
Hand injuries
90
HAND INJURIES Group D 2015
-
Upload
monther-alkhawlany -
Category
Health & Medicine
-
view
159 -
download
1
Transcript of Hand injuries

HAND INJURIES
Group D
2015

HAND INJURIES• The hands as the human executing organs are in the
center of daily life activities’, thus are always exposed to
injuries and overuse .
• We are more aware of our hands than any part of the
body
• Are important out of all proportion to their apparent
severity ,because of the need for perfect functions .
• Local edema and stiffness of the joints –common
accompaniments of all injuries- are more threatening in
the hand than anywhere else .

HAND INJURIES• Problems of hand arise for 3 reasons :
1- the defect may be unacceptable
2- function is impaired
3- deformed part becomes nuisance during
daily activities
HAND INJURIES• Superficial injuries and severe fracture are obvious but
deeper injuries are often poorly disclosed ,so it is
important in the initial examination to assess the
• circulation
• soft tissue cover
• bones
• joints and tendon
• nerves
• X-rays should include at least 3 views PA ,Lateral and
oblique

HAND INJURIES• Hand injuries the commonest of all injuries .
• in avarage the hand injuries account for 14-30% of all pt
in ED .
• Fractures 46% , tendon injuries 29% and skin lesions .

HAND INJURIESgeneral principle of treatment
• ABC
• Most hand injuries can be dealt with under local or
regional anaesthesia .
• Definitive treatment is dictated by the nature of the injury
, but common to all injuries are
• safe splintage
• prevention of swelling
• dedicated rehabilitation

HAND INJURIESgeneral principle of treatment
• Safe splintage
_ incorrect splintage is a potent cause of stiffness
so must be appropriate and kept to a minimum
-if the whole hand is splinted or bandage this must be in
‘’the position of safe immobilization’’

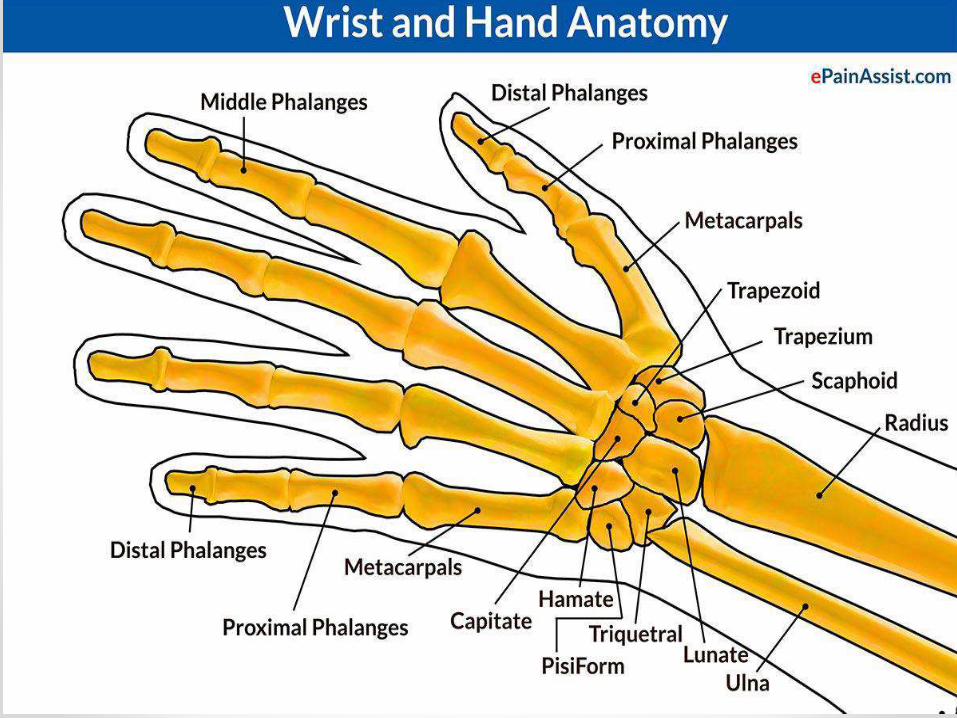
Anatomy of the hand• Bones
• Areas
• Zones
• Arches
• Ligaments
• Muscles
• Innervation
⥤is a prehensile, multi-fingered extremity located at the end of an arm or forelimb .
⥤...& are the richest source of tactile feedback, and have the greatest positioning capability of the body; thus the sense of touch is intimately associated with hands.
PALMAR DORSAL


