Gordon principles and practice of surgery for the colon rectum and anus 3rd ed
1354
-
Upload
scu-hospital -
Category
Health & Medicine
-
view
251 -
download
12
Transcript of Gordon principles and practice of surgery for the colon rectum and anus 3rd ed
- 1. Principles and Practice of Surgery for the Colon, Rectum, and Anus Third Edition New York London Philip H. Gordon M.D., F.R.C.S. (C), F.A.C.S., F.A.S.C.R.S., Hon. F.R.S.M., Hon. F.A.C.G.B.I Professor of Surgery and Oncology, McGill University Director of Colon and Rectal Surgery Sir Mortimer B. Davis-Jewish General Hospital and McGill University Montreal, Quebec, Canada Santhat Nivatvongs M.D., F.A.C.S., F.A.S.C.R.S., Hon. F.R.C.S.T. (Thailand), Hon. F.R.A.C.S. Consultant Surgeon and Professor of Surgery Mayo Clinic College of Medicine Rochester, Minnesota, U.S.A. ILLUSTRATORS Scott Thorn Barrows, C.M.I., F.A.M.I Director and Clinical Assistant Professor, Biomedical Visualization University of Illinois at Chicago Medical Center with the assistance of Carla Gunn, Gregory Blew, David Ehlert, Craig Kiefer, and Kim Martens
- 2. Informa Healthcare USA, Inc. 270 Madison Avenue New York, NY 10016 2007 by Informa Healthcare USA, Inc. Informa Healthcare is an Informa business No claim to original U.S. Government works Printed in the United States of America on acidfree paper 10 9 8 7 6 5 4 3 2 1 International Standard Book Number10: 0824729617 (Hardcover) International Standard Book Number13: 9780824729615 (Hardcover) This book contains information obtained from authentic and highly regarded sources. Reprinted material is quoted with permission, and sources are indicated. A wide variety of references are listed. Reasonable efforts have been made to publish reliable data and information, but the author and the publisher cannot assume responsibility for the validity of all materials or for the consequences of their use. No part of this book may be reprinted, reproduced, transmitted, or utilized in any form by any electronic, mechanical, or other means, now known or here after invented, including photocopying, microfilming, and recording, or in any information storage or retrieval system, without written permission from the publishers. For permission to photocopy or use material electronically from this work, please access www.copyright.com (http://www.copyright.com/) or contact the Copy right Clearance Center, Inc. (CCC) 222 Rosewood Drive, Danvers, MA 01923, 9787508400. CCC is a notforprofit organization that provides licenses and registration for a variety of users. For organizations that have been granted a photocopy license by the CCC, a separate system of payment has been arranged. Trademark Notice: Product or corporate names may be trademarks or registered trademarks, and are used only for identification and explanation without intent to infringe. Library of Congress CataloginginPublication Data Gordon, Philip H. Principles and practice of surgery for the colon, rectum, and anus / by Philip H. Gordon, Santhat Nivatvongs. 3rd ed. p. ; cm. Includes bibliographical references and index. ISBN13: 9780824729615 (alk. paper) ISBN10: 0824729617 (alk. paper) 1. Colon (Anatomy)Surgery. 2. RectumSurgery. 3. AnusSurgery. I. Nivatvongs, Santhat. II. Title. [DNLM: 1. Colonic Diseasessurgery. 2. Anus Diseasessurgery. 3. Colorectal Neoplasmssurgery. 4. Rectal Diseasessurgery. WI 520 G664p 2006] RD544.G67 2006 617.5547dc22 2006050379 Visit the Informa Web site at www.informa.com and the Informa Healthcare Web site at www.informahealthcare.com
- 3. Contributors Peter A. Cataldo & Associate Professor of Surgery, University of Vermont College of Medicine, Fletcher Allen Health Care, Burlington, Vermont, U.S.A. Jean MacDonald & E.T. Nurse Consultant, Sir Mortimer B. DavisJewish General Hospital, Montreal, Quebec, Canada W. Rudolf Schouten & Department of Surgery, Division of Colon and Rectal Surgery, University Hospital Dijkzigt, Rotterdam, The Netherlands Lee E. Smith & Clinical Professor of Surgery, George Washington University, Director, Section of Colon and Rectal Surgery, Washington Hospital Center, Washington, D.C. iii
- 4. I am once again deeply indebted to my wife Rosalie for her constant patience and understanding through the burden of this third edition. Her constant life-long support has made all my professional accomplishments possible. To my wonderful children Laurel and Elliot of whom I am extremely proud. My love and gratitude to all. PHG To my two angels Marisa and Nitara. Thinking of them makes me smile; talking to them recharges my energy. SN
