
Handout ASHP CKD Slides 12.4 - ceconcepts.com ASHP CKD Slides 12.4... · 2 Trends in CKD Anemia...
39
1 Disclaimer • This slide deck in its original and unaltered format is for educational purposes and is current as of the date of the presentation. All materials contained herein reflect the views of the faculty, and not those of Creative Educational Concepts, Inc. or the commercial supporter(s). • Participants have an implied responsibility to use the newly acquired information to enhance patient outcomes and their own professional development. The information presented in this activity is not meant to serve as a guideline for specific patient management. • Any procedures, medications, or other courses of diagnosis or treatment discussed or suggested in this activity should not be used by clinicians without evaluation of their patient’s conditions and possible contraindications on dangers in use, review or any applicable manufacturer’s product information, and comparison with recommendations of other authorities. • Usage Rights: This slide deck is provided for educational purposes and individual slides may be used for personal, non‐commercial presentations only if the content and references remain unchanged. No part of this slide deck may be published or distributed in print or electronic format without prior written permission from Creative Educational Concepts, Inc. Additional terms and conditions may apply. CKD, chronic kidney disease. Learning Objectives • Appraise recent shifts in treatment patterns that have occurred in the management of anemia in CKD and the potential implications for patient care. • Examine the role of hepcidin in iron metabolism and its contribution to the pathophysiology of anemia of CKD. • Explore hypoxia‐inducible factor (HIF) as a treatment target in anemia of CKD and elucidate the potential role of investigational HIF prolyl hydroxylase (HIF‐PH) inhibitors in anemia management. • Analyze team‐based care of patients with CKD and methods to improve the recognition and safe management of anemia to improve patient quality of life. CKD, chronic kidney disease. 1 2
Transcript of Handout ASHP CKD Slides 12.4 - ceconcepts.com ASHP CKD Slides 12.4... · 2 Trends in CKD Anemia...

1
Disclaimer• This slide deck in its original and unaltered format is for educational purposes and is current as
of the date of the presentation. All materials contained herein reflect the views of the faculty, and not those of Creative Educational Concepts, Inc. or the commercial supporter(s).
• Participants have an implied responsibility to use the newly acquired information to enhance patient outcomes and their own professional development. The information presented in this activity is not meant to serve as a guideline for specific patient management.
• Any procedures, medications, or other courses of diagnosis or treatment discussed or suggested in this activity should not be used by clinicians without evaluation of their patient’s conditions and possible contraindications on dangers in use, review or any applicable manufacturer’s product information, and comparison with recommendations of other authorities.
• Usage Rights: This slide deck is provided for educational purposes and individual slides may be used for personal, non‐commercial presentations only if the content and references remain unchanged. No part of this slide deck may be published or distributed in print or electronic format without prior written permission from Creative Educational Concepts, Inc. Additional terms and conditions may apply.
CKD, chronic kidney disease.
Learning Objectives• Appraise recent shifts in treatment patterns that have occurred in the management of anemia in CKD and the potential implications for patient care.
• Examine the role of hepcidin in iron metabolism and its contribution to the pathophysiology of anemia of CKD.
• Explore hypoxia‐inducible factor (HIF) as a treatment target in anemia of CKD and elucidate the potential role of investigational HIF prolyl hydroxylase (HIF‐PH) inhibitors in anemia management.
• Analyze team‐based care of patients with CKD and methods to improve the recognition and safe management of anemia to improve patient quality of life.
CKD, chronic kidney disease.
1
2

2
Trends in CKD Anemia ManagementChanges in Hemoglobin Targets, Treatment
Approaches, and Targets of Therapy
Joanna Q. Hudson, PharmD, BCPS, FASN, FCCP, FNKFProfessor
The University of Tennessee Health Science CenterDepartment of Clinical Pharmacy and Translational Science
Department of Medicine (Nephrology)Memphis, Tennessee
Response to HypoxiaEPO Production and Erythropoiesis
Reduces O2levels in blood
Erythropoietin stimulates red bone marrow
Enhanced erythropoiesis increases RBC count
Normal blood oxygen levels Stimulus: Hypoxia due to decreased RBC count, decreased availability of O2 to blood, or increased tissue demands for O2
Kidney (and liver to a smaller extent) releases erythropoietin
Increases O2‐carrying ability of blood
RBC, red blood cell.
3
4

3
Normal Process of Red Blood Cell Production
00 2525212119191515
Time to Mature Cell Development (days)Time to Mature Cell Development (days)
Bone MarrowBone Marrow CirculationCirculation
Stem CellStem CellBurst Forming
UnitBurst Forming
UnitColony
Forming UnitColony
Forming Unit RBCRBC
Erythropoietin
ReticulocyteReticulocyte
Iron
Pro‐erythroblast
Pro‐erythroblast
Adapted from Brook JH. Iron Metabolism in Health and Disease. 1994.
Effect of CKD on Erythropoiesis
00 2525212119191515
Time to Mature Cell Development (days)Time to Mature Cell Development (days)
CirculationCirculation
Stem CellStem CellBurst Forming
UnitBurst Forming
UnitColony
Forming UnitColony
Forming Unit RBCRBC
Erythropoietin
ReticulocyteReticulocyte
Iron
Pro‐erythroblast
Pro‐erythroblast
Adapted from Brook JH. Iron Metabolism in Health and Disease. 1994.
Bone MarrowBone Marrow
5
6

4
● Iron deficiency (characterized as microcytic anemia)
● Primary cause of resistance to therapy for anemia of CKD!
● Result of reduced iron uptake and absorption
● Affected by changes in hepcidin
● Malnutrition
● Inflammatory conditions
● Secondary hyperparathyroidism
● Other disease states (eg, cancer, HIV)
Factors Contributing to Anemia of CKD
HIV, human immunodeficiency virus.
Iron recycled
200 mg per unit of
RBCs
Tissue
Gut
Loss 1 mg/day
Absorption 1 mg/day
Transferrin
Reticuloendothelial Stores(measured as ferritin)
Erythroid Marrow
Red Blood Cells
Body Iron Distribution and Pathways Altered in CKD
Adapted from Urrechaga E, et al. Assessing Iron Status in CKD Patients: New Laboratory Parameters. 2012; KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int Suppl. 2013.
7
8

