Hemostatic markers and atrial fibrillation in ARIC
18
Hemostatic markers are associated with the risk and prognosis of atrial fibrillation The ARIC Study Alvaro Alonso, 1 Weihong Tang, 1 Elsayed Z. Soliman, 2 Sunil K. Agarwal, 2 Alanna M. Chamberlain, 1 Aaron R. Folsom 1 1. School of Public Health, University of Minnesota; 2. Wake Forest University School of Medicine; 3. School of Global Public Health, University of North Carolina San Francisco, March 2010
-
Upload
alonso1976 -
Category
Documents
-
view
229 -
download
1
description
Association of hemostatic markers with the risk and prognosis of atrial fibrillation in the ARIC Study. Slides presented at the 50th AHA EPI/NPAM meeting, San Francisco, March 2010
Transcript of Hemostatic markers and atrial fibrillation in ARIC

Hemostatic markers are associated with the risk and prognosis of atrial
fibrillationThe ARIC Study
Alvaro Alonso,1 Weihong Tang,1 Elsayed Z. Soliman,2 Sunil K. Agarwal,2 Alanna M.
Chamberlain,1 Aaron R. Folsom1
1. School of Public Health, University of Minnesota; 2. Wake Forest University School of Medicine; 3. School of Global Public Health, University of North Carolina
San Francisco, March 2010

Background
• Increasing knowledge on risk factors and biomarkers of atrial fibrillation (AF)
• Hemostatic markers may be associated with the risk of AF, but limited evidence exists
• Hemostatic markers predict CV outcomes– Is this the case in AF patients?

