Heart Failure and Renal Failure - HFAI. Acute Heart Failure Dr... · Gerasimos Filippatos, MD,...
38
Gerasimos Filippatos, MD, FESC, FHFA President HFA Heart Failure and Renal Failure
Transcript of Heart Failure and Renal Failure - HFAI. Acute Heart Failure Dr... · Gerasimos Filippatos, MD,...
Gerasimos Filippatos, MD, FESC, FHFA
President HFA
Heart Failure and Renal Failure
• Definition
• Epidemiology
• Pathophysiology
• Management (?)
Recommendations for NHLBI in cardio-
renal interactions related to heart failure
• “The result of interactions between the kidneys and
other circulatory compartments that increase
circulating volume and symptoms of heart failure
and disease progression are exacerbated. At its
extreme, cardio-renal dysregulation leads to what
is termed ‘cardio-renal syndrome’ in which
therapy to relieve congestive symptoms of heart
failure is limited by further decline in renal function”
NHLBI Working Group. Cardio-renal connections in heart failure and cardiovascular disease: executive summary .
Available at: http://www.nhlbi.nih.gov/meetings/workshops/cardiorenal-hf-hd.htm.
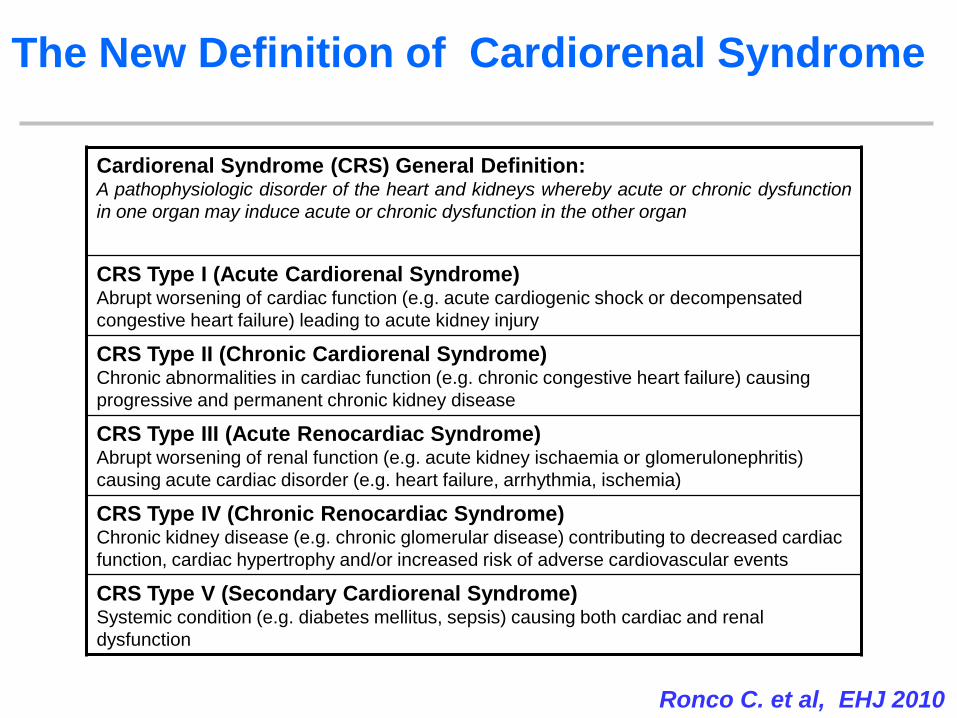
The New Definition of Cardiorenal Syndrome
Cardiorenal Syndrome (CRS) General Definition: A pathophysiologic disorder of the heart and kidneys whereby acute or chronic dysfunction
in one organ may induce acute or chronic dysfunction in the other organ
CRS Type I (Acute Cardiorenal Syndrome) Abrupt worsening of cardiac function (e.g. acute cardiogenic shock or decompensated
congestive heart failure) leading to acute kidney injury
CRS Type II (Chronic Cardiorenal Syndrome) Chronic abnormalities in cardiac function (e.g. chronic congestive heart failure) causing
progressive and permanent chronic kidney disease
CRS Type III (Acute Renocardiac Syndrome) Abrupt worsening of renal function (e.g. acute kidney ischaemia or glomerulonephritis)
causing acute cardiac disorder (e.g. heart failure, arrhythmia, ischemia)
CRS Type IV (Chronic Renocardiac Syndrome) Chronic kidney disease (e.g. chronic glomerular disease) contributing to decreased cardiac
function, cardiac hypertrophy and/or increased risk of adverse cardiovascular events
CRS Type V (Secondary Cardiorenal Syndrome) Systemic condition (e.g. diabetes mellitus, sepsis) causing both cardiac and renal
dysfunction
Ronco C. et al, EHJ 2010
The Definition
What defines the above factors?
Any degree of
cardiac
dysfunction
Any degree of
anemia
Any degree of
kidney failure
Iron Deficiency
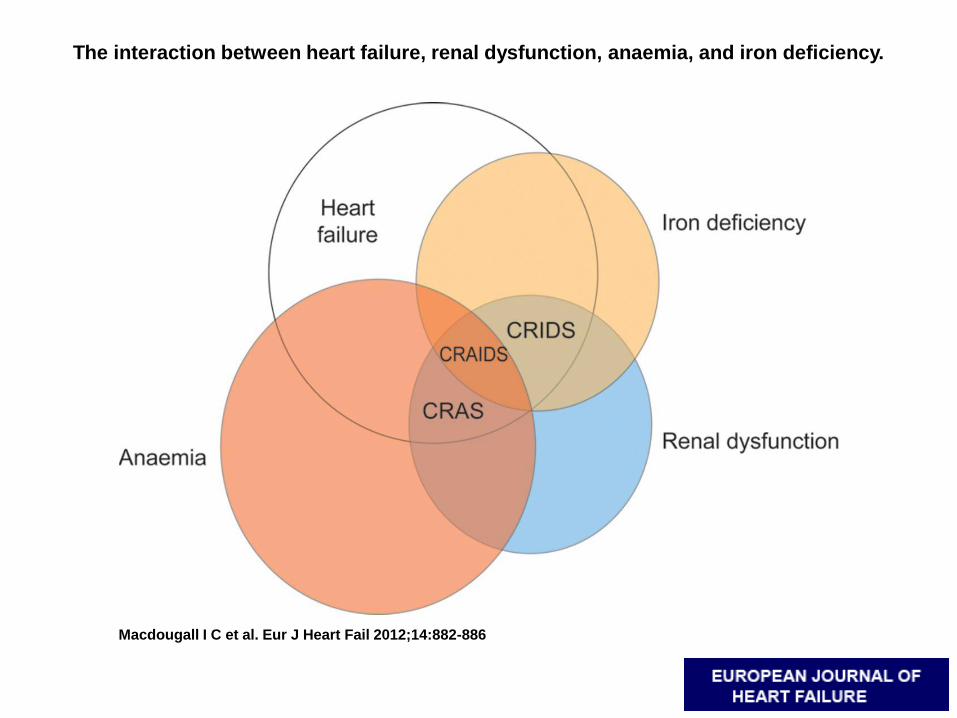
The interaction between heart failure, renal dysfunction, anaemia, and iron deficiency.