5
Parameter KDOQI* KDIGO**
TSat >20% ≥30% all CKD
Serum ferritin[Acute phase reactant]• Need to use clinical judgment when ferritin >500 ng/mL*
>100 ng/mL CKD‐ND and CKD‐PD
>200 ng/mL CKD‐HD≥500 ng/mL all CKD
*KDOQI: Goal is to maintain TSat and ferritin above these thresholds during ESA treatment, but avoid iron overload.** KDIGO: Goal is to use these values when deciding if iron supplementation is indicated.
KDOQI, NKF. Am J Kidney Dis. 2006; KDIGO 2012 Clinical Practice Guideline for the Evaluation and
Management of Chronic Kidney Disease. Kidney Int Suppl. 2013.
Targets for TSat and Ferritin
CKD‐HD, CKD hemodialysis; CKD‐ND, CKD non‐dialysis; CKD‐PD, CKD peritoneal dialysis; KDIGO, Kidney Disease: Improving Global Outcomes; KDOQI, Kidney Disease Outcomes Quality Initiative; TSat, transferrin saturation.
ESA + consider maintenance iron to avoid iron deficiency
CKD DiagnosisHb <12 g/dL (females)Hb <13.5 g/dL (males)
Evaluate RBC, iron parameters
Correct iron deficiency(oral, parenteral)Iron
deficient
Anemia correctedNo
Maintenance iron
Yes
Evaluation and Management of Anemia of CKD
At goal
FDA Prescribing Information; KDOQI, NKF. Am J Kidney Dis. 2006; KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int Suppl. 2013.Hb, hemoglobin.
9
10
6
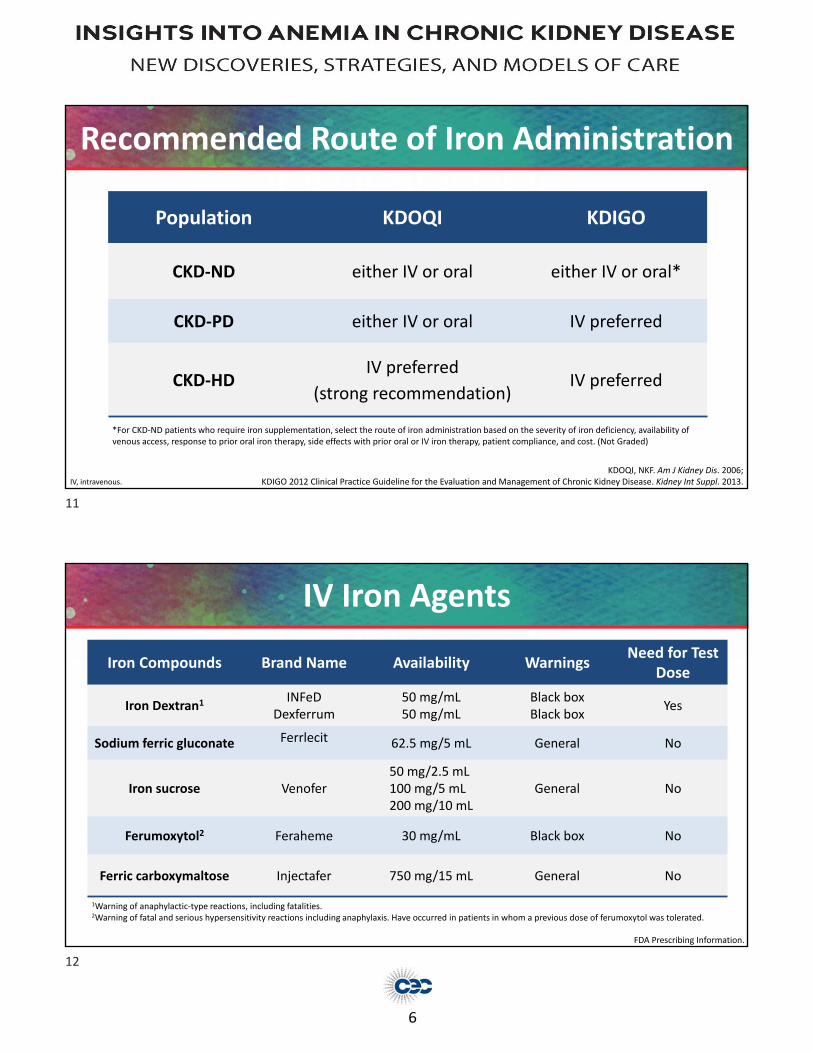
Population KDOQI KDIGO
CKD‐ND either IV or oral either IV or oral*
CKD‐PD either IV or oral IV preferred
CKD‐HDIV preferred
(strong recommendation)IV preferred
*For CKD‐ND patients who require iron supplementation, select the route of iron administration based on the severity of iron deficiency, availability of venous access, response to prior oral iron therapy, side effects with prior oral or IV iron therapy, patient compliance, and cost. (Not Graded)
Recommended Route of Iron Administration
KDOQI, NKF. Am J Kidney Dis. 2006; KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int Suppl. 2013.IV, intravenous.
Iron Compounds Brand Name Availability WarningsNeed for Test
Dose
Iron Dextran1INFeD
Dexferrum50 mg/mL50 mg/mL
Black boxBlack box
Yes
Sodium ferric gluconate Ferrlecit 62.5 mg/5 mL General No
Iron sucrose Venofer50 mg/2.5 mL100 mg/5 mL200 mg/10 mL
General No
Ferumoxytol2 Feraheme 30 mg/mL Black box No
Ferric carboxymaltose Injectafer 750 mg/15 mL General No
IV Iron Agents
1Warning of anaphylactic‐type reactions, including fatalities.2Warning of fatal and serious hypersensitivity reactions including anaphylaxis. Have occurred in patients in whom a previous dose of ferumoxytol was tolerated.
FDA Prescribing Information.
11
12

7
• Adverse effects: dyspnea, wheezing, itching, hypotension, anaphylaxis, infection(?), risks of non‐transferrin bound iron
• Major risk of iron dextrans is anaphylaxis and possible death—requires test dose
• Non‐dextran iron agents have less risk of hypersensitivity reactions and anaphylaxis (no test dose required); however, patients should be monitored during and at least 30 minutes after administration. Black box warning added for ferumoxytol in 2015 regarding hypersensitivity reactions, including risk of anaphylaxis
• Resuscitative medication and personnel trained to evaluate and resuscitate anaphylaxis should be available whenever a dose of IV iron is administered.
• Iron overload—Treat with iron chelators (deferoxamine, deferasirox, deferiprone)
Safety of IV Iron Preparations
FDA Prescribing Information.
Monthly Percent IV Iron Use and Mean Monthly IV Iron Dose in Adult Hemodialysis Patients on Dialysis ≥90 Days
https://www.usrds.org/2018/view/v2_02.aspx.
Medicare Claims2005–2016
13
14

8
Monthly IV Iron Use and Mean Monthly IV Iron Dose in Adult Peritoneal Dialysis Patients
Medicare Claims2005–2016
https://www.usrds.org/2018/view/v2_02.aspx.
ESA + consider maintenance iron to avoid iron deficiency
CKD DiagnosisHb <12 g/dL (females)Hb <13.5 g/dL (males)
Evaluate RBC, iron parameters
Correct iron deficiency (oral, parenteral)Iron
deficient
Anemia correctedNo
Maintenance iron
Yes
Measure Hb during initiation and
maintenance phaseConsider target Hb
Increase ESA dose by 25% Decrease ESA dose by 25%
Hb <1 g/dL in 4 weeks after dose change Hb >1 g/dL in 2‐week period
Evaluation and Management of Anemia of CKD
At goal
FDA Prescribing Information; KDOQI, NKF. Am J Kidney Dis. 2006; KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int Suppl. 2013.
15
16

