Hip, Pelvis and Thigh : Anatomy, Evaluation. BONY ANATOMY.
56
Hip, Pelvis and Hip, Pelvis and Thigh : Thigh : Anatomy, Evaluation Anatomy, Evaluation
-
Upload
jonah-mccoy -
Category
Documents
-
view
239 -
download
1
Transcript of Hip, Pelvis and Thigh : Anatomy, Evaluation. BONY ANATOMY.

Hip, Pelvis and Thigh : Hip, Pelvis and Thigh : Anatomy, EvaluationAnatomy, Evaluation

BONY ANATOMYBONY ANATOMY




Hip Capsule LigamentsHip Capsule Ligaments
Iliopsoas bursa




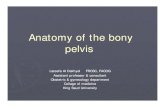
Hip - AnatomyHip - Anatomy
Multiaxial ball & socket jointMultiaxial ball & socket joint AcetabulumAcetabulum
1/2 sphere1/2 sphere Femoral headFemoral head
2/3 sphere2/3 sphere Strong ligaments & capsuleStrong ligaments & capsule Maximally stableMaximally stable




ObservationObservation
GaitGait PosturePosture BalanceBalance Limb positionLimb position
shortened, adducted, medially rotatedshortened, adducted, medially rotated abducted, laterally rotatedabducted, laterally rotated shortened, laterally rotatedshortened, laterally rotated
Leg shorteningLeg shortening

InspectionInspection
Pelvic unleveling (iliac crest levels)Pelvic unleveling (iliac crest levels) Pelvic rotation (PSIS levels)Pelvic rotation (PSIS levels) If asymmetric, measure leg lengthsIf asymmetric, measure leg lengths

Leg Length MeasurementsLeg Length Measurements
Eyeball methodEyeball method Measurement methodMeasurement method


Range of MotionRange of Motion
Flexion: 110 to 120 Flexion: 110 to 120 degreesdegrees
Extension: 10 to 15 Extension: 10 to 15 degreesdegrees

Abduction: 30 to 50 Abduction: 30 to 50 degreesdegrees
Adduction: 30 Adduction: 30 degreesdegrees

External rotation: 40 External rotation: 40 to 60 degreesto 60 degrees
Internal rotation: 30 Internal rotation: 30 to 40 degreesto 40 degrees

ExaminationExamination
Strength testingStrength testing isometricisometric eccentriceccentric knee extensionknee extension knee flexionknee flexion

Hip Flexion StrengthHip Flexion Strength
Iliopsoas, rectus femoris, sartorius, tensor fascia lata, pectineus

Hip Extension StrengthHip Extension Strength
Hamstrings, gluteus maximus

Hip Adduction StrengthHip Adduction Strength
Adductor longus, adductor brevis, adductor magnus, gracilis, pectineus, oburator externus

Hip Abduction TestingHip Abduction Testing
Gluteus medius, gluteus minimus, tensor fascia lata

Internal Rotation Internal Rotation StrengthStrength
Gluteus medius, gluteus minimus, tensor fascia lata

External Rotation External Rotation StrengthStrength
Piriformis, Obturator internus & externus, Superior/inferior Gemelli, Quadratus femoris, Gluteus maximus

Special TestsSpecial Tests
Patrick’s TestPatrick’s Test(FAbER)(FAbER) hip joint hip joint SI jointSI joint

Gaenslen’s SignGaenslen’s Sign
Pain at ipsilateral SIJ is positive test

Special TestsSpecial Tests
modified Thomas Testmodified Thomas Test hip flexor and quad flexibilityhip flexor and quad flexibility

Special TestsSpecial Tests
Ober TestOber Test iliotibial band flexibilityiliotibial band flexibility

Special TestsSpecial Tests
Piriformis TestPiriformis Test Piriformis flexibility or Piriformis flexibility or
painpain

Special TestsSpecial Tests
Popliteal AnglePopliteal Angle Hamstring flexibiltyHamstring flexibilty


Special TestsSpecial Tests
Labral InjuryLabral Injury FAdAxL: FAdAxL: flexion, flexion,
Adduction, Axial Adduction, Axial Load + some IR/ERLoad + some IR/ER pain +/- clickpain +/- click

