Healthcare Reform and Accountable Care: Where Do We - Amerinet
16
2011 Executive Briefing Healthcare Reform and Accountable Care: Where Do We Stand?
Transcript of Healthcare Reform and Accountable Care: Where Do We - Amerinet

2011 Executive Briefing
Healthcare Reform and Accountable Care: Where Do We Stand?
page B | Executive Briefing
AMERINET BOARD
ChairAlbert ZimmerliSenior Vice President and CFOIntermountain Healthcare
Vice ChairRobert MulcaheyVice President and COOStratum Med, Inc.
MemberEdward AndersenPresident and CEOCGH Medical Center
MemberDouglas BlackBoard of DirectorsAmerinet
MemberChristopher CoonsCEO and Regional Vice President Southwest RegionCEO, Home Health ServicesIntermountain Healthcare
MemberMichael FarrellCEOSomerset Hospital
Tim Barnett President and CEO Yavapai Regional Medical Center
Tim BriertySenior Vice President/ Hospital Administrator University Health System
Todd EbertPresident and CEO Amerinet
David H. FreedPresident and CEO Nyack Hospital
John E. Horns President of Regionalization ProMedica Health System
Kathleen KruegerPresident Supply Chain ProMedica Health System
John MatessinoPresident and CEO Louisiana Hospital Association
Robert MillerCEO Coshocton Hospital
Anne MitchellSenior Director Quality and Patient Safety Amerinet
James MooreCEO OSF Healthcare System
Larry A. Mullins, M.D.President and CEO Samaritan Health Services
Scott ParkerPresident Emeritus Intermountain Healthcare
Ted PasinskiPresident St. Joseph’s Hospital Health Center
Kevin SchoepleinExecutive Vice President OSF Healthcare System
Charles Sorenson, M.D. President and CEO Intermountain Healthcare
Brian StraebExecutive Vice President Sales and Marketing Amerinet
Mina UbbingPresident and CEO Fairfield Medical Center
Randy WalterFACHE, Executive Vice President Contracting and Enterprise Solutions Amerinet
William Weeks, M.D., M.B.A. Associate Professor and Course Director The Dartmouth Institute for Health Policy and Clinical Practice
Craig Westling, M.S., M.P.H. Managing Director, Accountable Care and of the Office of Professional Education and Outreach The Dartmouth Institute for Health Policy and Clinical Practice
Roundtable Attendees
Table of Contents
Roundtable Moderators
2 The Issues
5 What is an ACO?
7 How Does an ACO Achieve Results?
8 What You Can Work on Right Now
11 Best Practice – Center for Shared Decision Making
13 What Now...

Amerinet | page 1
One of the most important components of the recently enacted Patient Protection and Affordable Care Act (PPACA) is the establishment of Accountable Care Organizations (ACOs), which are designed to improve the overall value of patient care delivery, as measured by cost and quality.While the healthcare community is still trying to determine the benefits and challenges of becoming an ACO, it is clear that the accountable care model will significantly change the way providers care for their patients, are reimbursed for care and are held ‘accountable’ for the health outcomes of patients they treat.
Everywhere you turn in healthcare media today, various entities are professing to have all the answers concerning ACOs. These claims generally ring hollow because of the great unknown that still exists. A few things are certain, however – cost reduction, improved quality, alignment of services and value-based purchasing will be key in any impending reform.
In response to this important need for accurate information and guidance, Amerinet has engaged both the leaders among our executive membership, and the organization that brought the concept of Accountable Care to the forefront of our nation’s dialogue, the Dartmouth Institute for Healthcare Policy and Clinical Practice (TDI). Amerinet has chosen to engage these members and industry leaders in exploring the issues that are most relevant to them, and create dialogue and resources that can provide members the greatest benefit. TDI is a preeminent research and educational institution dedicated to improving healthcare through education, research, policy reform, leadership improvement and communication with patients and the public. We also surveyed our members in October 2010 with the objective of reviewing their perceptions and opinions regarding healthcare reform and ACOs. The survey results that form the basis of this report illustrate the challenges our members are experiencing. The accompanying discussion and presentation provide further information and guidance in navigating the waters of healthcare reform and ACO implementation.
