History & Evolution of Foot and Lower Extremity Biomechanics and Foot Orthoses… · 2017-10-16 ·...
15
3/26/2015 1 History and Evolution of Foot and Lower Extremity Biomechanics and Foot Orthoses Kevin A. Kirby, DPM Adjunct Associate Professor Department of Applied Biomechanics California School of Podiatric Medicine Oakland, California Private Practice, Sacramento, California 2015 PAC Symposium: “Biomechanics and the Future of Footcare” Vancouver, BC April 17-18, 2015 Biomechanics and foot orthoses have evolved over the centuries Many talented individuals have increased our knowledge in foot and lower extremity biomechanics and about foot orthoses What people and events have shaped history and evolution of podiatric biomechanics and orthoses? What is the History of Foot Biomechanics and Foot Orthoses? Aristotle Aristotle (384-322 BC), Greek scientist and philosopher, was one of earliest biomechanics authors His treatise, About the Movement of Animals (350 BC) provided first scientific analysis of gait and first geometric analysis of muscular actions on bones First accurately described GRF as : “…for just as the pusher pushes, so the pusher is pushed” Aristotle (384 BC – 322 BC) Archimedes Archimedes (287-212 BC) was Greek scientist who is considered one of greatest mathematicians of antiquity Discovered principles of hydrostatics, statics and physics of levers, working to solve the problem of moving a given weight by a given force “Give me a place to stand on, and I will move the Earth” Archimedes (287-212 BC) Galen Galen (129-201 AD) was Roman physician and surgeon Considered first “sports physician” Was “team doctor” to Roman gladiators by age 28 In his work De Motu Musculorum (On the Motion of Muscles), he first explained difference between motor and sensory nerves and agonist and antagonist muscles Sought to raise medicine to level of exact science Galen (129-201 AD) Leonardo DaVinci Leonardo DaVinci (1452-1519), Italian painter, sculptor and inventor, had keen interest in form & function of human body Inspired by desire to accurately represent human movement in his paintings and sculptures In regard to running form on varied surfaces, DaVinci wrote: “He who runs down a slope has his axis on his heels; and he who runs uphill has it on the toes of his feet; and a man running on level ground has it first on his heels and then on the toes of his feet.” Leonardo DaVinci (1452-1519)
Transcript of History & Evolution of Foot and Lower Extremity Biomechanics and Foot Orthoses… · 2017-10-16 ·...

3/26/2015
1
History and Evolution of Foot and Lower Extremity Biomechanics
and Foot Orthoses
Kevin A. Kirby, DPMAdjunct Associate Professor
Department of Applied Biomechanics California School of Podiatric Medicine
Oakland, California Private Practice, Sacramento, California
2015 PAC Symposium: “Biomechanics and the Future of Footcare” Vancouver, BC
April 17-18, 2015
Biomechanics and foot orthoses have evolved over the centuries
Many talented individuals have increased our knowledge in foot and lower extremity biomechanics and about foot orthoses
What people and events have shaped history and evolution of podiatric biomechanics and orthoses?
What is the History of Foot Biomechanics and Foot Orthoses?
Aristotle
Aristotle (384-322 BC), Greek scientist and philosopher, was one of earliest biomechanics authors
His treatise, About the Movement of Animals (350 BC) provided first scientific analysis of gait and first geometric analysis of muscular actions on bones
First accurately described GRF as : “…for just as the pusher pushes, so the pusher is pushed”
Aristotle (384 BC – 322 BC)
Archimedes
Archimedes (287-212 BC) was Greek scientist who is considered one of greatest mathematicians of antiquity
Discovered principles of hydrostatics, statics and physics of levers, working to solve the problem of moving a given weight by a given force
“Give me a place to stand on, and I will move the Earth”
Archimedes (287-212 BC)
GalenGalen (129-201 AD) was Roman physician and surgeon
Considered first “sports physician”
Was “team doctor” to Roman gladiators by age 28
In his work De Motu Musculorum(On the Motion of Muscles), he first explained difference between motor and sensory nerves and agonist and antagonist muscles
Sought to raise medicine to level of exact science
Galen (129-201 AD)
Leonardo DaVinci
Leonardo DaVinci (1452-1519), Italian painter, sculptor and inventor, had keen interest in form & function of human body Inspired by desire to accurately represent human movement in his paintings and sculpturesIn regard to running form on varied surfaces, DaVinci wrote:
“He who runs down a slope has his axis on his heels; and he who runs uphill has it on the toes of his feet; and a man running on level ground has it first on his heels and then on the toes of his feet.”