Objectives
1. To assess whether hemostatic markers are associated with the incidence of AF independently of other CV risk factors
2. To determine whether associations of hemostatic markers with stroke, MI, or mortality are different in those with and without AF
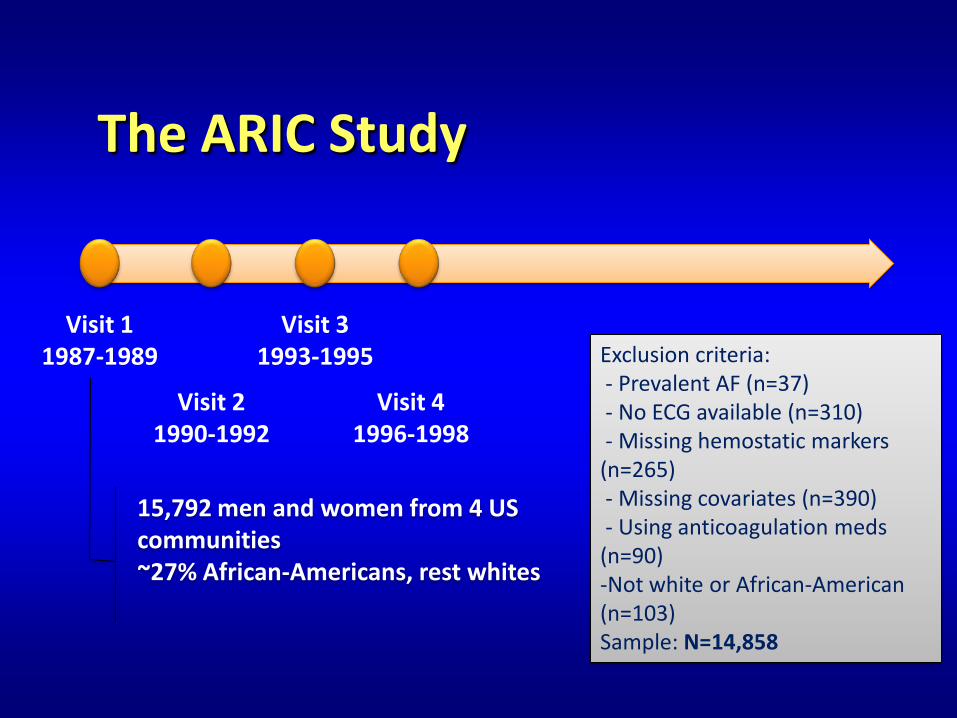
The ARIC Study
Visit 11987-1989
Visit 31993-1995
Visit 21990-1992
Visit 41996-1998
15,792 men and women from 4 US communities~27% African-Americans, rest whites
Exclusion criteria:- Prevalent AF (n=37)- No ECG available (n=310)- Missing hemostatic markers (n=265)- Missing covariates (n=390)- Using anticoagulation meds (n=90)-Not white or African-American (n=103)Sample: N=14,858
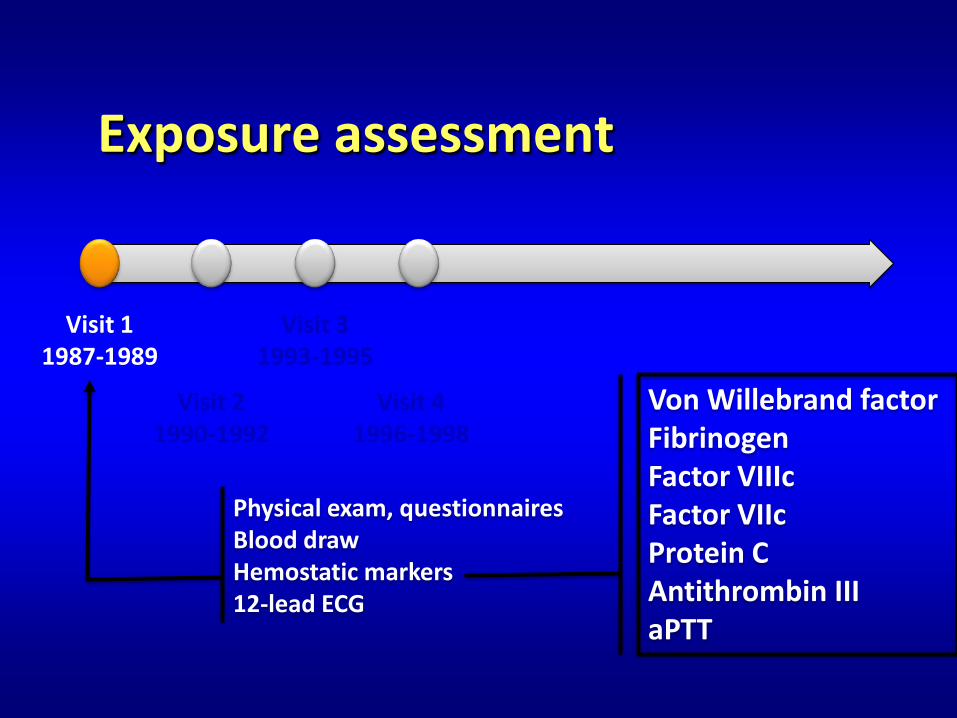
Exposure assessment
Visit 11987-1989
Visit 31993-1995
Visit 21990-1992
Visit 41996-1998
Physical exam, questionnairesBlood drawHemostatic markers12-lead ECG
Von Willebrand factorFibrinogenFactor VIIIcFactor VIIcProtein CAntithrombin IIIaPTT
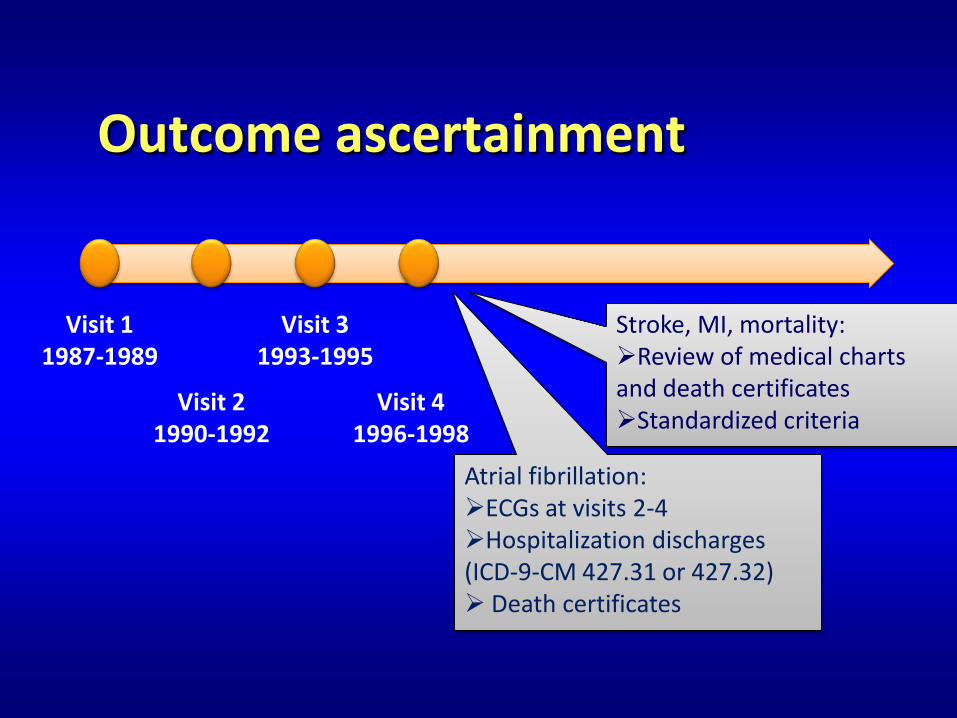
Outcome ascertainment
Visit 11987-1989
Visit 31993-1995
Visit 21990-1992
Visit 41996-1998
Atrial fibrillation:ECGs at visits 2-4Hospitalization discharges (ICD-9-CM 427.31 or 427.32) Death certificates
Stroke, MI, mortality:Review of medical charts and death certificatesStandardized criteria
Statistical analysis• Cox proportional hazards models with time
to AF as main outcome (end of follow-up, 12/31/2005)– Adjusted for age, gender, race, study center, education, income,
smoking, alcohol intake, physical activity, body mass index, height, left ventricular hypertrophy, systolic blood pressure, antihypertensive meds, diabetes, cholesterol meds, HDLc, total cholesterol
– Additional adjustment for MI and HF at baseline
• Additional models with stroke, MI or total mortality as outcomes– Including incident AF as a time-varying covariate