I would like to thank Craig Westling and Dr. Bill Weeks of The Dartmouth Institute for leading the discussion on the need for accountability and how these elements must be part of the successful healthcare model going forward, no matter what specific form they may take.
A Letter from Amerinet’s President and CEO

page 2 | Executive Briefing
The IssuesThe term “healthcare reform” means many different things to many different people. Over the past several years, it has taken on added significance as President Obama has advanced plans to restructure healthcare delivery and make changes to how facilities are reimbursed for care.Although many disagree on whether reform as currently envisioned addresses these issues properly, it is generally agreed on both sides of the political aisle that real reform must reduce costs, improve the quality of care and improve the health of the population. In short, we must create payment models that reward value and not volume.
The common thread binding the foundations of reform is the idea of accountable care, which can be defined as a group of healthcare providers working together to assume shared accountability for the quality and cost of the care they provide to their community, with an overall focus on improving healthcare value. Moving to an accountable care model is a bold strategic initiative designed to position an organization for long-term success … in an uncertain future operating environment. This new, value-based system, is built around the integration and cooperation of providers who manage a population through team-based care. To do this, incentives must be aligned, and all stakeholders must focus on quality, efficiency and value.
Against this backdrop, the 2011 Amerinet Executive Roundtable and corresponding survey sought to gather feedback and enhance knowledge concerning attitudes toward healthcare reform and accountable care.
Amerinet engaged The Dartmouth Institute for Health Policy and Clinical Practice (TDI) to moderate the roundtable session and share nearly 40 years of research and information on the subject of accountable care. TDI was founded in 1988 by Dr. John E. Wennberg as the Center for the Evaluative Clinical Sciences (CECS). Over the years, TDI has established a new discipline and educational focus in the evaluative clinical sciences, introduced and
advanced the concept of shared decision-making for patients, demonstrated unwarranted variation in the practice and outcomes of medical treatment, and shown that more healthcare is not necessarily better care. By demonstrating a healthy skepticism about new treatments and medical “breakthroughs,” investigating the risks and benefits of many common therapies and surgeries, and offering unique educational programs, TDI has produced more informed agents of change among physicians, health professionals, the media and the public. The organization actually traces its roots back to 1973, when Dr. Wennberg published his first article on geographic variation in healthcare, which eventually led to a series of groundbreaking Dartmouth Atlas reports. In 2008, Dr. Wennberg received the Institute of Medicine’s highest honor, the Lienhard Award, for “his impact on the evolution of healthcare delivery in the United States.”
In terms of the Amerinet Executive Roundtable survey, respondents expressed a negative opinion about healthcare reform, which appears to be mainly due to the uncertainty and lack of direction surrounding it. Respondents were more positive about the general concept of ACOs, with more than 80 percent considering the implementation of an ACO.
“The issue of healthcare reform is somewhat negative because assessing the real impact to consumers and providers is extremely difficult. While ACO’s have been touted as a step towards trying to manage the
population’s health, the current proposed regulations will make it very difficult for providers to participate, with the risks great and the rewards small,” said John Matessino,” president and CEO of the Louisiana Hospital Association.

“Through the ACO, we have the opportunity of putting providers back into the role of creating some solutions to help deal with the overall cost and quality of care and the fragmentation of care. With the ACO, we also begin
to look at the appropriate utilization of scarce resources and access to those resources,” said Kevin Schoeplein, executive vice president, OSF Healthcare System.
What became abundantly clear during the roundtable session was that whether ACO models take hold or not, the theory of accountable care – using systematic efforts to improve quality and reduce costs across the organization by addressing key issues such as capacity, patient engagement, process improvement and physician alignment – is essential for the survival of any healthcare organization in the future.
Further illustrating the points to the left, the Amerinet survey asked member executives to identify their top priorities over the next two years (2011 and 2012). Their most frequent responses included:
• Meaningful use – 43 percent• Physician alignment – 26 percent• Quality – 22 percent• Cost containment – 18 percent
Other pressing issues included possible facility expansion, evaluation of service lines and physician recruitment. Among the highest impact healthcare trends identified were reimbursement cuts and episode of care/bundled payment options. The biggest drivers of healthcare costs centered on labor costs, overutilization of services and government laws.
Amerinet | page 3
Overall do you view the ACO as...