- 5. Preface to the Third Edition In the rst edition of this textbook our goal was to produce a comprehensive book that would encompass the gamit of colon and anorectal diseases. It was not intended to be encyclopedic but to provide information for the busy sur- geon who needed to extract information as quickly as possible. With this in mind, the contents were divided into ve major sections that we have been told were helpful and so we have maintained the basic format through the second and third editions. In the eight years that have elapsed since our last edi- tion, the proliferation of information published in the surgical literature makes it necessary to update and elabo- rate on these developments. Highlights in the revision include a new discussion of fascial attachments of the rec- tum and relationship to the lateral pelvic wall with specic reference to the application for operations on rectal carcinoma. Newer pharmacologic effects on the internal sphincter and new investigative modalities for anorectal physiology are described. The value and role of virtual colonoscopy is discussed as is the controversy regarding the need for mechanical bowel preparation. There is a detailed description of the newest modality of hemorrhoid therapy, namely the stapler hemorrhoidopexy and its potential role in the armamentarium of hemorrhoid treat- ment. An extensive section on pharmacologic therapy for ssure-in-ano has been added and the efcacy of various agents for chemical sphincterotomy are described. The value of intra-anal ultrasound and MRI in the diagnosis of complicated recurrent stula-in-ano have been high- lighted as has the efcacy of brin glue. A new section on the technique of the repair of rectourethral stula has been added. Topical agents for condyloma accuminata and drugs and their dosage for various sexually trans- mitted diseases have been updated. An extensive review on the therapy for fecal incontinence including the articial sphincter, hyperbaric oxygen, Secca procedure, implanta- tion of silicone biomaterial and detailed description of sacral neuromodulation has been added. The chapter on the etiology and management of peri- anal neoplasms and anal carcinoma has been extensively revised reecting new information, in particular the discus- sion on anal intraepithelial neoplsia (AIN). This included the new method of diagnosis and management of high grade AIN of the perianal skin or Bowens disease. In the benign neoplasms chapter, the relatively new interest and better understanding of serrated adenoma has been added. The hot topic on the management of malignant polyps of the low rectum has been updated. Information on uncommon benign polyps has been expanded. New data regarding the incidence, prevalence, and trends in colorectal carcinoma are included. There is an update on the genetics of colorectal carcinoma in general and in particular HNPCC. Extensive discussion of the indi- cations for and interpretation of genetic testing and the invaluable role of genetic counseling are described in detail. There is an update on the propriety of adjuvant therapy with its limitations and complications and possible ne tuning of indications for adjuvant therapy. There is updated informa- tion on the treatment of recurrent metastatic carcinoma providing prognostic indicators for recurrence following therapy. A section on intra-luminal stenting for obstruction has been added. There is new information on the staging of rectal carcinoma. There is revised description of sphincter saving operations (pouch, coloplasty, coloanal anastomosis). There is a discussion of total mesorectal excision with results of the use of this technique. There are updated results on the treatment of carcinoma of the rectum with a discussion of the propriety of the use of local excision of rectal carcinoma. There is expansion on the section on palliative management of patients with rectal carcinoma and there is a discussion on the role of preoperative neoadjuvant treatment for rectal carcinoma. A new section on the management of presacral bleeding has been included. Screening, surveillance, and fol- low-up for large bowel carcinoma continue to evolve rapidly with better understanding. The new algorithm for colorectal carcinoma screening has been revised. The controversy in the surveillance after surgery has been laid out as guidelines from different major societies and institutions. The controversy on ileal pouch-anal anastomosis (IPAA) as primary treatment of chronic ulcercative colitis has