Hemodynamic Alterations in Hemorrhagic...
13
Hemodynamic Alterations in Hemorrhagic Fever By GEORGE ENTWISLE, CAPTAIN, M.C., AND EDWARD HALE, CAPTAIN, M.C. The cardiac output during the shock phase of hemorrhagic fever was very low. Increases in mean arterial pressure resulted from therapy with albumin or norepinephrine. With the former, this in- crease was associated with an increased cardiac output; with the latter, an increase in peripheral resistan(e. During the hypertensive phase, patients were found to have an incrcased( carildiac output if they) were also oliguric, and a relatively normal cardiac output if diuresis had begun. Some of the hypertensive patients presented the clinical syndrome of the "hypeidynamic state"; this occurred almost exclusively during the oliguric phase and was associated * ith high cardiac outl)ut and metabolic acidosis. T HE patient severely ill with hemorrhagic fever progresses through a prolonged course of rapidly changing phases of the disease, each with its own peculiar clinical state and physio- logic problems.' During this course there are violent fluctuations in a variety of physiologic adjustments.2 The initial febrile phase is fairly sudden in onset and lasts 4 to 5 days. Wide- spread capillary damage becomes evident late in the febrile phase and is manifested by leak- age of plasma from the blood vessels and by the development of some hemoconcentration. In 30 per cent of the cases, a phase of hypotension or shock lasting 24 to 36 hours follows the febrile phase and is accompanied by further hemo- concentration and continued plasma leakage.3 When hypotension is no longer a clinical prob- lem, anuria or oliguria and their complications become prominent and characterize the next phase. At this time maintenance of fluid and electrolyte balance may be a particular prob- lem. Late in the oliguric phase hypertension may be marked and complicated by pulmonary edema, and some patients show marked sensi- tivity to small alterations in fluid balance. Diuresis usually begins on the eleventh to thirteenth day of the disease, is marked for 2 or 3 days, and gradually the urine volume falls as the patient enters convalescence. Early in the diuretic phase electrolyte imbalance may again occur and at times is difficult to manage. Nor- mal renal function returns completely within 45 days in most cases.1 From the 48th Surgical Hospital (MIobile Army) APO 301. This work was done under the auspices of the Hemorrhagic Fever Commission, Walter Reed Army Medical Center. 414 The mortality of epidemics from 1951 to 1954 averaged about 5 per cent, and most deaths occurred in the shock or oligurie-hyper- tensive phases of the illness. Much work to clarify the physiologic problems of the different phases is available in the recent literature.4 Extensive physiologic studies were carried out on patients ill with hemorrhagic fever at the 48th Surgical Hospital, in the fall of 1953. As part of this over-all investigation, a hemody- namic study was performed, and is the subject of the present report. The previous year a pre- liminary study of similar nature was performed, and this was reported recently by Cugell,5 who found that the cardiac index was increased during the febrile and hypertenisiv-e phases, and low normal or decreased during the period of hemoconcentration. METHODS All observations were mad(e o hospitalized United Nations personnel. Forty-three patients were studied. Nine were control subjects, and consiste(l of hospitalized soldiers who had recovere(l from mild medical illnesses, such as infectious mononucleosis or upper respiratory infections. The other 34 pa- tients had hemorrhagic fever. All studies were (lone with the patients in the recumbent position and in the overnight fasting state, except for patients in shock who were studied at the onset of their shock phase. The measurements were begun within 30 minutes after the diagnosis of shock had been made and the wvard physician had decided to start therapy. This therapyI was postponed in patients being studied until initial data had been gathered. Since all patients in this phase had marked anorexia and some degree of vomiting, they were also for the most plart in the fasting state. Arterial pressure was measured direetly through an inlying Cournand needle, placed usually in the femoral artery. Miean arterial pressure was recorded Circulation, Volume XV, March 1957 by guest on July 6, 2018 http://circ.ahajournals.org/ Downloaded from
Transcript of Hemodynamic Alterations in Hemorrhagic...

Hemodynamic Alterations in Hemorrhagic FeverBy GEORGE ENTWISLE, CAPTAIN, M.C., AND EDWARD HALE, CAPTAIN, M.C.
The cardiac output during the shock phase of hemorrhagic fever was very low. Increases in meanarterial pressure resulted from therapy with albumin or norepinephrine. With the former, this in-crease was associated with an increased cardiac output; with the latter, an increase in peripheralresistan(e. During the hypertensive phase, patients were found to have an incrcased( carildiac outputif they) were also oliguric, and a relatively normal cardiac output if diuresis had begun. Some of thehypertensive patients presented the clinical syndrome of the "hypeidynamic state"; this occurredalmost exclusively during the oliguric phase and was associated * ith high cardiac outl)ut andmetabolic acidosis.
T HE patient severely ill with hemorrhagicfever progresses through a prolonged course
of rapidly changing phases of the disease, eachwith its own peculiar clinical state and physio-logic problems.' During this course there areviolent fluctuations in a variety of physiologicadjustments.2 The initial febrile phase is fairlysudden in onset and lasts 4 to 5 days. Wide-spread capillary damage becomes evident latein the febrile phase and is manifested by leak-age of plasma from the blood vessels and by thedevelopment of some hemoconcentration. In 30per cent of the cases, a phase of hypotension orshock lasting 24 to 36 hours follows the febrilephase and is accompanied by further hemo-concentration and continued plasma leakage.3When hypotension is no longer a clinical prob-lem, anuria or oliguria and their complicationsbecome prominent and characterize the nextphase. At this time maintenance of fluid andelectrolyte balance may be a particular prob-lem. Late in the oliguric phase hypertensionmay be marked and complicated by pulmonaryedema, and some patients show marked sensi-tivity to small alterations in fluid balance.Diuresis usually begins on the eleventh tothirteenth day of the disease, is marked for 2 or3 days, and gradually the urine volume falls asthe patient enters convalescence. Early in thediuretic phase electrolyte imbalance may againoccur and at times is difficult to manage. Nor-mal renal function returns completely within45 days in most cases.1
From the 48th Surgical Hospital (MIobile Army)APO 301.
This work was done under the auspices of theHemorrhagic Fever Commission, Walter Reed ArmyMedical Center.
414
The mortality of epidemics from 1951 to1954 averaged about 5 per cent, and mostdeaths occurred in the shock or oligurie-hyper-tensive phases of the illness. Much work toclarify the physiologic problems of the differentphases is available in the recent literature.4
Extensive physiologic studies were carriedout on patients ill with hemorrhagic fever at the48th Surgical Hospital, in the fall of 1953. Aspart of this over-all investigation, a hemody-namic study was performed, and is the subjectof the present report. The previous year a pre-liminary study of similar nature was performed,and this was reported recently by Cugell,5 whofound that the cardiac index was increasedduring the febrile and hypertenisiv-e phases, andlow normal or decreased during the period ofhemoconcentration.