ZONESExtensor Zones of Hand
Flexor Zones:Flexor Zones: The hand is divided into following 5 zones, which would determine the prognosis and approach to treatment. Zone 1:Only FDP involvedLoss of flx of DIP jointInstability in pinchLoss of grip strengthGood prognosisZone 2:“No man’s land”Pulleys present (prevent bow stringing) A2 and A4Vincula in area–provide vascular supply. Injury thus causes decreased tendon vascular nutrition.Poor prognosisZone 3:Good prognosisGood vascularity and no pulleysZone 4:Carpal tunnelUsually more than 1 tendon involvedIntendinous adhesions (close proximity of tendons)Relatively good prognosisZone 5:Usually presents with nerve involvement (ulnar / median nerve)Tendons superficial, thus adhesions to skin probable
The hand is divided into 8 zones when dealing with extensor tendon injuries.

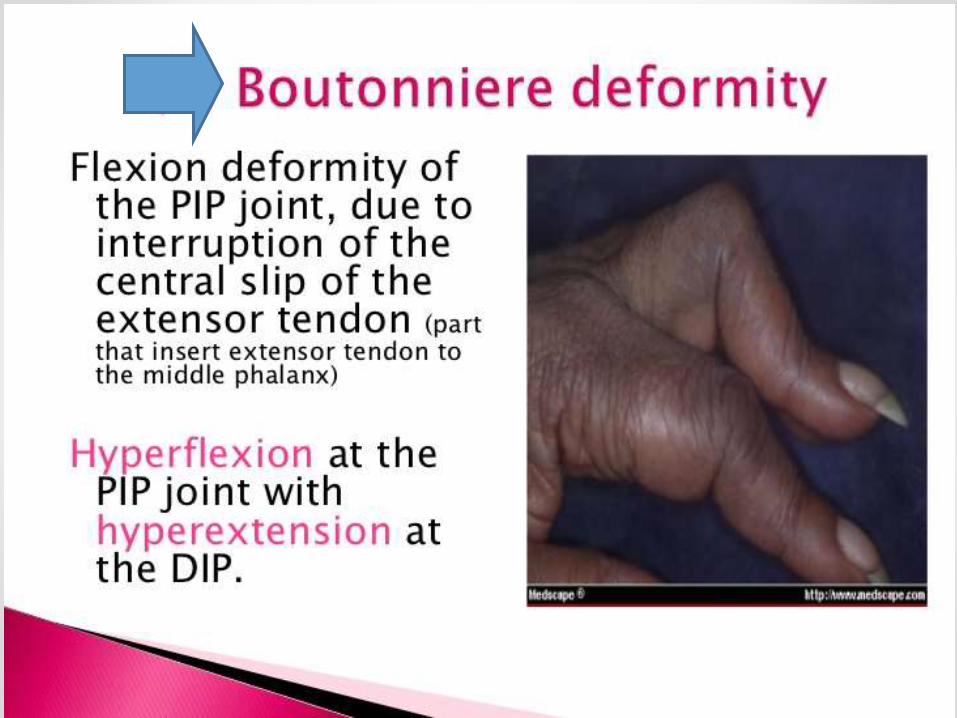
Muscles & tendons* Extensor tendons of fingers :
-of the long extrinsic muscles .
-attaches to the middle phalanx in
central slip .
* system of flexor tendons of fingers :
-functional unit of tendons, tendon sheath and pulleys .
- flexor digitorum profundus .
- flexor digitorum superficial .
- flexor pollicis longus of the thumb .
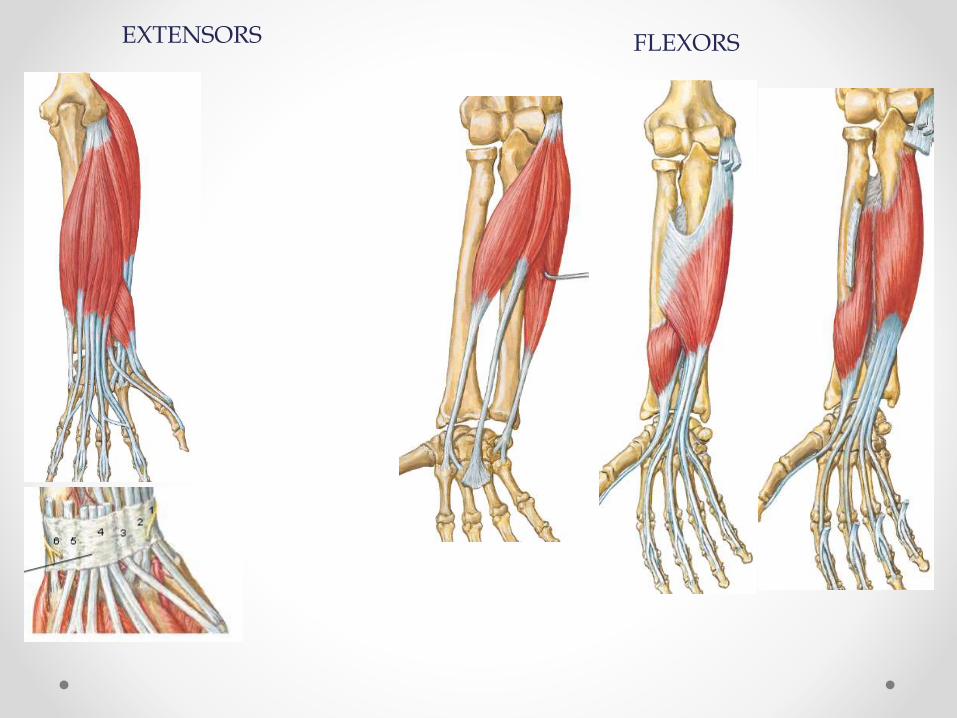
FLEXORSEXTENSORS





