Group3zpresentationmacysjcpenney 13317479695627-phpapp01-120314130426-phpapp01
Upload
linderendieCategory
view
212download
0description

By Dr Rubzzz

Inguinal Canal 3.75cm long directed downwards and medially
from the deep to superficial inguinal ring.Just above the medial half of inguinal ligament.
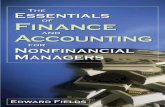
The inguinal canal can be thought of as a tunnel that travels from an "entrance", which is lateral and deep, to an "exit", which is medial and superficial. It, like a tunnel, also has a roof, a floor, and two walls.
Or pathway for the spermatic cord in males +
ilioinguinal Nerve or round ligament of the uterus + ilioinguinal nerve in females

Entrance- deep inguinal ring in the transversalis fascia (U-shape). Lies 1.25cm above the inguinal ligament.
Exit- superficial inguinal ring ,slitlike opening in the external oblique aponeurosis.Lies 1.25cm above the pubic tubercle
Roof -fibers of internal abdominal oblique ,transversus abdominis muscles and medial crus of external oblique muscle
Floor – inguinal ligament throughout, with lacunar ligament (Gimbernat's ligament) added medially and iliopubic tract
Anterior wall- external abdominal oblique aponeurosis throughout, with internal abdominal oblique aponeurosis added laterally and superficial inguinal ring
Posterior wall - mostly transversalis fascia, with conjoint tendon (falx inguinalis/Henle's ligament) which is the joining of internal abdominal oblique and transversus abdominis aponeuroses, medially.and deep inguinal ring


Inguinal Triangle (of Hesselbach)
1. Medially: lateral edge of rectus abdominis (linea semilunaris)
2. Laterally: inferior epigastric artery
3. Inferiorly: inguinal ligament (Poupart’s ligament)
the weak fascia, where direct hernias occur, is located in the inferior portion of this triangleIndirect Hernias protrude lateral to Hesselbach's Triangle.

Blood supply and Nerve innervation
Artery – Inferior Epigastric (lie posteriorly and medially to deep inguinal ring)
Vein – Inferior Epigastric Nerve – Ilioinguinal and Iliogastric
During an open hernia repair, careful dissection of the ilioinguinal nerve is important for two reasons.
1. Because of the nerve distributions cited above, injury during incision or closure can result in pain following the L1 dermatome (including the scrotum or labium majorum).
2. Because the ilioinguinal nerve has motor distributions to the internal oblique (which are inserted into the lateral border of the conjoint tendon), division of the nerve paralyzes these muscle fibers, weakening the conjoint tendon, which can precipitate a direct inguinal hernia.

Spermatic cord The classic description of the contents
of spermatic cord in the male are: 3 arteries: artery to vas deferens (or
ductus deferens), testicular artery,cremasteric artery;
3 fascial layers: external spermatic, cresmasteric and internal spermatic fascia;
3 other structures: pampiniform plexua, vas deferens(ductus deferens), testicular lymphatics;
3 nerves: genital branch of the genitofemoral nerve (L1/2), autonomic and visceral afferent fibres, ilioinguinal nerve (
The ilioinguinal nerve passes through the superficial ring to descend into the scrotum, but does not formally run through the canal.

Inguinal hernia “Affect 9% of men and 1% of female but it is more common
in female compare to femoral hernia” - (Browse’s introduction to the symptoms and sign of surgical disease 4th edition)
Classification Direct ,Indirect Congenital , Acquired (by causes). Complete , Incomplete, Bubonocele (type of indirect inguinal hernia) Enterocle, Epiplocele/ Omentocele, Cystocle (content of hernia) Special type :1. Pantaloon hernia ( Direct and indirect in the same groin) – two sacs
by the inferior epigastric artery2. Sliding hernia –Extraperitoneal bowel (cecum/terminall ileum on the
Rt and sigmoid colon on the Lt) which slides down into the inguinal canal, pulling a sac of peritonuem on its surface
3. Maydl’s hernia –two loops of bowel in the sac with the strangulation of the loop of bowel in the abdomen which connects them.
Clinically : Reducible, Irreducible, Obstructed/Incarcerated, Strangulated, Inflamed

Etiology Wall defect – weakness of the anterior wallEx:Omphocele and Gastroschisis Embriogenic defect – EX: Patent Processus Vaginalis and Patent canal of
Nuck in Female Increased intraabdominal pressure Pregnancy Heavy lifting Excessive weight Straining during bowel movement or urination Chronic coughing or sneezing Smoking Damage to ilioinguinal nerve due to previous
appendectomy

