Governance and management arrangements for health Sector-Wide Approaches (SWAps) (WP8)
16
KNOWLEDGE HUBS FOR HEALTH Strengthening health systems through evidence in Asia and the Pacific The Nossal Institute for Global Health www.ni.unimelb.edu.au HEALTH POLICY AND HEALTH FINANCE KNOWLEDGE HUB WORKING PAPER SERIES NUMBER 8 | NOVEMBER 2010 Governance and management arrangements for health Sector-Wide Approaches (SWAps): Examples from Africa, Asia and the Pacific Joel Negin Sydney School of Public Health and Menzies Centre for Health Policy, University of Sydney Krishna Hort Nossal Institute for Global Health, The University of Melbourne
-
Upload
nossal-institute-for-global-health -
Category
Documents
-
view
37 -
download
3
description
There are many types of approaches to health involving the whole sector, but what features are relevant to exploring a sector-wide approach for the Solomon Islands?
Transcript of Governance and management arrangements for health Sector-Wide Approaches (SWAps) (WP8)

KNOWLEDGE HUBS FOR HEALTHStrengthening health systems through evidence in Asia and the Pacific
The Nossal Institute for Global Health
www.ni.unimelb.edu.au
HEALTH POLICY AND HEALTH FINANCE KNOWLEDGE HUB
WORKING PAPER SERIES NUMBER 8 | NOVEMBER 2010
Governance and management arrangements for health Sector-Wide Approaches
(SWAps): Examples from Africa, Asia and the Pacific
Joel Negin Sydney School of Public Health and Menzies Centre for Health Policy, University of Sydney
Krishna Hort Nossal Institute for Global Health, The University of Melbourne

WORKING PAPER SERIES HEALTH POLICY AND HEALTH FINANCE KNOWLEDGE HUB
Governance and management arrangements for health Sector-Wide Approaches (SWAPs): NUMBER 8 | NOVEMBER 2010Examples from Africa, Asia and the Pacific
ABOUT THIS SERIES This Working Paper is produced by the Nossal Institute for Global Health at the University of Melbourne, Australia.
The Australian Agency for International Development (AusAID) has established four Knowledge Hubs for Health, each addressing different dimensions of the health system: Health Policy and Health Finance; Health Information Systems; Human Resources for Health; and Women’s and Children’s Health.
Based at the Nossal Institute for Global Health, the Health Policy and Health Finance Knowledge Hub aims to support regional, national and international partners to develop effective evidence-informed policy making, particularly in the field of health finance and health systems.
The Working Paper series is not a peer-reviewed journal; papers in this series are works-in-progress. The aim is to stimulate discussion and comment among policy makers and researchers.
The Nossal Institute invites and encourages feedback. We would like to hear both where corrections are needed to published papers and where additional work would be useful. We also would like to hear suggestions for new papers or the investigation of any topics that health planners or policy makers would find helpful. To provide comment or obtain further information about the Working Paper series please contact; [email protected] with “Working Papers” as the subject.
For updated Working Papers, the title page includes the date of the latest revision.
Governance and management arrangements for health Sector-Wide Approaches (SWAps): Examples from Africa, Asia and the Pacific
First draft – November 2010
Corresponding author: Joel Negin Address: Sydney School of Public Health and Menzies Centre for Health Policy, University of Sydney, [email protected]
Other contributors: Kris Hort, The Nossal Institute for Global Health, University of Melbourne
This Working Paper represents the views of its author/s and does not represent any official position of The University of Melbourne, AusAID or the Australian Government.
ACKOWLEDGEMENTSThe author would like to thank World Bank staff in the Pacific region for their comments on an earlier draft of this paper.

