Hemodynamic-BasedEvaluationonThrombosisRiskofFusiform...
11
Research Article Hemodynamic-BasedEvaluationonThrombosisRiskofFusiform CoronaryArteryAneurysmsUsingComputationalFluidDynamic Simulation Method HaoranWang, 1,2 HitomiAnzai, 1 YoujunLiu, 3 AikeQiao , 3 JinshengXie, 4 andMakotoOhta 1,5 1 Institute of Fluid Science, Tohoku University, 2-1-1, Katahira, Aoba-Ku, Sendai, Miyagi 980-8577, Japan 2 Graduate School of Biomedical Engineering, Tohoku University, 6-6 Aramaki-Aza-Aoba, Aoba-Ku, Sendai, Miyagi 980-8579, Japan 3 College of Life Science and Bioengineering, Beijing University of Technology, No. 100 Pingleyuan, Chaoyang District, Beijing 100022, China 4 Department of Cardiac Surgery, Beijing Anzhen Hospital Capital Medical University, Beijing Institute of Heart Lung and Blood Vessel Diseases, Beijing 100029, China 5 ELyTMaX UMI 3757, CNRS–Universit´ e de Lyon, Tohoku University, Sendai, Japan Correspondence should be addressed to Makoto Ohta; ohta@biofluid.ifs.tohoku.ac.jp Received 15 May 2020; Revised 13 July 2020; Accepted 20 July 2020; Published 20 October 2020 Guest Editor: Zhihan Lv Copyright © 2020 Haoran Wang et al. is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Coronary artery aneurysms (CAAs) have been reported to associate with an increased risk for thrombosis. Distinct to the brain aneurysm, which can cause a rupture, CAA’s threat is more about its potential to induce thrombosis, leading to myocardial infarction. Case reports suggest that thrombosis risk varied with the different CAA diameters and hemodynamics effects (usually wall shear stress (WSS), oscillatory shear index (OSI), and relative residence time (RRT)) may relate to the thrombosis risk. However, currently, due to the rareness of the disease, there is limited knowledge of the hemodynamics effects of CAA. e aim of the study was to estimate the relationship between hemodynamic effects and different diameters of CAAs. Computational fluid dynamics (CFD) provides a noninvasive means of hemodynamic research. Four three-dimensional models were constructed, representing coronary arteries with a normal diameter (1x) and CAAs with diameters two (2x), three (3x), and five times (5x) that of the normal diameter. A lumped parameter model (LPM) which can capture the feature of coronary blood flow supplied the boundary conditions. WSS in the aneurysm decreased 97.7% apparently from 3.51Pa (1x) to 0.08 Pa (5x). OSI and RRT in the aneurysm were increased apparently by two orders of magnitude from 0.01 (1x) to 0.30 (5x), and from 0.38 Pa −1 (1x)to51.59Pa −1 (5x), separately. Changes in the local volume of the CAA resulted in dramatic changes in local hemodynamic parameters. e findings demonstrated that thrombosis risk increased with increasing diameter and was strongly exacerbated at larger diameters ofCAA.e2x model exhibited the lowest thrombosis risk among the models, suggesting the low-damage (medication) treatment may work. High-damage (surgery) treatment may need to be considered when CAA diameter is 3 times or higher. is diameter classification method may be a good example for constructing a more complex hemodynamic-based risk stratification method and could support clinical decision-making in the assessment of CAA. 1.Introduction A coronary artery aneurysm (CAA) is a localized swelling in one of the coronary arteries that supply oxygen to the heart. It is typically defined by a diameter at least 1.5 times that of the adjacent normal segments of the artery. It is called the giant CAA when the diameter of a CAA exceeds four times the diameter of its adjacent coronary artery [1]. e inci- dence of CAAs has been reported as 0.3%-5.3% [2]. How- ever, the prevalence of CAA in different literature varies due Hindawi Complexity Volume 2020, Article ID 8507273, 11 pages https://doi.org/10.1155/2020/8507273
Transcript of Hemodynamic-BasedEvaluationonThrombosisRiskofFusiform...

Research ArticleHemodynamic-Based Evaluation on Thrombosis Risk of FusiformCoronary Artery Aneurysms Using Computational Fluid DynamicSimulation Method
Haoran Wang12 Hitomi Anzai1 Youjun Liu3 Aike Qiao 3 Jinsheng Xie4
and Makoto Ohta 15
1Institute of Fluid Science Tohoku University 2-1-1 Katahira Aoba-Ku Sendai Miyagi 980-8577 Japan2Graduate School of Biomedical Engineering Tohoku University 6-6 Aramaki-Aza-Aoba Aoba-Ku SendaiMiyagi 980-8579 Japan3College of Life Science and Bioengineering Beijing University of Technology No 100 Pingleyuan Chaoyang DistrictBeijing 100022 China4Department of Cardiac Surgery Beijing Anzhen Hospital Capital Medical UniversityBeijing Institute of Heart Lung and Blood Vessel Diseases Beijing 100029 China5ELyTMaX UMI 3757 CNRSndashUniversite de Lyon Tohoku University Sendai Japan
Correspondence should be addressed to Makoto Ohta ohtabiofluidifstohokuacjp
Received 15 May 2020 Revised 13 July 2020 Accepted 20 July 2020 Published 20 October 2020
Guest Editor Zhihan Lv
Copyright copy 2020HaoranWang et al-is is an open access article distributed under the Creative Commons Attribution Licensewhich permits unrestricted use distribution and reproduction in any medium provided the original work is properly cited
Coronary artery aneurysms (CAAs) have been reported to associate with an increased risk for thrombosis Distinct to the brainaneurysm which can cause a rupture CAArsquos threat is more about its potential to induce thrombosis leading to myocardialinfarction Case reports suggest that thrombosis risk varied with the different CAA diameters and hemodynamics effects (usuallywall shear stress (WSS) oscillatory shear index (OSI) and relative residence time (RRT)) may relate to the thrombosis riskHowever currently due to the rareness of the disease there is limited knowledge of the hemodynamics effects of CAA-e aim ofthe study was to estimate the relationship between hemodynamic effects and different diameters of CAAs Computational fluiddynamics (CFD) provides a noninvasive means of hemodynamic research Four three-dimensional models were constructedrepresenting coronary arteries with a normal diameter (1x) and CAAs with diameters two (2x) three (3x) and five times (5x) thatof the normal diameter A lumped parameter model (LPM) which can capture the feature of coronary blood flow supplied theboundary conditions WSS in the aneurysm decreased 977 apparently from 351 Pa (1x) to 008 Pa (5x) OSI and RRT in theaneurysm were increased apparently by two orders of magnitude from 001 (1x) to 030 (5x) and from 038 Paminus1 (1x) to 5159 Paminus1
(5x) separately Changes in the local volume of the CAA resulted in dramatic changes in local hemodynamic parameters -efindings demonstrated that thrombosis risk increased with increasing diameter and was strongly exacerbated at larger diametersof CAA-e 2xmodel exhibited the lowest thrombosis risk among themodels suggesting the low-damage (medication) treatmentmay work High-damage (surgery) treatment may need to be considered when CAA diameter is 3 times or higher -is diameterclassificationmethodmay be a good example for constructing amore complex hemodynamic-based risk stratificationmethod andcould support clinical decision-making in the assessment of CAA
1 Introduction
A coronary artery aneurysm (CAA) is a localized swelling inone of the coronary arteries that supply oxygen to the heartIt is typically defined by a diameter at least 15 times that of
the adjacent normal segments of the artery It is called thegiant CAA when the diameter of a CAA exceeds four timesthe diameter of its adjacent coronary artery [1] -e inci-dence of CAAs has been reported as 03-53 [2] How-ever the prevalence of CAA in different literature varies due
HindawiComplexityVolume 2020 Article ID 8507273 11 pageshttpsdoiorg10115520208507273
to statistical data [3ndash6] lack of standardization for diagnosison angiography [5 7] and different CAA definitions [8]CAA is generally associated with the risk of complicationssuch as infarction ischemia and thrombosis with thethrombosis being the most common [9] Unlike other typesof aneurysms which pose a risk of rupture the main riskcaused by CAA is thrombosis rather than rupture [1]
Current American Heart Association (AHA) guidelinesfor risk stratification rely on aneurysm size alone as thecriterion for initiating systemic anticoagulation howeverstudies suggest risk may also depend on hemodynamicparameters such as low wall shear stress (WSS) high os-cillatory shear index (OSI) and high relative residence time(RRT) which are not available through image data alone[10ndash13] Indeed CAAsrsquo complex geometries such as thediameter may contribute to abnormal hemodynamics andcorrelate with patient outcome Considering the other risksdoctors may be confused about the dilemma of whether toadopt the watch-and-wait approach with the risk of suddendeterioration or to expose the patient to the risks oftreatment if just based on the image data alone -erefore itis necessary to evaluate the relationship between CAA di-ameter and level of thrombosis risk based on the hemo-dynamic study which could provide support for the doctors
Patient-specific hemodynamic simulations by usingcomputational fluid dynamics (CFD) can non-invasivelysupply informative hemodynamic parameters for betterthrombotic risk assessment however existing studies havebeen limited and struggle to quantify effects of aneurysmshape on local hemodynamics With such limitations inmind existing patient-specific models can be augmented byintroducing artificial aneurysms of specified diameter toachieve a systematic evaluation of the relationship betweenCAA size and the local hemodynamics Ultimately eluci-dating the relationship between hemodynamics and aneu-rysmal size characteristics may underlie more powerful riskstratification methods to support clinical decision-makingUsually these treatments include high-risk surgical treat-ment and conservative treatment regarding initiation ofanticoagulant therapy Surgery has multiple risks such as therisk of anesthesia postoperative complications and the likeDue to the large changes in the cardiovascular structure ofthe operation even if the surgical operation has completerisk management some postoperative complications such asweakened cardiac function and arrhythmia cannot becompletely avoided
CFD has been used widely in the research of vasculardiseases in recent years [14ndash16] and can be used to estimateimportant hemodynamic parameters including mass flowWSS OSI and RRT -e mass-flow rate can usually becalculated based on speed measurement using non-invasiveultrasonic velocimetry However other parameter WSSOSI and RRT measurements are much more complicatedand cannot be accurately measured directly -e indirectcalculation method of in vitro experiments which meansthe need to build an experimental system and need toconsider every potential problem in the system also hashigh cost -e advantages of CFD such as gaining insightinto systems that might be difficult to test through
experimentation and lower costs can overcome theshortcomings of other measurement methods mentionedabove Simulations have played important roles in otherstudies such as bypass grafts [17 18] and abdominal andcerebral aneurysms [19ndash21] but this technique has rarelybeen applied to CAAs One of the important factors is thatthe characteristics of the coronary artery make its simu-lation difficult In the human physiological environmentthe resistance of the coronary arteries changes repeatedlyduring systole the resistance of the coronary circulationincreases considerably due to the contraction of the heartIn contrast during diastole the pressure decreases whichreduces coronary microcirculation resistance As a con-sequence the coronary blood supply increased In ordernot to lose the characteristics of the coronary artery wehave adopted a circuit model called lumped parametermodel (LPM) to simulate the coronary artery to provide theboundary conditions for the CFD simulation work [22]
-e aim of the study was to estimate the relationshipbetween hemodynamic effects and different diameter ofCAAs We quantified hemodynamic parameters of likelyclinical relevance for assessing the thrombotic risk includingWSS OSI and RRTWe created virtual models by artificiallyconstructing models of normal coronary and different di-ameter of CAAs to compare normal and pathological he-modynamics -is study will allow us to estimate the risk ofthrombosis of CAAs from a hemodynamic perspective andprovide more comprehensive support for doctorsrsquo decisions
2 Materials and Methods
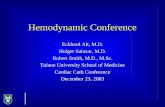
21 Model Development and SimulationMethods A patient-specific anatomy model was constructed based on patientdata provided by Anzhen Hospital All patient informationfor this analysis was anonymized -is study has been ap-proved by the Medical Ethics Committee of Beijing AnzhenHospital and Tohoku University -e images used for the 3Dmodel reconstruction were obtained by CT A personalizedreal 3D anatomic geometry model was built with manual andthreshold segmentation by using Mimics processing software(Materialise NV Leuven Belgium)-e single fusiformCAAsof different diameters were added to the left anteriordescending artery by using the PHANTOM Desktop inFreeform software (3D Systems USA)We have only changedthe diameter of CAA and have not changed the length of CAAalong the coronary artery -e link between CAA and normalcoronary artery was smoothed All the changes have beenconfirmed by the medical doctor CAA models were con-structed with diameters two three and five times that of thenormal segments of the coronary artery as well as a model ofa normal coronary artery without an aneurysm (Models 2x3x and 5x respectively Figure 1) so that we can studyhemodynamics on both regular and giant size (Figure 1)
-e computational models were generated by 3D modelmeshing using a hexahedral mesh controlled by size controlusing ANSYSMeshing software (Swanson Analysis SystemsInc USA) -e grids of the regions local to the CAA wererefined to allow more precise simulation calculations inthese areas for more accurate results
2 Complexity
To confirm the reliability of the simulation results weperformed a grid independence test on the number of elementsand nodes [22] See Figure 2 to check more information of theindependence test It can be found that the simulation resultstend to be stable when the number of grids exceeds a certainstandard-e total numbers of nodes and elements for the fourmodels differed (Table 1) but they were all of the same order ofmagnitude number Blood flow simulations were performed byusing the NavierndashStokes solver in the ANSYS-CFX software(Swanson Analysis Systems Inc) -e simulation calculationassumed that the artery wall was rigid and stationary the bloodflow was Newtonian and the density and viscosity were1050kgm3 and 00035Pa s respectively Based on the Rey-nolds number the fluid is set as laminar flow -e simulationswere run for three cardiac cycles We selected a time step of00025 s to satisfy the calculation of stability conditions -emaximum residual of momentum and continuity of the it-erative calculation was set to 00001
22 Lumped Parameter Boundary Conditions -e coronaryartery blood flow simulation required careful considerationof the physiological function of the coronary circulationand microcirculation especially the drastic change inmicrocirculatory resistance due to heart contractions -iscould be simulated appropriately by using an LPM -eLPM construction method for the boundary conditions wasbased on previous research [22 23] -e LPM systemcomprised a heart left ventricle module coronary arterymodules and arterial modules -ese modules were de-veloped based on the concept of the three-elementWindkessel RCR (resistor-capacitor-resistor) model [24] asimple circuit model in which blood flow and bloodpressure were considered to be analogous to electricalcurrent and voltage and the resistance and compliance ofblood vessels were characterized by resistance and capac-itance respectively-e entire multiscale model is shown inFigure 3 -e heart module can be built using somecomponents such as power source and variable capacitoron the basis of the RCR model -e power can simulate the
blood pressure and the variable capacitor can simulate thevolume change of the ventricular during the systole anddiastole-e inlet flow via the ascending aorta was providedby the LPM heart module and the LPM heart model wasconnected to the LPM coronary artery models throughintramyocardial pressure -e components of this moduleincluded resistors capacitors inductors and diodes whichwere used to simulate coronary resistance vascular com-pliance blood flow inertia and the heart valves respec-tively -e pressurendashvolume relationship representing thevascular compliance was calculated as follows
C(t) V(t) minus V0
P(t)
1E(t)
(1)
(a) (b) (c) (d)
Figure 1 -ree-dimensional models with a normal coronary artery (Model 0) and with coronary artery aneurysms with diameters twothree and five times that of the normal diameter (Models 2x 3x and 5x respectively) (a) Model 0 (b)Model 2x (c) Model 3x (d)Model 5x
The i
nlet
area
aver
age p
ress
ure (
Pa)
Number of elements (times104)
430428426424422
420
418416414
4120 50 100 150 200 250
Figure 2 -e result of grid independence test and the trend line ofthe results
Table 1-e numbers of nodes and elements of the grid in the fourcomputational models
Model 0 Model 2x Model 3x Model 5xNodes 1098996 940577 1047183 936749Elements 1437901 1231913 1370433 1230434
Complexity 3
where V(t) and P(t) are the pressure and volume of theventricle and V0 is the reference pressure E(t) characterizesthe time-varying elastic properties and was calculated asfollows
E(t) Emin + Emax minus Emin( 1113857 middot En tn( 1113857 (2)
-e units of E used were mL and mmHg Normalizedtime-varying elasticity En(tn) was calculated using a methodbased on previous research [25] as follows
En tn( 1113857 1551
1 + tn117( 1113857219
⎡⎣ ⎤⎦tn07( 1113857
19
1 + tn07( 111385719
⎡⎣ ⎤⎦ (3)
In the present study we set Emin 0002458 andEmax 20 tn t(02 + 015tc))( -e cardiac cycle tc wasset to 08 s
Compared with normal arterial blood vessels thecoronary artery module required the addition of a mi-crocirculation module to take account of the specialphysiology of coronary arteries -is module comprised aresistor (Rv-micro) and a capacitor (Ci-micro) with thecathode of the capacitor coupled to the internal pressure ofthe heart module to simulate changes in systolic pressure-e target mean flow of every branch of the LPM coronaryarteries was determined by the area of each branch [23 26]Based on previous studies [22 27] we assumed that thetotal perfusion of the coronary arteries was 4 of thecardiac output and that the total perfusion of the left andright coronary arteries was 60 and 40 of the totalperfusion of the coronary arteries respectively As shownin Figure 2 the simulation of coronary microcirculation isto add a module on the basis of the common artery tosimulate the pressure from the left ventricle and the re-sistance change caused by the pressure change -edebugging of the entire circuit model parameters is basedon previous research [22] in which the pressure adjustmentneeds to match the patientrsquos blood pressure
-e RCR model can be used to directly simulate arterialblood vessels because these do not undergo drastic changesin resistance -e RCR boundary conditions were set as theoutlets of the descending aorta and supra-aortic arteries
-e CFD boundary conditions provided by the LPM forthe inlet and outlets of the computational model corre-sponded to different modules known as the 0D3D mul-tiscale coupled method [22 23] -e important reasons foradopting LPM are the easy-to-deploy circuit model and thecharacteristics of not requiring a mainframe computer -eeasy-to-deploy circuit model means that a complex circuitmodel composed of many different components can besimulated by programming All four 3D models shared thesame LPM because apart from the CAA lesion the pe-ripheral vascular geometry did not change between themodels this ensured changes in the geometric structure ofthe CAA were the main cause of the different simulationresults Clinical observation has shown that the coronarystructure of the distal end of the coronary artery is notaffected by the CAA this was important evidence supportingthe selection of this method
3 Results
31 Mass Flow and Pressure Waveforms Figure 4 shows thecomputedmass flow and pressure over a cardiac cycle for theascending aorta (the inlet to the model) the descendingaorta an outlet artery and a coronary artery branch (ex-amples of outlets from the model) for the four 3D models-e results confirmed that except for the mass flow at thecoronary artery boundary mass flow in the outlets peakedduring systole -e coronary mass flow peaked during di-astole -ese results confirmed that the expected life-likecharacteristics of the coronary circulation which bloodsupply mainly occurred during diastole were successfullycaptured in the model [22] High systolic intra-myocardialpressure resulted in increased distal downstream resistance
A1
A2 A3 A4
a
bc
de
fg
ijk
lh
m
n
DAO
AAO
LPM coronary artery module coupled with 3D outlet
(coronary andashn)
LPM artery module coupled with outlet
DAO A1ndashA4)
LPM heart module coupled with 3D inlet (AAO)
Figure 3 Details of the multiscale model used in the study showing the coupled interface between the lumped parameter model(LPM) and the three-dimensional model an coronary arteries A1A4 arteries AAO ascending aorta DAO descending aorta RCRresistor-capacitor-resistor
4 Complexity
and decreased blood flow through the coronary artery theopposite was the case during diastole Changes in the di-ameter of the CAA did not have a significant effect oncoronary outlet flow
32 Wall Shear Stress -e WSS is the force per unit areaexerted by the wall on the fluid in a direction along the planeof the local tangent [28] calculated as follows
τω 4μQ
πR3 (4)
where μ represents the blood viscosity Q is mass-flowrate and R is vessel radius Previous studies have reportedan association between thrombosis formation and lowWSS [29] -e area average values of WSS in coronaryartery aneurysm over a cardiac cycle in the four models
are listed in Table 2 and the values over a cycle anddistribution contours are shown in Figures 5 and 6 -eaverage WSS over a cycle in Model 0 (with no CAA) was351 Pa -e averages for Models 2x 3x and 5x were 068026 and 008 Pa respectively substantially reduced in theCAA due to blood flow stagnation and recirculation withthe reduction increasing in CAAs of greater diameters-e distribution contours in Figure 6 confirm that theCAA results only in local hemodynamic disturbanceswithout wider hemodynamic changes in the arteries Atsome distance downstream in the coronary artery thecoronary diameter and WSS both return to normal levels
33 Oscillatory Shear Index OSI is a parameter thatquantifies the magnitude of theWSS and directional changes[18] calculated as follows
Inle
t AAO
Out
let D
AOO
utle
t A1
Out
let f
Mas
s flo
w (m
lmin
)
Pres
sure
(Pa)
Pres
sure
(Pa)
Pres
sure
(Pa)
Pres
sure
(Pa)
Mas
s flo
w (m
lmin
)M
ass f
low
(mlm
in)
Mas
s flo
w (m
lmin
)
20000
00
0
16500
10000008 08
13000
ndash20008
17000
100000 08
1600
00 08
16000
100000 08
45
00 08
Mass flow Pressure
16000
8000080
Cardiac cycle (s)
Cardiac cycle (s) Cardiac cycle (s)
Cardiac cycle (s)Cardiac cycle (s)
Cardiac cycle (s)
Cardiac cycle (s) Cardiac cycle (s)
Model 0
Model 3x Model 5x
Model 2x
DAO
A1
fAAO
Model 0Model 2x
Model 3xModel 5x
Figure 4 Mass flow and pressure curves for the inlet (ascending aorta AAO) and three outlets (descending aorta (DAO) artery 1 (A1) andcoronary artery f ) over a cardiac cycle
Complexity 5
OSI 05 times 1 minus1113938
T
0 τωdt11138681113868111386811138681113868
11138681113868111386811138681113868
1113938T
0 τω1113868111386811138681113868
1113868111386811138681113868dt
⎛⎝ ⎞⎠ (5)
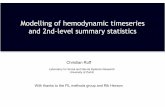
where T is the cardiac cycle OSI has values in the range 005with 0 representing undisturbed flow with no change in thedirection of the shear stress and 05 representing disturbedflow with oscillating shear stress Previous studies havereported an association between high OSI and the formationof intimal hyperplasia [30] -e average values of OSI in theaneurysm and OSI distribution contours are shown in Table 2and Figure 7 respectively -e average value of OSI over thecardiac cycle inModel 0 was 001-e averages forModels 2x3x and 5x were substantially higher at 003 013 and 030respectively Previous studies have pointed out that when OSIis greater than 02 it will cause endothelial cell damage [31]As shown in Table 3 the ratio of high OSI area in theaneurysm to the area of aneurysm was 0 125 253 and662 respectively Model 0 has OSI close to zero throughoutthe cardiac cycle and the flow in Model 0 is unidirectionalwithout circulation Normal coronary blood flow is unidi-rectional usually without flow recirculation so the OSI of thenormal coronary artery (Model 0) was close to zerothroughout the entire cardiac cycle-e highOSI values in theCAA models which reached 30 times higher in model 5xwere due to the increased storage time resulting from theincreased size of the cavity which led to recirculation withinthe CAA lesion -e effect on OSI was locally confined there
was little difference between the OSI in the distal coronaryarteries in Models 2x 3x and 5x and those in Model 0
34 Relative Residence Time -e RRT is an indicator thatcomprehensively characterizes the values and oscillation ofWSS [32] as well as the time of local blood flow and vascularinteraction [33] It is calculated as follows
RRT 1
(1 minus 2 middot OSI) middot TAWSS (6)
where
TAWSS WSS
T (7)
Here TAWSS isWSS average over one cardiac cycle andT is a cardiac cycle Figure 8 shows the distribution contoursfor RRT in the four models and Table 2 shows the areaaverage values of RRT within the CAA lesion over thecardiac cycle -e average value of RRT in Model 0 was038 Paminus1 -e averages for Models 2x 3x and 5x weresubstantially higher at 288 2312 and 5159 Paminus1 respec-tively showing a dramatic increase in RRT with increasingdiameter of the CAA Studies have reported a significantlyincreased risk of thrombosis when RRT is gt10 Paminus1 [12 34]As shown in Table 3 the ratio of high RRT area in theaneurysm to the area of aneurysm was 0 05 271 and786 respectively -e increased diameter of the CAAmakes it easier for blood to remain resident within ithampering the blood flow to the distal coronary artery -echange in RRT was locally confined to the CAA there waslittle difference between the RRT in the distal coronaryarteries in Models 2x 3x and 5x and that in the distalcoronary artery in Model 0
4 Discussion
We have shown that the relationship between hemodynamiceffects and different diameters of CAAs can be achieved byusing CFD simulation method direct comparison withvirtual control case based on the same patient We foundthat changes in the diameter of CAA have a strong effect onlocal hemodynamics while they do not have a significanteffect on global hemodynamics -e potential risk ofthrombosis increases significantly with increasing CAAdiameter indicated through decreasing WSS increasing OSIand RRT -is research will allow us to estimate thethrombosis risk of CAAs from a hemodynamic perspectiveand provide more comprehensive support for doctorsrsquodecisions
When making treatment decisions about CAAs doctorstypically depend on their own clinical experience [35] -ismay be because of the lack of useful diagnostic tools -ecurrent used tool is the method of imaging which canprovide geometric information and almost no other infor-mation -e lack of other information cannot provide morehelp for the doctorrsquos diagnosis -erefore it is necessary tofind a way to provide more information to help the doctor Ithas been shown that WSS over aneurysmal regions is
Table 2 Average values over a cardiac cycle for wall shear stress(WSS) the oscillatory shear index (OSI) and relative residencetime (RRT) in the coronary artery aneurysm
Model 0 Model2x
Model3x
Model5x
Area averageWSS (Pa) 351 068 026 008Area average OSI 001 003 013 030Area average RRT(Paminus1) 038 288 2312 5159
0
45
4
35
3
252
15
1
05
Wal
l she
ar st
ress
(Pa)
0 01 02 03 04 05 06 07 08Time (s)
Model 0Model 2x
Model 3xModel 5x
Figure 5 Wall shear stress in the coronary artery aneurysm over acardiac cycle for the four models
6 Complexity
associated with risk of thrombosis and that is a morepredictive factor of thrombosis than aneurysm diameter[36] We confirmed that hemodynamic research is beneficialfor aneurysm diagnosis and treatment [37] -erefore in
this study we quantitatively calculated the hemodynamicparameters of CAA of different diameters in order to esti-mate the relationship between the risk level of thrombosisand the size of CAA -e results showed that CAAs only
Front Back
OSI0495
0330
0165
0000
Model 0
Model 2x
Model 3x
Model 5x
Figure 7 Oscillatory shear index (OSI) distribution in the coronary artery aneurysm for the four models
Table 3 -e area of high OSI and RRT in the aneurysm and the area of aneurysm
Model 0 Model 2x Model 3x Model 5xHigh OSI areaCAA area (mm2) (ratio) 046362 (0) 952976238 (125) 29853117997 (253) 141389213579 (662)High RRT areaCAA area (mm2) (ratio) 046362 (0) 381276238 (05) 31977117997 (271) 167873213579 (786)
Front Back
Model 0
Model 2x
Model 3x
Model 5x
WSS
(Pa)
6936
4624
2312
0000
Figure 6 Wall shear stress (WSS) distribution in the coronary artery aneurysm at its peak (t 02 s) for the four models
Complexity 7
affect the blood flow and pressure within the region of thelesion itself with little effect on global blood flow Howeverthere were substantial changes in local hemodynamic pa-rameters related to thrombosis in the lesion locationCompared with the model without a lesion all three CAAmodels showed low WSS high OSI and high RRT withthese changes exacerbated as the CAA diameter increased-ese changes were the results of the sudden increase in thediameter of the lumen on entering the CAA -ese resultssuggest there may be a high correlation between CAA di-ameter and the risk of thrombosis CAA hemodynamicstudies may therefore allow the development of a prelimi-nary classification of the risk of thrombosis helping toimprove the effectiveness of anticoagulation therapy andfacilitating better personalization of treatment according to aquantitative hemodynamic plan
Simulation provides a powerful and effective method forestimating important hemodynamic parameters that aredifficult to measure As mentioned above except mass-flowrate which can be easily detected by non-invasive ultra-sound other parameters WSS OSI and RRT cannot bedirectly measured which are usually obtained through invitro experiments or indirect measurements Simulation is anon-invasive way providing a low cost way and avoiding thepotential risk of some invasive ways to obtain hemodynamicparameters
LPM boundary conditions can provide realistic physi-ologic flow conditions as what has been confirmed inprevious studies [38 39] In addition the coronary mi-crocirculation was introduced into the downstreamboundary condition via the LPM Resistance and pressurechanges downstream of the coronary artery could be
accurately captured in this way helping to ensure the ac-curate simulation of physiological conditions in the coro-nary artery -ere was no difference between the models inthe peripheral vascular structure so the CFD models sharedthe same LPM minimizing the impact of factors other thanthe diameter of the CAA -us the differences in resultsbetween the models were due to the differences in CAAdiameters
As the diameter of the CAA increased theWSS in the CAAlesion area progressively decreased with the WSS in Model 5xobserved to be gt10 times lower than that of the normalcoronary artery (Model 0) Parallel plate flow experiments haveshown that a large number of platelets accumulate at locationswith low WSS (lt04 Pa) [40] and animal endothelial cell ex-periments have shown that thrombosis is associated with adecrease in WSS to within the range 00770279Pa [10] In thepresent study the area average values for WSS in Models 3xand 5x were within this range suggesting that CAAs withdiametersgt3 times that of the normal artery are likely to carry ahigh risk of thrombosis Although the area average WSS forModel 2x was much lower than that of the model withoutCAA it was higher than 04Pa suggesting that CAAs withdiameters double that of the normal artery may not be at highrisk of thrombosis Another important pathophysiologicalfactor in vascular disease is endothelial dysfunction Low WSScan locally inhibit the production of certain important sub-stances such as NO [41] An abnormal response to vasodilationagents including the deactivation of NO by free radicals due tothe impairment of acetylcholine or endothelial NO synthasecan lead to abnormal vasoconstriction which can be associatedwith endothelial dysfunction [41] In addition platelets areprone to aggregation in areas of low WSS which further
Front Back
RRT99083
66055
33028
0000
(Pandash1)
Model 0
Model 2x
Model 3x
Model 5x
Figure 8 Relative residence time (RRT) distribution in the coronary artery aneurysm for the four models
8 Complexity
exacerbates the risk of thrombosis WSS in the CAA lesion ofModel 2x was lower than that in the normal model howeverfurther development is still to be studied just taking WSS as areference -e risk for thrombosis in CAAs progresses withincreasing diameter so the risk associatedwithModel 2xwouldbe lower than that for Models 3x and 5x -e development ofCAAs needs further study Although studies have investigatedthe association between WSS and thrombosis the currentunderstanding is not yet comprehensive -erefore the pos-sibility of WSS and thrombosis in the corresponding in vitroexperiments should be the focus of continued research
