
Healthy Babies are Worth the Wait ®: Preventable Preterm Births Katrina Thompson, Karla Damus, Dr....
26
Healthy Babies are Healthy Babies are Worth the Wait Worth the Wait ®: ®: Preventable Preterm Births Preventable Preterm Births Katrina Thompson, Karla Damus, Dr. Diane Ashton, Dr. Ruth Ann Shepherd
-
Upload
samantha-small -
Category
Documents
-
view
218 -
download
0
Transcript of Healthy Babies are Worth the Wait ®: Preventable Preterm Births Katrina Thompson, Karla Damus, Dr....

Healthy Babies Healthy Babies are Worth the are Worth the
WaitWait®:®:
Preventable Preterm BirthsPreventable Preterm Births
Katrina Thompson, Karla Damus, Dr. Diane Ashton, Dr. Ruth Ann Shepherd
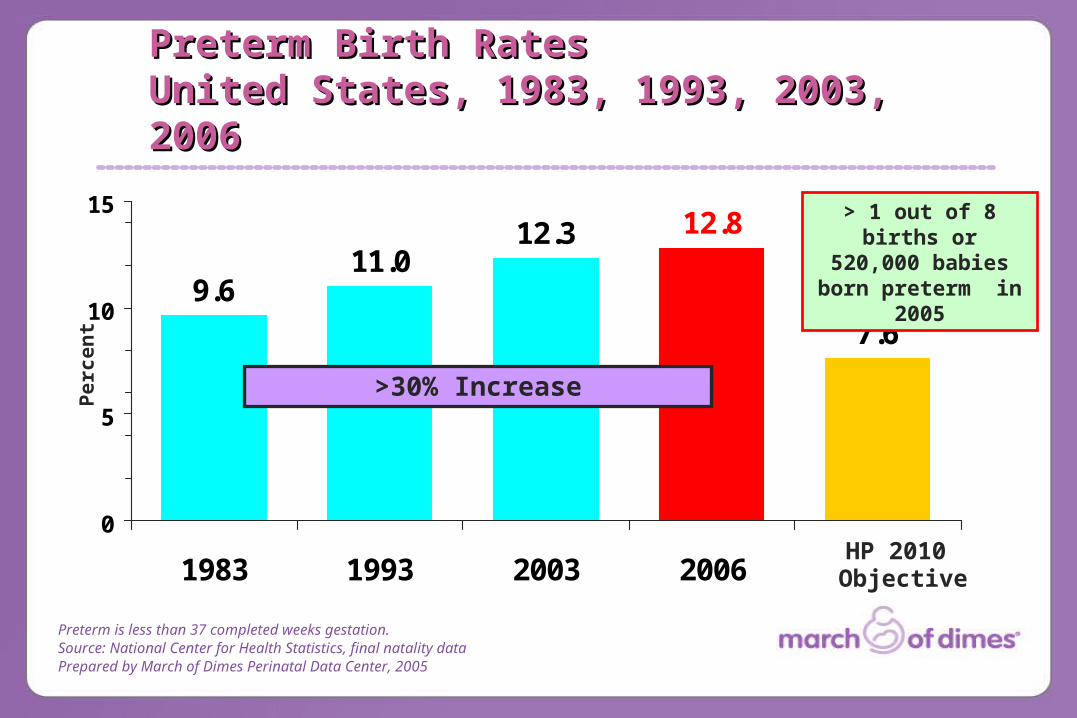
9.611.0
12.3
7.6
12.8
0
5
10
15
1983 1993 2003 2006
Preterm is less than 37 completed weeks gestation.Source: National Center for Health Statistics, final natality dataPrepared by March of Dimes Perinatal Data Center, 2005
Pe
rce
nt
HP 2010 Objective
>30% Increase
Preterm Birth RatesPreterm Birth RatesUnited States, 1983, 1993, 2003, United States, 1983, 1993, 2003, 20062006
> 1 out of 8 births or 520,000 babies born
preterm in 2005
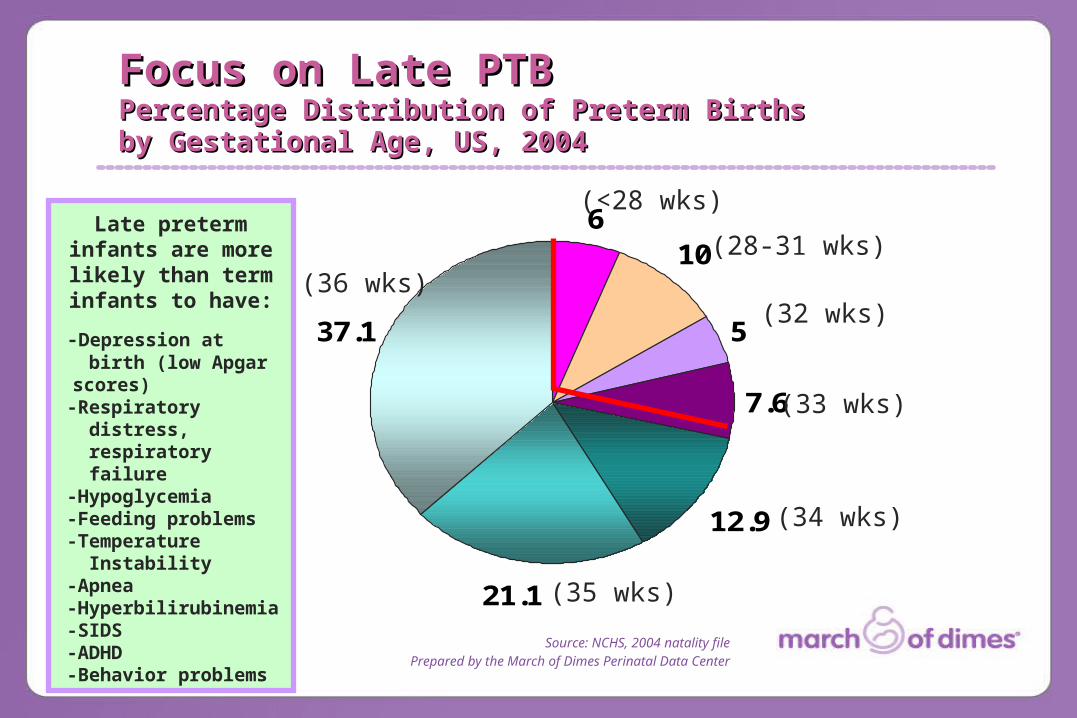
Focus on Late PTBFocus on Late PTBPercentage Distribution of Preterm Births Percentage Distribution of Preterm Births by Gestational Age, US, 2004by Gestational Age, US, 2004
Source: NCHS, 2004 natality filePrepared by the March of Dimes Perinatal Data Center
610
5
7.6
12.9
21.1
37.1
(34 wks)
(33 wks)
(32 wks)
(<28 wks)
(35 wks)
(36 wks)
(28-31 wks)Late preterm infants are
more likely than term infants to have:
-Depression at birth (low Apgar scores)-Respiratory distress, respiratory failure -Hypoglycemia-Feeding problems-Temperature Instability-Apnea-Hyperbilirubinemia-SIDS-ADHD-Behavior problems
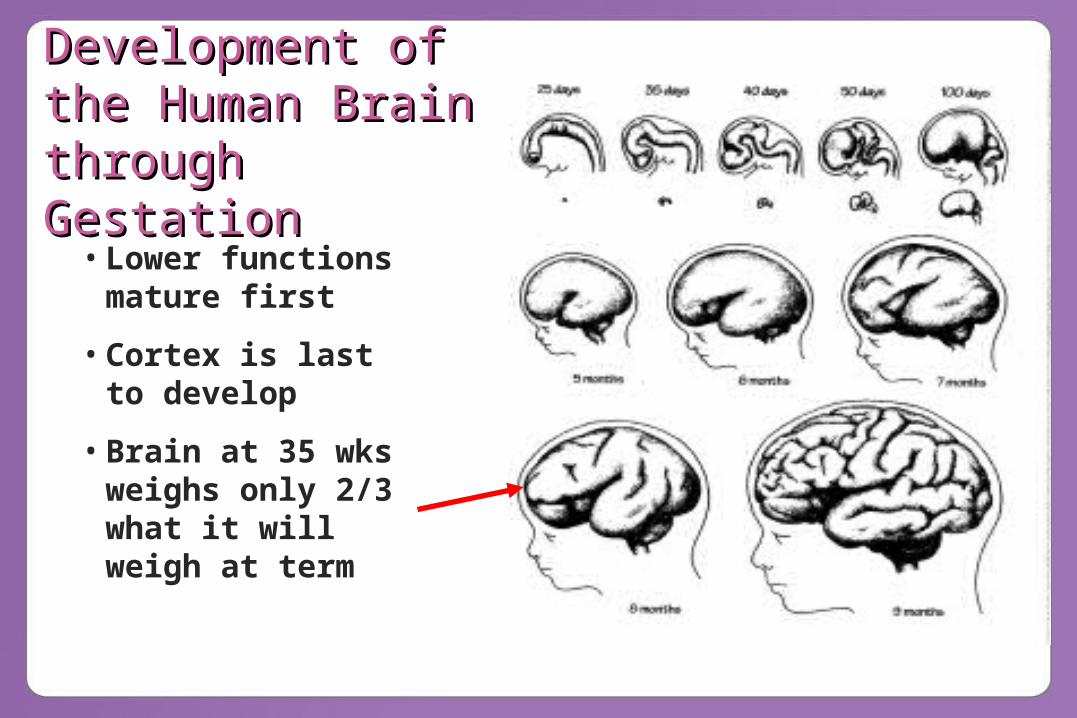
• Lower functions mature first
• Cortex is last to develop
• Brain at 35 wks weighs only 2/3 what it will weigh at term
Development of Development of the Human Brain the Human Brain through through GestationGestation

A Collaborative PartnershipA Collaborative Partnership
The “Prematurity Prevention Partnership”:
– March of Dimes– Johnson & Johnson Pediatric Institute– Kentucky Department for Public Health
Kentucky ChapterProfessional Organizations (ACOG, AAP,
AWHONN)Kentucky Perinatal Leaders

Healthy Babies are Worth the Wait® • Prevent “preventable” preterm births in target areas
of Kentucky• Three-year Initiative (2007-2009) in partnership with
Johnson & Johnson Pediatric Institute and Kentucky Department for Public Health
• Evidence-based interventions-clinical-public health
• Focus on late preterm birth (34-36 weeks)• Targets both perinatal providers and childbearing
women• System of collaboration between clinical and public
health leadership
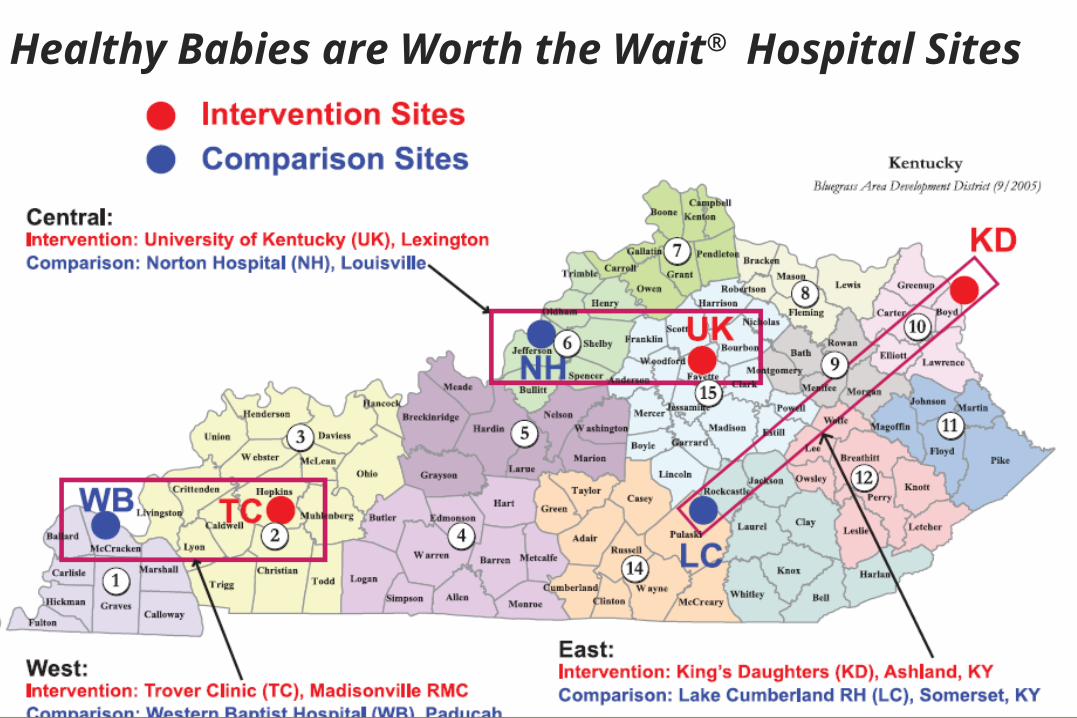
Healthy Babies are Worth the Wait®
Hospital Sites

InterventionsInterventions “Bundled” Evidence-Based Interventions Linked elements of clinical care, public health and consumer education:– Consumer Awareness and Education
• Health literacy in context of prenatal care• Community outreach
– Professional Continuing Education• Grand Rounds & Training
– Public Health Intervention• Augmenting existing services for case management, screening & referral
– Clinical Intervention in Prenatal Period• Standard clinical guidelines (folic acid, smoking cessation, progesterone)• Patient safety