HEALTH POLICY AND HEALTH FINANCE KNOWLEDGE HUB WORKING PAPER SERIES
NUMBER 8 | NOVEMBER 2010 Governance and management arrangements for health Sector-Wide Approaches (SWAPs):Examples from Africa, Asia and the Pacific 1
INTRODUCTIONThis Working Paper summarises the experience of Sector-Wide Approaches (SWAps) or similar arrangements in the health sector in seven countries in Africa, Asia and the Pacific. A SWAp is characterised by an emphasis on governments and development partners working together in a ‘whole-of-sector’ manner to support one agreed health plan, and a related monitoring and evaluation framework, in order to maximise the use of resources available to the sector. Some SWAps include pooled funding arrangements and aligned financial management, while non-pooled SWAps focus on harmonisation and improved aid effectiveness. According to Walt, Pavignani et al (1999), a SWAp provides a broad framework within which all resources in the health sector are coordinated in a coherent and well-managed way, in partnership and with recipients in the lead.
The impetus for this Working Paper came from World Bank colleagues in the Pacific region, where the Bank works closely with governments in developing systems to support various SWAp arrangements. An earlier version of the paper was shared with partners in the Pacific to contribute to discussions about management systems for SWAps.
This Working Paper follows three others on the topic of SWAps in the Pacific region by Joel Negin, with examples drawn from Samoa and the Solomon Islands. The three papers are:
• Sector-WideApproachesforhealth:anintroductiontoSWApsandtheirimplementationinthePacificregion.HPHF Knowledge Hub Working Paper No. 2, March 2010.
• Sector-WideApproachesforhealth:acomparativestudyofexperiencesinSamoaandtheSolomonIslands.HPHF Knowledge Hub Working Paper No. 3, March 2010.
• Sector-WideApproachesforhealth:lessonsfromSamoaandtheSolomonIslands.HPHFKnowledgeHubWorking Paper No. 4, March 2010.
The paper aims to provide examples of governance and management arrangements of health SWAps and similar arrangements in a number of countries. The purpose of the paper is to inform discussion of options for the Government of the Solomon Islands. It does not provide an assessment of the effectiveness or appropriateness of the arrangements, or endeavour to compare arrangements across countries.
Examples of SWAps and similar arrangements were identified through a literature search. Accepted evidence included National Ministry of Health and development partner reports, SWAp reviews, conference presentations and academic literature describing and/or evaluating SWAps. The seven country examples were selected on the basis of availability of relevant information and longevity, under the assumption that SWAps that have been in existence for five or more years are more likely to have more settled and tested management structures. The exception is the Samoan health SWAp, which is included as a Pacific regional comparator to the Solomon Islands.
The emphasis for inclusion of country-level SWAps was on identifying management structures and arrangements that might be relevant to the Government of the Solomon Islands. The establishment of various committees and working groups and their roles and interaction with government bodies, including during formal review processes, were extracted from relevant documents.
The main findings of this review were:
• AllSWApsareadaptedtolocalcircumstancesandlocalneeds;thereisnoone-size-fits-allapproach.
• ThemechanismspresentedherearemostlyfrommuchlargercountriesthantheSolomonIslands,withmany more development partners, and therefore suitability to the Solomon Islands will need to be assessed.
• MostSWApshaveformalisedgovernancearrangements,includingannualorbiannualsectorreviews,morefrequent sector coordination meetings and a SWAp secretariat of some kind. Most SWAps also have a formal Memorandum of Understanding (MOU) between development partners and the government.
• Thelargerannualsectorreviewsgenerallyhavewideparticipation.Theyreviewperformance,developaprogram of work for the upcoming year and provide a forum to agree on financial contributions.

WORKING PAPER SERIES HEALTH POLICY AND HEALTH FINANCE KNOWLEDGE HUB
Governance and management arrangements for health Sector-Wide Approaches (SWAPs): NUMBER 8 | NOVEMBER 2010Examples from Africa, Asia and the Pacific2
• Sectorcoordinationmeetingsgenerallytakeplaceapproximatelymonthlyandincludeatleastdevelopmentpartners and government and, in some cases, NGOs and private providers. All of the coordination committees are chaired by government representatives— most commonly from the Ministry of Health.
• AsmallernumberofSWApcountriesmaintainseparateformaldevelopment-partner-onlycoordinationgroups that report to the wider coordination meetings through a donor focal point.
• MostSWApsalsohavesubgroupsthatprovideforumsforin-depthdiscussionsoncertaintechnicaltopicsand that report to the SWAp management. Most SWAps include subgroups on technical issues related to SWAp functioning, such as human resources, monitoring, procurement or finance.
• Thepersistenceofdisease-specificcoordinationmechanismshasbeenanongoingchallengeforhealthsector coherence.
• Mostcountries’governanceandmanagementarrangementshavechangedovertimetorespondtoemerging challenges and shortcomings.

HEALTH POLICY AND HEALTH FINANCE KNOWLEDGE HUB WORKING PAPER SERIES
NUMBER 8 | NOVEMBER 2010 Governance and management arrangements for health Sector-Wide Approaches (SWAPs):Examples from Africa, Asia and the Pacific 3
SWAp GOVERNANCE STRUCTURES: INTERNATIONAL EXAMPLESThe following table summarises information on the management and governance arrangements of seven SWAps or similar arrangements: four in African countries (Zambia, Malawi, Uganda, Mozambique), two in Asia (Cambodia and Bangladesh) and one in a Pacific Island country (Samoa).
In Cambodia the Ministry of Health has adopted sector-wide management or SWiM. Under the SWiM, some funds are pooled (especially from the World Bank through the Health Sector Support Project), and the pooled funds are used within project structures with a commitment to harmonisation and alignment of donor funding in support of the Ministry’s Health Strategic Plan. Despite the somewhat different mechanism and different name, the Cambodian SWiM represents a similar arrangement to SWAps (especially that of the Solomon Islands, which is more focused on harmonisation and alignment rather than pooled funding) and is therefore included in this paper.
The table provides information on key governance elements identified, such as the format of annual reviews, coordination meetings and subgroups. Following it are examples of governance mechanisms from three SWAp countries. The brief then provides more information on the various governance arrangements and other issues for consideration.
The countries with health SWAps and similar arrangements described here are generally larger in terms of population and established their SWAps considerably earlier than the Solomon Islands. Additionally, some of the countries reviewed have considerably more development partners and stakeholders active in the sector than the Solomon Islands. Therefore, caution should be taken in interpreting the examples.