9 (14%)11 (17%)
42 (67%)
1 (2%)
50
Not positive at all
Somewhat negative
Somewhat positive
Very positive
40
30
20
10
0
How extensively has your organization (and collaborating payers and providers)
considered implementing an ACO?
11 (18%)
1 (2%)
50
Planning for potential
implementation
Currently exploring
Currently implementing
40
30
20
10
0
49 (80%)
Chart data from Amerinet Survey

page 4 | Executive Briefing
Choice A is the “do nothing” approach. It means that there will be no payment reform and costs will continue to grow from 10-16 percent of GDP (twice the rate in other developed countries, with equivalent or better outcomes), eventually spiraling up to 30 percent of GDP. The result will be a bankrupt economy.
Choice B shows that there will be limited reform that includes expanded coverage with no way to pay for it. This will result in slashed reimbursements and financial losses on every patient. The industry will react to these changes by getting more efficient and seeking out the procedures where reimbursement is profitable. Healthcare will survive, but on life support with almost no financial flexibility.
Choice C is to reinvent the care model entirely. This includes understanding unwarranted variation in supply sensitive care to identify and eliminate waste; implementing shared decision making for patient-centered care; using comparative effectiveness research to identify and increase the use of effective care; dramatically increase the quality of care as measured by patient reported outcomes; and increase employee and patient satisfaction along the way.
“Choice C is really about transforming the care model. We want to improve the quality of care, reduce unwarranted variation and control costs. This is the heart of the accountable care concept. Of all possible solutions, Choice C offers
the most comprehensive approach to addressing our national priorities, as well as the economic trends and cost drivers,” said Craig Westling, M.S., M.P.H., managing director of Accountable Care and of the Office of Professional Education and Outreach at The Dartmouth Institute for Health Policy and Clinical Practice. “We don’t think that ACOs are the only solution – other innovative models emerge, too. But all the models will address the same core issues, and will ultimately result in ‘accountable care.’”
This new approach would feature providers driving care improvement through:
• Care coordination
• Shared risk and rewards for cost and quality outcomes
• Transparent reporting of metrics, ensuring a continuous focus on improvement
• Freedom of beneficiary choice, so patients will be free to seek care from any provider
Echoed Mina Ubbing, president and CEO, Fairfield Medical Center, “I think that the ACO has the very high potential of putting the patient back into the equation. We’re managing every other aspect through legislation and so on.
And even though there’s certainly a lot of legislative risks with healthcare reform and specifically ACOs, it still gives us a chance to make sure that the providers are doing the right things for their patients.”
With this in mind, TDI offered three possible scenarios for the future of healthcare:
Choice CChoice A Choice B
The care model remains unchanged and costs continue
to spiral
Coverage expands, the care model evolves, and reimbursements
are slashed
The care model is transformed, quality improves, unwarranted
variation is addressed, and cost is controlled

Amerinet | page 5
What is an ACO?On March 31, 2011, The Department of Health and Human Services (HHS) released for public comment the long-awaited proposed rules governing accountable care organizations. In a fact sheet accompanying the 413 page document, HHS said,“ACOs create incentives for healthcare providers to work together to treat an individual patient across care settings – including doctor’s offices, hospitals and long-term care facilities. The Medicare Shared Savings Program will reward ACOs that lower growth in healthcare costs while meeting performance standards on quality of care and putting patients first. Patient and provider participation in an ACO is purely voluntary.”
Further detailing the rationale behind ACOs, HHS said, “Today, more than half of Medicare beneficiaries have five or more chronic conditions such as diabetes, arthritis, hypertension and kidney disease. These patients often receive care from multiple physicians. A failure to coordinate care can often lead to patients not getting the care they need, receiving duplicative care and being at an increased risk of suffering medical errors. On average, each year, one in seven Medicare patients admitted to a hospital has been subject to a harmful medical mistake in the course of their care. And nearly one in five Medicare patients discharged from the hospital is readmitted within 30 days – a readmission many patients could have avoided if their care outside of the hospital had been aggressive and better coordinated.”
Improving coordination and communication among physicians and other providers and suppliers through ACOs will help improve the care Medicare beneficiaries receive, while also helping lower costs. According to the analysis of the proposed regulation for ACOs, Medicare could potentially save as much as $960 million over three years.