Leonardo DaVinci(1452-1519)

3/26/2015
2
Giovanni BorelliGiovanni Borelli (1608-1679), Italian physicist, physiologist and mathematician, wrote first book on biomechanics, De MotuAnimalium, in 1685 First to fully describe geometrical principles of levers of musculo-skeletal system and that muscles produce much larger forces than resisting external forcesBorelli found forces required for equilibrium in various joints of human body before NewtonBorelli is often called: “Father of Biomechanics”
Giovanni Borelli (1608-1679)
Isaac Newton
Isaac Newton (1642-1727), British mathematician and physicist, is considered by many to be greatest scientist of all time
Invented calculus at age 24
Published Philosophiae Naturalis Principia Mathematica in 1686 which contained his now famous Three Laws of Motion
Credited with creating the laws of inertia, acceleration, action and reaction forces and of gravity
Isaac Newton (1642-1727)
Nicolas Andry
Nicolas Andry (1658-1742), a French physician, first coined the term “orthopedics” meaning “straight child”
Published book, Orthopaedia: The Art of Correcting and Preventing Deformities in Children in1740
“If the feet incline too much to one side, you must give the child shoes that are higher on that side, both in the sole and heel, which will make him incline to the opposite side.“
Nicolas Andry(1658-1742)
Petrus Camper
Petrus Camper (1722-1789) was a Dutch physician and pioneer in pediatrics
Published one of first books on foot deformities, “On the Best Form of Shoe” in 1781, which was reprinted into 14 editions
Camper’s book stimulated interest in placing arch-supporting orthoses into shoes for children’s flatfoot
Petrus Camper (1722-1789)
“It is surprising that while mankind in all ages have bestowed the greatest attention upon the feet of horses, mules, oxen, and other animals of burthen of draught, they have entirely neglected those of their own species, abandoning them to the ignorance of workmen, who, in general, can only make a shoe upon routine principles, and according to the absurdities of fashion, or the depraved taste of the day. Thus, from our earliest infancy, shoes, as at present worn, serve but to deform the toes and cover the feet with corns, which not only render walking painful, but, in some cases, absolutely impossible.” P. Camper, 1781
Petrus Camper
Shoe Fashions from 1760
Lewis Durlacher
Lewis Durlacher (1792-1864), a British chiropodist, was royal chiropodist appointed to Queen Victoria
In 1845, he developed leather foot orthosis to correct for “plantar pressure lesions” and “foot imbalances”
Durlacher first described intermetatarsal neuroma, over 30 years before T.G. Morton

3/26/2015
3
Hugh Owen Thomas
Hugh Owen Thomas (1834-1891) was a British orthopedic surgeon with interest in treating feet
In 1874, Thomas suggested using a “few pennies worth of leather” for lifts, bars, and wedges on shoes to treat foot problems
Invented, in 1876, “crooking” of shoe heel, to extend the heel under the antero-medial aspect of shoe sole for treating pronated feet (now called “Thomas heel”)
Hugh Owen Thomas(1834-1891)
Newton Melman Shaffer
Newton M. Shaffer (1846-1928), a New York City orthopedist, first described high arched foot with multiple clawtoes
Became widely known as “Shaffer’s Foot”
Also designed a high-medial arched orthosis with a heel cup which became known as a “Shaffer Plate”
Newton M. Shaffer (1846-1928)
Royal Whitman
Royal Whitman (1857-1946) was a 1882 Harvard Medical School graduate and New York City orthopedic surgeon that had special interest in foot function
Wrote numerous textbooks on orthopedic surgery and taught orthopedics for 40 years
Royal Whitman (1857-1946)
Whitman’s “Weak Foot”
Whitman’s description of “weak foot” very closely matches our current description of the pronated, flat-arched foot with an internally rotated tibia
Whitman’s Three Grades of “Weak Foot”
1st Degree: The normal foot improperly used, as shown by the method of standing and walking
2nd Degree: The foot in which the range of voluntary motion is restricted, showing disuse of function, and in which the elements of deformity are apparent when weight is borne
3rd Degree: That in which the passive range of motion is restricted, or in which there are evident weakness and deformity. This limitation of motion depends, as a rule, on accommodative changes in structure to the habitual postures or to the deformity
Whitman R: A study of the weak foot, with reference to its causes, its diagnosis, and its cure; with an analysis of a thousand cases of so-called flat-foot. JBJS, 8:42-77, 1896.
Whitman’s Foot Brace
Developed in 1885
Made from plaster cast taken with foot in supinated position
18-20 gauge sheet steel was formed into a high medial arch brace
Goal was to raise medial arch so foot would be less pronated

3/26/2015
4
Percy Willard Roberts
Percy W. Roberts (1867-1937), American orthopedic surgeon, developed metal foot orthosis in 1912
Roberts foot orthosis had deep inverted heel cup that attempted to tilt rearfoot into inverted position
Had medial and lateral clips and narrow heel cup
Roberts brace applied too much force over too little area and tended to cause irritation to plantar foot
1895 - Beginning of Chiropody
During most of 19th century, medical doctors showed little interest in treating foot problems
Barbers, families and practically anyone that showed an interest in treating feet adopted the “craft” of foot care to fill the void in healthcare of the foot that was left by medical doctors
In 1895, group of dedicated practitioners in New York successfully appealed to NY State Legislature to first establish chiropody (now podiatry) as a licensed profession
First Podiatry Society & School Formed
In 1895, Pedic Society of New York became first official society for chiropody/podiatry
First school of chiropody established in New York in 1911
In 1912, first national podiatry association, and precursor to current APMA, American National Chiropody Association, was formed and is now 100 years old
First Issue of Pedic Society Items – First “Podiatry Journal”
Alfred Joseph, First President of National
Association of Chiropodists”
Podiatric Approach to Foot Biomechanics in Early 20th Century
Approach to foot mechanics in early 20th century was based largely on shape of medial longitudinal arch with “normal foot” being viewed as having “normally arched architecture” with treatments geared toward restoring a “normal arch”
Many podiatrists relied on orthopedic shoe makers to make custom leather foot or steel appliances to treat “weak feet”
Early 20th Century Treatment of “Weak
Feet” Used Whitman’s Concepts
Otto Frederick Schuster
Otto F. Schuster (1881-1936) arrived in US in 1906 from Hamburg, Germany where he had trained as a brace maker
Schuster started making Whitman braces for Royal Whitman and other orthopedists in NY in 1909
Became a podiatrist in 1911 Otto F. Schuster (1881-1936)
First Podiatric Orthopedics TextOtto F. Schuster became professor of orthopedics at NY Podiatry School
In 1927, published first podiatric orthopedics text, Foot Orthopedics, later rewritten by his podiatrist-son, Otto N. Schuster
Foot Orthopedics remained in use as a valuable textbook until 1950s

3/26/2015
5
Roberts-Whitman Brace
In the 1920s, Otto F. Schuster combined ideas of Roberts brace with Whitman brace to make Roberts-Whitman brace
Roberts-Whitman brace had deep inverted heel cup, high medial arch and wider profile that provided better pronation control and allowed for more comfortable medial arch
Otto Schuster created Roberts-Whitman Brace
Dudley J. Morton
Dudley Joy Morton (1884-1960) was physician, anatomist and anthropologist
Work focused on shortened 1st metatarsal, “hypermobility” of 1st metatarsal segment and correlation of 1st ray mechanics to excessive foot pronation
Published book, The Human Foot, It’s Evolution, Physiology and Functional Disorders, in 1935
Dudley J. Morton (1884-1960)
Morton Was First to Describe Load-Deformation of 1st Ray in 1935
“If the plantar ligaments of any segment are slack when the head of its metatarsal bone lies on the same plane as the others whose ligaments are taut, that segment will fail to share in the carriage of body weight….”