WO
RK
ING
PA
PE
R S
ER
IES
H
EA
LTH
PO
LIC
Y A
ND
HE
ALT
H F
INA
NC
E K
NO
WLE
DG
E H
UB
4 G
over
nanc
e an
d m
anag
emen
t arr
ange
men
ts fo
r hea
lth S
ecto
r-W
ide
App
roac
hes
(SW
AP
s): E
xam
ples
from
Afri
ca, A
sia
and
the
Paci
fic
NU
MB
ER
8 |
NO
VEM
BE
R 2
010
HE
ALT
H P
OLI
CY
AN
D H
EA
LTH
FIN
AN
CE
KN
OW
LED
GE
HU
B
WO
RK
ING
PA
PE
R S
ER
IES
NU
MB
ER
8 |
NO
VEM
BE
R 2
010
Gov
erna
nce
and
man
agem
ent a
rran
gem
ents
for h
ealth
Sec
tor-
Wid
e A
ppro
ache
s (S
WA
Ps)
: Exa
mpl
es fr
om A
frica
, Asi
a an
d th
e Pa
cific
5
Cat
ego
ryS
amo
aZ
amb
iaM
alaw
iU
gan
da
Cam
bo
dia
Mo
zam
biq
ue
Ban
gla
des
h
Po
pul
atio
n20
0,00
013
mill
ion
15 m
illio
n33
mill
ion
15 m
illio
n20
mill
ion
162
mill
ion
Dat
e o
f est
ablis
hm
ent
of S
WA
p20
07E
arly
199
0s20
0419
99S
WiM
ado
pted
in 2
000
2000
1998
SW
Ap
sec
reta
riat
(c
om
po
siti
on
, fu
nd
ing)
SW
Ap
Coo
rdin
atio
n U
nit h
ouse
d an
d ru
n by
gov
ernm
ent.
Rep
orts
to C
EO o
f M
OH
. Com
pose
d of
co
ordi
nato
r, ac
coun
tant
, pr
ocur
emen
t spe
cial
ist
and
four
oth
er s
taff
(all
loca
l).
Dire
ctor
ate
of P
lann
ing
and
Dev
elop
men
t w
ithin
MO
H; d
onor
co
ordi
natio
n of
ficer
with
in M
OH
. E
stab
lishe
d on
ly in
20
03.
SW
Ap
secr
etar
iat i
n th
e P
lann
ing
Uni
t of M
OH
.Te
chni
cal W
orki
ng
Gro
up fo
r Hea
lth
secr
etar
iat h
as
repr
esen
tativ
es o
f MO
H
and
DP
s—fo
rmul
ates
M
&E
indi
cato
rs, a
nnua
l w
ork
plan
s.
Co
ord
inat
ion
com
mit
tees
Pro
gram
Ste
erin
g C
omm
ittee
.
Mem
bers
: Min
istri
es
of H
ealth
, Fin
ance
, S
ocia
l Dev
elop
men
t, D
Ps,
priv
ate
sect
or a
nd
NG
Os.
Func
tion:
pro
vide
hi
gh-le
vel o
vers
ight
for
impl
emen
tatio
n an
d ac
t as
foru
m fo
r vie
ws
and
conc
erns
of p
artn
ers.
Det
ails
: Mee
ts q
uarte
rly.
Cha
ired
by M
OH
or
Fina
nce.
Polic
y C
onsu
ltativ
e M
eetin
g (1
2 pe
r yea
r).
Mem
bers
: MO
H, D
Ps.
Func
tion:
add
ress
ge
nera
l hea
lth s
ecto
r-re
late
d is
sues
.
Det
ails
: pre
side
d ov
er
by th
e P
S.
Hea
lth S
ecto
r Rev
iew
G
roup
.
Mem
bers
: poo
led
and
non-
pool
ed p
artn
ers;
N
GO
s; p
rivat
e se
ctor
.
Func
tion:
revi
ew
impl
emen
tatio
n pr
ogre
ss a
nd a
nnua
l w
ork
plan
s.
Det
ails
: cha
ired
by
MO
H.
Sec
tor W
orki
ng G
roup
.
Mem
bers
: MO
H,
Fina
nce,
DP
s.
Func
tion:
set
bud
get
prio
ritie
s an
d ap
prov
e pr
ojec
ts.
Det
ails
: cha
ired
by P
S.
Hea
lth P
olic
y A
dvis
ory
Com
mitt
ee: m
embe
rs:
MO
H, F
inan
ce,
Educ
atio
n, lo
cal
gove
rnm
ent,
DP
s,
priv
ate
prov
ider
s.
Det
ails
: mee
ts m
onth
ly.
Tech
nica
l Wor
king
G
roup
for H
ealth
.
Mem
bers
: 74
(gov
ernm
ent,
NG
Os,
D
Ps)
.
Func
tion:
focu
s on
br
oade
r stra
tegi
es a
nd
heal
th s
yste
ms.
MO
H T
ask
Forc
e on
Dee
peni
ng
Har
mon
isat
ion
and
Alig
nmen
t.
Mem
bers
: MO
H
Dep
artm
ent o
f In
tern
atio
nal
Coo
pera
tion.
SW
Ap
Foru
m.
Mem
bers
: MO
H a
nd
exte
rnal
par
tner
s.
Det
ails
: Rec
ent p
ush
to
mak
e it
mor
e in
clus
ive
and
incl
ude
all D
Ps.
HN
PS
P C
oord
inat
ion
Com
mitt
ee.
Mem
bers
: MO
H a
nd
two
deve
lopm
ent
part
ners
who
re
pres
ent v
iew
s of
all
deve
lopm
ent p
artn
ers.
Func
tion:
revi
ew
impl
emen
tatio
n pr
ogre
ss (t
o da
te h
as
been
too
form
al a
nd n
ot
focu
sed
on d
etai
l).

