Health Psychology Lecture 4 Health Behaviors. Lecture 4 - Outline Part 1 –Health Promoting...
60
Health Psychology Lecture 4 Health Behaviors
Transcript of Health Psychology Lecture 4 Health Behaviors. Lecture 4 - Outline Part 1 –Health Promoting...

Health Psychology
Lecture 4
Health Behaviors

Lecture 4 - Outline
• Part 1– Health Promoting Behavior– Diet– Exercise
• Part 2– Health Harming Behavior– Smoking– Alcohol
• Part 3– Self-Change (Goal setting theory and false hope syndrome)

Question
How strong is the link between behavior and health?
• Genetics = 20%
• Medical care = 10%
• Other factors = 30%
• Behavior = 40%
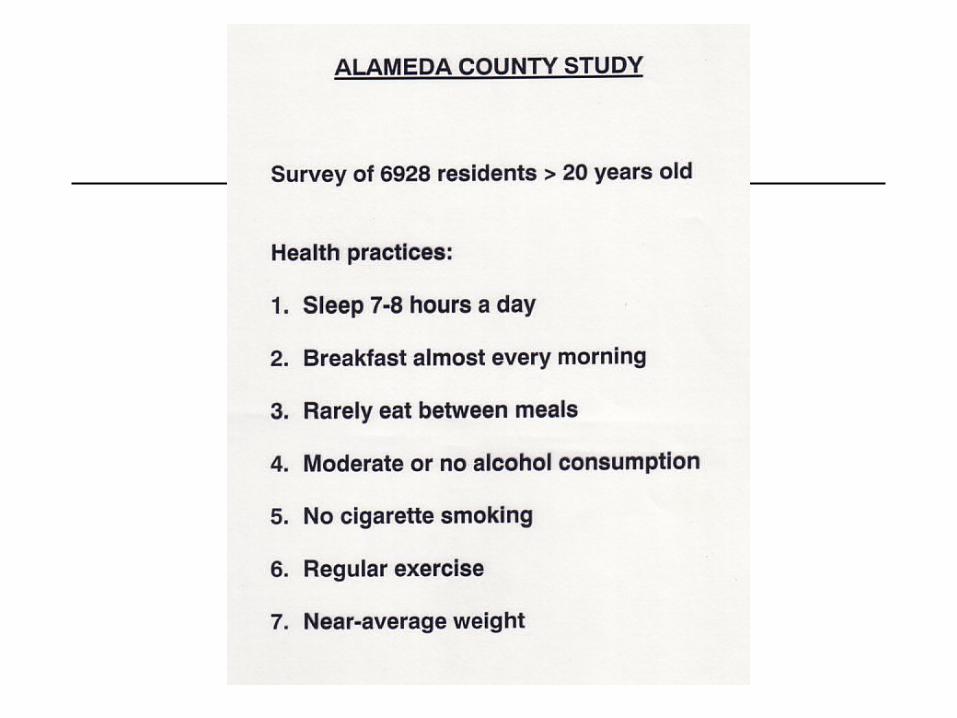
Kaplan et al (1993)
Health Behaviors
Behaviors which are related to the health status of the individual.
Divided into two types:1. Health-enhancing behaviors (“immunogens”)2. Health-harming behaviors (“pathogens”)


Barriers to good health behaviors
• Within medicine
• Within society
• Within individual– Early learning
– Delayed vs. immediate reward
– Unrealistic optimism
– Lack of motivation
– Health behaviors unrelated and unstable

Why unrelated and unstable?
• Health behaviors are acquired, elicited, and maintained by different factors for different people. These factors may change over time.

Health-Enhancing Behaviors
Behavioral Immunogens…
.
.
.
.
.
.
.