Macdougall I C et al. Eur J Heart Fail 2012;14:882-886
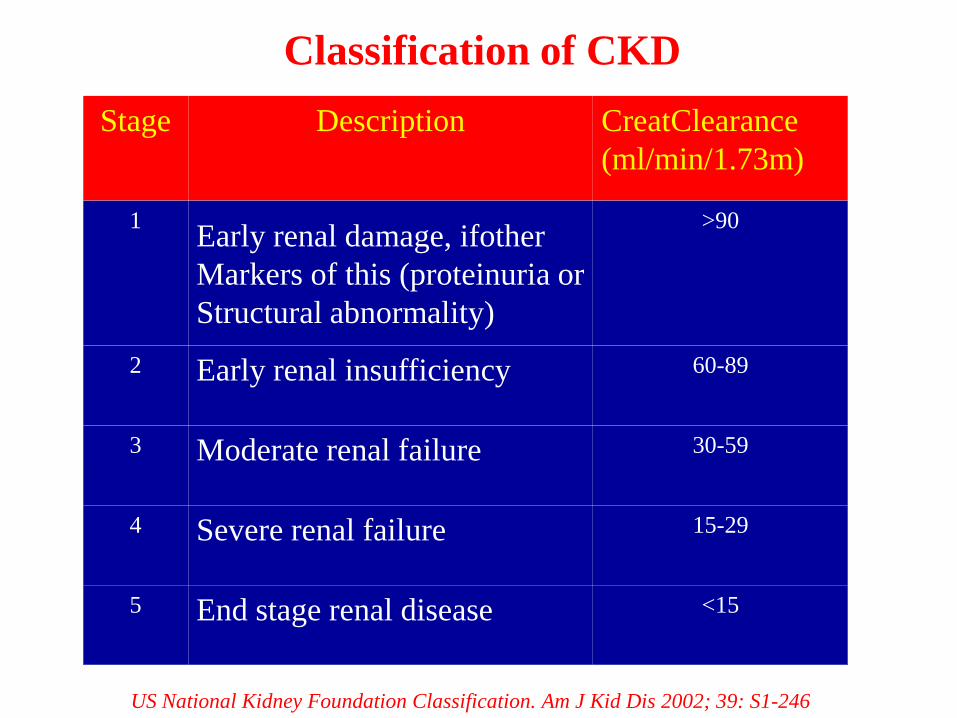
Stage Description CreatClearance
(ml/min/1.73m)
1 Early renal damage, ifother
Markers of this (proteinuria or
Structural abnormality)
>90
2 Early renal insufficiency 60-89
3 Moderate renal failure 30-59
4 Severe renal failure 15-29
5 End stage renal disease <15
Classification of CKD
US National Kidney Foundation Classification. Am J Kid Dis 2002; 39: S1-246
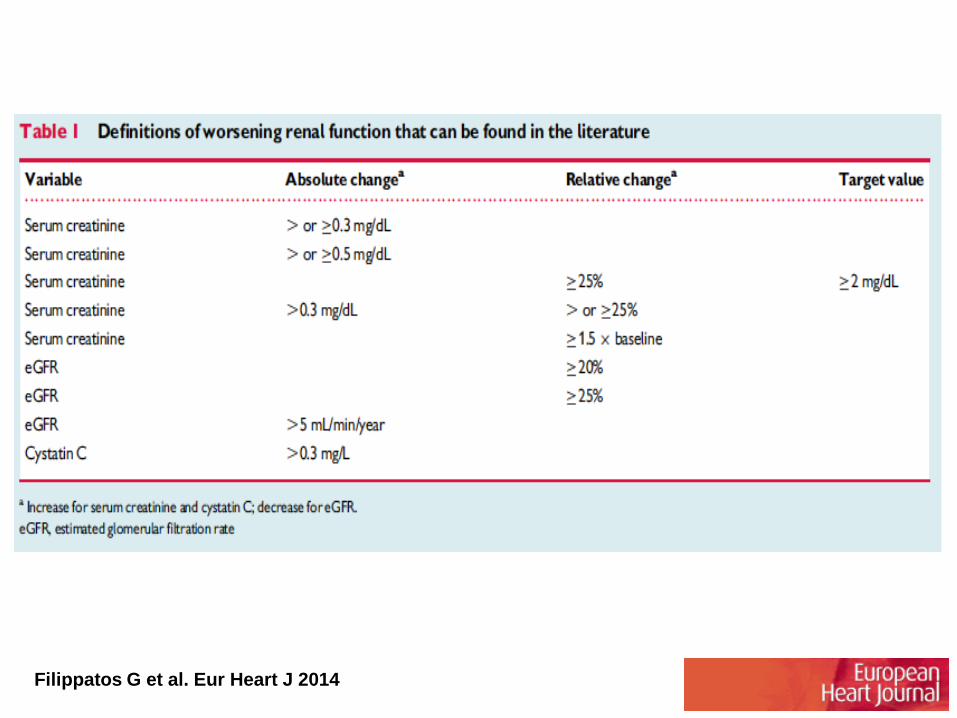
Filippatos G et al. Eur Heart J 2014
• Definition
• Epidemiology
• Pathophysiology
• Management (?)
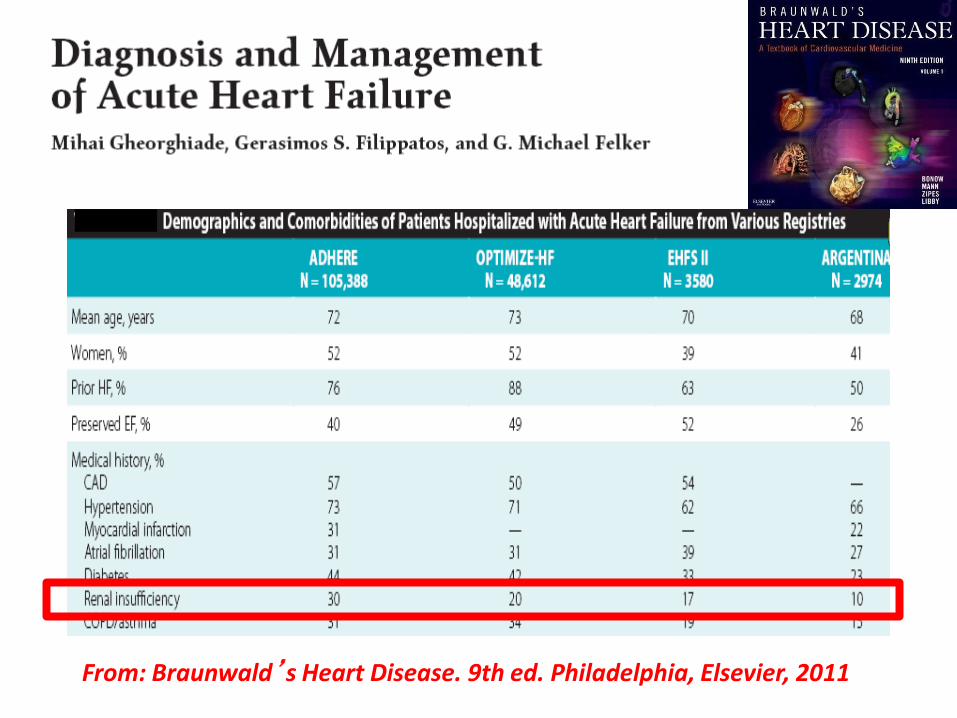
From: Braunwald’s Heart Disease. 9th ed. Philadelphia, Elsevier, 2011
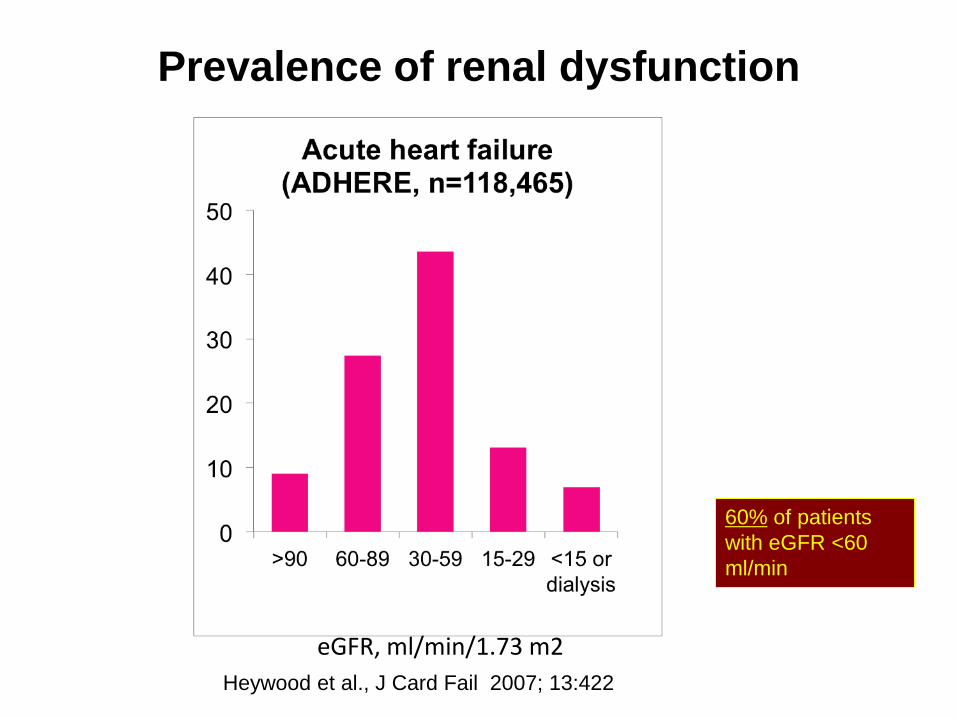
eGFR, ml/min/1.73 m2
60% of patients
with eGFR <60
ml/min