-e OSIs for the CAAs increased rapidly with increasingdiameter of the lesion with the OSI in Model 5x around 30times greater than that of the normal coronary artery (whichwas close to zero throughout the CAA) Previous studieshave pointed out that when OSI is greater than 02 it willcause endothelial cell damage [31] -e high OSI area(OSIgt 02) ratio increased from 01 to 662 betweenModel 0 and Model 5x In vivo experimental studies ofporcine aortas have reported that disturbed flow (ie anincrease in OSI) promoted the expression of proin-flammatory cytokines in endothelial cells [11] In additionan in vitro study of bovine endothelial cells reported that theexpression of monocyte chemoattractant protein-1 could beinduced by applying a low-amplitude oscillating shear stressof 03 Pa at 1Hz (equivalent to an OSI of 05) and thishemodynamic environment enhanced the binding of en-dothelial cells to monocytes [42] -ese findings suggest thatthe elevated OSI values observed in the CAA models may beassociated with conditions that can trigger thrombosis
-e RRT values for the CAAs increased dramatically withincreasing diameters of the lesions with the RRT for Model5xgt100 times greater than that of the normal coronary artery-e high RRTarea ratio increased from 01 to 786 betweenModel 0 and Model 5x -ese findings indicate that the bloodflow in the CAA recirculates when the diameter of the lumenincreases resulting in prolonged contact time between the CAAwall and the blood Studies have reported a significantly in-creased risk of thrombosis when RRT is gt10Paminus1 [12 34] -eRRTvalues forModels 3x and 5x in the present study were bothgt10Paminus1 suggesting a high risk of thrombosis when the di-ameter of a CAA exceeds three times that of the normal cor-onary artery Conversely the RRTforModel 2xwasmuch lowerthan 10Paminus1 suggesting that the risk of thrombosis may be lowwhen the diameter of the CAA is only double that of the normalartery Although there have been various studies of the rela-tionship between RRTand aneurysms [43] the current state ofknowledge remains insufficient for patient classification forexample there are no appropriate ranges of RRT values fordistinguishing the risk level of thrombosis which needs furtherstudy
In summary the comparison of our modeling resultswith the findings of previous studies suggested that the lowWSS high OSI and high RRT observed in the CAAs wouldsignificantly increase the risk of thrombosis However therisk varied considerably between the different diameters ofCAA -e WSS OSI and RRT values for Models 3x and 5xall suggested a high risk of thrombosis based on the previousstudy results-us for CAAs with diameters gt3 times that of
the normal coronary artery the risk of uncertainty withconservative treatment may be higher than the risk asso-ciated with surgery suggesting that the surgical operationshould be considered Conversely although the WSS OSIand RRT values for Model 2x were unfavorable comparedwith those of the model of the normal coronary arteryimplying an increased risk of thrombosis the magnitude ofthese differences was insufficient to support a prediction ofthe future development of the CAA For CAAs with a di-ameter up to two times that of the normal coronary arteryconservative drug treatment may be the better optionavoiding the risks associated with surgery
-e limitations of this study are as follows First this studyhas only one patientrsquos data and the conclusion may be ac-cidental We need to use more data for research Secondly animportant assumption used in the CFD calculation is the rigidwall where in fact elastic walls should be used In particularthe coronary artery will deform greatly as the heart contractswhich can be solved by two-way FSI in the future
5 Conclusion
-e evaluation of the relationship between hemodynamiceffects and different diameters of CAAs was performed inthis research through the CFD simulation method -erelationship between thrombosis risk and the size of theCAA diameter could be preliminarily evaluated from ahemodynamic perspective
We found that as the diameter of the CAA increased therisk of thrombosis increased substantially -e results sug-gested that when the diameter of a CAA is small (less thandouble that of the normal coronary artery) the risk ofthrombosis may be relatively low suggesting that medica-tion may be a sufficient approach for the patient avoidingthe uncertain risks associated with surgery If the diameter ofCAA is large (gt3 times that of the normal coronary artery)there may be a high risk of thrombosis and surgicaltreatment could be considered A similar approach could betaken in future studies to systematically assess the risk as-sociated with different shapes sizes and locations of an-eurysms Such approaches may form the basis for moresophisticated hemodynamic-based risk stratificationmethods supporting clinical decision-making in assessmentof CAA
Data Availability
-e data used to support the findings of this study areavailable from the corresponding author upon request
Conflicts of Interest
-e authors declare no conflicts of interest
Acknowledgments
-is research was supported by the National Natural ScienceFoundation of China (nos 11832003 and 11772016) andJSPS KAKENHI under Grant no JP18K18355 -is researchwas partially supported by the Creation of a Development
Complexity 9
Platform for ImplantableWearable Medical Devices by aNovel Physiological Data Integration System of the Programon Open Innovation Platform with Enterprises ResearchInstitute and Academia (OPERA) from the Japan Scienceand Technology Agency (JST) -is research was also sup-ported by Collaborative Research Project 2020 Institute ofFluid Science Tohoku University (J20R001) with the GrantNumber JP18K18355
References
[1] H Kato T Sugimura T Akagi et al ldquoLong-term conse-quences of kawasaki diseaserdquo Circulation vol 94 no 6pp 1379ndash1385 1996
[2] S A Sherif O O Tok O Taskoylu O Goktekin andI D Kilic ldquoCoronary artery aneurysms a review of theepidemiology pathophysiology diagnosis and treatmentrdquoFrontiers in Cardiovascular Medicine vol 4 2017
[3] E Beckmann S Rustum S Marquardt et al ldquoSurgicaltreatment of coronary artery aneurysmsrdquo Journal of CardiacSurgery vol 32 no 11 pp 674ndash679 2017
[4] M Syed M Lesch and A D Syed ldquoCoronary artery aneu-rysm a reviewrdquo Progress in Cardiovascular Diseases vol 40no 1 pp 77ndash84 1997
[5] G G Hartnell B M Parnell and R B Pridie ldquoCoronaryartery ectasia Its prevalence and clinical significance in 4993patientsrdquo British Heart Journal vol 54 no 4 1985
[6] A Satran B A Bart C R Henry et al ldquoIncreased prevalenceof coronary artery aneurysms among cocaine usersrdquo Circu-lation vol 111 no 19 pp 2424ndash2429 2005
[7] O Topaz M S Rutherford S M Bojack et al ldquoGiant an-eurysms of coronary arteries and saphenous vein graftsangiographic findings and histopathological correlatesrdquoCardiovascular Pathology vol 14 no 6 pp 298ndash302 2005
[8] A P Antoniadis Y S Chatzizisis and G D GiannoglouldquoPathogenetic mechanisms of coronary ectasiardquo InternationalJournal of Cardiology vol 130 no 3 pp 335ndash343 2008
[9] J B Gordon A M Kahn and J C Burns ldquoWhen childrenwith kawasaki disease grow uprdquo Journal of the AmericanCollege of Cardiology vol 54 no 21 pp 1911ndash1920 2009
[10] P Sriramarao L Languino and D Altieri ldquoFibrinogenmediates leukocyte-endothelium bridging in vivo at low shearforcesrdquo Blood vol 88 no 9 pp 3416ndash3423 1996
[11] A G Passerini D C Polacek C Shi et al ldquoCoexistingproinflammatory and antioxidative endothelial transcriptionprofiles in a disturbed flow region of the adult porcine aortardquoProceedings of the National Academy of Sciences vol 101no 89 pp 2482ndash2487
[12] U Morbiducci D Gallo R Ponzini et al ldquoQuantitativeanalysis of bulk flow in image-based hemodynamic models ofthe carotid bifurcation the influence of outflow conditions astest caserdquo Annals of Biomedical Engineering vol 38 no 12pp 3688ndash3705 2010
[13] T Ohkubo R Fukazawa E Ikegami and S Ogawa ldquoReducedshear stress and disturbed flow may lead to coronary aneu-rysm and thrombus formationsrdquo Pediatrics Internationalvol 49 no 1 pp 1ndash7 2007
[14] H Anzai T Watanabe X Han et al ldquoEndothelial cell dis-tributions and migration under conditions of flow shear stressaround a stent wirerdquo Technology and Health Care vol 28no 4 pp 345ndash354 2020
[15] M Zhang Y Li X Zhao et al ldquoHaemodynamic effects ofstent diameter and compaction ratio on flow-diversion
treatment of intracranial aneurysms a numerical study of asuccessful and an unsuccessful caserdquo Journal of Biomechanicsvol 58 pp 179ndash186 2017
[16] H Anzai B Chopard and M Ohta ldquoCombinational opti-mization of strut placement for intracranial stent using arealistic aneurysmrdquo Journal of Flow Control Measurement ampVisualization vol 2 no 2 pp 67ndash77 2014
[17] J P Ku M T Draney F R Arko et al ldquoIn vivo validation ofnumerical prediction of blood flow in arterial bypass graftsrdquoAnnals of Biomedical Engineering vol 30 no 6 pp 743ndash7522002
[18] A R Soler F Kabinejadian M A Slevin P J Bartolo andA Keshmiri ldquoOptimisation of a novel spiral-inducing bypassgraft using computational fluid dynamicsrdquo Scientific Reportsvol 7 no 1 p 1865 2017
[19] H Zhang L Li C Cheng and X Sun ldquoClinical value ofhomodynamic numerical simulation applied in the treatmentof cerebral aneurysmrdquo Experimental and Gerapeutic Medi-cine vol 4 no 6 pp 5401ndash5494 2017
[20] A S Les S C Shadden C A Figueroa et al ldquoQuantificationof hemodynamics in abdominal aortic aneurysms during restand exercise using magnetic resonance imaging and com-putational fluid dynamicsrdquo Annals of Biomedical Engineeringvol 38 no 4 pp 1288ndash1313 2010
[21] M Piccinelli A Veneziani D A Steinman A Remuzzi andL Antiga ldquoA framework for geometric analysis of vascularstructures application to cerebral aneurysmsrdquo IEEE Trans-actions on Medical Imaging vol 28 no 8 pp 1141ndash11552009
[22] H J Kim I E Vignon-Clementel J S CooganC A Figueroa K E Jansen and C A Taylor ldquoPatient-specific modeling of blood flow and pressure in humancoronary arteriesrdquo Annals of Biomedical Engineering vol 38no 10 pp 3195ndash3209 2010
[23] C A Taylor T A Fonte and J K Min ldquoComputational fluiddynamics applied to cardiac computed tomography fornoninvasive quantification of fractional flow reserverdquo Journalof the American College of Cardiology vol 61 no 22pp 2233ndash2241 2013
[24] I E V Clementel C A Figueroa K E Jansen andC A Taylor ldquoOutflow boundary conditions for 3D simula-tions of non-periodic blood flow and pressure fields in de-formable arteriesrdquo Computer Methods in Biomechanics andBiomedical Engineering vol 13 no 5 pp 625ndash640 2010
[25] N Stergiopulos J J Meister and N Westerhof ldquoDetermi-nants of stroke volume and systolic and diastolic aorticpressurerdquoGe American Journal of Physiology vol 270 no 6pp 2050ndash2059 1996
[26] M Zamir P Sinclair and T H Wonnacott ldquoRelation be-tween diameter and flow in major branches of the arch of theaortardquo Journal of Biomechanics vol 25 no 11 pp 1303ndash13101992
[27] K Johnson P Sharma and J Oshinski ldquoCoronary artery flowmeasurement using navigator echo gated phase contrastmagnetic resonance velocity mapping at 30 teslardquo Journal ofBiomechanics vol 41 no 3 pp 595ndash602 2008
[28] F P Salvuccia C A Perazzob S Sallesa J G Barrac andR L Armentano ldquoInfluence of inlet conditions in wall shearstress distributions of left coronary arteries in patient-specificsimulationsrdquo Mecanica Computacional vol XXIXpp 5953ndash5960 2010
[29] B C Lopez B Calvo and P Estefanıa Patient-SpecificComputational Modeling Springer Berlin Germany 2012thedition 2012
10 Complexity
[30] D N Ghista and F Kabinejadian ldquoCoronary artery bypassgrafting hemodynamics and anastomosis design a biomedicalengineering reviewrdquo BioMedical Engineering Online vol 12no 129 2013
[31] F P Glor F P Glor B Ariff et al ldquoImage-based carotid flowreconstruction a comparison between MRI and ultrasoundrdquoPhysiological Measurement vol 25 no 6 pp 1495ndash15092004
[32] S-W Lee L Antiga and D A Steinman ldquoCorrelationsamong indicators of disturbed flow at the normal carotidbifurcationrdquo Journal of Biomechanical Engineering vol 131no 6 Article ID 061013 2009
[33] H A Himburg ldquoSpatial comparison between wall shear stressmeasures and porcine arterial endothelial permeabilityrdquo AJPHeart and Circulatory Physiology vol 286 no 5 pp 1916ndash1922 2004
[34] T Suess J Anderson L Danielson et al ldquoExamination ofnear-wall hemodynamic parameters in the renal bridgingstent of various stent graft configurations for repairing vis-ceral branched aortic aneurysmsrdquo Journal of Vascular Sur-gery vol 64 no 3 pp 788ndash796 2016
[35] H Zhang X Yu F Ji and F Sun ldquoCoronary artery aneurysmformation after drug-coatedrdquo Medicine vol 97 no 45 2018
[36] N G Gutierrez M Mathew B W McCrindle et al ldquoHe-modynamic variables in aneurysms are associated withthrombotic risk in children with Kawasaki diseaserdquo Inter-national Journal of Cardiology vol 281 pp 15ndash21 2019
[37] C Karmonik G Chintalapani T Redel et al ldquoHemody-namics at the ostium of cerebral aneurysms with relation topost-treatment changes by a virtual flow diverter a compu-tational fluid dynamics studyrdquo in Proceedings of the AnnualInternational Conference of the IEEE Engineering in Medicineand Biology Society EMBS pp 1895ndash1898 Osaka Japan July2013
[38] J T Marcus H G Smeenk J P A KuijerR J Van Der Geest R M Heethaar and A C Van RossumldquoFlow profiles in the left anterior descending and the rightcoronary artery assessed byMR velocity quantification effectsof through-plane and in-plane motion of the heartrdquo Journal ofComputer Assisted Tomography vol 23 no 4 pp 567ndash5761999
[39] Y Shi P Lawford and R Hose ldquoReview of zero-D and 1-Dmodels of blood flow in the cardiovascular systemrdquo Bio-Medical Engineering Online vol 10 no 1 p 33 2011
[40] M Kroll J Hellums L McIntire A Schafer and J MoakeldquoPlatelets and shear stressrdquo Blood vol 88 no 5pp 1525ndash1541 1996
[41] J-J Chiu and S Chien ldquoEffects of disturbed flow on vascularendothelium pathophysiological basis and clinical perspec-tivesrdquo Physiological Reviews vol 91 no 1 pp 327ndash387 2011
[42] J Hwang M H Ing A Salazar et al ldquoPulsatile versus os-cillatory shear stress regulates NADPH oxidase subunit ex-pressionrdquo Circulation Research vol 93 no 12 pp 1225ndash12322003
[43] S-i Sugiyama K Niizuma T Nakayama et al ldquoRelativeresidence time prolongation in intracranial aneurysmsrdquoNeurosurgery vol 73 no 5 pp 767ndash776 2013
Complexity 11

to statistical data [3ndash6] lack of standardization for diagnosison angiography [5 7] and different CAA definitions [8]CAA is generally associated with the risk of complicationssuch as infarction ischemia and thrombosis with thethrombosis being the most common [9] Unlike other typesof aneurysms which pose a risk of rupture the main riskcaused by CAA is thrombosis rather than rupture [1]
Current American Heart Association (AHA) guidelinesfor risk stratification rely on aneurysm size alone as thecriterion for initiating systemic anticoagulation howeverstudies suggest risk may also depend on hemodynamicparameters such as low wall shear stress (WSS) high os-cillatory shear index (OSI) and high relative residence time(RRT) which are not available through image data alone[10ndash13] Indeed CAAsrsquo complex geometries such as thediameter may contribute to abnormal hemodynamics andcorrelate with patient outcome Considering the other risksdoctors may be confused about the dilemma of whether toadopt the watch-and-wait approach with the risk of suddendeterioration or to expose the patient to the risks oftreatment if just based on the image data alone -erefore itis necessary to evaluate the relationship between CAA di-ameter and level of thrombosis risk based on the hemo-dynamic study which could provide support for the doctors
Patient-specific hemodynamic simulations by usingcomputational fluid dynamics (CFD) can non-invasivelysupply informative hemodynamic parameters for betterthrombotic risk assessment however existing studies havebeen limited and struggle to quantify effects of aneurysmshape on local hemodynamics With such limitations inmind existing patient-specific models can be augmented byintroducing artificial aneurysms of specified diameter toachieve a systematic evaluation of the relationship betweenCAA size and the local hemodynamics Ultimately eluci-dating the relationship between hemodynamics and aneu-rysmal size characteristics may underlie more powerful riskstratification methods to support clinical decision-makingUsually these treatments include high-risk surgical treat-ment and conservative treatment regarding initiation ofanticoagulant therapy Surgery has multiple risks such as therisk of anesthesia postoperative complications and the likeDue to the large changes in the cardiovascular structure ofthe operation even if the surgical operation has completerisk management some postoperative complications such asweakened cardiac function and arrhythmia cannot becompletely avoided
CFD has been used widely in the research of vasculardiseases in recent years [14ndash16] and can be used to estimateimportant hemodynamic parameters including mass flowWSS OSI and RRT -e mass-flow rate can usually becalculated based on speed measurement using non-invasiveultrasonic velocimetry However other parameter WSSOSI and RRT measurements are much more complicatedand cannot be accurately measured directly -e indirectcalculation method of in vitro experiments which meansthe need to build an experimental system and need toconsider every potential problem in the system also hashigh cost -e advantages of CFD such as gaining insightinto systems that might be difficult to test through
experimentation and lower costs can overcome theshortcomings of other measurement methods mentionedabove Simulations have played important roles in otherstudies such as bypass grafts [17 18] and abdominal andcerebral aneurysms [19ndash21] but this technique has rarelybeen applied to CAAs One of the important factors is thatthe characteristics of the coronary artery make its simu-lation difficult In the human physiological environmentthe resistance of the coronary arteries changes repeatedlyduring systole the resistance of the coronary circulationincreases considerably due to the contraction of the heartIn contrast during diastole the pressure decreases whichreduces coronary microcirculation resistance As a con-sequence the coronary blood supply increased In ordernot to lose the characteristics of the coronary artery wehave adopted a circuit model called lumped parametermodel (LPM) to simulate the coronary artery to provide theboundary conditions for the CFD simulation work [22]
-e aim of the study was to estimate the relationshipbetween hemodynamic effects and different diameter ofCAAs We quantified hemodynamic parameters of likelyclinical relevance for assessing the thrombotic risk includingWSS OSI and RRTWe created virtual models by artificiallyconstructing models of normal coronary and different di-ameter of CAAs to compare normal and pathological he-modynamics -is study will allow us to estimate the risk ofthrombosis of CAAs from a hemodynamic perspective andprovide more comprehensive support for doctorsrsquo decisions
2 Materials and Methods
21 Model Development and SimulationMethods A patient-specific anatomy model was constructed based on patientdata provided by Anzhen Hospital All patient informationfor this analysis was anonymized -is study has been ap-proved by the Medical Ethics Committee of Beijing AnzhenHospital and Tohoku University -e images used for the 3Dmodel reconstruction were obtained by CT A personalizedreal 3D anatomic geometry model was built with manual andthreshold segmentation by using Mimics processing software(Materialise NV Leuven Belgium)-e single fusiformCAAsof different diameters were added to the left anteriordescending artery by using the PHANTOM Desktop inFreeform software (3D Systems USA)We have only changedthe diameter of CAA and have not changed the length of CAAalong the coronary artery -e link between CAA and normalcoronary artery was smoothed All the changes have beenconfirmed by the medical doctor CAA models were con-structed with diameters two three and five times that of thenormal segments of the coronary artery as well as a model ofa normal coronary artery without an aneurysm (Models 2x3x and 5x respectively Figure 1) so that we can studyhemodynamics on both regular and giant size (Figure 1)
-e computational models were generated by 3D modelmeshing using a hexahedral mesh controlled by size controlusing ANSYSMeshing software (Swanson Analysis SystemsInc USA) -e grids of the regions local to the CAA wererefined to allow more precise simulation calculations inthese areas for more accurate results
2 Complexity
To confirm the reliability of the simulation results weperformed a grid independence test on the number of elementsand nodes [22] See Figure 2 to check more information of theindependence test It can be found that the simulation resultstend to be stable when the number of grids exceeds a certainstandard-e total numbers of nodes and elements for the fourmodels differed (Table 1) but they were all of the same order ofmagnitude number Blood flow simulations were performed byusing the NavierndashStokes solver in the ANSYS-CFX software(Swanson Analysis Systems Inc) -e simulation calculationassumed that the artery wall was rigid and stationary the bloodflow was Newtonian and the density and viscosity were1050kgm3 and 00035Pa s respectively Based on the Rey-nolds number the fluid is set as laminar flow -e simulationswere run for three cardiac cycles We selected a time step of00025 s to satisfy the calculation of stability conditions -emaximum residual of momentum and continuity of the it-erative calculation was set to 00001
22 Lumped Parameter Boundary Conditions -e coronaryartery blood flow simulation required careful considerationof the physiological function of the coronary circulationand microcirculation especially the drastic change inmicrocirculatory resistance due to heart contractions -iscould be simulated appropriately by using an LPM -eLPM construction method for the boundary conditions wasbased on previous research [22 23] -e LPM systemcomprised a heart left ventricle module coronary arterymodules and arterial modules -ese modules were de-veloped based on the concept of the three-elementWindkessel RCR (resistor-capacitor-resistor) model [24] asimple circuit model in which blood flow and bloodpressure were considered to be analogous to electricalcurrent and voltage and the resistance and compliance ofblood vessels were characterized by resistance and capac-itance respectively-e entire multiscale model is shown inFigure 3 -e heart module can be built using somecomponents such as power source and variable capacitoron the basis of the RCR model -e power can simulate the
blood pressure and the variable capacitor can simulate thevolume change of the ventricular during the systole anddiastole-e inlet flow via the ascending aorta was providedby the LPM heart module and the LPM heart model wasconnected to the LPM coronary artery models throughintramyocardial pressure -e components of this moduleincluded resistors capacitors inductors and diodes whichwere used to simulate coronary resistance vascular com-pliance blood flow inertia and the heart valves respec-tively -e pressurendashvolume relationship representing thevascular compliance was calculated as follows
C(t) V(t) minus V0
P(t)
1E(t)
(1)
(a) (b) (c) (d)
Figure 1 -ree-dimensional models with a normal coronary artery (Model 0) and with coronary artery aneurysms with diameters twothree and five times that of the normal diameter (Models 2x 3x and 5x respectively) (a) Model 0 (b)Model 2x (c) Model 3x (d)Model 5x
The i
nlet
area
aver
age p
ress
ure (
Pa)
Number of elements (times104)
430428426424422
420
418416414
4120 50 100 150 200 250
Figure 2 -e result of grid independence test and the trend line ofthe results
Table 1-e numbers of nodes and elements of the grid in the fourcomputational models
Model 0 Model 2x Model 3x Model 5xNodes 1098996 940577 1047183 936749Elements 1437901 1231913 1370433 1230434
Complexity 3
where V(t) and P(t) are the pressure and volume of theventricle and V0 is the reference pressure E(t) characterizesthe time-varying elastic properties and was calculated asfollows
E(t) Emin + Emax minus Emin( 1113857 middot En tn( 1113857 (2)
-e units of E used were mL and mmHg Normalizedtime-varying elasticity En(tn) was calculated using a methodbased on previous research [25] as follows
En tn( 1113857 1551
1 + tn117( 1113857219
⎡⎣ ⎤⎦tn07( 1113857
19
1 + tn07( 111385719
⎡⎣ ⎤⎦ (3)
In the present study we set Emin 0002458 andEmax 20 tn t(02 + 015tc))( -e cardiac cycle tc wasset to 08 s
Compared with normal arterial blood vessels thecoronary artery module required the addition of a mi-crocirculation module to take account of the specialphysiology of coronary arteries -is module comprised aresistor (Rv-micro) and a capacitor (Ci-micro) with thecathode of the capacitor coupled to the internal pressure ofthe heart module to simulate changes in systolic pressure-e target mean flow of every branch of the LPM coronaryarteries was determined by the area of each branch [23 26]Based on previous studies [22 27] we assumed that thetotal perfusion of the coronary arteries was 4 of thecardiac output and that the total perfusion of the left andright coronary arteries was 60 and 40 of the totalperfusion of the coronary arteries respectively As shownin Figure 2 the simulation of coronary microcirculation isto add a module on the basis of the common artery tosimulate the pressure from the left ventricle and the re-sistance change caused by the pressure change -edebugging of the entire circuit model parameters is basedon previous research [22] in which the pressure adjustmentneeds to match the patientrsquos blood pressure
-e RCR model can be used to directly simulate arterialblood vessels because these do not undergo drastic changesin resistance -e RCR boundary conditions were set as theoutlets of the descending aorta and supra-aortic arteries
-e CFD boundary conditions provided by the LPM forthe inlet and outlets of the computational model corre-sponded to different modules known as the 0D3D mul-tiscale coupled method [22 23] -e important reasons foradopting LPM are the easy-to-deploy circuit model and thecharacteristics of not requiring a mainframe computer -eeasy-to-deploy circuit model means that a complex circuitmodel composed of many different components can besimulated by programming All four 3D models shared thesame LPM because apart from the CAA lesion the pe-ripheral vascular geometry did not change between themodels this ensured changes in the geometric structure ofthe CAA were the main cause of the different simulationresults Clinical observation has shown that the coronarystructure of the distal end of the coronary artery is notaffected by the CAA this was important evidence supportingthe selection of this method
3 Results
31 Mass Flow and Pressure Waveforms Figure 4 shows thecomputedmass flow and pressure over a cardiac cycle for theascending aorta (the inlet to the model) the descendingaorta an outlet artery and a coronary artery branch (ex-amples of outlets from the model) for the four 3D models-e results confirmed that except for the mass flow at thecoronary artery boundary mass flow in the outlets peakedduring systole -e coronary mass flow peaked during di-astole -ese results confirmed that the expected life-likecharacteristics of the coronary circulation which bloodsupply mainly occurred during diastole were successfullycaptured in the model [22] High systolic intra-myocardialpressure resulted in increased distal downstream resistance
A1
A2 A3 A4
a
bc
de
fg
ijk
lh
m
n
DAO
AAO
LPM coronary artery module coupled with 3D outlet
(coronary andashn)
LPM artery module coupled with outlet
DAO A1ndashA4)
LPM heart module coupled with 3D inlet (AAO)
Figure 3 Details of the multiscale model used in the study showing the coupled interface between the lumped parameter model(LPM) and the three-dimensional model an coronary arteries A1A4 arteries AAO ascending aorta DAO descending aorta RCRresistor-capacitor-resistor
4 Complexity
and decreased blood flow through the coronary artery theopposite was the case during diastole Changes in the di-ameter of the CAA did not have a significant effect oncoronary outlet flow
32 Wall Shear Stress -e WSS is the force per unit areaexerted by the wall on the fluid in a direction along the planeof the local tangent [28] calculated as follows
τω 4μQ
πR3 (4)
where μ represents the blood viscosity Q is mass-flowrate and R is vessel radius Previous studies have reportedan association between thrombosis formation and lowWSS [29] -e area average values of WSS in coronaryartery aneurysm over a cardiac cycle in the four models
are listed in Table 2 and the values over a cycle anddistribution contours are shown in Figures 5 and 6 -eaverage WSS over a cycle in Model 0 (with no CAA) was351 Pa -e averages for Models 2x 3x and 5x were 068026 and 008 Pa respectively substantially reduced in theCAA due to blood flow stagnation and recirculation withthe reduction increasing in CAAs of greater diameters-e distribution contours in Figure 6 confirm that theCAA results only in local hemodynamic disturbanceswithout wider hemodynamic changes in the arteries Atsome distance downstream in the coronary artery thecoronary diameter and WSS both return to normal levels
33 Oscillatory Shear Index OSI is a parameter thatquantifies the magnitude of theWSS and directional changes[18] calculated as follows
Inle
t AAO
Out
let D
AOO
utle
t A1
Out
let f
Mas
s flo
w (m
lmin
)
Pres
sure
(Pa)
Pres
sure
(Pa)
Pres
sure
(Pa)
Pres
sure
(Pa)
Mas
s flo
w (m
lmin
)M
ass f
low
(mlm
in)
Mas
s flo
w (m
lmin
)
20000
00
0
16500
10000008 08
13000
ndash20008
17000
100000 08
1600
00 08
16000
100000 08
45
00 08
Mass flow Pressure
16000
8000080
Cardiac cycle (s)
Cardiac cycle (s) Cardiac cycle (s)
Cardiac cycle (s)Cardiac cycle (s)
Cardiac cycle (s)
Cardiac cycle (s) Cardiac cycle (s)
Model 0
Model 3x Model 5x
Model 2x
DAO
A1
fAAO
Model 0Model 2x
Model 3xModel 5x
Figure 4 Mass flow and pressure curves for the inlet (ascending aorta AAO) and three outlets (descending aorta (DAO) artery 1 (A1) andcoronary artery f ) over a cardiac cycle
Complexity 5
OSI 05 times 1 minus1113938
T
0 τωdt11138681113868111386811138681113868
11138681113868111386811138681113868
1113938T
0 τω1113868111386811138681113868
1113868111386811138681113868dt
⎛⎝ ⎞⎠ (5)
where T is the cardiac cycle OSI has values in the range 005with 0 representing undisturbed flow with no change in thedirection of the shear stress and 05 representing disturbedflow with oscillating shear stress Previous studies havereported an association between high OSI and the formationof intimal hyperplasia [30] -e average values of OSI in theaneurysm and OSI distribution contours are shown in Table 2and Figure 7 respectively -e average value of OSI over thecardiac cycle inModel 0 was 001-e averages forModels 2x3x and 5x were substantially higher at 003 013 and 030respectively Previous studies have pointed out that when OSIis greater than 02 it will cause endothelial cell damage [31]As shown in Table 3 the ratio of high OSI area in theaneurysm to the area of aneurysm was 0 125 253 and662 respectively Model 0 has OSI close to zero throughoutthe cardiac cycle and the flow in Model 0 is unidirectionalwithout circulation Normal coronary blood flow is unidi-rectional usually without flow recirculation so the OSI of thenormal coronary artery (Model 0) was close to zerothroughout the entire cardiac cycle-e highOSI values in theCAA models which reached 30 times higher in model 5xwere due to the increased storage time resulting from theincreased size of the cavity which led to recirculation withinthe CAA lesion -e effect on OSI was locally confined there
was little difference between the OSI in the distal coronaryarteries in Models 2x 3x and 5x and those in Model 0
34 Relative Residence Time -e RRT is an indicator thatcomprehensively characterizes the values and oscillation ofWSS [32] as well as the time of local blood flow and vascularinteraction [33] It is calculated as follows
RRT 1
(1 minus 2 middot OSI) middot TAWSS (6)
where
TAWSS WSS
T (7)
Here TAWSS isWSS average over one cardiac cycle andT is a cardiac cycle Figure 8 shows the distribution contoursfor RRT in the four models and Table 2 shows the areaaverage values of RRT within the CAA lesion over thecardiac cycle -e average value of RRT in Model 0 was038 Paminus1 -e averages for Models 2x 3x and 5x weresubstantially higher at 288 2312 and 5159 Paminus1 respec-tively showing a dramatic increase in RRT with increasingdiameter of the CAA Studies have reported a significantlyincreased risk of thrombosis when RRT is gt10 Paminus1 [12 34]As shown in Table 3 the ratio of high RRT area in theaneurysm to the area of aneurysm was 0 05 271 and786 respectively -e increased diameter of the CAAmakes it easier for blood to remain resident within ithampering the blood flow to the distal coronary artery -echange in RRT was locally confined to the CAA there waslittle difference between the RRT in the distal coronaryarteries in Models 2x 3x and 5x and that in the distalcoronary artery in Model 0
4 Discussion
We have shown that the relationship between hemodynamiceffects and different diameters of CAAs can be achieved byusing CFD simulation method direct comparison withvirtual control case based on the same patient We foundthat changes in the diameter of CAA have a strong effect onlocal hemodynamics while they do not have a significanteffect on global hemodynamics -e potential risk ofthrombosis increases significantly with increasing CAAdiameter indicated through decreasing WSS increasing OSIand RRT -is research will allow us to estimate thethrombosis risk of CAAs from a hemodynamic perspectiveand provide more comprehensive support for doctorsrsquodecisions