Health-Enhancing Behaviors
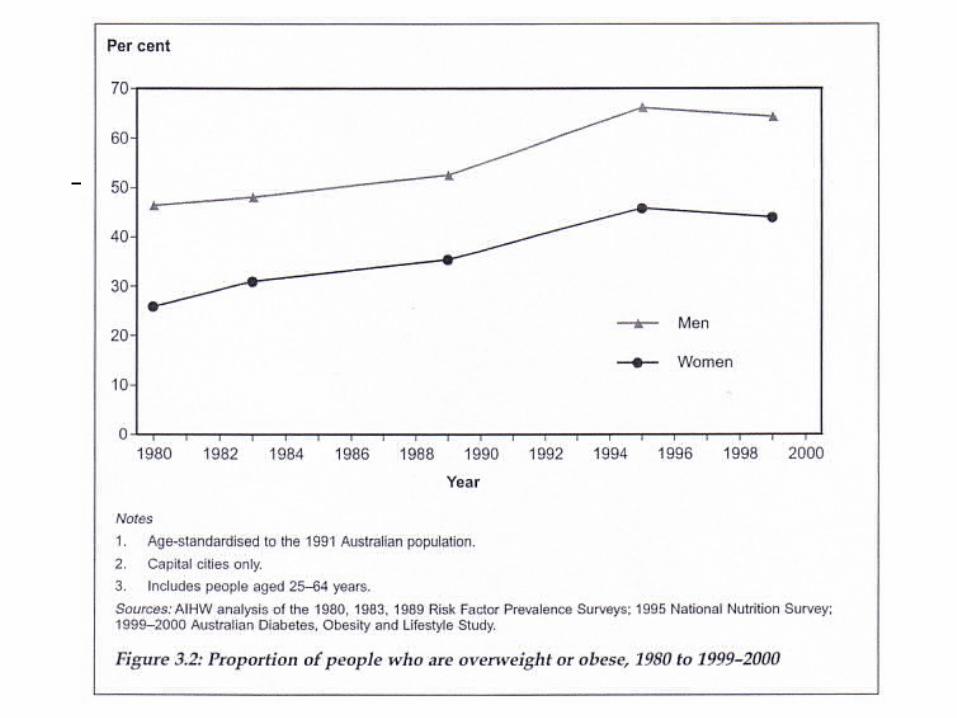
Diet…• Until 1940s, illness due to lack of food/nutrients• Now illness due to excess food/nutrients
• Current Western diet linked to:– Obesity– Heart disease– Diabetes– Osteoporosis– Cancer
Health-Enhancing Behaviors
Diet and Obesity– Body Mass Index (BMI)
– Weight (kgs) / Height (m)2
• 18.5-25 = normal
• 26-30 = overweight
• >30 = obese

Proportion of people with high blood cholesterol, 1999-2000.
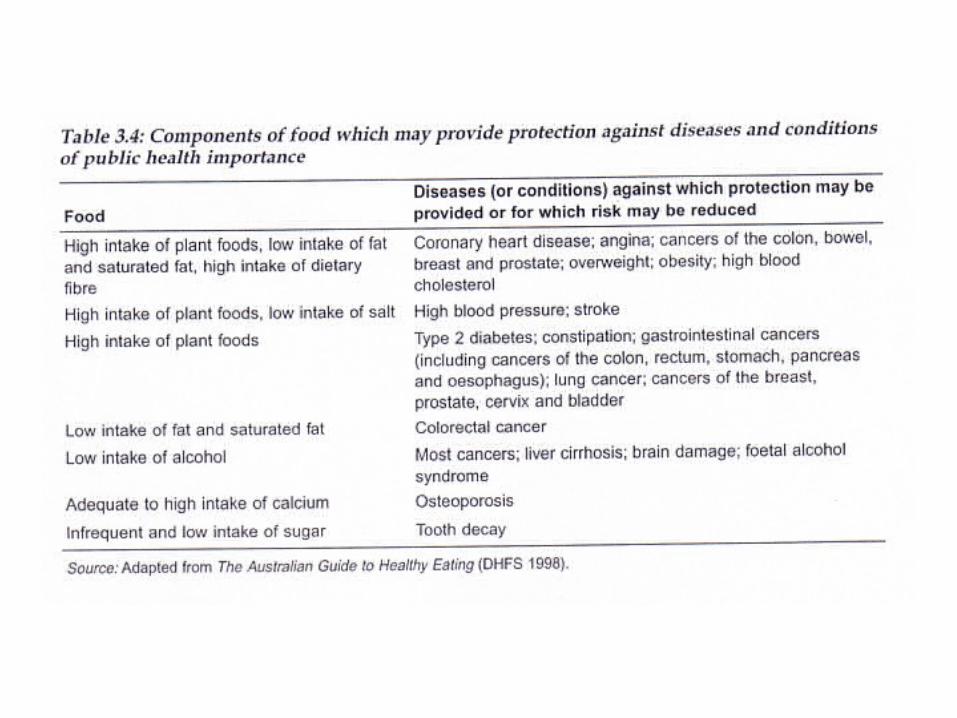

Diet and Cancer (?)