been claried. A better understanding of the risk of car- cinoma in the ileal pouch and the retained anal canal is elucidated. The management of chronic pouchitis now includes immunosuppressive drugs. The long-term out- come of IPAA is now better understood. The Crohns disease chapter has been extensively revised with an elabo- rate discussion on the natural history and classication of the disease and an extensive discussion of the medical therapies with their limitations and the consideration of chemoprevention of colorectal carcinoma in inammatory bowel disease. The changing paradigm regarding the indi- cations for elective operation in diverticular disease has been revisited along with the most recent data on results of the treatment of diverticulitis. The laparoscopy chapter has been totally revised and expanded. The indications for laparoscopic colectomy have been revisited and expanded as newer technology has become available and increased experience has been gained. The new instrumen- tation of equipment that is available has been outlined including subjects such as handports and robotic surgery. Techniques of laparoscopic colectomy have been added. The results of laparoscopic colectomy, conversion rates, detailed morbidity, and mortality by disease process have been updated. Difcult situations such as obesity, vii
- 6. inammatory masses, and stulas have been described. Quality of life and cost issues have been included. A major expansion of the complications, including incidence and prevention of complications with laparoscopic colectomy have been described. In the miscellaneous chapter, an entire new section on colon interposition has been added. The book is replete with color illustrations and photo- graphs adjacent to the text material rather than grouped at the beginning, middle, or end of the book. New illustrations have been added and others redrawn to conform to better understanding and improvement in operative technique. Color has been added to many previous black and white illustrations to enhance the visual image and better display the anatomic details. Each chapter is heavily referenced. We hope we have accomplished our goal of summar- izing the enormous body of knowledge published in the literature and share our personal experience and prefer- ences with our readers. We strove for a book that strikes a balance of being authoritative and detailed without being so inclusive that somewhat irrelevant material and minutia are included. We sincerely hope our efforts will provide the practicing surgeon and surgeon in training, the appropriate information to permit them to provide a rational and up-to- date course of action to the ultimate benet of each of their patients. Philip H. Gordon Santhat Nivatvongs viii & PREFACE TO THE THIRD EDITION
- 7. Preface from the Second Edition Seven years have elapsed since the rst edition of this book was published and we have been amazed at the new devel- opments relevant to diseases affecting the colon, rectum, and anus that have occurred in that relatively short span of time. Some of these developments have been an out- growth of the increased knowledge of the disease process and the underlying genetic factors that inuence it. Others are a reection of more sophisticated modalities of investi- gation such as intrarectal ultrasonographic assessment of rectal carcinoma and positron emission tomography (PET) scanning for recurrent carcinoma or improved thera- peutic options such as sphincter-saving operations and newer procedures for fecal incontinence. Added to this is the yet undened and still controversial role of laparo- scopic operations to manage a host of colon and rectal disorders. This proliferation of knowledge has prompted a major revision of the last edition of this book. Parts have been entirely rewritten (perianal and anal canal neoplasms, early detection and follow-up of large bowel carcinoma, and ischemic colitis), others have been extensively updated (anal incontinence and adjuvant therapy for colorectal car- cinoma), whereas still others have been greatly expanded (ssures and Crohns disease). An entirely new chapter on laparoscopy has been added in view of the current inter- est in this technique. The exciting new developments in the genetics of colorectal carcinoma have received the in-depth coverage they deserve. In our quest to present a balanced view throughout this book, this endeavor has become almost encyclopedic. As a result, this textbook has even grown beyond its origi- nal intimidating size. Despite