Morton DJ: The Human Foot: Its Evolution, Physiology and Functional Disorders. Columbia University Press. Morningside Heights, New York, 1935.
“…the plantar ligaments of the first metatarsal segment in these feet were lax when the other ligaments had become tense under body weight; hence the first metatarsal still retained a margin of dorsal extension and therefore was ineffective as a weightbearing structure.”
Morton DJ: The Human Foot: Its Evolution, Physiology and Functional Disorders. Columbia University Press. Morningside Heights, New York, 1935.
Morton believed “hypermobility of first metatarsal” affects foot in three ways:1. Second metatarsal has “increased burden”
since first metatarsal “fails to assume” its normal share of weight
2. Foot pronates because “medial buttress” is ineffective until “slack in its ligaments is taken up” as pronation increases
3. As pronation advances, “functional stresses are thrown increasingly on muscles on inner side of ankle, imposing them undue strain”
Morton DJ: Physiological considerations in the treatment of foot deformities. JBJS, 19:1052-1056, 1937.
Morton’s Compensating Insole
In 1932, Morton designed a “compensating insole” that focused on elevating first metatarsal head and preventing pronation compensation for short, “hypermobile” first ray
Morton also designed in-shoe support with high medial arch-flange to resist pronation
3/26/2015
6
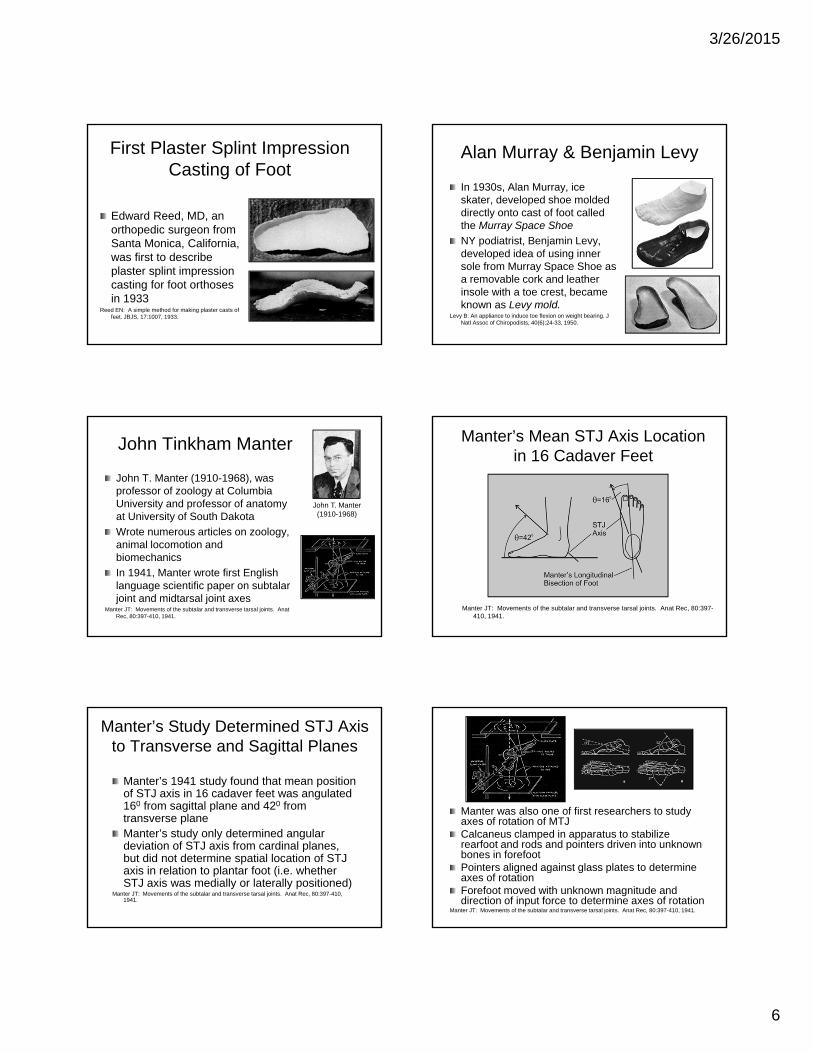
First Plaster Splint Impression Casting of Foot
Edward Reed, MD, an orthopedic surgeon from Santa Monica, California, was first to describe plaster splint impression casting for foot orthoses in 1933
Reed EN: A simple method for making plaster casts of feet. JBJS, 17:1007, 1933.
Alan Murray & Benjamin Levy
In 1930s, Alan Murray, ice skater, developed shoe molded directly onto cast of foot called the Murray Space Shoe
NY podiatrist, Benjamin Levy, developed idea of using inner sole from Murray Space Shoe as a removable cork and leather insole with a toe crest, became known as Levy mold.