ligaments• Tow important structures called collateral ligaments are
found in either sides of each finger joint .
• Volar plate is the strongest ligament .

Blood Supply
1. Ulnar A.
Forms the superficial palmar arch ?with superficial palmar br. of radial artery
Gives 4 common palmar digital art.
2. Radial A.
Forms the Deep
palmar arch with
deep br. of ulnar ar. 1
cm proximal to
Superficial arch


Nerve supply

Nerve supply

Median
Nerve
Ulnar
Nerve
Radial
Nerve

Bone & jointsinjuries

Metacarpal Fractures
The metacarpal bones are vulnerable to blows and falls upon the hands or the force of the boxer’s punch .
Injuries are common
Agulatory deformity is usually not very marked ,rotational deformity is serious .

2)Metacarpal Fractures Head
Intraarticular
Neck Usually unstable
Forwards tilting of distal fragement
Shaft Direct blow
Transverse or oblique #
Base Associated carpal bone injury
Impacted #
1st metacarpal Usually occurs at base

Presentation Pain/Tenderness
Swelling
Discoloration
Sensation
Circulation
ROM
Plain Films
Deformity of hand
Localized tenderness
Swelling of hand
Discoloration
Decreased movement
Numbness
Unequal temperatures
What next?

Midshaft vs. Base vs. Neck
Complete vs. Incomplete vs. Comminuted
Dorsal vs. Volar Angulation
Transverse vs. Oblique vs. Spiral
Unstable vs. Stable

Management of metacarpal #
A- undispalced # :
require only a firm crepe-bandage for comfort
2-3 wks

Management of metacarpal #
B- dispalced # :
1-of the shaft
- reducion by traction and pressure hand then held by plaster slap for 3 wks .
-ORIF with small plates and screws
or by percutaneous K-ware
is the best because these
unstable #

Management of metacarpal #
B- dispalced # :
2- of the neck (boxer’s fracture )
* usually of the 5th finger
* angulation of upto 40 degrees can be accepted as long as there is no rotational deformity .
* reduction traction and pressure then held by plaster slap 1-2wks
* fixation with percutaneous
intramedullary wires
usually preferred