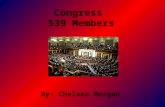
Inguinal Hernia Direct IH- Enter the inguinal canal
through the medial half of its weak posterior wall (through Hesselbach’s triangle) to the inferior epigastric artery and then protruded out from the superficial inguinal ring separate from the spermatic cord.
Indirect IH- Comes out of the abdomen
cavity through out the deep inguinal ring,travel along the inguinal canal and then protruded out from the superficial inguinal ring
- descends along the spermatic cord in males or the round ligament in females.
Congenital; through patent processus vaginalis
Acquired: passes through deep inguinal ring initially, i.e lateral to the inferior epigastric artery and exits through the superficial ring.

It is not always possible to distinguish clinically between a direct and indirect inguinal hernia
Direct Inguinal Hernia Indirect Inguinal Hernia
In older men. These hernias never occur in females.All Acquired Common in young men. Congenital and acquired
Lies posteriomedial to the spermatid cord Lies anterolateral to the spermatid cord
Wider Neck and lies medial to inferior epigastric artery.Uncommon to reach down into the scrotum, and its generally smaller. Common to bulge forward. They are often bilateral in the older person.
Narrow Neck and lies lateral to inferior epigastric artery
Bulge from the Hesselbach triangle Descend through deep inguinal hernia
Cough impulse :usually not increased in size Cough impulse: increased in size
Weakness anterior wall. Mostly do not descend the scrotum Patent Processus vaginalis. The persistence of the processus vaginalis sac at birth associated with and following the descent of the testis
Easy to reduce Difficult to reduce
Less chance of strangulation Generally indirect herniae should be surgically repaired because they become larger, cause symptoms and may obstruct and strangulate. Especially in children


Processus vaginalis is an embrogenic developmental outpouching of the peritoneum
Gubernaculum -are embryonic structures which begin as undifferentiated mesenchyme attaching to the caudal end of the gonads (testes in males and ovaries in females).
Congenital Inguinal Hernia

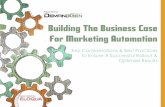
• An obvious bulge at the internal or external ring or within the scrotum. The parents typically provide the history of a visible swelling or bulge, commonly intermittent, in the inguinoscrotal region in boys and inguinolabial region in girls. The image shows depicts a 4-month-old baby boy with a large right-sided indirect inguinal hernia.
• The swelling may or may not be associated with any pain or discomfort. The parents may perceive the bulge as being painful when, in truth, it causes no discomfort to the patient.
• The bulge commonly occurs after crying or straining and often resolves during the night while the baby is sleeping.
• Indirect hernias are more common on the right side because of delayed descent of the right testicle. Hernias are present on the right side in 60% of patients, on the left in 30%, and bilaterally in 10% of patients.
• If the patient or the family provides a history of a painful bulge in the inguinal region, one must suspect the presence of an incarcerated inguinal hernia. Patients with an incarcerated hernia generally present with a tender firm mass in the inguinal canal or scrotum. The child may be fussy, unwilling to feed, and inconsolably crying. The skin overlying the bulge may be edematous, erythematous, and discolored.

Sign and symptoms an inguinal hernia either may not cause any symptoms or may
cause only a feeling of heaviness or pressure in the groin. Symptoms are most likely to appear after standing for long periods, or when you engage in activities that increase pressure inside the abdomen, such as heavy lifting, persistent coughing or straining while urinating or moving the bowels.
As the hernia grows, it eventually causes an abnormal bulge under the skin near the groin. This bulge may become increasingly more uncomfortable or tender to the touch.
In strangulated type: severe pain will occur so must do give immediate treament. Cx: Necrosis due to blood supply cut.
In obstructed type: cardinal symptoms of intestinal obstruction (colicky pain in abdomen, vomiting, abdominal distension and absolute constipation)