WO
RK
ING
PA
PE
R S
ER
IES
H
EA
LTH
PO
LIC
Y A
ND
HE
ALT
H F
INA
NC
E K
NO
WLE
DG
E H
UB
4 G
over
nanc
e an
d m
anag
emen
t arr
ange
men
ts fo
r hea
lth S
ecto
r-W
ide
App
roac
hes
(SW
AP
s): E
xam
ples
from
Afri
ca, A
sia
and
the
Paci
fic
NU
MB
ER
8 |
NO
VEM
BE
R 2
010
HE
ALT
H P
OLI
CY
AN
D H
EA
LTH
FIN
AN
CE
KN
OW
LED
GE
HU
B
WO
RK
ING
PA
PE
R S
ER
IES
NU
MB
ER
8 |
NO
VEM
BE
R 2
010
Gov
erna
nce
and
man
agem
ent a
rran
gem
ents
for h
ealth
Sec
tor-
Wid
e A
ppro
ache
s (S
WA
Ps)
: Exa
mpl
es fr
om A
frica
, Asi
a an
d th
e Pa
cific
5
Cat
ego
ryS
amo
aZ
amb
iaM
alaw
iU
gan
da
Cam
bo
dia
Mo
zam
biq
ue
Ban
gla
des
h
Dev
elo
pm
ent p
artn
er
onl
y co
ord
inat
ion
foru
ms
Non
e.N
one.
Hea
lth d
onor
sub
grou
p re
port
s to
Hea
lth S
ecto
r R
evie
w G
roup
.
Hea
lth D
evel
opm
ent
Part
ners
Gro
up m
eets
m
onth
ly to
coo
rdin
ate.
O
ne a
genc
y se
rves
as
chai
r and
con
tact
poi
nt
with
MO
H.
Hea
lth P
artn
ers
Gro
up
(onl
y D
Ps)
.N
one.
Don
or c
onso
rtiu
m
mee
ting
incl
udes
all
DP
s.
Sep
arat
e m
eetin
g fo
r poo
led
fund
ing
part
ners
.
An
nu
al r
evie
ws
Hea
lth s
umm
it in
M
arch
and
join
t re
view
in S
epte
mbe
r ea
ch y
ear o
rgan
ised
by
gov
ernm
ent.
All
part
ners
invi
ted,
in
clud
ing
civi
l soc
iety
an
d pr
ivat
e se
ctor
.
Ann
ual c
onsu
ltativ
e m
eetin
g; s
ecto
r ad
viso
ry g
roup
mee
ting
(2 p
er y
ear).
Mul
ti-st
akeh
olde
r joi
nt
revi
ews
held
twic
e ea
ch y
ear w
ith a
ides
-m
emoi
res
aris
ing
from
re
view
s. C
oord
inat
ed b
y S
WA
p se
cret
aria
t.
Join
t rev
iew
s he
ld tw
ice
each
yea
r. P
rogr
ess
is re
view
ed a
nd p
lans
ar
e ag
reed
for c
omin
g si
x m
onth
s, in
clud
ing
prio
ritie
s an
d bu
dget
al
loca
tions
.
Con
duct
ed th
roug
h th
e ro
utin
e ac
tiviti
es o
f the
M
OH
; inc
lude
s an
nual
he
alth
con
gres
s an
d an
nual
ope
ratio
nal p
lan.
Sec
tor C
oord
inat
ion
Com
mitt
ee m
eets
tw
ice
a ye
ar, c
haire
d by
Min
iste
r of H
ealth
, in
clud
es M
OH
and
DP
s.
Ann
ual p
rogr
am re
view
in
clud
es jo
int fi
eld
visi
ts
and
revi
ew o
f pro
gres
s.
Sec
tora
l sub
gro
ups
Non
e.Ye
s, in
clud
ing
finan
cing
, hu
man
reso
urce
s,
proc
urem
ent a
nd
tech
nica
l are
as.
Tech
nica
l wor
king
gr
oups
incl
udin
g pr
ocur
emen
t, hu
man
re
sour
ces.
Incl
udes
D
Ps.
Eigh
t wor
king
gr
oups
, inc
ludi
ng
hum
an re
sour
ces,
in
frast
ruct
ure,
fina
nce,
m
onito
ring.
A n
umbe
r of
prog
ram
mat
ic a
nd
dise
ase-
spec
ific
tech
nica
l wor
king
gr
oups
.
SW
Ap
-rel
ated
them
atic
w
orki
ng g
roup
s—w
here
m
ore
in-d
epth
ana
lysi
s is
nee
ded
prio
r to
broa
der f
orum
s.
Non
e.
Mem
ora
nd
um
of
Un
der
stan
din
gA
join
t par
tner
ship
ar
rang
emen
t des
crib
es
the
prin
cipl
es o
f the
S
WA
p, ro
les
and
resp
onsi
bilit
ies
of D
Ps
and
gove
rnm
ent.
Hea
lth M
OU
and
Joi
nt
Ass
ista
nce
Stra
tegy
bo
th s
igne
d.
MO
U b
etw
een
DP
s an
d M
OH
. Ref
ers
to c
oord
inat
ion
and
mon
itorin
g, fi
nanc
ing
arra
ngem
ents
.
SW
Ap
MO
U.
Cur
rent
ly n
o S
WA
p M
OU
; the
pro
cess
op
erat
es a
s a
SW
iM
with
DP
and
MO
H
agre
emen
t.
Cod
e of
con
duct
that
se
ts th
e ba
sic
rule
s of
en
gage
men
t bet
wee
n th
e M
OH
and
par
tner
s.
Not
es:
1. S
WiM
: Sec
tor-
Wid
e M
anag
emen
t; D
P: D
evel
opm
ent P
artn
er; M
OU
: Mem
oran
dum
of U
nder
stan
ding
; MO
H: M
inis
try
of H
ealth
; NG
O: N
on-G
over
nmen
t Org
anis
atio
n; M
&E
: Mon
itorin
g an
d E
valu
atio
n; P
S: P
erm
anen
t Sec
reta
ry; H
NP
SP
: Hea
lth
Nut
ritio
n P
opul
atio
n S
ecto
r Pro
gram
2. T
he in
form
atio
n in
the
tabl
e w
as c
ompi
led
from
a re
view
of n
umer
ous
doc
umen
ts, a
ll lis
ted
in th
e “C
ited
refe
renc
es a
nd o
ther
sou
rces
” se
ctio
n. F
or s
impl
icity
, the
sum
mar
y he
re d
oes
not c
ite th
ese
sour
ces.