When making treatment decisions about CAAs doctorstypically depend on their own clinical experience [35] -ismay be because of the lack of useful diagnostic tools -ecurrent used tool is the method of imaging which canprovide geometric information and almost no other infor-mation -e lack of other information cannot provide morehelp for the doctorrsquos diagnosis -erefore it is necessary tofind a way to provide more information to help the doctor Ithas been shown that WSS over aneurysmal regions is
Table 2 Average values over a cardiac cycle for wall shear stress(WSS) the oscillatory shear index (OSI) and relative residencetime (RRT) in the coronary artery aneurysm
Model 0 Model2x
Model3x
Model5x
Area averageWSS (Pa) 351 068 026 008Area average OSI 001 003 013 030Area average RRT(Paminus1) 038 288 2312 5159
0
45
4
35
3
252
15
1
05
Wal
l she
ar st
ress
(Pa)
0 01 02 03 04 05 06 07 08Time (s)
Model 0Model 2x
Model 3xModel 5x
Figure 5 Wall shear stress in the coronary artery aneurysm over acardiac cycle for the four models
6 Complexity
associated with risk of thrombosis and that is a morepredictive factor of thrombosis than aneurysm diameter[36] We confirmed that hemodynamic research is beneficialfor aneurysm diagnosis and treatment [37] -erefore in
this study we quantitatively calculated the hemodynamicparameters of CAA of different diameters in order to esti-mate the relationship between the risk level of thrombosisand the size of CAA -e results showed that CAAs only
Front Back
OSI0495
0330
0165
0000
Model 0
Model 2x
Model 3x
Model 5x
Figure 7 Oscillatory shear index (OSI) distribution in the coronary artery aneurysm for the four models
Table 3 -e area of high OSI and RRT in the aneurysm and the area of aneurysm
Model 0 Model 2x Model 3x Model 5xHigh OSI areaCAA area (mm2) (ratio) 046362 (0) 952976238 (125) 29853117997 (253) 141389213579 (662)High RRT areaCAA area (mm2) (ratio) 046362 (0) 381276238 (05) 31977117997 (271) 167873213579 (786)
Front Back
Model 0
Model 2x
Model 3x
Model 5x
WSS
(Pa)
6936
4624
2312
0000
Figure 6 Wall shear stress (WSS) distribution in the coronary artery aneurysm at its peak (t 02 s) for the four models
Complexity 7
affect the blood flow and pressure within the region of thelesion itself with little effect on global blood flow Howeverthere were substantial changes in local hemodynamic pa-rameters related to thrombosis in the lesion locationCompared with the model without a lesion all three CAAmodels showed low WSS high OSI and high RRT withthese changes exacerbated as the CAA diameter increased-ese changes were the results of the sudden increase in thediameter of the lumen on entering the CAA -ese resultssuggest there may be a high correlation between CAA di-ameter and the risk of thrombosis CAA hemodynamicstudies may therefore allow the development of a prelimi-nary classification of the risk of thrombosis helping toimprove the effectiveness of anticoagulation therapy andfacilitating better personalization of treatment according to aquantitative hemodynamic plan
Simulation provides a powerful and effective method forestimating important hemodynamic parameters that aredifficult to measure As mentioned above except mass-flowrate which can be easily detected by non-invasive ultra-sound other parameters WSS OSI and RRT cannot bedirectly measured which are usually obtained through invitro experiments or indirect measurements Simulation is anon-invasive way providing a low cost way and avoiding thepotential risk of some invasive ways to obtain hemodynamicparameters
LPM boundary conditions can provide realistic physi-ologic flow conditions as what has been confirmed inprevious studies [38 39] In addition the coronary mi-crocirculation was introduced into the downstreamboundary condition via the LPM Resistance and pressurechanges downstream of the coronary artery could be
accurately captured in this way helping to ensure the ac-curate simulation of physiological conditions in the coro-nary artery -ere was no difference between the models inthe peripheral vascular structure so the CFD models sharedthe same LPM minimizing the impact of factors other thanthe diameter of the CAA -us the differences in resultsbetween the models were due to the differences in CAAdiameters
As the diameter of the CAA increased theWSS in the CAAlesion area progressively decreased with the WSS in Model 5xobserved to be gt10 times lower than that of the normalcoronary artery (Model 0) Parallel plate flow experiments haveshown that a large number of platelets accumulate at locationswith low WSS (lt04 Pa) [40] and animal endothelial cell ex-periments have shown that thrombosis is associated with adecrease in WSS to within the range 00770279Pa [10] In thepresent study the area average values for WSS in Models 3xand 5x were within this range suggesting that CAAs withdiametersgt3 times that of the normal artery are likely to carry ahigh risk of thrombosis Although the area average WSS forModel 2x was much lower than that of the model withoutCAA it was higher than 04Pa suggesting that CAAs withdiameters double that of the normal artery may not be at highrisk of thrombosis Another important pathophysiologicalfactor in vascular disease is endothelial dysfunction Low WSScan locally inhibit the production of certain important sub-stances such as NO [41] An abnormal response to vasodilationagents including the deactivation of NO by free radicals due tothe impairment of acetylcholine or endothelial NO synthasecan lead to abnormal vasoconstriction which can be associatedwith endothelial dysfunction [41] In addition platelets areprone to aggregation in areas of low WSS which further
Front Back
RRT99083
66055
33028
0000
(Pandash1)
Model 0
Model 2x
Model 3x
Model 5x
Figure 8 Relative residence time (RRT) distribution in the coronary artery aneurysm for the four models
8 Complexity
exacerbates the risk of thrombosis WSS in the CAA lesion ofModel 2x was lower than that in the normal model howeverfurther development is still to be studied just taking WSS as areference -e risk for thrombosis in CAAs progresses withincreasing diameter so the risk associatedwithModel 2xwouldbe lower than that for Models 3x and 5x -e development ofCAAs needs further study Although studies have investigatedthe association between WSS and thrombosis the currentunderstanding is not yet comprehensive -erefore the pos-sibility of WSS and thrombosis in the corresponding in vitroexperiments should be the focus of continued research
-e OSIs for the CAAs increased rapidly with increasingdiameter of the lesion with the OSI in Model 5x around 30times greater than that of the normal coronary artery (whichwas close to zero throughout the CAA) Previous studieshave pointed out that when OSI is greater than 02 it willcause endothelial cell damage [31] -e high OSI area(OSIgt 02) ratio increased from 01 to 662 betweenModel 0 and Model 5x In vivo experimental studies ofporcine aortas have reported that disturbed flow (ie anincrease in OSI) promoted the expression of proin-flammatory cytokines in endothelial cells [11] In additionan in vitro study of bovine endothelial cells reported that theexpression of monocyte chemoattractant protein-1 could beinduced by applying a low-amplitude oscillating shear stressof 03 Pa at 1Hz (equivalent to an OSI of 05) and thishemodynamic environment enhanced the binding of en-dothelial cells to monocytes [42] -ese findings suggest thatthe elevated OSI values observed in the CAA models may beassociated with conditions that can trigger thrombosis
-e RRT values for the CAAs increased dramatically withincreasing diameters of the lesions with the RRT for Model5xgt100 times greater than that of the normal coronary artery-e high RRTarea ratio increased from 01 to 786 betweenModel 0 and Model 5x -ese findings indicate that the bloodflow in the CAA recirculates when the diameter of the lumenincreases resulting in prolonged contact time between the CAAwall and the blood Studies have reported a significantly in-creased risk of thrombosis when RRT is gt10Paminus1 [12 34] -eRRTvalues forModels 3x and 5x in the present study were bothgt10Paminus1 suggesting a high risk of thrombosis when the di-ameter of a CAA exceeds three times that of the normal cor-onary artery Conversely the RRTforModel 2xwasmuch lowerthan 10Paminus1 suggesting that the risk of thrombosis may be lowwhen the diameter of the CAA is only double that of the normalartery Although there have been various studies of the rela-tionship between RRTand aneurysms [43] the current state ofknowledge remains insufficient for patient classification forexample there are no appropriate ranges of RRT values fordistinguishing the risk level of thrombosis which needs furtherstudy
In summary the comparison of our modeling resultswith the findings of previous studies suggested that the lowWSS high OSI and high RRT observed in the CAAs wouldsignificantly increase the risk of thrombosis However therisk varied considerably between the different diameters ofCAA -e WSS OSI and RRT values for Models 3x and 5xall suggested a high risk of thrombosis based on the previousstudy results-us for CAAs with diameters gt3 times that of
the normal coronary artery the risk of uncertainty withconservative treatment may be higher than the risk asso-ciated with surgery suggesting that the surgical operationshould be considered Conversely although the WSS OSIand RRT values for Model 2x were unfavorable comparedwith those of the model of the normal coronary arteryimplying an increased risk of thrombosis the magnitude ofthese differences was insufficient to support a prediction ofthe future development of the CAA For CAAs with a di-ameter up to two times that of the normal coronary arteryconservative drug treatment may be the better optionavoiding the risks associated with surgery
-e limitations of this study are as follows First this studyhas only one patientrsquos data and the conclusion may be ac-cidental We need to use more data for research Secondly animportant assumption used in the CFD calculation is the rigidwall where in fact elastic walls should be used In particularthe coronary artery will deform greatly as the heart contractswhich can be solved by two-way FSI in the future
5 Conclusion
-e evaluation of the relationship between hemodynamiceffects and different diameters of CAAs was performed inthis research through the CFD simulation method -erelationship between thrombosis risk and the size of theCAA diameter could be preliminarily evaluated from ahemodynamic perspective
We found that as the diameter of the CAA increased therisk of thrombosis increased substantially -e results sug-gested that when the diameter of a CAA is small (less thandouble that of the normal coronary artery) the risk ofthrombosis may be relatively low suggesting that medica-tion may be a sufficient approach for the patient avoidingthe uncertain risks associated with surgery If the diameter ofCAA is large (gt3 times that of the normal coronary artery)there may be a high risk of thrombosis and surgicaltreatment could be considered A similar approach could betaken in future studies to systematically assess the risk as-sociated with different shapes sizes and locations of an-eurysms Such approaches may form the basis for moresophisticated hemodynamic-based risk stratificationmethods supporting clinical decision-making in assessmentof CAA
Data Availability
-e data used to support the findings of this study areavailable from the corresponding author upon request
Conflicts of Interest
-e authors declare no conflicts of interest
Acknowledgments
-is research was supported by the National Natural ScienceFoundation of China (nos 11832003 and 11772016) andJSPS KAKENHI under Grant no JP18K18355 -is researchwas partially supported by the Creation of a Development
Complexity 9
Platform for ImplantableWearable Medical Devices by aNovel Physiological Data Integration System of the Programon Open Innovation Platform with Enterprises ResearchInstitute and Academia (OPERA) from the Japan Scienceand Technology Agency (JST) -is research was also sup-ported by Collaborative Research Project 2020 Institute ofFluid Science Tohoku University (J20R001) with the GrantNumber JP18K18355
References
[1] H Kato T Sugimura T Akagi et al ldquoLong-term conse-quences of kawasaki diseaserdquo Circulation vol 94 no 6pp 1379ndash1385 1996
[2] S A Sherif O O Tok O Taskoylu O Goktekin andI D Kilic ldquoCoronary artery aneurysms a review of theepidemiology pathophysiology diagnosis and treatmentrdquoFrontiers in Cardiovascular Medicine vol 4 2017
[3] E Beckmann S Rustum S Marquardt et al ldquoSurgicaltreatment of coronary artery aneurysmsrdquo Journal of CardiacSurgery vol 32 no 11 pp 674ndash679 2017
[4] M Syed M Lesch and A D Syed ldquoCoronary artery aneu-rysm a reviewrdquo Progress in Cardiovascular Diseases vol 40no 1 pp 77ndash84 1997
[5] G G Hartnell B M Parnell and R B Pridie ldquoCoronaryartery ectasia Its prevalence and clinical significance in 4993patientsrdquo British Heart Journal vol 54 no 4 1985
[6] A Satran B A Bart C R Henry et al ldquoIncreased prevalenceof coronary artery aneurysms among cocaine usersrdquo Circu-lation vol 111 no 19 pp 2424ndash2429 2005
[7] O Topaz M S Rutherford S M Bojack et al ldquoGiant an-eurysms of coronary arteries and saphenous vein graftsangiographic findings and histopathological correlatesrdquoCardiovascular Pathology vol 14 no 6 pp 298ndash302 2005
[8] A P Antoniadis Y S Chatzizisis and G D GiannoglouldquoPathogenetic mechanisms of coronary ectasiardquo InternationalJournal of Cardiology vol 130 no 3 pp 335ndash343 2008
[9] J B Gordon A M Kahn and J C Burns ldquoWhen childrenwith kawasaki disease grow uprdquo Journal of the AmericanCollege of Cardiology vol 54 no 21 pp 1911ndash1920 2009
[10] P Sriramarao L Languino and D Altieri ldquoFibrinogenmediates leukocyte-endothelium bridging in vivo at low shearforcesrdquo Blood vol 88 no 9 pp 3416ndash3423 1996
[11] A G Passerini D C Polacek C Shi et al ldquoCoexistingproinflammatory and antioxidative endothelial transcriptionprofiles in a disturbed flow region of the adult porcine aortardquoProceedings of the National Academy of Sciences vol 101no 89 pp 2482ndash2487
[12] U Morbiducci D Gallo R Ponzini et al ldquoQuantitativeanalysis of bulk flow in image-based hemodynamic models ofthe carotid bifurcation the influence of outflow conditions astest caserdquo Annals of Biomedical Engineering vol 38 no 12pp 3688ndash3705 2010
[13] T Ohkubo R Fukazawa E Ikegami and S Ogawa ldquoReducedshear stress and disturbed flow may lead to coronary aneu-rysm and thrombus formationsrdquo Pediatrics Internationalvol 49 no 1 pp 1ndash7 2007
[14] H Anzai T Watanabe X Han et al ldquoEndothelial cell dis-tributions and migration under conditions of flow shear stressaround a stent wirerdquo Technology and Health Care vol 28no 4 pp 345ndash354 2020
[15] M Zhang Y Li X Zhao et al ldquoHaemodynamic effects ofstent diameter and compaction ratio on flow-diversion
treatment of intracranial aneurysms a numerical study of asuccessful and an unsuccessful caserdquo Journal of Biomechanicsvol 58 pp 179ndash186 2017
[16] H Anzai B Chopard and M Ohta ldquoCombinational opti-mization of strut placement for intracranial stent using arealistic aneurysmrdquo Journal of Flow Control Measurement ampVisualization vol 2 no 2 pp 67ndash77 2014
[17] J P Ku M T Draney F R Arko et al ldquoIn vivo validation ofnumerical prediction of blood flow in arterial bypass graftsrdquoAnnals of Biomedical Engineering vol 30 no 6 pp 743ndash7522002
[18] A R Soler F Kabinejadian M A Slevin P J Bartolo andA Keshmiri ldquoOptimisation of a novel spiral-inducing bypassgraft using computational fluid dynamicsrdquo Scientific Reportsvol 7 no 1 p 1865 2017
[19] H Zhang L Li C Cheng and X Sun ldquoClinical value ofhomodynamic numerical simulation applied in the treatmentof cerebral aneurysmrdquo Experimental and Gerapeutic Medi-cine vol 4 no 6 pp 5401ndash5494 2017
[20] A S Les S C Shadden C A Figueroa et al ldquoQuantificationof hemodynamics in abdominal aortic aneurysms during restand exercise using magnetic resonance imaging and com-putational fluid dynamicsrdquo Annals of Biomedical Engineeringvol 38 no 4 pp 1288ndash1313 2010
[21] M Piccinelli A Veneziani D A Steinman A Remuzzi andL Antiga ldquoA framework for geometric analysis of vascularstructures application to cerebral aneurysmsrdquo IEEE Trans-actions on Medical Imaging vol 28 no 8 pp 1141ndash11552009
[22] H J Kim I E Vignon-Clementel J S CooganC A Figueroa K E Jansen and C A Taylor ldquoPatient-specific modeling of blood flow and pressure in humancoronary arteriesrdquo Annals of Biomedical Engineering vol 38no 10 pp 3195ndash3209 2010
[23] C A Taylor T A Fonte and J K Min ldquoComputational fluiddynamics applied to cardiac computed tomography fornoninvasive quantification of fractional flow reserverdquo Journalof the American College of Cardiology vol 61 no 22pp 2233ndash2241 2013
[24] I E V Clementel C A Figueroa K E Jansen andC A Taylor ldquoOutflow boundary conditions for 3D simula-tions of non-periodic blood flow and pressure fields in de-formable arteriesrdquo Computer Methods in Biomechanics andBiomedical Engineering vol 13 no 5 pp 625ndash640 2010
[25] N Stergiopulos J J Meister and N Westerhof ldquoDetermi-nants of stroke volume and systolic and diastolic aorticpressurerdquoGe American Journal of Physiology vol 270 no 6pp 2050ndash2059 1996
[26] M Zamir P Sinclair and T H Wonnacott ldquoRelation be-tween diameter and flow in major branches of the arch of theaortardquo Journal of Biomechanics vol 25 no 11 pp 1303ndash13101992
[27] K Johnson P Sharma and J Oshinski ldquoCoronary artery flowmeasurement using navigator echo gated phase contrastmagnetic resonance velocity mapping at 30 teslardquo Journal ofBiomechanics vol 41 no 3 pp 595ndash602 2008
[28] F P Salvuccia C A Perazzob S Sallesa J G Barrac andR L Armentano ldquoInfluence of inlet conditions in wall shearstress distributions of left coronary arteries in patient-specificsimulationsrdquo Mecanica Computacional vol XXIXpp 5953ndash5960 2010
[29] B C Lopez B Calvo and P Estefanıa Patient-SpecificComputational Modeling Springer Berlin Germany 2012thedition 2012
10 Complexity
[30] D N Ghista and F Kabinejadian ldquoCoronary artery bypassgrafting hemodynamics and anastomosis design a biomedicalengineering reviewrdquo BioMedical Engineering Online vol 12no 129 2013
[31] F P Glor F P Glor B Ariff et al ldquoImage-based carotid flowreconstruction a comparison between MRI and ultrasoundrdquoPhysiological Measurement vol 25 no 6 pp 1495ndash15092004
[32] S-W Lee L Antiga and D A Steinman ldquoCorrelationsamong indicators of disturbed flow at the normal carotidbifurcationrdquo Journal of Biomechanical Engineering vol 131no 6 Article ID 061013 2009
[33] H A Himburg ldquoSpatial comparison between wall shear stressmeasures and porcine arterial endothelial permeabilityrdquo AJPHeart and Circulatory Physiology vol 286 no 5 pp 1916ndash1922 2004
[34] T Suess J Anderson L Danielson et al ldquoExamination ofnear-wall hemodynamic parameters in the renal bridgingstent of various stent graft configurations for repairing vis-ceral branched aortic aneurysmsrdquo Journal of Vascular Sur-gery vol 64 no 3 pp 788ndash796 2016
[35] H Zhang X Yu F Ji and F Sun ldquoCoronary artery aneurysmformation after drug-coatedrdquo Medicine vol 97 no 45 2018
[36] N G Gutierrez M Mathew B W McCrindle et al ldquoHe-modynamic variables in aneurysms are associated withthrombotic risk in children with Kawasaki diseaserdquo Inter-national Journal of Cardiology vol 281 pp 15ndash21 2019
[37] C Karmonik G Chintalapani T Redel et al ldquoHemody-namics at the ostium of cerebral aneurysms with relation topost-treatment changes by a virtual flow diverter a compu-tational fluid dynamics studyrdquo in Proceedings of the AnnualInternational Conference of the IEEE Engineering in Medicineand Biology Society EMBS pp 1895ndash1898 Osaka Japan July2013
[38] J T Marcus H G Smeenk J P A KuijerR J Van Der Geest R M Heethaar and A C Van RossumldquoFlow profiles in the left anterior descending and the rightcoronary artery assessed byMR velocity quantification effectsof through-plane and in-plane motion of the heartrdquo Journal ofComputer Assisted Tomography vol 23 no 4 pp 567ndash5761999
[39] Y Shi P Lawford and R Hose ldquoReview of zero-D and 1-Dmodels of blood flow in the cardiovascular systemrdquo Bio-Medical Engineering Online vol 10 no 1 p 33 2011
[40] M Kroll J Hellums L McIntire A Schafer and J MoakeldquoPlatelets and shear stressrdquo Blood vol 88 no 5pp 1525ndash1541 1996
[41] J-J Chiu and S Chien ldquoEffects of disturbed flow on vascularendothelium pathophysiological basis and clinical perspec-tivesrdquo Physiological Reviews vol 91 no 1 pp 327ndash387 2011
[42] J Hwang M H Ing A Salazar et al ldquoPulsatile versus os-cillatory shear stress regulates NADPH oxidase subunit ex-pressionrdquo Circulation Research vol 93 no 12 pp 1225ndash12322003
[43] S-i Sugiyama K Niizuma T Nakayama et al ldquoRelativeresidence time prolongation in intracranial aneurysmsrdquoNeurosurgery vol 73 no 5 pp 767ndash776 2013
Complexity 11

To confirm the reliability of the simulation results weperformed a grid independence test on the number of elementsand nodes [22] See Figure 2 to check more information of theindependence test It can be found that the simulation resultstend to be stable when the number of grids exceeds a certainstandard-e total numbers of nodes and elements for the fourmodels differed (Table 1) but they were all of the same order ofmagnitude number Blood flow simulations were performed byusing the NavierndashStokes solver in the ANSYS-CFX software(Swanson Analysis Systems Inc) -e simulation calculationassumed that the artery wall was rigid and stationary the bloodflow was Newtonian and the density and viscosity were1050kgm3 and 00035Pa s respectively Based on the Rey-nolds number the fluid is set as laminar flow -e simulationswere run for three cardiac cycles We selected a time step of00025 s to satisfy the calculation of stability conditions -emaximum residual of momentum and continuity of the it-erative calculation was set to 00001
22 Lumped Parameter Boundary Conditions -e coronaryartery blood flow simulation required careful considerationof the physiological function of the coronary circulationand microcirculation especially the drastic change inmicrocirculatory resistance due to heart contractions -iscould be simulated appropriately by using an LPM -eLPM construction method for the boundary conditions wasbased on previous research [22 23] -e LPM systemcomprised a heart left ventricle module coronary arterymodules and arterial modules -ese modules were de-veloped based on the concept of the three-elementWindkessel RCR (resistor-capacitor-resistor) model [24] asimple circuit model in which blood flow and bloodpressure were considered to be analogous to electricalcurrent and voltage and the resistance and compliance ofblood vessels were characterized by resistance and capac-itance respectively-e entire multiscale model is shown inFigure 3 -e heart module can be built using somecomponents such as power source and variable capacitoron the basis of the RCR model -e power can simulate the
blood pressure and the variable capacitor can simulate thevolume change of the ventricular during the systole anddiastole-e inlet flow via the ascending aorta was providedby the LPM heart module and the LPM heart model wasconnected to the LPM coronary artery models throughintramyocardial pressure -e components of this moduleincluded resistors capacitors inductors and diodes whichwere used to simulate coronary resistance vascular com-pliance blood flow inertia and the heart valves respec-tively -e pressurendashvolume relationship representing thevascular compliance was calculated as follows
C(t) V(t) minus V0
P(t)
1E(t)
(1)
(a) (b) (c) (d)
Figure 1 -ree-dimensional models with a normal coronary artery (Model 0) and with coronary artery aneurysms with diameters twothree and five times that of the normal diameter (Models 2x 3x and 5x respectively) (a) Model 0 (b)Model 2x (c) Model 3x (d)Model 5x
The i
nlet
area
aver
age p
ress
ure (
Pa)
Number of elements (times104)
430428426424422
420
418416414
4120 50 100 150 200 250
Figure 2 -e result of grid independence test and the trend line ofthe results
Table 1-e numbers of nodes and elements of the grid in the fourcomputational models
Model 0 Model 2x Model 3x Model 5xNodes 1098996 940577 1047183 936749Elements 1437901 1231913 1370433 1230434
Complexity 3
where V(t) and P(t) are the pressure and volume of theventricle and V0 is the reference pressure E(t) characterizesthe time-varying elastic properties and was calculated asfollows
E(t) Emin + Emax minus Emin( 1113857 middot En tn( 1113857 (2)
-e units of E used were mL and mmHg Normalizedtime-varying elasticity En(tn) was calculated using a methodbased on previous research [25] as follows
En tn( 1113857 1551
1 + tn117( 1113857219
⎡⎣ ⎤⎦tn07( 1113857
19
1 + tn07( 111385719
⎡⎣ ⎤⎦ (3)
In the present study we set Emin 0002458 andEmax 20 tn t(02 + 015tc))( -e cardiac cycle tc wasset to 08 s
Compared with normal arterial blood vessels thecoronary artery module required the addition of a mi-crocirculation module to take account of the specialphysiology of coronary arteries -is module comprised aresistor (Rv-micro) and a capacitor (Ci-micro) with thecathode of the capacitor coupled to the internal pressure ofthe heart module to simulate changes in systolic pressure-e target mean flow of every branch of the LPM coronaryarteries was determined by the area of each branch [23 26]Based on previous studies [22 27] we assumed that thetotal perfusion of the coronary arteries was 4 of thecardiac output and that the total perfusion of the left andright coronary arteries was 60 and 40 of the totalperfusion of the coronary arteries respectively As shownin Figure 2 the simulation of coronary microcirculation isto add a module on the basis of the common artery tosimulate the pressure from the left ventricle and the re-sistance change caused by the pressure change -edebugging of the entire circuit model parameters is basedon previous research [22] in which the pressure adjustmentneeds to match the patientrsquos blood pressure
-e RCR model can be used to directly simulate arterialblood vessels because these do not undergo drastic changesin resistance -e RCR boundary conditions were set as theoutlets of the descending aorta and supra-aortic arteries
-e CFD boundary conditions provided by the LPM forthe inlet and outlets of the computational model corre-sponded to different modules known as the 0D3D mul-tiscale coupled method [22 23] -e important reasons foradopting LPM are the easy-to-deploy circuit model and thecharacteristics of not requiring a mainframe computer -eeasy-to-deploy circuit model means that a complex circuitmodel composed of many different components can besimulated by programming All four 3D models shared thesame LPM because apart from the CAA lesion the pe-ripheral vascular geometry did not change between themodels this ensured changes in the geometric structure ofthe CAA were the main cause of the different simulationresults Clinical observation has shown that the coronarystructure of the distal end of the coronary artery is notaffected by the CAA this was important evidence supportingthe selection of this method
3 Results
31 Mass Flow and Pressure Waveforms Figure 4 shows thecomputedmass flow and pressure over a cardiac cycle for theascending aorta (the inlet to the model) the descendingaorta an outlet artery and a coronary artery branch (ex-amples of outlets from the model) for the four 3D models-e results confirmed that except for the mass flow at thecoronary artery boundary mass flow in the outlets peakedduring systole -e coronary mass flow peaked during di-astole -ese results confirmed that the expected life-likecharacteristics of the coronary circulation which bloodsupply mainly occurred during diastole were successfullycaptured in the model [22] High systolic intra-myocardialpressure resulted in increased distal downstream resistance
A1
A2 A3 A4
a
bc
de
fg
ijk
lh
m
n
DAO
AAO
LPM coronary artery module coupled with 3D outlet
(coronary andashn)
LPM artery module coupled with outlet
DAO A1ndashA4)
LPM heart module coupled with 3D inlet (AAO)
Figure 3 Details of the multiscale model used in the study showing the coupled interface between the lumped parameter model(LPM) and the three-dimensional model an coronary arteries A1A4 arteries AAO ascending aorta DAO descending aorta RCRresistor-capacitor-resistor
4 Complexity
and decreased blood flow through the coronary artery theopposite was the case during diastole Changes in the di-ameter of the CAA did not have a significant effect oncoronary outlet flow
32 Wall Shear Stress -e WSS is the force per unit areaexerted by the wall on the fluid in a direction along the planeof the local tangent [28] calculated as follows
τω 4μQ
πR3 (4)
where μ represents the blood viscosity Q is mass-flowrate and R is vessel radius Previous studies have reportedan association between thrombosis formation and lowWSS [29] -e area average values of WSS in coronaryartery aneurysm over a cardiac cycle in the four models
are listed in Table 2 and the values over a cycle anddistribution contours are shown in Figures 5 and 6 -eaverage WSS over a cycle in Model 0 (with no CAA) was351 Pa -e averages for Models 2x 3x and 5x were 068026 and 008 Pa respectively substantially reduced in theCAA due to blood flow stagnation and recirculation withthe reduction increasing in CAAs of greater diameters-e distribution contours in Figure 6 confirm that theCAA results only in local hemodynamic disturbanceswithout wider hemodynamic changes in the arteries Atsome distance downstream in the coronary artery thecoronary diameter and WSS both return to normal levels
33 Oscillatory Shear Index OSI is a parameter thatquantifies the magnitude of theWSS and directional changes[18] calculated as follows
Inle
t AAO
Out
let D
AOO
utle
t A1
Out
let f
Mas
s flo
w (m
lmin
)
Pres
sure
(Pa)
Pres
sure
(Pa)
Pres
sure
(Pa)
Pres
sure
(Pa)
Mas
s flo
w (m
lmin
)M
ass f
low
(mlm
in)
Mas
s flo
w (m
lmin
)
20000
00
0
16500
10000008 08
13000
ndash20008
17000
100000 08
1600
00 08
16000
100000 08
45
00 08
Mass flow Pressure
16000
8000080
Cardiac cycle (s)
Cardiac cycle (s) Cardiac cycle (s)
Cardiac cycle (s)Cardiac cycle (s)
Cardiac cycle (s)
Cardiac cycle (s) Cardiac cycle (s)
Model 0
Model 3x Model 5x
Model 2x
DAO
A1
fAAO
Model 0Model 2x
Model 3xModel 5x
Figure 4 Mass flow and pressure curves for the inlet (ascending aorta AAO) and three outlets (descending aorta (DAO) artery 1 (A1) andcoronary artery f ) over a cardiac cycle
Complexity 5
OSI 05 times 1 minus1113938
T
0 τωdt11138681113868111386811138681113868
11138681113868111386811138681113868
1113938T
0 τω1113868111386811138681113868
1113868111386811138681113868dt
⎛⎝ ⎞⎠ (5)
where T is the cardiac cycle OSI has values in the range 005with 0 representing undisturbed flow with no change in thedirection of the shear stress and 05 representing disturbedflow with oscillating shear stress Previous studies havereported an association between high OSI and the formationof intimal hyperplasia [30] -e average values of OSI in theaneurysm and OSI distribution contours are shown in Table 2and Figure 7 respectively -e average value of OSI over thecardiac cycle inModel 0 was 001-e averages forModels 2x3x and 5x were substantially higher at 003 013 and 030respectively Previous studies have pointed out that when OSIis greater than 02 it will cause endothelial cell damage [31]As shown in Table 3 the ratio of high OSI area in theaneurysm to the area of aneurysm was 0 125 253 and662 respectively Model 0 has OSI close to zero throughoutthe cardiac cycle and the flow in Model 0 is unidirectionalwithout circulation Normal coronary blood flow is unidi-rectional usually without flow recirculation so the OSI of thenormal coronary artery (Model 0) was close to zerothroughout the entire cardiac cycle-e highOSI values in theCAA models which reached 30 times higher in model 5xwere due to the increased storage time resulting from theincreased size of the cavity which led to recirculation withinthe CAA lesion -e effect on OSI was locally confined there
was little difference between the OSI in the distal coronaryarteries in Models 2x 3x and 5x and those in Model 0
34 Relative Residence Time -e RRT is an indicator thatcomprehensively characterizes the values and oscillation ofWSS [32] as well as the time of local blood flow and vascularinteraction [33] It is calculated as follows
RRT 1
(1 minus 2 middot OSI) middot TAWSS (6)
where
TAWSS WSS
T (7)
Here TAWSS isWSS average over one cardiac cycle andT is a cardiac cycle Figure 8 shows the distribution contoursfor RRT in the four models and Table 2 shows the areaaverage values of RRT within the CAA lesion over thecardiac cycle -e average value of RRT in Model 0 was038 Paminus1 -e averages for Models 2x 3x and 5x weresubstantially higher at 288 2312 and 5159 Paminus1 respec-tively showing a dramatic increase in RRT with increasingdiameter of the CAA Studies have reported a significantlyincreased risk of thrombosis when RRT is gt10 Paminus1 [12 34]As shown in Table 3 the ratio of high RRT area in theaneurysm to the area of aneurysm was 0 05 271 and786 respectively -e increased diameter of the CAAmakes it easier for blood to remain resident within ithampering the blood flow to the distal coronary artery -echange in RRT was locally confined to the CAA there waslittle difference between the RRT in the distal coronaryarteries in Models 2x 3x and 5x and that in the distalcoronary artery in Model 0
4 Discussion
We have shown that the relationship between hemodynamiceffects and different diameters of CAAs can be achieved byusing CFD simulation method direct comparison withvirtual control case based on the same patient We foundthat changes in the diameter of CAA have a strong effect onlocal hemodynamics while they do not have a significanteffect on global hemodynamics -e potential risk ofthrombosis increases significantly with increasing CAAdiameter indicated through decreasing WSS increasing OSIand RRT -is research will allow us to estimate thethrombosis risk of CAAs from a hemodynamic perspectiveand provide more comprehensive support for doctorsrsquodecisions
