Sage
The retinoblastoma gene (RB) was the first tumor suppressor gene cloned. But, until recently, little clinical progress had been made to target human tumors deficient in RB function. A new approach emerges from studying retinoblastoma tumors.
The author is in the Departments of Pediatrics and
Genetics, Stanford University, Stanford, California
94305, USA.
e-mail: [email protected]
Most, if not all, human tumor cells have muta-tions in the RB pathway, which acts as a check-point at the G1/S transition of the cell cycle. Thus, therapeutic approaches against cells with altered function of the pRB protein would benefit a large number of cancer patients1. However, limited progress has been made in identifying drugs that specifically recognize tumor cells with loss of pRB function. For instance, retinoblastoma, the pediatric retinal tumor that is the archetypal RB-mutant tumor, is still often treated by enucleation, radiation and systemic chemotherapy, resulting in blind-ness and increased risk of secondary tumors2.
More than 20 years—and 20,000 references in PubMed—after its original discovery, tar-geted strategies against RB-mutant tumors are finally beginning to emerge, as shown in a recent report in Nature. Laurie et al. attack RB-mutant cancer cells not by focusing on RB itself, but by targeting molecules related to the RB pathway (ref. 3 and Fig. 1).
The authors noticed that inactivation of pRB usually leads to the compensatory acti-vation of p53, a tumor suppressor that acts as a potent inducer of cell cycle arrest and cell death and is mutated in more than half of human tumors4. Retinoblastomas are part of the group of human tumors with intact p53 molecules, leading the authors to reason that these tumors may harbor alterations in other members of the p53 pathway. Indeed, they found that MDMX, a negative regulator of p53, was amplified in more than 60% of
retinoblastomas, resulting in dampened p53 function.
This observation led to the idea that increas-ing p53 activity by inhibiting MDMX with nutlin-3—a small molecule that inhibits the degradation of p53 by MDM2, a protein related to MDMX—may stop the proliferation of reti-noblastoma cells. Indeed, in culture and in a mouse xenograft model, nutlin-3 promoted cell cycle arrest and cell death in retinoblas-toma cells. In addition, nutlin-3 cooperated potently with topotecan, a chemotherapeutic agent used in patients, to stop the growth of retinoblastomas3.
A note of caution is raised by another recent report indicating that altering the interactions between MDMX/MDM2 and p53 may produce detrimental effects5. Nevertheless, the new findings by Laurie et al. are a major advance in the development of new approaches against
30 VOLUME 13 | NUMBER 1 | JANUARY 2007 NATURE MEDICINE
©20
07 N
atur
e P
ublis
hing
Gro
up
http
://w
ww
.nat
ure.
com
/nat
urem
edic
ine

N E W S A N D V I E W S
RB-deficient tumors, especially for local thera-pies against retinoblastomas. In addition, com-bining this approach with others may improve the efficacy of treatments against tumors with loss of pRB function. For instance, Johnson et al. have taken advantage of the activation of E2F transcription factors induced by loss of pRB (Fig. 1) to selectively kill cells with muta-tions in the RB pathway6.
There are other tactics also worth consider-ing. One is to increase pRB activity in cancer cells. Reintroducing RB cDNAs into RB-mutant tumor cells by gene therapy7, while feasible in theory, remains challenging. But because pRB levels in cells are actively controlled by the proteasome machinery8, the stability of
endogenous pRB could be increased by treat-ing tumor cells carrying mutations in the RB pathway (but not in RB itself) with proteasome inhibitors.
Another tactic is to increase the compensa-tory effects of the pRB family members p107 and p130, which share redundant functions with pRB but are rarely mutated in human tumors9. For instance, the stability of p130 could be increased by inhibiting its normal deg-radation in cycling cells by the proteasome10. Because proteasome inhibitors are already in clinical trials11, their use to treat RB-mutant tumors may be relatively straightforward. However, cyclin D/CDK4,6 kinases, which directly control the function of pRB family
Kat
ie R
is
Demethylation
Proteasome inhibitors Inhibitors (nutlin-3) Activators Nutlin-3
Kinaseinhibitors
p16Ink4a
Cyclin DCDK4,6
pRB, p107, p130
Modulators
Chromatinremodelingcomplexes
Inducible lytic virus
E2Fsp19ARF
Cyclin ECDK2 p21
MDM2 p53 MDMX
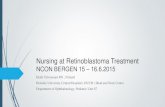
Figure 1 Possible points of therapeutic interventions against human cancers with alterations in the RB pathway. The RB pathway is mutated in most human cancers. Strategies to reactivate pRB function include re-expressing p16Ink4a by using methylation inhibitors, inhibiting the kinase activity of CDK4,6 and stabilizing the levels of pRB family proteins. In addition, it may be possible to take advantage of the consequences of loss of pRB function, such as activated E2F and p53 transcription factors, or changes in the structure of the chromatin. Laurie et al. used nutlin-3, an inhibitor of MDMX, to activate p53 function and stop retinoblastoma tumor cells3.