METHODSAll observations were mad(e o hospitalized
United Nations personnel. Forty-three patients werestudied. Nine were control subjects, and consiste(l ofhospitalized soldiers who had recovere(l from mildmedical illnesses, such as infectious mononucleosisor upper respiratory infections. The other 34 pa-tients had hemorrhagic fever. All studies were (lonewith the patients in the recumbent position and inthe overnight fasting state, except for patients inshock who were studied at the onset of their shockphase. The measurements were begun within 30minutes after the diagnosis of shock had been madeand the wvard physician had decided to start therapy.This therapyIwas postponed in patients beingstudied until initial data had been gathered. Since allpatients in this phase had marked anorexia and somedegree of vomiting, they were also for the most plartin the fasting state.
Arterial pressure was measured direetly throughan inlying Cournand needle, placed usually in thefemoral artery. Miean arterial pressure was recorded
Circulation, Volume XV, March 1957
by guest on July 6, 2018http://circ.ahajournals.org/
Dow
nloaded from

ENTWISLE AND HALE
through an electromanometer connected with adirect-writing electrocardiograph. Venous pressurewas measured through a thin-walled 18-gage needleconnected to a saline manometer. The "zero" levelin all patients was taken to be 10 cm. above thedorsal spine with the patient in the supine position.Occasional use was made of an antecubital vein.
Cardiac output was measured by the indicator-dilution technic with Evans blue dye.6 Accuratelycalibrated syringes were used to inject a fixed amountof dye (varying from 2.4 to 2.7 ml. of T-1824, 26 mg.per ml.). The dye was injected through the indwell-ing 18-gage venous needle and serial samples of bloodwere taken at 2- to 4-second intervals from the intra-arterial needle. A minute amount of liquid heparinwas placed in each of the collecting test tubes.The serial samples were continued for a total of 1
to 3 minutes. Thereafter 6 blood samples were takenat 5-minute intervals to determine plasma volume.7Plasma concentration of T-1824 was measured witha Coleman junior spectrophotometer. Dye-tingedplasma standards were calibrated individually foreach study during the first part of this investigation.When it became obvious that the optical density ofthe plasma dye standard was remaining constant,the same standard optical density was used for allpatients subsequently studied, with periodic checksto assure that the base standard was maintained.The total blood volumes (TBV) were calculated
from the equation:
TBV = Plasma volume X 100.100 - (Hct X 0.96) X10
Red cell mass was derived from the difference be-tween TBV and plasma volume.
Sixty-one studies were done in 43 patients (1 studyeach in 9 normal and 52 studies in 34 patients withhemorrhagic fever). Serial determinations weredone in 13 patients. Duplicate cardiac outputdeterminations were done in 20 instances withcardiac indices varying from 1.49 to 5.54 L./M.2/min. The average per cent difference betweenduplicate determinations for the whole series was 8.1per cent. There was no detectable reduction in re-producibility of the method when applied to lowcardiac outputs.
Nine patients with shock were separated into 2groups of 5 patients each (1 patient, studied twice,appeared in both groups), and after an initial cardiacoutput and plasma volume determination, one groupreceived albumin as therapy and the other groupreceived norepinephrine. Two units of albumin (50Gm. of salt-poor human serum albumin in 200 ml.)were injected into the femoral vein. This proceduretook 12 to 25 minutes. At least half an hour wasallowed to pass after completion of the albumininfusion before the cardiac output determinationswere repeated. In the group receiving norepineph-rine, initial dosage was 10 to 15 y per minute inmost cases, infused through an intravenous poly-ethylene catheter. After 30 minutes when the bloodpressure had stabilized and while the infusion wasstill running, the cardiac output determination wasrepeated. Repeat plasma volume determinationsusing the second injection of Evans blue dye werenot performed. Alterations in the plasma volume
TABLE 1. Hemodynamic Studies in Hemorrhagic Fever
Stage of disease& no. pts.
Normal9
Febrile5
Shock13
Postfebrile3
Hypertensive oli-guric
13Hypertensive
diuretic7
Normotensivediuretic
5
2-6
4-7
7-9
6-14
11-16
12-26
deay Hematocrit
44.8t+3.3049.2+8.0156.7+4.2442.1+-1.8036.3+3.94
38.9+7.02
41.5+6.49
Cardiacindex
(L./M.2/min.)
3.6140.503.48+0.981.78+0.523.54+-0.474.69±1.02
3.55+1.23
2.71+0.97
Peripheral* Venous
resistance (pressure(CM. water)
19.1+4.3119.4+5.7033.9+11.4721.3+2.4021.7+4.84
29.4+8.41
29.6±11.04
12.0+0.7111.4+2.5010.842.7910.8±6.2114.3+4.66
10.4+12. 40
9.2+1.86
Pulserate
75+1299
+19110+2396
+3491
+19
82+13
66414
* Expressed in units (mean arterial pressure -venous pressure).cardiac index
t Mean values and standard deviation.
Meanarterialpressure(mm. Hg)
75.64t5.2271.6+8.0164.2+5.7982.7+7.52108.0+12.66
99.3+11.08
78.2+4.38
Plasmavolume(ml./Kg.)
41.3+7.5140.8+4.0328.9+6.0745.8
+11.7547.5+t8.40
44.0+7.60
43.6+9.71
Bloodvolume
(ml./Kg.)
70.1+9.6570.2+7.1060.6
410.5874.5
+18. 1771.5
+10.51
68.3+5.81
70.5+14.26
Red cellmass
(mL/Kg.)
28.8+3.2129.643.2331.8+5.3828.7+6.6923.942.91
24.2+3.11
26.9+6.74
-~~~~~~
415
by guest on July 6, 2018http://circ.ahajournals.org/
Dow
nloaded from
HEMODYNA'MIC ALTERATIONS IN HEMORRHAGIC FEVER
6
5
4
3
2
9 5 11 3 13 7 5
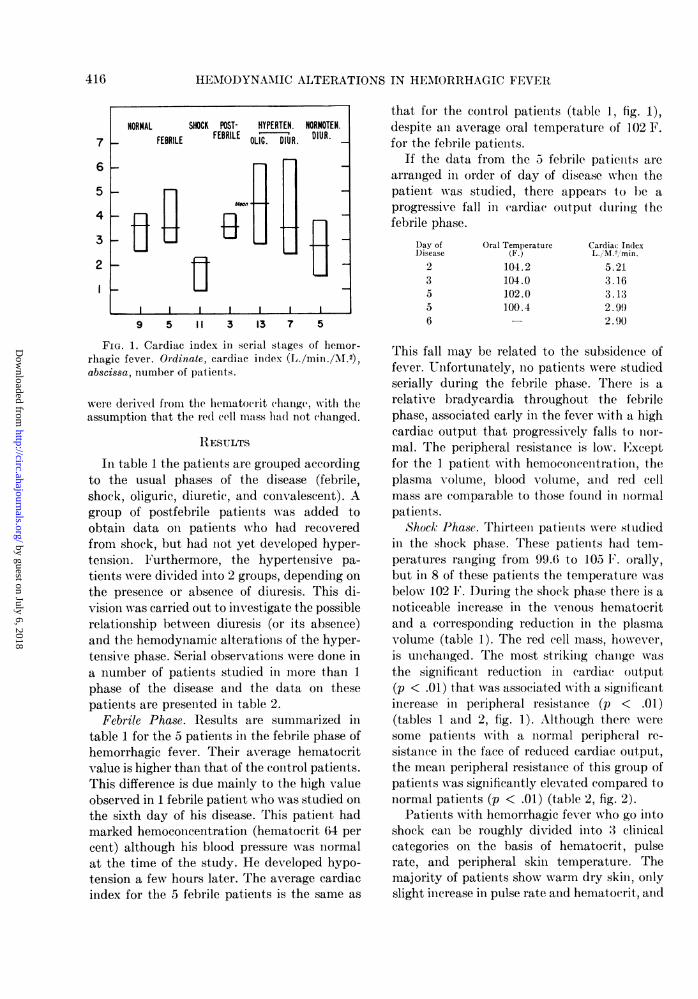
FIG. 1. Cardiac index in serial stages of hemor-rhagic fever. Ordinate, cardiac index (L./min./M1.2),abscissa, number of patients.