When making treatment decisions about CAAs doctorstypically depend on their own clinical experience [35] -ismay be because of the lack of useful diagnostic tools -ecurrent used tool is the method of imaging which canprovide geometric information and almost no other infor-mation -e lack of other information cannot provide morehelp for the doctorrsquos diagnosis -erefore it is necessary tofind a way to provide more information to help the doctor Ithas been shown that WSS over aneurysmal regions is
Table 2 Average values over a cardiac cycle for wall shear stress(WSS) the oscillatory shear index (OSI) and relative residencetime (RRT) in the coronary artery aneurysm
Model 0 Model2x
Model3x
Model5x
Area averageWSS (Pa) 351 068 026 008Area average OSI 001 003 013 030Area average RRT(Paminus1) 038 288 2312 5159
0
45
4
35
3
252
15
1
05
Wal
l she
ar st
ress
(Pa)
0 01 02 03 04 05 06 07 08Time (s)
Model 0Model 2x
Model 3xModel 5x
Figure 5 Wall shear stress in the coronary artery aneurysm over acardiac cycle for the four models
6 Complexity
associated with risk of thrombosis and that is a morepredictive factor of thrombosis than aneurysm diameter[36] We confirmed that hemodynamic research is beneficialfor aneurysm diagnosis and treatment [37] -erefore in
this study we quantitatively calculated the hemodynamicparameters of CAA of different diameters in order to esti-mate the relationship between the risk level of thrombosisand the size of CAA -e results showed that CAAs only
Front Back
OSI0495
0330
0165
0000
Model 0
Model 2x
Model 3x
Model 5x
Figure 7 Oscillatory shear index (OSI) distribution in the coronary artery aneurysm for the four models
Table 3 -e area of high OSI and RRT in the aneurysm and the area of aneurysm
Model 0 Model 2x Model 3x Model 5xHigh OSI areaCAA area (mm2) (ratio) 046362 (0) 952976238 (125) 29853117997 (253) 141389213579 (662)High RRT areaCAA area (mm2) (ratio) 046362 (0) 381276238 (05) 31977117997 (271) 167873213579 (786)
Front Back
Model 0
Model 2x
Model 3x
Model 5x
WSS
(Pa)
6936
4624
2312
0000
Figure 6 Wall shear stress (WSS) distribution in the coronary artery aneurysm at its peak (t 02 s) for the four models
Complexity 7
affect the blood flow and pressure within the region of thelesion itself with little effect on global blood flow Howeverthere were substantial changes in local hemodynamic pa-rameters related to thrombosis in the lesion locationCompared with the model without a lesion all three CAAmodels showed low WSS high OSI and high RRT withthese changes exacerbated as the CAA diameter increased-ese changes were the results of the sudden increase in thediameter of the lumen on entering the CAA -ese resultssuggest there may be a high correlation between CAA di-ameter and the risk of thrombosis CAA hemodynamicstudies may therefore allow the development of a prelimi-nary classification of the risk of thrombosis helping toimprove the effectiveness of anticoagulation therapy andfacilitating better personalization of treatment according to aquantitative hemodynamic plan
Simulation provides a powerful and effective method forestimating important hemodynamic parameters that aredifficult to measure As mentioned above except mass-flowrate which can be easily detected by non-invasive ultra-sound other parameters WSS OSI and RRT cannot bedirectly measured which are usually obtained through invitro experiments or indirect measurements Simulation is anon-invasive way providing a low cost way and avoiding thepotential risk of some invasive ways to obtain hemodynamicparameters
LPM boundary conditions can provide realistic physi-ologic flow conditions as what has been confirmed inprevious studies [38 39] In addition the coronary mi-crocirculation was introduced into the downstreamboundary condition via the LPM Resistance and pressurechanges downstream of the coronary artery could be
accurately captured in this way helping to ensure the ac-curate simulation of physiological conditions in the coro-nary artery -ere was no difference between the models inthe peripheral vascular structure so the CFD models sharedthe same LPM minimizing the impact of factors other thanthe diameter of the CAA -us the differences in resultsbetween the models were due to the differences in CAAdiameters
As the diameter of the CAA increased theWSS in the CAAlesion area progressively decreased with the WSS in Model 5xobserved to be gt10 times lower than that of the normalcoronary artery (Model 0) Parallel plate flow experiments haveshown that a large number of platelets accumulate at locationswith low WSS (lt04 Pa) [40] and animal endothelial cell ex-periments have shown that thrombosis is associated with adecrease in WSS to within the range 00770279Pa [10] In thepresent study the area average values for WSS in Models 3xand 5x were within this range suggesting that CAAs withdiametersgt3 times that of the normal artery are likely to carry ahigh risk of thrombosis Although the area average WSS forModel 2x was much lower than that of the model withoutCAA it was higher than 04Pa suggesting that CAAs withdiameters double that of the normal artery may not be at highrisk of thrombosis Another important pathophysiologicalfactor in vascular disease is endothelial dysfunction Low WSScan locally inhibit the production of certain important sub-stances such as NO [41] An abnormal response to vasodilationagents including the deactivation of NO by free radicals due tothe impairment of acetylcholine or endothelial NO synthasecan lead to abnormal vasoconstriction which can be associatedwith endothelial dysfunction [41] In addition platelets areprone to aggregation in areas of low WSS which further
Front Back
RRT99083
66055
33028
0000
(Pandash1)
Model 0
Model 2x
Model 3x
Model 5x
Figure 8 Relative residence time (RRT) distribution in the coronary artery aneurysm for the four models
8 Complexity
exacerbates the risk of thrombosis WSS in the CAA lesion ofModel 2x was lower than that in the normal model howeverfurther development is still to be studied just taking WSS as areference -e risk for thrombosis in CAAs progresses withincreasing diameter so the risk associatedwithModel 2xwouldbe lower than that for Models 3x and 5x -e development ofCAAs needs further study Although studies have investigatedthe association between WSS and thrombosis the currentunderstanding is not yet comprehensive -erefore the pos-sibility of WSS and thrombosis in the corresponding in vitroexperiments should be the focus of continued research
-e OSIs for the CAAs increased rapidly with increasingdiameter of the lesion with the OSI in Model 5x around 30times greater than that of the normal coronary artery (whichwas close to zero throughout the CAA) Previous studieshave pointed out that when OSI is greater than 02 it willcause endothelial cell damage [31] -e high OSI area(OSIgt 02) ratio increased from 01 to 662 betweenModel 0 and Model 5x In vivo experimental studies ofporcine aortas have reported that disturbed flow (ie anincrease in OSI) promoted the expression of proin-flammatory cytokines in endothelial cells [11] In additionan in vitro study of bovine endothelial cells reported that theexpression of monocyte chemoattractant protein-1 could beinduced by applying a low-amplitude oscillating shear stressof 03 Pa at 1Hz (equivalent to an OSI of 05) and thishemodynamic environment enhanced the binding of en-dothelial cells to monocytes [42] -ese findings suggest thatthe elevated OSI values observed in the CAA models may beassociated with conditions that can trigger thrombosis
-e RRT values for the CAAs increased dramatically withincreasing diameters of the lesions with the RRT for Model5xgt100 times greater than that of the normal coronary artery-e high RRTarea ratio increased from 01 to 786 betweenModel 0 and Model 5x -ese findings indicate that the bloodflow in the CAA recirculates when the diameter of the lumenincreases resulting in prolonged contact time between the CAAwall and the blood Studies have reported a significantly in-creased risk of thrombosis when RRT is gt10Paminus1 [12 34] -eRRTvalues forModels 3x and 5x in the present study were bothgt10Paminus1 suggesting a high risk of thrombosis when the di-ameter of a CAA exceeds three times that of the normal cor-onary artery Conversely the RRTforModel 2xwasmuch lowerthan 10Paminus1 suggesting that the risk of thrombosis may be lowwhen the diameter of the CAA is only double that of the normalartery Although there have been various studies of the rela-tionship between RRTand aneurysms [43] the current state ofknowledge remains insufficient for patient classification forexample there are no appropriate ranges of RRT values fordistinguishing the risk level of thrombosis which needs furtherstudy
In summary the comparison of our modeling resultswith the findings of previous studies suggested that the lowWSS high OSI and high RRT observed in the CAAs wouldsignificantly increase the risk of thrombosis However therisk varied considerably between the different diameters ofCAA -e WSS OSI and RRT values for Models 3x and 5xall suggested a high risk of thrombosis based on the previousstudy results-us for CAAs with diameters gt3 times that of
the normal coronary artery the risk of uncertainty withconservative treatment may be higher than the risk asso-ciated with surgery suggesting that the surgical operationshould be considered Conversely although the WSS OSIand RRT values for Model 2x were unfavorable comparedwith those of the model of the normal coronary arteryimplying an increased risk of thrombosis the magnitude ofthese differences was insufficient to support a prediction ofthe future development of the CAA For CAAs with a di-ameter up to two times that of the normal coronary arteryconservative drug treatment may be the better optionavoiding the risks associated with surgery
-e limitations of this study are as follows First this studyhas only one patientrsquos data and the conclusion may be ac-cidental We need to use more data for research Secondly animportant assumption used in the CFD calculation is the rigidwall where in fact elastic walls should be used In particularthe coronary artery will deform greatly as the heart contractswhich can be solved by two-way FSI in the future
5 Conclusion
-e evaluation of the relationship between hemodynamiceffects and different diameters of CAAs was performed inthis research through the CFD simulation method -erelationship between thrombosis risk and the size of theCAA diameter could be preliminarily evaluated from ahemodynamic perspective
We found that as the diameter of the CAA increased therisk of thrombosis increased substantially -e results sug-gested that when the diameter of a CAA is small (less thandouble that of the normal coronary artery) the risk ofthrombosis may be relatively low suggesting that medica-tion may be a sufficient approach for the patient avoidingthe uncertain risks associated with surgery If the diameter ofCAA is large (gt3 times that of the normal coronary artery)there may be a high risk of thrombosis and surgicaltreatment could be considered A similar approach could betaken in future studies to systematically assess the risk as-sociated with different shapes sizes and locations of an-eurysms Such approaches may form the basis for moresophisticated hemodynamic-based risk stratificationmethods supporting clinical decision-making in assessmentof CAA
Data Availability
-e data used to support the findings of this study areavailable from the corresponding author upon request
Conflicts of Interest
-e authors declare no conflicts of interest
Acknowledgments
-is research was supported by the National Natural ScienceFoundation of China (nos 11832003 and 11772016) andJSPS KAKENHI under Grant no JP18K18355 -is researchwas partially supported by the Creation of a Development
Complexity 9
Platform for ImplantableWearable Medical Devices by aNovel Physiological Data Integration System of the Programon Open Innovation Platform with Enterprises ResearchInstitute and Academia (OPERA) from the Japan Scienceand Technology Agency (JST) -is research was also sup-ported by Collaborative Research Project 2020 Institute ofFluid Science Tohoku University (J20R001) with the GrantNumber JP18K18355
References
[1] H Kato T Sugimura T Akagi et al ldquoLong-term conse-quences of kawasaki diseaserdquo Circulation vol 94 no 6pp 1379ndash1385 1996
[2] S A Sherif O O Tok O Taskoylu O Goktekin andI D Kilic ldquoCoronary artery aneurysms a review of theepidemiology pathophysiology diagnosis and treatmentrdquoFrontiers in Cardiovascular Medicine vol 4 2017
[3] E Beckmann S Rustum S Marquardt et al ldquoSurgicaltreatment of coronary artery aneurysmsrdquo Journal of CardiacSurgery vol 32 no 11 pp 674ndash679 2017
[4] M Syed M Lesch and A D Syed ldquoCoronary artery aneu-rysm a reviewrdquo Progress in Cardiovascular Diseases vol 40no 1 pp 77ndash84 1997
[5] G G Hartnell B M Parnell and R B Pridie ldquoCoronaryartery ectasia Its prevalence and clinical significance in 4993patientsrdquo British Heart Journal vol 54 no 4 1985
[6] A Satran B A Bart C R Henry et al ldquoIncreased prevalenceof coronary artery aneurysms among cocaine usersrdquo Circu-lation vol 111 no 19 pp 2424ndash2429 2005
[7] O Topaz M S Rutherford S M Bojack et al ldquoGiant an-eurysms of coronary arteries and saphenous vein graftsangiographic findings and histopathological correlatesrdquoCardiovascular Pathology vol 14 no 6 pp 298ndash302 2005
[8] A P Antoniadis Y S Chatzizisis and G D GiannoglouldquoPathogenetic mechanisms of coronary ectasiardquo InternationalJournal of Cardiology vol 130 no 3 pp 335ndash343 2008
[9] J B Gordon A M Kahn and J C Burns ldquoWhen childrenwith kawasaki disease grow uprdquo Journal of the AmericanCollege of Cardiology vol 54 no 21 pp 1911ndash1920 2009
[10] P Sriramarao L Languino and D Altieri ldquoFibrinogenmediates leukocyte-endothelium bridging in vivo at low shearforcesrdquo Blood vol 88 no 9 pp 3416ndash3423 1996
[11] A G Passerini D C Polacek C Shi et al ldquoCoexistingproinflammatory and antioxidative endothelial transcriptionprofiles in a disturbed flow region of the adult porcine aortardquoProceedings of the National Academy of Sciences vol 101no 89 pp 2482ndash2487
[12] U Morbiducci D Gallo R Ponzini et al ldquoQuantitativeanalysis of bulk flow in image-based hemodynamic models ofthe carotid bifurcation the influence of outflow conditions astest caserdquo Annals of Biomedical Engineering vol 38 no 12pp 3688ndash3705 2010
[13] T Ohkubo R Fukazawa E Ikegami and S Ogawa ldquoReducedshear stress and disturbed flow may lead to coronary aneu-rysm and thrombus formationsrdquo Pediatrics Internationalvol 49 no 1 pp 1ndash7 2007
[14] H Anzai T Watanabe X Han et al ldquoEndothelial cell dis-tributions and migration under conditions of flow shear stressaround a stent wirerdquo Technology and Health Care vol 28no 4 pp 345ndash354 2020
[15] M Zhang Y Li X Zhao et al ldquoHaemodynamic effects ofstent diameter and compaction ratio on flow-diversion
treatment of intracranial aneurysms a numerical study of asuccessful and an unsuccessful caserdquo Journal of Biomechanicsvol 58 pp 179ndash186 2017
[16] H Anzai B Chopard and M Ohta ldquoCombinational opti-mization of strut placement for intracranial stent using arealistic aneurysmrdquo Journal of Flow Control Measurement ampVisualization vol 2 no 2 pp 67ndash77 2014
[17] J P Ku M T Draney F R Arko et al ldquoIn vivo validation ofnumerical prediction of blood flow in arterial bypass graftsrdquoAnnals of Biomedical Engineering vol 30 no 6 pp 743ndash7522002
[18] A R Soler F Kabinejadian M A Slevin P J Bartolo andA Keshmiri ldquoOptimisation of a novel spiral-inducing bypassgraft using computational fluid dynamicsrdquo Scientific Reportsvol 7 no 1 p 1865 2017
[19] H Zhang L Li C Cheng and X Sun ldquoClinical value ofhomodynamic numerical simulation applied in the treatmentof cerebral aneurysmrdquo Experimental and Gerapeutic Medi-cine vol 4 no 6 pp 5401ndash5494 2017
[20] A S Les S C Shadden C A Figueroa et al ldquoQuantificationof hemodynamics in abdominal aortic aneurysms during restand exercise using magnetic resonance imaging and com-putational fluid dynamicsrdquo Annals of Biomedical Engineeringvol 38 no 4 pp 1288ndash1313 2010
[21] M Piccinelli A Veneziani D A Steinman A Remuzzi andL Antiga ldquoA framework for geometric analysis of vascularstructures application to cerebral aneurysmsrdquo IEEE Trans-actions on Medical Imaging vol 28 no 8 pp 1141ndash11552009
[22] H J Kim I E Vignon-Clementel J S CooganC A Figueroa K E Jansen and C A Taylor ldquoPatient-specific modeling of blood flow and pressure in humancoronary arteriesrdquo Annals of Biomedical Engineering vol 38no 10 pp 3195ndash3209 2010
[23] C A Taylor T A Fonte and J K Min ldquoComputational fluiddynamics applied to cardiac computed tomography fornoninvasive quantification of fractional flow reserverdquo Journalof the American College of Cardiology vol 61 no 22pp 2233ndash2241 2013
[24] I E V Clementel C A Figueroa K E Jansen andC A Taylor ldquoOutflow boundary conditions for 3D simula-tions of non-periodic blood flow and pressure fields in de-formable arteriesrdquo Computer Methods in Biomechanics andBiomedical Engineering vol 13 no 5 pp 625ndash640 2010
[25] N Stergiopulos J J Meister and N Westerhof ldquoDetermi-nants of stroke volume and systolic and diastolic aorticpressurerdquoGe American Journal of Physiology vol 270 no 6pp 2050ndash2059 1996
[26] M Zamir P Sinclair and T H Wonnacott ldquoRelation be-tween diameter and flow in major branches of the arch of theaortardquo Journal of Biomechanics vol 25 no 11 pp 1303ndash13101992
[27] K Johnson P Sharma and J Oshinski ldquoCoronary artery flowmeasurement using navigator echo gated phase contrastmagnetic resonance velocity mapping at 30 teslardquo Journal ofBiomechanics vol 41 no 3 pp 595ndash602 2008
[28] F P Salvuccia C A Perazzob S Sallesa J G Barrac andR L Armentano ldquoInfluence of inlet conditions in wall shearstress distributions of left coronary arteries in patient-specificsimulationsrdquo Mecanica Computacional vol XXIXpp 5953ndash5960 2010
[29] B C Lopez B Calvo and P Estefanıa Patient-SpecificComputational Modeling Springer Berlin Germany 2012thedition 2012
10 Complexity
[30] D N Ghista and F Kabinejadian ldquoCoronary artery bypassgrafting hemodynamics and anastomosis design a biomedicalengineering reviewrdquo BioMedical Engineering Online vol 12no 129 2013
[31] F P Glor F P Glor B Ariff et al ldquoImage-based carotid flowreconstruction a comparison between MRI and ultrasoundrdquoPhysiological Measurement vol 25 no 6 pp 1495ndash15092004
[32] S-W Lee L Antiga and D A Steinman ldquoCorrelationsamong indicators of disturbed flow at the normal carotidbifurcationrdquo Journal of Biomechanical Engineering vol 131no 6 Article ID 061013 2009
[33] H A Himburg ldquoSpatial comparison between wall shear stressmeasures and porcine arterial endothelial permeabilityrdquo AJPHeart and Circulatory Physiology vol 286 no 5 pp 1916ndash1922 2004
[34] T Suess J Anderson L Danielson et al ldquoExamination ofnear-wall hemodynamic parameters in the renal bridgingstent of various stent graft configurations for repairing vis-ceral branched aortic aneurysmsrdquo Journal of Vascular Sur-gery vol 64 no 3 pp 788ndash796 2016
[35] H Zhang X Yu F Ji and F Sun ldquoCoronary artery aneurysmformation after drug-coatedrdquo Medicine vol 97 no 45 2018
[36] N G Gutierrez M Mathew B W McCrindle et al ldquoHe-modynamic variables in aneurysms are associated withthrombotic risk in children with Kawasaki diseaserdquo Inter-national Journal of Cardiology vol 281 pp 15ndash21 2019
[37] C Karmonik G Chintalapani T Redel et al ldquoHemody-namics at the ostium of cerebral aneurysms with relation topost-treatment changes by a virtual flow diverter a compu-tational fluid dynamics studyrdquo in Proceedings of the AnnualInternational Conference of the IEEE Engineering in Medicineand Biology Society EMBS pp 1895ndash1898 Osaka Japan July2013
[38] J T Marcus H G Smeenk J P A KuijerR J Van Der Geest R M Heethaar and A C Van RossumldquoFlow profiles in the left anterior descending and the rightcoronary artery assessed byMR velocity quantification effectsof through-plane and in-plane motion of the heartrdquo Journal ofComputer Assisted Tomography vol 23 no 4 pp 567ndash5761999
[39] Y Shi P Lawford and R Hose ldquoReview of zero-D and 1-Dmodels of blood flow in the cardiovascular systemrdquo Bio-Medical Engineering Online vol 10 no 1 p 33 2011
[40] M Kroll J Hellums L McIntire A Schafer and J MoakeldquoPlatelets and shear stressrdquo Blood vol 88 no 5pp 1525ndash1541 1996
[41] J-J Chiu and S Chien ldquoEffects of disturbed flow on vascularendothelium pathophysiological basis and clinical perspec-tivesrdquo Physiological Reviews vol 91 no 1 pp 327ndash387 2011
[42] J Hwang M H Ing A Salazar et al ldquoPulsatile versus os-cillatory shear stress regulates NADPH oxidase subunit ex-pressionrdquo Circulation Research vol 93 no 12 pp 1225ndash12322003
[43] S-i Sugiyama K Niizuma T Nakayama et al ldquoRelativeresidence time prolongation in intracranial aneurysmsrdquoNeurosurgery vol 73 no 5 pp 767ndash776 2013
Complexity 11

where V(t) and P(t) are the pressure and volume of theventricle and V0 is the reference pressure E(t) characterizesthe time-varying elastic properties and was calculated asfollows
E(t) Emin + Emax minus Emin( 1113857 middot En tn( 1113857 (2)
-e units of E used were mL and mmHg Normalizedtime-varying elasticity En(tn) was calculated using a methodbased on previous research [25] as follows
En tn( 1113857 1551
1 + tn117( 1113857219
⎡⎣ ⎤⎦tn07( 1113857
19
1 + tn07( 111385719
⎡⎣ ⎤⎦ (3)
In the present study we set Emin 0002458 andEmax 20 tn t(02 + 015tc))( -e cardiac cycle tc wasset to 08 s
Compared with normal arterial blood vessels thecoronary artery module required the addition of a mi-crocirculation module to take account of the specialphysiology of coronary arteries -is module comprised aresistor (Rv-micro) and a capacitor (Ci-micro) with thecathode of the capacitor coupled to the internal pressure ofthe heart module to simulate changes in systolic pressure-e target mean flow of every branch of the LPM coronaryarteries was determined by the area of each branch [23 26]Based on previous studies [22 27] we assumed that thetotal perfusion of the coronary arteries was 4 of thecardiac output and that the total perfusion of the left andright coronary arteries was 60 and 40 of the totalperfusion of the coronary arteries respectively As shownin Figure 2 the simulation of coronary microcirculation isto add a module on the basis of the common artery tosimulate the pressure from the left ventricle and the re-sistance change caused by the pressure change -edebugging of the entire circuit model parameters is basedon previous research [22] in which the pressure adjustmentneeds to match the patientrsquos blood pressure
-e RCR model can be used to directly simulate arterialblood vessels because these do not undergo drastic changesin resistance -e RCR boundary conditions were set as theoutlets of the descending aorta and supra-aortic arteries
-e CFD boundary conditions provided by the LPM forthe inlet and outlets of the computational model corre-sponded to different modules known as the 0D3D mul-tiscale coupled method [22 23] -e important reasons foradopting LPM are the easy-to-deploy circuit model and thecharacteristics of not requiring a mainframe computer -eeasy-to-deploy circuit model means that a complex circuitmodel composed of many different components can besimulated by programming All four 3D models shared thesame LPM because apart from the CAA lesion the pe-ripheral vascular geometry did not change between themodels this ensured changes in the geometric structure ofthe CAA were the main cause of the different simulationresults Clinical observation has shown that the coronarystructure of the distal end of the coronary artery is notaffected by the CAA this was important evidence supportingthe selection of this method
3 Results
31 Mass Flow and Pressure Waveforms Figure 4 shows thecomputedmass flow and pressure over a cardiac cycle for theascending aorta (the inlet to the model) the descendingaorta an outlet artery and a coronary artery branch (ex-amples of outlets from the model) for the four 3D models-e results confirmed that except for the mass flow at thecoronary artery boundary mass flow in the outlets peakedduring systole -e coronary mass flow peaked during di-astole -ese results confirmed that the expected life-likecharacteristics of the coronary circulation which bloodsupply mainly occurred during diastole were successfullycaptured in the model [22] High systolic intra-myocardialpressure resulted in increased distal downstream resistance
A1
A2 A3 A4
a
bc
de
fg
ijk
lh
m
n
DAO
AAO
LPM coronary artery module coupled with 3D outlet
(coronary andashn)
LPM artery module coupled with outlet
DAO A1ndashA4)
LPM heart module coupled with 3D inlet (AAO)
Figure 3 Details of the multiscale model used in the study showing the coupled interface between the lumped parameter model(LPM) and the three-dimensional model an coronary arteries A1A4 arteries AAO ascending aorta DAO descending aorta RCRresistor-capacitor-resistor
4 Complexity
and decreased blood flow through the coronary artery theopposite was the case during diastole Changes in the di-ameter of the CAA did not have a significant effect oncoronary outlet flow
32 Wall Shear Stress -e WSS is the force per unit areaexerted by the wall on the fluid in a direction along the planeof the local tangent [28] calculated as follows
τω 4μQ
πR3 (4)
where μ represents the blood viscosity Q is mass-flowrate and R is vessel radius Previous studies have reportedan association between thrombosis formation and lowWSS [29] -e area average values of WSS in coronaryartery aneurysm over a cardiac cycle in the four models
are listed in Table 2 and the values over a cycle anddistribution contours are shown in Figures 5 and 6 -eaverage WSS over a cycle in Model 0 (with no CAA) was351 Pa -e averages for Models 2x 3x and 5x were 068026 and 008 Pa respectively substantially reduced in theCAA due to blood flow stagnation and recirculation withthe reduction increasing in CAAs of greater diameters-e distribution contours in Figure 6 confirm that theCAA results only in local hemodynamic disturbanceswithout wider hemodynamic changes in the arteries Atsome distance downstream in the coronary artery thecoronary diameter and WSS both return to normal levels
33 Oscillatory Shear Index OSI is a parameter thatquantifies the magnitude of theWSS and directional changes[18] calculated as follows
Inle
t AAO
Out
let D
AOO
utle
t A1
Out
let f
Mas
s flo
w (m
lmin
)
Pres
sure
(Pa)
Pres
sure
(Pa)
Pres
sure
(Pa)
Pres
sure
(Pa)
Mas
s flo
w (m
lmin
)M
ass f
low
(mlm
in)
Mas
s flo
w (m
lmin
)
20000
00
0
16500
10000008 08
13000
ndash20008
17000
100000 08
1600
00 08
16000
100000 08
45
00 08
Mass flow Pressure
16000
8000080
Cardiac cycle (s)
Cardiac cycle (s) Cardiac cycle (s)
Cardiac cycle (s)Cardiac cycle (s)
Cardiac cycle (s)
Cardiac cycle (s) Cardiac cycle (s)
Model 0
Model 3x Model 5x
Model 2x
DAO
A1
fAAO
Model 0Model 2x
Model 3xModel 5x
Figure 4 Mass flow and pressure curves for the inlet (ascending aorta AAO) and three outlets (descending aorta (DAO) artery 1 (A1) andcoronary artery f ) over a cardiac cycle
Complexity 5
OSI 05 times 1 minus1113938
T
0 τωdt11138681113868111386811138681113868
11138681113868111386811138681113868
1113938T
0 τω1113868111386811138681113868
1113868111386811138681113868dt
⎛⎝ ⎞⎠ (5)
where T is the cardiac cycle OSI has values in the range 005with 0 representing undisturbed flow with no change in thedirection of the shear stress and 05 representing disturbedflow with oscillating shear stress Previous studies havereported an association between high OSI and the formationof intimal hyperplasia [30] -e average values of OSI in theaneurysm and OSI distribution contours are shown in Table 2and Figure 7 respectively -e average value of OSI over thecardiac cycle inModel 0 was 001-e averages forModels 2x3x and 5x were substantially higher at 003 013 and 030respectively Previous studies have pointed out that when OSIis greater than 02 it will cause endothelial cell damage [31]As shown in Table 3 the ratio of high OSI area in theaneurysm to the area of aneurysm was 0 125 253 and662 respectively Model 0 has OSI close to zero throughoutthe cardiac cycle and the flow in Model 0 is unidirectionalwithout circulation Normal coronary blood flow is unidi-rectional usually without flow recirculation so the OSI of thenormal coronary artery (Model 0) was close to zerothroughout the entire cardiac cycle-e highOSI values in theCAA models which reached 30 times higher in model 5xwere due to the increased storage time resulting from theincreased size of the cavity which led to recirculation withinthe CAA lesion -e effect on OSI was locally confined there
was little difference between the OSI in the distal coronaryarteries in Models 2x 3x and 5x and those in Model 0
34 Relative Residence Time -e RRT is an indicator thatcomprehensively characterizes the values and oscillation ofWSS [32] as well as the time of local blood flow and vascularinteraction [33] It is calculated as follows
RRT 1
(1 minus 2 middot OSI) middot TAWSS (6)
where
TAWSS WSS
T (7)
Here TAWSS isWSS average over one cardiac cycle andT is a cardiac cycle Figure 8 shows the distribution contoursfor RRT in the four models and Table 2 shows the areaaverage values of RRT within the CAA lesion over thecardiac cycle -e average value of RRT in Model 0 was038 Paminus1 -e averages for Models 2x 3x and 5x weresubstantially higher at 288 2312 and 5159 Paminus1 respec-tively showing a dramatic increase in RRT with increasingdiameter of the CAA Studies have reported a significantlyincreased risk of thrombosis when RRT is gt10 Paminus1 [12 34]As shown in Table 3 the ratio of high RRT area in theaneurysm to the area of aneurysm was 0 05 271 and786 respectively -e increased diameter of the CAAmakes it easier for blood to remain resident within ithampering the blood flow to the distal coronary artery -echange in RRT was locally confined to the CAA there waslittle difference between the RRT in the distal coronaryarteries in Models 2x 3x and 5x and that in the distalcoronary artery in Model 0
4 Discussion
We have shown that the relationship between hemodynamiceffects and different diameters of CAAs can be achieved byusing CFD simulation method direct comparison withvirtual control case based on the same patient We foundthat changes in the diameter of CAA have a strong effect onlocal hemodynamics while they do not have a significanteffect on global hemodynamics -e potential risk ofthrombosis increases significantly with increasing CAAdiameter indicated through decreasing WSS increasing OSIand RRT -is research will allow us to estimate thethrombosis risk of CAAs from a hemodynamic perspectiveand provide more comprehensive support for doctorsrsquodecisions
When making treatment decisions about CAAs doctorstypically depend on their own clinical experience [35] -ismay be because of the lack of useful diagnostic tools -ecurrent used tool is the method of imaging which canprovide geometric information and almost no other infor-mation -e lack of other information cannot provide morehelp for the doctorrsquos diagnosis -erefore it is necessary tofind a way to provide more information to help the doctor Ithas been shown that WSS over aneurysmal regions is
Table 2 Average values over a cardiac cycle for wall shear stress(WSS) the oscillatory shear index (OSI) and relative residencetime (RRT) in the coronary artery aneurysm
Model 0 Model2x
Model3x
Model5x
Area averageWSS (Pa) 351 068 026 008Area average OSI 001 003 013 030Area average RRT(Paminus1) 038 288 2312 5159
0
45
4
35
3
252
15
1
05
Wal
l she
ar st
ress
(Pa)
0 01 02 03 04 05 06 07 08Time (s)
Model 0Model 2x
Model 3xModel 5x
Figure 5 Wall shear stress in the coronary artery aneurysm over acardiac cycle for the four models
6 Complexity
associated with risk of thrombosis and that is a morepredictive factor of thrombosis than aneurysm diameter[36] We confirmed that hemodynamic research is beneficialfor aneurysm diagnosis and treatment [37] -erefore in
this study we quantitatively calculated the hemodynamicparameters of CAA of different diameters in order to esti-mate the relationship between the risk level of thrombosisand the size of CAA -e results showed that CAAs only
Front Back
OSI0495
0330
0165
0000
Model 0
Model 2x
Model 3x
Model 5x
Figure 7 Oscillatory shear index (OSI) distribution in the coronary artery aneurysm for the four models
Table 3 -e area of high OSI and RRT in the aneurysm and the area of aneurysm
Model 0 Model 2x Model 3x Model 5xHigh OSI areaCAA area (mm2) (ratio) 046362 (0) 952976238 (125) 29853117997 (253) 141389213579 (662)High RRT areaCAA area (mm2) (ratio) 046362 (0) 381276238 (05) 31977117997 (271) 167873213579 (786)
Front Back
Model 0
Model 2x
Model 3x
Model 5x
WSS
(Pa)
6936
4624
2312
0000
Figure 6 Wall shear stress (WSS) distribution in the coronary artery aneurysm at its peak (t 02 s) for the four models
Complexity 7
affect the blood flow and pressure within the region of thelesion itself with little effect on global blood flow Howeverthere were substantial changes in local hemodynamic pa-rameters related to thrombosis in the lesion locationCompared with the model without a lesion all three CAAmodels showed low WSS high OSI and high RRT withthese changes exacerbated as the CAA diameter increased-ese changes were the results of the sudden increase in thediameter of the lumen on entering the CAA -ese resultssuggest there may be a high correlation between CAA di-ameter and the risk of thrombosis CAA hemodynamicstudies may therefore allow the development of a prelimi-nary classification of the risk of thrombosis helping toimprove the effectiveness of anticoagulation therapy andfacilitating better personalization of treatment according to aquantitative hemodynamic plan