WORKING PAPER SERIES HEALTH POLICY AND HEALTH FINANCE KNOWLEDGE HUB
Governance and management arrangements for health Sector-Wide Approaches (SWAPs): NUMBER 8 | NOVEMBER 2010Examples from Africa, Asia and the Pacific6
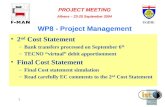
EXAMPLES OF SWAp MANAGEMENT STRUCTURESExamples of SWAp management structures and reporting lines in three countries are provided here in graphic form to demonstrate the variety of systems developed.
Malawi• SWApmanagementstructureisownedandcentredontheMinistryofHealth(MOH),withtheSWAp
secretariat housed within MOH and reporting to MOH management committees.
• HealthSectorReviewGroupincludesMOHanddevelopmentpartnersaswellasNGOsandprivatesectorand reports to MOH (and consults with SWAp secretariat). (DFID 2004)
Technical Working Groups
Financial Management and Procurement Working Group
Human Resources Working Group
Ad hoc groups
Cabinet Committee on Health Parliamentary Health Committee
Health Sector Review Groups
Co-chaired Ministry/Dxxxx, NGOs, private sector providers.
Health Sub- Groups
SWAp
Secretariat
Zonal Offices
Top Management Committee
Chair: Health Minister, also Treasury, Local Government, Economic Planning.
Departmental Meetings and Committees
Senior Management Committee
Chair: Principal Secretary of Health, Health Directors, Central Hospitals, Professional Councils.

HEALTH POLICY AND HEALTH FINANCE KNOWLEDGE HUB WORKING PAPER SERIES
NUMBER 8 | NOVEMBER 2010 Governance and management arrangements for health Sector-Wide Approaches (SWAPs):Examples from Africa, Asia and the Pacific 7
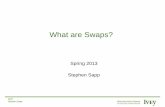
Uganda• HealthPolicyAdvisoryCommitteemeetsmonthlyandincludesdevelopmentpartners,governmentand
private providers.
• HealthdevelopmentpartnersonlymeetmonthlyandreporttoHealthPolicyAdvisoryCommittee. (Hutton 2004)
Top Management Committee*
Sector Working Group*Health Policy Advisory Comittee*
Partnership Fund
Working Groups*
Office of the Minister
Permanent Secretary
Director General
MoH Structure
Inter-Agency Coordinating Committees*
Senior Management Committee*
Health Developement Partners* (HDP Group)