Prevalence of renal dysfunction
Heywood et al., J Card Fail 2007; 13:422
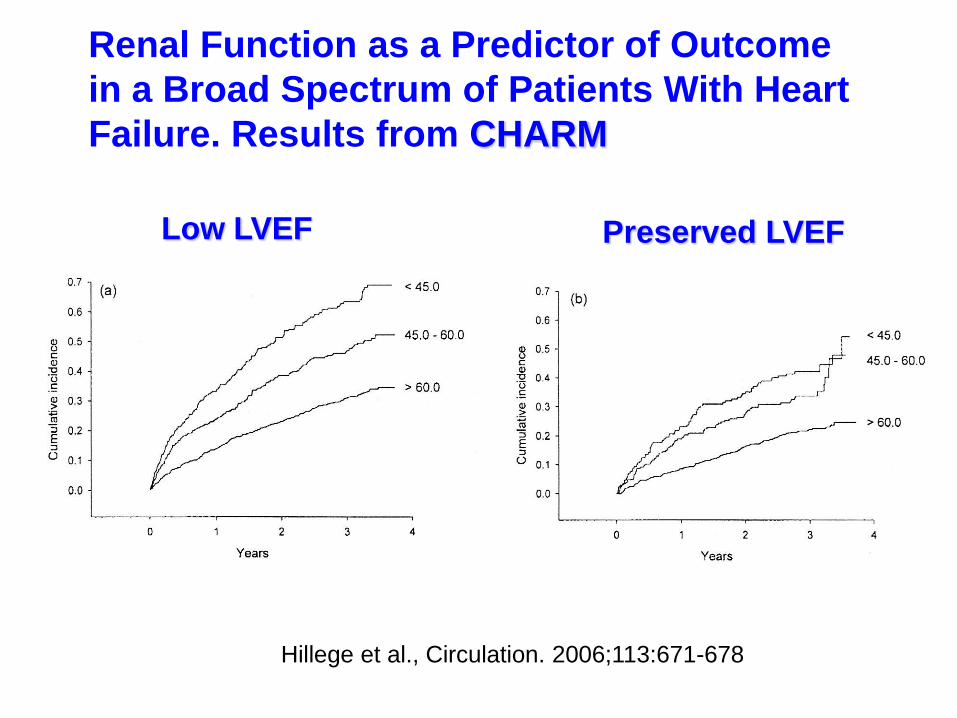
Renal Function as a Predictor of Outcome
in a Broad Spectrum of Patients With Heart
Failure. Results from CHARM
Low LVEF Preserved LVEF
Hillege et al., Circulation. 2006;113:671-678

BUN and Death or HF Rehospitalization
Log-Rank Test
P-Value = 0.0005
PR
OP
OR
TIO
N O
F R
EM
AIN
ING
IN
ST
UD
Y
0.5
0.6
0.7
0.8
0.9
1.0
DAYS IN STUDY
0 10 20 30 40 50 60 70
BUN > 40 mg/dL
BUN < 18 mg/dL
BUN 19-26 mg/dL
BUN 27-39 mg/dL
Filippatos G et al .J Cardiac Failure 2007
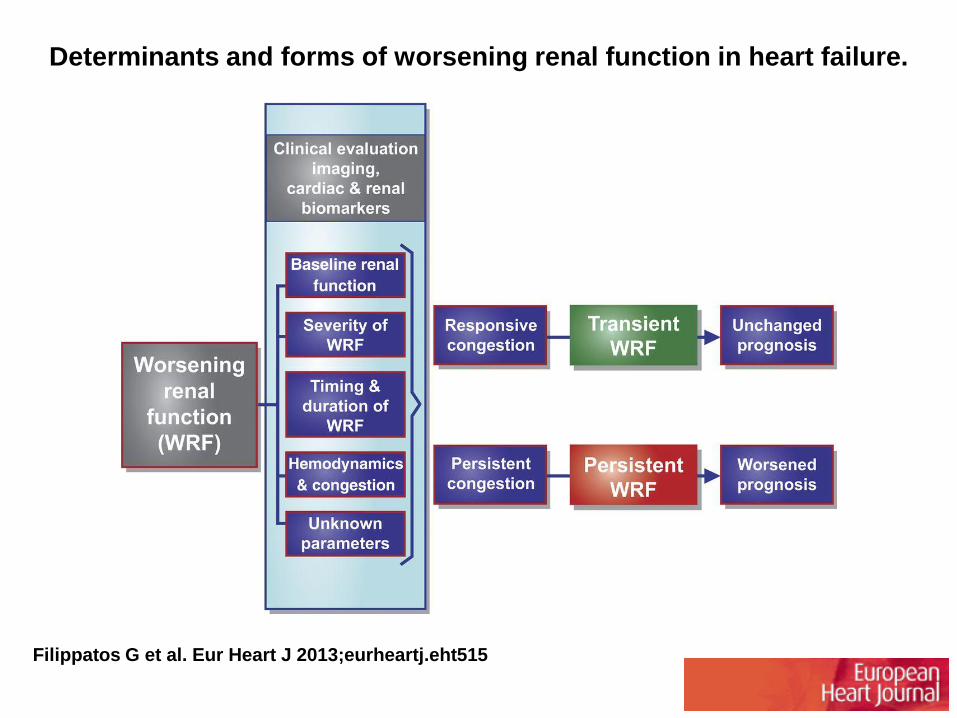
Determinants and forms of worsening renal function in heart failure.
Filippatos G et al. Eur Heart J 2013;eurheartj.eht515
• Definition
• Epidemiology
• Pathophysiology
• Management (?)