Simulation provides a powerful and effective method forestimating important hemodynamic parameters that aredifficult to measure As mentioned above except mass-flowrate which can be easily detected by non-invasive ultra-sound other parameters WSS OSI and RRT cannot bedirectly measured which are usually obtained through invitro experiments or indirect measurements Simulation is anon-invasive way providing a low cost way and avoiding thepotential risk of some invasive ways to obtain hemodynamicparameters
LPM boundary conditions can provide realistic physi-ologic flow conditions as what has been confirmed inprevious studies [38 39] In addition the coronary mi-crocirculation was introduced into the downstreamboundary condition via the LPM Resistance and pressurechanges downstream of the coronary artery could be
accurately captured in this way helping to ensure the ac-curate simulation of physiological conditions in the coro-nary artery -ere was no difference between the models inthe peripheral vascular structure so the CFD models sharedthe same LPM minimizing the impact of factors other thanthe diameter of the CAA -us the differences in resultsbetween the models were due to the differences in CAAdiameters
As the diameter of the CAA increased theWSS in the CAAlesion area progressively decreased with the WSS in Model 5xobserved to be gt10 times lower than that of the normalcoronary artery (Model 0) Parallel plate flow experiments haveshown that a large number of platelets accumulate at locationswith low WSS (lt04 Pa) [40] and animal endothelial cell ex-periments have shown that thrombosis is associated with adecrease in WSS to within the range 00770279Pa [10] In thepresent study the area average values for WSS in Models 3xand 5x were within this range suggesting that CAAs withdiametersgt3 times that of the normal artery are likely to carry ahigh risk of thrombosis Although the area average WSS forModel 2x was much lower than that of the model withoutCAA it was higher than 04Pa suggesting that CAAs withdiameters double that of the normal artery may not be at highrisk of thrombosis Another important pathophysiologicalfactor in vascular disease is endothelial dysfunction Low WSScan locally inhibit the production of certain important sub-stances such as NO [41] An abnormal response to vasodilationagents including the deactivation of NO by free radicals due tothe impairment of acetylcholine or endothelial NO synthasecan lead to abnormal vasoconstriction which can be associatedwith endothelial dysfunction [41] In addition platelets areprone to aggregation in areas of low WSS which further
Front Back
RRT99083
66055
33028
0000
(Pandash1)
Model 0
Model 2x
Model 3x
Model 5x
Figure 8 Relative residence time (RRT) distribution in the coronary artery aneurysm for the four models
8 Complexity
exacerbates the risk of thrombosis WSS in the CAA lesion ofModel 2x was lower than that in the normal model howeverfurther development is still to be studied just taking WSS as areference -e risk for thrombosis in CAAs progresses withincreasing diameter so the risk associatedwithModel 2xwouldbe lower than that for Models 3x and 5x -e development ofCAAs needs further study Although studies have investigatedthe association between WSS and thrombosis the currentunderstanding is not yet comprehensive -erefore the pos-sibility of WSS and thrombosis in the corresponding in vitroexperiments should be the focus of continued research
-e OSIs for the CAAs increased rapidly with increasingdiameter of the lesion with the OSI in Model 5x around 30times greater than that of the normal coronary artery (whichwas close to zero throughout the CAA) Previous studieshave pointed out that when OSI is greater than 02 it willcause endothelial cell damage [31] -e high OSI area(OSIgt 02) ratio increased from 01 to 662 betweenModel 0 and Model 5x In vivo experimental studies ofporcine aortas have reported that disturbed flow (ie anincrease in OSI) promoted the expression of proin-flammatory cytokines in endothelial cells [11] In additionan in vitro study of bovine endothelial cells reported that theexpression of monocyte chemoattractant protein-1 could beinduced by applying a low-amplitude oscillating shear stressof 03 Pa at 1Hz (equivalent to an OSI of 05) and thishemodynamic environment enhanced the binding of en-dothelial cells to monocytes [42] -ese findings suggest thatthe elevated OSI values observed in the CAA models may beassociated with conditions that can trigger thrombosis
-e RRT values for the CAAs increased dramatically withincreasing diameters of the lesions with the RRT for Model5xgt100 times greater than that of the normal coronary artery-e high RRTarea ratio increased from 01 to 786 betweenModel 0 and Model 5x -ese findings indicate that the bloodflow in the CAA recirculates when the diameter of the lumenincreases resulting in prolonged contact time between the CAAwall and the blood Studies have reported a significantly in-creased risk of thrombosis when RRT is gt10Paminus1 [12 34] -eRRTvalues forModels 3x and 5x in the present study were bothgt10Paminus1 suggesting a high risk of thrombosis when the di-ameter of a CAA exceeds three times that of the normal cor-onary artery Conversely the RRTforModel 2xwasmuch lowerthan 10Paminus1 suggesting that the risk of thrombosis may be lowwhen the diameter of the CAA is only double that of the normalartery Although there have been various studies of the rela-tionship between RRTand aneurysms [43] the current state ofknowledge remains insufficient for patient classification forexample there are no appropriate ranges of RRT values fordistinguishing the risk level of thrombosis which needs furtherstudy
In summary the comparison of our modeling resultswith the findings of previous studies suggested that the lowWSS high OSI and high RRT observed in the CAAs wouldsignificantly increase the risk of thrombosis However therisk varied considerably between the different diameters ofCAA -e WSS OSI and RRT values for Models 3x and 5xall suggested a high risk of thrombosis based on the previousstudy results-us for CAAs with diameters gt3 times that of
the normal coronary artery the risk of uncertainty withconservative treatment may be higher than the risk asso-ciated with surgery suggesting that the surgical operationshould be considered Conversely although the WSS OSIand RRT values for Model 2x were unfavorable comparedwith those of the model of the normal coronary arteryimplying an increased risk of thrombosis the magnitude ofthese differences was insufficient to support a prediction ofthe future development of the CAA For CAAs with a di-ameter up to two times that of the normal coronary arteryconservative drug treatment may be the better optionavoiding the risks associated with surgery
-e limitations of this study are as follows First this studyhas only one patientrsquos data and the conclusion may be ac-cidental We need to use more data for research Secondly animportant assumption used in the CFD calculation is the rigidwall where in fact elastic walls should be used In particularthe coronary artery will deform greatly as the heart contractswhich can be solved by two-way FSI in the future
5 Conclusion
-e evaluation of the relationship between hemodynamiceffects and different diameters of CAAs was performed inthis research through the CFD simulation method -erelationship between thrombosis risk and the size of theCAA diameter could be preliminarily evaluated from ahemodynamic perspective
We found that as the diameter of the CAA increased therisk of thrombosis increased substantially -e results sug-gested that when the diameter of a CAA is small (less thandouble that of the normal coronary artery) the risk ofthrombosis may be relatively low suggesting that medica-tion may be a sufficient approach for the patient avoidingthe uncertain risks associated with surgery If the diameter ofCAA is large (gt3 times that of the normal coronary artery)there may be a high risk of thrombosis and surgicaltreatment could be considered A similar approach could betaken in future studies to systematically assess the risk as-sociated with different shapes sizes and locations of an-eurysms Such approaches may form the basis for moresophisticated hemodynamic-based risk stratificationmethods supporting clinical decision-making in assessmentof CAA
Data Availability
-e data used to support the findings of this study areavailable from the corresponding author upon request
Conflicts of Interest
-e authors declare no conflicts of interest
Acknowledgments
-is research was supported by the National Natural ScienceFoundation of China (nos 11832003 and 11772016) andJSPS KAKENHI under Grant no JP18K18355 -is researchwas partially supported by the Creation of a Development
Complexity 9
Platform for ImplantableWearable Medical Devices by aNovel Physiological Data Integration System of the Programon Open Innovation Platform with Enterprises ResearchInstitute and Academia (OPERA) from the Japan Scienceand Technology Agency (JST) -is research was also sup-ported by Collaborative Research Project 2020 Institute ofFluid Science Tohoku University (J20R001) with the GrantNumber JP18K18355
References
[1] H Kato T Sugimura T Akagi et al ldquoLong-term conse-quences of kawasaki diseaserdquo Circulation vol 94 no 6pp 1379ndash1385 1996
[2] S A Sherif O O Tok O Taskoylu O Goktekin andI D Kilic ldquoCoronary artery aneurysms a review of theepidemiology pathophysiology diagnosis and treatmentrdquoFrontiers in Cardiovascular Medicine vol 4 2017
[3] E Beckmann S Rustum S Marquardt et al ldquoSurgicaltreatment of coronary artery aneurysmsrdquo Journal of CardiacSurgery vol 32 no 11 pp 674ndash679 2017
[4] M Syed M Lesch and A D Syed ldquoCoronary artery aneu-rysm a reviewrdquo Progress in Cardiovascular Diseases vol 40no 1 pp 77ndash84 1997
[5] G G Hartnell B M Parnell and R B Pridie ldquoCoronaryartery ectasia Its prevalence and clinical significance in 4993patientsrdquo British Heart Journal vol 54 no 4 1985
[6] A Satran B A Bart C R Henry et al ldquoIncreased prevalenceof coronary artery aneurysms among cocaine usersrdquo Circu-lation vol 111 no 19 pp 2424ndash2429 2005
[7] O Topaz M S Rutherford S M Bojack et al ldquoGiant an-eurysms of coronary arteries and saphenous vein graftsangiographic findings and histopathological correlatesrdquoCardiovascular Pathology vol 14 no 6 pp 298ndash302 2005
[8] A P Antoniadis Y S Chatzizisis and G D GiannoglouldquoPathogenetic mechanisms of coronary ectasiardquo InternationalJournal of Cardiology vol 130 no 3 pp 335ndash343 2008
[9] J B Gordon A M Kahn and J C Burns ldquoWhen childrenwith kawasaki disease grow uprdquo Journal of the AmericanCollege of Cardiology vol 54 no 21 pp 1911ndash1920 2009
[10] P Sriramarao L Languino and D Altieri ldquoFibrinogenmediates leukocyte-endothelium bridging in vivo at low shearforcesrdquo Blood vol 88 no 9 pp 3416ndash3423 1996
[11] A G Passerini D C Polacek C Shi et al ldquoCoexistingproinflammatory and antioxidative endothelial transcriptionprofiles in a disturbed flow region of the adult porcine aortardquoProceedings of the National Academy of Sciences vol 101no 89 pp 2482ndash2487
[12] U Morbiducci D Gallo R Ponzini et al ldquoQuantitativeanalysis of bulk flow in image-based hemodynamic models ofthe carotid bifurcation the influence of outflow conditions astest caserdquo Annals of Biomedical Engineering vol 38 no 12pp 3688ndash3705 2010
[13] T Ohkubo R Fukazawa E Ikegami and S Ogawa ldquoReducedshear stress and disturbed flow may lead to coronary aneu-rysm and thrombus formationsrdquo Pediatrics Internationalvol 49 no 1 pp 1ndash7 2007
[14] H Anzai T Watanabe X Han et al ldquoEndothelial cell dis-tributions and migration under conditions of flow shear stressaround a stent wirerdquo Technology and Health Care vol 28no 4 pp 345ndash354 2020
[15] M Zhang Y Li X Zhao et al ldquoHaemodynamic effects ofstent diameter and compaction ratio on flow-diversion
treatment of intracranial aneurysms a numerical study of asuccessful and an unsuccessful caserdquo Journal of Biomechanicsvol 58 pp 179ndash186 2017
[16] H Anzai B Chopard and M Ohta ldquoCombinational opti-mization of strut placement for intracranial stent using arealistic aneurysmrdquo Journal of Flow Control Measurement ampVisualization vol 2 no 2 pp 67ndash77 2014
[17] J P Ku M T Draney F R Arko et al ldquoIn vivo validation ofnumerical prediction of blood flow in arterial bypass graftsrdquoAnnals of Biomedical Engineering vol 30 no 6 pp 743ndash7522002
[18] A R Soler F Kabinejadian M A Slevin P J Bartolo andA Keshmiri ldquoOptimisation of a novel spiral-inducing bypassgraft using computational fluid dynamicsrdquo Scientific Reportsvol 7 no 1 p 1865 2017
[19] H Zhang L Li C Cheng and X Sun ldquoClinical value ofhomodynamic numerical simulation applied in the treatmentof cerebral aneurysmrdquo Experimental and Gerapeutic Medi-cine vol 4 no 6 pp 5401ndash5494 2017
[20] A S Les S C Shadden C A Figueroa et al ldquoQuantificationof hemodynamics in abdominal aortic aneurysms during restand exercise using magnetic resonance imaging and com-putational fluid dynamicsrdquo Annals of Biomedical Engineeringvol 38 no 4 pp 1288ndash1313 2010
[21] M Piccinelli A Veneziani D A Steinman A Remuzzi andL Antiga ldquoA framework for geometric analysis of vascularstructures application to cerebral aneurysmsrdquo IEEE Trans-actions on Medical Imaging vol 28 no 8 pp 1141ndash11552009
[22] H J Kim I E Vignon-Clementel J S CooganC A Figueroa K E Jansen and C A Taylor ldquoPatient-specific modeling of blood flow and pressure in humancoronary arteriesrdquo Annals of Biomedical Engineering vol 38no 10 pp 3195ndash3209 2010
[23] C A Taylor T A Fonte and J K Min ldquoComputational fluiddynamics applied to cardiac computed tomography fornoninvasive quantification of fractional flow reserverdquo Journalof the American College of Cardiology vol 61 no 22pp 2233ndash2241 2013
[24] I E V Clementel C A Figueroa K E Jansen andC A Taylor ldquoOutflow boundary conditions for 3D simula-tions of non-periodic blood flow and pressure fields in de-formable arteriesrdquo Computer Methods in Biomechanics andBiomedical Engineering vol 13 no 5 pp 625ndash640 2010
[25] N Stergiopulos J J Meister and N Westerhof ldquoDetermi-nants of stroke volume and systolic and diastolic aorticpressurerdquoGe American Journal of Physiology vol 270 no 6pp 2050ndash2059 1996
[26] M Zamir P Sinclair and T H Wonnacott ldquoRelation be-tween diameter and flow in major branches of the arch of theaortardquo Journal of Biomechanics vol 25 no 11 pp 1303ndash13101992
[27] K Johnson P Sharma and J Oshinski ldquoCoronary artery flowmeasurement using navigator echo gated phase contrastmagnetic resonance velocity mapping at 30 teslardquo Journal ofBiomechanics vol 41 no 3 pp 595ndash602 2008
[28] F P Salvuccia C A Perazzob S Sallesa J G Barrac andR L Armentano ldquoInfluence of inlet conditions in wall shearstress distributions of left coronary arteries in patient-specificsimulationsrdquo Mecanica Computacional vol XXIXpp 5953ndash5960 2010
[29] B C Lopez B Calvo and P Estefanıa Patient-SpecificComputational Modeling Springer Berlin Germany 2012thedition 2012
10 Complexity
[30] D N Ghista and F Kabinejadian ldquoCoronary artery bypassgrafting hemodynamics and anastomosis design a biomedicalengineering reviewrdquo BioMedical Engineering Online vol 12no 129 2013
[31] F P Glor F P Glor B Ariff et al ldquoImage-based carotid flowreconstruction a comparison between MRI and ultrasoundrdquoPhysiological Measurement vol 25 no 6 pp 1495ndash15092004
[32] S-W Lee L Antiga and D A Steinman ldquoCorrelationsamong indicators of disturbed flow at the normal carotidbifurcationrdquo Journal of Biomechanical Engineering vol 131no 6 Article ID 061013 2009
[33] H A Himburg ldquoSpatial comparison between wall shear stressmeasures and porcine arterial endothelial permeabilityrdquo AJPHeart and Circulatory Physiology vol 286 no 5 pp 1916ndash1922 2004
[34] T Suess J Anderson L Danielson et al ldquoExamination ofnear-wall hemodynamic parameters in the renal bridgingstent of various stent graft configurations for repairing vis-ceral branched aortic aneurysmsrdquo Journal of Vascular Sur-gery vol 64 no 3 pp 788ndash796 2016
[35] H Zhang X Yu F Ji and F Sun ldquoCoronary artery aneurysmformation after drug-coatedrdquo Medicine vol 97 no 45 2018
[36] N G Gutierrez M Mathew B W McCrindle et al ldquoHe-modynamic variables in aneurysms are associated withthrombotic risk in children with Kawasaki diseaserdquo Inter-national Journal of Cardiology vol 281 pp 15ndash21 2019
[37] C Karmonik G Chintalapani T Redel et al ldquoHemody-namics at the ostium of cerebral aneurysms with relation topost-treatment changes by a virtual flow diverter a compu-tational fluid dynamics studyrdquo in Proceedings of the AnnualInternational Conference of the IEEE Engineering in Medicineand Biology Society EMBS pp 1895ndash1898 Osaka Japan July2013
[38] J T Marcus H G Smeenk J P A KuijerR J Van Der Geest R M Heethaar and A C Van RossumldquoFlow profiles in the left anterior descending and the rightcoronary artery assessed byMR velocity quantification effectsof through-plane and in-plane motion of the heartrdquo Journal ofComputer Assisted Tomography vol 23 no 4 pp 567ndash5761999
[39] Y Shi P Lawford and R Hose ldquoReview of zero-D and 1-Dmodels of blood flow in the cardiovascular systemrdquo Bio-Medical Engineering Online vol 10 no 1 p 33 2011
[40] M Kroll J Hellums L McIntire A Schafer and J MoakeldquoPlatelets and shear stressrdquo Blood vol 88 no 5pp 1525ndash1541 1996
[41] J-J Chiu and S Chien ldquoEffects of disturbed flow on vascularendothelium pathophysiological basis and clinical perspec-tivesrdquo Physiological Reviews vol 91 no 1 pp 327ndash387 2011
[42] J Hwang M H Ing A Salazar et al ldquoPulsatile versus os-cillatory shear stress regulates NADPH oxidase subunit ex-pressionrdquo Circulation Research vol 93 no 12 pp 1225ndash12322003
[43] S-i Sugiyama K Niizuma T Nakayama et al ldquoRelativeresidence time prolongation in intracranial aneurysmsrdquoNeurosurgery vol 73 no 5 pp 767ndash776 2013
Complexity 11

and decreased blood flow through the coronary artery theopposite was the case during diastole Changes in the di-ameter of the CAA did not have a significant effect oncoronary outlet flow
32 Wall Shear Stress -e WSS is the force per unit areaexerted by the wall on the fluid in a direction along the planeof the local tangent [28] calculated as follows
τω 4μQ
πR3 (4)
where μ represents the blood viscosity Q is mass-flowrate and R is vessel radius Previous studies have reportedan association between thrombosis formation and lowWSS [29] -e area average values of WSS in coronaryartery aneurysm over a cardiac cycle in the four models
are listed in Table 2 and the values over a cycle anddistribution contours are shown in Figures 5 and 6 -eaverage WSS over a cycle in Model 0 (with no CAA) was351 Pa -e averages for Models 2x 3x and 5x were 068026 and 008 Pa respectively substantially reduced in theCAA due to blood flow stagnation and recirculation withthe reduction increasing in CAAs of greater diameters-e distribution contours in Figure 6 confirm that theCAA results only in local hemodynamic disturbanceswithout wider hemodynamic changes in the arteries Atsome distance downstream in the coronary artery thecoronary diameter and WSS both return to normal levels
33 Oscillatory Shear Index OSI is a parameter thatquantifies the magnitude of theWSS and directional changes[18] calculated as follows
Inle
t AAO
Out
let D
AOO
utle
t A1
Out
let f
Mas
s flo
w (m
lmin
)
Pres
sure
(Pa)
Pres
sure
(Pa)
Pres
sure
(Pa)
Pres
sure
(Pa)
Mas
s flo
w (m
lmin
)M
ass f
low
(mlm
in)
Mas
s flo
w (m
lmin
)
20000
00
0
16500
10000008 08
13000
ndash20008
17000
100000 08
1600
00 08
16000
100000 08
45
00 08
Mass flow Pressure
16000
8000080
Cardiac cycle (s)
Cardiac cycle (s) Cardiac cycle (s)
Cardiac cycle (s)Cardiac cycle (s)
Cardiac cycle (s)
Cardiac cycle (s) Cardiac cycle (s)
Model 0
Model 3x Model 5x
Model 2x
DAO
A1
fAAO
Model 0Model 2x
Model 3xModel 5x
Figure 4 Mass flow and pressure curves for the inlet (ascending aorta AAO) and three outlets (descending aorta (DAO) artery 1 (A1) andcoronary artery f ) over a cardiac cycle
Complexity 5
OSI 05 times 1 minus1113938
T
0 τωdt11138681113868111386811138681113868
11138681113868111386811138681113868
1113938T
0 τω1113868111386811138681113868
1113868111386811138681113868dt
⎛⎝ ⎞⎠ (5)
where T is the cardiac cycle OSI has values in the range 005with 0 representing undisturbed flow with no change in thedirection of the shear stress and 05 representing disturbedflow with oscillating shear stress Previous studies havereported an association between high OSI and the formationof intimal hyperplasia [30] -e average values of OSI in theaneurysm and OSI distribution contours are shown in Table 2and Figure 7 respectively -e average value of OSI over thecardiac cycle inModel 0 was 001-e averages forModels 2x3x and 5x were substantially higher at 003 013 and 030respectively Previous studies have pointed out that when OSIis greater than 02 it will cause endothelial cell damage [31]As shown in Table 3 the ratio of high OSI area in theaneurysm to the area of aneurysm was 0 125 253 and662 respectively Model 0 has OSI close to zero throughoutthe cardiac cycle and the flow in Model 0 is unidirectionalwithout circulation Normal coronary blood flow is unidi-rectional usually without flow recirculation so the OSI of thenormal coronary artery (Model 0) was close to zerothroughout the entire cardiac cycle-e highOSI values in theCAA models which reached 30 times higher in model 5xwere due to the increased storage time resulting from theincreased size of the cavity which led to recirculation withinthe CAA lesion -e effect on OSI was locally confined there
was little difference between the OSI in the distal coronaryarteries in Models 2x 3x and 5x and those in Model 0
34 Relative Residence Time -e RRT is an indicator thatcomprehensively characterizes the values and oscillation ofWSS [32] as well as the time of local blood flow and vascularinteraction [33] It is calculated as follows
RRT 1
(1 minus 2 middot OSI) middot TAWSS (6)
where
TAWSS WSS
T (7)
Here TAWSS isWSS average over one cardiac cycle andT is a cardiac cycle Figure 8 shows the distribution contoursfor RRT in the four models and Table 2 shows the areaaverage values of RRT within the CAA lesion over thecardiac cycle -e average value of RRT in Model 0 was038 Paminus1 -e averages for Models 2x 3x and 5x weresubstantially higher at 288 2312 and 5159 Paminus1 respec-tively showing a dramatic increase in RRT with increasingdiameter of the CAA Studies have reported a significantlyincreased risk of thrombosis when RRT is gt10 Paminus1 [12 34]As shown in Table 3 the ratio of high RRT area in theaneurysm to the area of aneurysm was 0 05 271 and786 respectively -e increased diameter of the CAAmakes it easier for blood to remain resident within ithampering the blood flow to the distal coronary artery -echange in RRT was locally confined to the CAA there waslittle difference between the RRT in the distal coronaryarteries in Models 2x 3x and 5x and that in the distalcoronary artery in Model 0
4 Discussion
We have shown that the relationship between hemodynamiceffects and different diameters of CAAs can be achieved byusing CFD simulation method direct comparison withvirtual control case based on the same patient We foundthat changes in the diameter of CAA have a strong effect onlocal hemodynamics while they do not have a significanteffect on global hemodynamics -e potential risk ofthrombosis increases significantly with increasing CAAdiameter indicated through decreasing WSS increasing OSIand RRT -is research will allow us to estimate thethrombosis risk of CAAs from a hemodynamic perspectiveand provide more comprehensive support for doctorsrsquodecisions
When making treatment decisions about CAAs doctorstypically depend on their own clinical experience [35] -ismay be because of the lack of useful diagnostic tools -ecurrent used tool is the method of imaging which canprovide geometric information and almost no other infor-mation -e lack of other information cannot provide morehelp for the doctorrsquos diagnosis -erefore it is necessary tofind a way to provide more information to help the doctor Ithas been shown that WSS over aneurysmal regions is
Table 2 Average values over a cardiac cycle for wall shear stress(WSS) the oscillatory shear index (OSI) and relative residencetime (RRT) in the coronary artery aneurysm
Model 0 Model2x
Model3x
Model5x
Area averageWSS (Pa) 351 068 026 008Area average OSI 001 003 013 030Area average RRT(Paminus1) 038 288 2312 5159
0
45
4
35
3
252
15
1
05
Wal
l she
ar st
ress
(Pa)
0 01 02 03 04 05 06 07 08Time (s)
Model 0Model 2x
Model 3xModel 5x
Figure 5 Wall shear stress in the coronary artery aneurysm over acardiac cycle for the four models
6 Complexity
associated with risk of thrombosis and that is a morepredictive factor of thrombosis than aneurysm diameter[36] We confirmed that hemodynamic research is beneficialfor aneurysm diagnosis and treatment [37] -erefore in
this study we quantitatively calculated the hemodynamicparameters of CAA of different diameters in order to esti-mate the relationship between the risk level of thrombosisand the size of CAA -e results showed that CAAs only
Front Back
OSI0495
0330
0165
0000
Model 0
Model 2x
Model 3x
Model 5x
Figure 7 Oscillatory shear index (OSI) distribution in the coronary artery aneurysm for the four models
Table 3 -e area of high OSI and RRT in the aneurysm and the area of aneurysm
Model 0 Model 2x Model 3x Model 5xHigh OSI areaCAA area (mm2) (ratio) 046362 (0) 952976238 (125) 29853117997 (253) 141389213579 (662)High RRT areaCAA area (mm2) (ratio) 046362 (0) 381276238 (05) 31977117997 (271) 167873213579 (786)
Front Back
Model 0
Model 2x
Model 3x
Model 5x
WSS
(Pa)
6936
4624
2312
0000
Figure 6 Wall shear stress (WSS) distribution in the coronary artery aneurysm at its peak (t 02 s) for the four models
Complexity 7
affect the blood flow and pressure within the region of thelesion itself with little effect on global blood flow Howeverthere were substantial changes in local hemodynamic pa-rameters related to thrombosis in the lesion locationCompared with the model without a lesion all three CAAmodels showed low WSS high OSI and high RRT withthese changes exacerbated as the CAA diameter increased-ese changes were the results of the sudden increase in thediameter of the lumen on entering the CAA -ese resultssuggest there may be a high correlation between CAA di-ameter and the risk of thrombosis CAA hemodynamicstudies may therefore allow the development of a prelimi-nary classification of the risk of thrombosis helping toimprove the effectiveness of anticoagulation therapy andfacilitating better personalization of treatment according to aquantitative hemodynamic plan
Simulation provides a powerful and effective method forestimating important hemodynamic parameters that aredifficult to measure As mentioned above except mass-flowrate which can be easily detected by non-invasive ultra-sound other parameters WSS OSI and RRT cannot bedirectly measured which are usually obtained through invitro experiments or indirect measurements Simulation is anon-invasive way providing a low cost way and avoiding thepotential risk of some invasive ways to obtain hemodynamicparameters
LPM boundary conditions can provide realistic physi-ologic flow conditions as what has been confirmed inprevious studies [38 39] In addition the coronary mi-crocirculation was introduced into the downstreamboundary condition via the LPM Resistance and pressurechanges downstream of the coronary artery could be
accurately captured in this way helping to ensure the ac-curate simulation of physiological conditions in the coro-nary artery -ere was no difference between the models inthe peripheral vascular structure so the CFD models sharedthe same LPM minimizing the impact of factors other thanthe diameter of the CAA -us the differences in resultsbetween the models were due to the differences in CAAdiameters
As the diameter of the CAA increased theWSS in the CAAlesion area progressively decreased with the WSS in Model 5xobserved to be gt10 times lower than that of the normalcoronary artery (Model 0) Parallel plate flow experiments haveshown that a large number of platelets accumulate at locationswith low WSS (lt04 Pa) [40] and animal endothelial cell ex-periments have shown that thrombosis is associated with adecrease in WSS to within the range 00770279Pa [10] In thepresent study the area average values for WSS in Models 3xand 5x were within this range suggesting that CAAs withdiametersgt3 times that of the normal artery are likely to carry ahigh risk of thrombosis Although the area average WSS forModel 2x was much lower than that of the model withoutCAA it was higher than 04Pa suggesting that CAAs withdiameters double that of the normal artery may not be at highrisk of thrombosis Another important pathophysiologicalfactor in vascular disease is endothelial dysfunction Low WSScan locally inhibit the production of certain important sub-stances such as NO [41] An abnormal response to vasodilationagents including the deactivation of NO by free radicals due tothe impairment of acetylcholine or endothelial NO synthasecan lead to abnormal vasoconstriction which can be associatedwith endothelial dysfunction [41] In addition platelets areprone to aggregation in areas of low WSS which further
Front Back
RRT99083
66055
33028
0000
(Pandash1)
Model 0
Model 2x
Model 3x
Model 5x
Figure 8 Relative residence time (RRT) distribution in the coronary artery aneurysm for the four models
8 Complexity
exacerbates the risk of thrombosis WSS in the CAA lesion ofModel 2x was lower than that in the normal model howeverfurther development is still to be studied just taking WSS as areference -e risk for thrombosis in CAAs progresses withincreasing diameter so the risk associatedwithModel 2xwouldbe lower than that for Models 3x and 5x -e development ofCAAs needs further study Although studies have investigatedthe association between WSS and thrombosis the currentunderstanding is not yet comprehensive -erefore the pos-sibility of WSS and thrombosis in the corresponding in vitroexperiments should be the focus of continued research
-e OSIs for the CAAs increased rapidly with increasingdiameter of the lesion with the OSI in Model 5x around 30times greater than that of the normal coronary artery (whichwas close to zero throughout the CAA) Previous studieshave pointed out that when OSI is greater than 02 it willcause endothelial cell damage [31] -e high OSI area(OSIgt 02) ratio increased from 01 to 662 betweenModel 0 and Model 5x In vivo experimental studies ofporcine aortas have reported that disturbed flow (ie anincrease in OSI) promoted the expression of proin-flammatory cytokines in endothelial cells [11] In additionan in vitro study of bovine endothelial cells reported that theexpression of monocyte chemoattractant protein-1 could beinduced by applying a low-amplitude oscillating shear stressof 03 Pa at 1Hz (equivalent to an OSI of 05) and thishemodynamic environment enhanced the binding of en-dothelial cells to monocytes [42] -ese findings suggest thatthe elevated OSI values observed in the CAA models may beassociated with conditions that can trigger thrombosis
-e RRT values for the CAAs increased dramatically withincreasing diameters of the lesions with the RRT for Model5xgt100 times greater than that of the normal coronary artery-e high RRTarea ratio increased from 01 to 786 betweenModel 0 and Model 5x -ese findings indicate that the bloodflow in the CAA recirculates when the diameter of the lumenincreases resulting in prolonged contact time between the CAAwall and the blood Studies have reported a significantly in-creased risk of thrombosis when RRT is gt10Paminus1 [12 34] -eRRTvalues forModels 3x and 5x in the present study were bothgt10Paminus1 suggesting a high risk of thrombosis when the di-ameter of a CAA exceeds three times that of the normal cor-onary artery Conversely the RRTforModel 2xwasmuch lowerthan 10Paminus1 suggesting that the risk of thrombosis may be lowwhen the diameter of the CAA is only double that of the normalartery Although there have been various studies of the rela-tionship between RRTand aneurysms [43] the current state ofknowledge remains insufficient for patient classification forexample there are no appropriate ranges of RRT values fordistinguishing the risk level of thrombosis which needs furtherstudy
In summary the comparison of our modeling resultswith the findings of previous studies suggested that the lowWSS high OSI and high RRT observed in the CAAs wouldsignificantly increase the risk of thrombosis However therisk varied considerably between the different diameters ofCAA -e WSS OSI and RRT values for Models 3x and 5xall suggested a high risk of thrombosis based on the previousstudy results-us for CAAs with diameters gt3 times that of
the normal coronary artery the risk of uncertainty withconservative treatment may be higher than the risk asso-ciated with surgery suggesting that the surgical operationshould be considered Conversely although the WSS OSIand RRT values for Model 2x were unfavorable comparedwith those of the model of the normal coronary arteryimplying an increased risk of thrombosis the magnitude ofthese differences was insufficient to support a prediction ofthe future development of the CAA For CAAs with a di-ameter up to two times that of the normal coronary arteryconservative drug treatment may be the better optionavoiding the risks associated with surgery
-e limitations of this study are as follows First this studyhas only one patientrsquos data and the conclusion may be ac-cidental We need to use more data for research Secondly animportant assumption used in the CFD calculation is the rigidwall where in fact elastic walls should be used In particularthe coronary artery will deform greatly as the heart contractswhich can be solved by two-way FSI in the future
5 Conclusion