WORKING PAPER SERIES HEALTH POLICY AND HEALTH FINANCE KNOWLEDGE HUB
Governance and management arrangements for health Sector-Wide Approaches (SWAPs): NUMBER 8 | NOVEMBER 2010Examples from Africa, Asia and the Pacific8
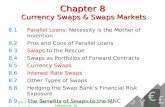
Bangladesh• MinistryofHealthanddevelopmentpartnersbothcontributetoannualprogramreview.
• Separatecoordinationforumsexistforpoolfundersandforalldevelopmentpartners (including non-pooled partners).
• RecentlyestablishedHealthNutritionPopulationSectorProgrammeCoordinationCommitteemeetsquarterly and includes two development partners who represent the wider donor consortium (Sundewall, Forsberg et al 2006)
Donor Consortium (All development partners)
Development Partners
HPSO Steering Committee (Pool funders)
Annual Programme Review/Policy Dialogue
Ministry of Health and Family Welfare
Directorate of Family Planning
Directorate of Health Services

HEALTH POLICY AND HEALTH FINANCE KNOWLEDGE HUB WORKING PAPER SERIES
NUMBER 8 | NOVEMBER 2010 Governance and management arrangements for health Sector-Wide Approaches (SWAPs):Examples from Africa, Asia and the Pacific 9
SUMMARY OF GOVERNANCE AND MANAGEMENT ISSUESSWAp SecretariatsSome, but not all, countries with health SWAps have formally convened SWAp secretariats. Samoa, Zambia and Malawi—some of the countries with the strongest SWAps—have secretariats based within the MOH and reporting to the Minister of Health.
The SWAp secretariat manages the day-to-day functioning of the SWAp, including donor coordination, accounting and procurement related to SWAp funds and other management roles.
Zambia explicitly places its SWAp secretariat as the go-between for development partners and the government. In other countries, management functions are retained within regular MOH functions.
Coordination CommitteesThough named differently, ongoing coordination mechanisms between various health sector stakeholders exist in each SWAp country. All include development partners and government. Government representatives are generally from the central MOH but sometimes also include finance, education, social development and other relevant Ministries involved in the health sector response.
Most but not all include others, such as private providers and NGOs. Both pooled and non-pooled partners are included.
All of the coordination committees are chaired by government representatives—most commonly from the MOH but occasionally from other Ministries. These bodies variously review progress, develop work plans, support implementation and discuss issues as they arise.
In Bangladesh, coordination meetings, which included the full suite of development partners, were deemed to be too large to permit meaningful discussion.
Development-Partner-Only Coordination ForumsMost countries do not have formal coordination forums exclusively for development partners. Malawi, Bangladesh and Uganda, however, all maintain development-partner-only forums that then report a coordinated perspective to a wider meeting including the national government. The development partner forums generally share information about program planning and program assessments and seek to reduce transaction costs for both agencies and government.
Bangladesh’s recently established Health Nutrition Population Sector Programme Coordination Committee meets approximately quarterly and is made up of senior MOH officers and two development partners, the latter representing the views of the wider partner community.
Analysis of sector coordination in Zambia reveals that even without a formal development partner forum, informal gatherings of donors still occur. According to one report: ‘a number of issues get discussed “over a cup of coffee”’ and ‘… in the past the Ministry has expressed opposition to such gatherings, rejecting any need to exclude policy-makers in a climate of openness and consultation. However, their continued existence demonstrates the inevitability of donor-donor communication.’ Furthermore, ‘senior MOH officials welcome the opportunity for partners to present a common position’ (Lake and Musumali 1999).
In the 1990s, Mozambique tried appointing one donor as the focal point to interface between the MOH and the donor community to relieve the MOH of part of the burden of discussing every issue with each agency. This endeavour was ultimately abandoned, however, as it was felt by both the MOH and other development partners that the focal donor had become too influential (Pavignani and Durao 1999).

WORKING PAPER SERIES HEALTH POLICY AND HEALTH FINANCE KNOWLEDGE HUB
Governance and management arrangements for health Sector-Wide Approaches (SWAPs): NUMBER 8 | NOVEMBER 2010Examples from Africa, Asia and the Pacific10
Annual ReviewsAll SWAp countries have annual or biannual processes to review performance, develop a program of work for the upcoming year and agree on financial contributions. Some countries go down to the level of a procurement plan for the upcoming year.
Development partners generally prepare detailed reports on what they have done over the past year and specific details on what they plan to do in the coming year. In this way, the development partners work around an agreed national calendar or timetable.
One document in Mozambique noted that ‘a serious concern has been the lack of systematic follow up’ by the MOH and development partners of the recommendations made in the annual review. The document lamented that the reports emerging from the review were ‘not followed by implementation plans’ that facilitated and directed action (Martinez 2006).
Sectoral SubgroupsMost SWAps, in addition to coordination mechanisms and reviews, have subgroups that provide forums for in-depth discussions on technical issues related to SWAp functioning such as human resources, monitoring, procurement and finance. A number of countries also maintain disease-specific technical working groups. All of these subgroups report back to the SWAp secretariat or coordination mechanism.
Memoranda of UnderstandingMost countries with SWAps have some sort of agreement between development partners and the government (though most do not include private sector organisations or NGOs).
Overall, MoUs set the basic rules of engagement between the government and development partners. MoUs can describe some combination of the principles of the SWAp, roles and responsibilities of the development partners and the government related to the SWAp, institutional and fiduciary arrangements, approach to capacity building, monitoring and evaluation, disbursement arrangements for contributions of the pooled partners, conflict resolution and steps for adding new partners to the pooled arrangement.
Involvement of Non-State ActorsA number of sector coordination mechanisms include only the government and development partners, to the exclusion of non-state actors such as faith-based organisations, NGOs and the private sector. Malawi and Uganda, however, in which private providers and NGOs deliver a significant percentage of health services, both include non-state actors in their ongoing coordination meetings. Most annual or biannual reviews include a wide range of the health sector, including NGOs and private/not-for-profit providers such as churches. Commentators have acknowledged that ‘the role of NGOs in the SWAp process has all along been ambiguous’ (Jeppsson 2002).
Separate HIV Coordination MechanismsA number of countries (such as Mali, Madagascar and Mozambique) that have well-developed coordination for the health sector maintain separate mechanisms for coordination of the HIV response. This is partly due to the Global Fund requirement to have a country coordinating mechanism with specific membership requirements.
Following from this, in a few countries, technical units of the MOH continue to operate in a vertical fashion, holding technical meetings with donors, arranging separate training workshops and generally not coordinating activities and plans centrally. In Mozambique, technical departments maintain close links with technical partners that hinder central coordination.
Technical Assistance to SWAp SecretariatsFor SWAps in Africa, donors including the World Bank and the UK Department for International Development (DFID) have provided technical assistance in the establishment and initial staffing of SWAp secretariats. Technical assistance is thus provided explicitly with a clear mentoring and capacity-building role to strengthen the government’s ability to manage the SWAp.