proteins, are often highly active in tumor cells, which may be sufficient to phosphorylate and inactivate any pool of pRB, p107 and p130.
This problem could be addressed by specific inhibitors of the CDK4,6 kinases. Some of these inhibitors, such as roscovitine, are currently being tested in clinical trials12. These molecules may also work in cancer cells in which the pRB protein is absent by decreasing the phosphor-ylation of p107 and p130, thereby increasing their compensatory effects. However, this strategy may also have nonspecific effects by inhibiting the proliferation of normally cycling cells in the organism.
None of the current approaches are perfect, but combining them may help tremendously to treat patients with cancers associated with loss of pRB function. In addition, the fact that we only realize now, after more than 20 years of research, that MDMX may be such a critical target in retinoblastoma cells emphasizes the need to better understand the complex cellular networks centered on RB.
1. Weinberg, R.A. Cell 81, 323–330 (1995).2. Abramson, D.H. & Schefler, A.C. Retina 24, 828–848
(2004).3. Laurie, N.A. et al. Nature 444, 61–66 (2006).4. Sherr, C.J. & McCormick, F. Cancer Cell 2, 103–112
(2002).5. Ringshausen, I., O’Shea, C.C., Finch, A.J., Brown
Swigart, L. & Evan, G.I. Cancer Cell 10, 501–514 (2006).
6. Johnson, L. et al. Cancer Cell 1, 325–337 (2002).7. Nikitin, A.Y., Juarez-Perez, M.I., Li, S., Huang, L. &
Lee, W.H. Proc. Natl. Acad. Sci. USA 96, 3916–3921 (1999).
8. Ying, H. & Xiao, Z.X. Cell Cycle 5, 506–508 (2006).9. Classon, M. & Harlow, E. Nat. Rev. Cancer 2, 910–917
(2002).10. Tedesco, D., Lukas, J. & Reed, S.I. Genes Dev. 16,
2946–2957 (2002).11. Adams, J. Cancer Cell 5, 417–421 (2004).12. Meijer, L. & Raymond, E. Acc. Chem. Res. 36, 417–
425 (2003).
Bad signals jam organelle trafficEsteban C Dell’Angelica
Defects in organelle biogenesis and trafficking underlie a newly described genetic disorder. These defects are traced to the gene encoding a scaffolding protein that coordinates signal transduction events on late endosomes (pages 38–45).
The author is in the Department of Human
Genetics, David Geffen School of Medicine,
University of California Los Angeles, Los Angeles,
California 90095, USA.
e-mail: [email protected]
In this issue, Bohn et al.1 examine the basis for a rare genetic disease in which albinism is com-bined with other symptoms such as primary immunodeficiency. The authors find that this
disease arises from defects in multiple organelles related to lysosomes and that it is due to a muta-tion in the gene encoding the endosomal adaptor protein p14. Because p14 is a known regulator of the mitogen-activated protein kinase (MAPK) signal transduction cascade2, the work by Bohn et al. uncovers an exciting link between signal transduction and organelle biogenesis.
Some of the unique functions of highly spe-cialized cells, including those of the immune
system, rely on membrane-bounded organ-elles specific to these cell types. Examples of these organelles include the lytic granules of cytotoxic T lymphocytes (CTLs), which participate in the killing of virus-infected cells, and the azurophilic granules of neu-trophils, which store molecules involved in the destruction of phagocytosed bacteria3. Despite substantial differences in morpho-logy and content, several of these cell
NATURE MEDICINE VOLUME 13 | NUMBER 1 | JANUARY 2007 31
©20
07 N
atur
e P
ublis
hing
Gro
up
http
://w
ww
.nat
ure.
com
/nat
urem
edic
ine