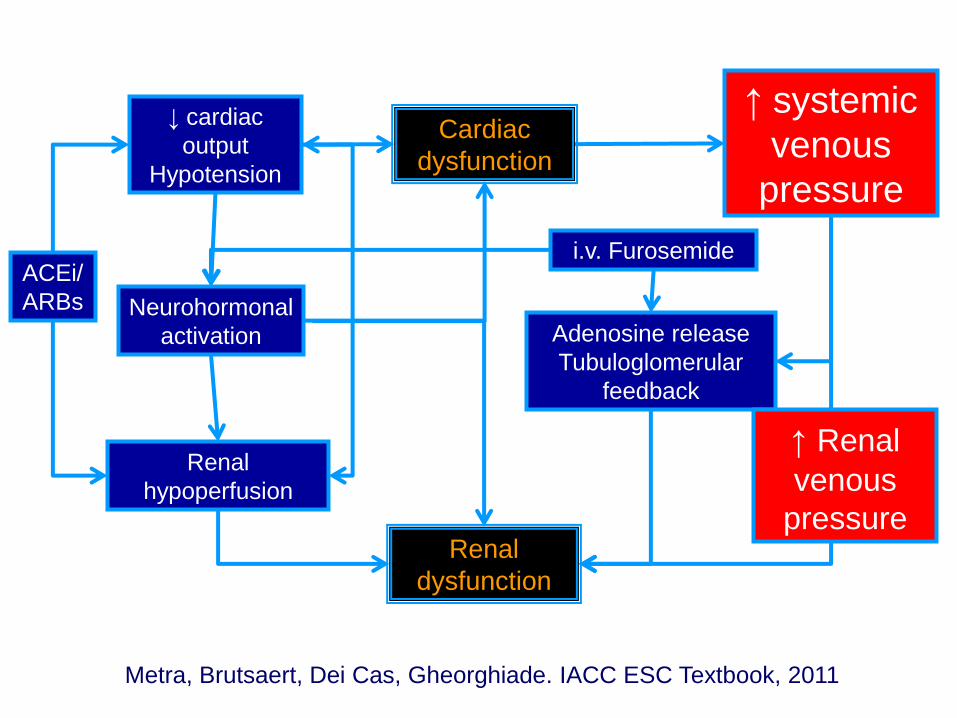
i.v. Furosemide
↑ systemic
venous
pressure
Renal
dysfunction
Neurohormonal
activation
Renal
hypoperfusion
Adenosine release
Tubuloglomerular
feedback
↓ cardiac
output
Hypotension
ACEi/
ARBs
Cardiac
dysfunction
Metra, Brutsaert, Dei Cas, Gheorghiade. IACC ESC Textbook, 2011
↑ Renal
venous
pressure
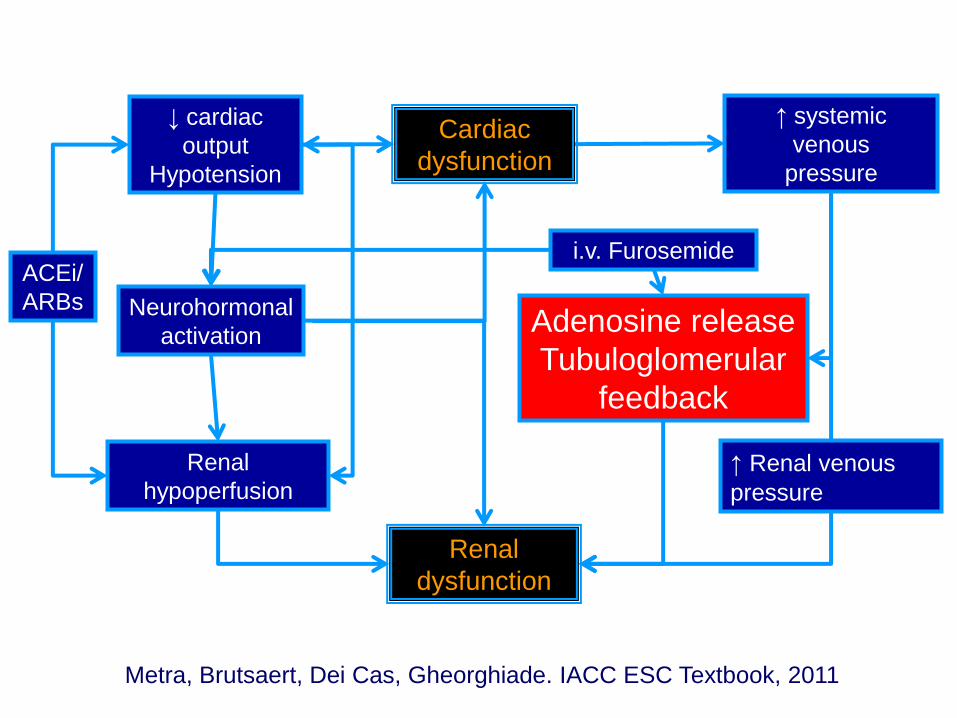
i.v. Furosemide
↑ systemic
venous
pressure
Renal
dysfunction
Neurohormonal
activation
Renal
hypoperfusion
Adenosine release
Tubuloglomerular
feedback
↓ cardiac
output
Hypotension
ACEi/
ARBs
Cardiac
dysfunction
Metra, Brutsaert, Dei Cas, Gheorghiade. IACC ESC Textbook, 2011
↑ Renal venous
pressure
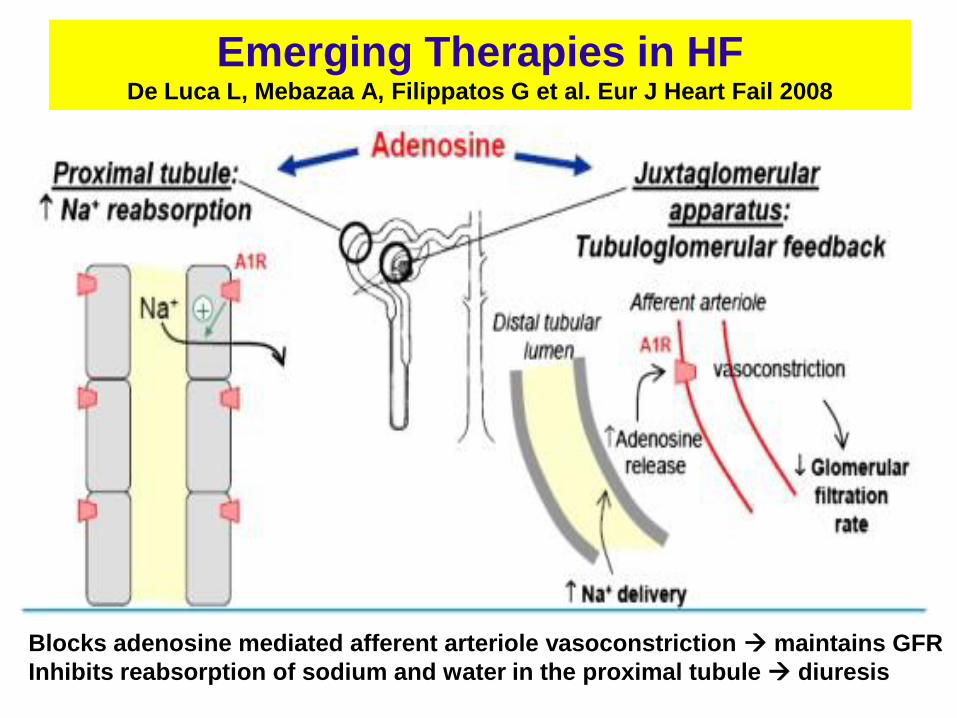