Examination Position:Ask Pt to stand .Dr sit Size/shape : Indirect (pyriform with a stalk at the external inguinal ring.Usually
extend down to scrotum) Direct (spherical and little tendency to enter into scrotum) Position of penis: Large hernia push the penis to other side Skin colour :Normal,Red(inflammed or strangulated). Longer term of truss
usage – discolouration and streaks of hyperpigmentation due to deposition of hemosiderin). Scar in previous operation.
Temperature : Normal or warm (strangulated/Inflamed) Composition: Gut (soft,resonant,bowel sound and fluctuant), Bowel
( resonant,hard ,tense and fluctuant), Small intestine ( Visible peritalsis, large scrotal hernia), Omentum ( firm like rubber, non –fluctuant and dull to percussion)
Tenderness : Manual pressure is uncomfortable but not painful. Pain (strangulated, Inflamed)
Reducibility: No painful but sometime with excessive pressure can cause pain. Cough impulse: Most lumps in the groin moves up and down with coughing
but in hernia, it expand in all direction.

Gentle continuous pressure on the hernial mass towards the inguinal ring is generally effective (Trendelenburg)

Management
Plan for surgery after routine investigation
Investigation- FBC – TWC, HB- Blood sugar, urea and creatinine- Urine for routine examination- CXR PA view- ECG

SurgicalIndirect inguinal herniaInguinal herniotomy (disect out and opening the hernial sac,reducing any content and then transfixing the neck of the sac and removing the remainder) +- with herniorrhaphyProcedure: 1.Excision of the hernial sac2.Repair of the strecthed internal inguinal ring and the transversalis fascia3.Reinforcement of posterior wall of inguinal canal

Direct Inguinal herniaShouldice (Canadian) repair
Utilizes a multi-layered imbricated repair of the inguinal canal floor where ring and fascia are incised and carefully separated from the deep inferior epigastric vessels and ectraperitoneal fat before an overlapping repair (double breasting) of the lower flap behind the upper flap

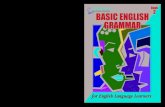
Lichtenstein (tension-free) RepairOne of the most commonly performed
proceduresThe tails of mesh are overflapped and
crossed and single is placed to create a new “internal “ ring
A Marlex mesh patch is sutured over the defect with a slit to allow passage of the spermatic cord

Lichtenstein Repair

McVay (Cooper’s ligament) RepairIs for the repair of large inguinal hernias, direct
inguinal hernias, recurrent hernias and femoral hernias
The conjoined tendon is sutured to Cooper’s ligament from the pubic cubicle laterally

Laparoscopic hernia repair-Current techniques include
○ Transabdominal preperitoneal repair (TAPP)○ Totally extraperitoneal approach (TEPA)○ TAPP- pneumoperitoneum and places a synthetic
mes preperitoneally by dissecting the perionuem off the hernial orifices and positioning the mesh beneath the peritoneum before closing.
○ TEPA-completely periperitoneal. Used in any inguinal hernia, unilateral, recurrent or bilateral hernia, and femoral hernia



Strangulated Hernia – EMERGENCY OPPreop: resuscitate with adequate fluid,empty the stomach with NG tube, Gv antibiotic to contain infection and catherize to monitor hemodynamic stateInguinal herniotomy:incision on the prominent part of swelling.

Femoral Hernias
More common in females than in males Through a space bounded by the
ileopubic tract Demonstrated by a mass below the
inguinal ligament

Femoral Canal 1.25cm in long and 1.25cm wide at its base,directed
upwards.Occupied most medial compartment of femoral sheath and extends from femoral ring above the saphenous opening.
Anterior – Inguinal ligament Posterior- iliopectineal ligament, pubic bone and
fascia over Pectineus Muscle Medial – Lacunar ligament and prolonged along the
iliopectineal ligament Lateral – thin septum separating it from the femoral
veinSpace – Loose areolar tissue and lymph gland (Gland
of Cloquet)


Clinical features Common in right side twice more than left
side.Occasionally Bilateral Rare in children. Common in age 50.More
common in Female than man Sign and symptoms similar to Inguinal hernia Rarely large sac present 40% presented with strangulation Richter’s Hernia – intestinal obstruction Thick walled with layer of fat and CT, cut cross
look like onion Cannot control by truss Urgent operation due to strangulation.