the size, we have tried to make this information readily accessible to our readers while maintaining the authors personal imprint. There- fore, we have preserved our prerogative to state our preferences when applicable and to reect our individual perspectives. The basic organization of the subject matter has also been maintained to permit ready access to infor- mation which we have attempted to present in a systematic format. New illustrations have been added and others have been redrawn to better clarify procedures or disease processes and to further enhance the learning process. A comprehensive bibliography also accompanies each chapter. We hope we have accomplished our goal of summar- izing the staggering body of current knowledge and sharing our own personal experience and preferences with our readers. Our ultimate objective has been to address the needs of practicing surgeons, gastroenterologists, other physicians, residents in training, and medical students so that they can develop a rational course of action for each individual patient. Philip H. Gordon Santhat Nivatvongs ix
- 8. Preface from the First Edition The creation of any medical textbook begins as a labor of love but rapidly takes on a life of its own. This book was no exception. Our goal was to produce a comprehensive textbook that would encompass the gamut of colon and anorectal diseases. Emphasis was placed on the fundamen- tals of disease, with explanation of etiology and pathogenesis given when applicable, so that the rationale of the proposed treatment would be better understood. In addition to the what and why, the reader will learn when and how to institute therapy. This book is not simply a revision or extension of our previous book, Essentials of Anorectal Surgery. Since the concepts, thoughts, and practices of colon and rectal surgery have changed a great deal during the past decade, current thinking is presented here. This book was not intended to be encyclopedic. It was written with the busy practicing surgeon in mindthe sur- geon who needs to extract information as quickly and easily as possible. Therefore we have divided the contents of the book into ve major sections. Since our aim was to be both practical and didactic, we have included theory along with detailed descriptions of operative procedures. Part I covers anatomy and physiology and discusses the general principles of investigation and preparation of the patient for operation. Part II focuses on anorectal disor- ders, offering discussions of the various disease entities. It also includes a chapter that highlights outpatient proce- dures, which play an increasingly important role in the management of patients with anorectal disorders. Part III describes colorectal disorders and their management. Cer- tain subjects that are combined in a miscellaneous chapter in other books have been ascribed chapter status here. We believe that this arrangement offers a great convenience to the reader. Part IV groups a series of subjects related to problem solving. For example, we have chosen to present together the complications of diseases and their manage- ment and the complications of colorectal operations rather than to repeat these discussions in several chapters. Part V comprises a group of miscellaneous entities. A number of this books special features are worthy of comment. Principles and Practice of Surgery for the Colon, Rec- tum, and Anus is the rst textbook on colon and rectal surgery to incorporate the liberal use of color. It contains 956 illustrationsx-rays, photographs, and drawings 300 of which are in color. We strongly believe that the use of color will enhance the readers understanding of the material. A prime example is the chapter on perianal der- matologic disease, which is greatly strengthened by the addition of color. We realize that the chapters on malignant neoplasms of the colon and the rectum arc lengthy, but the importance of the subject matter mandates the amount of material included. Indeed, certain subsections were inten- tionally abbreviated but extensively referenced. The chapter on diverticular disease is also long, but because of the controversial nature of the management of this dis- ease, the size was deemed necessary to provide a full account of the problem. One subject that is often not ade- quately addressed in textbooks is the construction and care of stomas. In contrast, we believe that this topic is important enough to command an entire chapter. Constipa- tion, which is only a symptom, may present such a