-e evaluation of the relationship between hemodynamiceffects and different diameters of CAAs was performed inthis research through the CFD simulation method -erelationship between thrombosis risk and the size of theCAA diameter could be preliminarily evaluated from ahemodynamic perspective
We found that as the diameter of the CAA increased therisk of thrombosis increased substantially -e results sug-gested that when the diameter of a CAA is small (less thandouble that of the normal coronary artery) the risk ofthrombosis may be relatively low suggesting that medica-tion may be a sufficient approach for the patient avoidingthe uncertain risks associated with surgery If the diameter ofCAA is large (gt3 times that of the normal coronary artery)there may be a high risk of thrombosis and surgicaltreatment could be considered A similar approach could betaken in future studies to systematically assess the risk as-sociated with different shapes sizes and locations of an-eurysms Such approaches may form the basis for moresophisticated hemodynamic-based risk stratificationmethods supporting clinical decision-making in assessmentof CAA
Data Availability
-e data used to support the findings of this study areavailable from the corresponding author upon request
Conflicts of Interest
-e authors declare no conflicts of interest
Acknowledgments
-is research was supported by the National Natural ScienceFoundation of China (nos 11832003 and 11772016) andJSPS KAKENHI under Grant no JP18K18355 -is researchwas partially supported by the Creation of a Development
Complexity 9
Platform for ImplantableWearable Medical Devices by aNovel Physiological Data Integration System of the Programon Open Innovation Platform with Enterprises ResearchInstitute and Academia (OPERA) from the Japan Scienceand Technology Agency (JST) -is research was also sup-ported by Collaborative Research Project 2020 Institute ofFluid Science Tohoku University (J20R001) with the GrantNumber JP18K18355
References
[1] H Kato T Sugimura T Akagi et al ldquoLong-term conse-quences of kawasaki diseaserdquo Circulation vol 94 no 6pp 1379ndash1385 1996
[2] S A Sherif O O Tok O Taskoylu O Goktekin andI D Kilic ldquoCoronary artery aneurysms a review of theepidemiology pathophysiology diagnosis and treatmentrdquoFrontiers in Cardiovascular Medicine vol 4 2017
[3] E Beckmann S Rustum S Marquardt et al ldquoSurgicaltreatment of coronary artery aneurysmsrdquo Journal of CardiacSurgery vol 32 no 11 pp 674ndash679 2017
[4] M Syed M Lesch and A D Syed ldquoCoronary artery aneu-rysm a reviewrdquo Progress in Cardiovascular Diseases vol 40no 1 pp 77ndash84 1997
[5] G G Hartnell B M Parnell and R B Pridie ldquoCoronaryartery ectasia Its prevalence and clinical significance in 4993patientsrdquo British Heart Journal vol 54 no 4 1985
[6] A Satran B A Bart C R Henry et al ldquoIncreased prevalenceof coronary artery aneurysms among cocaine usersrdquo Circu-lation vol 111 no 19 pp 2424ndash2429 2005
[7] O Topaz M S Rutherford S M Bojack et al ldquoGiant an-eurysms of coronary arteries and saphenous vein graftsangiographic findings and histopathological correlatesrdquoCardiovascular Pathology vol 14 no 6 pp 298ndash302 2005
[8] A P Antoniadis Y S Chatzizisis and G D GiannoglouldquoPathogenetic mechanisms of coronary ectasiardquo InternationalJournal of Cardiology vol 130 no 3 pp 335ndash343 2008
[9] J B Gordon A M Kahn and J C Burns ldquoWhen childrenwith kawasaki disease grow uprdquo Journal of the AmericanCollege of Cardiology vol 54 no 21 pp 1911ndash1920 2009
[10] P Sriramarao L Languino and D Altieri ldquoFibrinogenmediates leukocyte-endothelium bridging in vivo at low shearforcesrdquo Blood vol 88 no 9 pp 3416ndash3423 1996
[11] A G Passerini D C Polacek C Shi et al ldquoCoexistingproinflammatory and antioxidative endothelial transcriptionprofiles in a disturbed flow region of the adult porcine aortardquoProceedings of the National Academy of Sciences vol 101no 89 pp 2482ndash2487
[12] U Morbiducci D Gallo R Ponzini et al ldquoQuantitativeanalysis of bulk flow in image-based hemodynamic models ofthe carotid bifurcation the influence of outflow conditions astest caserdquo Annals of Biomedical Engineering vol 38 no 12pp 3688ndash3705 2010
[13] T Ohkubo R Fukazawa E Ikegami and S Ogawa ldquoReducedshear stress and disturbed flow may lead to coronary aneu-rysm and thrombus formationsrdquo Pediatrics Internationalvol 49 no 1 pp 1ndash7 2007
[14] H Anzai T Watanabe X Han et al ldquoEndothelial cell dis-tributions and migration under conditions of flow shear stressaround a stent wirerdquo Technology and Health Care vol 28no 4 pp 345ndash354 2020
[15] M Zhang Y Li X Zhao et al ldquoHaemodynamic effects ofstent diameter and compaction ratio on flow-diversion
treatment of intracranial aneurysms a numerical study of asuccessful and an unsuccessful caserdquo Journal of Biomechanicsvol 58 pp 179ndash186 2017
[16] H Anzai B Chopard and M Ohta ldquoCombinational opti-mization of strut placement for intracranial stent using arealistic aneurysmrdquo Journal of Flow Control Measurement ampVisualization vol 2 no 2 pp 67ndash77 2014
[17] J P Ku M T Draney F R Arko et al ldquoIn vivo validation ofnumerical prediction of blood flow in arterial bypass graftsrdquoAnnals of Biomedical Engineering vol 30 no 6 pp 743ndash7522002
[18] A R Soler F Kabinejadian M A Slevin P J Bartolo andA Keshmiri ldquoOptimisation of a novel spiral-inducing bypassgraft using computational fluid dynamicsrdquo Scientific Reportsvol 7 no 1 p 1865 2017
[19] H Zhang L Li C Cheng and X Sun ldquoClinical value ofhomodynamic numerical simulation applied in the treatmentof cerebral aneurysmrdquo Experimental and Gerapeutic Medi-cine vol 4 no 6 pp 5401ndash5494 2017
[20] A S Les S C Shadden C A Figueroa et al ldquoQuantificationof hemodynamics in abdominal aortic aneurysms during restand exercise using magnetic resonance imaging and com-putational fluid dynamicsrdquo Annals of Biomedical Engineeringvol 38 no 4 pp 1288ndash1313 2010
[21] M Piccinelli A Veneziani D A Steinman A Remuzzi andL Antiga ldquoA framework for geometric analysis of vascularstructures application to cerebral aneurysmsrdquo IEEE Trans-actions on Medical Imaging vol 28 no 8 pp 1141ndash11552009
[22] H J Kim I E Vignon-Clementel J S CooganC A Figueroa K E Jansen and C A Taylor ldquoPatient-specific modeling of blood flow and pressure in humancoronary arteriesrdquo Annals of Biomedical Engineering vol 38no 10 pp 3195ndash3209 2010
[23] C A Taylor T A Fonte and J K Min ldquoComputational fluiddynamics applied to cardiac computed tomography fornoninvasive quantification of fractional flow reserverdquo Journalof the American College of Cardiology vol 61 no 22pp 2233ndash2241 2013
[24] I E V Clementel C A Figueroa K E Jansen andC A Taylor ldquoOutflow boundary conditions for 3D simula-tions of non-periodic blood flow and pressure fields in de-formable arteriesrdquo Computer Methods in Biomechanics andBiomedical Engineering vol 13 no 5 pp 625ndash640 2010
[25] N Stergiopulos J J Meister and N Westerhof ldquoDetermi-nants of stroke volume and systolic and diastolic aorticpressurerdquoGe American Journal of Physiology vol 270 no 6pp 2050ndash2059 1996
[26] M Zamir P Sinclair and T H Wonnacott ldquoRelation be-tween diameter and flow in major branches of the arch of theaortardquo Journal of Biomechanics vol 25 no 11 pp 1303ndash13101992
[27] K Johnson P Sharma and J Oshinski ldquoCoronary artery flowmeasurement using navigator echo gated phase contrastmagnetic resonance velocity mapping at 30 teslardquo Journal ofBiomechanics vol 41 no 3 pp 595ndash602 2008
[28] F P Salvuccia C A Perazzob S Sallesa J G Barrac andR L Armentano ldquoInfluence of inlet conditions in wall shearstress distributions of left coronary arteries in patient-specificsimulationsrdquo Mecanica Computacional vol XXIXpp 5953ndash5960 2010
[29] B C Lopez B Calvo and P Estefanıa Patient-SpecificComputational Modeling Springer Berlin Germany 2012thedition 2012
10 Complexity
[30] D N Ghista and F Kabinejadian ldquoCoronary artery bypassgrafting hemodynamics and anastomosis design a biomedicalengineering reviewrdquo BioMedical Engineering Online vol 12no 129 2013
[31] F P Glor F P Glor B Ariff et al ldquoImage-based carotid flowreconstruction a comparison between MRI and ultrasoundrdquoPhysiological Measurement vol 25 no 6 pp 1495ndash15092004
[32] S-W Lee L Antiga and D A Steinman ldquoCorrelationsamong indicators of disturbed flow at the normal carotidbifurcationrdquo Journal of Biomechanical Engineering vol 131no 6 Article ID 061013 2009
[33] H A Himburg ldquoSpatial comparison between wall shear stressmeasures and porcine arterial endothelial permeabilityrdquo AJPHeart and Circulatory Physiology vol 286 no 5 pp 1916ndash1922 2004
[34] T Suess J Anderson L Danielson et al ldquoExamination ofnear-wall hemodynamic parameters in the renal bridgingstent of various stent graft configurations for repairing vis-ceral branched aortic aneurysmsrdquo Journal of Vascular Sur-gery vol 64 no 3 pp 788ndash796 2016
[35] H Zhang X Yu F Ji and F Sun ldquoCoronary artery aneurysmformation after drug-coatedrdquo Medicine vol 97 no 45 2018
[36] N G Gutierrez M Mathew B W McCrindle et al ldquoHe-modynamic variables in aneurysms are associated withthrombotic risk in children with Kawasaki diseaserdquo Inter-national Journal of Cardiology vol 281 pp 15ndash21 2019
[37] C Karmonik G Chintalapani T Redel et al ldquoHemody-namics at the ostium of cerebral aneurysms with relation topost-treatment changes by a virtual flow diverter a compu-tational fluid dynamics studyrdquo in Proceedings of the AnnualInternational Conference of the IEEE Engineering in Medicineand Biology Society EMBS pp 1895ndash1898 Osaka Japan July2013
[38] J T Marcus H G Smeenk J P A KuijerR J Van Der Geest R M Heethaar and A C Van RossumldquoFlow profiles in the left anterior descending and the rightcoronary artery assessed byMR velocity quantification effectsof through-plane and in-plane motion of the heartrdquo Journal ofComputer Assisted Tomography vol 23 no 4 pp 567ndash5761999
[39] Y Shi P Lawford and R Hose ldquoReview of zero-D and 1-Dmodels of blood flow in the cardiovascular systemrdquo Bio-Medical Engineering Online vol 10 no 1 p 33 2011
[40] M Kroll J Hellums L McIntire A Schafer and J MoakeldquoPlatelets and shear stressrdquo Blood vol 88 no 5pp 1525ndash1541 1996
[41] J-J Chiu and S Chien ldquoEffects of disturbed flow on vascularendothelium pathophysiological basis and clinical perspec-tivesrdquo Physiological Reviews vol 91 no 1 pp 327ndash387 2011
[42] J Hwang M H Ing A Salazar et al ldquoPulsatile versus os-cillatory shear stress regulates NADPH oxidase subunit ex-pressionrdquo Circulation Research vol 93 no 12 pp 1225ndash12322003
[43] S-i Sugiyama K Niizuma T Nakayama et al ldquoRelativeresidence time prolongation in intracranial aneurysmsrdquoNeurosurgery vol 73 no 5 pp 767ndash776 2013
Complexity 11

OSI 05 times 1 minus1113938
T
0 τωdt11138681113868111386811138681113868
11138681113868111386811138681113868
1113938T
0 τω1113868111386811138681113868
1113868111386811138681113868dt
⎛⎝ ⎞⎠ (5)
where T is the cardiac cycle OSI has values in the range 005with 0 representing undisturbed flow with no change in thedirection of the shear stress and 05 representing disturbedflow with oscillating shear stress Previous studies havereported an association between high OSI and the formationof intimal hyperplasia [30] -e average values of OSI in theaneurysm and OSI distribution contours are shown in Table 2and Figure 7 respectively -e average value of OSI over thecardiac cycle inModel 0 was 001-e averages forModels 2x3x and 5x were substantially higher at 003 013 and 030respectively Previous studies have pointed out that when OSIis greater than 02 it will cause endothelial cell damage [31]As shown in Table 3 the ratio of high OSI area in theaneurysm to the area of aneurysm was 0 125 253 and662 respectively Model 0 has OSI close to zero throughoutthe cardiac cycle and the flow in Model 0 is unidirectionalwithout circulation Normal coronary blood flow is unidi-rectional usually without flow recirculation so the OSI of thenormal coronary artery (Model 0) was close to zerothroughout the entire cardiac cycle-e highOSI values in theCAA models which reached 30 times higher in model 5xwere due to the increased storage time resulting from theincreased size of the cavity which led to recirculation withinthe CAA lesion -e effect on OSI was locally confined there
was little difference between the OSI in the distal coronaryarteries in Models 2x 3x and 5x and those in Model 0
34 Relative Residence Time -e RRT is an indicator thatcomprehensively characterizes the values and oscillation ofWSS [32] as well as the time of local blood flow and vascularinteraction [33] It is calculated as follows
RRT 1
(1 minus 2 middot OSI) middot TAWSS (6)
where
TAWSS WSS
T (7)
Here TAWSS isWSS average over one cardiac cycle andT is a cardiac cycle Figure 8 shows the distribution contoursfor RRT in the four models and Table 2 shows the areaaverage values of RRT within the CAA lesion over thecardiac cycle -e average value of RRT in Model 0 was038 Paminus1 -e averages for Models 2x 3x and 5x weresubstantially higher at 288 2312 and 5159 Paminus1 respec-tively showing a dramatic increase in RRT with increasingdiameter of the CAA Studies have reported a significantlyincreased risk of thrombosis when RRT is gt10 Paminus1 [12 34]As shown in Table 3 the ratio of high RRT area in theaneurysm to the area of aneurysm was 0 05 271 and786 respectively -e increased diameter of the CAAmakes it easier for blood to remain resident within ithampering the blood flow to the distal coronary artery -echange in RRT was locally confined to the CAA there waslittle difference between the RRT in the distal coronaryarteries in Models 2x 3x and 5x and that in the distalcoronary artery in Model 0
4 Discussion
We have shown that the relationship between hemodynamiceffects and different diameters of CAAs can be achieved byusing CFD simulation method direct comparison withvirtual control case based on the same patient We foundthat changes in the diameter of CAA have a strong effect onlocal hemodynamics while they do not have a significanteffect on global hemodynamics -e potential risk ofthrombosis increases significantly with increasing CAAdiameter indicated through decreasing WSS increasing OSIand RRT -is research will allow us to estimate thethrombosis risk of CAAs from a hemodynamic perspectiveand provide more comprehensive support for doctorsrsquodecisions
When making treatment decisions about CAAs doctorstypically depend on their own clinical experience [35] -ismay be because of the lack of useful diagnostic tools -ecurrent used tool is the method of imaging which canprovide geometric information and almost no other infor-mation -e lack of other information cannot provide morehelp for the doctorrsquos diagnosis -erefore it is necessary tofind a way to provide more information to help the doctor Ithas been shown that WSS over aneurysmal regions is
Table 2 Average values over a cardiac cycle for wall shear stress(WSS) the oscillatory shear index (OSI) and relative residencetime (RRT) in the coronary artery aneurysm
Model 0 Model2x
Model3x
Model5x
Area averageWSS (Pa) 351 068 026 008Area average OSI 001 003 013 030Area average RRT(Paminus1) 038 288 2312 5159
0
45
4
35
3
252
15
1
05
Wal
l she
ar st
ress
(Pa)
0 01 02 03 04 05 06 07 08Time (s)
Model 0Model 2x
Model 3xModel 5x
Figure 5 Wall shear stress in the coronary artery aneurysm over acardiac cycle for the four models
6 Complexity
associated with risk of thrombosis and that is a morepredictive factor of thrombosis than aneurysm diameter[36] We confirmed that hemodynamic research is beneficialfor aneurysm diagnosis and treatment [37] -erefore in
this study we quantitatively calculated the hemodynamicparameters of CAA of different diameters in order to esti-mate the relationship between the risk level of thrombosisand the size of CAA -e results showed that CAAs only
Front Back
OSI0495
0330
0165
0000
Model 0
Model 2x
Model 3x
Model 5x
Figure 7 Oscillatory shear index (OSI) distribution in the coronary artery aneurysm for the four models
Table 3 -e area of high OSI and RRT in the aneurysm and the area of aneurysm
Model 0 Model 2x Model 3x Model 5xHigh OSI areaCAA area (mm2) (ratio) 046362 (0) 952976238 (125) 29853117997 (253) 141389213579 (662)High RRT areaCAA area (mm2) (ratio) 046362 (0) 381276238 (05) 31977117997 (271) 167873213579 (786)
Front Back
Model 0
Model 2x
Model 3x
Model 5x
WSS
(Pa)
6936
4624
2312
0000
Figure 6 Wall shear stress (WSS) distribution in the coronary artery aneurysm at its peak (t 02 s) for the four models
Complexity 7
affect the blood flow and pressure within the region of thelesion itself with little effect on global blood flow Howeverthere were substantial changes in local hemodynamic pa-rameters related to thrombosis in the lesion locationCompared with the model without a lesion all three CAAmodels showed low WSS high OSI and high RRT withthese changes exacerbated as the CAA diameter increased-ese changes were the results of the sudden increase in thediameter of the lumen on entering the CAA -ese resultssuggest there may be a high correlation between CAA di-ameter and the risk of thrombosis CAA hemodynamicstudies may therefore allow the development of a prelimi-nary classification of the risk of thrombosis helping toimprove the effectiveness of anticoagulation therapy andfacilitating better personalization of treatment according to aquantitative hemodynamic plan
Simulation provides a powerful and effective method forestimating important hemodynamic parameters that aredifficult to measure As mentioned above except mass-flowrate which can be easily detected by non-invasive ultra-sound other parameters WSS OSI and RRT cannot bedirectly measured which are usually obtained through invitro experiments or indirect measurements Simulation is anon-invasive way providing a low cost way and avoiding thepotential risk of some invasive ways to obtain hemodynamicparameters
LPM boundary conditions can provide realistic physi-ologic flow conditions as what has been confirmed inprevious studies [38 39] In addition the coronary mi-crocirculation was introduced into the downstreamboundary condition via the LPM Resistance and pressurechanges downstream of the coronary artery could be
accurately captured in this way helping to ensure the ac-curate simulation of physiological conditions in the coro-nary artery -ere was no difference between the models inthe peripheral vascular structure so the CFD models sharedthe same LPM minimizing the impact of factors other thanthe diameter of the CAA -us the differences in resultsbetween the models were due to the differences in CAAdiameters
As the diameter of the CAA increased theWSS in the CAAlesion area progressively decreased with the WSS in Model 5xobserved to be gt10 times lower than that of the normalcoronary artery (Model 0) Parallel plate flow experiments haveshown that a large number of platelets accumulate at locationswith low WSS (lt04 Pa) [40] and animal endothelial cell ex-periments have shown that thrombosis is associated with adecrease in WSS to within the range 00770279Pa [10] In thepresent study the area average values for WSS in Models 3xand 5x were within this range suggesting that CAAs withdiametersgt3 times that of the normal artery are likely to carry ahigh risk of thrombosis Although the area average WSS forModel 2x was much lower than that of the model withoutCAA it was higher than 04Pa suggesting that CAAs withdiameters double that of the normal artery may not be at highrisk of thrombosis Another important pathophysiologicalfactor in vascular disease is endothelial dysfunction Low WSScan locally inhibit the production of certain important sub-stances such as NO [41] An abnormal response to vasodilationagents including the deactivation of NO by free radicals due tothe impairment of acetylcholine or endothelial NO synthasecan lead to abnormal vasoconstriction which can be associatedwith endothelial dysfunction [41] In addition platelets areprone to aggregation in areas of low WSS which further
Front Back
RRT99083
66055
33028
0000
(Pandash1)
Model 0
Model 2x
Model 3x
Model 5x
Figure 8 Relative residence time (RRT) distribution in the coronary artery aneurysm for the four models
8 Complexity
exacerbates the risk of thrombosis WSS in the CAA lesion ofModel 2x was lower than that in the normal model howeverfurther development is still to be studied just taking WSS as areference -e risk for thrombosis in CAAs progresses withincreasing diameter so the risk associatedwithModel 2xwouldbe lower than that for Models 3x and 5x -e development ofCAAs needs further study Although studies have investigatedthe association between WSS and thrombosis the currentunderstanding is not yet comprehensive -erefore the pos-sibility of WSS and thrombosis in the corresponding in vitroexperiments should be the focus of continued research
-e OSIs for the CAAs increased rapidly with increasingdiameter of the lesion with the OSI in Model 5x around 30times greater than that of the normal coronary artery (whichwas close to zero throughout the CAA) Previous studieshave pointed out that when OSI is greater than 02 it willcause endothelial cell damage [31] -e high OSI area(OSIgt 02) ratio increased from 01 to 662 betweenModel 0 and Model 5x In vivo experimental studies ofporcine aortas have reported that disturbed flow (ie anincrease in OSI) promoted the expression of proin-flammatory cytokines in endothelial cells [11] In additionan in vitro study of bovine endothelial cells reported that theexpression of monocyte chemoattractant protein-1 could beinduced by applying a low-amplitude oscillating shear stressof 03 Pa at 1Hz (equivalent to an OSI of 05) and thishemodynamic environment enhanced the binding of en-dothelial cells to monocytes [42] -ese findings suggest thatthe elevated OSI values observed in the CAA models may beassociated with conditions that can trigger thrombosis
-e RRT values for the CAAs increased dramatically withincreasing diameters of the lesions with the RRT for Model5xgt100 times greater than that of the normal coronary artery-e high RRTarea ratio increased from 01 to 786 betweenModel 0 and Model 5x -ese findings indicate that the bloodflow in the CAA recirculates when the diameter of the lumenincreases resulting in prolonged contact time between the CAAwall and the blood Studies have reported a significantly in-creased risk of thrombosis when RRT is gt10Paminus1 [12 34] -eRRTvalues forModels 3x and 5x in the present study were bothgt10Paminus1 suggesting a high risk of thrombosis when the di-ameter of a CAA exceeds three times that of the normal cor-onary artery Conversely the RRTforModel 2xwasmuch lowerthan 10Paminus1 suggesting that the risk of thrombosis may be lowwhen the diameter of the CAA is only double that of the normalartery Although there have been various studies of the rela-tionship between RRTand aneurysms [43] the current state ofknowledge remains insufficient for patient classification forexample there are no appropriate ranges of RRT values fordistinguishing the risk level of thrombosis which needs furtherstudy
In summary the comparison of our modeling resultswith the findings of previous studies suggested that the lowWSS high OSI and high RRT observed in the CAAs wouldsignificantly increase the risk of thrombosis However therisk varied considerably between the different diameters ofCAA -e WSS OSI and RRT values for Models 3x and 5xall suggested a high risk of thrombosis based on the previousstudy results-us for CAAs with diameters gt3 times that of
the normal coronary artery the risk of uncertainty withconservative treatment may be higher than the risk asso-ciated with surgery suggesting that the surgical operationshould be considered Conversely although the WSS OSIand RRT values for Model 2x were unfavorable comparedwith those of the model of the normal coronary arteryimplying an increased risk of thrombosis the magnitude ofthese differences was insufficient to support a prediction ofthe future development of the CAA For CAAs with a di-ameter up to two times that of the normal coronary arteryconservative drug treatment may be the better optionavoiding the risks associated with surgery
-e limitations of this study are as follows First this studyhas only one patientrsquos data and the conclusion may be ac-cidental We need to use more data for research Secondly animportant assumption used in the CFD calculation is the rigidwall where in fact elastic walls should be used In particularthe coronary artery will deform greatly as the heart contractswhich can be solved by two-way FSI in the future
5 Conclusion
-e evaluation of the relationship between hemodynamiceffects and different diameters of CAAs was performed inthis research through the CFD simulation method -erelationship between thrombosis risk and the size of theCAA diameter could be preliminarily evaluated from ahemodynamic perspective
We found that as the diameter of the CAA increased therisk of thrombosis increased substantially -e results sug-gested that when the diameter of a CAA is small (less thandouble that of the normal coronary artery) the risk ofthrombosis may be relatively low suggesting that medica-tion may be a sufficient approach for the patient avoidingthe uncertain risks associated with surgery If the diameter ofCAA is large (gt3 times that of the normal coronary artery)there may be a high risk of thrombosis and surgicaltreatment could be considered A similar approach could betaken in future studies to systematically assess the risk as-sociated with different shapes sizes and locations of an-eurysms Such approaches may form the basis for moresophisticated hemodynamic-based risk stratificationmethods supporting clinical decision-making in assessmentof CAA
Data Availability
-e data used to support the findings of this study areavailable from the corresponding author upon request
Conflicts of Interest
-e authors declare no conflicts of interest
Acknowledgments
-is research was supported by the National Natural ScienceFoundation of China (nos 11832003 and 11772016) andJSPS KAKENHI under Grant no JP18K18355 -is researchwas partially supported by the Creation of a Development
Complexity 9
Platform for ImplantableWearable Medical Devices by aNovel Physiological Data Integration System of the Programon Open Innovation Platform with Enterprises ResearchInstitute and Academia (OPERA) from the Japan Scienceand Technology Agency (JST) -is research was also sup-ported by Collaborative Research Project 2020 Institute ofFluid Science Tohoku University (J20R001) with the GrantNumber JP18K18355
References
[1] H Kato T Sugimura T Akagi et al ldquoLong-term conse-quences of kawasaki diseaserdquo Circulation vol 94 no 6pp 1379ndash1385 1996
[2] S A Sherif O O Tok O Taskoylu O Goktekin andI D Kilic ldquoCoronary artery aneurysms a review of theepidemiology pathophysiology diagnosis and treatmentrdquoFrontiers in Cardiovascular Medicine vol 4 2017
[3] E Beckmann S Rustum S Marquardt et al ldquoSurgicaltreatment of coronary artery aneurysmsrdquo Journal of CardiacSurgery vol 32 no 11 pp 674ndash679 2017
[4] M Syed M Lesch and A D Syed ldquoCoronary artery aneu-rysm a reviewrdquo Progress in Cardiovascular Diseases vol 40no 1 pp 77ndash84 1997
[5] G G Hartnell B M Parnell and R B Pridie ldquoCoronaryartery ectasia Its prevalence and clinical significance in 4993patientsrdquo British Heart Journal vol 54 no 4 1985
[6] A Satran B A Bart C R Henry et al ldquoIncreased prevalenceof coronary artery aneurysms among cocaine usersrdquo Circu-lation vol 111 no 19 pp 2424ndash2429 2005
[7] O Topaz M S Rutherford S M Bojack et al ldquoGiant an-eurysms of coronary arteries and saphenous vein graftsangiographic findings and histopathological correlatesrdquoCardiovascular Pathology vol 14 no 6 pp 298ndash302 2005
[8] A P Antoniadis Y S Chatzizisis and G D GiannoglouldquoPathogenetic mechanisms of coronary ectasiardquo InternationalJournal of Cardiology vol 130 no 3 pp 335ndash343 2008
[9] J B Gordon A M Kahn and J C Burns ldquoWhen childrenwith kawasaki disease grow uprdquo Journal of the AmericanCollege of Cardiology vol 54 no 21 pp 1911ndash1920 2009
[10] P Sriramarao L Languino and D Altieri ldquoFibrinogenmediates leukocyte-endothelium bridging in vivo at low shearforcesrdquo Blood vol 88 no 9 pp 3416ndash3423 1996
[11] A G Passerini D C Polacek C Shi et al ldquoCoexistingproinflammatory and antioxidative endothelial transcriptionprofiles in a disturbed flow region of the adult porcine aortardquoProceedings of the National Academy of Sciences vol 101no 89 pp 2482ndash2487
[12] U Morbiducci D Gallo R Ponzini et al ldquoQuantitativeanalysis of bulk flow in image-based hemodynamic models ofthe carotid bifurcation the influence of outflow conditions astest caserdquo Annals of Biomedical Engineering vol 38 no 12pp 3688ndash3705 2010
[13] T Ohkubo R Fukazawa E Ikegami and S Ogawa ldquoReducedshear stress and disturbed flow may lead to coronary aneu-rysm and thrombus formationsrdquo Pediatrics Internationalvol 49 no 1 pp 1ndash7 2007
[14] H Anzai T Watanabe X Han et al ldquoEndothelial cell dis-tributions and migration under conditions of flow shear stressaround a stent wirerdquo Technology and Health Care vol 28no 4 pp 345ndash354 2020
[15] M Zhang Y Li X Zhao et al ldquoHaemodynamic effects ofstent diameter and compaction ratio on flow-diversion
treatment of intracranial aneurysms a numerical study of asuccessful and an unsuccessful caserdquo Journal of Biomechanicsvol 58 pp 179ndash186 2017
[16] H Anzai B Chopard and M Ohta ldquoCombinational opti-mization of strut placement for intracranial stent using arealistic aneurysmrdquo Journal of Flow Control Measurement ampVisualization vol 2 no 2 pp 67ndash77 2014
[17] J P Ku M T Draney F R Arko et al ldquoIn vivo validation ofnumerical prediction of blood flow in arterial bypass graftsrdquoAnnals of Biomedical Engineering vol 30 no 6 pp 743ndash7522002
[18] A R Soler F Kabinejadian M A Slevin P J Bartolo andA Keshmiri ldquoOptimisation of a novel spiral-inducing bypassgraft using computational fluid dynamicsrdquo Scientific Reportsvol 7 no 1 p 1865 2017
[19] H Zhang L Li C Cheng and X Sun ldquoClinical value ofhomodynamic numerical simulation applied in the treatmentof cerebral aneurysmrdquo Experimental and Gerapeutic Medi-cine vol 4 no 6 pp 5401ndash5494 2017
[20] A S Les S C Shadden C A Figueroa et al ldquoQuantificationof hemodynamics in abdominal aortic aneurysms during restand exercise using magnetic resonance imaging and com-putational fluid dynamicsrdquo Annals of Biomedical Engineeringvol 38 no 4 pp 1288ndash1313 2010
[21] M Piccinelli A Veneziani D A Steinman A Remuzzi andL Antiga ldquoA framework for geometric analysis of vascularstructures application to cerebral aneurysmsrdquo IEEE Trans-actions on Medical Imaging vol 28 no 8 pp 1141ndash11552009
[22] H J Kim I E Vignon-Clementel J S CooganC A Figueroa K E Jansen and C A Taylor ldquoPatient-specific modeling of blood flow and pressure in humancoronary arteriesrdquo Annals of Biomedical Engineering vol 38no 10 pp 3195ndash3209 2010
[23] C A Taylor T A Fonte and J K Min ldquoComputational fluiddynamics applied to cardiac computed tomography fornoninvasive quantification of fractional flow reserverdquo Journalof the American College of Cardiology vol 61 no 22pp 2233ndash2241 2013
[24] I E V Clementel C A Figueroa K E Jansen andC A Taylor ldquoOutflow boundary conditions for 3D simula-tions of non-periodic blood flow and pressure fields in de-formable arteriesrdquo Computer Methods in Biomechanics andBiomedical Engineering vol 13 no 5 pp 625ndash640 2010
[25] N Stergiopulos J J Meister and N Westerhof ldquoDetermi-nants of stroke volume and systolic and diastolic aorticpressurerdquoGe American Journal of Physiology vol 270 no 6pp 2050ndash2059 1996
[26] M Zamir P Sinclair and T H Wonnacott ldquoRelation be-tween diameter and flow in major branches of the arch of theaortardquo Journal of Biomechanics vol 25 no 11 pp 1303ndash13101992
[27] K Johnson P Sharma and J Oshinski ldquoCoronary artery flowmeasurement using navigator echo gated phase contrastmagnetic resonance velocity mapping at 30 teslardquo Journal ofBiomechanics vol 41 no 3 pp 595ndash602 2008
[28] F P Salvuccia C A Perazzob S Sallesa J G Barrac andR L Armentano ldquoInfluence of inlet conditions in wall shearstress distributions of left coronary arteries in patient-specificsimulationsrdquo Mecanica Computacional vol XXIXpp 5953ndash5960 2010
[29] B C Lopez B Calvo and P Estefanıa Patient-SpecificComputational Modeling Springer Berlin Germany 2012thedition 2012
10 Complexity
[30] D N Ghista and F Kabinejadian ldquoCoronary artery bypassgrafting hemodynamics and anastomosis design a biomedicalengineering reviewrdquo BioMedical Engineering Online vol 12no 129 2013
[31] F P Glor F P Glor B Ariff et al ldquoImage-based carotid flowreconstruction a comparison between MRI and ultrasoundrdquoPhysiological Measurement vol 25 no 6 pp 1495ndash15092004
[32] S-W Lee L Antiga and D A Steinman ldquoCorrelationsamong indicators of disturbed flow at the normal carotidbifurcationrdquo Journal of Biomechanical Engineering vol 131no 6 Article ID 061013 2009
[33] H A Himburg ldquoSpatial comparison between wall shear stressmeasures and porcine arterial endothelial permeabilityrdquo AJPHeart and Circulatory Physiology vol 286 no 5 pp 1916ndash1922 2004
[34] T Suess J Anderson L Danielson et al ldquoExamination ofnear-wall hemodynamic parameters in the renal bridgingstent of various stent graft configurations for repairing vis-ceral branched aortic aneurysmsrdquo Journal of Vascular Sur-gery vol 64 no 3 pp 788ndash796 2016
[35] H Zhang X Yu F Ji and F Sun ldquoCoronary artery aneurysmformation after drug-coatedrdquo Medicine vol 97 no 45 2018
[36] N G Gutierrez M Mathew B W McCrindle et al ldquoHe-modynamic variables in aneurysms are associated withthrombotic risk in children with Kawasaki diseaserdquo Inter-national Journal of Cardiology vol 281 pp 15ndash21 2019