Baseline characteristicsWhites African-Americans
AF status No AF AF No AF AF
N 10131 976 3518 233
Age, years 54.1 (5.7) 57.3 (5.3) 53.4 (5.8) 56.2 (5.7)
Women 53.8 41.6 62.2 55.3
College educ 37.9 32.3 30.9 21.3
BMI 26.9 (4.8) 28.4 (5.6) 29.5 (6.1) 31.0 (6.8)
Current smk 24 30 30 34
Hypertension 25.5 44.3 54.4 73.3
Diabetes 8.4 15.9 18.3 34.0
ECG LVH 0.8 3.2 5.3 8.9
Hx MI 3.6 10.1 3.4 6.8
Hx HF 3.2 9.5 6.5 12.3Values correspond to means (SD) or percentages

Baseline characteristics
Whites African-Americans
AF status No AF AF No AF AF
vWf, % 111.5 125.0 132.7 149.1
Factor VIIIc, % 125.1 134.1 146.7 159.0
Fibrinogen, mg/dL 295.9 314.2 318.9 333.2
Factor VIIc, % 119.2 118.2 118.0 119.6
AT III, % 110.2 109.4 114.9 115.6
Protein C, mcg/mL 3.2 3.2 3.1 3.1
aPTT, s 29.1 29.1 29.1 29.0
Values correspond to means

Hemostatic markers and atrial fibrillationHR (95% CI) by quartiles of hemostatic markers at baseline
Cox model adjusted for age, gender, race, study center, education, income, smoking, alcohol intake, physical activity, body mass index, height, left ventricular hypertrophy, systolic blood pressure, antihypertensive meds, diabetes, cholesterol meds, HDLc, total cholesterol
0.5
1
2
vWF Fibrinogen Factor VIIIc Factor VIIc Protein C
HR
(95%
CI)
Q1
Q2
Q3
Q4