Several characteristics that will be essential for all ACOs:
• Managing the continuum of care for patients as a real or virtually integrated delivery system
• Being of sufficient size to support comprehensive performance measurement and expenditure projections
• Having the capability of internally distributing shared savings and prospectively planning budgets and resource needs
“As we move forward in terms of who the ACOs are, two things are really important: (1) Physician involvement, and (2) being community based. I know a lot of organizations are trying to pre-position themselves just because of who
they are. So they might say, ‘We are the insurance company,’ ‘we are the hospital,’ ‘we are the physician group.’ And actually, what it’s going to require, I think, is an inclusiveness of all those parties to make it happen,” said Larry A. Mullins, president and CEO, Samaritan Health Services.
Westling echoed those thoughts by adding, “CMS is not going to let anybody just repackage what they’re doing and call it an ACO. You’ve got to really show that you’re transforming care.”
There are several key elements associated with accountable care models:
Local Accountability • Fostering provider accountability for quality and per
capita cost for patient population
Standardized Performance Measurement • Increasing accountability on the part of providers should
be accompanied by improved incentives and information for consumers
Payment Reform • Transitioning payments from rewarding volume/intensity
to increasing value
• Restructuring payments to encourage collaboration and shared responsibility among providers and consistent incentives from payers

Dr. William Weeks, associate professor of Psychiatry and of Community and Family Medicine at Dartmouth Medical School and associate professor and course director at TDI, explained a key area of the local accountability concept
will be a firm grasp of local healthcare utilization patterns. “First we have to understand, Who are the patients? Who is it we’re talking about? And then we have to understand, What are their utilization patterns? And then we have to provide higher value by altering the processes, structures and outcomes of the care we provide.”
Continued Craig Westling, “Local accountability is why the concept of ACOs has bipartisan support. Ultimately it’s about figuring out what works in your town. A key thing here is standardized performance measurement around quality and cost. CMS needs to create some level of standardized, transparent metrics so we can compare programs across the country.”
The ACO model establishes a spending benchmark based on expected spending. If an ACO can improve quality while
slowing spending growth, it receives shared savings from the payers. ACO-specific expenditure benchmarks will be based on historical trends and adjusted for patient mix. Contingent on meeting designated quality thresholds, ACOs with expenditures below their particular benchmark will be eligible for shared savings payments, which can be distributed among the providers within the ACO. These shared savings allow for investments – in health IT or medical homes, for example – that can in turn improve care and slow cost growth.
The ACO model is addressing payment reform by moving away from volume into increasing value. “The movement toward collaboration carries a lot of risks, but it’s actually the only way that this will work,” said Westling. “The idea is to improve the value of care delivered. And I think it’s an important distinction. There’s obviously a lot of lingering bitterness toward managed care and HMOs in the past because too many decisions were based on cost. In ACOs, the quality piece is just as important as the cost piece. If you don’t meet your quality metrics, you’re not going to reap major savings.”
Time
How Do “Shared Savings” Models Work?Initial shared savings derived from spending below benchmarks
ACO Launch
Actual Spending
Projected SpendingSpending Benchmark
Shared Savings
Spen
ding
page 6 | Executive Briefing
}
Model data courtesy of The Dartmouth Institute
Clearly, healthcare IT will be one of the foundational building blocks of accountable care. This is true from a coordination of care and ease of information sharing perspective, and also in the sense of using data to maximize results. Leveraging technology for business intelligence and modeling to predict use patterns will be important to proactively manage continuums of care.
“Without the data, we can’t get the information we need to manage care,” said Westling. “We need the ability to know our
community so we can assess risk and prevent illness before we see it in an acute setting.”
“In terms of processes, there must be improved care coordination to reduce variation and waste. Up to 60 percent of the CMS spending goes towards chronic care. Overall, we’re trying to reduce waste … and a primary driver of costs is redundancy, so part of that coordination of care is eliminating unwarranted variation and providing the right care at the right place at the right time, every time,” continued Westling.