Levy B: An appliance to induce toe flexion on weight bearing. J Natl Assoc of Chiropodists, 40(6):24-33, 1950.
John Tinkham Manter
John T. Manter (1910-1968), was professor of zoology at Columbia University and professor of anatomy at University of South Dakota
Wrote numerous articles on zoology, animal locomotion and biomechanics
In 1941, Manter wrote first English language scientific paper on subtalar joint and midtarsal joint axes
Manter JT: Movements of the subtalar and transverse tarsal joints. Anat Rec, 80:397-410, 1941.
John T. Manter (1910-1968)
Manter’s Mean STJ Axis Location in 16 Cadaver Feet
Manter JT: Movements of the subtalar and transverse tarsal joints. Anat Rec, 80:397-410, 1941.
Manter’s Study Determined STJ Axis to Transverse and Sagittal Planes
Manter’s 1941 study found that mean position of STJ axis in 16 cadaver feet was angulated 160 from sagittal plane and 420 from transverse planeManter’s study only determined angular deviation of STJ axis from cardinal planes, but did not determine spatial location of STJ axis in relation to plantar foot (i.e. whether STJ axis was medially or laterally positioned)
Manter JT: Movements of the subtalar and transverse tarsal joints. Anat Rec, 80:397-410, 1941.
Manter was also one of first researchers to study axes of rotation of MTJ Calcaneus clamped in apparatus to stabilize rearfoot and rods and pointers driven into unknown bones in forefootPointers aligned against glass plates to determine axes of rotationForefoot moved with unknown magnitude and direction of input force to determine axes of rotation
Manter JT: Movements of the subtalar and transverse tarsal joints. Anat Rec, 80:397-410, 1941.
3/26/2015
7
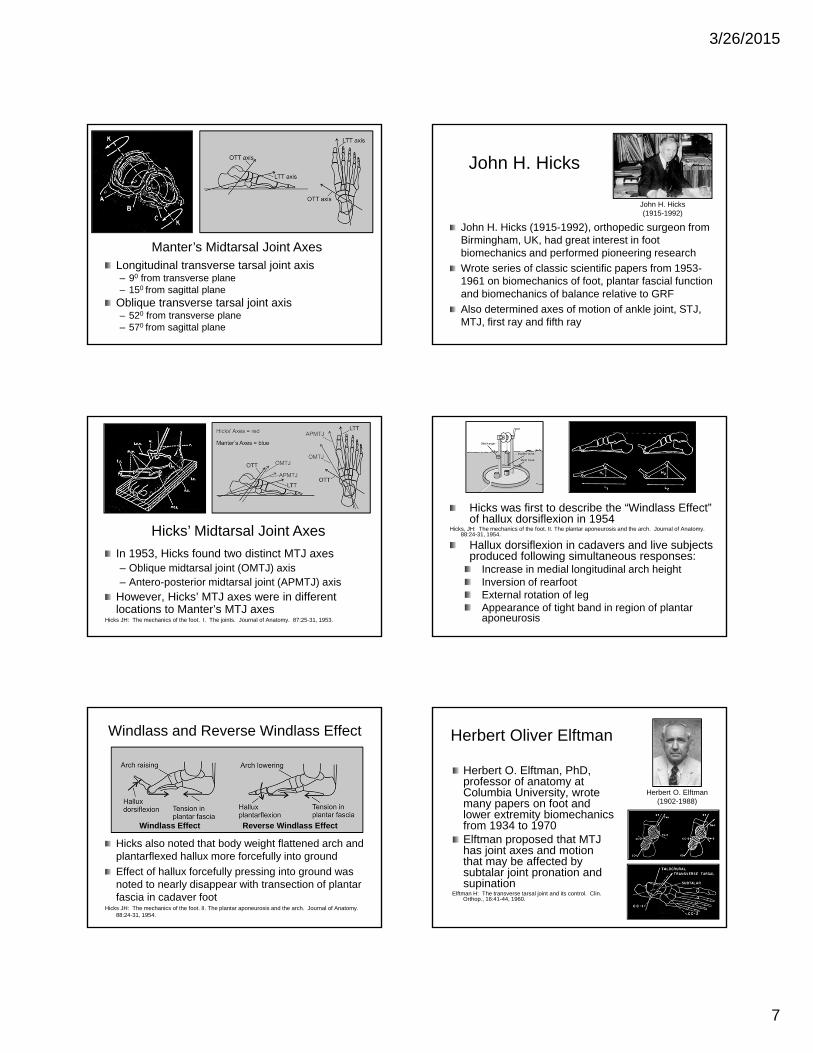
Longitudinal transverse tarsal joint axis– 90 from transverse plane– 150 from sagittal plane
Oblique transverse tarsal joint axis– 520 from transverse plane– 570 from sagittal plane
Manter’s Midtarsal Joint Axes
Oblique axis
Longitudinal axis
John H. Hicks
John H. Hicks (1915-1992), orthopedic surgeon from Birmingham, UK, had great interest in foot biomechanics and performed pioneering research
Wrote series of classic scientific papers from 1953-1961 on biomechanics of foot, plantar fascial function and biomechanics of balance relative to GRF
Also determined axes of motion of ankle joint, STJ, MTJ, first ray and fifth ray
John H. Hicks (1915-1992)
In 1953, Hicks found two distinct MTJ axes– Oblique midtarsal joint (OMTJ) axis– Antero-posterior midtarsal joint (APMTJ) axis
However, Hicks’ MTJ axes were in different locations to Manter’s MTJ axes
Hicks JH: The mechanics of the foot. I. The joints. Journal of Anatomy. 87:25-31, 1953.