Dietary Change
Possible targets of intervention…
• Schools, e.g., psychoeducation
• Community, e.g., supermarkets, mass-media
• Individual, e.g., cognitive-behavioral
Dietary Change
Eat, Drink, and Be Healthy (Willet, 2003)
• Maintain a stable, healthy weight• Replace saturated and trans fats with unsaturated fats• Replace refined carbohydrates with whole-grain
carbohydrates• Choose healthier sources of protein by trading red meat for
nuts, beans, chicken, and fish.• Eat plenty of fruits and vegetables, but hold on the potatoes• Use alcohol in moderation (1 glass a day is good)• Take a multivitamin for insurance
Health-Enhancing Behavior
Aerobic Exercise…
• Exercise which requires 70% of maximum oxygen consumption
• Direct Benefits– Improve fitness, muscle strength, muscle endurance,
flexibility, cardiorespiratory fitness, weight control

American College of Sports Medicine
• Recommendations for Exercise– Type: Large muscle activity that is rhythmic
and repetitive (e.g., walking, running, swimming, cycling)
– Duration: At least 20 minutes continuously– Frequency: 3 to 4 times per week– Intensity: Vigorous (defined as at least 60 to
80% of maximal capacity)
Pale et al. (1995)
• Recommendations for Exercise– Every adult should accumulate 30 minutes of
moderate physical activity every day, or at least on most days.

Why Exercise?
• Western population sedentary. – Less than 10% of US population meet
recommendations for exercise (esp. 30+)– Physical inactivity ranks second to cigarette smoking in
burden of disease– Physical exercise can…
• promote fitness (regular, vigorous)• promote health (moderate, less vigorous)
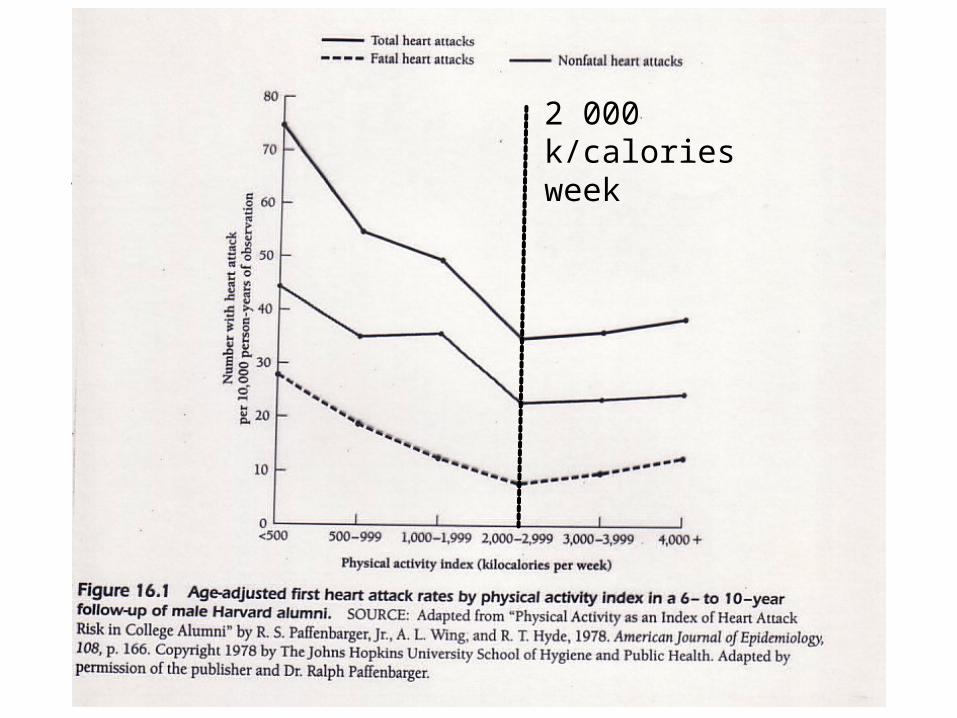
2 000 k/calories week

Benefits of Exercise
• Fitness• Physical health• Psychological wellbeing
– Decreased depression– Decreased state anxiety– Buffer against stress– Increased self-esteem

Drop out from Exercise
• Drop out rates– 50% in first 6 months– 20 in 3 years
• Why drop out?– Person variables– Social-environmental variables– Exercise program variables
• Behavioral programs best at promoting adherence

Health-Harming Behaviors
Behavioral Pathogens…
.
.
.
.
.
.
.