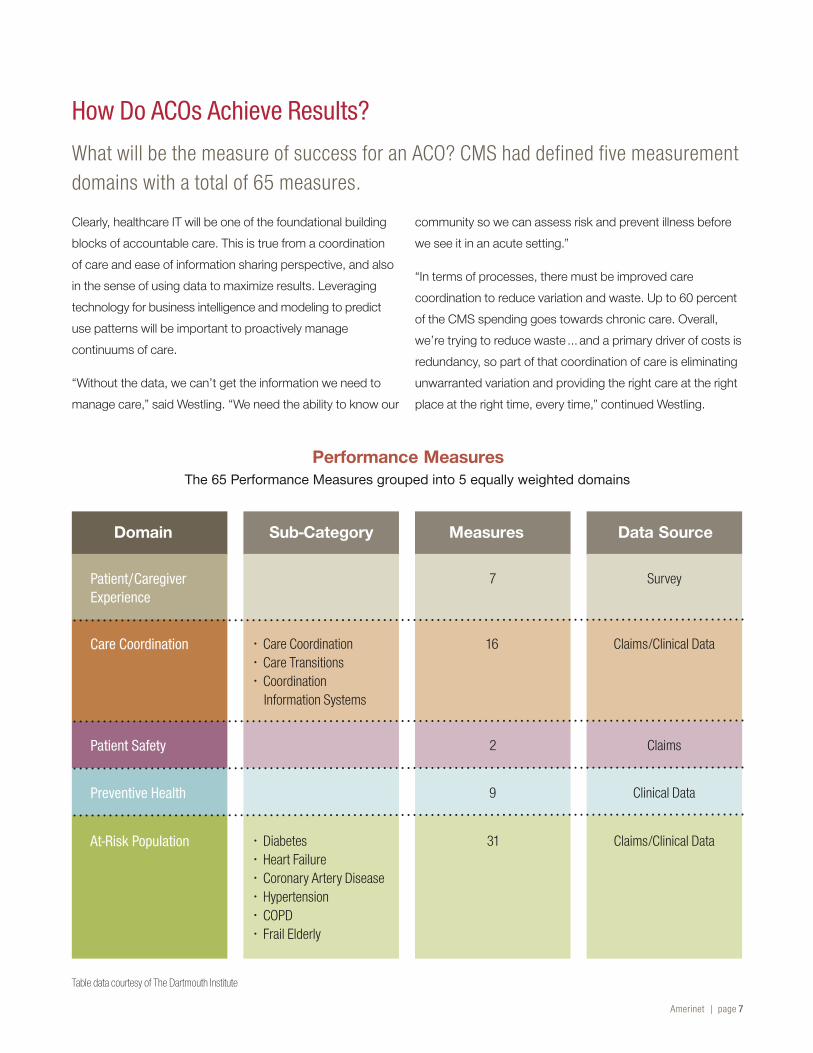
Performance MeasuresThe 65 Performance Measures grouped into 5 equally weighted domains
Table data courtesy of The Dartmouth Institute
How Do ACOs Achieve Results?What will be the measure of success for an ACO? CMS had defined five measurement domains with a total of 65 measures.
Amerinet | page 7
Domain Sub-Category Measures Data Source
Patient/Caregiver Experience
Patient Safety
Preventive Health
Care Coordination
At-Risk Population
• Care Coordination • Care Transitions • Coordination
Information Systems
• Diabetes • Heart Failure • Coronary Artery Disease • Hypertension • COPD • Frail Elderly
7
2
9
16
31
Survey
Claims
Clinical Data
Claims/Clinical Data
Claims/Clinical Data

page 8 | Executive Briefing
Next, organizations can start working on the following activities, even with current resources:
Statistical Analysis – Assessing utilization patterns to find best practices and address supply-sensitive care.
Shared Decision Making – Helping patients make informed, evidence-based choices about preference-sensitive care.
Microsystem Strategies – Improving clinical quality and to increase utilization of effective care.
Comprehensive Care Centers – Improving coordination of care, support the efficient use of healthcare resources.
Statistical AnalysisAccording to the Dartmouth Atlas, supply-sensitive care refers to services where the supply of a specific resource has a major influence on utilization rates. The frequency of use of supply-sensitive care is largely due to differences in local capacity, and a payment system that ensures that existing capacity remains fully deployed. Simply put, in regions where there are more hospital beds per capita, patients will be more likely to be admitted to the hospital. In regions where there are more intensive care unit beds, more patients will be cared for in the ICU. More specialists will result in more visits to specialists.