[37] C Karmonik G Chintalapani T Redel et al ldquoHemody-namics at the ostium of cerebral aneurysms with relation topost-treatment changes by a virtual flow diverter a compu-tational fluid dynamics studyrdquo in Proceedings of the AnnualInternational Conference of the IEEE Engineering in Medicineand Biology Society EMBS pp 1895ndash1898 Osaka Japan July2013
[38] J T Marcus H G Smeenk J P A KuijerR J Van Der Geest R M Heethaar and A C Van RossumldquoFlow profiles in the left anterior descending and the rightcoronary artery assessed byMR velocity quantification effectsof through-plane and in-plane motion of the heartrdquo Journal ofComputer Assisted Tomography vol 23 no 4 pp 567ndash5761999
[39] Y Shi P Lawford and R Hose ldquoReview of zero-D and 1-Dmodels of blood flow in the cardiovascular systemrdquo Bio-Medical Engineering Online vol 10 no 1 p 33 2011
[40] M Kroll J Hellums L McIntire A Schafer and J MoakeldquoPlatelets and shear stressrdquo Blood vol 88 no 5pp 1525ndash1541 1996
[41] J-J Chiu and S Chien ldquoEffects of disturbed flow on vascularendothelium pathophysiological basis and clinical perspec-tivesrdquo Physiological Reviews vol 91 no 1 pp 327ndash387 2011
[42] J Hwang M H Ing A Salazar et al ldquoPulsatile versus os-cillatory shear stress regulates NADPH oxidase subunit ex-pressionrdquo Circulation Research vol 93 no 12 pp 1225ndash12322003
[43] S-i Sugiyama K Niizuma T Nakayama et al ldquoRelativeresidence time prolongation in intracranial aneurysmsrdquoNeurosurgery vol 73 no 5 pp 767ndash776 2013
Complexity 11

associated with risk of thrombosis and that is a morepredictive factor of thrombosis than aneurysm diameter[36] We confirmed that hemodynamic research is beneficialfor aneurysm diagnosis and treatment [37] -erefore in
this study we quantitatively calculated the hemodynamicparameters of CAA of different diameters in order to esti-mate the relationship between the risk level of thrombosisand the size of CAA -e results showed that CAAs only
Front Back
OSI0495
0330
0165
0000
Model 0
Model 2x
Model 3x
Model 5x
Figure 7 Oscillatory shear index (OSI) distribution in the coronary artery aneurysm for the four models
Table 3 -e area of high OSI and RRT in the aneurysm and the area of aneurysm
Model 0 Model 2x Model 3x Model 5xHigh OSI areaCAA area (mm2) (ratio) 046362 (0) 952976238 (125) 29853117997 (253) 141389213579 (662)High RRT areaCAA area (mm2) (ratio) 046362 (0) 381276238 (05) 31977117997 (271) 167873213579 (786)
Front Back
Model 0
Model 2x
Model 3x
Model 5x
WSS
(Pa)
6936
4624
2312
0000
Figure 6 Wall shear stress (WSS) distribution in the coronary artery aneurysm at its peak (t 02 s) for the four models
Complexity 7
affect the blood flow and pressure within the region of thelesion itself with little effect on global blood flow Howeverthere were substantial changes in local hemodynamic pa-rameters related to thrombosis in the lesion locationCompared with the model without a lesion all three CAAmodels showed low WSS high OSI and high RRT withthese changes exacerbated as the CAA diameter increased-ese changes were the results of the sudden increase in thediameter of the lumen on entering the CAA -ese resultssuggest there may be a high correlation between CAA di-ameter and the risk of thrombosis CAA hemodynamicstudies may therefore allow the development of a prelimi-nary classification of the risk of thrombosis helping toimprove the effectiveness of anticoagulation therapy andfacilitating better personalization of treatment according to aquantitative hemodynamic plan
Simulation provides a powerful and effective method forestimating important hemodynamic parameters that aredifficult to measure As mentioned above except mass-flowrate which can be easily detected by non-invasive ultra-sound other parameters WSS OSI and RRT cannot bedirectly measured which are usually obtained through invitro experiments or indirect measurements Simulation is anon-invasive way providing a low cost way and avoiding thepotential risk of some invasive ways to obtain hemodynamicparameters
LPM boundary conditions can provide realistic physi-ologic flow conditions as what has been confirmed inprevious studies [38 39] In addition the coronary mi-crocirculation was introduced into the downstreamboundary condition via the LPM Resistance and pressurechanges downstream of the coronary artery could be
accurately captured in this way helping to ensure the ac-curate simulation of physiological conditions in the coro-nary artery -ere was no difference between the models inthe peripheral vascular structure so the CFD models sharedthe same LPM minimizing the impact of factors other thanthe diameter of the CAA -us the differences in resultsbetween the models were due to the differences in CAAdiameters
As the diameter of the CAA increased theWSS in the CAAlesion area progressively decreased with the WSS in Model 5xobserved to be gt10 times lower than that of the normalcoronary artery (Model 0) Parallel plate flow experiments haveshown that a large number of platelets accumulate at locationswith low WSS (lt04 Pa) [40] and animal endothelial cell ex-periments have shown that thrombosis is associated with adecrease in WSS to within the range 00770279Pa [10] In thepresent study the area average values for WSS in Models 3xand 5x were within this range suggesting that CAAs withdiametersgt3 times that of the normal artery are likely to carry ahigh risk of thrombosis Although the area average WSS forModel 2x was much lower than that of the model withoutCAA it was higher than 04Pa suggesting that CAAs withdiameters double that of the normal artery may not be at highrisk of thrombosis Another important pathophysiologicalfactor in vascular disease is endothelial dysfunction Low WSScan locally inhibit the production of certain important sub-stances such as NO [41] An abnormal response to vasodilationagents including the deactivation of NO by free radicals due tothe impairment of acetylcholine or endothelial NO synthasecan lead to abnormal vasoconstriction which can be associatedwith endothelial dysfunction [41] In addition platelets areprone to aggregation in areas of low WSS which further
Front Back
RRT99083
66055
33028
0000
(Pandash1)
Model 0
Model 2x
Model 3x
Model 5x
Figure 8 Relative residence time (RRT) distribution in the coronary artery aneurysm for the four models
8 Complexity
exacerbates the risk of thrombosis WSS in the CAA lesion ofModel 2x was lower than that in the normal model howeverfurther development is still to be studied just taking WSS as areference -e risk for thrombosis in CAAs progresses withincreasing diameter so the risk associatedwithModel 2xwouldbe lower than that for Models 3x and 5x -e development ofCAAs needs further study Although studies have investigatedthe association between WSS and thrombosis the currentunderstanding is not yet comprehensive -erefore the pos-sibility of WSS and thrombosis in the corresponding in vitroexperiments should be the focus of continued research
-e OSIs for the CAAs increased rapidly with increasingdiameter of the lesion with the OSI in Model 5x around 30times greater than that of the normal coronary artery (whichwas close to zero throughout the CAA) Previous studieshave pointed out that when OSI is greater than 02 it willcause endothelial cell damage [31] -e high OSI area(OSIgt 02) ratio increased from 01 to 662 betweenModel 0 and Model 5x In vivo experimental studies ofporcine aortas have reported that disturbed flow (ie anincrease in OSI) promoted the expression of proin-flammatory cytokines in endothelial cells [11] In additionan in vitro study of bovine endothelial cells reported that theexpression of monocyte chemoattractant protein-1 could beinduced by applying a low-amplitude oscillating shear stressof 03 Pa at 1Hz (equivalent to an OSI of 05) and thishemodynamic environment enhanced the binding of en-dothelial cells to monocytes [42] -ese findings suggest thatthe elevated OSI values observed in the CAA models may beassociated with conditions that can trigger thrombosis
-e RRT values for the CAAs increased dramatically withincreasing diameters of the lesions with the RRT for Model5xgt100 times greater than that of the normal coronary artery-e high RRTarea ratio increased from 01 to 786 betweenModel 0 and Model 5x -ese findings indicate that the bloodflow in the CAA recirculates when the diameter of the lumenincreases resulting in prolonged contact time between the CAAwall and the blood Studies have reported a significantly in-creased risk of thrombosis when RRT is gt10Paminus1 [12 34] -eRRTvalues forModels 3x and 5x in the present study were bothgt10Paminus1 suggesting a high risk of thrombosis when the di-ameter of a CAA exceeds three times that of the normal cor-onary artery Conversely the RRTforModel 2xwasmuch lowerthan 10Paminus1 suggesting that the risk of thrombosis may be lowwhen the diameter of the CAA is only double that of the normalartery Although there have been various studies of the rela-tionship between RRTand aneurysms [43] the current state ofknowledge remains insufficient for patient classification forexample there are no appropriate ranges of RRT values fordistinguishing the risk level of thrombosis which needs furtherstudy
In summary the comparison of our modeling resultswith the findings of previous studies suggested that the lowWSS high OSI and high RRT observed in the CAAs wouldsignificantly increase the risk of thrombosis However therisk varied considerably between the different diameters ofCAA -e WSS OSI and RRT values for Models 3x and 5xall suggested a high risk of thrombosis based on the previousstudy results-us for CAAs with diameters gt3 times that of
the normal coronary artery the risk of uncertainty withconservative treatment may be higher than the risk asso-ciated with surgery suggesting that the surgical operationshould be considered Conversely although the WSS OSIand RRT values for Model 2x were unfavorable comparedwith those of the model of the normal coronary arteryimplying an increased risk of thrombosis the magnitude ofthese differences was insufficient to support a prediction ofthe future development of the CAA For CAAs with a di-ameter up to two times that of the normal coronary arteryconservative drug treatment may be the better optionavoiding the risks associated with surgery
-e limitations of this study are as follows First this studyhas only one patientrsquos data and the conclusion may be ac-cidental We need to use more data for research Secondly animportant assumption used in the CFD calculation is the rigidwall where in fact elastic walls should be used In particularthe coronary artery will deform greatly as the heart contractswhich can be solved by two-way FSI in the future
5 Conclusion
-e evaluation of the relationship between hemodynamiceffects and different diameters of CAAs was performed inthis research through the CFD simulation method -erelationship between thrombosis risk and the size of theCAA diameter could be preliminarily evaluated from ahemodynamic perspective
We found that as the diameter of the CAA increased therisk of thrombosis increased substantially -e results sug-gested that when the diameter of a CAA is small (less thandouble that of the normal coronary artery) the risk ofthrombosis may be relatively low suggesting that medica-tion may be a sufficient approach for the patient avoidingthe uncertain risks associated with surgery If the diameter ofCAA is large (gt3 times that of the normal coronary artery)there may be a high risk of thrombosis and surgicaltreatment could be considered A similar approach could betaken in future studies to systematically assess the risk as-sociated with different shapes sizes and locations of an-eurysms Such approaches may form the basis for moresophisticated hemodynamic-based risk stratificationmethods supporting clinical decision-making in assessmentof CAA
Data Availability
-e data used to support the findings of this study areavailable from the corresponding author upon request
Conflicts of Interest
-e authors declare no conflicts of interest
Acknowledgments
-is research was supported by the National Natural ScienceFoundation of China (nos 11832003 and 11772016) andJSPS KAKENHI under Grant no JP18K18355 -is researchwas partially supported by the Creation of a Development
Complexity 9
Platform for ImplantableWearable Medical Devices by aNovel Physiological Data Integration System of the Programon Open Innovation Platform with Enterprises ResearchInstitute and Academia (OPERA) from the Japan Scienceand Technology Agency (JST) -is research was also sup-ported by Collaborative Research Project 2020 Institute ofFluid Science Tohoku University (J20R001) with the GrantNumber JP18K18355
References
[1] H Kato T Sugimura T Akagi et al ldquoLong-term conse-quences of kawasaki diseaserdquo Circulation vol 94 no 6pp 1379ndash1385 1996
[2] S A Sherif O O Tok O Taskoylu O Goktekin andI D Kilic ldquoCoronary artery aneurysms a review of theepidemiology pathophysiology diagnosis and treatmentrdquoFrontiers in Cardiovascular Medicine vol 4 2017
[3] E Beckmann S Rustum S Marquardt et al ldquoSurgicaltreatment of coronary artery aneurysmsrdquo Journal of CardiacSurgery vol 32 no 11 pp 674ndash679 2017
[4] M Syed M Lesch and A D Syed ldquoCoronary artery aneu-rysm a reviewrdquo Progress in Cardiovascular Diseases vol 40no 1 pp 77ndash84 1997
[5] G G Hartnell B M Parnell and R B Pridie ldquoCoronaryartery ectasia Its prevalence and clinical significance in 4993patientsrdquo British Heart Journal vol 54 no 4 1985
[6] A Satran B A Bart C R Henry et al ldquoIncreased prevalenceof coronary artery aneurysms among cocaine usersrdquo Circu-lation vol 111 no 19 pp 2424ndash2429 2005
[7] O Topaz M S Rutherford S M Bojack et al ldquoGiant an-eurysms of coronary arteries and saphenous vein graftsangiographic findings and histopathological correlatesrdquoCardiovascular Pathology vol 14 no 6 pp 298ndash302 2005
[8] A P Antoniadis Y S Chatzizisis and G D GiannoglouldquoPathogenetic mechanisms of coronary ectasiardquo InternationalJournal of Cardiology vol 130 no 3 pp 335ndash343 2008
[9] J B Gordon A M Kahn and J C Burns ldquoWhen childrenwith kawasaki disease grow uprdquo Journal of the AmericanCollege of Cardiology vol 54 no 21 pp 1911ndash1920 2009
[10] P Sriramarao L Languino and D Altieri ldquoFibrinogenmediates leukocyte-endothelium bridging in vivo at low shearforcesrdquo Blood vol 88 no 9 pp 3416ndash3423 1996
[11] A G Passerini D C Polacek C Shi et al ldquoCoexistingproinflammatory and antioxidative endothelial transcriptionprofiles in a disturbed flow region of the adult porcine aortardquoProceedings of the National Academy of Sciences vol 101no 89 pp 2482ndash2487
[12] U Morbiducci D Gallo R Ponzini et al ldquoQuantitativeanalysis of bulk flow in image-based hemodynamic models ofthe carotid bifurcation the influence of outflow conditions astest caserdquo Annals of Biomedical Engineering vol 38 no 12pp 3688ndash3705 2010
[13] T Ohkubo R Fukazawa E Ikegami and S Ogawa ldquoReducedshear stress and disturbed flow may lead to coronary aneu-rysm and thrombus formationsrdquo Pediatrics Internationalvol 49 no 1 pp 1ndash7 2007
[14] H Anzai T Watanabe X Han et al ldquoEndothelial cell dis-tributions and migration under conditions of flow shear stressaround a stent wirerdquo Technology and Health Care vol 28no 4 pp 345ndash354 2020
[15] M Zhang Y Li X Zhao et al ldquoHaemodynamic effects ofstent diameter and compaction ratio on flow-diversion
treatment of intracranial aneurysms a numerical study of asuccessful and an unsuccessful caserdquo Journal of Biomechanicsvol 58 pp 179ndash186 2017
[16] H Anzai B Chopard and M Ohta ldquoCombinational opti-mization of strut placement for intracranial stent using arealistic aneurysmrdquo Journal of Flow Control Measurement ampVisualization vol 2 no 2 pp 67ndash77 2014
[17] J P Ku M T Draney F R Arko et al ldquoIn vivo validation ofnumerical prediction of blood flow in arterial bypass graftsrdquoAnnals of Biomedical Engineering vol 30 no 6 pp 743ndash7522002
[18] A R Soler F Kabinejadian M A Slevin P J Bartolo andA Keshmiri ldquoOptimisation of a novel spiral-inducing bypassgraft using computational fluid dynamicsrdquo Scientific Reportsvol 7 no 1 p 1865 2017
[19] H Zhang L Li C Cheng and X Sun ldquoClinical value ofhomodynamic numerical simulation applied in the treatmentof cerebral aneurysmrdquo Experimental and Gerapeutic Medi-cine vol 4 no 6 pp 5401ndash5494 2017
[20] A S Les S C Shadden C A Figueroa et al ldquoQuantificationof hemodynamics in abdominal aortic aneurysms during restand exercise using magnetic resonance imaging and com-putational fluid dynamicsrdquo Annals of Biomedical Engineeringvol 38 no 4 pp 1288ndash1313 2010
[21] M Piccinelli A Veneziani D A Steinman A Remuzzi andL Antiga ldquoA framework for geometric analysis of vascularstructures application to cerebral aneurysmsrdquo IEEE Trans-actions on Medical Imaging vol 28 no 8 pp 1141ndash11552009
[22] H J Kim I E Vignon-Clementel J S CooganC A Figueroa K E Jansen and C A Taylor ldquoPatient-specific modeling of blood flow and pressure in humancoronary arteriesrdquo Annals of Biomedical Engineering vol 38no 10 pp 3195ndash3209 2010
[23] C A Taylor T A Fonte and J K Min ldquoComputational fluiddynamics applied to cardiac computed tomography fornoninvasive quantification of fractional flow reserverdquo Journalof the American College of Cardiology vol 61 no 22pp 2233ndash2241 2013
[24] I E V Clementel C A Figueroa K E Jansen andC A Taylor ldquoOutflow boundary conditions for 3D simula-tions of non-periodic blood flow and pressure fields in de-formable arteriesrdquo Computer Methods in Biomechanics andBiomedical Engineering vol 13 no 5 pp 625ndash640 2010
[25] N Stergiopulos J J Meister and N Westerhof ldquoDetermi-nants of stroke volume and systolic and diastolic aorticpressurerdquoGe American Journal of Physiology vol 270 no 6pp 2050ndash2059 1996
[26] M Zamir P Sinclair and T H Wonnacott ldquoRelation be-tween diameter and flow in major branches of the arch of theaortardquo Journal of Biomechanics vol 25 no 11 pp 1303ndash13101992
[27] K Johnson P Sharma and J Oshinski ldquoCoronary artery flowmeasurement using navigator echo gated phase contrastmagnetic resonance velocity mapping at 30 teslardquo Journal ofBiomechanics vol 41 no 3 pp 595ndash602 2008
[28] F P Salvuccia C A Perazzob S Sallesa J G Barrac andR L Armentano ldquoInfluence of inlet conditions in wall shearstress distributions of left coronary arteries in patient-specificsimulationsrdquo Mecanica Computacional vol XXIXpp 5953ndash5960 2010
[29] B C Lopez B Calvo and P Estefanıa Patient-SpecificComputational Modeling Springer Berlin Germany 2012thedition 2012
10 Complexity
[30] D N Ghista and F Kabinejadian ldquoCoronary artery bypassgrafting hemodynamics and anastomosis design a biomedicalengineering reviewrdquo BioMedical Engineering Online vol 12no 129 2013
[31] F P Glor F P Glor B Ariff et al ldquoImage-based carotid flowreconstruction a comparison between MRI and ultrasoundrdquoPhysiological Measurement vol 25 no 6 pp 1495ndash15092004
[32] S-W Lee L Antiga and D A Steinman ldquoCorrelationsamong indicators of disturbed flow at the normal carotidbifurcationrdquo Journal of Biomechanical Engineering vol 131no 6 Article ID 061013 2009
[33] H A Himburg ldquoSpatial comparison between wall shear stressmeasures and porcine arterial endothelial permeabilityrdquo AJPHeart and Circulatory Physiology vol 286 no 5 pp 1916ndash1922 2004
[34] T Suess J Anderson L Danielson et al ldquoExamination ofnear-wall hemodynamic parameters in the renal bridgingstent of various stent graft configurations for repairing vis-ceral branched aortic aneurysmsrdquo Journal of Vascular Sur-gery vol 64 no 3 pp 788ndash796 2016
[35] H Zhang X Yu F Ji and F Sun ldquoCoronary artery aneurysmformation after drug-coatedrdquo Medicine vol 97 no 45 2018
[36] N G Gutierrez M Mathew B W McCrindle et al ldquoHe-modynamic variables in aneurysms are associated withthrombotic risk in children with Kawasaki diseaserdquo Inter-national Journal of Cardiology vol 281 pp 15ndash21 2019
[37] C Karmonik G Chintalapani T Redel et al ldquoHemody-namics at the ostium of cerebral aneurysms with relation topost-treatment changes by a virtual flow diverter a compu-tational fluid dynamics studyrdquo in Proceedings of the AnnualInternational Conference of the IEEE Engineering in Medicineand Biology Society EMBS pp 1895ndash1898 Osaka Japan July2013
[38] J T Marcus H G Smeenk J P A KuijerR J Van Der Geest R M Heethaar and A C Van RossumldquoFlow profiles in the left anterior descending and the rightcoronary artery assessed byMR velocity quantification effectsof through-plane and in-plane motion of the heartrdquo Journal ofComputer Assisted Tomography vol 23 no 4 pp 567ndash5761999
[39] Y Shi P Lawford and R Hose ldquoReview of zero-D and 1-Dmodels of blood flow in the cardiovascular systemrdquo Bio-Medical Engineering Online vol 10 no 1 p 33 2011
[40] M Kroll J Hellums L McIntire A Schafer and J MoakeldquoPlatelets and shear stressrdquo Blood vol 88 no 5pp 1525ndash1541 1996
[41] J-J Chiu and S Chien ldquoEffects of disturbed flow on vascularendothelium pathophysiological basis and clinical perspec-tivesrdquo Physiological Reviews vol 91 no 1 pp 327ndash387 2011
[42] J Hwang M H Ing A Salazar et al ldquoPulsatile versus os-cillatory shear stress regulates NADPH oxidase subunit ex-pressionrdquo Circulation Research vol 93 no 12 pp 1225ndash12322003
[43] S-i Sugiyama K Niizuma T Nakayama et al ldquoRelativeresidence time prolongation in intracranial aneurysmsrdquoNeurosurgery vol 73 no 5 pp 767ndash776 2013
Complexity 11

affect the blood flow and pressure within the region of thelesion itself with little effect on global blood flow Howeverthere were substantial changes in local hemodynamic pa-rameters related to thrombosis in the lesion locationCompared with the model without a lesion all three CAAmodels showed low WSS high OSI and high RRT withthese changes exacerbated as the CAA diameter increased-ese changes were the results of the sudden increase in thediameter of the lumen on entering the CAA -ese resultssuggest there may be a high correlation between CAA di-ameter and the risk of thrombosis CAA hemodynamicstudies may therefore allow the development of a prelimi-nary classification of the risk of thrombosis helping toimprove the effectiveness of anticoagulation therapy andfacilitating better personalization of treatment according to aquantitative hemodynamic plan
Simulation provides a powerful and effective method forestimating important hemodynamic parameters that aredifficult to measure As mentioned above except mass-flowrate which can be easily detected by non-invasive ultra-sound other parameters WSS OSI and RRT cannot bedirectly measured which are usually obtained through invitro experiments or indirect measurements Simulation is anon-invasive way providing a low cost way and avoiding thepotential risk of some invasive ways to obtain hemodynamicparameters
LPM boundary conditions can provide realistic physi-ologic flow conditions as what has been confirmed inprevious studies [38 39] In addition the coronary mi-crocirculation was introduced into the downstreamboundary condition via the LPM Resistance and pressurechanges downstream of the coronary artery could be
accurately captured in this way helping to ensure the ac-curate simulation of physiological conditions in the coro-nary artery -ere was no difference between the models inthe peripheral vascular structure so the CFD models sharedthe same LPM minimizing the impact of factors other thanthe diameter of the CAA -us the differences in resultsbetween the models were due to the differences in CAAdiameters
As the diameter of the CAA increased theWSS in the CAAlesion area progressively decreased with the WSS in Model 5xobserved to be gt10 times lower than that of the normalcoronary artery (Model 0) Parallel plate flow experiments haveshown that a large number of platelets accumulate at locationswith low WSS (lt04 Pa) [40] and animal endothelial cell ex-periments have shown that thrombosis is associated with adecrease in WSS to within the range 00770279Pa [10] In thepresent study the area average values for WSS in Models 3xand 5x were within this range suggesting that CAAs withdiametersgt3 times that of the normal artery are likely to carry ahigh risk of thrombosis Although the area average WSS forModel 2x was much lower than that of the model withoutCAA it was higher than 04Pa suggesting that CAAs withdiameters double that of the normal artery may not be at highrisk of thrombosis Another important pathophysiologicalfactor in vascular disease is endothelial dysfunction Low WSScan locally inhibit the production of certain important sub-stances such as NO [41] An abnormal response to vasodilationagents including the deactivation of NO by free radicals due tothe impairment of acetylcholine or endothelial NO synthasecan lead to abnormal vasoconstriction which can be associatedwith endothelial dysfunction [41] In addition platelets areprone to aggregation in areas of low WSS which further
Front Back
RRT99083
66055
33028
0000
(Pandash1)
Model 0
Model 2x
Model 3x
Model 5x
Figure 8 Relative residence time (RRT) distribution in the coronary artery aneurysm for the four models
8 Complexity
exacerbates the risk of thrombosis WSS in the CAA lesion ofModel 2x was lower than that in the normal model howeverfurther development is still to be studied just taking WSS as areference -e risk for thrombosis in CAAs progresses withincreasing diameter so the risk associatedwithModel 2xwouldbe lower than that for Models 3x and 5x -e development ofCAAs needs further study Although studies have investigatedthe association between WSS and thrombosis the currentunderstanding is not yet comprehensive -erefore the pos-sibility of WSS and thrombosis in the corresponding in vitroexperiments should be the focus of continued research
-e OSIs for the CAAs increased rapidly with increasingdiameter of the lesion with the OSI in Model 5x around 30times greater than that of the normal coronary artery (whichwas close to zero throughout the CAA) Previous studieshave pointed out that when OSI is greater than 02 it willcause endothelial cell damage [31] -e high OSI area(OSIgt 02) ratio increased from 01 to 662 betweenModel 0 and Model 5x In vivo experimental studies ofporcine aortas have reported that disturbed flow (ie anincrease in OSI) promoted the expression of proin-flammatory cytokines in endothelial cells [11] In additionan in vitro study of bovine endothelial cells reported that theexpression of monocyte chemoattractant protein-1 could beinduced by applying a low-amplitude oscillating shear stressof 03 Pa at 1Hz (equivalent to an OSI of 05) and thishemodynamic environment enhanced the binding of en-dothelial cells to monocytes [42] -ese findings suggest thatthe elevated OSI values observed in the CAA models may beassociated with conditions that can trigger thrombosis
-e RRT values for the CAAs increased dramatically withincreasing diameters of the lesions with the RRT for Model5xgt100 times greater than that of the normal coronary artery-e high RRTarea ratio increased from 01 to 786 betweenModel 0 and Model 5x -ese findings indicate that the bloodflow in the CAA recirculates when the diameter of the lumenincreases resulting in prolonged contact time between the CAAwall and the blood Studies have reported a significantly in-creased risk of thrombosis when RRT is gt10Paminus1 [12 34] -eRRTvalues forModels 3x and 5x in the present study were bothgt10Paminus1 suggesting a high risk of thrombosis when the di-ameter of a CAA exceeds three times that of the normal cor-onary artery Conversely the RRTforModel 2xwasmuch lowerthan 10Paminus1 suggesting that the risk of thrombosis may be lowwhen the diameter of the CAA is only double that of the normalartery Although there have been various studies of the rela-tionship between RRTand aneurysms [43] the current state ofknowledge remains insufficient for patient classification forexample there are no appropriate ranges of RRT values fordistinguishing the risk level of thrombosis which needs furtherstudy
In summary the comparison of our modeling resultswith the findings of previous studies suggested that the lowWSS high OSI and high RRT observed in the CAAs wouldsignificantly increase the risk of thrombosis However therisk varied considerably between the different diameters ofCAA -e WSS OSI and RRT values for Models 3x and 5xall suggested a high risk of thrombosis based on the previousstudy results-us for CAAs with diameters gt3 times that of
the normal coronary artery the risk of uncertainty withconservative treatment may be higher than the risk asso-ciated with surgery suggesting that the surgical operationshould be considered Conversely although the WSS OSIand RRT values for Model 2x were unfavorable comparedwith those of the model of the normal coronary arteryimplying an increased risk of thrombosis the magnitude ofthese differences was insufficient to support a prediction ofthe future development of the CAA For CAAs with a di-ameter up to two times that of the normal coronary arteryconservative drug treatment may be the better optionavoiding the risks associated with surgery
-e limitations of this study are as follows First this studyhas only one patientrsquos data and the conclusion may be ac-cidental We need to use more data for research Secondly animportant assumption used in the CFD calculation is the rigidwall where in fact elastic walls should be used In particularthe coronary artery will deform greatly as the heart contractswhich can be solved by two-way FSI in the future
5 Conclusion
-e evaluation of the relationship between hemodynamiceffects and different diameters of CAAs was performed inthis research through the CFD simulation method -erelationship between thrombosis risk and the size of theCAA diameter could be preliminarily evaluated from ahemodynamic perspective
We found that as the diameter of the CAA increased therisk of thrombosis increased substantially -e results sug-gested that when the diameter of a CAA is small (less thandouble that of the normal coronary artery) the risk ofthrombosis may be relatively low suggesting that medica-tion may be a sufficient approach for the patient avoidingthe uncertain risks associated with surgery If the diameter ofCAA is large (gt3 times that of the normal coronary artery)there may be a high risk of thrombosis and surgicaltreatment could be considered A similar approach could betaken in future studies to systematically assess the risk as-sociated with different shapes sizes and locations of an-eurysms Such approaches may form the basis for moresophisticated hemodynamic-based risk stratificationmethods supporting clinical decision-making in assessmentof CAA
Data Availability
-e data used to support the findings of this study areavailable from the corresponding author upon request
Conflicts of Interest
-e authors declare no conflicts of interest
Acknowledgments
-is research was supported by the National Natural ScienceFoundation of China (nos 11832003 and 11772016) andJSPS KAKENHI under Grant no JP18K18355 -is researchwas partially supported by the Creation of a Development
Complexity 9
Platform for ImplantableWearable Medical Devices by aNovel Physiological Data Integration System of the Programon Open Innovation Platform with Enterprises ResearchInstitute and Academia (OPERA) from the Japan Scienceand Technology Agency (JST) -is research was also sup-ported by Collaborative Research Project 2020 Institute ofFluid Science Tohoku University (J20R001) with the GrantNumber JP18K18355
References
[1] H Kato T Sugimura T Akagi et al ldquoLong-term conse-quences of kawasaki diseaserdquo Circulation vol 94 no 6pp 1379ndash1385 1996
[2] S A Sherif O O Tok O Taskoylu O Goktekin andI D Kilic ldquoCoronary artery aneurysms a review of theepidemiology pathophysiology diagnosis and treatmentrdquoFrontiers in Cardiovascular Medicine vol 4 2017
[3] E Beckmann S Rustum S Marquardt et al ldquoSurgicaltreatment of coronary artery aneurysmsrdquo Journal of CardiacSurgery vol 32 no 11 pp 674ndash679 2017
[4] M Syed M Lesch and A D Syed ldquoCoronary artery aneu-rysm a reviewrdquo Progress in Cardiovascular Diseases vol 40no 1 pp 77ndash84 1997
[5] G G Hartnell B M Parnell and R B Pridie ldquoCoronaryartery ectasia Its prevalence and clinical significance in 4993patientsrdquo British Heart Journal vol 54 no 4 1985
[6] A Satran B A Bart C R Henry et al ldquoIncreased prevalenceof coronary artery aneurysms among cocaine usersrdquo Circu-lation vol 111 no 19 pp 2424ndash2429 2005
[7] O Topaz M S Rutherford S M Bojack et al ldquoGiant an-eurysms of coronary arteries and saphenous vein graftsangiographic findings and histopathological correlatesrdquoCardiovascular Pathology vol 14 no 6 pp 298ndash302 2005
[8] A P Antoniadis Y S Chatzizisis and G D GiannoglouldquoPathogenetic mechanisms of coronary ectasiardquo InternationalJournal of Cardiology vol 130 no 3 pp 335ndash343 2008
[9] J B Gordon A M Kahn and J C Burns ldquoWhen childrenwith kawasaki disease grow uprdquo Journal of the AmericanCollege of Cardiology vol 54 no 21 pp 1911ndash1920 2009
[10] P Sriramarao L Languino and D Altieri ldquoFibrinogenmediates leukocyte-endothelium bridging in vivo at low shearforcesrdquo Blood vol 88 no 9 pp 3416ndash3423 1996
[11] A G Passerini D C Polacek C Shi et al ldquoCoexistingproinflammatory and antioxidative endothelial transcriptionprofiles in a disturbed flow region of the adult porcine aortardquoProceedings of the National Academy of Sciences vol 101no 89 pp 2482ndash2487
[12] U Morbiducci D Gallo R Ponzini et al ldquoQuantitativeanalysis of bulk flow in image-based hemodynamic models ofthe carotid bifurcation the influence of outflow conditions astest caserdquo Annals of Biomedical Engineering vol 38 no 12pp 3688ndash3705 2010
[13] T Ohkubo R Fukazawa E Ikegami and S Ogawa ldquoReducedshear stress and disturbed flow may lead to coronary aneu-rysm and thrombus formationsrdquo Pediatrics Internationalvol 49 no 1 pp 1ndash7 2007