challenge to the treating physician that a separate chapter has been devoted to it. Finally, an innovative chapter on unexpected intraoperative ndings was included to help meet those demanding situations that test the skill and ingenuity of the surgeon. In discussions of all controversial issues, an effort was made to present an even-handed and fair presentation of the problem but always to provide the reader with the preference of the author. We hope that the reader, who might be any surgeon or surgeon-in-training who has an interest in the treatment of colorectal disease, will nd both the information in this book and its presentation useful. We trust that the numer- ous illustrations and the use of color will facilitate understanding and allow us to achieve our goal. Philip H. Gordon Santhat Nivatvongs xi
- 9. Acknowledgments Preparation of a major textbook involves the cooperation and contributions of many people and we would like to acknowledge the assistance of several individuals. We are most grateful for the continued friendships, contributions, and support of Lee E. Smith, M.D., and W. Rudolph Schouten, M.D., who have provided the time, expertise, and advice through the third edition of this text- book. We are most appreciative of their unwavering help. We are also grateful to Peter A. Cataldo, M.D., and Jean MacDonald, RN CETN for their contributions. For a book of this magnitude, an enormous amount of skilled secretarial support was required. We would like to thank Lianna Mantley of the Sir Mortimer B. DavisJewish General Hospital, Montreal, Canada and Nancy Beckmann of the Mayo Clinic, Rochester, Minnesota, for their care in typing and retyping the manuscript. We wish to thank Silvie Damico for her secretarial assistance throughout the process and Carmela Masella for handling ofce duties while the manuscript was being typed. Thanks to Elliot Gordon for gathering the many journal references required for researching the various topics and thanks to Laurel Gordon for her lial words of wisdom. A very special word of thanks to Rosalie Gordon for her unwavering support and advice, and from whom precious hours were stolen to permit the writing of the book. Thanks to Marisa Nivat- vongs and Nitara Layton for their good nature and love. We continue to be blessed and fortunate to have the very talented medical illustrator Scott Barrows provide his expertise to this edition. His enormous skill, coopera- tion, and ability to convert words into images have greatly enhanced the book. We would also like to thank Joanne Jay of The Egerton Group Ltd. for her efforts in suc- cessfully assembling a book of this magnitude and complexity. xiii
- 10. Contents Contributors / iii Dedication / v Preface to the Third Edition / vii Preface from the Second Edition / ix Preface from the First Edition / xi Acknowledgments / xiii Part I: Essential Considerations & 1: Surgical Anatomy / 1 Santhat Nivatvongs and Philip H. Gordon Colon / 2 Rectum / 4 Mesorectum / 7 Histology / 7 Anal Canal / 7 Muscles of the Anorectal Region / 10 Anorectal Spaces / 11 Arterial Supply / 15 Venous Drainage / 20 Lymphatic Drainage / 21 Innervation / 23 References / 27 & 2: Physiology / 29 W. Rudolf Schouten and Philip H. Gordon Colonic Physiology / 29 Functions / 29 Microora / 38 Intestinal Gas / 40 Anorectal Physiology / 41 Anal Continence / 41 Defecation / 47 Investigative Techniques / 50 Clinical Application / 58 References / 61 & 3: Diagnosis / 65 Santhat Nivatvongs Patient History / 66 Physical Examination / 69 Radiologic Examination / 74 Capsule Endoscopy / 82 Colonoscopy / 82 Examination of Stool / 93 References / 95 & 4: Preoperative and Postoperative Management / 99 W. Rudolf Schouten and Philip H. Gordon General Considerations / 99 Colon Operation / 102 Anorectal Operation / 112 References / 114 & 5: Local Anesthesia in Anorectal Surgery / 117 Santhat Nivatvongs Introduction / 117 Selection of Patients / 117 Applicable Conditions / 117 Actions of Agent / 118 Disposition of Agent / 118 Choice of Agent / 118 Minimizing Pain in Local Anesthesia / 119 Adverse Reactions / 119 Treatment of Adverse Reactions / 120 Prevention of Adverse Reactions / 120 Induction of Anesthesia / 120 Techniques of Local Anesthesia / 121 References / 123 & 6: Pharmacology of Anorectal Preparations / 125 Philip H. Gordon Introduction / 125 Classication / 126 Dosage Forms / 128 Product Selection Guidelines / 128 Discussion / 128 References / 129 & 7: Electrosurgery and Laser Surgery: Basic Applications / 131 Santhat Nivatvongs and Lee E. Smith Electrosurgery / 131 Denition / 131 Monopolar and Bipolar Electrodes / 131 Basic Principles / 132 Snare Polypectomy / 133 Hazards / 134 Laser Surgery / 136 History / 136 Basic Properties of Lasers / 136 Comparison of Surgical Lasers / 137 Clinical Applications / 138 References / 141 xv