Surgical Lockwood (low operation)-sac dissect out below the inguinal ligament via groin
crease incision. Peel off all the anatomical layers that cover the sac, deal with content. Then pull down the neck of sac and ligate as high as possible and allow to retract through femoral canal. Close the canal by suturing to inguinal ligament to iliopectineal line.
McEvedy (high operation) Lotheissen (inguinal operation)- Open the inguinal canal by inguinal herniorrhaphy.
Tranversalis fascia is incised to medial side of peigastric vessel and enlarged the opening. Open peritoneum,withdraw sac from femoral canal.Deal with the content. Suture the conjoined tendon to the iliopectineal line to form a shutter

Umbilical hernia Congenital (exomphalos) 1 in 6000 births due to failure of all or part of midgut to return to the coelom during the early fetal life
Age: Hernia wont be noticed till the umbilical is separated and healed.Noticed after some months
Common in Afro- Carribean race Symptoms: Swelling, others are rare. Sometime parental anxiety
or intestinal obstruction Examination : hemispherical shape,overlie and easy to palpate
on the abdominal Size can be 0.5cm – 10cm) Composition: Soft, compresibble, and reducible.usually contained bowel and resonant to percussion.Cough impulse invariable

Omphocele (contain organ outside the abdomen) More common
Gastroschisis (umblical cord is not involved and usually at right mid.)

In adult:acquired ( due to defect to umbilical cicatrix)True umbilical herniaSecondary to intraabdominal pressure, pregnancy and ascitesP/E: Distended abdomen

Management Non-opFor premature infant with gigantic intact sac. Daily apply with desiccating
antiseptic solution.If successful,an eschar forms over the sac.Once the granulisation tissue grow- ventral hernia can be repaired later age.
Skin flap closure-sace is gently trimmed.The skin is freed from the fascial edges and
undermined laterally.Ligate the umbilical vessel for monitoring. Put skin flap at midline with simple sutures and ventral hernia closed later
Primary closure-sac dissect away from skin edge and fascia,evacuate the intestinal fully
from meconium,fluid and etc through NG tube.Strect abdominal wall gradually to double the volume.Then replace the viscera and close the fascia layer under moderate tension.
Herniorrhaphy after 2 years Op-small curved incision immediately below the umbilicus. The sin cicatrix is
dissected upwards and the neck of the sac isolated.Once the sac is empty,either invert it into abdomen or ligate by transfixation and excised.

Paraumbilical hernia Common acquired umbilical hernia. Common in mid age and old age.Common in women and men
especially in parous and obese women Defect that is adjacent to the umbilical scar Does not bulge into the centre of umblicus and not attach to the centre
of sac Symptoms: Discomfort and swelling, pain worsen by prolong standing
and sternous exercise Strangulated type contain extraperitoneal fat or omentum. Normally
bowel is not obstructed P/E: bulge at beside umbilicus (pushed one side and stretched into a
cresent shape)maybe infected with foul smelling discharge ,collection of dried- up sebacuoes secretion)
Smooth surface and edge is easy to define Composition : firm, usually contain omentum .if contain bowel,(soft and
resonant). Reducible Expansile cough impulse

Treatment If untreated, hernia will increase in size and strangulation
can occur. Indication: present symptoms and patient is not obese Umbilical herniorrhaphy ( small )– primary herniorrhaphyTransverse incision around the umbilicus and subcutaneous
tissue are dissected off the rectus sheath to expose the neck of sac.Deal with content. Remove sac and close peritoneum. Aponeurosis on both side of umbilical ring is mobilised to allow an overlap.Interrupted matress sutures are inserted into aponeurosis.
- If large- prosthetic buttressing of the abdominal wall. (paraumbilical hernio plasty)

Incisional hernia Age: all ages but common in adult.Mostly in obese pt. Acquired scar in the abdominal wall caused by a previous
surgical operation (peritonitis) and injury Pt remembered that it caused by the scar.usually occur in
first year of operation but maybe also in later age. Might has hx of weakened the abdominal msuculature,
chronic cough,obesity or steroid therapy Symptoms :lump and pain.Maybe intestinal obstruction
(distension, colic , vomit, constipation and severe pain in the lump)
Irreducible , expansile cough impulse, local tissue thin and weak

Treatment
If pt obese- weight reduction by dieting before op.
Simple apposition Complex apposition (various type of
layered closure) Plastic fibre mesh or net closures
- Method of choice but in defect <4cm

References Bailey & Love’s 25th Edition A manual On Clinical Surgery By S.Das Browse’s Introduction To The Symptoms
And Sign of Surgical Disease 4th Edition Dissector Answers by University of
Michigan Medical School University of Connecticut Health Center Bedside Clinics in Surgery by Makhan Lal
Saha Melbourne Hernia Clinic