Hicks’ Midtarsal Joint Axes
Hicks was first to describe the “Windlass Effect” of hallux dorsiflexion in 1954
Hicks, JH: The mechanics of the foot. II. The plantar aponeurosis and the arch. Journal of Anatomy. 88:24-31, 1954.
Hallux dorsiflexion in cadavers and live subjects produced following simultaneous responses:
Increase in medial longitudinal arch heightInversion of rearfootExternal rotation of legAppearance of tight band in region of plantar aponeurosis
Windlass and Reverse Windlass Effect
Hicks also noted that body weight flattened arch and plantarflexed hallux more forcefully into ground
Effect of hallux forcefully pressing into ground was noted to nearly disappear with transection of plantar fascia in cadaver foot
Hicks JH: The mechanics of the foot. II. The plantar aponeurosis and the arch. Journal of Anatomy. 88:24-31, 1954.
Windlass Effect Reverse Windlass Effect
Herbert Oliver Elftman
Herbert O. Elftman, PhD, professor of anatomy at Columbia University, wrote many papers on foot and lower extremity biomechanics from 1934 to 1970Elftman proposed that MTJ has joint axes and motion that may be affected by subtalar joint pronation and supination
Elftman H: The transverse tarsal joint and its control. Clin. Orthop., 16:41-44, 1960.
Herbert O. Elftman (1902-1988)

3/26/2015
8
Elftman thought that in the pronated foot major axis of TNJ (TN-1) was directly in line with CC-1:
“allows the forepart of the foot to move freely with respect to hindpart without movement of the talus with respect to the calcaneus”
Thought that MTJ axis changes in location as STJ rotates from pronated to supinated position:
“In passing from pronated to supinated position there is a continuous change in positions of significant joint elements and, consequently, of instantaneous transverse tarsal axis.”
Verne Thompson Inman
Verne T. Inman, MD, PhD (1905-1980) began to research lower extremity biomechanics in 1957 at UC Berkeley due to need for better prostheses in post-WW II amputees
His two books: The Joints of the Ankle and Human Walking are classics in foot and lower extremity biomechanics
Verne T. Inman (1905-1980)
Howard Davis Eberhart
Howard D. Eberhart was professor in civil engineering at UC Berkeley, when accident required BK amputation
Verne Inman, professor of orthopedic surgery at UC Berkeley, was surgeon that amputated Eberhart’s leg in 1944
In order to research lower limb biomechanics and develop better prosthesis designs, Eberhart teamed with Inman and became director of Prosthetics Devices Research Project at UC Berkeley Dept. of Engineering
Howard D. Eberhart (1906-1993)
UC Biomechanics Lab
UCBL was center of research in foot and lower extremity biomechanics and prosthetics research from 1957 to 1974 at UCSF and UC Berkeley
During its time, UCBL produced more research and notable researchers in foot and lower extremity biomechanics than any other in world
Dr. Verne Inman (center), Professor Howard Eberhart (right), and W.H. Henderson (in wheelchair) in Biomechanics Laboratory at U.C. Berkeley.
D. Gilbert Wright
Researcher at UC Biomechanics Lab who, in 1964, performed classic studies of range of motion of STJ during walking and on elastic properties of plantar fascia
Wright DG, Rennels DC: A study of the elastic properties of plantar fascia. JBJS, 46 (A):482-492, 1964.
Wright DG, Desai SM, Henderson WH: Action of the subtalar and ankle-joint complex during the stance phase of walking. JBJS, 46 (A): 361, 1964.
John B. Saunders
Chairman of Dept of Anatomy at UC Berkeley from 1938-1956
Coauthored classic article on determinants of gait, described how locomotion mechanisms minimize excursion of CoM during gait
Saunders JB, Inman VT, Eberhart HD: The major determinants in normal and pathological gait. JBJS, 35A:543-558, 1953.
John B. Saunders (1903-1991)
3/26/2015
9
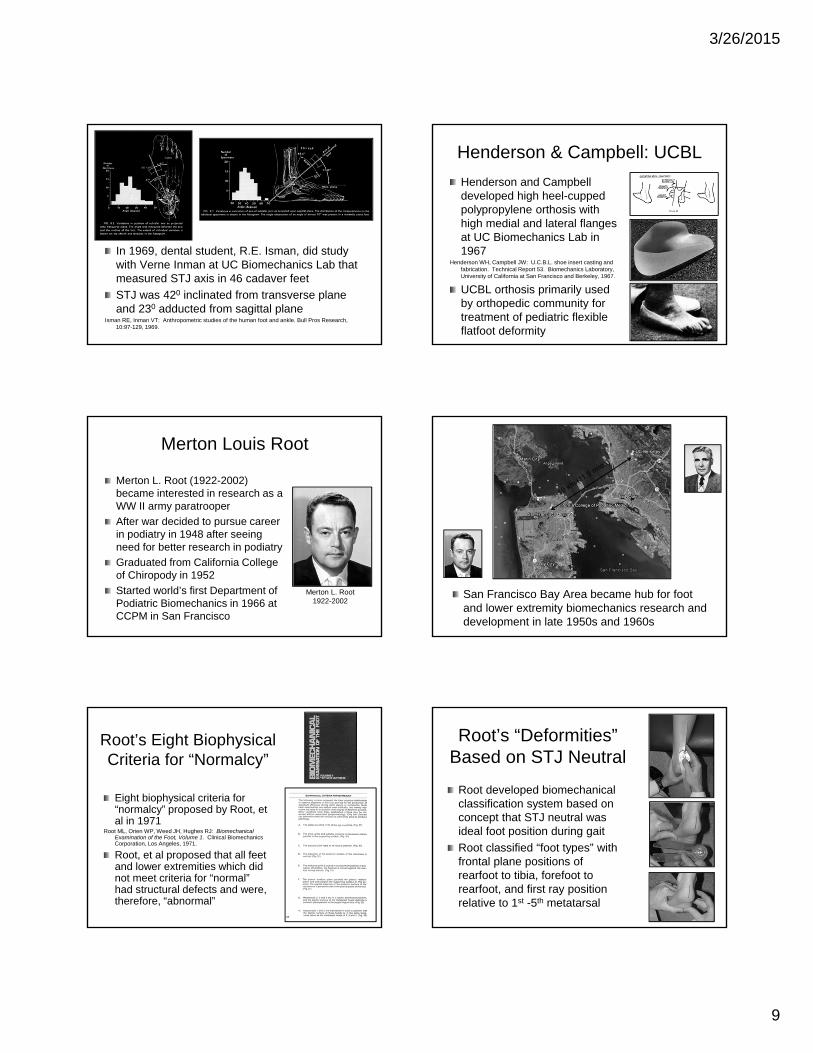
In 1969, dental student, R.E. Isman, did study with Verne Inman at UC Biomechanics Lab that measured STJ axis in 46 cadaver feet
STJ was 420 inclinated from transverse plane and 230 adducted from sagittal plane
Isman RE, Inman VT: Anthropometric studies of the human foot and ankle. Bull Pros Research, 10:97-129, 1969.