HEALTH POLICY AND HEALTH FINANCE KNOWLEDGE HUB WORKING PAPER SERIES
NUMBER 8 | NOVEMBER 2010 Governance and management arrangements for health Sector-Wide Approaches (SWAPs):Examples from Africa, Asia and the Pacific 11
The Samoan SWAp secretariat has recently hired one adviser focused on procurement (of items as diverse as vehicles, civil works, pharmaceuticals and information technology equipment) and one on program management, who are both international advisers and are both donor funded. The technical assistance was in response to discussions between development partners and government on SWAp secretariat needs and skill gaps.
Documents describing the Malawi SWAp went into significant detail on technical assistance. The Malawi MOH and the SWAp donor group conducted a human resources needs assessment that included effective SWAp management. The technical assistance needs identified were to be funded through the SWAp and included procurement specialists, human resources management specialists, M&E specialists and financial management specialists.
The ten technical assistant (TA) posts in Malawi were recruited directly by the MOH through a competitive and open process facilitated by one of the SWAp partners, and the funds for the posts were provided by DFID. The advisers are managed and monitored by the MOH—this differed from the past, when technical assistants reported to the funding donor.
A review of past technical assistance in Malawi (Malawi MOH and Health SWAp Donor Group 2007) revealed that although the assistance was effective in terms of output, the impact of capacity building and skills transfer was often very poor due to lack of government counterparts for technical advisors or insufficient focus by the adviser. Improvement in capacity building is part of the commitment for new technical assistance, and the long-term objective of SWAp partners is to phase out technical assistance over a ten to fifteen year period.
The needs assessment in Malawi is to be conducted annually, with procurement of assistance to respond to needs identified. Technical assistance is funded from within the pooled funding.
CONCLUSIONThe various SWAps and similar arrangements have all adapted their management mechanisms to suit local circumstances and needs. Despite this, a few common trends appear, including formal annual or biannual sector reviews, monthly sector coordination meetings and a secretariat within the MOH that manages the day-to-day elements of the SWAp. In countries with many donors, some have tried separate donor coordination forums to allow for a coordinated donor perspective. Separate disease-specific coordination bodies have also been attempted, but the trend seems to be towards a more streamlined whole-of-sector approach. Importantly, most countries’ management arrangements have changed over time in response to challenges and shortcomings, suggesting that SWAp governance must be dynamic and must be evaluated frequently to ensure that it is functioning effectively.