9
ESA Half‐life Starting Dose*Epoetin alfa (Epogen, Procrit)
Epoetin alfa‐epbx (Retacrit)
8.5 hours (IV)
24 hours (SQ)
CKD (including dialysis)
50–100 Units/kg TIW (IV or SQ)
Darbepoetin
alfa (Aranesp)
21 hours (IV dialysis)
46 hours (SQ dialysis)
70 hours (SQ non‐dialysis)
CKD (dialysis)
0.45 mcg/kg/week or 0.75 mcg/kg every 2 weeks (IV or SQ)
CKD (non‐dialysis)
0.45 mcg/kg once every 4 weeks
Methoxy PEG epoetin beta (Mircera)
119 hours (IV dialysis)124 hours (SQ dialysis)
CKD (including dialysis) 0.6 mcg/kg every 2 weeks (IV or SQ)
*Dosing adjustments based on Hb response.
FDA Prescribing Information; MacDougall IC, et al. J Am Soc Nephrol. 1999; Jurado Garcia JM, et al. Clin Transl Oncol. 2007.
Erythropoiesis Stimulating Agents
SQ, subcutaneous; TIW, three times per week.
ESA + consider maintenance iron to avoid iron deficiency
CKD DiagnosisHb <12 g/dL (females)Hb <13.5 g/dL (males)
Evaluate RBC, iron parameters
Correct iron deficiency (oral, parenteral)Iron
deficient
Anemia correctedNo
Maintenance iron
Yes
Measure Hb during initiation and
maintenance phaseConsider target Hb
Increase ESA dose by 25% Decrease ESA dose by 25%
Hb <1 g/dL in 4 weeks after dose change Hb >1 g/dL in 2‐week period
Evaluation and Management of Anemia of CKD
At goal
FDA Prescribing Information; KDOQI, NKF. Am J Kidney Dis. 2006; KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int Suppl. 2013.
17
18
10
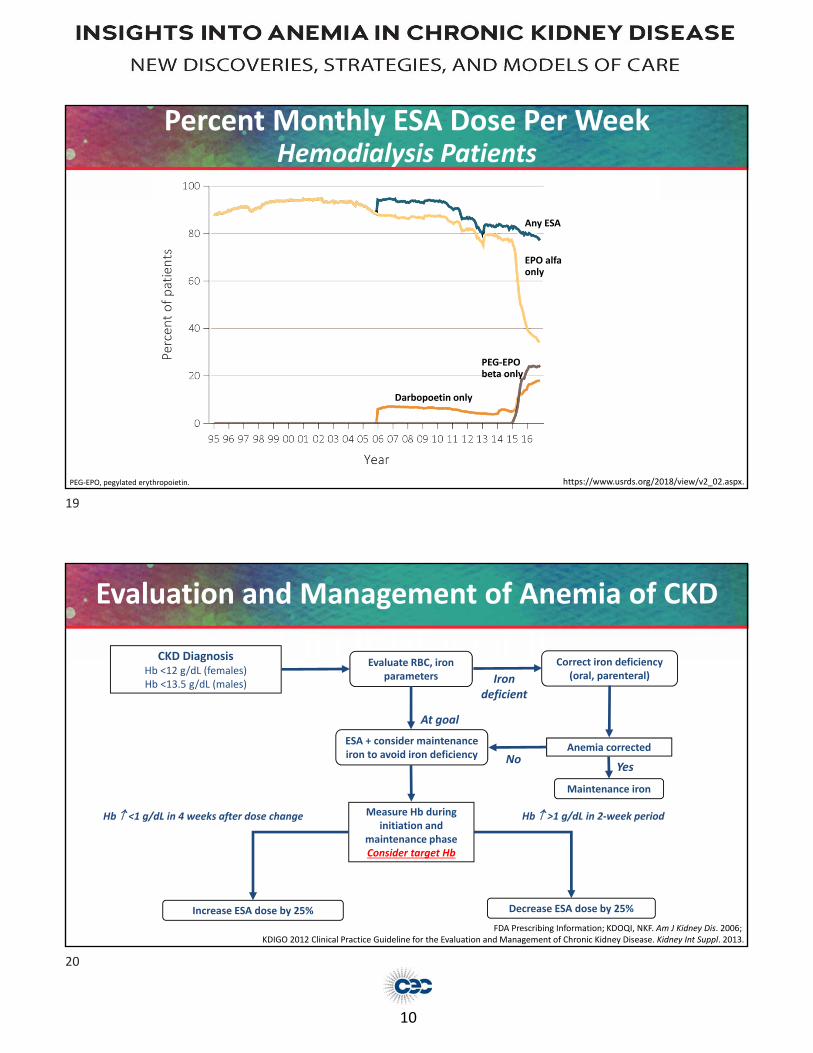
Percent Monthly ESA Dose Per WeekHemodialysis Patients
https://www.usrds.org/2018/view/v2_02.aspx.PEG‐EPO, pegylated erythropoietin.
Any ESA
EPO alfaonly
Darbopoetin only
PEG‐EPO beta only
ESA + consider maintenance iron to avoid iron deficiency
CKD DiagnosisHb <12 g/dL (females)Hb <13.5 g/dL (males)
Evaluate RBC, iron parameters
Correct iron deficiency (oral, parenteral)Iron
deficient
Anemia correctedNo
Maintenance iron
Yes
Measure Hb during initiation and
maintenance phaseConsider target Hb
Increase ESA dose by 25% Decrease ESA dose by 25%
Hb <1 g/dL in 4 weeks after dose change Hb >1 g/dL in 2‐week period
Evaluation and Management of Anemia of CKD
At goal
FDA Prescribing Information; KDOQI, NKF. Am J Kidney Dis. 2006; KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int Suppl. 2013.
19
20
11
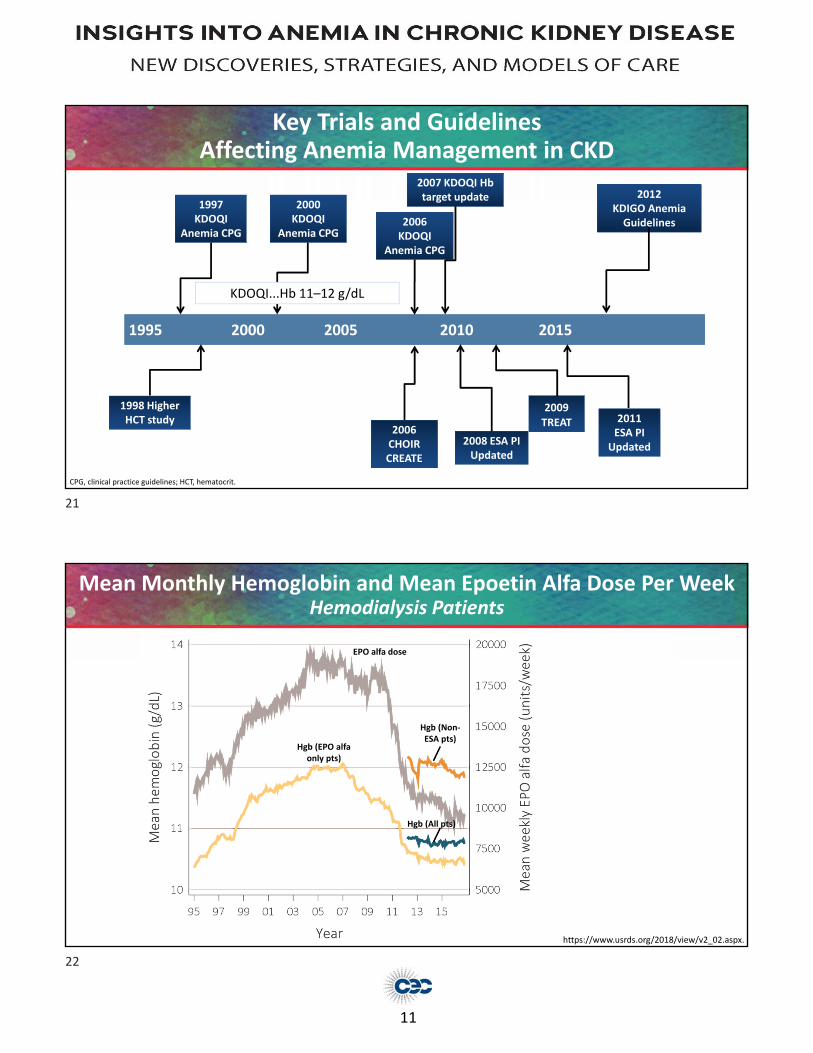
Key Trials and Guidelines Affecting Anemia Management in CKD
1995 2000 2005 2010 2015
1998 Higher HCT study
2007 KDOQI Hb target update
2006 CHOIR CREATE
2006KDOQI
Anemia CPG
2009TREAT
2000KDOQI
Anemia CPG
2011 ESA PI
Updated
2012KDIGO Anemia Guidelines
1997KDOQI
Anemia CPG
2008 ESA PI Updated
KDOQI...Hb 11–12 g/dL
CPG, clinical practice guidelines; HCT, hematocrit.
Mean Monthly Hemoglobin and Mean Epoetin Alfa Dose Per WeekHemodialysis Patients
https://www.usrds.org/2018/view/v2_02.aspx.
Hgb (All pts)
Hgb (EPO alfa only pts)
EPO alfa dose
Hgb (Non‐ESA pts)
21
22

12
Mean Monthly Hemoglobin and Mean Darbepoetin Dose Per Week Hemodialysis Patients
https://www.usrds.org/2018/view/v2_02.aspx.
Study (ESA) Patients Included Target Hb (g/dL)
Besarab A, et al1,2
(Epoetin alfa)ESRD patients with cardiac disease on HD 14 ± 1 vs 10 ± 1
CHOIR3
(Epoetin alfa)Patients with CKD not on dialysis 13.5 vs 11.3
CREATE4
(Epoetin beta)Patients with CKD not on dialysis 13–15 vs 10.5–11.5
TREAT5
(Darbepoetin alfa)Patients with CKD and type 2 diabetes
not on dialysis
13 vs Hb in placebo group (rescue darbepoetin dose
given if Hb <9)
Studies Evaluating Higher Hb Targets with ESAs in Patients with Anemia of CKD
1Besarab A, et al. N Engl J Med. 1998; 2Besarab A, et al. N Engl J Med. 2008; 3Singh AK, et al. N Engl J Med. 2006;
4Drüeke, et al. N Engl J Med 2006; 5Pfeffer et al. N Engl J Med 2009.
CHOIR = Correction of Hemoglobin and Outcomes in Renal InsufficiencyCREATE = CV Risk Reduction by Early Anemia Treatment with Epoetin BetaTREAT = Trial to Reduce CV Events with Aranesp (Darbepoetin alfa) Therapy
23
24