Henderson & Campbell: UCBL
Henderson and Campbell developed high heel-cupped polypropylene orthosis with high medial and lateral flanges at UC Biomechanics Lab in 1967
Henderson WH, Campbell JW: U.C.B.L. shoe insert casting and fabrication. Technical Report 53. Biomechanics Laboratory, University of California at San Francisco and Berkeley, 1967.
UCBL orthosis primarily used by orthopedic community for treatment of pediatric flexible flatfoot deformity
Merton Louis Root
Merton L. Root (1922-2002) became interested in research as a WW II army paratrooper
After war decided to pursue career in podiatry in 1948 after seeing need for better research in podiatry
Graduated from California College of Chiropody in 1952
Started world’s first Department of Podiatric Biomechanics in 1966 at CCPM in San Francisco
Merton L. Root 1922-2002
San Francisco Bay Area became hub for foot and lower extremity biomechanics research and development in late 1950s and 1960s
Root’s Eight Biophysical Criteria for “Normalcy”
Eight biophysical criteria for “normalcy” proposed by Root, et al in 1971
Root ML, Orien WP, Weed JH, Hughes RJ: Biomechanical Examination of the Foot, Volume 1. Clinical Biomechanics Corporation, Los Angeles, 1971.
Root, et al proposed that all feet and lower extremities which did not meet criteria for “normal” had structural defects and were, therefore, “abnormal”
Root’s “Deformities” Based on STJ Neutral
Root developed biomechanical classification system based on concept that STJ neutral was ideal foot position during gait
Root classified “foot types” with frontal plane positions of rearfoot to tibia, forefoot to rearfoot, and first ray position relative to 1st -5th metatarsal

3/26/2015
10
Root Developed “Neutral Suspension Casting Method”
In 1971, Root, Weed and Orien described “neutral suspension casting technique” with plaster splints to accomplish the following objectives:
Capture STJ in neutral position
Dorsiflex the 4th and 5th metatarsals
Pronate midtarsal joint to maximum to “lock” forefoot against rearfoot
Preserve NWB plantar contour of footRoot ML, Weed JH, Orien WP: Neutral Position Casting Techniques,
Clinical Biomechanics Corp., Los Angeles, 1971.
Root Functional Orthosis
Root was one of first to experiment with new materials called thermoplastics and began to develop his Root Functional Orthosis in 1958
RFO had lower MLA than previous orthoses since Root didn’t believe that high MLA or arch pain was necessary to control abnormal pronation
Root designed his RFO to allow the STJ to function in neutral position by preventing “compensation” for rearfoot and forefoot “deformities”
Root’s Lectures Notes Published by Sgarlato
Thomas E. Sgarlato, DPM, took over as chairman of world’s first Department of Podiatric Biomechanics from Root (due to illness) in 1969Sgarlato worked with podiatry students and biomechanics faculty to publish Root’s lecture notes as “A Compendium of Podiatric Biomechanics” in March 1971
Thomas E. SgarlatoNormal and Abnormal Function of the Foot, by Root, Orien and Weed in 1977, was foot and lower extremity biomechanics textbook
Text described normal and abnormal mechanics of foot and lower extremity, biomechanics of foot pathologies and how foot structure may predict foot function
John Herbert Weed (1938-1992)
William Phillip Orien
E.J. Van Langelaan
E.J. Van Langelaan, orthopedic surgeon in Netherlands, did first modern study on motions of STJ and MTJ in 1983 in his landmark PhD thesis using 3D xray photogrammetry
Performed under guidance of Antony Huson, PhD at University of Leiden, Netherlands
Van Langelaan EJ: A kinematical analysis of the tarsal joints. Acta Orthop Scand, 54:Suppl. 204, 135-229, 1983.