What Pregnant Women Can Do to Help Prevent Preterm What Pregnant Women Can Do to Help Prevent Preterm BirthBirthMessages for pregnant women (and women of childbearing age)• Some preterm births—especially late preterm—could be prevented if all
pregnant women:– Get early, regular prenatal care – Quit smoking or at least cut back and avoid secondhand smoke– Avoid all alcohol – Take folic acid daily before, during and between pregnancies– Pay careful attention to good nutrition and eat a balanced diet with lots of fruits
and vegetables – Gain only the weight recommended by your health care provider– Receive timely and appropriate treatment for existing medical conditions such as
diabetes, high blood pressure, thyroid disease, addictions, and all infections including STIs
– Take good care of their teeth--brush, floss, and visit a dentist regularly– Try to avoid stress and ask for help from their health care provider or support
person to manage stressful situations in your life– Question the reason to schedule any delivery before 39 weeks unless there are
medical reasons for an early delivery– Avoid elective induction or elective cesarean delivery including cesarean delivery
on maternal request before 39 weeks– Talk to their doctor if you have a history of spontaneous preterm labor or birth and
are carrying a single baby about possible receiving progesterone to help prevent another preterm delivery

What Communities Can Do to Help Prevent What Communities Can Do to Help Prevent Preterm Birth Preterm Birth Messages for the community• Preterm birth has consequences for many facets of our
communities, including school systems, employers and insurers