were derived from the hematoIrit (h1iange. with theassumption that the red cell mass had not (hanged.
RESULTS
In table 1 the patients are grouped accordingto the usual phases of the disease (febrile,shock, oliguric, diuretic, and convalescent). Agroup of postfebrile patients was added toobtain data on patients who had recoveredfrom shock, but had not yet developed hyper-tension. Furthermore, the hypertensive pa-
tients were divided into 2 groups, depending on
the presence or absence of diuresis. This di-vision was carried out to investigate the possiblerelationship between diuresis (or its absence)and the hemodynamic alterations of the hyper-tensive phase. Serial observations were done ina number of patients studied in more than 1phase of the disease and the data on thesepatients are presented in table 2.
Febrile Phase. Results are summarized intable 1 for the 5 patients in the febrile phase ofhemorrhagic fever. Their average hematocritvalue is higher than that of the control patients.This difference is due mainly to the high valueobserved in 1 febrile patient who was studied on
the sixth day of his disease. This patient hadmarked hemoconcentration (hematocrit 64 per
cent) although his blood pressure was normalat the time of the study. He developed hypo-tension a few hours later. The average cardiacindex for the 5 febrile patients is the same as
that for the control patients (table 1, fig. 1),despite an average oral temperature of 102 F.for the febrile patients.
If the data from the a febrile patients are
arranged in order of day of disease when thepatient wsas studied, there appears to be a
progressive fall in cardiac output duiring. thefebrile phase.
Day ofDisease
2
3
5
5
6
Oral Temperature(R.)104.2
104.0
102.0100.4
Cardiac In(lexL./1M.2 min.
5.21
3.16
3.13
2. 99
2.90
This fall may be related to the subsidence offever. Unfortunately, no patients were studiedserially during the febrile phase. There is a
relative bradyeardia throughout the febrilephase, associated early in the fever with a highcardiac output that progressively falls to nor-mal. The peripheral resistance is low. Exceptfor the 1 patient with hemoconcentrationi, theplasma volume, blood volume, and red cellmass are comparable to those found ill normalpatients.
Shock Phase. Thirteen patients were studiedin the shock phase. These patients had tem-peratures ranging from 99.6 to 105 F. orally,but in 8 of these patients the temperature was
below 102 F. During the shock phase there is a
noticeable increase in the venous hematocritand a corresponding reduction ill the plasmavolume (table 1). The red cell mass, however,is unchanged. The most striking change was
the significant reduction in cardiac output(p < .01) that was associated with a significantincrease in peripheral resistance (p < .01)(tables 1 and 2, fig. 1). Although there were
some patients with a normal peripheral re-
sistance ill the face of reduced cardiac output,the mean peripheral resistance of this group ofpatients was significantly elevated compared tonormal patients (p < .01) (table 2, fig. 2).
Patients with hemorrhagic fever who go intoshock can be roughly divided into 3 clinicalcategories on the basis of hematocrit, pulserate, and peripheral skin temperature. Themajority of patients show warmn dry skin, onlyslight increase in pulse rate and hematocrit, and
NORMAL SHOCK POST- HYPERTEN. NORMOTEN._ FEBRILE FEBRILE OUC.DIUR DIUR.
FBI L OI C D R.
, . .~~~~~~~,Wo. . .
416
7
by guest on July 6, 2018http://circ.ahajournals.org/
Dow
nloaded from

ENTWISLE AN!) HALE
TABLE 2.-Serial Observations in Patients with Hemnorrhagic Fever
HypertensiveShock Postfebrile Convalescent
Phase Oliguric Diuretic
C. 1.t P1. Vol.§ C. I. P1. Vol. C. I. P1. Vol. C. I. P1. Vol. C. I. P1. Vol.
Ulr 0.96 20.2 4.78 56.5 3.43 48.9 2.59 46.8Ham 2.17 33.9 6.37 48.3Kim 1.79* 30.5 3.44 34.7 4.12 54.6Til 1.40 27.6 3.40 37.9RoMr 1.14 17.8 3.55 36.6Tho 1.86 24.9 3.39 33.5And 2.37 31.0 2.04 37.1Ger 2.27 34.7 1.55 30.2Port 1.95 33.6 3.13 58.1 2.95 42.3Ellt 1.92 34.3 5.80 57.2Row 4.05 44.6 3.96 43.1
Gal 2.85 47.5 ~~~~~~~~~~~~~~~~~~~~~~~~~f3. 8o 50.0Gal 2. 85 47.5 ~~~~~~~~~~~~3.59 53.8Gel 5.25 48.9 6.10 53. 6
* After norepinephrine infusion. Preinfusion data inadequate. t Studies after 24 hours of treatmentfor shock (normotensive at time of study). t Cardiac index (L. /MI2/min.). § Plasma volume (nfl./Kg.).