E.J. Van Langelaan
Apparatus Used in Van Langelaan Study
(Videos courtesy of A. Huson, MD, PhD)

3/26/2015
11
Thoughts from Van Langelaan“ ...intertarsal joints are not ‘complicatedly structured but functionally simple hinge joints’. Movements are found to take place around an axis which moves continuously, and the position of which could be approximated with the aid of a bundle of discrete helical axes.”“The relative axes within a bundle proved to approach each other more closely at characteristic sites in the tarsus.” TNJ: central portion of talar head, CCJ: dorsal-medial-superior corner of CCJ
Benno M. Nigg
Benno Nigg, trained as nuclear physicist, became interested in biomechanics in 1971
Founded and developed world’s largest biomechanics research facility at University of Calgary in 1981
Has authored/edited 10 books and has authored over 290 scientific papers on sports shoes and foot and lower extremity biomechanics
Benno M. Nigg
Howard J. Dananberg
Howard Dananberg popularized concept that functional hallux limitus was key to abnormal foot functionFnHL thought to produce “sagittal plane blockade“ during walking that caused pronation of foot as resultPatented “kinetic wedge” to address his theory of “sagittal plane blockade”
Dananberg, HJ: Gait style as an etiology to chronic postural pain. Part I. Functional hallux limitus. JAPMA, 83:433-441, 1993.
Howard J. Dananberg
Richard L. Blake
Richard Blake, a 1981 CCPM Biomechanics Fellowship graduate, developed the Blake Inverted Orthosis from 1981-1982
Blake RL, Denton J: Functional foot orthoses for athletic injuries. JAPMA, 75:359-362,1985.
Blake RL, Ferguson H: Foot orthosis for the severe flatfoot in sports. JAPMA, 81:549, 1991.
Blake RL: Inverted functional orthoses. JAPMA, 76:275-276, 1986.
Blake RL, Ferguson H: "The inverted orthotic technique:”, in Valmassy, R.L.(editor), Clinical Biomechanics of the Lower Extremities, Mosby-Year Book, St. Louis, 1996.
Richard Blake
Blake Inverted Orthosis
As Dr. Blake developed his BIO, he discovered that increasing levels of cast inversion increased pronation control from his inverted orthosis due to increased MLA height and inverted heel cup
However, as cast inversion approached 100, Dr. Blake noted new orthosis problems:– Plantar fascial irritation
– Foot slid laterally off of orthosis plate
– Excessive orthosis arch height caused late midstance pronation, instead of late midstance supination, during walking
Blake Inverted Orthosis
Positive cast of BIO inverted 15, 25 or 350 which causes varus heel cup and higher medial arch to orthosis
Modified medial arch fill and plantar fascial accommodation are added to prevent plantar fascial irritation
Heel cups of 20 mm and flat rearfoot posts are standard

3/26/2015
12
New Research on STJ Axis Location Emphasized STJ Kinetics
In 1987, concept that STJ axis location may be determined clinically and that GRF medial to STJ axis causes supination moments and GRF lateral to axis causes STJ pronation moments was first introduced
Kirby KA: Methods for determination of positional variations in the subtalar joint axis. JAPMA, 77: 228-234, 1987.
In 1989, concept of rotational equilibrium used to explain how balance of STJ moments may explain abnormal internal forces within foot and different types of foot pathology
Kirby KA: Rotational equilibrium across the subtalar joint axis. JAPMA, 79: 1-14, 1989.
In 1992, medial heel skive technique, was first described as method to increase varus shape of heel cup in functional foot orthosis
Designed to increase STJ supination moment from orthosis and more effectively treat symptoms caused by excessive pronation moments such as PTTD and children’s flatfoot deformity
Kirby KA: The medial heel skive technique: improving pronation control in foot orthoses. JAPMA, 82: 177-188, 1992.
In 2001, new theory of foot function, Subtalar Joint Axis Location and Rotational Equilibrium (SALRE) Theory was first introduced
Described how concepts of STJ axis spatial location and rotational equilibrium may be combined to explain many observations relating to biomechanical function
Also offered explanation for biomechanical effect of certain foot surgeries
Kirby KA: Subtalar joint axis location and rotational equilibrium theory of foot function. JAPMA, 91:465-488, 2001.
SALRE Theory Explains How Orthoses Alter STJ Moments
If orthosis is designed to “control pronation”, ORF will be shifted medially so STJ supination moment is increasedIf orthosis is designed to “control STJ supination”, then ORF will be shifted laterally so STJ pronation moment is increased
Kirby KA: Subtalar joint axis location and rotational equilibrium theory of foot function. JAPMA, 91:465-488, 2001.
ORFORF
ORFORF
As STJ axis becomes medially deviated, orthosis has decreased area medial to STJ axis to cause STJ supination momentsMedial deviation of STJ decreases orthosis ability to supinate STJ
Child with Flatfoot Deformity
Supination Area of Foot Orthosis
Normal STJ Axis Location
Supination Area of Foot Orthosis

3/26/2015
13
Tissue Stress Model
Tissue stress model first proposed as a model for mechanical foot therapy in 1995 by McPoil and Hunt
McPoil TG, Hunt GC: Evaluation and management of foot and ankle disorders: Present problems and future directions. JOSPT, 21:381-388, 1995.
Tissue stress model is not a novel idea since it is based on same ideas are already in current use in treatment of parts of body other than foot and lower extremity Tissue stress model doesn’t rely on “unreliable measurement techniques”
Thomas G. McPoil
Gary C. Hunt
Tissue Stress Model
Tissue stress model and its clinical applications have been discussed by other authors as a clinical method by which to more effectively prescribe custom foot orthoses
Fuller EA: Center of pressure and its theoretical relationship to foot pathology. JAPMA, 89 (6):278-291, 1999.
Fuller EA: Reinventing biomechanics. Podiatry Today, 13:(3), December 2000.Kirby KA: Tissue stress approach to mechanical foot therapy. Precision Intricast Newsletter,
February 2002.Kirby KA: The biomechanics of tissue stress. Precision Intricast Newsletter, Payson, Arizona,
March 2002.Kirby KA: Using the tissue stress approach in clinical practice. Precision Intricast Newsletter,
April 2002.