Health-Harming Behaviors
Deaths from Drugs
1. Tobacco 72%2. Alcohol 25%3. Opiate 2%4. Other illegal drugs 1%
Total 100%


Health Risks of Smoking
• Smoking is the greatest single cause of preventable deaths (> 20% of all deaths)
– Half of those who smoke throughout their life will die as a direct result of their habit
– Half of these deaths will occur in middle age with an average of 21 years of life lost
– The rest will occur in old age, with around 8 years lost
– Average reduction of life expectancy = 5-9 years

Health Risks of Smoking
• Smoking contributes to…
– Heart disease– Cancer– Stroke– Influenza and pneumonia
– Chronic bronchitis– Emphysema– Peptic ulcers– Respiratory disorders– Lower birth weight in offspring
– ** May have synergistic effects (Perkins, 1985) **
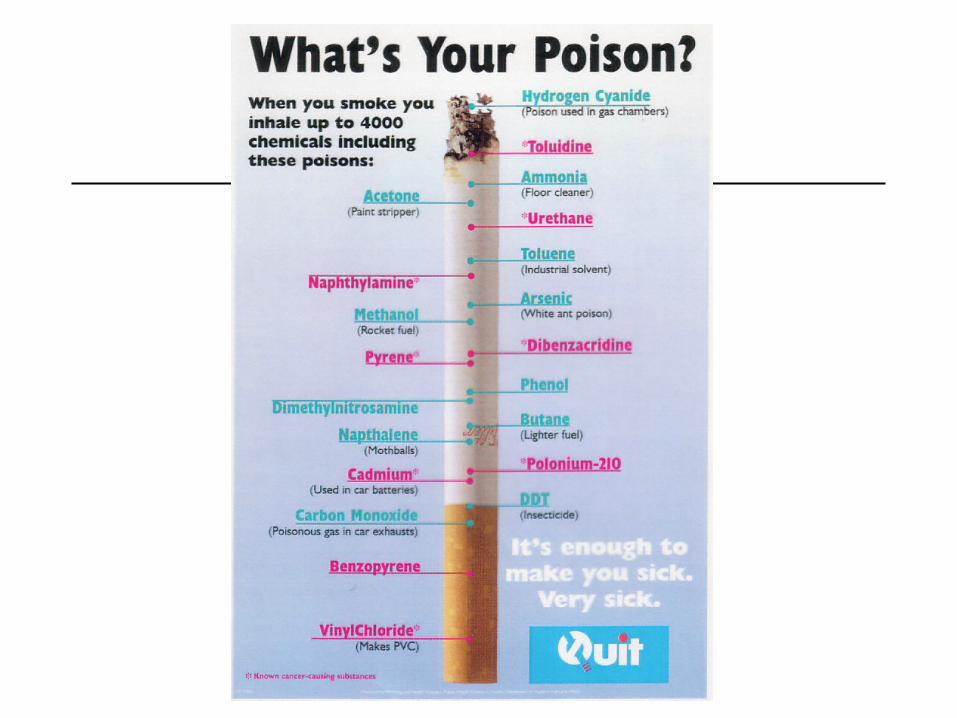
Components of Cigarette Smoke
• Nicotine– Primary addictive substance, pleasurable– Acts directly on CNS
• Tars– Chemicals which are carcinogenic
• Carbon Monoxide (CO)– CO reduced amount of O2 in blood and places strain on
heart muscle

Who smokes?
• About 25% (US, Canada, Australia, etc)– Men (28%), Women (23%), gap is narrowing
• Unemployed and less educated smoke more
• Smoking rates have decreased– Teenage girls’ levels decreased least

Proportion of people who are daily smokers (2001)

Proportion of people who are daily smokers
Why do people smoke?
• Start– Social learning (modeling)– Peer pressure
• 95% begin in teen years• Know smoking is dangerous but say will stop• Rule of thumb …
• Continue– Genetic (?) – Dependence (nicotine-regulation)– Reinforcement (peers, feeling good, performance)