they are usually given norepinephrine intra-venously and may be successfully carriedthrough the shock phase with this treatmentalone. Other patients present marked hemo-concentration, tachycardia, and cool, oftenmoist skin; they are treated initially with 1 to2 units of albumin. No other treatment may beneeded. The interpretation is that, in the lattergroup, reduction in blood (plasma) volumecontributes more to production of shock thanin the former group, where insufficientperipheral vasoconstriction predominates. Thethird group is comprised of patients whoinitially do not obviously fall into the 2 cate-gories just described. The third group is treatedinitially with norepinephrine, but albumin isfrequently also needed.4 Also included in thisthird group are the patients who initially re-
(uire either albumin or norepinephrine on thebasis of the clinical criteria, but who subse-(uently require the other agent for control ofblood pressure. The last patients described are
seriously ill patients with severe shock. Figure 2
depicts the course of such a patient.These arbitrary rules for deciding initial
treatment were followed to some extent in the
treatment of patients shown in table 3. In
order to obtain additional information about
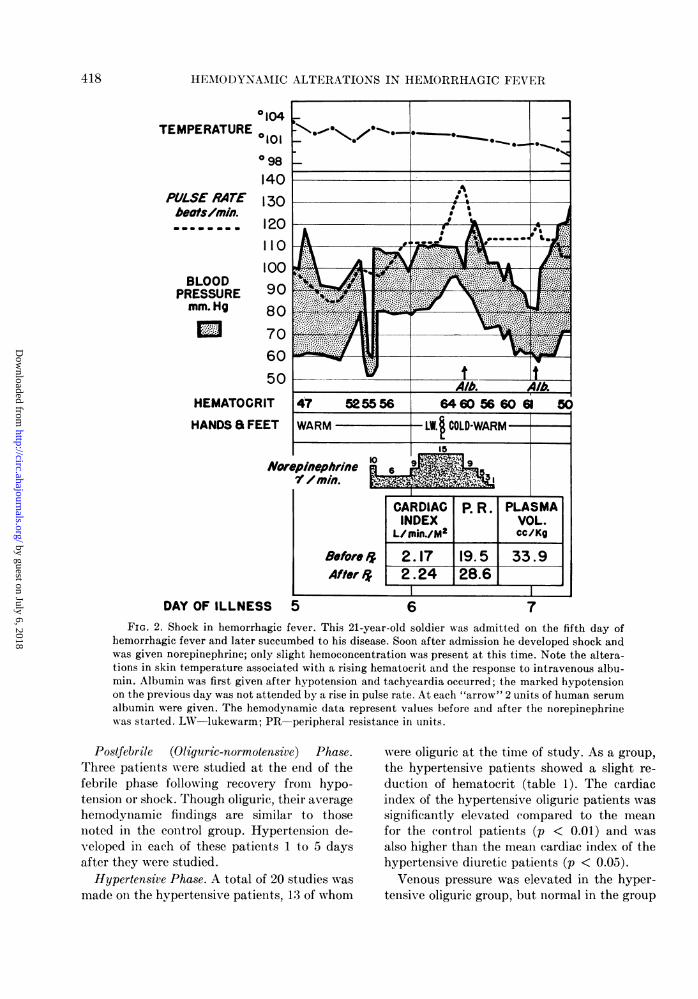
the effects of these agents, however, 1 patientwith a low hematocrit "Tho" was purposelygiven albumin initially, and 1 patient with ahigh hematocrit "Joh" was given norepi-nephrine initially. Patient "Ham," thoughpresenting with the same hematocrit level as"Joh," did, however, have warm dry skin andno increase ill pulse rate at the time of shockand was started oln norepinephrine. The com-plete course of this patient during shock isrepresented in figure 2. In addition, 1 patient,"TI,"was studied before and after treatmentwith both albumin and niorepinephrine, and thispatient appears twice ill table 3.Mean arterial pressures were essentially the
same for the 2 groups, but the average heima-tocrit was somewhat higher in the group receiv-ing albumin. The increase in mean arterialpressure that occurred ill the patients receivingalbumin was mainly due to all increase illcardiac output in each patient; the peripheralresistance actually fell in 4 of the 5 patients.There was slowing of the pulse and a fall inhematocrit. The increase in mean arterial pres-sure following therapy with norepinephrineappears to be wholly due to a significant inI-crease ill peripheral resistance (p 0.02). Thecardiac output and hematocrit level remainedunchanged.
41 7
by guest on July 6, 2018http://circ.ahajournals.org/
Dow
nloaded from
HEMODYNAMIC ALTERATIONS IN HEMORRHAGIC FEVER
0104TEMPERATURE 0101
098140
PULSE RArTE 130beoftsrnin., m m m m m 120
110100
BLOOD 9PRESSURE 90mm.Hg 80
70
60
50
HEMATOCRIT
HANDS a FEET
A/b A/b47 525556 64 6Y66 061 50
WARM LW. COLD-WARM15
NorepinephrineD/r min.
Before ,4After i&
DAY OF ILLNESS 5
6
CARDIAC P. R. PLASMAINDEX VOL.
L/Usin./M2 cc/Kg
2.17 19.5 33.92.24 28.6
6 7FIG. 2. Shock in hemorrhagic fever. This 21-year-old soldier was admitted on the fifth day of
hemorrhagic fever and later succumbed to his disease. Soon after admission he developed shock andwas given norepinephrine; only slight hemoconcentration was present at this time. Note the altera-tions in skin temperature associated with a rising hematocrit and the response to intravenous albu-min. Albumin was first given after hypotension and tachycardia occurred; the marked hypotensionon the previous day was not attended by a rise in pulse rate. At each "arrow" 2 units of human serumalbumin were given. The hemodynamic data represent values before and after the norepinephrinewas started. LW-lukewarm; PR peripheral resistance in units.
Postfebrile (Oliguric-normotensive) Phase.Three patients were studied at the end of thefebrile phase following recovery from hypo-tension or shock. Though oliguric, their averagehemodynamic findings are similar to thosenoted in the control group. Hypertension de-veloped in each of these patients 1 to 5 daysafter they were studied.
Hypertensive Phase. A total of 20 studies wasmade on the hypertensive patients, 13 of whom
were oliguric at the time of study. As a group,the hypertensive patients showed a slight re-duction of hematocrit (table 1). The cardiacindex of the hypertensive oliguric patients wassignificantly elevated compared to the meanfor the control patients (p < 0.01) and wasalso higher than the mean cardiac index of thehypertensive diuretic patients (p < 0.05).Venous pressure was elevated in the hyper-
tensiv e oliguric group, but normal in the group
a
418
by guest on July 6, 2018http://circ.ahajournals.org/
Dow
nloaded from
ENTWISLE AND HALE4
TABLE 3.-Shock in Hemorrhagic Fever. Immediate Response to Early Therapy
Patient Treatment
Ulv AlbuminRom Albumin
And AlbuminTho Albumin
Til Albumin
Til Norepinephrine
Joh Norepinephrine
Ger Norepinephrine
Ham NorepinephrineBas Norepinephrine
Mean Blood pressure Hematocrit
(mm. Hg)
Before*treat.
63627565587070665262
After* Beforetreat. treat.
72 6376 6390 5884 5370 5694 5199 5673 5175 5688 51
Aftertreat.
58575248515157535952
Cardiac index P(L./M.2/min.) Peripheral resistancet
Before After Before Aftertreat. treat. treat. treat.
0.96 1.37 56.1 38.51.14 1.98 46.0 34.62.37 2.54 28.4 31.81.86 2.32 35.5 27.81.40 2.24 34.4 27.12.24 2.06 27.1 41.51.40 1.68 45.0 54.82.27 1.96 26.5 34.12.17 2.24 19.5 28.61.96 1.99 27.8 40.7
* Data obtained just prior to and following therapy with either albumin or norepinephrine.t Expressed in units (mean arterial pressure - venous pressure).
cardiac index
whose diuresis had begun. The lack of a signifi-cant difference between the venous pressures ofthese 2 groups is probably due to the presence
in the latter group of the only hypertensivepatient who developed the "hyperdynamicsyndrome" during the diuretic phase and whosevenous pressure was 20 cm. of saline. Theperipheral resistance of patients in diuresis was
significantly elevated compared either to thenormal subjects (p < 0.01) or the hyperten-sive-oliguric patients (p < 0.02).