In regions where there are relatively fewer medical resources, patients get less care; however, there is no evidence that these patients are worse off than their counterparts in high-resourced, high-spending regions. Patients do not experience improved survival or better quality of life if they live in regions with more care. In fact, the care they receive appears to be worse.
What You Can Work on Right NowWhether or not healthcare organizations take the leap into joining or becoming an ACO, there are several things that any size and type of healthcare organization can do to prepare themselves for success in the upcoming era of value-based payment reform. Healthcare facilities must take a critical look at their operations in terms of the following areas:
Leadership4 Administrative leaders4 Clinical leaders
Partnerships4 Payers4 Community-based
organizations
4 Provider groups
Processes4 Improved care
coordination
4 Chronic disease management
4 Point of care reminders4 Reduced waste
Patients4 Informed patient choices4 Health risk assessments
Physicians4 Aligned incentives4 Access to timely data
Information Technology4 Ability to support
ACO operations
Capacity4 Appropriate workforce
4 Reduction/conversion of current capacity
4 Health information technology

Amerinet | page 9
They report being less satisfied with their care than patients in regions that spend less, and having more trouble getting in to see their physicians.
Most studies have found that mortality is no better in high-spending regions, almost certainly because the benefits to some patients are counterbalanced by the harms to others. Hospitals can be dangerous places, where patients face the risk of medical error, adverse events and hospital-acquired antibiotic-resistant infections. As more physicians get involved in a patient’s care, it becomes less and less clear who is responsible, and miscommunication and mistakes become more likely. Greater use of diagnostic tests increases the risk of finding – and being treated for – abnormalities that are unlikely to have caused the patient any problem. Patients who receive care for conditions that would have never caused a problem can only experience the risk of the intervention.
Supply-sensitive care also accounts for more than half of all Medicare spending. Understanding the problem of supply-sensitive care is a critical first step toward improving the quality and affordability of healthcare, building organized delivery systems and scaling back costs and cost growth.
Shared Decision MakingShared decision making is the collaboration between patients and caregivers to come to an agreement about a healthcare decision. It is especially useful when there is no clear “best” treatment option.
The caregiver offers the patient information that will help him or her:• Understand the likely outcomes of various options
• Think about what is personally important about the risks and benefits of each option
• Participate in decisions about medical care
“This is probably the most important thing when it comes to the right thing to do. This is where it’s not just informed consent, this is where patients are understanding what their options are, and what the consequences of each decision
might be. And then, making a fully-informed decision that is aligned with their values. Patients are then invested in their decisions and in the care that they receive. That is treating the patient in the right way. Doing this kind of thing is what’s going to make everything else flow better,” explained Westling.
Microsystem StrategiesA microsystem in healthcare delivery can be defined as a small group of people who work together on a regular basis to provide care to discrete subpopulations including the patients. It has clinical and business aims, linked processes, shared information environment and produces performance outcomes. They evolve over time and are (often) embedded in larger organizations. As a type of complex adaptive system, they must do the work, meet staff needs and maintain themselves as a clinical unit.
Clinical microsystems are the front-line units that provide most healthcare to most people. They are the places where patients, families and care teams meet. Microsystems also include support staff, processes, technology and recurring patterns of information, behavior and results. Central to every clinical microsystem is the patient.
The microsystem is the place where:• Care is made
• Quality, safety, reliability, efficiency and innovation are made
• Staff morale and patient satisfaction are made
Microsystems are the building blocks that form hospitals and clinics. The quality of care can be no better than the quality produced by the small systems that come together to provide care.
All healthcare professionals – and we believe all front-line clinical and support staff are professionals – have two jobs: Job 1 is to provide care. Job 2 is to improve care.

page 10 | Executive Briefing
Microsystem Strategies (continued) Finding time to improve care can be difficult, but the only way to improve and maintain quality, safety, efficiency and flexibility is by blending analysis, change, measuring and redesigning into the regular patterns and the daily habits of front-line clinicians and staff. Absent the intelligent and dedicated improvement work by all staff in all units, the quality, efficiency and pride in work will not be made nor sustained.
Explained Westling, “You don’t have to get super-fancy or complicated with any performance improvement methodology. People need just a fundamental understanding of the concepts. For instance, if someone says ‘most of the time,’ what does that mean? Does it mean 51 percent? 96 percent? Or when looking at variation, people need to understand when to intervene in a process. What kind of variation is just normal in this process? Don’t intervene until you have an outlier that indicates a real issue. Because sometimes the most damaging thing you can do is tamper with something that doesn’t need an intervention. That potentially creates a whole new slew of problems. The bottom line is that it’s really important to use a common language throughout an organization, and to make it easy to understand.”