- 11. Part II: Anorectal Disorders & 8: Hemorrhoids / 143 Santhat Nivatvongs What Are Hemorrhoids? / 144 Prevalence / 144 Etiology and Pathogenesis / 145 Predisposing and Associated Factors / 145 Function of Anal Cushions / 145 Nomenclature and Classication / 146 Diagnosis / 146 Nonoperative Treatment and Minor Operative Procedures / 148 Hemorrhoidectomy / 150 Special Situations / 152 Early Postoperative Problems / 157 Stapled Hemorrhoidopexy / 158 References / 164 & 9: Fissure-in-Ano / 167 Philip H. Gordon Introduction / 167 Clinical Features / 167 Pathology / 167 Etiology / 168 Predisposing Factors / 168 Pathogenesis / 168 Symptoms / 169 Diagnosis / 170 Differential Diagnosis / 171 Treatment / 172 References / 187 & 10: Anorectal Abscesses and Fistula-in-Ano / 191 Philip H. Gordon Anatomy / 192 Etiology / 192 Pathogenesis / 192 Avenues of Extension / 193 Diagnosis / 193 Anorectal Abscess / 197 Fistula-in-Ano / 203 Special Considerations / 220 References / 230 & 11: Pilonidal Disease / 235 Santhat Nivatvongs Introduction / 235 Etiology and Pathogenesis / 235 Surgical Pathology / 236 Natural History / 236 Predisposing Factors / 236 Clinical Manifestations / 237 Diagnosis / 237 Treatment / 238 Summary / 241 Role of Hair / 243 Recurrent Disease / 243 Unhealed Wound / 243 Pilonidal Sinus and Carcinoma / 245 References / 246 & 12: Perianal Dermatologic Disease / 247 Lee E. Smith Introduction / 247 Pruritic Conditions / 247 Idiopathic Pruritus Ani / 247 Primary Etiologies / 250 Nonpruritic Lesions / 258 Infections / 258 Neoplastic Lesions / 258 Inammatory Bowel Disease / 259 References / 259 & 13: Condyloma Acuminatum / 261 Philip H. Gordon Introduction / 261 Clinical Features / 261 Pathology / 262 Symptoms / 263 Diagnosis / 263 Treatment / 263 Recurrence / 268 Posttreatment Follow-Up / 269 Resumption of Sexual Intercourse / 269 Condylomata Acuminata in Children / 269 Verrucous Carcinoma / 269 Condyloma Acuminatum and Squamous Cell Carcinoma / 270 References / 271 & 14: Sexually Transmitted Diseases / 275 Lee E. Smith Gastrointestinal Sexually Transmitted Diseases / 275 Epidemiology / 275 Diagnosis / 276 Bacterial Infection / 277 Spirochete Infection / 279 Viral Infection / 280 Parasitic Infection / 280 Acquired Immunodeciency Syndrome / 281 Short History of AIDS / 281 Pathogenesis / 282 Clinical Presentation / 282 Seroconversions / 283 Gastrointestinal Manifestations / 283 Opportunistic Infection / 284 Malignancies / 286 Colorectal Surgery in AIDS Patients / 286 AIDS and the Health Care Worker / 288 References / 288 xvi & CONTENTS
- 12. & 15: Fecal Incontinence / 293 Philip H. Gordon and W. Rudolf Schouten Introduction / 293 Etiology / 295 Diagnosis / 300 Treatment / 305 References / 326 & 16: Rectovaginal Fistula / 333 Philip H. Gordon Introduction / 333 Clinical Evaluation / 333 Classication / 334 Etiology / 334 Operative Repair / 336 Rectourethral Fistula / 347 References / 351 & 17: Retrorectal Tumors / 353 Philip H. Gordon Anatomy / 353 Classication / 353 Incidence / 354 Pathology / 354 Clinical Presentation / 360 Diagnostic Measures / 361 Operative Approaches / 363 Adjuvant Therapy / 366 Results / 366 References / 367 & 18: Perianal and Anal Canal Neoplasms / 369 Santhat Nivatvongs Introduction / 369 Anatomic Landmarks / 369 Incidence / 370 Etiology and Pathogenesis / 370 Staging / 371 Screening for Anal Carcinoma Precursors / 371 Human Papilloma Virus Type 16 Vaccine / 371 Perianal Neoplasms (Anal Margin) / 373 Neoplasms of the Anal Canal / 379 References / 388 & 19: Transanal Techniques / 391 Santhat Nivatvongs Introduction / 391 Rectal Biopsy / 391 Electrocoagulation of Rectal Polyps / 392 Snare Polypectomy / 392 Transanal Excision of Rectal Adenoma / 392 Transanal Excision for Carcinoma of the Low Rectum / 396 Posterior Approach to the Rectum / 396 Transanal Endoscopic Microsurgery / 399 Electrocoagulation of Carcinoma of the Rectum / 401 References / 402 & 20: Ambulatory Procedures / 405 Peter A. Cataldo and Philip H. Gordon Introduction / 405 Preoperative Assessment / 407 Operative Management / 407 Procedures / 408 Postoperative Care / 411 Complications / 412 Benets / 412 References / 413 Part III: Colorectal Disorders & 21: Rectal Procidentia / 415 Philip H. Gordon Introduction / 415 Etiology / 415 Classication / 416 Predisposing Factors / 417 Pathologic Anatomy / 417 Physiologic Dysfunction / 417 Clinical Features / 418 Investigation / 420 Operative Repair / 421 Subsequent Management / 439 Complications / 440 Recurrent Rectal Prolapse / 441 Prolapse in Children / 442 Hidden Prolapse (Internal Procidentia) / 442 Summary / 443 Solitary Ulcer Syndrome of the Rectum / 444 References / 448 & 22: Benign Neoplasms of the Colon and Rectum / 451 Santhat Nivatvongs Polyps of Colon and Rectum / 452 Familial Adenomatous Polyposis / 466 Hemangiomas of Large Bowel / 480 Leiomyomas of Large Bowel / 481 Lipomas of Large Bowel / 482 References / 483 & 23: Malignant Neoplasms of the Colon / 489 Philip H. Gordon Classication / 490 Adenocarcinoma / 490 Incidence, Prevalence, and Trends / 490 Epidemiology / 491 Age / 491 Sex / 491 Family History / 491 Site / 492 Geographic Distribution / 492 Race and Religion / 492 Occupation / 492 Etiology and Pathogenesis / 493 Polyp-Cancer Sequence / 493 Inammatory Bowel Disease / 493 Genetics / 493 Dietary Factors / 510 CONTENTS & xvii
- 13. Irradiation / 515 Ureteric Implantation / 515 Cholecystectomy / 516 Diverticular Disease / 516 Activity and Exercise / 516 Other Factors / 517 Juvenile vs. Adult Carcinoma / 518 Prospects for Prevention / 519 Pathology / 520 Macroscopic Appearance / 520 Microscopic Appearance / 521 Depressed Carcinoma / 523 Sentinel Lymph Node Mapping / 525 Modes of Spread / 526 Site of Spread / 527 Staging / 527 Biology of Growth / 530 Clinical Features / 532 Symptoms / 532 General and Abdominal Examinations / 533 Digital Rectal Examination / 533 Extraintestinal Manifestations / 533 Synchronous Carcinomas / 533 Associated Polyps / 533 Other Associated Malignancies / 534 Complications / 534 Obstruction / 534 Perforation / 535 Bleeding / 535 Unusual Infections Associated with Colorectal Carcinoma / 535 Diagnosis / 535 Investigations / 536 Occult Blood Testing / 536 Endoscopy / 536 Radiology / 536 Radioimmunodetection / 539 Cytology / 540 Blood Markers / 540 Treatment / 542 Curative Resection / 542 Adjuvant Therapy / 555 Complicated Carcinomas / 561 Perforation / 566 Bleeding / 566 Obstructive Colitis / 566 Invasion of Adjacent Viscera / 567 Urinary Tract Involvement by Colorectal Carcinoma / 569 Primary Involvement of the Urinary Tract / 569 Bladder Involvement / 570 Ureteric Involvement / 570 Fistula / 570 Hydronephrosis / 571 Radiotherapy / 571 Unexpected Intraoperative Involvement / 571 Recurrent Colorectal Carcinoma / 571 Abnormal Renal Function / 571 Palliation / 571 Unresectable Carcinoma / 571 Palliative Resection / 571 Synchronous Carcinomas / 572 Synchronous Polyps and Carcinoma / 572 Metachronous Carcinoma / 572 Treatment of Metastatic Disease / 573 Carcinoma in Young Patients / 585 Postoperative Complications / 585 Results / 586 Prognostic Discriminants / 590 Clinical Features / 590 Pathologic Features / 598 Biochemical and Special Investigations / 602 Recurrent Disease / 604 Follow-Up / 604 Incidence / 604 Contributing Factors / 604 Patterns / 605 Clinical Features / 606 Investigations / 606 Role of Carcinoembryonic Antigen / 607 Treatment / 608 Results of Reoperation / 613 Intestinal Obstruction Due to Recurrent Carcinoma / 613 Colorectal Carcinoma Complicating Pregnancy / 614 Ovarian Carcinoma Involving the Colon / 615 Malakoplakia and Colorectal Carcinoma / 615 Other Malignant Lesions / 615 Carcinoid / 615 Incidence / 616 Clinical Features / 616 Pathology / 616 Imaging Procedures / 617 Chemical Activity / 617 Treatment / 618 Results / 618 Lymphoma / 618 Incidence / 618 Pathology / 618 Clinical Features / 619 Treatment / 620 Results / 620 Sarcoma / 620 Squamous Cell Carcinoma / 621 Adenosquamous Carcinoma / 622 Plasmacytoma / 622 Melanoma / 622 Leukemic Inltration / 623 Neuroendocrine Lesions of the Colorectum / 623 Medullary Carcinoma of the Colon / 623 Carcinosarcoma / 624 Schwannoma / 624 Angiosarcoma / 624 Choriocarcinoma / 624 Metastases from Other Sources / 625 References / 625 & 24: Malignant Neoplasms of the Rectum / 645 Philip H. Gordon Adenocarcinoma / 646 Mechanisms of Spread of Rectal Carcinoma / 646 Direct Extension / 646 Transperitoneal Spread / 646 Implantation / 646 Lymphatic Spread / 646 Venous Spread / 646 Clinical Features / 647 Symptoms / 647 General and Abdominal Examination / 647 Investigations / 647 Endoscopy / 647 Routine Laboratory Blood Work / 647 Radiology / 647 Preoperative Preparation / 651 Radical Extirpative Operations / 652 Assessment of Resectability / 652 Selection of Appropriate Operation / 652 Operative Procedures / 654 Postoperative Care / 674 Results / 674 xviii & CONTENTS