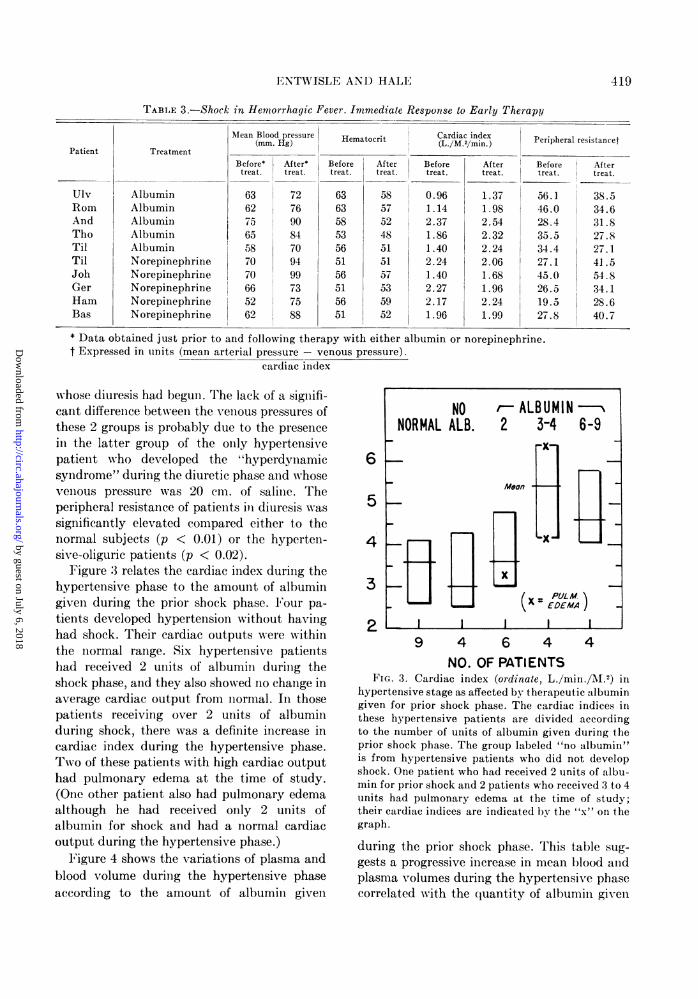
Figure 3 relates the cardiac index during thehypertensive phase to the amount of albumingiven during the prior shock phase. 1'our pa-
tients developed hypertension without havinghad shock. Their cardiac outputs were withinthe normal range. Six hypertensive patientshad received 2 units of albumin during theshock phase, and they also showed no change inaverage cardiac output from normal. In thosepatients receiving over 2 units of albuminduring shock, there was a definite increase incardiac index during the hypertensive phase.Two of these patients with high cardiac outputhad pulmonary edema at the time of study.(One other patient also had pulmonary edemaalthough he had received only 2 units ofalbumin for shock and had a normal cardiacoutput during the hypertensive phase.)
Figure 4 shows the variations of plasma andblood volume during the hypertensive phaseaccording to the amount of albumin given
6H
4
3(X = EM)
2
9 4 6 4 4NO. OF PATIENTS
FIG. 3. Cardiac index (ordinate, L./min./I.2) inhypertensive stage as affected by therapeutic albumingiven for prior shock phase. The cardiac indices inthese hypertensive patients are divided accordingto the number of units of albumin given during theprior shock phase. The group labeled "no albumin"is from hypertensive patients who did not developshock. One patient who had received 2 units of albu-min for prior shock and 2 patients who received 3 to 4units had pulmonary edema at the time of study;their cardiac indices are indicated b1 the "x" on thegraph.
during the prior shock phase. This table sug-
gests a progressive increase in mean blood andplasma volumes during the hypertensive phasecorrelated with the quantity of albumin given
NO r-ALBUMIN----NORMAL ALB. 2 3-4 6-9
rx
419
by guest on July 6, 2018http://circ.ahajournals.org/
Dow
nloaded from

HEMODYNAMIC ALTERATIONS IN HE.MORRHAGIC FE1V1ER
90
80
70
60
50
40
30
NO '-ALBUMINNORMAL ALB. 2 3-4 6-9
(X - PULM. )I-
IWIX XX
1A A
9 4 6 4 4NO. OF PATIENTS
FIG. 4. Blood (shaded bars) and plasma (emptybars) volumes in hypertensive stage as affected bytherapeutic albumin given for prior shock phase. Theplasma and blood volumes in these hypertensivepatients are divided according to the number of unitsof albumin given during the prior shock phase. Thegroup labeled "no albumin" is from hypertensivepatients who did not develop shock. One patient whohad received 2 units of albumin for prior shock and2 patients who received 3 to 4 units had pulmonaryedema at the time of study.
during the shock phase. All values for blood andplasma volumes in this figure are within therange found in normal patients, however.Phlebotomy (400 to 500 ml.) was performed
in 3 hypertensive patients on whom hemo-dynamic studies were done. The series wassmall because of reluctance to perform phle-botomy on patients with anemia (low hema-tocrit), and without specific indications forphlebotomy.2 Two phlebotomy patients were inpulmonary edema and had normal bloodvolumes and high cardiac indices. The venouspressure of each of these patients was elevated.They responded well to phlebotomy with fall invenous pressure, decrease in intensity of thesecond pulmonic sound, and disappearance ofgallop rhythm and abnormal breath sounds.The postphlebotomy cardiac index was re-duced 16 per cent in one, but only 7 per centin the other patient. Phlebotomy has beenrecommended for treatment of patients who
have convulsions during the hypertensivephase,2 and the effects of phlebotomy weredetermined in another hypertensive patient,not in pulmonary edema. His cardiac index wasnormal and blood volume low. No clinicalchange was noted follow-ing phlebotomy, andthe cardiac index was reduced only 7 per cent.These changes are similar to those previouslyreported.5
Normotensive Diuretic Phase. F,ive patients inthis stage were studied. Two patients could beconsidered convalescent though still havingpolyuria from impaired renal function; other-wise they felt subjectively well and their hemo-dynamic findings were normal. The 3 remainingpatients in this group were still on bed rest andwere weak and malnourished; 2 had low cardiacindices (2.04 and 1.55 L./M1.'/min.) and theirblood pressures were normal. Anemia, com-monly seen at this phase,' was present in some,but the average red cell mass was normal.Plasma and blood volumes were normal. In-creased peripheral resistance persisted into thisstage in some patients.