Emerging Therapies in HF De Luca L, Mebazaa A, Filippatos G et al. Eur J Heart Fail 2008
Blocks adenosine mediated afferent arteriole vasoconstriction maintains GFR
Inhibits reabsorption of sodium and water in the proximal tubule diuresis
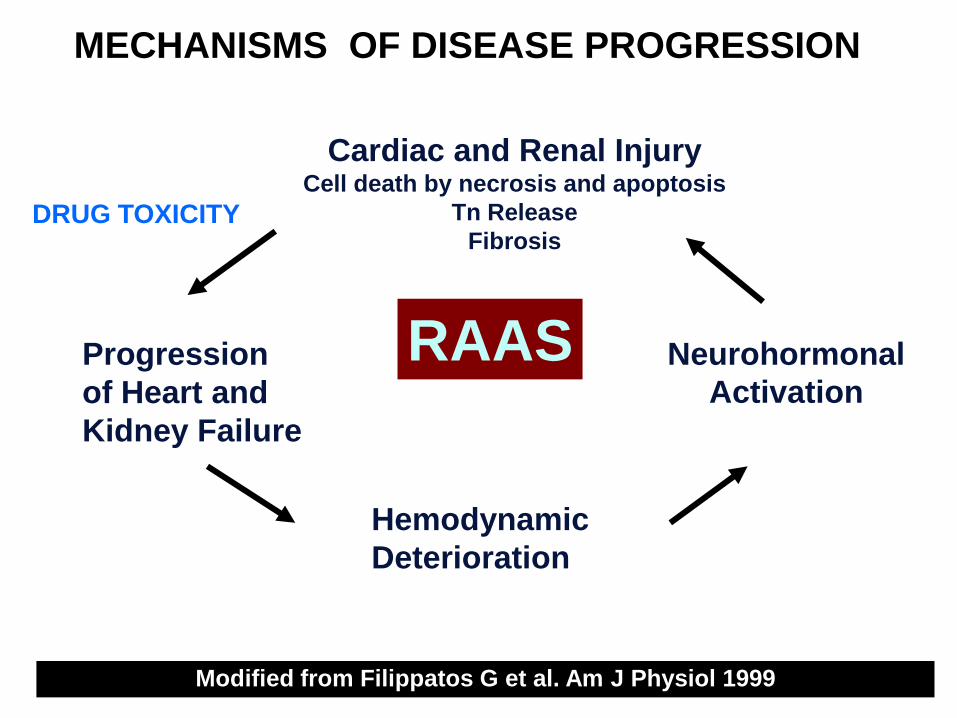
MECHANISMS OF DISEASE PROGRESSION
Cardiac and Renal Injury Cell death by necrosis and apoptosis
Tn Release
Fibrosis
Progression
of Heart and
Kidney Failure
Neurohormonal
Activation
Hemodynamic
Deterioration
Modified from Filippatos G et al. Am J Physiol 1999
RAAS
DRUG TOXICITY
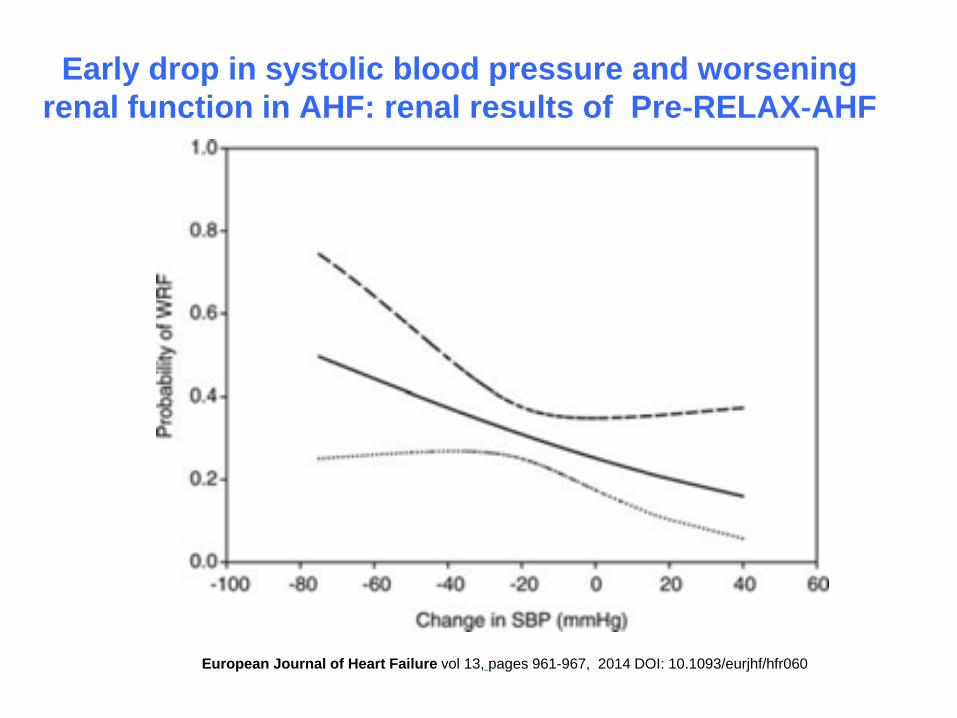
Early drop in systolic blood pressure and worsening
renal function in AHF: renal results of Pre‐RELAX‐AHF