0.5
1
2
vWf Fibrinogen Factor VIIIc
Factor VIIc Protein C AT III aPTT
HR
(95%
CI)
Cox model adjusted for age, gender, race, study center, education, income, smoking, alcohol intake, physical activity, body mass index, height, left ventricular hypertrophy, systolic blood pressure, antihypertensive meds, diabetes, cholesterol meds, HDLc, total cholesterol
Hemostatic markers and atrial fibrillationHR (95% CI) of AF comparing ≥95th percentile to <95th percentile
(5th percentile for factor VIIc and protein C) in hemostatic markers at baseline
0.5
1
2
No AF AF No AF AF No AF AF No AF AF No AF AF
vWf Fibrinogen Factor VIIIc Factor VIIc Protein C
HR
(95%
CI)
Cox model adjusting for age, gender, race, site, education, smoking, alcohol, physical activity, body mass index, diabetes, systolic blood pressure, antihypertensive medication, HDLc, total cholesterol, lipid lowering medications, and left ventricular hypertrophy, and including incident AF as a time-dependent variable
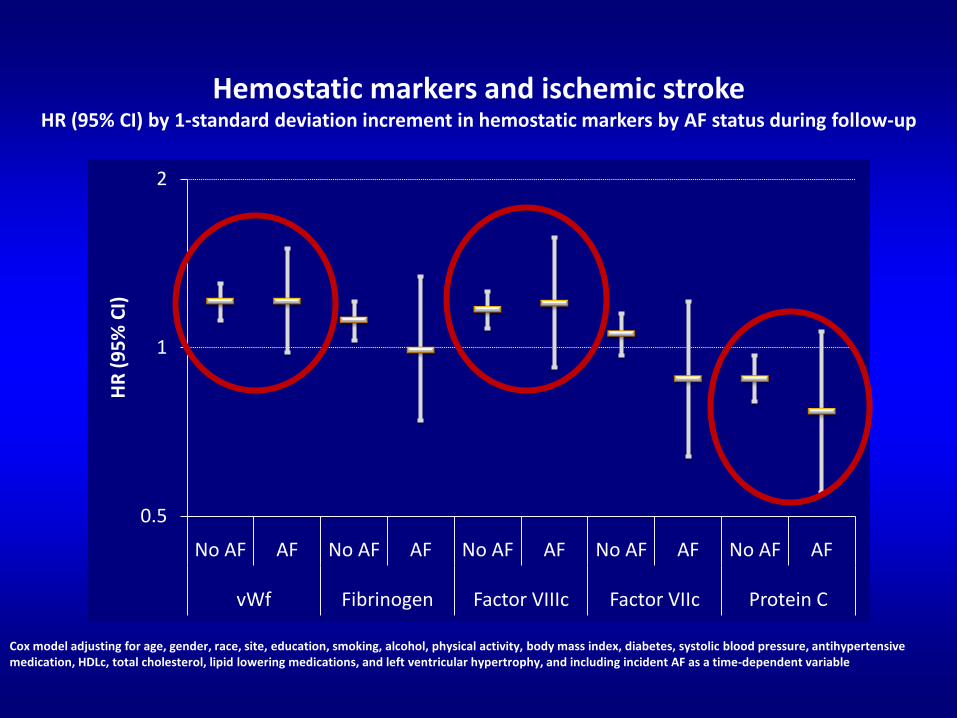
Hemostatic markers and ischemic stroke HR (95% CI) by 1-standard deviation increment in hemostatic markers by AF status during follow-up

0.5
1
2
No AF AF No AF AF No AF AF No AF AF No AF AF
vWf Fibrinogen Factor VIIIc Factor VIIc Protein C
HR
(95%
CI)
Cox model adjusting for age, gender, race, site, education, smoking, alcohol, physical activity, body mass index, diabetes, systolic blood pressure, antihypertensive medication, HDLc, total cholesterol, lipid lowering medications, and left ventricular hypertrophy, and including incident AF as a time-dependent variable
Hemostatic markers and myocardial infarctionHR (95% CI) by 1-standard deviation increment in hemostatic markers by AF status during follow-up

0.5
1
2
No AF AF No AF AF No AF AF No AF AF No AF AF
vWf Fibrinogen Factor VIIIc Factor VIIc Protein C
HR
(95%
CI)
Cox model adjusting for age, gender, race, site, education, smoking, alcohol, physical activity, body mass index, diabetes, systolic blood pressure, antihypertensive medication, HDLc, total cholesterol, lipid lowering medications, and left ventricular hypertrophy, and including incident AF as a time-dependent variable
Hemostatic markers and mortalityHR (95% CI) by 1-standard deviation increment in hemostatic markers by AF status during follow-up

Potential mechanisms
• Fibrinogen and von Willebrand factor as markers of inflammation and endothelial dysfunction
• Hemostatic markers associated with CVD• Reverse causation?

• Large sample size• Control for potential
confounders• Excellent follow-up
retention
Strengths and limitations
Strengths Limitations• Measurement error
in exposure• Misclassification of
the outcome• No information on
other biomarkers (e.g. CRP, BNP)

Conclusion
• Certain markers of hemostaticfunction are associated with the incidence of AF
• These hemostatic markers were similarly associated with CV outcomes in individuals with and without AF– Useful in risk stratification of AF patients

Acknowledgments
• The Atherosclerosis Risk in Communities Study is carried out as a collaborative study supported by National Heart, Lung, and Blood Institute contracts N01-HC-55015, N01-HC-55016, N01-HC-55018, N01-HC-55019, N01-HC-55020, N01-HC-55021, and N01-HC-55022
• This work was additionally supported by National Heart, Lung, and Blood Institute grant RC1HL099452 and American Heart Association grant 09SDG2280087
• The authors thank the staff and participants of the ARIC study for their important contributions