DISCUSSIONFebrile Phase. The febrile phase of hemor-
rhagic fever lasts from 4 to 6 days and late inthis phase there is usually a progressive in-crease in the venous hematocrit. This increaseis believed to be due to leakage of plasma fromthe intravascular compartment.2 Only 1 of thepatients studied during this phase showedhemoconcentration. The majority of patientswith marked hemoconcentration develop mani-festations of shock during defervescence.
Shock Phase. The most consistent and im-pressive finding in all patients with shock isreduced cardiac output. The cause of this re-duced output is probably multiple.2 3 Reducedcirculating blood volume owing to extravascu-lar plasma leakage and pooling in capillaries isa most likely major cause. Inadequate vaso-constriction in the face of hypotension and themyocardial damage often seen at postmortemexamination are considered to be the otherchief causes of shock in hemorrhagic fever. Al-though adrenal medullary hemorrhage andcortical damage can occur, adrenal insufficiency
420
by guest on July 6, 2018http://circ.ahajournals.org/
Dow
nloaded from

ENTWISLE AND HALE4
does not seem to be a contributing cause ofshock in most instances of this disease.2
Late in shock, whether it is untreated ortreated with albumin, norepinephrine, or both,almost all patients demonstrate cool, if notmoist skin, and cannot be divided clinically orhemodynamically into the 2 groups mentionedearlier. Two patients were studied 24 and 42hours after the onset of shock. Both patientshad been treated with albumin and were rela-tively normotensive (although still on shockblocks) at the time of study. In both cases theperipheral resistance was significantly elevated.M1any of these patients develop hypotension
or shock with warm dry extremities, and theclinical impression of "insufficient peripheralvasoconstriction" is supported by the findingsof normal or only slightly elevated calculatedperipheral resistance in patients with low bloodpressure and reduced cardiac output (table 3).The choice of initial treatment in shock on
the basis of clinical criteria of pulse rate, hema-tocrit, and skin temperature seems justified bythe hemodynamic data gathered in this study.In addition, for patients studied early in shock,those with the highest hematocrit levels hadthe lowest cardiac indices (r = -0.70), and thehighest calculated peripheral resistances (r =+0.73). The course of a patient in shock,"Ham," where indications for treatmentchanged from an initial choice of norepi-nephrine to a later choice of albumin is shown infigure 2.The charts of patients who developed shock
during the fall epidemic of hemorrhagic fever(1953) were reviewed to see if the immediateresponse to therapy could be correlated withpulse rate or hematocrit at the time of therapy.Approximately 35 charts were reviewed. Theimmediate response to albumin was equallygood in patients with tachycardia or relativebradyeardia. In general, the response to al-bumin therapy was much better in those pa-tients with the highest hematocrit values. Arise in mean arterial pressure was obtained fromsmall doses of norepinephrine in practically allcases, irrespective of pulse rate or hematocrit(although no cases were started on norepi-nephrine with a hematocrit of 60 or more).
Hemoconcentration in shock of other in-
fections has been noted, but mostly this is mildand does not reach the severe degree seen inpatients with hemorrhagic fever. The hemocon-centration and reduced blood volume togetherare probably the cause of the precarious clinicalstate of these patients. Shock in patients withsevere burns is similar, in that hemoconcentra-tion and low plasma volume occur. A few pa-tients with "burn shock" have had cardiacoutput studies.8 These patients show consist-ently low cardiac output and usually a veryhigh peripheral resistance.
Cardiac output determinations were re-cently reported for 5 patients in shock due tobacterial infection.9 These patients showednormal or slightly reduced cardiac outputs andlow peripheral resistance. The response to nor-epinephrine and albumin in these patients wasreported to be similar to the response seen inhemorrhagic fever. Norepinephrine caused arise in total peripheral resistance in all 4 pa-tients, and a slight reduction in cardiac outputoccurred in 3 patients. One patient was given asmall amount of albumin intravenously, andthis was followed by an increase in cardiacoutput.The effect of changes in viscosity on hemo-
dynamics in dogs with and without reduction inblood volume has been studied extensively bySeligman, Frank, and Fine.'0 With bloodvolume remaining constant, slight increases inhematocrit are associated with a fall in periph-eral resistance and with a rise in relativeviscosity; the mean arterial pressure andcardiac output remain normal. Further in-creases in hematocrit and apparent relativeviscosity are associated with a rise in peripheralresistance, a fall in cardiac output, with themean arterial pressure remaining unchanged.When hemoconcentration is produced in dogswith reduced blood volume, they become quitesensitive to further reduction in blood volume.Cardiac output reaches a critically low limit athigher mean pressures than would be the casewere the blood viscosity not elevated. Thislevel of blood pressure may produce a decep-tively favorable impression of the state of thecirculation. Indeed, such dogs may have ir-reversible shock at relatively high blood pres-sures, 80 mm. Hg and higher.10
421
by guest on July 6, 2018http://circ.ahajournals.org/
Dow
nloaded from

HEMODYNAMIC ALTERATIONS IN HEMORRHAGIC FEVER
Hypertensive Phase. Hypertension occurs inapproximately one fourth of patients withhemorrhagic fever and may be quite labile. Itusually lasts about 5 days and may be severeand associated with convulsions and pulmo-nary edema.3 Only 15 of the 20 patients studiedhad mean arterial pressures over 100 mm. Hg,although all were in the hypertensive phase bysphygnomanometric readings at the time. Ofthe 15 patients with mean arterial pressuresover 100 mm. Hg, 8 had elevated cardiacindices with normal peripheral resistance, 2 hadelevated peripheral resistance with normalcardiac indices, and 5 showed both elevatedcardiac indices and elevated peripheral re-sistance. When divided into 2 groups on thepresence or absence of diuresis, significantdifferences are noted with higher cardiac index,venous pressure, and pulse rate in the oliguricpatients, although there is no significant differ-
40
20HEMATOCRIT
URINE OUTPUTcc/24hn.
B.U.N.VENOUS PRESSURECARDIAC INDEXPERIPHERALRESISTANCE
DAY OF ILLNESS
ence in mean arterial pressures between the 2groups (p 0.2).
During the hypertensive phase, some of thepatients present the clinical syndrome of fullveins, bounding pulse, unusual finger and toepulses, exaggerated apical thrust, wide pulsepressure, and hypertension. This has beentermed "relative hypervolemia" by Earle.2Perhaps a more descriptive term is "hyper-dynamic state." Seven of the patients studiedduring the hypertensive phase presented thesefindings. Six were oliguric or anuric and 1 wasin the second day of the diuretic phase. Gener-ally, the cardiac index was high, peripheralresistance and hematocrit low. These findingsare correlated with high foot and toe peripheralblood flow determinations done in 4 of thesepatients. The course of a patient "Ham"demonstrating these findings is shown infigure 5.