• Make preventing preterm birth a priority in each community, as it will result in healthier babies, children, future parents and less chronic disease in all residents
• Visit and use materials from the Healthy Babies Are Worth the Wait website www.prematurityprevention.org
• Do not smoke around pregnant women, babies or children• Host a Healthy Babies Are Wroth the Wait Prematurity
Prevention awareness session where participants learn about preterm birth and how they can help to make a difference in their community
• Raise awareness of services and resources available to pregnant women and their families from the local clinical sites and the health department
• Work together on this leading public health problem as everyone can make a difference for the health of families in Kentucky
Barriers Barriers (due to dynamic conditions contributing to (due to dynamic conditions contributing to preterm birth)preterm birth)• high rates of high risk factors (such as smoking, abuse of
pain medication/oxycodone, illicit drug use, stress, infections, obesity)
• significant changes in the culture of childbearing by pregnant women (scheduling deliveries, CDMR)
• significant changes in obstetrical management with more inductions, cesareans and other procedures contributing to higher rates of iatrogenic late preterm birth
• changes in health care delivery systems, reimbursement structures and a litigious environment for obstetrical care
• These barriers are being overcome by successful implementation of the components of HBWW and with the close collaboration and guidance of key leadership in clinical, public health and communications/media. A focus on patient safety protocols is being implemented in year 2.