European Journal of Heart Failure vol 13, pages 961-967, 2014 DOI: 10.1093/eurjhf/hfr060
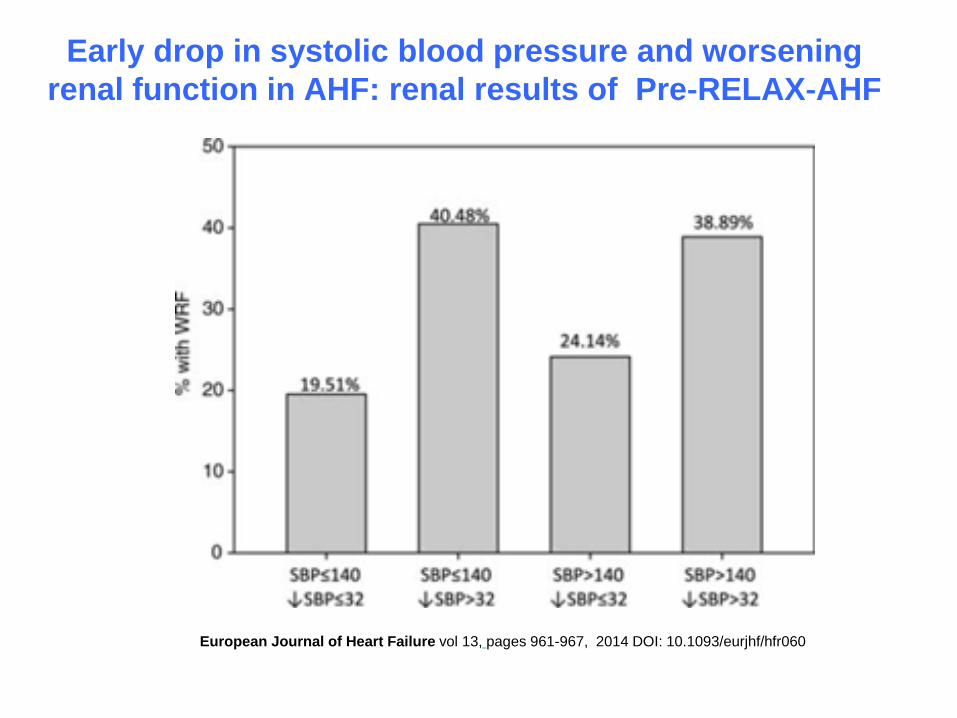
Early drop in systolic blood pressure and worsening
renal function in AHF: renal results of Pre‐RELAX‐AHF
European Journal of Heart Failure vol 13, pages 961-967, 2014 DOI: 10.1093/eurjhf/hfr060
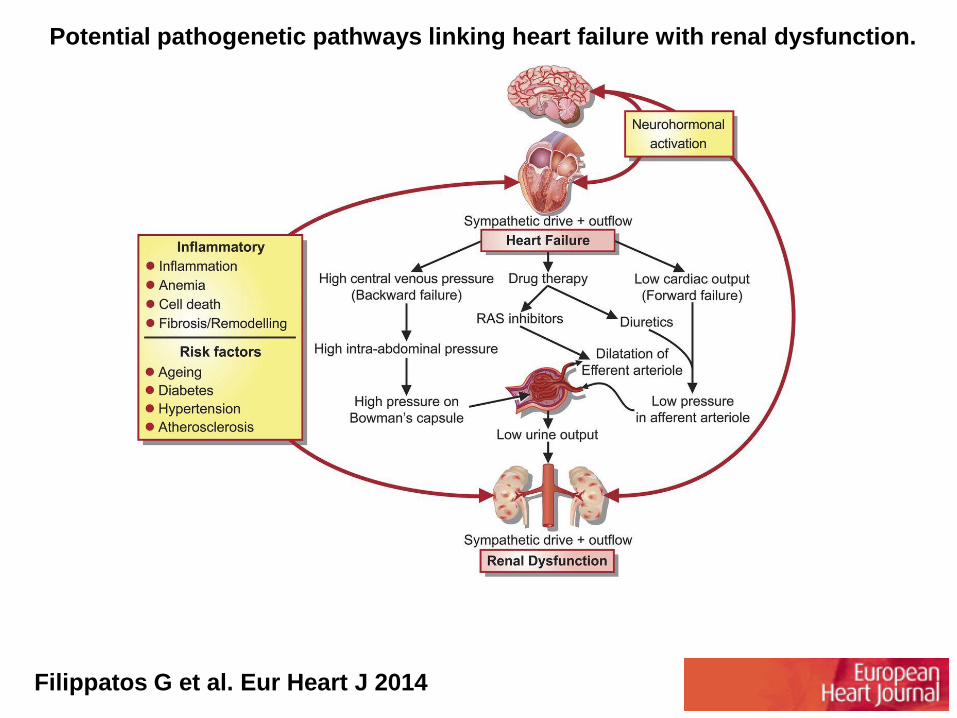
Potential pathogenetic pathways linking heart failure with renal dysfunction.
Filippatos G et al. Eur Heart J 2014
• Definition
• Epidemiology
• Pathophysiology
• Management (?)
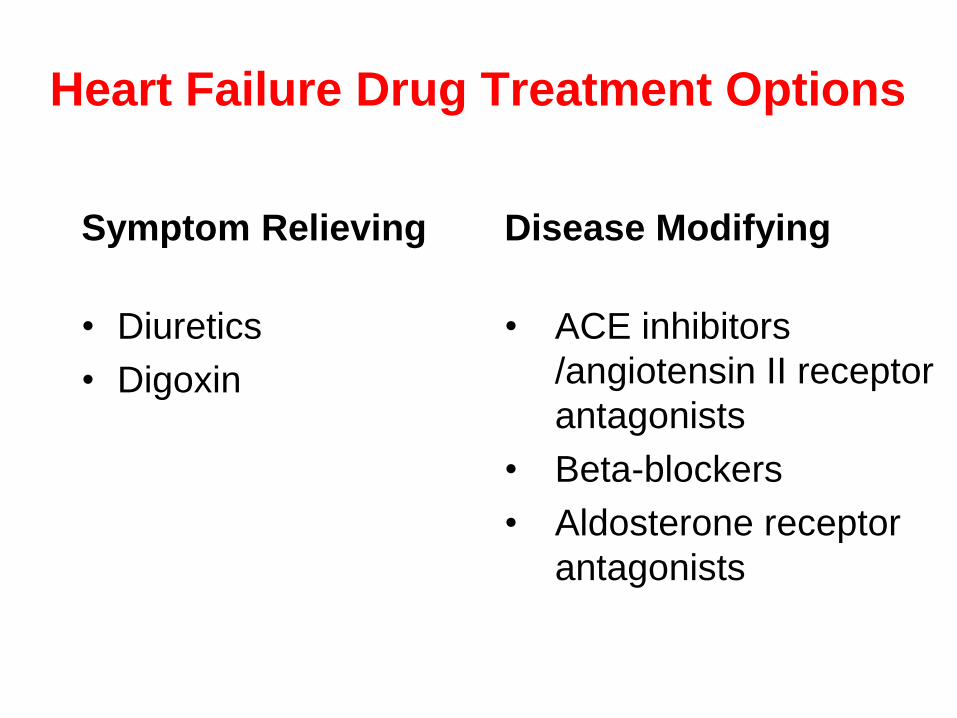
Heart Failure Drug Treatment Options
Symptom Relieving
• Diuretics
• Digoxin
Disease Modifying
• ACE inhibitors
/angiotensin II receptor
antagonists
• Beta-blockers
• Aldosterone receptor