47 54 645661 50 365 265 26.21300 390 190 0 0 0
22 24 180 173 182137 17 172.17 6.37
19.5 13.7
PERIPHERAL BLOOD FLOW Foor- 6.ecc/IOOgm/min. TOE- 7.O
5 6 7 8 9 10
t
FIG. 5. Hemorrhagic fever, fatal case. This figure represents the complete hospital course of thepatient whose shock phase is shown in figure 2. In addition to norepinephrine 4 units of albumin weregiven. On the eighth hospital day pulmonary edema developed with a high cardiac output and anelevated venous pressure. Following phlebotomy (500 ml.) the venous pressure fell to normal andsigns of pulmonary edema cleared. The cardiac index after phlebotomy was 5.3 L./M.2/min. He re-mained febrile throughout the hospital course and died on the tenth day, again in shock, unresponsiveto norepinephrine, transfusion, cortisone, and aqueous adrenal extract. Autopsy revealed broncho-pneumonia, minimal pulmonary congestion, and the usual pathologic changes noted at this stage ofthe disease.4
422
by guest on July 6, 2018http://circ.ahajournals.org/
Dow
nloaded from

ENTWISLE AND HALE
The blood volume of these hyperdynamicpatients was over 72 ml./Kg. with 1 exception.Trhe blood volume in the hypertensive nonhyper-dynamic patients was below 72 ml./Kg. with 2exceptions. From these findings there appearsto be a close correspondence between the clin-ical picture of the hyperdynaamic state andcalculated blood volume. However, as noted intable 1, the average and standard deviation ofblood volumes in both hypertenisive groups arethe same as in the normal group and becauseof these essential findings the condition wasspecifically labeled as "relative hypervxolemia"by Elarle.2
Accurate calculations of "central hyper-volemia" were not obtained. In the absence ofthese determinations, other indirect evidenceon the subject has been gathered. There is apositive relationship between the amount ofalbumin given in the treatment of shock andthe cardiac index of the hypertensive phase(fig. 3). This is also true of the blood andplasma volumes after albumin (fig. 4). The pos-sibility that this relationship is due to over-allseverity of the disease has, however, not beencompletely ruled out.Pulmonary edema occurred in 3 of 10 pa-
tients who had received 2 to 4 units of albumin,whereas it did not occur in 4 patients who didnot receive albumin nor in 4 patients who re-ceived 6 to 9 units of albumin. This observationsuggests that albumin therapy may lead topulmonary edema, but perhaps only in thepresence of other factors not illuminated bythis study.
Since the hyperdynamic state occurs duringthe stage of renal insufficiency of hemorrhagicfever, it is logical to consider what part, if any,the manifestations of renal insufficiency mayplay in producing this condition. As alreadymentioned, high cardiac outputs are usuallynoted in the patients before diuresis has begun.Although many of these hypertensive patientswere mildly anemic (low hemoglobin in thisgroup was 9.3 Gm.), anemia was not consideredto be a factor in the increases in cardiac out-put.13 Analysis of chemical changes in the bloodrevealed no consistent relation between thelevel of blood urea nitrogen and cardiac output,although high cardiac outputs were noted more
frequently when the blood urea nitrogen wasrising or at its peak. However, consistent differ-ences could not be demonstrated between theaverage blood urea nitrogen for the group ofpatients with high cardiac outputs and thegroup with low cardiac outputs. The potassiumlevels were normal in all these patients and thesodium and chloride levels were normal to lowin both groups, and changes in electrolytesbore no relation to changes in cardiac output.On the positive side, there was a relation be-
tween acidosis and cardiac output. Highcardiac outputs were most commonly seen withmild (carbon dioxide content of 15 to 20 mEq.per L.) to moderate acidosis (carbon dioxidecontent of 10 to 12 mEq. per L.) On the otherhand, normal cardiac outputs were seen in theabsence of, or with only mild, acidosis. Al-though the argument for relative hypervolemiais fairly cogent,2 it is suggested that oliguria andacidosis, particularly in combination, may playa significant role in the production of thehyperdynamic state. This conclusion is sup-ported by experimental evidence in dogs thatmetabolic acidosis was associate d with in-creased cardiac output."2Pulmonary edema is an uncommon but fre-
quently fatal complication of hemorrhagicfever. It has been suggested that internalshifts of fluid, perhaps the result of re-absorp-tion of the retroperitoneal edema fluid, mayoverload the vascular compartment.3 As agroup, patients who developed pulmonaryedema during the epidemic of 1952 did notshow enlargement of heart by x-ray, elevatedvenous pressure, or response to the usualtherapy for acute left ventricular failure.3 Thisgroup of patients was not divided according tothe presence or absence of hypertension at thetime of this complication.During the epidemic of 1953, it was noted
that patients who developed pulmonary edemawith normal or low blood pressure had a highmortality and uniformly showed hemorrhagicpulmonary edema at autopsy. The 2 patientswith this complication studied in this report,however, developed signs and symptoms ofpulmonary edema with hypertension and re-sponded to phlebotomy, with clearing of theirsymptoms and fall in elevated venous pressure.
423
by guest on July 6, 2018http://circ.ahajournals.org/
Dow
nloaded from

HEMIOD)YNAMIC ALTERATIONS IN HEM()RRHAGIC FEVER
X-ray films of the chest were not taken todetermine heart size. It appears then that somepatients with hemiorrhagic fever ill pulmonaryedema xvill respond with complete clearing ofthis complication by phlebotomy. Observationsof other patients with pulmonary edema during1953, who were not included in this hemo-dynamic study, suggest that some improvementto complete clearing of pulmonary edema occursin patients who are hypertensive while illpulmonary edema, but pulmonary edema inpatients with normal blood pressure or hypo-tension is almost uniformly fatal.
Normotensive Diuretic Phase. The low cardiacindices occasionally seen ill this phase (2 of 5studies) may well account for the occasionalpatient who has late shock2' and may con-tribute to the precarious fluid balance noted insome patients at this time. In the 2 cases ob-served, the peripheral resistance was high andthe blood pressure was normal. Lyons"4 has re-ported that the peripheral blood flow at thisstage (15 to 20 days) was low normal. Thecause of the low cardiac output is likely de-hydration, sodium depletion, or reduced venousreturn resulting from poor skeletal muscle andvenous tone. One patient was studied who hadbeen moderately ill with scrub typhus and inbed for 12 days. His hemodynamic findings werevery similar to those of the normotensivepatients in the diuretic phase of hemorrhagicfever. It seems probable that these same find-ings are present in the early recovery phase ofother infectious illnesses.