Metacarpal Neck Fractures
(Boxer’s Fracture)
Common Direct impact with closed fist
Dorsal angulation Unstable
Treatment Reduction (90-90 method)
Splint
Follow-up within 1 week
Complications Malunion with volar angulation
Pain
Rotational deformity
Stiffness

Metacarpal Base Fractures
Stable
Infrequent
Associated injury Ulnar nerve
Carpal bone injury
Treatment Volar splint
Complications Tendon damage
Stiffness

Thumb Metacarpal Fractures
Uncommon Most involve the base Extraarticular
Direct trauma or impaction 20-30 degrees of angulation is
tolerated
Intraarticular Bennett’s Fracture Rolando’s Fracture
Treatment Thumb spica
Complications Malunion and arthritis
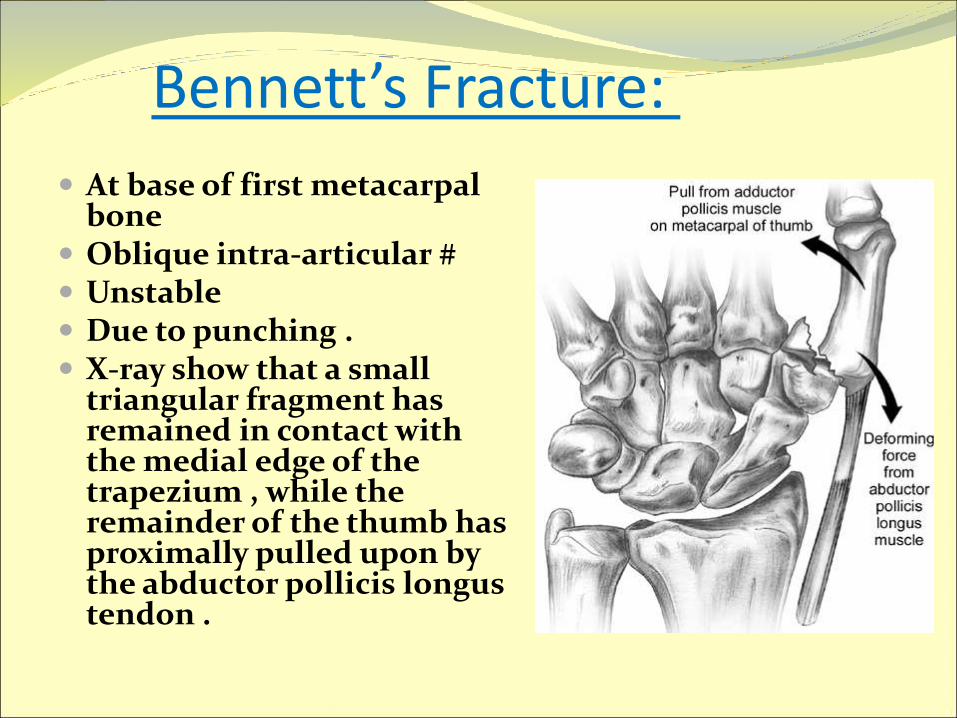
Bennett’s Fracture:
At base of first metacarpal bone
Oblique intra-articular # Unstable Due to punching . X-ray show that a small
triangular fragment has remained in contact with the medial edge of the trapezium , while the remainder of the thumb has proximally pulled upon by the abductor pollicis longustendon .

Bennett’s Fracture: Perfect reduction is essential by pulling on the thumb
,abducting it and extending it .and then held by plaster or internal fixation
Surgical fixation is achieved by passing a k-ware across the metacarpal base into the carpus

a)Bennett’s Fracture:
Intraarticular fracture
Dislocation/Subluxation CMC joint
Fragment pulled dorsally Abductor pollicis longus
Adductor pollicis
Ligament disruption
Treatment Thumb spica
Early referral

b)Rolando’s Fracture
Comminuted intraarticular fracture
Less common than Bennett’s Fracture Worse prognosis
Treatment Thumb spica
Early referral
Complications Malunion and pain

fractures of phalanges
Phalangeal # usually result from direct trauma and therefore any part may be affected .
Management :
A) undisplaced # :
functional splintage (buddy splintage )
for 2-3 wks .
- movement are encouraged from the outset .

fractures of phalanges
B) – displaced fractures
1- of the proximal or the middle phalanx :
* the bone # reduced and immobilized under
local anaesthesia , carefully avoiding
malrotation , then splintaed leaving the other
fingers free 3 wks .

fractures of phalanges
B) – displaced fractures
1- of the distal phalanx :
distal phalangeal # are usually due to crushing injuries or a blow from a hammer .
- the soft tissue damage must be treated .
-The majority of fractures can be treated
conservatively, and it is normally the initial repair
of the surrounding soft tissues that is most
important .