13
Black Box Warning for ESAs in CKD
Chronic Kidney Disease
In controlled trials, patients experienced greater risks for death, serious adverse cardiovascular reactions, and stroke when administered erythropoiesis‐stimulating agents (ESAs) to target a hemoglobin level of greater than 11 g/dL.
No trial has identified a hemoglobin target level, ESA dose, or dosing strategy that does not increase these risks.
Use the lowest dose sufficient to reduce the need for red blood cell (RBC) transfusions.
Prescribers and patients should weigh the possible benefits of decreasing transfusions against the increased risks of death and other serious cardiovascular adverse events.
Limitations of use: ESAs have not been shown to improve quality of life, fatigue, or patient well‐being.
FDA Prescribing Information (epoetin alfa).
Initiation of ESA
ND‐CKD ESRD
KDIGO
Consider potential benefits of reducing transfusions and anemia‐related symptoms against the risks of harm (eg, stroke, vascular access loss, hypertension).
Hb <10 g/dLConsider the rate of fall of Hb, prior response to iron therapy, the risk of needing a transfusion, the risks related to ESA therapy, and the presence of symptoms.
Hb 9–10 g/dL
FDAIf <10 g/dL AND the rate of Hb decline indicates RBC transfusion likely and reducing the risk of alloimmunization and/or other RBC transfusion‐related risks is a goal
If <10 g/dL
Target Hb (g/dL)
ND‐CKD ESRD
KDIGO Do not exceed 11.5 Do not exceed 11.5
FDA 10 avoid transfusions 10–11 avoid transfusions
https://www.fda.gov/Drugs/DrugSafety/ucm259639.htm; KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int Suppl. 2013.
KDIGO and FDA Guidelines for Initiation of ESAs and Hb Targets
ESRD, end‐stage renal disease; FDA, Food and Drug Administration.
25
26

14
IV Iron • Benefits—improve Hb levels, reduce dosing requirements for ESA
• Risks—accumulation in tissue, increase in oxidative stress (?), risk of infection (?), increase in non‐transferrin bound iron
ESAs• Benefits—decrease need for RBC transfusions, improvement in QoL (?)
• Risks—CV events, stroke, vascular thrombosis, black box warning
Balancing Risks/Benefits of IV Iron and ESAs
Fishbane S, et al. Nephrol Dial Transplant. 2014; FDA Prescribing Information.QoL, quality of life.
Targets for Other Therapies
27
28
15
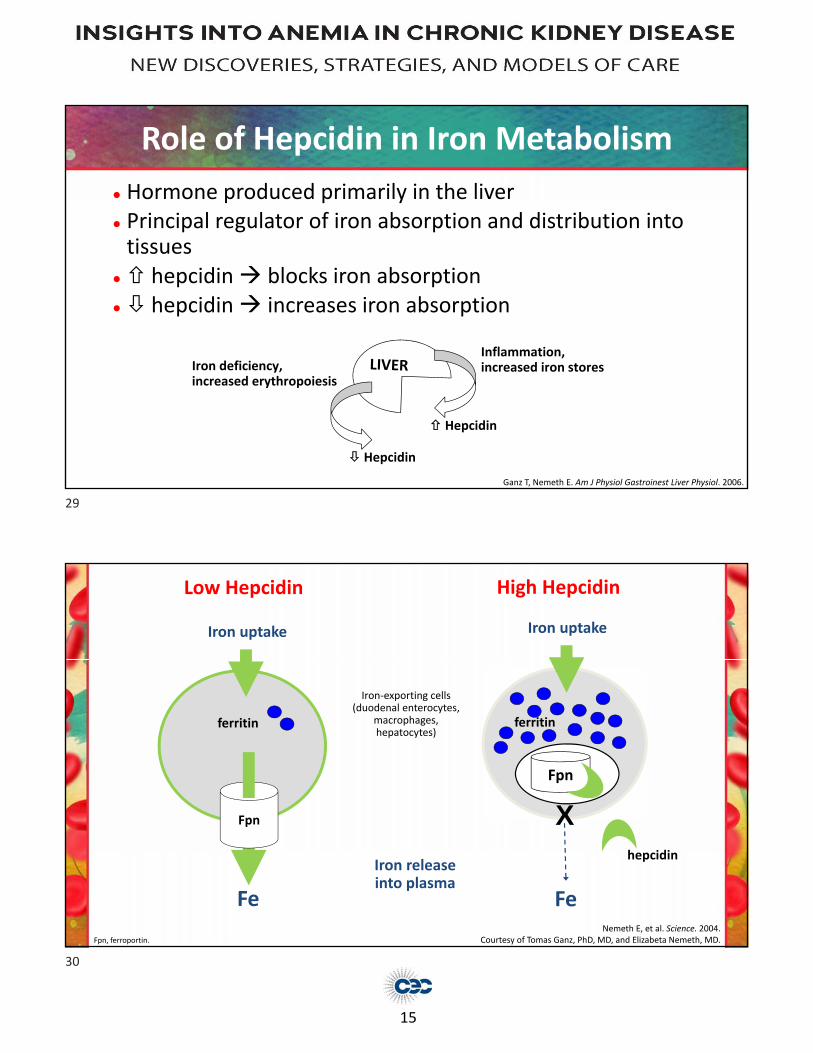
● Hormone produced primarily in the liver● Principal regulator of iron absorption and distribution into tissues
● hepcidin blocks iron absorption● hepcidin increases iron absorption
Hepcidin
Inflammation, increased iron storesIron deficiency,
increased erythropoiesis
Hepcidin
Role of Hepcidin in Iron Metabolism
Ganz T, Nemeth E. Am J Physiol Gastroinest Liver Physiol. 2006.
High Hepcidin
Fe
hepcidin
ferritin
X
Fpn
Iron uptake
Fpn
Fe
ferritin
Low Hepcidin
Iron uptake
Iron releaseinto plasma
Iron‐exporting cells (duodenal enterocytes,
macrophages, hepatocytes)
Nemeth E, et al. Science. 2004.Courtesy of Tomas Ganz, PhD, MD, and Elizabeta Nemeth, MD.Fpn, ferroportin.
29
30

16
Hepcidin—An Iron‐Regulatory and Host Defense Peptide Hormone
Hepcidin 50 mg IP/mouse
Rivera S, et al. Blood. 2005.
Diseases of Hepcidin Dysregulation
Hereditary haemochromatosisiron‐loading anemias
Anemia of inflammationiron‐refractory iron‐deficiency
anemia hepcidin‐secreting tumors
HepcidinIron
Normal homeostasis
Courtesy of Tomas Ganz, PhD, MD.Ganz T. J Am Soc Nephol. 2007; Ganz T, Nemeth E. Am J Physiol Gastrointest Liver Physiol. 2006.
31
32

17
• ESAs and iron are necessary for treatment of anemia of CKD; however, practitioners need to be cognizant of the limitations in using these agents.
• Evidence of mortality risk associated with higher Hb in select populations has raised many questions and changed treatment approaches for anemia management.
• While available guidelines and recommendations by the FDA differ, the general theme is a more conservative treatment approach.
• New treatment options are emerging that help optimize management of anemia of CKD.
Summary
Moving Forward with Novel Treatments for AnemiaThe Potential Role of HIF‐PD Inhibitors
Thomas Dowling, PharmD, PhD, FCCPProfessor and Assistant DeanDirector, Office of Research
Ferris State University
33
34