antagonists
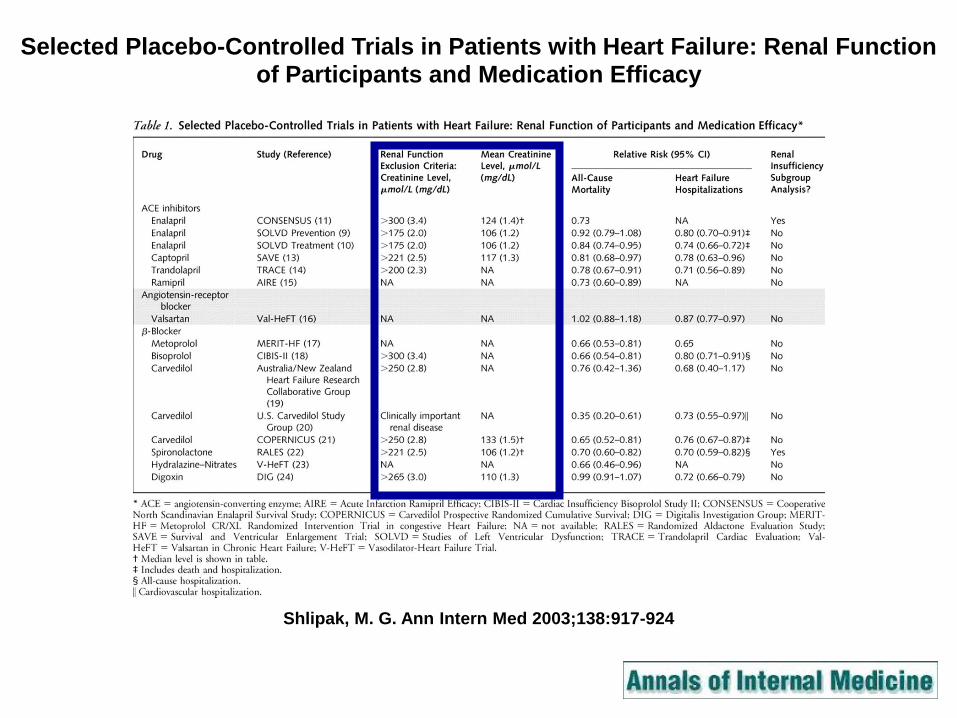
Shlipak, M. G. Ann Intern Med 2003;138:917-924
Selected Placebo-Controlled Trials in Patients with Heart Failure: Renal Function of Participants and Medication Efficacy
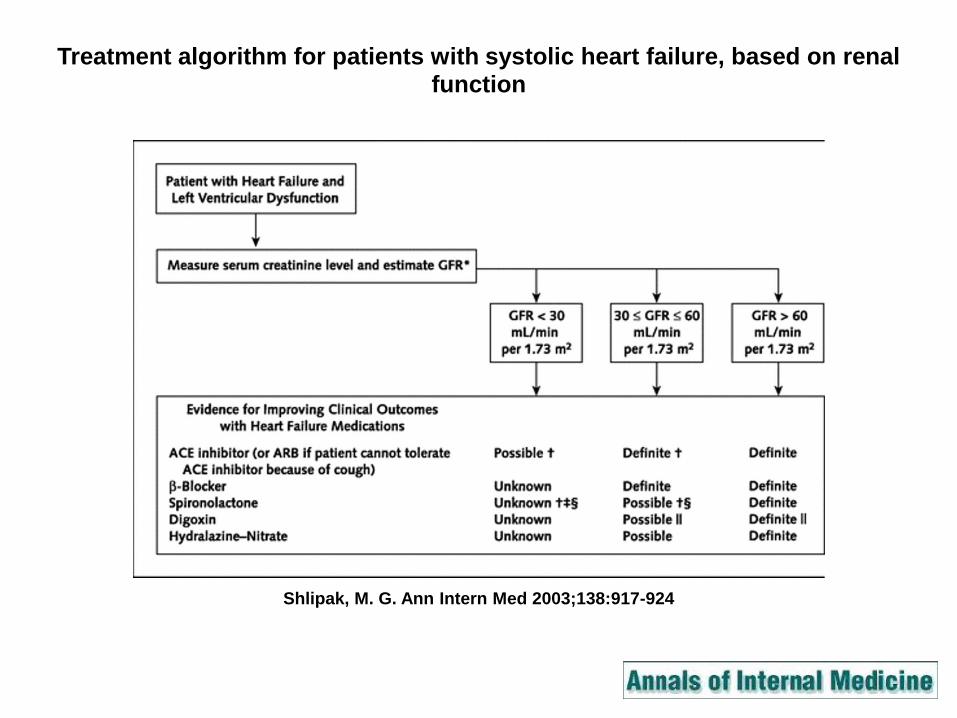
Shlipak, M. G. Ann Intern Med 2003;138:917-924
Treatment algorithm for patients with systolic heart failure, based on renal function
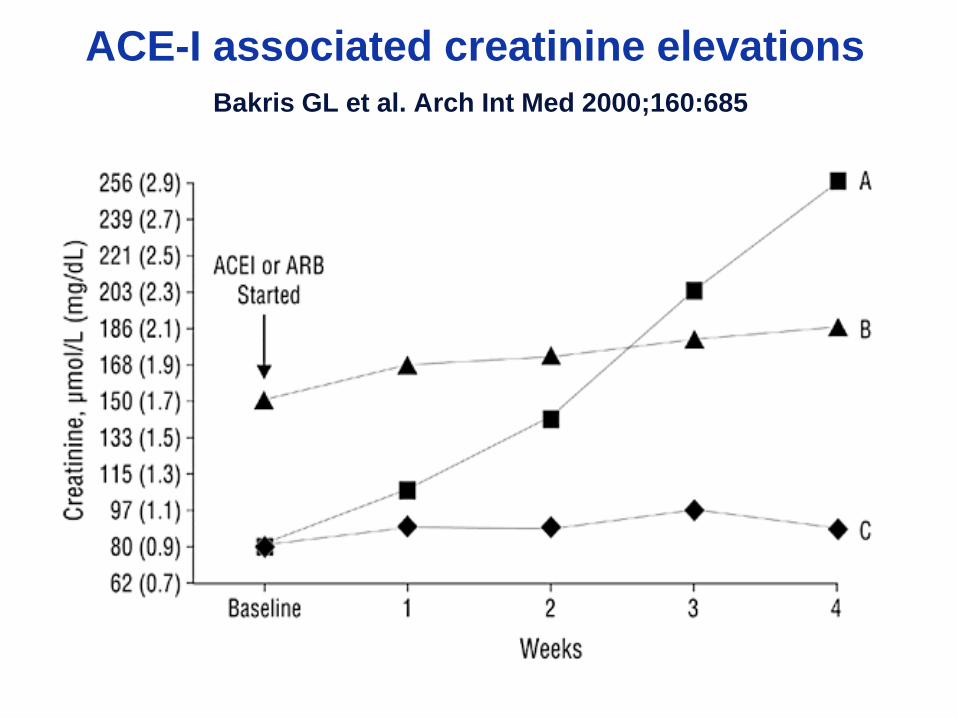
ACE-I associated creatinine elevations
Bakris GL et al. Arch Int Med 2000;160:685
ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure
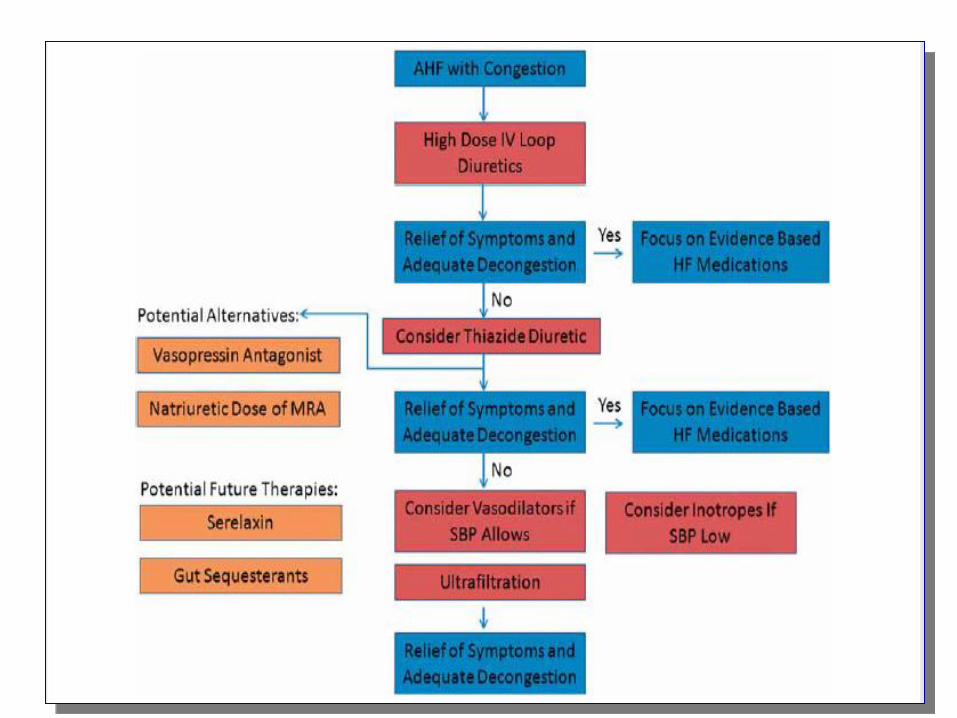
Decompensated chronic HF
• Consider higher dose of diuretics in
renal dysfunction or with chronic
diuretic use.