Dr. Charles Sorenson, president and CEO, Intermountain Healthcare, offered, “Something that’s given us significant traction in quality improvement over the past 12 or so years is our extended senior management team having
accountability to our board for the accomplishment of specific goals in clinical quality improvement, along with the other goals set by the board. It’s no longer just the doctor’s job, or the chief nursing officer’s job or somebody else’s job. Reviewing those goals is one of the first things we do when we meet with our regional operators – not just review the finance or the building program, but ask, ‘Where are you in your clinical quality, your patient safety goals?’ And that has helped also in terms of our alignment with physicians, because I’ve always felt that the most important component
of learning with physicians has to be a shared understanding of our outcomes, and how we can improve them.”
Comprehensive Care Centers “The idea behind comprehensive care centers is that you’re putting the patient at the center through the entire continuum of care, from education in the community, tools for the primary care providers, to help the patients make informed decisions. And then if the decision is made to have surgery, it’s really well-coordinated throughout the hospital and follow-up. Medical home is a similar concept built around the primary care physician as care coordinator,” said Westling.
The medical home concept is one in which patients are cared for by a primary care physician who leads the medical team coordinating all aspects of preventive, acute and chronic needs of patients.
The American Academy of Pediatrics (AAP) introduced the medical home concept in 1967. In 2007, the AAP, American Academy of Family Physicians, American College of Physicians and American Osteopathic Association released the Joint Principles of the Patient-Centered Medical Home. Among the main principles listed were:
Physician directed medical practice – The personal physician leads a team of individuals at the practice level who collectively take responsibility for the ongoing care of patients.
Whole person orientation – The personal physician is responsible for providing for all the patient’s healthcare needs for all stages of life and taking responsibility for appropriately arranging care with other qualified providers.
Care is coordinated and/or integrated across all elements of the healthcare system and the community, care is facilitated by registries, information technology, health information exchange and other means to assure that patients get the indicated care when and where they need and want it in a culturally and linguistically appropriate manner.

A Best Practice – Center for Shared Decision Making
The Center for Shared Decision Making at Dartmouth-Hitchcock is the first patient-focused facility of its kind in the United States.
Counselors help patients make informed decisions about healthcare treatment choices. Support services include:
• One-On-One Counseling Sessions
• Decision Aid Library of helpful videotapes, audiotapes, booklets, CD-ROMs and websites
• Healthcare Decision Guide worksheet to help patients work through decisions with guidance or on their own
Their mission:
• To provide an excellent support service that fosters shared decision making between patients and healthcare providers
• To characterize the ways in which decision support and aids are most helpful for patients, providers, the healthcare institution, insurers and the community
• To document the life of the Center as the prototype of a dedicated decision support service for other healthcare entities worldwide
For more information on the Center for Shared Decision Making, contact Craig Westling at [email protected].
Amerinet | page 11
Quality and safety are rooted in:• Evidence-based medicine and clinical decision-support
tools guide decision making
• Accountability for continuous quality improvement through performance measurement and improvement
• Active participation by the patient in decision-making
• Utilization of information technology support optimal patient care, performance measurement, patient education and enhanced communication
Enhanced access to care is available through systems such as open scheduling and expanded hours.
“The medical home model is one of the pilot projects that’s out there right now to actually enroll the most at-risk populations to see how effectively they can be managed, and what the cost of care is,” said Dr. Larry Mullins, president and CEO of Samaritan Health, whose organization recently undertook a pilot project in the development of a medical home concept. “In our case, we took the highest cost population we could find. Because we thought if we’re going to make a difference anywhere let’s start with that.”
Regardless of an organization’s urgency in exploring the possibilities of ACO participation, there are a number of things they can do to assess their actual readiness.
“From an organizational perspective you need to think about who is going to be on the leadership team. And you need to think about who’s participating: which physicians are participating, which practices are participating, which payers will be your best partners,” said Westling.