WORKING PAPER SERIES HEALTH POLICY AND HEALTH FINANCE KNOWLEDGE HUB
Governance and management arrangements for health Sector-Wide Approaches (SWAPs): NUMBER 8 | NOVEMBER 2010Examples from Africa, Asia and the Pacific12
CITED REFERENCES AND OTHER SOURCESBoesen, N. and D. Dietvorst. 2007. SWAps in motion: Sector wide approaches—from an aid delivery to a sector development perspective. http://www.swisstph.ch/fileadmin/user_upload/Pdfs/swap/swap456_Boesen_2007.pdf (accessed 14 January 2010).
Carlson, C., M. Boivin, A. Chirwa, Simon Chirwa, Fenwick Chitalu, Geoff Hoare, Mechtild Huelsmann, Wedex Ilunga, Ken Maleta, Andrew Marsden, Tim Martineau, Chris Minett, Albert Mlambala, Friedrich von Massow, Hatib Njie and Ingvar Theo Olsen. 2008. Malawi health SWAp mid-term review: Summary report. Norad Collected Reviews 22/2008. Oslo: Norwegian Agency for Development Cooperation.
Chansa, C. 2007. Zambian health SWAp revisited—has it made the intended effects? http://www.gtz.rhp.com/conferences/madagascar07/ChansaCollins_final.pdf (accessed 14 January 2010).
Chansa, C., J. Sundewall, D. McIntyre, G. Tomson and B.C. Forsberg. 2008. Exploring SWAp’s contribution to the efficient allocation and use of resources in the health sector in Zambia. Health Policy & Planning 23(4): 244-251.
DFID. 2004. Improving health in Malawi. £100 million UK aid (2005/6-2010/11). A sector wide approach including essential health package and emergency human resources programme. Programme memorandum. UK Department for International Development.
http://www.u4.no/themes/health/dfidmalawifinalreport.pdf (accessed 14 January 2010).
Hutton G. 2004. Case study of a successful’ sector-wide approach: the Uganda health sector SWAp. A lessons learned paper established in the frame of the SDC-STI SWAp Mandate 2003-4. http://www.sti.ch/fileadmin/user_upload/Pdfs/swap/swap351.pdf (accessed 14 January 2010).
International Health Partnership. 2008. Cambodia Taking Stock Report. http://www.internationalhealthpartnership.net/pdf/03_CAMBODIA_TSR_EN_FINAL.pdf (accessed 14 January 2010).
International Health Partnership. 2008. Madagascar Taking Stock Report. http://www.internationalhealthpartnership.net/pdf/05_MADAGASCAR_TSR_EN_FINAL.pdf (accessed 14 January 2010).
International Health Partnership. 2008. Mali Taking Stock Report. http://www.internationalhealthpartnership.net/pdf/06_MALI_TSR_EN_FINAL.pdf (accessed 14 January 2010).
International Health Partnership. 2008. Mozambique Taking Stock Report. http://www.internationalhealthpartnership.net/pdf/07_MOZAMBIQUE_TSR_EN_FINAL.pdf (accessed 14 January 2010).
International Health Partnership. 2008. Nepal Taking Stock Report. http://www.internationalhealthpartnership.net/pdf/08_TSR_Nepal_FINAL_July_2008.pdf (accessed 14 January 2010).
International Health Partnership. 2008. Zambia Update: Scaling-Up for Better Health. http://www.internationalhealthpartnership.net/pdf/IHP%20Update%2013/MINISTERIAL/Zambia.pdf (accessed 14 January 2010).
Jeppsson, A. 2002. SWAp dynamics in a decentralized context: experiences from Uganda. Social Science & Medicine. 55(11): 2053-2060.
Lake S., and C. Musumali. 1999. Zambia: The role of aid management in sustaining visionary reform. Health Policy & Planning 14(3): 254-263.
Malawi Ministry of Health and Malawi Health SWAp Donor Group. 2007. Human resources / capacity development within the health sector needs assessment study: Final report. http://www.jica.go.jp/cdstudy/library/pdf/c20071127_05.pdf (accessed 14 January 2010).
Martinez, J. 2006. Implementing a sector wide approach in health: the case of Mozambique. London: HLSP Institute.
Martinez, J. 2008. Sector wide approaches at critical times: the case of Bangladesh. London: HLSP Institute.

HEALTH POLICY AND HEALTH FINANCE KNOWLEDGE HUB WORKING PAPER SERIES
NUMBER 8 | NOVEMBER 2010 Governance and management arrangements for health Sector-Wide Approaches (SWAPs):Examples from Africa, Asia and the Pacific 13
Örtendahl C., 2007. The Uganda health SWAp: new approaches for a more balanced aid architecture? London: HLSP Institute.
Pavignani, E. and J.R. Durao. 1999. Managing external resources in Mozambique: building new aid relationships on shifting sands? Health Policy & Planning 14(3): 243-253.
Sundewall, J., B.C. Forsberg and G. Tomson. 2006. Theory and practice—a case study of coordination and ownership in the Bangladesh health SWAp. Health Research Policy and Systems 16, 4: 5.
Sundewall, J. and K. Sahlin-Andersson. 2006. Translations of health sector SWAps—a comparative study of health sector development cooperation in Uganda, Zambia and Bangladesh. Health Policy 76(3): 277-287.
Walt, G., E. Pavignani, L. Gilson and K. Buse. 1999. Managing external resources in the health sector: are there lessons for SWAps (sector-wide approaches)? Health Policy and Planning 14(3): 273-284.
White, H. 2007. The Bangladesh health SWAp: Experience of a new aid instrument in practice. Development Policy Review 25(4): 451-472.
World Bank. 2008. Project appraisal document of the World Bank on a proposed credit in the amount of SDR 1.9M to the independent state of Samoa in support of health sector management project. http://www-wds.worldbank.org/external/default/wdscontentserver/wdsp/iv/2008/06/03/000333037_20080604000524/rendered/pdf/411300pad0p0861ly10ida1r20081017911.pdf (accessed on 14 January 2010).

14
KNOWLEDGE HUBS FOR HEALTHStrengthening health systems through evidence in Asia and the Pacific
A strategic partnerships initiative funded by the Australian Agency for International Development
The Nossal Institute for Global Health