Categories of Regular Smokers
• Positive affect smokers
• Negative affect smokers
• Habitual smokers
• Addictive smokers
stimuli affect smokers differently
(Tomkins, 1966)

Prevention of Smoking
• Public Health Measures
• Educational Programs
• Inoculation Programs

Quitting Smoking
• About 95% do so on their own– Easier for light smokers, motivated, social support,
persistent, self-efficacy
• Successful quitters tend to…– Quit cold turkey– Provide themselves with rewards– Use positive self-statements

Stages of Change
Trans-Theoretical Model (Prochaska & DiClemente)
1. .
2. .
3. .
4. .
5. .

Treatment Implications
Trans-Theoretical Model (Prochaska & DiClemente)
• Must intervene at the appropriate stage (ie action stage) for the intervention to be successful
• Relapse is common– Cycle through stages before successful termination of
target behavior


Treatments for Smoking
• Nicotine-replacement therapy
• Aversion therapies
• Self-management strategies
• Multi-modal approaches

Relapse
• Relapse rate = 70-80% after 1 year
• Factors– Abstinence-violation effect– Weight gain (2 pounds)– Social support– Intrinsic motivation (better than extrinsic)
– Stress
Good programs include relapse prevention

Health Risks of Alcohol?
• Alcohol abuse contributes to
– Some cancers– Motor vehicle and other accidents (users and bystanders)– Suicide– Cirrhosis of the liver– Brain damage (Korsakoff’s Syndrome)– Crime– Poor job performance and absenteeism– * side effects - mood and aggression *
“alcohol affects every organ in the body”


Who drinks?
• About 70% of adults drink alcohol at least occasionally– about 10% are ‘problem drinkers’ (health damage)– About 5% are ‘alcoholic’ (alcohol dependence)
• Two vulnerable times– Teenage years– Late middle age


Why do people drink?
• Start– Social learning (modeling)– Peer pressure
• Continue– Dependence– Reduce social anxiety– Tension relief– Reinforcement


Treatments for Alcohol Abuse
• Detoxification
• Alcoholics Anonymous
• Psychotherapy
• Aversion therapies

Health Behaviors
Theories of Self-Change
• Goal Setting Theory
• Expectancy-Value Theory (motivation to change)
• False Hope Syndrome
Goal-Setting Theory (Locke & Latham, 1990)
• Goals = performance targets
• Facilitate performance by:– motivate search for performance strategies & planning
– direct attention/effort towards task-relevant behaviors rather than unrelated activities
• Well-researched theory: tested using many different tasks, jobs, employees, etc

Basic Principles of Goal-Setting
Characteristics of effective goals:– specific, difficult goals result in higher performance than
general, do-your best, or no goals
– no difference between last 3 goal types on performance
Research has identified 6 key moderators of the relationship between specific, difficult goals and performance
• i.e,. Variables that affect the strength of this relationship
Moderator Variables
6 Key Moderator Variables1. Participative vs. Assigned Goals
2. Goal Commitment
3. Availability of Feedback
4. Individual Differences
5. Task Complexity
6. Group vs. Individual Goals

Expectancy-Value Theory
• 3 basic concepts: expectancy, instrumentality, valence– Expectancy (E) that effort will lead to successful change
– Instrumentality (I): strength of relationship between change and various outcomes (e.g., money, satisfaction, recognition from others)
– Valence (V): attractiveness / value attached to these outcomes
effort depends on expectancy that (a) effort will result in adequate self-change, and (b) that this self-change will result in valued/attractive outcomes

False-Hope Syndrome Model
Unrealistic Expectations (Amount, Speed, Ease,
Consequences)
Commitment to Change (Feelings of control)
Initial Efforts (Early successes)
Resistance to Change (Change stops)
Abandon Attempt (Failure)
Attributions for Failure (reasons for failure
can be corrected)
Recommitment to Goals (unrealistic expectations)

False-Hope Syndrome
Consequences of repeated failure - dieting– Physical health (weight fluctuations)– Psychological health (mood, fatigue, irritability)– Obsession with food (making weight loss difficult)
Is the theory overly pessimistic?– “can achieve anything if you work hard enough”– Overconfidence is at the heart of false-hope– Choose your goals wisely


