[14] H Anzai T Watanabe X Han et al ldquoEndothelial cell dis-tributions and migration under conditions of flow shear stressaround a stent wirerdquo Technology and Health Care vol 28no 4 pp 345ndash354 2020
[15] M Zhang Y Li X Zhao et al ldquoHaemodynamic effects ofstent diameter and compaction ratio on flow-diversion
treatment of intracranial aneurysms a numerical study of asuccessful and an unsuccessful caserdquo Journal of Biomechanicsvol 58 pp 179ndash186 2017
[16] H Anzai B Chopard and M Ohta ldquoCombinational opti-mization of strut placement for intracranial stent using arealistic aneurysmrdquo Journal of Flow Control Measurement ampVisualization vol 2 no 2 pp 67ndash77 2014
[17] J P Ku M T Draney F R Arko et al ldquoIn vivo validation ofnumerical prediction of blood flow in arterial bypass graftsrdquoAnnals of Biomedical Engineering vol 30 no 6 pp 743ndash7522002
[18] A R Soler F Kabinejadian M A Slevin P J Bartolo andA Keshmiri ldquoOptimisation of a novel spiral-inducing bypassgraft using computational fluid dynamicsrdquo Scientific Reportsvol 7 no 1 p 1865 2017
[19] H Zhang L Li C Cheng and X Sun ldquoClinical value ofhomodynamic numerical simulation applied in the treatmentof cerebral aneurysmrdquo Experimental and Gerapeutic Medi-cine vol 4 no 6 pp 5401ndash5494 2017
[20] A S Les S C Shadden C A Figueroa et al ldquoQuantificationof hemodynamics in abdominal aortic aneurysms during restand exercise using magnetic resonance imaging and com-putational fluid dynamicsrdquo Annals of Biomedical Engineeringvol 38 no 4 pp 1288ndash1313 2010
[21] M Piccinelli A Veneziani D A Steinman A Remuzzi andL Antiga ldquoA framework for geometric analysis of vascularstructures application to cerebral aneurysmsrdquo IEEE Trans-actions on Medical Imaging vol 28 no 8 pp 1141ndash11552009
[22] H J Kim I E Vignon-Clementel J S CooganC A Figueroa K E Jansen and C A Taylor ldquoPatient-specific modeling of blood flow and pressure in humancoronary arteriesrdquo Annals of Biomedical Engineering vol 38no 10 pp 3195ndash3209 2010
[23] C A Taylor T A Fonte and J K Min ldquoComputational fluiddynamics applied to cardiac computed tomography fornoninvasive quantification of fractional flow reserverdquo Journalof the American College of Cardiology vol 61 no 22pp 2233ndash2241 2013
[24] I E V Clementel C A Figueroa K E Jansen andC A Taylor ldquoOutflow boundary conditions for 3D simula-tions of non-periodic blood flow and pressure fields in de-formable arteriesrdquo Computer Methods in Biomechanics andBiomedical Engineering vol 13 no 5 pp 625ndash640 2010
[25] N Stergiopulos J J Meister and N Westerhof ldquoDetermi-nants of stroke volume and systolic and diastolic aorticpressurerdquoGe American Journal of Physiology vol 270 no 6pp 2050ndash2059 1996
[26] M Zamir P Sinclair and T H Wonnacott ldquoRelation be-tween diameter and flow in major branches of the arch of theaortardquo Journal of Biomechanics vol 25 no 11 pp 1303ndash13101992
[27] K Johnson P Sharma and J Oshinski ldquoCoronary artery flowmeasurement using navigator echo gated phase contrastmagnetic resonance velocity mapping at 30 teslardquo Journal ofBiomechanics vol 41 no 3 pp 595ndash602 2008
[28] F P Salvuccia C A Perazzob S Sallesa J G Barrac andR L Armentano ldquoInfluence of inlet conditions in wall shearstress distributions of left coronary arteries in patient-specificsimulationsrdquo Mecanica Computacional vol XXIXpp 5953ndash5960 2010
[29] B C Lopez B Calvo and P Estefanıa Patient-SpecificComputational Modeling Springer Berlin Germany 2012thedition 2012
10 Complexity
[30] D N Ghista and F Kabinejadian ldquoCoronary artery bypassgrafting hemodynamics and anastomosis design a biomedicalengineering reviewrdquo BioMedical Engineering Online vol 12no 129 2013
[31] F P Glor F P Glor B Ariff et al ldquoImage-based carotid flowreconstruction a comparison between MRI and ultrasoundrdquoPhysiological Measurement vol 25 no 6 pp 1495ndash15092004
[32] S-W Lee L Antiga and D A Steinman ldquoCorrelationsamong indicators of disturbed flow at the normal carotidbifurcationrdquo Journal of Biomechanical Engineering vol 131no 6 Article ID 061013 2009
[33] H A Himburg ldquoSpatial comparison between wall shear stressmeasures and porcine arterial endothelial permeabilityrdquo AJPHeart and Circulatory Physiology vol 286 no 5 pp 1916ndash1922 2004
[34] T Suess J Anderson L Danielson et al ldquoExamination ofnear-wall hemodynamic parameters in the renal bridgingstent of various stent graft configurations for repairing vis-ceral branched aortic aneurysmsrdquo Journal of Vascular Sur-gery vol 64 no 3 pp 788ndash796 2016
[35] H Zhang X Yu F Ji and F Sun ldquoCoronary artery aneurysmformation after drug-coatedrdquo Medicine vol 97 no 45 2018
[36] N G Gutierrez M Mathew B W McCrindle et al ldquoHe-modynamic variables in aneurysms are associated withthrombotic risk in children with Kawasaki diseaserdquo Inter-national Journal of Cardiology vol 281 pp 15ndash21 2019
[37] C Karmonik G Chintalapani T Redel et al ldquoHemody-namics at the ostium of cerebral aneurysms with relation topost-treatment changes by a virtual flow diverter a compu-tational fluid dynamics studyrdquo in Proceedings of the AnnualInternational Conference of the IEEE Engineering in Medicineand Biology Society EMBS pp 1895ndash1898 Osaka Japan July2013
[38] J T Marcus H G Smeenk J P A KuijerR J Van Der Geest R M Heethaar and A C Van RossumldquoFlow profiles in the left anterior descending and the rightcoronary artery assessed byMR velocity quantification effectsof through-plane and in-plane motion of the heartrdquo Journal ofComputer Assisted Tomography vol 23 no 4 pp 567ndash5761999
[39] Y Shi P Lawford and R Hose ldquoReview of zero-D and 1-Dmodels of blood flow in the cardiovascular systemrdquo Bio-Medical Engineering Online vol 10 no 1 p 33 2011
[40] M Kroll J Hellums L McIntire A Schafer and J MoakeldquoPlatelets and shear stressrdquo Blood vol 88 no 5pp 1525ndash1541 1996
[41] J-J Chiu and S Chien ldquoEffects of disturbed flow on vascularendothelium pathophysiological basis and clinical perspec-tivesrdquo Physiological Reviews vol 91 no 1 pp 327ndash387 2011
[42] J Hwang M H Ing A Salazar et al ldquoPulsatile versus os-cillatory shear stress regulates NADPH oxidase subunit ex-pressionrdquo Circulation Research vol 93 no 12 pp 1225ndash12322003
[43] S-i Sugiyama K Niizuma T Nakayama et al ldquoRelativeresidence time prolongation in intracranial aneurysmsrdquoNeurosurgery vol 73 no 5 pp 767ndash776 2013
Complexity 11

exacerbates the risk of thrombosis WSS in the CAA lesion ofModel 2x was lower than that in the normal model howeverfurther development is still to be studied just taking WSS as areference -e risk for thrombosis in CAAs progresses withincreasing diameter so the risk associatedwithModel 2xwouldbe lower than that for Models 3x and 5x -e development ofCAAs needs further study Although studies have investigatedthe association between WSS and thrombosis the currentunderstanding is not yet comprehensive -erefore the pos-sibility of WSS and thrombosis in the corresponding in vitroexperiments should be the focus of continued research
-e OSIs for the CAAs increased rapidly with increasingdiameter of the lesion with the OSI in Model 5x around 30times greater than that of the normal coronary artery (whichwas close to zero throughout the CAA) Previous studieshave pointed out that when OSI is greater than 02 it willcause endothelial cell damage [31] -e high OSI area(OSIgt 02) ratio increased from 01 to 662 betweenModel 0 and Model 5x In vivo experimental studies ofporcine aortas have reported that disturbed flow (ie anincrease in OSI) promoted the expression of proin-flammatory cytokines in endothelial cells [11] In additionan in vitro study of bovine endothelial cells reported that theexpression of monocyte chemoattractant protein-1 could beinduced by applying a low-amplitude oscillating shear stressof 03 Pa at 1Hz (equivalent to an OSI of 05) and thishemodynamic environment enhanced the binding of en-dothelial cells to monocytes [42] -ese findings suggest thatthe elevated OSI values observed in the CAA models may beassociated with conditions that can trigger thrombosis
-e RRT values for the CAAs increased dramatically withincreasing diameters of the lesions with the RRT for Model5xgt100 times greater than that of the normal coronary artery-e high RRTarea ratio increased from 01 to 786 betweenModel 0 and Model 5x -ese findings indicate that the bloodflow in the CAA recirculates when the diameter of the lumenincreases resulting in prolonged contact time between the CAAwall and the blood Studies have reported a significantly in-creased risk of thrombosis when RRT is gt10Paminus1 [12 34] -eRRTvalues forModels 3x and 5x in the present study were bothgt10Paminus1 suggesting a high risk of thrombosis when the di-ameter of a CAA exceeds three times that of the normal cor-onary artery Conversely the RRTforModel 2xwasmuch lowerthan 10Paminus1 suggesting that the risk of thrombosis may be lowwhen the diameter of the CAA is only double that of the normalartery Although there have been various studies of the rela-tionship between RRTand aneurysms [43] the current state ofknowledge remains insufficient for patient classification forexample there are no appropriate ranges of RRT values fordistinguishing the risk level of thrombosis which needs furtherstudy
In summary the comparison of our modeling resultswith the findings of previous studies suggested that the lowWSS high OSI and high RRT observed in the CAAs wouldsignificantly increase the risk of thrombosis However therisk varied considerably between the different diameters ofCAA -e WSS OSI and RRT values for Models 3x and 5xall suggested a high risk of thrombosis based on the previousstudy results-us for CAAs with diameters gt3 times that of
the normal coronary artery the risk of uncertainty withconservative treatment may be higher than the risk asso-ciated with surgery suggesting that the surgical operationshould be considered Conversely although the WSS OSIand RRT values for Model 2x were unfavorable comparedwith those of the model of the normal coronary arteryimplying an increased risk of thrombosis the magnitude ofthese differences was insufficient to support a prediction ofthe future development of the CAA For CAAs with a di-ameter up to two times that of the normal coronary arteryconservative drug treatment may be the better optionavoiding the risks associated with surgery
-e limitations of this study are as follows First this studyhas only one patientrsquos data and the conclusion may be ac-cidental We need to use more data for research Secondly animportant assumption used in the CFD calculation is the rigidwall where in fact elastic walls should be used In particularthe coronary artery will deform greatly as the heart contractswhich can be solved by two-way FSI in the future
5 Conclusion
-e evaluation of the relationship between hemodynamiceffects and different diameters of CAAs was performed inthis research through the CFD simulation method -erelationship between thrombosis risk and the size of theCAA diameter could be preliminarily evaluated from ahemodynamic perspective
We found that as the diameter of the CAA increased therisk of thrombosis increased substantially -e results sug-gested that when the diameter of a CAA is small (less thandouble that of the normal coronary artery) the risk ofthrombosis may be relatively low suggesting that medica-tion may be a sufficient approach for the patient avoidingthe uncertain risks associated with surgery If the diameter ofCAA is large (gt3 times that of the normal coronary artery)there may be a high risk of thrombosis and surgicaltreatment could be considered A similar approach could betaken in future studies to systematically assess the risk as-sociated with different shapes sizes and locations of an-eurysms Such approaches may form the basis for moresophisticated hemodynamic-based risk stratificationmethods supporting clinical decision-making in assessmentof CAA
Data Availability
-e data used to support the findings of this study areavailable from the corresponding author upon request
Conflicts of Interest
-e authors declare no conflicts of interest
Acknowledgments
-is research was supported by the National Natural ScienceFoundation of China (nos 11832003 and 11772016) andJSPS KAKENHI under Grant no JP18K18355 -is researchwas partially supported by the Creation of a Development
Complexity 9
Platform for ImplantableWearable Medical Devices by aNovel Physiological Data Integration System of the Programon Open Innovation Platform with Enterprises ResearchInstitute and Academia (OPERA) from the Japan Scienceand Technology Agency (JST) -is research was also sup-ported by Collaborative Research Project 2020 Institute ofFluid Science Tohoku University (J20R001) with the GrantNumber JP18K18355
References
[1] H Kato T Sugimura T Akagi et al ldquoLong-term conse-quences of kawasaki diseaserdquo Circulation vol 94 no 6pp 1379ndash1385 1996
[2] S A Sherif O O Tok O Taskoylu O Goktekin andI D Kilic ldquoCoronary artery aneurysms a review of theepidemiology pathophysiology diagnosis and treatmentrdquoFrontiers in Cardiovascular Medicine vol 4 2017
[3] E Beckmann S Rustum S Marquardt et al ldquoSurgicaltreatment of coronary artery aneurysmsrdquo Journal of CardiacSurgery vol 32 no 11 pp 674ndash679 2017
[4] M Syed M Lesch and A D Syed ldquoCoronary artery aneu-rysm a reviewrdquo Progress in Cardiovascular Diseases vol 40no 1 pp 77ndash84 1997
[5] G G Hartnell B M Parnell and R B Pridie ldquoCoronaryartery ectasia Its prevalence and clinical significance in 4993patientsrdquo British Heart Journal vol 54 no 4 1985
[6] A Satran B A Bart C R Henry et al ldquoIncreased prevalenceof coronary artery aneurysms among cocaine usersrdquo Circu-lation vol 111 no 19 pp 2424ndash2429 2005
[7] O Topaz M S Rutherford S M Bojack et al ldquoGiant an-eurysms of coronary arteries and saphenous vein graftsangiographic findings and histopathological correlatesrdquoCardiovascular Pathology vol 14 no 6 pp 298ndash302 2005
[8] A P Antoniadis Y S Chatzizisis and G D GiannoglouldquoPathogenetic mechanisms of coronary ectasiardquo InternationalJournal of Cardiology vol 130 no 3 pp 335ndash343 2008
[9] J B Gordon A M Kahn and J C Burns ldquoWhen childrenwith kawasaki disease grow uprdquo Journal of the AmericanCollege of Cardiology vol 54 no 21 pp 1911ndash1920 2009
[10] P Sriramarao L Languino and D Altieri ldquoFibrinogenmediates leukocyte-endothelium bridging in vivo at low shearforcesrdquo Blood vol 88 no 9 pp 3416ndash3423 1996
[11] A G Passerini D C Polacek C Shi et al ldquoCoexistingproinflammatory and antioxidative endothelial transcriptionprofiles in a disturbed flow region of the adult porcine aortardquoProceedings of the National Academy of Sciences vol 101no 89 pp 2482ndash2487
[12] U Morbiducci D Gallo R Ponzini et al ldquoQuantitativeanalysis of bulk flow in image-based hemodynamic models ofthe carotid bifurcation the influence of outflow conditions astest caserdquo Annals of Biomedical Engineering vol 38 no 12pp 3688ndash3705 2010
[13] T Ohkubo R Fukazawa E Ikegami and S Ogawa ldquoReducedshear stress and disturbed flow may lead to coronary aneu-rysm and thrombus formationsrdquo Pediatrics Internationalvol 49 no 1 pp 1ndash7 2007
[14] H Anzai T Watanabe X Han et al ldquoEndothelial cell dis-tributions and migration under conditions of flow shear stressaround a stent wirerdquo Technology and Health Care vol 28no 4 pp 345ndash354 2020
[15] M Zhang Y Li X Zhao et al ldquoHaemodynamic effects ofstent diameter and compaction ratio on flow-diversion
treatment of intracranial aneurysms a numerical study of asuccessful and an unsuccessful caserdquo Journal of Biomechanicsvol 58 pp 179ndash186 2017
[16] H Anzai B Chopard and M Ohta ldquoCombinational opti-mization of strut placement for intracranial stent using arealistic aneurysmrdquo Journal of Flow Control Measurement ampVisualization vol 2 no 2 pp 67ndash77 2014
[17] J P Ku M T Draney F R Arko et al ldquoIn vivo validation ofnumerical prediction of blood flow in arterial bypass graftsrdquoAnnals of Biomedical Engineering vol 30 no 6 pp 743ndash7522002
[18] A R Soler F Kabinejadian M A Slevin P J Bartolo andA Keshmiri ldquoOptimisation of a novel spiral-inducing bypassgraft using computational fluid dynamicsrdquo Scientific Reportsvol 7 no 1 p 1865 2017
[19] H Zhang L Li C Cheng and X Sun ldquoClinical value ofhomodynamic numerical simulation applied in the treatmentof cerebral aneurysmrdquo Experimental and Gerapeutic Medi-cine vol 4 no 6 pp 5401ndash5494 2017
[20] A S Les S C Shadden C A Figueroa et al ldquoQuantificationof hemodynamics in abdominal aortic aneurysms during restand exercise using magnetic resonance imaging and com-putational fluid dynamicsrdquo Annals of Biomedical Engineeringvol 38 no 4 pp 1288ndash1313 2010
[21] M Piccinelli A Veneziani D A Steinman A Remuzzi andL Antiga ldquoA framework for geometric analysis of vascularstructures application to cerebral aneurysmsrdquo IEEE Trans-actions on Medical Imaging vol 28 no 8 pp 1141ndash11552009
[22] H J Kim I E Vignon-Clementel J S CooganC A Figueroa K E Jansen and C A Taylor ldquoPatient-specific modeling of blood flow and pressure in humancoronary arteriesrdquo Annals of Biomedical Engineering vol 38no 10 pp 3195ndash3209 2010
[23] C A Taylor T A Fonte and J K Min ldquoComputational fluiddynamics applied to cardiac computed tomography fornoninvasive quantification of fractional flow reserverdquo Journalof the American College of Cardiology vol 61 no 22pp 2233ndash2241 2013
[24] I E V Clementel C A Figueroa K E Jansen andC A Taylor ldquoOutflow boundary conditions for 3D simula-tions of non-periodic blood flow and pressure fields in de-formable arteriesrdquo Computer Methods in Biomechanics andBiomedical Engineering vol 13 no 5 pp 625ndash640 2010
[25] N Stergiopulos J J Meister and N Westerhof ldquoDetermi-nants of stroke volume and systolic and diastolic aorticpressurerdquoGe American Journal of Physiology vol 270 no 6pp 2050ndash2059 1996
[26] M Zamir P Sinclair and T H Wonnacott ldquoRelation be-tween diameter and flow in major branches of the arch of theaortardquo Journal of Biomechanics vol 25 no 11 pp 1303ndash13101992
[27] K Johnson P Sharma and J Oshinski ldquoCoronary artery flowmeasurement using navigator echo gated phase contrastmagnetic resonance velocity mapping at 30 teslardquo Journal ofBiomechanics vol 41 no 3 pp 595ndash602 2008
[28] F P Salvuccia C A Perazzob S Sallesa J G Barrac andR L Armentano ldquoInfluence of inlet conditions in wall shearstress distributions of left coronary arteries in patient-specificsimulationsrdquo Mecanica Computacional vol XXIXpp 5953ndash5960 2010
[29] B C Lopez B Calvo and P Estefanıa Patient-SpecificComputational Modeling Springer Berlin Germany 2012thedition 2012
10 Complexity
[30] D N Ghista and F Kabinejadian ldquoCoronary artery bypassgrafting hemodynamics and anastomosis design a biomedicalengineering reviewrdquo BioMedical Engineering Online vol 12no 129 2013
[31] F P Glor F P Glor B Ariff et al ldquoImage-based carotid flowreconstruction a comparison between MRI and ultrasoundrdquoPhysiological Measurement vol 25 no 6 pp 1495ndash15092004
[32] S-W Lee L Antiga and D A Steinman ldquoCorrelationsamong indicators of disturbed flow at the normal carotidbifurcationrdquo Journal of Biomechanical Engineering vol 131no 6 Article ID 061013 2009
[33] H A Himburg ldquoSpatial comparison between wall shear stressmeasures and porcine arterial endothelial permeabilityrdquo AJPHeart and Circulatory Physiology vol 286 no 5 pp 1916ndash1922 2004
[34] T Suess J Anderson L Danielson et al ldquoExamination ofnear-wall hemodynamic parameters in the renal bridgingstent of various stent graft configurations for repairing vis-ceral branched aortic aneurysmsrdquo Journal of Vascular Sur-gery vol 64 no 3 pp 788ndash796 2016
[35] H Zhang X Yu F Ji and F Sun ldquoCoronary artery aneurysmformation after drug-coatedrdquo Medicine vol 97 no 45 2018
[36] N G Gutierrez M Mathew B W McCrindle et al ldquoHe-modynamic variables in aneurysms are associated withthrombotic risk in children with Kawasaki diseaserdquo Inter-national Journal of Cardiology vol 281 pp 15ndash21 2019
[37] C Karmonik G Chintalapani T Redel et al ldquoHemody-namics at the ostium of cerebral aneurysms with relation topost-treatment changes by a virtual flow diverter a compu-tational fluid dynamics studyrdquo in Proceedings of the AnnualInternational Conference of the IEEE Engineering in Medicineand Biology Society EMBS pp 1895ndash1898 Osaka Japan July2013
[38] J T Marcus H G Smeenk J P A KuijerR J Van Der Geest R M Heethaar and A C Van RossumldquoFlow profiles in the left anterior descending and the rightcoronary artery assessed byMR velocity quantification effectsof through-plane and in-plane motion of the heartrdquo Journal ofComputer Assisted Tomography vol 23 no 4 pp 567ndash5761999
[39] Y Shi P Lawford and R Hose ldquoReview of zero-D and 1-Dmodels of blood flow in the cardiovascular systemrdquo Bio-Medical Engineering Online vol 10 no 1 p 33 2011
[40] M Kroll J Hellums L McIntire A Schafer and J MoakeldquoPlatelets and shear stressrdquo Blood vol 88 no 5pp 1525ndash1541 1996
[41] J-J Chiu and S Chien ldquoEffects of disturbed flow on vascularendothelium pathophysiological basis and clinical perspec-tivesrdquo Physiological Reviews vol 91 no 1 pp 327ndash387 2011
[42] J Hwang M H Ing A Salazar et al ldquoPulsatile versus os-cillatory shear stress regulates NADPH oxidase subunit ex-pressionrdquo Circulation Research vol 93 no 12 pp 1225ndash12322003
[43] S-i Sugiyama K Niizuma T Nakayama et al ldquoRelativeresidence time prolongation in intracranial aneurysmsrdquoNeurosurgery vol 73 no 5 pp 767ndash776 2013
Complexity 11

Platform for ImplantableWearable Medical Devices by aNovel Physiological Data Integration System of the Programon Open Innovation Platform with Enterprises ResearchInstitute and Academia (OPERA) from the Japan Scienceand Technology Agency (JST) -is research was also sup-ported by Collaborative Research Project 2020 Institute ofFluid Science Tohoku University (J20R001) with the GrantNumber JP18K18355
References
[1] H Kato T Sugimura T Akagi et al ldquoLong-term conse-quences of kawasaki diseaserdquo Circulation vol 94 no 6pp 1379ndash1385 1996
[2] S A Sherif O O Tok O Taskoylu O Goktekin andI D Kilic ldquoCoronary artery aneurysms a review of theepidemiology pathophysiology diagnosis and treatmentrdquoFrontiers in Cardiovascular Medicine vol 4 2017
[3] E Beckmann S Rustum S Marquardt et al ldquoSurgicaltreatment of coronary artery aneurysmsrdquo Journal of CardiacSurgery vol 32 no 11 pp 674ndash679 2017
[4] M Syed M Lesch and A D Syed ldquoCoronary artery aneu-rysm a reviewrdquo Progress in Cardiovascular Diseases vol 40no 1 pp 77ndash84 1997
[5] G G Hartnell B M Parnell and R B Pridie ldquoCoronaryartery ectasia Its prevalence and clinical significance in 4993patientsrdquo British Heart Journal vol 54 no 4 1985
[6] A Satran B A Bart C R Henry et al ldquoIncreased prevalenceof coronary artery aneurysms among cocaine usersrdquo Circu-lation vol 111 no 19 pp 2424ndash2429 2005
[7] O Topaz M S Rutherford S M Bojack et al ldquoGiant an-eurysms of coronary arteries and saphenous vein graftsangiographic findings and histopathological correlatesrdquoCardiovascular Pathology vol 14 no 6 pp 298ndash302 2005
[8] A P Antoniadis Y S Chatzizisis and G D GiannoglouldquoPathogenetic mechanisms of coronary ectasiardquo InternationalJournal of Cardiology vol 130 no 3 pp 335ndash343 2008
[9] J B Gordon A M Kahn and J C Burns ldquoWhen childrenwith kawasaki disease grow uprdquo Journal of the AmericanCollege of Cardiology vol 54 no 21 pp 1911ndash1920 2009
[10] P Sriramarao L Languino and D Altieri ldquoFibrinogenmediates leukocyte-endothelium bridging in vivo at low shearforcesrdquo Blood vol 88 no 9 pp 3416ndash3423 1996
[11] A G Passerini D C Polacek C Shi et al ldquoCoexistingproinflammatory and antioxidative endothelial transcriptionprofiles in a disturbed flow region of the adult porcine aortardquoProceedings of the National Academy of Sciences vol 101no 89 pp 2482ndash2487
[12] U Morbiducci D Gallo R Ponzini et al ldquoQuantitativeanalysis of bulk flow in image-based hemodynamic models ofthe carotid bifurcation the influence of outflow conditions astest caserdquo Annals of Biomedical Engineering vol 38 no 12pp 3688ndash3705 2010
[13] T Ohkubo R Fukazawa E Ikegami and S Ogawa ldquoReducedshear stress and disturbed flow may lead to coronary aneu-rysm and thrombus formationsrdquo Pediatrics Internationalvol 49 no 1 pp 1ndash7 2007
[14] H Anzai T Watanabe X Han et al ldquoEndothelial cell dis-tributions and migration under conditions of flow shear stressaround a stent wirerdquo Technology and Health Care vol 28no 4 pp 345ndash354 2020
[15] M Zhang Y Li X Zhao et al ldquoHaemodynamic effects ofstent diameter and compaction ratio on flow-diversion
treatment of intracranial aneurysms a numerical study of asuccessful and an unsuccessful caserdquo Journal of Biomechanicsvol 58 pp 179ndash186 2017
[16] H Anzai B Chopard and M Ohta ldquoCombinational opti-mization of strut placement for intracranial stent using arealistic aneurysmrdquo Journal of Flow Control Measurement ampVisualization vol 2 no 2 pp 67ndash77 2014
[17] J P Ku M T Draney F R Arko et al ldquoIn vivo validation ofnumerical prediction of blood flow in arterial bypass graftsrdquoAnnals of Biomedical Engineering vol 30 no 6 pp 743ndash7522002
[18] A R Soler F Kabinejadian M A Slevin P J Bartolo andA Keshmiri ldquoOptimisation of a novel spiral-inducing bypassgraft using computational fluid dynamicsrdquo Scientific Reportsvol 7 no 1 p 1865 2017
[19] H Zhang L Li C Cheng and X Sun ldquoClinical value ofhomodynamic numerical simulation applied in the treatmentof cerebral aneurysmrdquo Experimental and Gerapeutic Medi-cine vol 4 no 6 pp 5401ndash5494 2017
[20] A S Les S C Shadden C A Figueroa et al ldquoQuantificationof hemodynamics in abdominal aortic aneurysms during restand exercise using magnetic resonance imaging and com-putational fluid dynamicsrdquo Annals of Biomedical Engineeringvol 38 no 4 pp 1288ndash1313 2010
[21] M Piccinelli A Veneziani D A Steinman A Remuzzi andL Antiga ldquoA framework for geometric analysis of vascularstructures application to cerebral aneurysmsrdquo IEEE Trans-actions on Medical Imaging vol 28 no 8 pp 1141ndash11552009
[22] H J Kim I E Vignon-Clementel J S CooganC A Figueroa K E Jansen and C A Taylor ldquoPatient-specific modeling of blood flow and pressure in humancoronary arteriesrdquo Annals of Biomedical Engineering vol 38no 10 pp 3195ndash3209 2010
[23] C A Taylor T A Fonte and J K Min ldquoComputational fluiddynamics applied to cardiac computed tomography fornoninvasive quantification of fractional flow reserverdquo Journalof the American College of Cardiology vol 61 no 22pp 2233ndash2241 2013
[24] I E V Clementel C A Figueroa K E Jansen andC A Taylor ldquoOutflow boundary conditions for 3D simula-tions of non-periodic blood flow and pressure fields in de-formable arteriesrdquo Computer Methods in Biomechanics andBiomedical Engineering vol 13 no 5 pp 625ndash640 2010
[25] N Stergiopulos J J Meister and N Westerhof ldquoDetermi-nants of stroke volume and systolic and diastolic aorticpressurerdquoGe American Journal of Physiology vol 270 no 6pp 2050ndash2059 1996
[26] M Zamir P Sinclair and T H Wonnacott ldquoRelation be-tween diameter and flow in major branches of the arch of theaortardquo Journal of Biomechanics vol 25 no 11 pp 1303ndash13101992
[27] K Johnson P Sharma and J Oshinski ldquoCoronary artery flowmeasurement using navigator echo gated phase contrastmagnetic resonance velocity mapping at 30 teslardquo Journal ofBiomechanics vol 41 no 3 pp 595ndash602 2008
[28] F P Salvuccia C A Perazzob S Sallesa J G Barrac andR L Armentano ldquoInfluence of inlet conditions in wall shearstress distributions of left coronary arteries in patient-specificsimulationsrdquo Mecanica Computacional vol XXIXpp 5953ndash5960 2010
[29] B C Lopez B Calvo and P Estefanıa Patient-SpecificComputational Modeling Springer Berlin Germany 2012thedition 2012
10 Complexity
[30] D N Ghista and F Kabinejadian ldquoCoronary artery bypassgrafting hemodynamics and anastomosis design a biomedicalengineering reviewrdquo BioMedical Engineering Online vol 12no 129 2013
[31] F P Glor F P Glor B Ariff et al ldquoImage-based carotid flowreconstruction a comparison between MRI and ultrasoundrdquoPhysiological Measurement vol 25 no 6 pp 1495ndash15092004
[32] S-W Lee L Antiga and D A Steinman ldquoCorrelationsamong indicators of disturbed flow at the normal carotidbifurcationrdquo Journal of Biomechanical Engineering vol 131no 6 Article ID 061013 2009
[33] H A Himburg ldquoSpatial comparison between wall shear stressmeasures and porcine arterial endothelial permeabilityrdquo AJPHeart and Circulatory Physiology vol 286 no 5 pp 1916ndash1922 2004
[34] T Suess J Anderson L Danielson et al ldquoExamination ofnear-wall hemodynamic parameters in the renal bridgingstent of various stent graft configurations for repairing vis-ceral branched aortic aneurysmsrdquo Journal of Vascular Sur-gery vol 64 no 3 pp 788ndash796 2016
[35] H Zhang X Yu F Ji and F Sun ldquoCoronary artery aneurysmformation after drug-coatedrdquo Medicine vol 97 no 45 2018
[36] N G Gutierrez M Mathew B W McCrindle et al ldquoHe-modynamic variables in aneurysms are associated withthrombotic risk in children with Kawasaki diseaserdquo Inter-national Journal of Cardiology vol 281 pp 15ndash21 2019
[37] C Karmonik G Chintalapani T Redel et al ldquoHemody-namics at the ostium of cerebral aneurysms with relation topost-treatment changes by a virtual flow diverter a compu-tational fluid dynamics studyrdquo in Proceedings of the AnnualInternational Conference of the IEEE Engineering in Medicineand Biology Society EMBS pp 1895ndash1898 Osaka Japan July2013
[38] J T Marcus H G Smeenk J P A KuijerR J Van Der Geest R M Heethaar and A C Van RossumldquoFlow profiles in the left anterior descending and the rightcoronary artery assessed byMR velocity quantification effectsof through-plane and in-plane motion of the heartrdquo Journal ofComputer Assisted Tomography vol 23 no 4 pp 567ndash5761999
[39] Y Shi P Lawford and R Hose ldquoReview of zero-D and 1-Dmodels of blood flow in the cardiovascular systemrdquo Bio-Medical Engineering Online vol 10 no 1 p 33 2011
[40] M Kroll J Hellums L McIntire A Schafer and J MoakeldquoPlatelets and shear stressrdquo Blood vol 88 no 5pp 1525ndash1541 1996
[41] J-J Chiu and S Chien ldquoEffects of disturbed flow on vascularendothelium pathophysiological basis and clinical perspec-tivesrdquo Physiological Reviews vol 91 no 1 pp 327ndash387 2011
[42] J Hwang M H Ing A Salazar et al ldquoPulsatile versus os-cillatory shear stress regulates NADPH oxidase subunit ex-pressionrdquo Circulation Research vol 93 no 12 pp 1225ndash12322003
[43] S-i Sugiyama K Niizuma T Nakayama et al ldquoRelativeresidence time prolongation in intracranial aneurysmsrdquoNeurosurgery vol 73 no 5 pp 767ndash776 2013
Complexity 11

[30] D N Ghista and F Kabinejadian ldquoCoronary artery bypassgrafting hemodynamics and anastomosis design a biomedicalengineering reviewrdquo BioMedical Engineering Online vol 12no 129 2013
[31] F P Glor F P Glor B Ariff et al ldquoImage-based carotid flowreconstruction a comparison between MRI and ultrasoundrdquoPhysiological Measurement vol 25 no 6 pp 1495ndash15092004
[32] S-W Lee L Antiga and D A Steinman ldquoCorrelationsamong indicators of disturbed flow at the normal carotidbifurcationrdquo Journal of Biomechanical Engineering vol 131no 6 Article ID 061013 2009
[33] H A Himburg ldquoSpatial comparison between wall shear stressmeasures and porcine arterial endothelial permeabilityrdquo AJPHeart and Circulatory Physiology vol 286 no 5 pp 1916ndash1922 2004
[34] T Suess J Anderson L Danielson et al ldquoExamination ofnear-wall hemodynamic parameters in the renal bridgingstent of various stent graft configurations for repairing vis-ceral branched aortic aneurysmsrdquo Journal of Vascular Sur-gery vol 64 no 3 pp 788ndash796 2016
[35] H Zhang X Yu F Ji and F Sun ldquoCoronary artery aneurysmformation after drug-coatedrdquo Medicine vol 97 no 45 2018
[36] N G Gutierrez M Mathew B W McCrindle et al ldquoHe-modynamic variables in aneurysms are associated withthrombotic risk in children with Kawasaki diseaserdquo Inter-national Journal of Cardiology vol 281 pp 15ndash21 2019
[37] C Karmonik G Chintalapani T Redel et al ldquoHemody-namics at the ostium of cerebral aneurysms with relation topost-treatment changes by a virtual flow diverter a compu-tational fluid dynamics studyrdquo in Proceedings of the AnnualInternational Conference of the IEEE Engineering in Medicineand Biology Society EMBS pp 1895ndash1898 Osaka Japan July2013
[38] J T Marcus H G Smeenk J P A KuijerR J Van Der Geest R M Heethaar and A C Van RossumldquoFlow profiles in the left anterior descending and the rightcoronary artery assessed byMR velocity quantification effectsof through-plane and in-plane motion of the heartrdquo Journal ofComputer Assisted Tomography vol 23 no 4 pp 567ndash5761999
[39] Y Shi P Lawford and R Hose ldquoReview of zero-D and 1-Dmodels of blood flow in the cardiovascular systemrdquo Bio-Medical Engineering Online vol 10 no 1 p 33 2011
[40] M Kroll J Hellums L McIntire A Schafer and J MoakeldquoPlatelets and shear stressrdquo Blood vol 88 no 5pp 1525ndash1541 1996
[41] J-J Chiu and S Chien ldquoEffects of disturbed flow on vascularendothelium pathophysiological basis and clinical perspec-tivesrdquo Physiological Reviews vol 91 no 1 pp 327ndash387 2011
[42] J Hwang M H Ing A Salazar et al ldquoPulsatile versus os-cillatory shear stress regulates NADPH oxidase subunit ex-pressionrdquo Circulation Research vol 93 no 12 pp 1225ndash12322003
[43] S-i Sugiyama K Niizuma T Nakayama et al ldquoRelativeresidence time prolongation in intracranial aneurysmsrdquoNeurosurgery vol 73 no 5 pp 767ndash776 2013
Complexity 11