18
Anemia of CKD—Pathophysiology
Anemia of CKD
Decreased erythropoietin production
Absolute iron deficiency (malnutrition and poor absorption)
Blood loss
Short RBC life span
Bone marrow suppression by uremia
CKD mineral and bone disorder
Deficiency of vitamin B12 and folate
High hepcidin level,inflammation, infection
All may contribute to functionaliron deficiency and impaired bone
marrow responsiveness to erythropoietin
What is Hypoxia‐Inducible Factor (HIF)?
HIF Target Genes• Vascular (VEGF)
• Erythropoietin (EPO)—production/receptor
• DMT1—iron absorption
• Transferrin Receptor (iron uptake)
• Reduce Hepcidin (Liver)
• Cellular metabolism (anaerobic glucose)
HIF‐α
Degradation
Prolyl Hydroxylase (PH)
HIF‐α/Gene TranscriptionLow O2
Tissue
Gupta N, Wish JB. Am J Kidney Dis. 2017; Fandrey J. Blood. 2008.DMT1, divalent metal transporter 1; VGEF, vascular endothelial growth factor.
35
36

19
HIF‐α
Degradation
Prolyl Hydroxylase (PH)
HIF‐α/Gene TranscriptionLow O2
Tissue
What is Hypoxia‐Inducible Factor (HIF)?
HIF‐PH Inhibitors
X
Gupta N, Wish JB. Am J Kidney Dis. 2017; Fandrey J. Blood. 2008.
HIF Target Genes• Vascular (VEGF)
• Erythropoietin (EPO)—production/receptor
• DMT1—iron absorption
• Transferrin Receptor (iron uptake)
• Reduce Hepcidin (Liver)
• Cellular metabolism (anaerobic glucose)
New Drug ClassHIF‐PH Inhibitors
• Investigational oral HIF‐PH inhibitors in development for anemia in CKD
• Work to stabilize HIF by inhibiting PH enzymes
• Mimics the effects of hypoxia—promotes HIF accumulation
• Stimulates EPO and RBC formation
• Improves iron utilization—decreases hepcidin, increases iron absorption, improve FID
Gupta N, Wish JB. Am J Kidney Dis. 2017.FID, functional iron deficiency.
37
38

20
Oral HIF‐PH Inhibitors in Clinical Development (CKD Anemia)
Name Sponsor Phase 3 Randomized Trials Primary Completion Date
Roxadustat(FG‐4592)
FibroGen/AstraZeneca
7 active/enrolling (n=7,950)8 completed (n=2,428)
Late 2018Early 2017–Mid 2018
Daprodustat(GSK 1278863)
Glaxo Smith Kline1 completed (n=271 Japan)5 underway (n=8,802 US)
Japan (late 2018)US (mid 2020)
Vadadustat(AKB‐6548;MT‐6548)
Akebia/Mitsubishi‐Tanabi
8 active/enrolling(n= 6,900 US; n=660 Japan)
Japan (late 2018)US (Jan–Aug 2018)
Molidustat(BAY 85‐3934)
Bayer 5 active/enrolling (n=628, Japan) Late 2018/2019
www.clinicaltrials.gov.
Oral HIF‐PH Inhibitors in Clinical Development (CKD Anemia)
Name SponsorHIF‐α
stabilizationHIF‐PHD targets
Half‐life(hours)
Dosing frequency
Roxadustat(FG‐4592)
FibroGen/AstraZeneca
HIF‐1α and HIF‐2α PHD1, 2, and 3 12‐13 3x/week
Daprodustat(GSK 1278863)
Glaxo Smith Kline HIF‐1α and HIF‐2α PHD2 and PHD3 4 Daily
Vadadustat(AKB‐6548;MT‐6548)
Akebia/Mitsubishi‐Tanabi
HIF‐2α > HIF‐1α PHD3 > PHD2 4.5 Daily
Molidustat(BAY 85‐3934)
Bayer HIF‐1α and HIF‐2α PHD2>PHD1/PHD3 ~5‐10 Daily
Haase VH. Exp Cell Res. 2017; Gupta N, Wish JB. Am J Kidney Dis. 2017; Böttcher M, et al. Br J Clin Pharmacol. 2018.
39
40

21
• Phase 2, 6‐week dose‐ranging in hemodialysis (n=54)
• Hemoglobin response rate similar or better than EPO
*Not currently approved by the FDA.
13
12
11
10
9
8
Mean (±SE) hem
oglobin (g/dL)
0 1 2 3 4 5 6
Treatment Duration (weeks)
Treatment Cohort (n)/Dosing Regimen/
Parameter
Hb Responders
Number (%) of Responders
p‐Value,Roxadustat vs Epoetin Alfa
A1 (n=9) 1.0 mg/kg TIW 4 (44.4) 1
A2 (n=10) 1.5 mg/kg TIW 8 (80.0) 0.07
A3 (n=9) 2.0 mg/kg TIW 7 (77.8) 0.15
A4 (n=5) 1.8 mg/kg TIW 4 (80.0) 0.27
Subtotal (n=33) 23 (69.7) 0.063
Subtotal A2–A4 (n=24) 19 (79.2) 0.033
Epoetin Alfa (n=9) 3 (33.3) —
Roxadustat
Roxadustat (FG‐4592)*Effect on Hemoglobin
1.8 mg/kg TIW
1.5 mg/kg TIW
2.0 mg/kg TIW
1.0 mg/kg TIW
Epoetin alfa
Roxadustat (FG‐4592)*Effects on Hepcidin
• Mean serum hepcidin levels reduced at 5‐week time point1
• 160% reduced in HD patients receiving 2.0 mg/kg (n=9)• 110% reduced in HD patients receiving 1.5 mg/kg (n=10)• 20% increased in HD patients receiving 1.0 mg/kg (n=9)
• No difference in AE/SAE compared to EPO1
• Common adverse events — gastrointestinal discomfort, infections, hypertension2
*Not currently approved by the FDA.1Provenzano R, et al. Am J Kidney Dis. 2016; 2Provenzano R, et al. Clin J Am Soc Nephrol. 2016.AE, adverse event; SAE, serious adverse event.
41
42

22
Roxadustat (FG‐4592)*Effect on EPO levels
*Not currently approved by the FDA. Provenzano R, et al. Am J Kidney Dis. 2016.
600
500
400
300
200
100
0
Mean (±SE) Plasm
a Erythropoietin Levels (m
IU/m
L)Epoetin alfa IV at screening (n=6)Roxadustat Day 2 (n=6)
0 8 16 24 32 40 48
Hours Post‐Dosing
Daprodustat (GSK1278863)*Effect on Hemoglobin
Holdstock L, et al. J Am Soc Nephrol. 2016.
• Phase 2, 4‐week studies in CKD (n=73) and HD (n=83)
• Hemoglobin levels increased in CKD and were maintained in HD patients (5 mg)
*Not currently approved by the FDA.
5 mg
5 mg
rhEPO
rhEPO
2 mg
2 mg
0.5 mg
0.5 mg
43
44

23
Vadudstat (AKB‐6548)*Effect on Hemoglobin
Pergola PE, et al. Kidney Int. 2016.
• Phase 2, 20‐week, randomized, placebo‐controlled study in CKD Stages 3–5 (n=160—per protocol population)
*Not currently approved by the FDA.
13
12
11
10
9
8
7
Hem
oglobin, g/dL
Time, weeksScreening Baseline Week 2 Week 4 Week 6 Week 8 Week 12 Week 16 Week 19 EOT Follow‐up
Treatment GroupVadadustatPlacebo
EOT, end of trial.
Vadudstat (AKB‐6548)*Effect on Hepcidin
Pergola PE, et al. Kidney Int. 2016.
*Not currently approved by the FDA
Treatment GroupVadadustatPlacebo500
450
400
350
300
250
200
150
100
50
Mean hep
cidin, ng/m
L
S B 4 8 12 16 EOT FU
Time, weeks
FU, follow‐up.
45
46

24
Vadudstat (AKB‐6548)*Effect on VEGF
*Not currently approved by the FDA Pergola PE, et al. Kidney Int. 2016.
300
250
200
150
100
50
0S B 4 8 12 16 EOT FU
Time, weeks
Treatment GroupVadadustatPlacebo
VEG
F, ng/m
L
Potential Pitfalls/Questions
• What are the long‐term safety concerns?• Remember—Cardiovascular risk of ESAs was not discovered until years after clinical use
• Induce chronic hypoxia state• Angiogenesis—role in metastasis?
• Cost/benefit ratio?• Future place in therapy?
• Pre‐emptive vs. CKD stage 2
47
48