3) Phalanx Fractures
15-30% of hand fxs
Tuft Nail bed injury
Shaft
Intraarticular Tendon injury
Complications Pain, hyperesthesia, cold
sensitivity, osteomyelitis
1)Distal Phalanx FracturesMechanism:

No Problem Refer!
Treatment: padded or “C” splint; extend past the tip
Refer: transverse, angulated
Healing Time: 3-4 weeks
Return to Work/Sport: okay with splint as tolerated
exception: transverse fx –needs longer protection from potential re-injury activity

•Mechanism: direct blow or twisting
•Sxs & Exam: local swelling; examine for deformity or malrotation; check PIP and DIP fxn
2)Middle Phalanx Fractures
•Transverse Fx or short oblique: Low risk

•Nondisplaced fx’s do well with buddy taping
•Healing Time: 4-6 weeks (buddy tape for 3-4 wk)
•Return to Work/Sport: okay as long as you have some protection via splint or buddy tape
•Refer: displaced, long oblique, spiral or intra-articular fx

•Mechanism:
direct blow: transverse; often unstable
due to tendon insertions
twisting: oblique or spiral; may be more
stable
Sxs & Exam: local
swelling; examine
for deformity or
malrotation
3)Proximal Phalanx Fractures
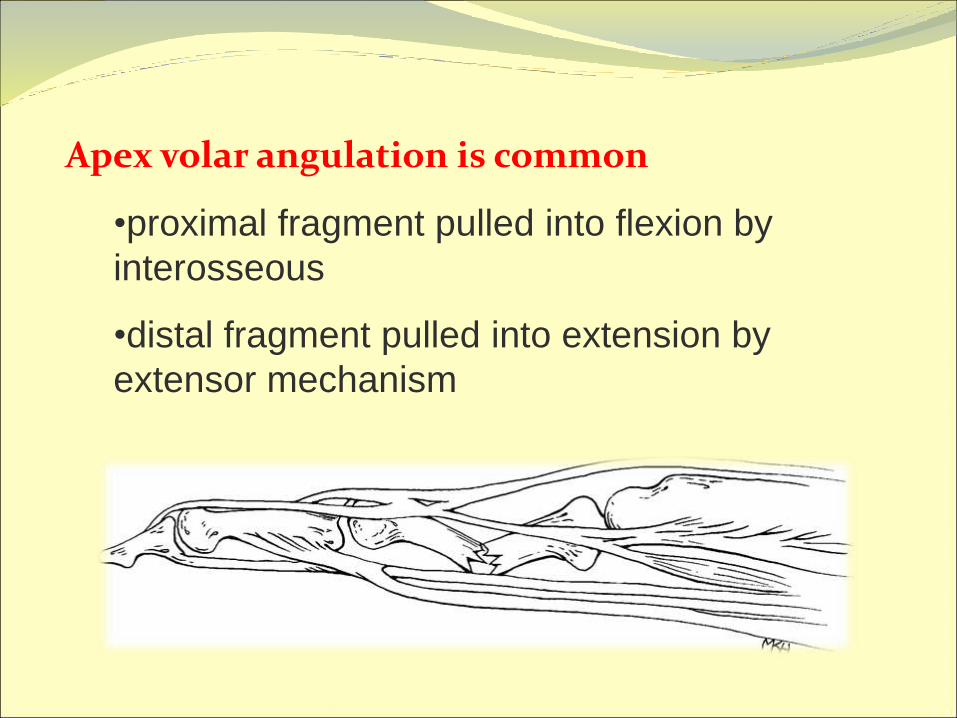
Apex volar angulation is common
•proximal fragment pulled into flexion by
interosseous
•distal fragment pulled into extension by
extensor mechanism