Consumer Survey: Methodology SnapshotConsumer Survey: Methodology Snapshot
KAB (knowledge, attitudes, beliefs/reported behaviors) survey– 39-item core questionnaire– 14-item optional supplement
Questions from PRAMS, BRFSS, and MOD surveys Original questions specific to needs of HBWW interventionsFocus groups and pilot testingAnonymous, voluntary, convenience samplingAnalysis done in SPSS®
WHO? Pregnant women presenting for prenatal care
WHAT? Questions assessing KAB regarding pregnancy and childbirth
WHERE Intervention and comparison sites (clinics, centering classes, private offices)
WHEN? January-May, 2007
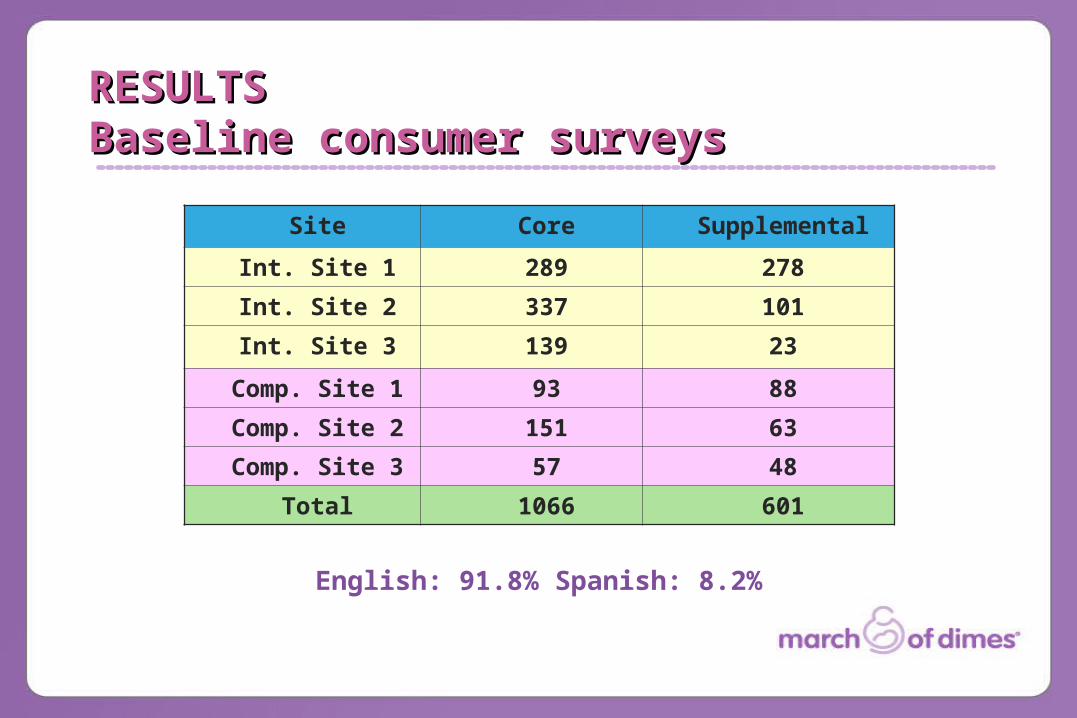
Site Core Supplemental
Int. Site 1 289 278
Int. Site 2 337 101
Int. Site 3 139 23
Comp. Site 1 93 88
Comp. Site 2 151 63
Comp. Site 3 57 48
Total 1066 601
English: 91.8% Spanish: 8.2%
RESULTSRESULTSBaseline consumer surveysBaseline consumer surveys

Demographic CharacteristicsDemographic CharacteristicsHBWW Consumer Survey RespondentsHBWW Consumer Survey Respondents
Maternal Age
<20 years 14%
20-34 years 77%
35+ years 6%
mean +/- sd 25.3 +/- 5.401
range 14-45
Race
White 80%
Black 9%
Hispanic Ethnicity
Yes 9%
Marital Status
Married 54%
Single/partner 20%
Single 22%
Maternal Education
<HS 18%
HS 26%
Some College 38%
Bachelors 14%
Payor
Medicaid 50%
Private 35%
Self 3%

Of women in their 3rd trimester, 66% reported that their hcp had discussed the signs and symptoms of preterm labor with them.
Of the 24% of pregnant women who had a
previous preterm birth, 13% reported that their
providers had discussed
progesterone with them in their current
pregnancy.