25
Conclusions
• Emerging data from Phase 2 studies suggest new oral HIF‐PH inhibitors increase hemoglobin and correct anemia
• May provide added benefit of improving iron utilization
• Long‐term safety and efficacy yet to be determined
Interprofessional Management in CKDFocus on the Patient
through Team‐based Care
Calvin J. Meaney, PharmD, BCPSClinical Assistant Professor
University at BuffaloSchool of Pharmacy and Pharmaceutical Sciences
49
50

26
Interprofessional Team
• Mutual respect and shared values• Role delineation• Communication• Team building
Interprofessional Education Collaborative. 2016.
Interprofessional Clinics Improve the Care of CKD Patients
Study Pharmacist? Major Findings
Chen PM, et al. Am J Med. 2015.
Yes• Better renal survival (aHR 0.64, 95% CI: 0.48–0.85)• No mortality difference• Cost savings $1,931/patient‐year
Chen YR, et al. Nephrol Dial Transplant. 2013.
Yes• 51% reduction in all‐cause mortality• 68% increased risk of dialysis initiation• Higher rate of guideline directed medication therapy
Hemmelgam BR, et al. J Am Soc Nephrol. 2007.
No • Lower risk of all‐cause mortality (aHR 0.50, 95% CI: 0.35–0.71)
Curtis BM, et al. Nephrol DialTransplant. 2005.
Yes• Standard clinic had higher risk of mortality (HR 2.17, 95% CI: 1.11–4.28)
• Higher hemoglobin, calcium, and albumin in multidisciplinary clinic
Bayliss EA, et al. Clin J Am Soc Nephrol. 2011.
Yes• GFR declined at 2.52ml/min/1.73m2 per year in historical control vs 1.17ml/min/1.73m2 per year with multidisciplinary care (P<0.0001)
aHR, adjusted hazard ratio; CI, confidence interval; HR, hazard ratio.
51
52

27
• Systematic review of pharmacists’ interventions in CKD included 37 studies with 4,743 patients
• The 8 controlled studies reports including 744 CKD patients showed that pharmacy intervention• Reduced composite of ESRD and mortality in diabetics 14.8 vs 28.2 per 100
patient‐years (P<0.001; 60% relative risk reduction)
• Reduced hospitalizations: 1.8 ± 2.4 vs 3.1 ± 3.0, P=0.02
• Increased target hemoglobin attainment 69.8% vs 43.9%, P=0.0001
• The 5 studies that reported humanistic outcomes showed the pharmacy intervention• Improved HRQOL in dimensions of general health (28% improvement, P<0.001)
and social functioning (26% improvement, P<0.001)
• Improvements in energy, daily activities, and general well being were reported (P<0.05 for all)
Pharmacists’ Interventions in CKD
Salgado TM, et al. Nephrol Dial Transplant. 2010.HRQOL, health‐related quality of life.
Nissenson AR. J Am Soc Nephrol. 2014.
53
54

28
• Treatment of anemia of CKD improves quality of life
• Targeting a higher hemoglobin does not improve quality of life and increases risks of thromboembolic events
Anemia of CKD and Quality of Life
Collister D, et al. Ann Intern Med. 2016.
Forest Plot of All Reported Data on KDQ Domains
• Multi‐center study at VA clinics followed 572 patients for 6 months
• Pharmacist‐based care• Most likely to achieve target hemoglobin
• Reduced darbepoetin alfa utilization by 26%–36% and epoetin alfa by 10%–24%
Aspinall SL, et al. Am J Kidney Dis. 2012.
Pharmacist‐based Anemia Management in CKD
19.3% 21.0%31.8%
71.1%56.9%
51.7%
9.6%22.1% 16.5%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Pharmacist ESA Clinic Usual Care Usual Care ESA Clinic
HB <10g/dL
HB <10g/dL
HB <10g/dL
HB >12g/dL
HB >12g/dL
HB >12g/dL
HB 10‐12g/dL
HB 10‐12g/dL
HB 10‐12g/dL
Aspinall SL, et al. Am J Kidney Dis. 2012.
55
56

29
• 12‐week, prospective, single‐center study in France enrolled 10 CKD non‐dialysis patients for 3 months
• Pharmacist education included• Medical and therapeutic information• Training of the epoetin pen administration device• Self‐injection of the first dose with pharmacist supervision
• Patient knowledge and comfort with self‐injection improved• Compliance was >90% • Quality of life improved significantly
Allenet B, et al. Pharm World Sci. 2007.
Pharmacist‐based Anemia Education in CKD
Pharmacist‐led Anemia Management in CKD
Study Design Major Findings
To LL, et al. Am J Health Sys Pharm. 2001.
Retrospective, before/after study of pharmacist vs physician anemia management in hemodialysis patients over 6‐month period
• Hematocrit was 36.2% ± 3.5% for pharmacists and 35.4% ± 3.3% for physicians (P=0.20).
• Epoetin alfa utilization was 7.7 million units with pharmacists vs 8.5 million units with physicians (P=0.37)
Quercia RA, et al. Hosp Pharm. 2001.
Drug use evaluation of pharmacist‐led anemia management in hemodialysis patients
• Hematocrit <31% decreased from 32% to 14%• Cost avoidance from using epoetin alfa overfill was $91,148/year
• Cost avoidance from pharmacy management of anemia was $203,985/year
Kimura T, et al.Biol Pharm Bull. 2004.
Observational before/after study of pharmacist vs physicianmanagement of anemia in hemodialysis (Japan)
• On target hematocrit improved from 17% to 78% • Epoetin alfa utilization decreased 30%, with 26% cost reduction
57
58

30
Pharmacist‐led Anemia Management in CKD
Study Design Major Findings
Walton T, et al. Hosp Pharm. 2005.
Observational: pharmacist vs US averages
• 80% of pharmacist managed patients had hemoglobin at target (>11g/dL at the time) compared to 75% in US average
• Epoetin alfa utilization decreased from 16,000 units/week in US average to 9,300 units/week with pharmacist management
• $3,000 cost savings per patient per year
Bucaloiu ID, et al. Managed Care Interface. 2007.
Observational: pharmacist vs primary care physician anemia management
• Reduced epoetin alfa utilization 44% (P=0.0001)• Maintained hemoglobin in target range more often (69.8% vs 43.9%, P=0.0001)
Joy MS, et al. Pharmacotherapy. 2007.
Observational: re‐engineeredmultidisciplinary clinic led by pharmacist
• 78% of patient achieved hemoglobin goal compared to 41% of historical patients
• Cross‐sectional cohort, single‐center study in Quebec, Canada
• 36.2% hemoglobin therapeutic range 10–11 g/dL• 39.7% below range• 24.1% above range
• “There are no pharmacists in the multidisciplinary clinic due to lack of budget”
Rinfret F, et al. Can J Kid Health Dis. 2018.
Multidisciplinary CKD Clinic—Anemia Results
59
60

31
• Formulary decision‐making process• Education
• Healthcare professionals
• Patients
• Caregivers
• Interprofessional team member• Develop and implement dosing protocols
• Detect and manage medication‐related problems
• Conduct studies to assess clinical outcomes, HRQOL, and cost‐effectiveness
• Monitoring of therapy• QA/QI
Role of the Pharmacist
Bacchus S, et al. Ann Pharmacother. 2009.QA, quality assurance; QI, quality improvement.
Patient Cases
61
62