Weber-Barstow Maneuver
*Can measuretrue vs. apparent

Gross Leg Length Discrepancy
Magee 4th
Edition – pg. 628

Prone Knee Flexion Test for Tibial Shortening
Magee 4th
Edition - pg. 630

Thomas Test
3 Muscle Kendall testAs above….but also look at….IP = hip flexor and hip ERRF = hip flexor and knee extensorTFL/ITB = hip flexor and hip abductor
Magee - 4th Edition

Ely’s Test
Prone, passive knee flexion
Positive for RF tightness if pelvic anterior tilting / hip flexion accompanies knee flexion before end range and if asymmetrical in bilateral comparison
Magee 4th Edition

FAIR Test
Cleland, J. – Orthopedic Clinical Examination
Fishman et. al (2002) Archives of Physical Medicine – 10 yr. PiriformisstudySen. .88Spec. .83+LR= 5.2-LR=.14
(+) = pain atintersection ofsciatic nerveand piriformis

Ober Test
Magee 4th Edition – pg. 633
Reese and Bandy (2003) JOSPTOber Test
Modified Ober Test (4-50 > Ober test)
Ober
ICC=.90
Modifie
d Ober
ICC=.91

Leg Length Tests
True Leg Length Discrepancy Measure ASIS to
medial malleolus Positive = 1-1.5 cm
Apparent (Functional) Leg Length Umbilicus to Medial
malleolus

Trendelenberg Test
Pt Position = standing on one leg with WB leg being the involved limb
Positive = pelvis on opposite side drops
Indications = weak Gluteua medius

Kendall Test
Pt Position = supine with knees bent over the table
Evaluation One hand under lordotic
curve Passively flex hip to chest Allow opposite leg to rest
on table Positive = knee move
into extension or leg rises off table

Thomas Test
Pt Position = supine with both leg on table
Evaluation One hand under lumbar
region Passively flex one leg to
chest
Positive = straight leg raises off table Increased lordotic curve

Measurements
True leg length Measure from A.S.I.S
to inferior border of medial malleolus

Measurements
True Shortening In true shortening the affected
limb is physically shorter than the other and this may be caused by pathology proximal or distal to the trochanters.
True shortening from causes distal to the trochanters most frequently results from previous fractures of the femur or tibia or growth disturbance (e.g. from polio or epiphyseal trauma). Proximal to the trochanters causes include femoral neck fractures, OA and hip dislocation.

Measurements
Apparent leg length Measure from tip of xiphoid
process to inferior border of medial malleolus
Apparent Shortening In apparent shortening the
limb is not altered in length, but appears shortened. This may be as a result of an adduction contracture of the hip joint, which has to be compensated for by tilting of the pelvis, or SIJ pathology causing pelvic rotation.

MovementExpected Range of Movement Flexion: 0-130
Degrees Abduction: 0-45 Degrees Adduction: 0-30 Degrees MR: 0-45 Degrees LR: 0-60 Degrees Extension: 0-20 Degrees

Movements
Thomas’ test:• Place your left hand in hollow of lumbar spine• Flex hip and knee of unaffected side • Look to see if hip of the affected side lifts
from bed Flexion:• Flex hip and knee of affected side and note
ROM (130°)

Movements
Abduction:
• Stabilise pelvis and hold ankle with other hand
• Abduct and note ROM (45°)
Adduction:
• As above and note ROM (30°)

Movements
Rotation:• Flex hip and knee to 90 degrees, externally
and internally rotate• Note ROM (45°)
Abnormal Movement (telescoping):• Alternately push and pull leg along its long
axis – demonstrates marked instability

Trendelenberg Test
Used to assess the ability of the hip abductors to stabilise the pelvis on the femur.
A positive test demonstrates that the hip abductors are not functioning.
Causes:• Disturbance in pivotal mechanism – dislocation
or subluxation of hip, shortening of femoral neck• Weakness of the hip abductors e.g. myopathy,
neuropathy

Trendelenberg Test
The test is performed with the patients back to the examiner. The model stands on the normal leg and flexes the knee of the other leg to a right angle.
The pelvis should remain level or tilt slightly upwards on the unsupported side.
The model then stands on the affected leg and flexes the knee of the other leg.
If the pelvis tilts downwards on the unsupported side, then this confirms a positive Trendelenberg sign.

Trendelenberg Test