Obstetrical-Related FactorsObstetrical-Related FactorsHBWW Consumer Survey RespondentsHBWW Consumer Survey Respondents
Previous C/S
None 63%
1 21%
2 7%
3+ 2%
range 0-4
Inductions
None 42%
1 38%
2+ 10%
range 0-6
Trimester
1st 9%
2nd 28%
3rd 59%
Planned Preg 39%
Previous Births
None 41%
1 31%
2 16%
3+ 11%
mean +/- sd1.02 +/- 1.129
range 0-6
Previous Preterm
None 71%
1 17%
2+ 7%
mean +/- sd0.35 +/- 0.709
range 0-5
Multiple Birth 2.5%
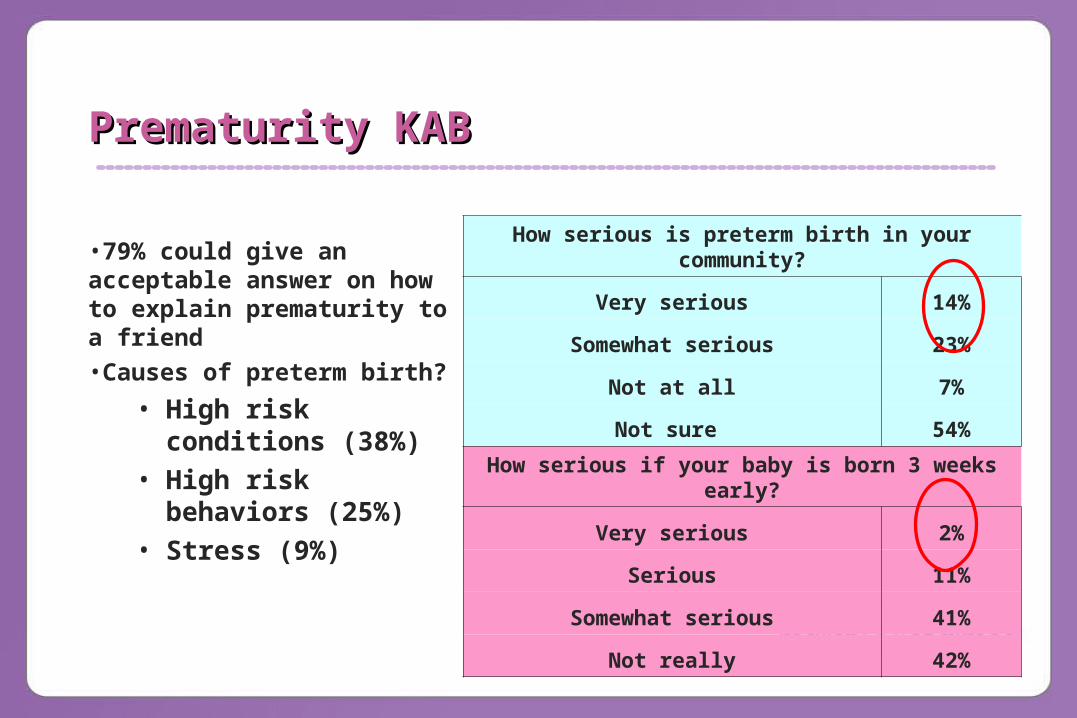
Prematurity KABPrematurity KAB
•79% could give an acceptable answer on how to explain prematurity to a friend•Causes of preterm birth?
• High risk conditions (38%)
• High risk behaviors (25%)
• Stress (9%)
How serious is preterm birth in your community?
Very serious 14%
Somewhat serious 23%
Not at all 7%
Not sure 54%
How serious if your baby is born 3 weeks early?