32
• 55‐year‐old African American male (188 cm, 76 kg dry weight) on hemodialysis Tuesday/Thursday/Saturday
• PMH: Hypertension; type 2 diabetes mellitus; peripheral vascular disease, s/p left below knee amputation and right total metatarsal amputation; COPD; gout; anemia of CKD and chronic disease; CKD‐mineral bone disease
• Social: smokes ½ pack of cigarettes per day, 50 pack/year history; lives with sister “most of the time”; missed ~20% of his dialysis appointments in the past 6 months
• Outpatient medications: nifedipine ER 60 mg PO BID; labetalol 800 mg PO BID; clonidine 0.3 mg PO TID; sevelamer carbonate 1600 mg PO TID with meals; calcium acetate 667 mg PO TID with meals; cinacalcet 60 mg PO daily; allopurinol 100 mg PO daily; Nephro Vite daily; insulin glargine 15 units SQ QHS; sitagliptin 25 mg PO daily; budesonide/formoterol 250/50 1 puff BID
• Dialysis medications: epoetin alfa 38,000 units SQ once weekly; ferric gluconate 62.5 mg IV once weekly (received 3 PRBC transfusions in past year)
Case 1
COPD, chronic obstructive pulmonary disease; ER, extended release; PO, by mouth; BID, twice daily; TID, three times daily; QHS, every bed time; PRBC, packed red blood cells.
Case 1—Patient Application
• Vitals: (pre‐dialysis) BP 168/92 mmHg; HR 78 bpm; RR 18 bpm; O2 saturation 92% on room air
• Labs: hemoglobin 9.2 g/dL (8.8–10.1g/dL in past 3 months); transferrin saturation 19%; ferritin 1800 ng/mL; calcium 7.8 mg/dL; phosphate 6.2 mg/dL; iPTH 580 pg/mL; albumin 2.8 g/dL
Questions
1. What is the role of a pharmacist in the care of this patient?
2. Identify 3 other health care professionals and their roles that can provide benefit to this patient.
3. What are this patient’s goals of anemia management? Is he achieving them?
4. What effects would a HIF‐PH inhibitor have in this patient?
BP, blood pressure; HR, heart rate; iPTH, intact parathyroid hormone; RR, respiratory rate.
63
64

33
• Anemia management (CDTM)• Mineral bone disease management (CDTM)• Medication therapy management/comprehensive medication management (Pai AB, et al. Hemodial Int. 2009.)
• Transitions of care• Adherence assessment and counseling• Patient education• Smoking cessation• Collaborate with other professionals to optimize care
What is the role of a pharmacist in the care of this patient?
CDTM, collaborative drug therapy management.
• Physician: supervise CDTM protocol, optimize medical therapy, and ensure appropriate referrals to specialists
• Nursing: wound care, medication administration, smoking cessation
• Social work: living situation, transportation, financial counseling
• Dietary: hemodialysis diet
• Dental: dental assessment and appropriate routine cleaning
• PT/OT: activities of daily living with amputations
Identify 3 other healthcare professionals and their roles that can provide benefit to this patient.
OT, occupational therapy; PT, physical therapy.
65
66
34
• Improve quality of life
• Prevent blood transfusions
• Maintain hemoglobin 10–11 g/dL
What are this patient’s goals of anemia management? Is he achieving them?
Unknown
No
Not reliably
• Durable hemoglobin response• Increase iron absorption• Decrease ferritin• Decrease transferrin saturation by increasing total iron binding capacity
• Decrease hepcidin
What effects would a HIF‐PH inhibitor have in this patient?
Gupta N, Wish JB. Am J Kid Dis. 2017.
67
68

35
• 165 patient capacity hemodialysis clinic• Academic medical center in an urban setting• Medical director oversees daily operations; 8 university affiliated nephrologists see patients ~once per month
• Nurse driven management of anemia protocol following KDIGO/FDA guidelines
• Epoetin alfa utilization 14,000 units/week/patient• Cost $2.4 million/year
• Time in therapeutic hemoglobin range of 10–11 g/dL: 42.7%
Case 2—Health‐System Application
How would you propose to integrate a pharmacist into this hemodialysis clinic?
Proposal• 1 FTE clinical pharmacist with 50% fringe = $172,500• Anemia protocol revision and CDTM contract with medical director• Goals
• 15% reduction in epoetin alfa utilization (Aspinall, et al.)
• $400,000 annual savings
• Time in therapeutic hemoglobin range >55%
• Increased HRQOL
• Long term: medication reconciliation program, CDTM protocol for MBD, QA/QI of pharmacy‐driven services
Case 2—Health‐System Application
MBD, mineral and bone disorder.
69
70

36
Summary
• Interprofessional team‐based care improves outcomes of CKD patients, but little is known about changes in health related quality of life
• Pharmacists are integral members of the interprofessional team
• Anemia management is an ideal opportunity for pharmacists to integrate into the team given the complexity of pharmacotherapy, relation to quality of life, and cost savings potential
71

References and Suggested Reading
Allenet B, Chen C, Romanet T, et al. Assessing a pharmacist‐run anaemia educational programme for patients with chronic renal insufficiency. Pharm World Sci. 2007;29(1):7–11.
Aspinall SL, Cunningham FE, Zhao X, et al; ESA Clinic Study Group. Impact of pharmacist‐managed erythropoiesis‐stimulating agents clinics for patients with non‐dialysis‐dependent CKD. Am J Kidney Dis. 2012;60(3):371–379.
Bacchus S, O'Mara N, Manley H, et al. Meeting new challenges in the management of anemia of chronic kidney disease through collaborative care with pharmacists. Ann Pharmacother. 2009;43(11):1857–1866.
Bayliss EA, Bhardwaja B, Ross C, et al. Multidisciplinary team care may slow the rate of decline in renal function. Clin J Am Soc Nephrol. 2011;6(4):704–710.
Besarab A, Bolton WK, Browne JK, et al. The effects of normal as compared with low hematocrit values in patients with cardiac disease who are receiving hemodialysis and epoetin. N Engl J Med. 1998;339(9):584–590.
Besarab A, Goodkin DA, Nissenson AR; Normal Hematocrit Cardiac Trial Authors. The normal hematocrit study‐‐follow‐up. N Engl J Med. 2008;358(4):433–434.
Böttcher M, Lentini S, Arens ER, et al. First‐in‐man‐proof of concept study with molidustat: a novel selective oral HIF‐prolyl hydroxylase inhibitor for the treatment of renal anaemia. Br J Clin Pharmacol. 2018;84(7):1557‐1565.
Brook JH. Iron Metabolism in Health and Disease. Philadelphia, Pennsylvania: WB Saunders; 1994.
Bucaloiu ID, Akers G, Bermudez MC, et al. Outpatient erythropoietin administered through a protocol‐driven, pharmacist‐managed program may produce significant patient and economic benefits. Manag Care Interface. 2007;20(6):26–30.
Chen PM, Lai TS, Chen PY, et al. Multidisciplinary care program for advanced chronic kidney disease: reduces renal replacement and medical costs. Am J Med. 2015;128(1):68–76.
Chen YR, Yang Y, Wang SC, et al. Effectiveness of multidisciplinary care for chronic kidney disease in Taiwan: a 3‐year prospective cohort study. Nephrol Dial Transplant. 2013;28(3):671–682.
Collister D, Komenda P, Hiebert B, et al. The effect of erythropoietin‐stimulating agents on health‐related quality of life in anemia of chronic kidney disease: a systematic review and meta‐analysis. Ann Intern Med. 2016;164(7):472–478.
Curtis BM, Ravani P, Malberti F, et al. The short‐ and long‐term impact of multi‐disciplinary clinics in addition to standard nephrology care on patient outcomes. Nephrol Dial Transplant. 2005;20(1):147–154.
Drüeke TB, Locatelli F, Clyne N, et al; CREATE Investigators. Normalization of hemoglobin level in patients with chronic kidney disease and anemia. N Engl J Med. 2006;355(20):2071–2084.
Fandrey J. Erythropoiesis‐‐once more HIF! Blood. 2008;112(4):931–932.
FDA Approved Drug: darbepoetin alfa. October 2017. U.S. Food and Drug Administration website. https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/103951s5374lbl.pdf. Accessed December 2018.
FDA Approved Drug: epoetin alfa‐epbx. May 2018. U.S. Food and Drug Administration website. https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/125545s000lbl.pdf. Accessed December 2018.
FDA Approved Drug: epoetin alfa. September 2017. U.S. Food and Drug Administration website. https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/103234s5363s5366lbl.pdf. Accessed December 2018.
FDA Approved Drug: ferric carboxymaltose. April 2018. U.S. Food and Drug Administration website. https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/203565s008lbl.pdf. Accessed December 2018.