Tissue Stress Allows Efficient Determination of Orthosis Goals
Orthosis goals are best achieved by specifically designing CFO to :– reduce stress on injured structural components
within foot and lower extremity– optimize function of foot and lower extremity for
specific weightbearing activities– prevent other injuries or pathologies from
occurring due to foot orthosis therapy
Steps to Using Tissue Stress
1. Specifically identify anatomical structures which are source of patient’s complaints
2. Determine structural and/or functional variables which may be source of pathological forces on injured structures
3. Design orthosis/shoe treatment plan which will most effectively reduce pathological forces on injured structural components, will optimize gait function and will not cause other pathology or symptoms
Paul Robert SchererPaul Scherer, DPM, is former professor of biomechanics at CCPM and current professor of biomechanics at CSPM
Scientific chair for first ten PFOLA Conferences which were world-class international events that presented latest knowledge in biomechanics and foot orthosis therapy
His book “Recent Advances in Orthotic Therapy” is premier educational resource detailing scientific research evidence for orthosis therapy
Benno Nigg’s Preferred Movement
Pathway Model
In 2001, Benno Nigg proposed “preferred movement pathway model” of orthosis functionNigg proposes that orthoses do not function by realigning skeleton but rather alter input signals into plantar foot that change “muscle tuningNigg proposed that if foot orthosis counteracts preferred movement path, then muscle activity will increase and that optimal shoe or foot orthosis design will reduce or minimize muscle activity
Nigg BM: The role of impact forces and foot pronation: a new paradigm. Clin J Sport Med, 11:2-9,2001.

3/26/2015
14
Chris Nester
Chris Nester, first a podiatrist then a PhD in biomechanics, became foot biomechanics researcher at University of Salford, UK
Along with coworkers, Nester has performed important pioneering bone pin research in kinematics of foot joints in both cadaver and live feet
Chris Nester Nester and coworkers were first to suggest that previous model of simultaneously occurring oblique and longitudinal MTJ axes can not occur and should be replaced by a single moving MTJ axis
Simple concept described by Nester et al is very important for understanding MTJ biomechanics: “axes of rotation do not determine the motion at a joint; rather, the motion determines the axis”
Nester CJ, Findlow A, Bowker P: Scientific approach to the axis of rotation of the midtarsal joint. JAPMA, 91(2):68-73, 2001.
Also proposed three “reference axes” for MTJ:– Medial-lateral MTJ axis (z-axis)– Anterior-posterior MTJ axis (x-axis)– Vertical MTJ axis (y-axis)
Nester CJ, Findlow AH: Clinical and experimental models of the midtarsal joint. Proposed terms of reference and associated terminology. JAPMA, 96:24-31, 2006.
Important Coworkers Have Further Developed STJ Theory
Eric Fuller, introduced concept that CoP position relative to STJ axis can be used to predict how different tissues will be stressed
Fuller EA: Center of pressure and its theoretical relationship to foot pathology. JAPMA, 89 (6):278-291, 1999.
Co-developed concept of STJ axis/tissue stress approach to biomechanical therapy
Fuller EA, Kirby KA: Subtalar joint equilibrium and tissue stress approach to biomechanical therapy of the foot and lower extremity. In Albert SF, Curran SA (eds): Biomechanics of the Lower Extremity: Theory and Practice, Volume 1. Bipedmed, LLC, Denver, 2013, pp. 205-264.
Eric Fuller
Simon Spooner, PhD, developed STJ axis locator and promoted analyzing orthosis function with FEA
Spooner SK, Kirby KA: The subtalar joint axis locator: A preliminary report. JAPMA, 96:212-219, 2006.
Craig Payne and coworkers showed correlation of STJ axis location to supination resistance
Payne C, Munteaunu S, Miller K: Position of the subtalar joint axis and resistance of the rearfoot to supination. JAPMA, 93(2):131-135, 2003.
Javier Pascual Huerta, PhD and coworkers demonstrated how max pronated STJ position affects foot resistance to supination with orthoses
Pascual Huerta J, Ropa Moreno JM, Kirby KA: Static response of maximally pronated and nonmaximally pronated feet to frontal plane wedging of foot orthoses. JAPMA, 99:13-19, 2009.
Simon Spooner
Craig Payne
Javier Pascual Huerta
Future for Foot and Lower Extremity Biomechanics and Orthoses?
Key to developing better understanding of gait function and pathologies will be dependent on research that determines forces and moments acting on foot and lower extremity
Research into new orthosis designs to reduce abnormal forces and moments causing certain pathologies will be important for further progress
Better understanding of biological and mechanical nature of human tissues will also be critical to developing better treatment methods

3/26/2015
15
Biomechanics and Historical Sources
W. Eric Lee: Podiatric Historian from UKLee W E: Merton L. Root: An appreciation. The Podiatric Biomechanics Group
Focus. 2(2): 32-68, 2003.
Richard O. Schuster: Podiatrist from US (nephew of Otto N. Schuster)
Schuster RO: A history of orthopedics in podiatry. JAPA, 64(5):332-345, 1974.
Benno Nigg: Biomechanics ResearcherNigg BM: “Selected historical highlights”, in Biomechanics of the Musculo-skeletal
System, 2nd Edition, (B.M. Nigg and W. Herzog, eds), John Wiley and Sons, New York, 1999, pp. 3-35.
William Eric Lee
Richard Schuster
Benno Nigg
Conclusion
History demonstrates that foot and lower extremity biomechanics theory and foot orthosis treatments have all evolved over time
Many individuals have made contributions towards better understanding of lower extremity function and treating foot and lower extremity mechanical pathologies with orthoses
Examples of those that changed history in foot-health professions show that advances in knowledge require sacrifice, determination and hard work