Very serious 2%
Serious 11%
Somewhat serious 41%
Not really 42%

24
614
76
5 6 4
44
0
20
40
60
80
Daily Weekly A FewTimes/Wk
Never
Preconception
During this Pregnancy
Pe
rce
nt
Periconceptional Vitamin UsePericonceptional Vitamin Use by Women of Childbearing Age by Women of Childbearing Age
HBWW Consumer Survey 2007

34
21
32
22
0
5
10
15
20
25
30
35
Preconceptional Prenatal KY (2005) US (2005)
www.marchofdimes.com/peristats
Pe
rce
nt
Behavioral Risk Factors:Behavioral Risk Factors:Smoking by Women of Childbearing Smoking by Women of Childbearing AgeAge
HBWW Survey 38% of respondents reported that at least 1 smoker lived in their home

40
28
34
47
60
0 10 20 30 40 50 60 70
At least one service needed
Did not see a hcp in year beforepregnancy
Provider did not say avoid alcohol
Teeth need work or in poorcondition
Feel blue, stressed, depressed 1+days/wk
Percent
Other Risk Factors for Preterm Other Risk Factors for Preterm BirthBirth
HBWW Consumer Survey, 2007
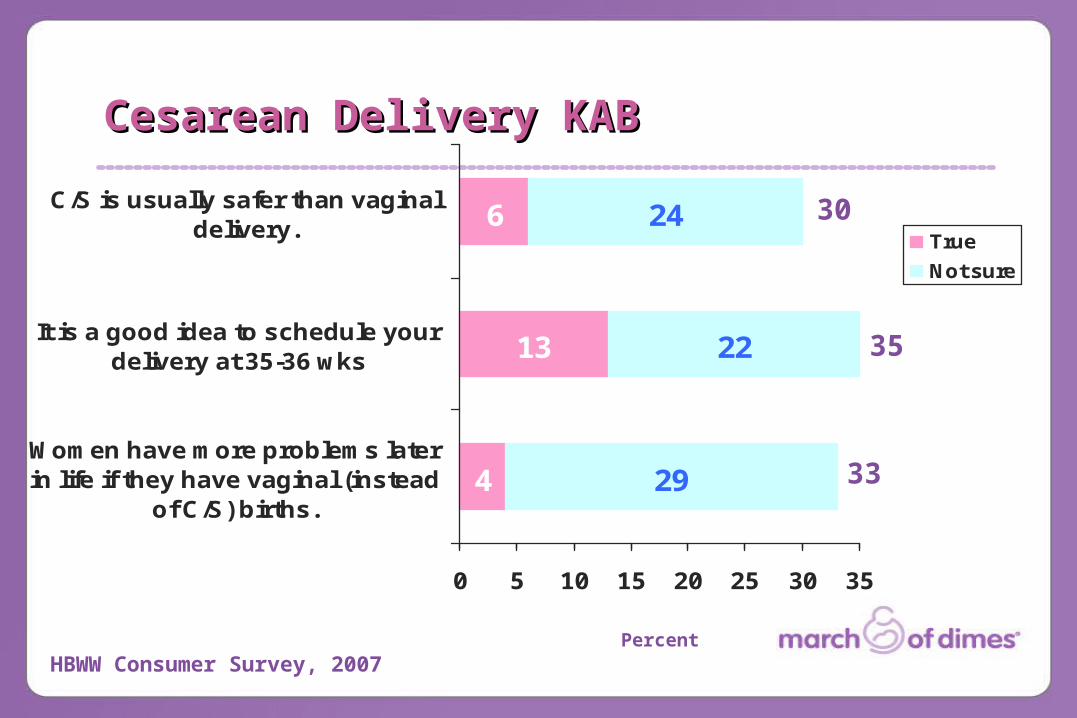
4
13
6
29
22
24
0 5 10 15 20 25 30 35
Women have more problems laterin life if they have vaginal (instead
of C/S) births.
It is a good idea to schedule yourdelivery at 35-36 wks
C/S is usually safer than vaginaldelivery.