•Nondisplaced fx’s do well with buddy taping; use
gutter splint for additional stability
•Healing Time: 4-6 weeks (buddy tape for 3-4
wk)
•Return to Work/Sport: okay as long as you have
some protection via splint or buddy tape
•Refer: angulated, displaced, intra-articular fx
Proximal Phalanx Fx: Treatment

Alternative:
Burkhalter
Splint
dorsal half to
PIP
volar half to
palmar crease

Joints

CMC joint dislocation:
Mechanism :forceful dorsiflexion of the wrist combined with longitudinal impact ,
Seen typically in boxers and in motorcyclists .
Dx : X-rays
After regional anaesthesia , the dislocation is reduced by traction , manipulation, and pressure on the metacarpal base , then protective slap is worn for 6 wks .

CMC joint dislocation
Carpometacarpal (CMC) dislocation(a) Thumb
dislocation. (b) Dislocation of the fourth andfifth CMC joints treated by closed reduction andKirschner wires (c). Complete CMC dislocation (d).
Thumb CMC dislocation :
Isolated dislocation is rare
compared to the more common Bennett fracture dislocation.
Easy to reduce but unstable after reduction.
Apply thumb spica splint after reduction.
Need surgical referral.

Dislocation of MCP joint

Metacarpophalangeal Joint Relatively rare injury
Dorsal displacement
Hyperextension forces
Dorsal displacement
Volar plate can enter joint space
Volar dislocations
Usually surgical
Treatment
Reduce
Splint in flexion

Dislocation of MCP joint The thumb is most frequently affected and clinically
the injury resembles a BENNETT’ fracture –dislocation
Dx : by Xrays
The displaced is easily reduced by traction & hyperpronation , but reduction is unstable and can be held by a K-wire for 5 wks and then protective splint for 8 wks because risk of instability .

MCP of the Thumb Strong but vulnerable
5 times more likely to be injured
Difficult reduction
Volar plate entrapment
Ulnar collateral ligament injury
Gamekeeper’s or Skier’s thumb
Radial collateral ligament injury
Less common
Forced adduction with or without hyperextension

Skier’s Thumb
Scottish gamekeeper’s Repeated twisting
Forced radial deviation Associated avulsion fracture
Valgus stress testing Extension and flexion
Complete ligament tears >35 degrees of laxity
Treatment Thumb spica

Dislocation InterphalangealJoint

1)Proximal Interphalangeal Joint Dislocation pattern
Dorsal
Most common ligamentous hand injury
Lateral
Volar
Associated fracture
> 33% of articular surface = unstable
Violent twist with finger flexed (palmer) or extended (dorsal)
SHARP, deformity, disability
RICE, splint, meds, reduction/surgery, protect

• Nondisplaced Fx: Initially use extension block
splint for first 2-3 weeks followed by buddy
taping in sight flexion. Work on restoring ROM.
• Healing Time: 6-12 weeks; monitor progress
every 2-3 weeks

2)Distal Interphalangeal Joint Most are dorsal
Often open
Reduction Traction
Hyperextension
Dorsal pressure
Irreducible Avulsion fracture
Buttonhole tear
Open dislocation Irrigation
Antibiotics

Tendons Injuries

Tendon injuries
• Are the second most common injuries of the hand
• After clinical examination , ultrasound and MRI imaging
have provide to be important diagnostic tools .
• Treated by conservative or surgical












• For later case where the joint is still passively correctable
, treated by is to divide the extensor tendon in just
proximal to its insertion into the distal phalanx .
• long standing fixed deformity may be better left alone .




Carpal Tunnel Syndrome
pressure in carpal tunnel (swelling, inflammation) via trauma, rep flexion
Pressure on median n
Sensory (lat palm), motor (wrist, finger flex) deficits
A. Mechanism: overuse, congenital, trauma
B. Pathology: Compression of the median nerve in the tunnel
, surgical decompression

Signs and Symptoms:
Pain in wrist
Numbness and tingling in the thumb and first two fingers
Positive Phalen’s test
Positive tap test

TreatmentConservative: Immobilization and Rest ice
.NSAIDS, corticosteroid injection
Radical: Surgery to increase space in the tunnel

وفق هللا الجميع
GDمحمد عبدالستار


