FDA Approved Drug: sodium ferric gluconate. August 2011. U.S. Food and Drug Administration website. https://www.accessdata.fda.gov/drugsatfda_docs/label/2011/020955s013s015lbl.pdf. Accessed December 2018.
FDA Approved Drug: ferumoxytol. February 2018. U.S. Food and Drug Administration website. https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/022180s009lbl.pdf. Accessed December 2018.
FDA Approved Drug: iron dextran. July 2009. U.S. Food and Drug Administration website. https://www.accessdata.fda.gov/drugsatfda_docs/label/2009/017441s171lbl.pdf. Accessed December 2018.
FDA Approved Drug: methoxy polyethylene glycol‐epoetin beta. June 2018. U.S. Food and Drug Administration website. https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/125164s078lbl.pdf. Accessed December 2018.
FDA Approved Drug: iron sucrose. November 2017. U.S. Food and Drug Administration website. https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/021135s032lbl.pdf. Accessed December 2018.
FDA Drug Safety Communication: Modified dosing recommendations to improve the safe use of Erythropoiesis‐Stimulating Agents (ESAs) in chronic kidney disease. Published June 24, 2011. U.S. Food and Drug Administration website. https://www.fda.gov/Drugs/DrugSafety/ucm259639.htm. Accessed December 2018.
Fishbane S, Mathew A, Vaziri ND. Iron toxicity: relevance for dialysis patients. Nephrol Dial Transplant. 2014;29:255–259.
Ganz T. Molecular control of iron transport. J Am Soc Nephrol. 2007;18(2):394–400.
Ganz T, Nemeth E. Iron imports. IV. Hepcidin and regulation of body iron metabolism. Am J Physiol Gastrointest Liver Physiol. 2006;290(2):G199–G203.
Gupta N, Wish JB. Hypoxia‐inducible factor prolyl hydroxylase inhibitors: a potential new treatment for anemia in patients with CKD [published correction appears in: Am J Kidney Dis. 2017;69(6):869]. Am J Kidney Dis. 2017;69(6):815–826.
Haase VH, Khawaja Z, Chan J, et al. Vadadustat maintains hemoglobin (Hb) levels in dialysis‐dependent chronic kidney disease (DD‐CKD) patients independent of systemic inflammation or prior dose of erythropoiesis‐stimulating agent (ESA). J Am Soc Nephrol. 2016; 27:318A.
Hemmelgam BR, Manns BJ, Zhang J, et al. Association between multidisciplinary care and survival for elderly patients with chronic kidney disease. J Am Soc Nephrol. 2007;18(3):993–999.
Holdstock L, Meadowcroft AM, Maier R, et al. Four‐week studies of oral hypoxia‐inducible factor‐prolyl hydroxylase inhibitor GSK1278863 for treatment of anemia. J Am Soc Nephrol. 2016;27(4):1234–1244.
Interprofessional Education Collaborative. Core competencies for interprofessional collaborative practice: 2016 update. Washington, DC: Interprofessional Education Collaborative; 2016.
Joint Commission of Pharmacy Practitioners (JCPP). Pharmacists’ patient care process. Published May 29, 2014. JCPP website. https://jcpp.net/wp‐content/uploads/2016/03/PatientCareProcess‐with‐supporting‐organizations.pdf. Accessed December 2018.
Joy MS, Candiani C, Vaillancourt BA, et al. Reengineering clinical operations in a medical practice to optimize the management of anemia of chronic kidney disease. Pharmacotherapy. 2007;27(5):734–744.
Jurado García JM, Torres Sánchez E, Olmos Hidalgo D, et al. Erythropoietin pharmacology. Clin Transl Oncol. 2007;9(11):715–722.
KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int Suppl. 2013;(3)1.

KDOQI; National Kidney Foundation. KDOQI Clinical Practice Guidelines and Clinical Practice Recommendations for Anemia in Chronic Kidney Disease [published correction appears in: Am J Kidney Dis. 2006;48(3):518]. Am J Kidney Dis. 2006;47(5 Suppl 3):S11–S145.
Kimura T, Arai M, Masuda H, et al. Impact of a pharmacist‐implemented anemia management in outpatients with end‐stage renal disease in Japan. Biol Pharm Bull. 2004;27(11):1831–1833.
Nissenson AR. Improving outcomes for ESRD patients: shifting the quality paradigm. Clin J Am Soc Nephrol. 2014;9(2):430–434.
MacDougall IC, Gray SJ, Elston O, et al. Pharmacokinetics of novel erythropoiesis stimulating protein compared with epotin alfa in dialysis patients. J Am Soc Nephrol. 1999;10(11):2392–2395.
Nemeth E, Tuttle MS, Powelson J, et al. Hepcidin regulates cellular iron efflux by binding to ferroportin and inducing its internalization. Science. 2004;306(5704):2090–2093.
Pergola PE, Spinowitz BS, Hartman CS, et al. Vadadustat, a novel oral HIF stabilizer, provides effective anemia treatment in nondialysis‐dependent chronic kidney disease. Kidney Int. 2016;90(5):1115–1122.
Pfeffer MA, Burdmann EA, Chen CY, et al; TREAT Investigators. A trial of darbepoetin alfa in type 2 diabetes and chronic kidney disease. N Engl J Med. 2009;361(21):2019–2032.
Provenzano R, Besarab A, Sun CH, et al. Oral hypoxia‐inducible factor prolyl hydroxylase inhibitor roxadustat (FG‐4592) for the treatment of anemia in patients with CKD. Clin J Am Soc Nephrol. 2016;11(6):982–991.
Provenzano R, Besarab A, Wright S, et al. Roxadustat (FG‐4592) versus epoetin alfa for anemia in patients receiving maintenance hemodialysis: a phase 2, randomized, 6‐ to 19‐week, open‐label, active‐comparator, dose‐ranging, safety and exploratory efficacy study. Am J Kidney Dis. 2016;67(6):912–924.
Quercia RA, Abrahams R, White CM, et al. Cost avoidance and clinical benefits derived from a pharmacy‐managed anemia program. Hosp Pharm. 2000;35(2):169‐175.
Rinfret F, Lambert F, Youmbissi JT, et al. Cross‐sectional assessment of achievement of therapeutic goals in a Canadian multidisciplinary clinic for patients with advanced chronic kidney disease. Can J Kidney Health Dis. 2018;5:2054358118775097.
Rivera S, Nemeth E, Gabayan V, et al. Synthetic hepcidin causes rapid dose‐dependent hypoferremia and is concentrated in ferroportin‐containing organs. Blood. 2005;106(6):2196–2199.
Salgado TM, Moles R, Benrimoj SI, et al. Pharmacists' interventions in the management of patients with chronic kidney disease: a systematic review. Nephrol Dial Transplant. 2012;27(1):276–292.
Singh AK, Szczech L, Tang KL, et al; CHOIR Investigators. Correction of anemia with epoetin alfa in chronic kidney disease. N Engl J Med. 2006;355(20):2085–2098.
To LL, Stoner CP, Stolley SN, et al. Effectiveness of a pharmacist‐implemented anemia management protocol in an outpatient hemodialysis unit. Am J Health Syst Pharm. 2001;58(21):2061–2065.
United States Renal Data System (USRDS). 2018 Annual Data Report: Epidemiology of Kidney Disease in the United States. Bethesda, Maryland: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2018. https://www.usrds.org/2018/view/v2_02.aspx. Accessed December 2018.
Urrechaga E, Borque L, Escanero JF. Assessing Iron Status in CKD Patients: New Laboratory Parameters. InTech: http://www.intechopen.com/articles/show/title/assessing‐iron‐status‐in‐ckd‐patients‐new‐laboratory‐parameters; 2012.
Walton T, Holloway KP, Knauss MD, et al. Pharmacist‐managed anemia program in an outpatient hemodialysis population. Hosp Pharm. 2005;40(12):1051‐1056.


















