Health Service Provision José Ruales Regional Advisor in Health Systems PAHO/WHO.
31
Health Service Provision José Ruales Regional Advisor in Health Systems PAHO/WHO
-
Upload
rosalyn-stafford -
Category
Documents
-
view
220 -
download
1
Transcript of Health Service Provision José Ruales Regional Advisor in Health Systems PAHO/WHO.

Health Service ProvisionJosé RualesRegional Advisor in Health SystemsPAHO/WHO

Functions and Objectives of the Health System
Health System
Values
Needs
Resources
StewardshipFinancing
Insurance
Provision
Maintain and improve health
Access – Quality - Efficiency
Protect financial risks
Satisfaction of expectations
Participation

Health Services: Definition
• Services delivered by health personnel in a direct manner, or by other people under the supervision of these personnel, with the goal of:
– Promoting, maintaining and/or recovering health
– Minimizing disparities both in access to health services and in the level of population health
(PAHO/WHO 2003; Modification of the IOM 1996)

Health Service Provision
•Public or Collective Health Services
– Disease prevention and control–Protection against environmental risks–Injury prevention–Promotion of healthy behaviors and mental health–Quality assurance and accessibility of health services
•Individual or Personal Health Services
–Individual prevention–Diagnosis–Recovery –Rehabilitation–Palliative care

Challenges for Health Services in the Americas
• Access to health services is not available for large segments of the population,
• The supply of health services does not always adjust to expectations, social values and cultural preferences,
• The provision of health services, for certain population groups, is of poor effectiveness and technical quality,
• There is fragmentation, duplication, concentration in urban areas, weak information and referral systems, with inefficiency and inequity in the supply.

Health Services in Social Protection Schemes
• 7/7 aim to extend coverage and increase access by reducing exclusion and economic barriers
• 4/7 increased equity in terms of access and use, but 3/7 increased inequity
• 2/7 the elimination of economic barriers was insufficient among the dispersed and indigenous populations
• 3/7 increased the demand without expanding the supply of resources or the infrastructure, which leads to overload and reduction of quality

Needs, expectations, demand and use of health services by people, families and communities
Response
Model ofcare
Model oforganization &management
Challenge
Other systemicvariablesthat are determinantsof health services
SUPPLY
DEMAND
AC
CES
S

• Concrete existence of services aimed at promoting, preventing, recovering and rehabilitating the target population’s health, both at the individual and collective level, under the conditions of the people and the environment.
• Human Resources
• Physical Resources
• Technological Resources
Health Service Supply

Health Service Demand
– Formal (explicit) requirements for health services.
– Utilization: Demand that is met through the supply of services to a target population in a specific time period.
– Access: Probability of obtaining health care when needed.

Comprehensive access
• Conditions of effective coverage:– Availability– Elimination of barriers (geographic, cultural,
economic and social)– Timeliness (moment and time)– Acceptability (satisfaction and respect)– Contact and real use (first contact or other)– Appropriate, effective services (procedures and
levels)• Ex. Maternal-Newborn Care: Contraceptives, Skilled
delivery care, Emergency obstetric and newborn care
– Based on social protection

Social Protection - Adequate access:
– Timeliness– Quality– Dignity
– Independent of ability to pay
– Includes•Health service coverage•Coverage for the entire population•Financial solidarity

Determinants of Access
• Prior to using health services:– The need for care should exist
• (pain, convincing, risk of death)
– Should believe in services’ efficacy
• (confidence in the provider)
– Should have the ability to access services
• (availability of income or insurance, time, transport)
Source: Restrepo, JH, 2006

Barriers to access: supply side
At the entranceAt the entrance Initial contact:•Travel time•Means of transport•Distance to service•Hours of operation
InsideInside Obtaining the service•Bureaucracy for the appointment•Waiting times
At the exitAt the exit Continuity•Regular source•Hours
Source: Restrepo, JH, 2006

Barriers to access: demand sidePredisposition •Demographic
•Social structure•Culture, ethnicity and religion
Ability Resources for demanding services:Income or Health Insurance, Recognition of Rights
Needs Illness episodes or preventive actions, which in their opinion warrant health care
Utilization Characteristics of the resources themselves:•Type of service, Purpose, Concentration
Satisfaction Provider perceptions:•Information and attitude of professionals, Length of doctor’s visit•Quality of waiting rooms, Size of exam rooms, Waiting times•Cure / Solution
Source: Restrepo, JH, 2006

Factors that influence access
Provision / Use of
Services
Socio-economic development
Health situation Health needs and care
Socio-cultural aspects
Geographic, environ-mental, road access
Resources, organization and management of services
Social protection in health
Policies, plans and resources related to health
Biological – demographic characteristics
Cultural access
Geographic access
Economic access

Social determinants of health
Need for health
Perceived
Unperceived
Expressed
Unmet
Repressed Access
How the factors interact
Demand for health
Met
Equitable
Inequitable
Social protection in health scheme
Health outcomes
Supply of Services

Health Care Model
• Content of health care and principal characteristics of the interaction between the service provider and service user.
• Includes:• Pertinence of the supply of services
to users’ needs and demands,• Accessibility and acceptability of
services,• Services oriented to people, families
and communities,• Role of people, families and the
community in self-care,• Level of integration of services.