SUMMARY
A hemodynamic study was done oni 34 pa-tients during the various stages of hemorrhagicfever. In the initial febrile phase some increasein cardiac output was noted, especially in pa-tients with high fever. During the subsequentshock or hypotensive phase, striking reductionsill cardiac output were associated ill most pa-tients with warm, dry extremities and mildhemoconcentration. A minority of patients pre-sented low cardiac outputs associated with ahigh peripheral resistaiice and moderate tomarked hemoconcentration. The latter groupresponded well to treatment with intravenoushuman serum albumin and showed a rise in
cardiac output. The former group was treatedwith norepinephrine and the resulting rise inmeain arterial pressure was due to increasedperipheral resistance.Twenty studies were performed during the
hypertensive phase of hemorrhagic fever. I'a-tients were divided into 2 groups accordingto the presence or absence of diuresis. When ahypertensive patient was also oliguric, highcardiac output was frequently found that wasassociated with a normal or slightly elevatedperipheral resistance. Hypertensive patientswho had begun a diuresis had normal cardiacoutputs and significantly elevated peripheralresistance.Some of the patients during the hypertensive
phase presented the clinical syndrome of"relative-hypervolemia" described by Earle.As a group, these patients were oliguric, hadhigh cardiac outputs with normal to low periph-eral resistance, and had higher blood volumesthan the hypertensive patients not presentingthis syndrome. Metabolic acidosis was commonin this group.Pulmonary edema, an infrequent but usually
fatal complication of hemorrhagic fever, re-sponded to therapy if the patient was alsohypertensive at the time of pulmonary edema,but this complication was uniformly fatal innormotenisive or hypotensive patients.
SUMMARIO IIN IN-TFERLINGUA
Elsseva executate uii studio hemodynamnic in34 patientes durante le varie stadios de febrehemorrhagic. Durante le prime phase febril, uncerte grado de augmento del rendimento cardiacesseva notate, specialmente in patientes con altenivellos de febrilitate. Durante le subsequenitephase de choe (o phase hypotensive), frappantereductiones del rendimento cardiac essevaassociate in le majoritate del patientes concalide extremitates sic e leve grados de hemo-concentration. Un minoritate del patientespresentava basse rendimentos cardiac, associatecon alte resistentia peripheric e gradosmoderate usque a marcate de hemoconcen-tration. Iste secunde gruppo respondeva benal tractamento con injectiones intravenose dehuman albumina seral e manifestava un aug-mento del rendimento cardiac. Le prime del
424
by guest on July 6, 2018http://circ.ahajournals.org/
Dow
nloaded from

ENTWISLE AND HALE
duo gruppos esseva tractate Con nor-
epinephrina, e le resultante augmento delpression arterial medie esseva le effecto deelevationes del resistentia peripheric.
Vinti studios esseva executate durante lephase hypertensive del febre hemorrhagic. Lepatientes esseva dividite in 2 gruppos secundoque illes habeva o non habeva diurese. Quandoun patiente hypertensive esseva etiam oliguric,un constatation frequente esseva un alterendimento cardiac associate con normal olevemente augmentate resistentia peripheric.Patientes hypertensive qui habeva comenciatelor diurese monstrava normal rendimentoscardiac e elevationes significative del resistentiaperipheric.
Durante le phase hypertensive, certepatientes presentava le syndrome clinic de"hypervolemia relative" describite per Earle.Iste gruppo de patientes esseva oliguric, habevaalte rendimentos cardiac con normal o basseresistentia peripheric, e monstrava plus altevolumines de sanguine que le patientes hyper-tensive qui non presentava iste syndrome.Acidosis metabolic esseva commun in istegruppo.
Edema pulmonar, un infrequente sed general-mente letal complication de febre hemorrhagic,respondeva al therapia si le patiente esseva
etiam hypertensive al tempore del declarationdel edema pulmonar, sed iste complicationesseva uniformemente mortal in patientesnormo- o hypotensive.
REFERENCES1 S EEEDY, J. A., FROEB, II. F., BATSON, H. A.,
CONLEY, C. C., M\URPHY, .J. P., HUNTER, R. B.,CUGELL, D. WV., GILES, R. B., BERSHADSKY, S.C., VESTER, J. WX., AND YOE, R. H.: The clinical
course of epidemic hemiorrhagic fever. Am. .J.Med. 16: 619, 1954.
2 EARLE, D. P.: Analysis of sequential physiologicderangements in epidemic hemorrhagic fever.Am. J. eIed. 16: 690, 1954.
3 GILES, R. B., SHEEDY, .J. A., ELKMAN, C. N., FROEB,H. F., CONLEY, C. C., STOCKARD, J. L., CUGELL,I). W., VESTER, J. WX., KIYASU, R. K.,EN-TWISLE, G., AND YOE, R. H.: The sequelae ofepidemic hemorrhagic fever. Am. J. i\Ied. 16:629, 1954.
4EARLE, D. P., 1D.: Symposium on epidemichemorrhagic fever. Am. J. _Med. 16: 617, 1954.
5CUGELL, D. W.: Cardiac output in epidemichemorrhagic fever. Am. J. MXed. 16: 668, 1954.
6 HAMILTON, WX. F., MOORE, J. W., KINSMAN, J. N.,AND SPURLING, R. G.: Studies on the circulation.Am. .J. Physiol. 99: 534, 1931-32.
7GILEuS, R. B., AND LANGDON, E. A.: Blood volumein epidemic hemorrhagic fever. Am. J. Med. 16:654, 1954.
8 COURNAND, A., RILEY, R. L., BRADLEY, S. E.,BREED, E. S., NOBLE, R. P., LAUSON, H. D.,GREGERSEN, M. I., AND RICHARDS, D. AV.:Studies of the circulation in clinical shock.Surgery 13: 964, 1943.
9 GILBERT, R. P., HONIG, K. P., AkDELSON, B. H.,GRIFFIN, J. A., AND BECKER, R.: The hemo-dynamics of shock due to infection. .J. Lab. &Clin. M\Ied. 44: 801, 1954.
10 SELIGMAN, A. M., FRANK, H. A., AND FINE, J.:Traumatic shock. XII. Hemodvnamic effects ofalterations of blood viscosity in normal dogs and(logs in shock. J. Clin. Invest. 25: 1, 1946.
"LYONS, R.: Personal communication.12 POPPELL, ,J. WX., ROBERTS, K. E., VANAMEE, P.,
AND RANDALL, H. T.: Cardiovascular alterationsin metabolic acidosis. Clinical Research Pro-ceedings 3: 104, 1955.
'3 BRANNON, E. S., IERRILL, .A. J., WARREN, .J. V.,AND STEAD, E. A. JR.: Cardiac output in anemia..J. Clin. Invest. 24: 332, 1945.
i4 LYONS, R. H., SYNER, J., AND MOE, G.: Hemo-lynamics of epidemic hemorrhagic fever. TI.Am. Clin. & Climatol. A. 66: 48, 1954.
425
by guest on July 6, 2018http://circ.ahajournals.org/
Dow
nloaded from
GEORGE ENTWISLE, CAPTAIN and EDWARD HALE, CAPTAINHemodynamic Alterations in Hemorrhagic Fever
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1957 American Heart Association, Inc. All rights reserved.
75231is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TXCirculation
doi: 10.1161/01.CIR.15.3.4141957;15:414-425Circulation.
http://circ.ahajournals.org/content/15/3/414located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer
of the Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle columnClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on July 6, 2018http://circ.ahajournals.org/
Dow
nloaded from