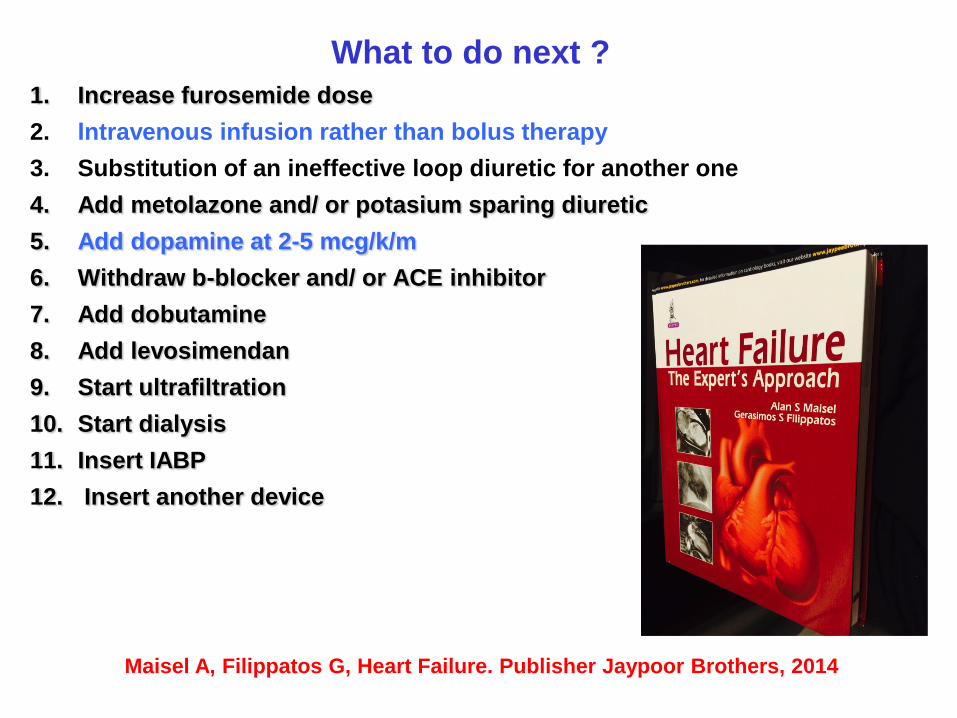
What to do next ?
1. Increase furosemide dose
2. Ιntravenous infusion rather than bolus therapy
3. Substitution of an ineffective loop diuretic for another one
4. Add metolazone and/ or potasium sparing diuretic
5. Add dopamine at 2-5 mcg/k/m
6. Withdraw b-blocker and/ or ACE inhibitor
7. Add dobutamine
8. Add levosimendan
9. Start ultrafiltration
10. Start dialysis
11. Insert IABP
12. Insert another device
Maisel A, Filippatos G, Heart Failure. Publisher Jaypoor Brothers, 2014
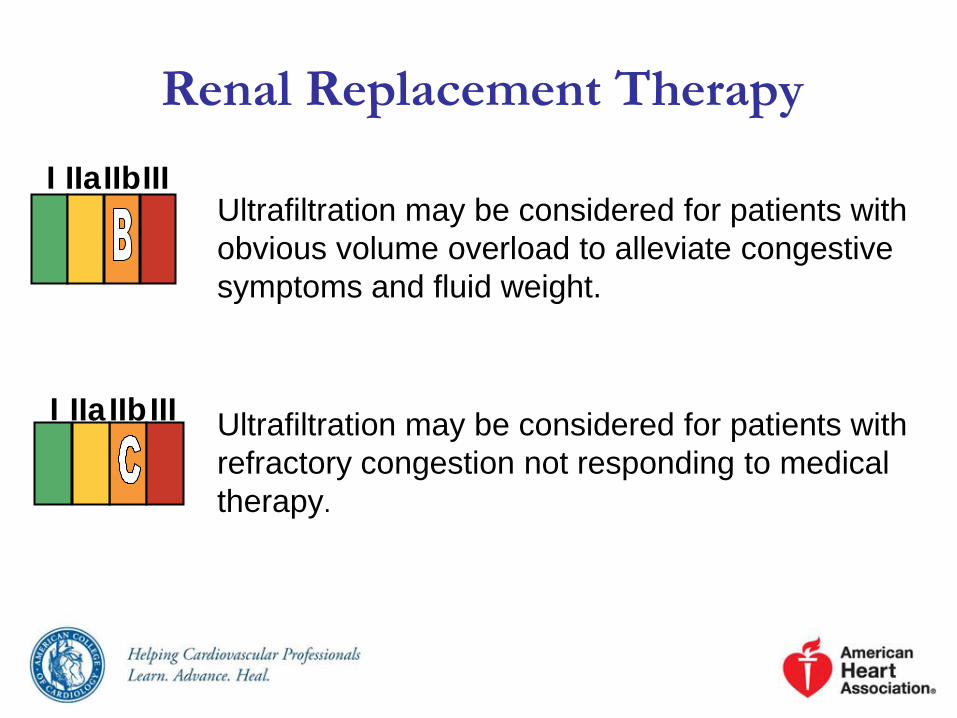
Renal Replacement Therapy
Ultrafiltration may be considered for patients with
obvious volume overload to alleviate congestive
symptoms and fluid weight.
Ultrafiltration may be considered for patients with
refractory congestion not responding to medical
therapy.
I IIa IIb III
I IIa IIb III
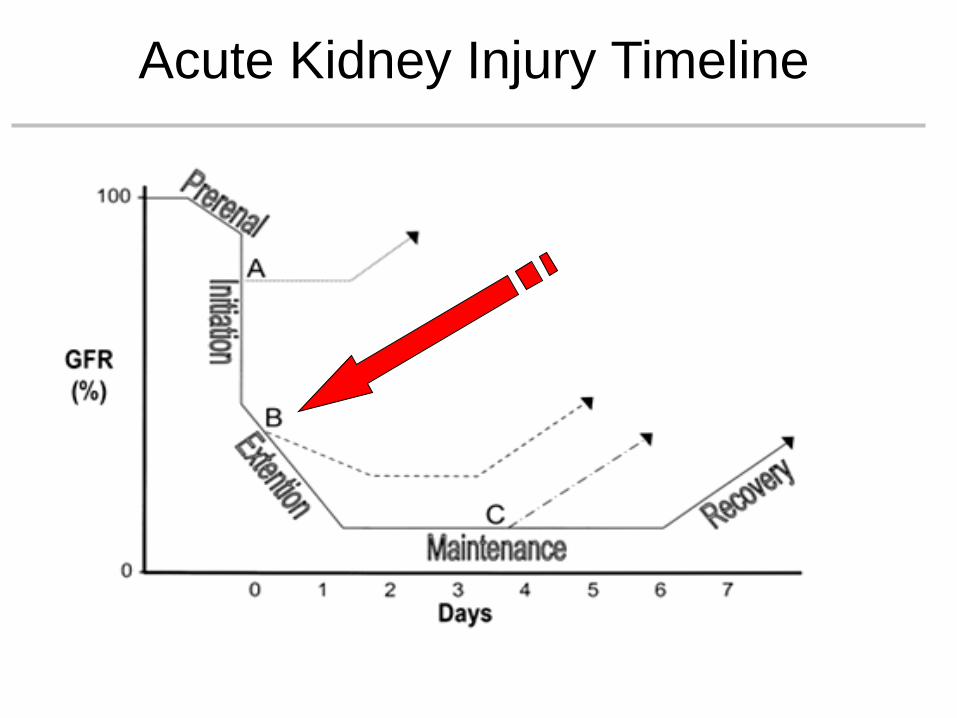
Acute Kidney Injury Timeline
Cardiorenal Interaction: The Future
We need to use meaningful definitions and
validate them in different clinical settings.
We need to evaluate the impact of early
biomarkers on diagnosis and various therapeutic
approaches
We need to appraise current evidence and
generate wise recommendations for practice.
We need research to generate the missing
evidence.