True
Not sure
Percent
Cesarean Delivery KABCesarean Delivery KAB
HBWW Consumer Survey, 2007
30
35
33
• Reduction of singleton LPTB rate
• Reduction in elective inductions and sections conducted prior to 39 weeks gestation
• Increase in baby’s average days of gestational age and birth weight
• Reduction in neonate’s length of hospital stay
• Reduction in hospital cost / charges associated with preterm births
• Positive change in consumer and provider knowledge, attitudes, and behaviors regarding PTB
More information: www.prematurityprevention.org
Goal: reduction of singleton PTB rate Goal: reduction of singleton PTB rate by 15% in Intervention Sitesby 15% in Intervention Sites
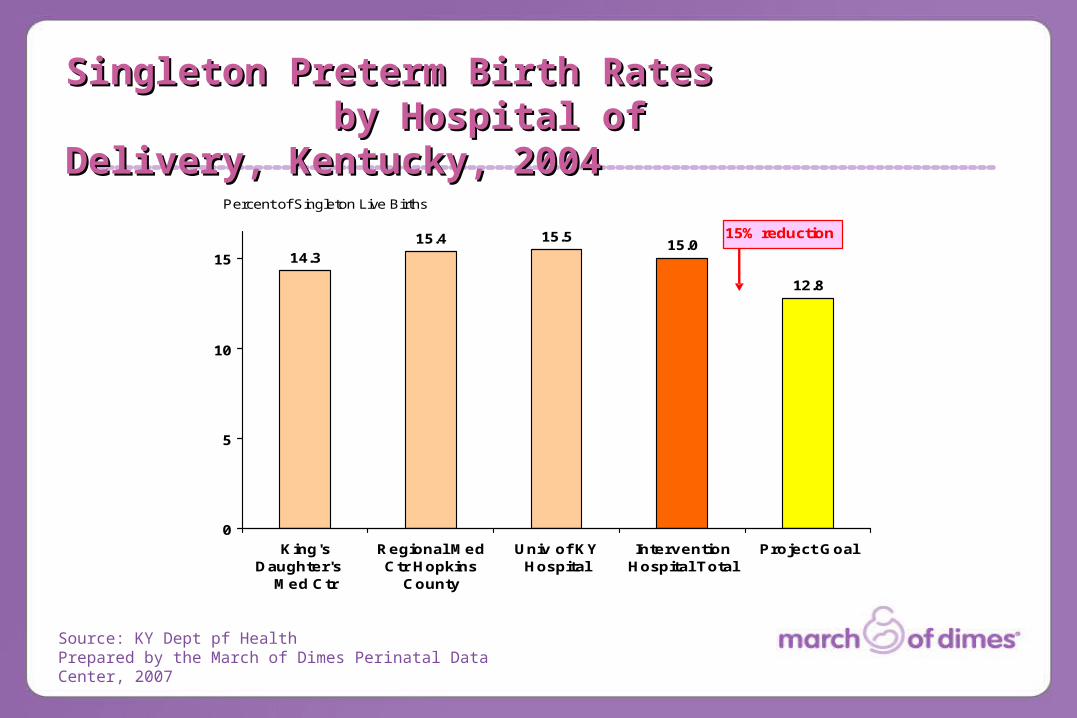
Singleton Preterm Birth RatesBy Hospital of Delivery, Kentucky, 2004
Preterm is less than 37 completed weeks gestationSource: KY Dept of HealthPrepared by the March of Dimes Perinatal Data Center, 2007
14.3
15.4 15.5
12.8
15.0
0
5
10
15
King'sDaughter's
Med Ctr
Regional MedCtr Hopkins
County
Univ of KYHospital
InterventionHospital Total
Project Goal
Percent of Singleton Live Births
15% reduction
Source: KY Dept pf HealthPrepared by the March of Dimes Perinatal Data Center, 2007
Singleton Preterm Birth Rates Singleton Preterm Birth Rates by Hospital of Delivery, by Hospital of Delivery, Kentucky, 2004Kentucky, 2004

www.prematurityprevention.org


Take Home Message-Take Home Message-You Can Prevent Some Preterm You Can Prevent Some Preterm BirthsBirths The overall message is that despite years of
research and programs to attempt to reduce preterm birth, the rates continue to rise reaching an all time high of 12.7% for the US and 15% for KY in 2005.
However, since most of this increase is due to the rising rates of late preterm birth (34-36 weeks) a thorough understanding of contributing modifiable risk factors and an innovative program to address local issues driven by timely local information can begin to reduce these seemingly run away rates and in doing improve health by decreasing morbidity and mortality for infants, children and ultimately adults.
““Because this is a real-world model, and Because this is a real-world model, and focuses on education and enhancing focuses on education and enhancing
existing systems of care, we anticipate existing systems of care, we anticipate that it will be feasible to implement the that it will be feasible to implement the
lessons learned statewide. We are lessons learned statewide. We are confident this initiative will improve the confident this initiative will improve the
lives of mothers and babies.”lives of mothers and babies.”Dr. Ruth Ann Shepherd
Director, Adult and Child Health Improvement
Kentucky Department for Public Health


