In addition to executive leadership, the involvement and buy-in of physicians is key. The new model must promote physician engagement at every level. Clinical and executive leadership must demonstrate they have a shared mission and vision or success of the accountability model. These objectives must also include programs of compensation and incentives that are viable internally among providers, but also must be aligned among all payers.

page 12 | Executive Briefing
Comprehensive Care Centers (continued) “Involvement in the quality improvement process is a great satisfier for most doctors. They no longer have to rely on how much money they make to figure out whether they’re being successful, but can see on objective indicators that they are accomplishing results for their patients that are on a level of the very best reported any place in the world. And that brings a whole lot of professional satisfaction. I think that becomes an important way to inspire and retain good clinical people,” said Sorenson.
The results of the Amerinet survey bear out some of the basics that must be in place. More than 44 percent of respondents said that they had implemented a leadership and management structure that included clinical and administrative systems.
In terms of infrastructure, a high number of respondents (59 percent) were reporting on quality and 37 percent were reporting on cost measures. A relatively high number had also implemented processes to promote evidence-based medicine.
Where respondents seem to be lagging is in the area of care coordination (only 11 percent reported the ability to produce patient-centered care reports) and the structure for payments for shared savings distribution (17 percent).
For many Amerinet members in the rural healthcare setting, many questions still linger and may as of yet be unresolved. “I’m concerned we’re talking about too many physicians in populated areas. Well, I’m in a rural area. I can’t attract
a physician to the rural area. Where are small hospitals, the communities and the patients going to receive care?” asked Bob Miller, CEO of Coshocton Hospital.
Indeed, some of the challenges facing smaller, less integrated providers include the degree to which potentially burdensome requirements for participation are phased in or modified for rural or less integrated ACOs and how bonuses and performance thresholds are structured to encourage participation by less well-established provider groups (e.g. rural providers, FQHCs, RHCs).
Which of the following stipulations for ACOs (listed by CMS) does your organization currently have in place?
19 (30%)
11 (17%)
4 (6%)
28 (44%)
25 (40%) 23 (37%)
7 (11%)
Minimum of 5,000 Medicare
beneficiaries required per ACO
At least three years
of participation
Leadership and management
structure that includes clinical and
administrative systems
Processes to promote
evidence-based medicine
Report on cost measures
Requirement to produce
reports demonstrating
the adoption of patient
centered care
Report on quality
A formal legal structure to receive and distribute
shared savings to
participating providers
40
30
20
10
0
37 (59%)
Chart data from Amerinet Survey

Providing a bridge to help fund
“the right way” to provide care
A final statement by one of the meeting participants may sum up the current situation best.
“Just as we bring this to a close, I think all of us who have been in the business for a long time have gone through a lot of iterations of healthcare reform. About every 10 years we have healthcare reform. I think the beauty of what we’re seeing now is – we talked all day long about collaboration – the fact that we now have a lightning rod that is forcing us all to focus on some key issues. And collaboration is going to occur.”
What Now…So what are providers to do at this point? Should they jump in with both feet, slowly test the waters or ignore it and hope it goes away? History shows that when Medicare funds a program, it often has a significant impact on care delivery and provider focus. The idea of accountable care seems to be the latest example.
A strong emphasis on quality
and coordinated care, with integration of
community resources
Leveraging technology and using predictive modeling to identify high risk
individuals
Enhancing transparency
measures
At its core, the concept, although idealistic, is grounded in goals and objectives that are keys to future success in healthcare:
Amerinet | page 13
Although, because of consolidation and collaboration, capacity will shrink and some providers may be closed or absorbed by other entities, some see promise for rural providers.
“Rural areas do have better outcomes with fewer resources,” said Weeks. “I think where they might have a bit of an
advantage is that they have been providing higher value care for a pretty long time. So if I’m a company and I want to increase my earnings per share, I buy a company that’s got better earnings per share than me. If I’m a provider and I want to get greater cost shared savings I might buy or affiliate with someone that’s got lower costs overall and better outcomes.”

Amerinet serves acute and non-acute care providers nationwide.Amerinet Customer Service: 877-711-5600 | [email protected] | www.amerinet-gpo.com
© 2011 Amerinet, Inc. This Executive Briefing is the property of Amerinet, except where noted. Permission is required to copy, download or use any text, photographs or image files.
Reducing healthcare costs. Improving healthcare quality.