Trends in the model of care
• Balance between personal services and public health services; curative, promotion and prevention services
• Services oriented to families and the community
• Promotion of self-care for the health of people, families and the community
• Search for the integrality of services:
– Comprehensive– Continuous– Longitudinal

Model of organization and management
• The manner in which the components of the health system are organized and managed with the goal of achieving the objectives proposed and facilitating its collective function.

Trends in the models of organization and
management• Organization of services based on
primary care• Definition of a population base• Prioritization of the most vulnerable
population groups• Emphasis on ambulatory care and
care beyond traditional clinical environments
• Decentralization of services• Management focused on quality and
results• Organization and management of
integrated health systems

Fragmentation
• Coexistence of many units or entities that are not integrated into the health service network.
• does not allow the standardization of contents, quality, cost and provision
• leads to providers not working in a coordinated or synergetic manner
• generates increases in the costs of care
• promotes inefficient allocation of resources in the system.

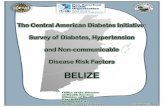
Segmentation of the system and Fragmentation of services
Tertiary Care
Primary Care
Social Security
Private, high complexity
MOH Professional Risks
Private, low complexity
NGOs
Municipalities
Universities
Secondary Care
Traditional Medicine

STRATEGIES FOR CONFRONTING SEGMENTATION AND
FRAGMENTATION
INTER-INSTITUTIONAL COORDINATION
OPERATIONAL INTEGRATION
Strengthening of the STEWARDSHIP / MANAGEMENT
of the Sectoral Policy
Leadership, Alignment and Harmonization of International
Cooperation
• Management of Integrated Service
NETWORKS •Integration of the
Programs in the System

Integration of the Population
• Involves the availability and the timeliness of access
• Guarantees the flow of users through all levels of care and complexity in order to ensure the continuity of care,
• Develops referral and counter-referral mechanisms, between different health services and, when required, other social services.

INTEGRATED HEALTH SERVICE SYSTEM
• ESTABLISHMENT OF AN INTEGRATED NETWORK OF HEALTH CARE DELIVERY THAT
– ALLOWS THE PROVISION OF CONTINUOUS CARE TO A SPECIFIC POPULATION
– AT A SPECIFIC TIME AND PLACE AND WITH DEFINED COST AND QUALITY
– IS RESPONSIBLE FOR THE HEALTH AND ECONOMIC OUTCOMES OF THIS POPULATION.
Source: MENDES (2001)

COMPONENTS OF INTEGRATED HEALTH SERVICE SYSTEMS
• COLLABORATIVE MANAGEMENT OF CARE
• MANAGEMENT OF POPULATION RISKS
• MANAGEMENT OF POINTS OF HEALTH CARE DELIVERY
• CLINICAL MANAGEMENT
SOURCE: MENDES (2001)

Levels of construction of networks
Level Actions Value at play5th Floor
AssociateShare objectives and projects
Confidence
4th Floor
CooperateShare activities and/or resources
Solidarity
3rd Floor
CollaborateProvide intermittent help
Reciprocity
2nd Floor
Gain knowledgeKnowledge of what the other is or does
Interest
1st Floor
RecognizeRecognize that the other exists as a peer or collaborator
Acceptance
Source: Rovere, M. 2004

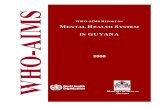
Organization and management of networked services
Segmentation of the resources, supply and population ORGANIZATION INTO
A NETWORK
PHC
Primary Care
Social Security
Private, high complexity
MOH Professional Risks
Private, low complexity
NGOs
Municipalities
Universities
Secondary Care
Traditional Medicine
Tertiary Care

HOSPITAL
DAY HOSPITAL
NURSING CENTER
HOME-BASED CARE
BASIC HEALTH
UNIT
SPECIALIZED AMBULATORY
CARE
HOSPITAL
DAY HOSPITAL
NURSING CENTER
HOME-BASED CARE
SPECIALIZED AMBULATORY
CARE
BASIC HEALTH
UNIT
HOSPITAL
A
AMBULA-TÓRY
B
AMBULA-TÓRY
A
HOSPITAL
B
From fragmentation to integration in a network
1
2
3
SOURCE: MENDES (2001)

From the INTEGRATION OF SOCIAL PROTECTION to INTER-SECTORAL
INTEGRATION
HEALTH SERVICE SYSTEM
SOCIAL PROTECTION
SYSTEM
HEALTH
CULTURESOCIAL PROTECTION
EDUCATION
HOUSING
EMPLOY-MENT
SOURCE: MENDES (2001)