- 14. Local Forms of Therapy / 683 Rationale / 683 Procedures / 683 Special Considerations / 691 Distal Margins / 691 Circumferential Margins / 692 Total Mesorectal Excision / 692 Radical Lymphadenectomy / 696 Concomitant Pelvic Organ Excision / 698 Palliative Therapy for Advanced Rectal Carcinoma / 699 Hartmanns Procedure / 702 Unresectable Carcinoma of the Rectum / 702 High Ligation of Inferior Mesenteric Artery / 703 Marking the Rectum / 703 Adjuvant Therapy for Carcinoma of the Rectum / 704 Radiotherapy / 704 Chemotherapy / 712 Combination Chemoradiotherapy / 712 Immunotherapy / 717 Summary / 718 Postoperative Complications / 718 Recurrent Disease / 718 Follow-up / 718 Incidence / 718 Factors Contributing to Recurrence / 719 Patterns of Recurrence / 719 Clinical Features / 720 Investigations / 720 Treatment of Recurrent Disease / 721 Results of Reoperation / 728 Other Malignant Lesions of the Rectum / 728 Carcinoid / 728 Clinical Presentation / 729 Investigation / 729 Pathology / 729 Treatment / 729 Results / 729 Lymphoma / 730 Clinical Presentation / 730 Treatment and Results / 730 Sarcoma / 730 Gastrointestinal Stromal Tumor (GIST) / 731 Secondary Carcinoma / 732 Miscellaneous Neoplasms / 732 References / 732 & 25: Large Bowel Carcinoma: Screening, Surveillance, and Follow-Up / 743 Santhat Nivatvongs Detection of Early Colorectal Carcinoma / 743 Early Diagnosis of Colorectal Carcinoma / 744 What Is Screening? / 744 Who Should Be Screened? / 744 Screening People at Average Risk for Colorectal Carcinoma / 745 Screening People at Increased Risk for Colorectal Carcinoma / 747 New Screening Tests / 748 When to Stop Screening / 748 Surveillance / 749 Follow-Up after Curative Resection / 750 Other Primary Malignancies / 751 Summary / 751 References / 752 & 26: Ulcerative Colitis / 755 Santhat Nivatvongs Introduction / 756 Epidemiology and Etiology / 756 Clinical Course / 757 Clinical Manifestations / 757 Diagnosis / 757 Assessment of Severity / 758 Pathologic Features / 759 Gross Appearance / 759 Microscopy / 760 Differential Diagnosis / 761 Crohns Disease / 761 Clostridium Difcile Colitis / 761 Campylobacter Gastroenteritis / 763 Salmonella Enterocolitis / 763 Escherichia Coli 0157:H7 / 764 Amebiasis / 765 Collagenous Colitis / 765 Risk of Carcinoma / 767 Surveillance / 767 Problems with Colonoscopy and Biopsy / 768 A Practical Guide / 768 Extracolonic Manifestations / 769 Hepatic Dysfunction / 769 Primary Sclerosing Cholangitis and Bile Duct Carcinoma / 769 Arthritis / 771 Ankylosing Spondylitis and Sacroiliitis / 771 Erythema Nodosum / 771 Pyoderma Gangrenosum / 771 Ulcers of Mouth / 772 Eye Diseases / 772 Ulcerative Colitis and Pregnancy / 772 Drugs for Ulcerative Colitis / 772 Sulfasalazine (Azuldine) / 772 Aminosalicylates / 773 Corticosteroids / 773 Budesonide / 773 Antibiotics / 773 Immunosuppressive Drugs / 773 Medical Management / 774 Proctitis / 774 Proctosigmoiditis / 774 Left-Sided Colitis and Pancolitis / 775 Anemia in Inammatory Bowel Disease / 775 Severe or Fulminant Colitis / 775 Steroid-Refractory Ulcerative Colitis / 776 Steroid-Dependent Ulcerative Colitis / 777 Natural History of Treated Ulcerative Colitis / 777 Course of Severe Ulcerative Colitis / 777 Course of Active and Chronic Ulcerative Colitis / 778 Indications for Operation / 778 Intractability / 778 Fulminant Colitis / 778 Toxic Megacolon / 778 Massive Bleeding / 779 Prophylaxis for Carcinoma / 779 Carcinoma / 779 Cutaneous and Systemic Complications / 780 Operative Options / 780 Total Proctocolectomy and Ileostomy / 780 Colectomy with Ileostomy and Hartmanns Procedure / 780 Colectomy with Ileorectal Anastomosis / 780 Total Proctocolectomy with Continent Ileostomy (Kocks Pouch) / 781 Total Proctocolectomy with Ileal PouchAnal Anastomosis / 784 Selection of Patients / 786 Special Situations / 795 Indeterminate Colitis / 795 Inadvertent Crohns Disease / 796 CONTENTS & xix
- 15. Ulcerative Colitis with Carcinoma / 797 Adenocarcinoma in Ileal PouchAnal Anastomosis / 797 Pregnancy / 799 Older Patients / 799 Complications / 800 Small Bowel Obstruction / 800 Pelvic Abscess / 800 Leakage of Pouch and PouchAnal Anastomosis / 801 Vaginal Fistula / 801 Anal Stricture / 802 Difcult Evacuation / 803 Portal Vein Thrombosis / 804 Pouchitis / 804 Reoperation for Pouch-Related Complications / 806 Sexual Dysfunction / 807 Complete Failure of Ileal PouchAnal Anastomosis / 808 Functional Results / 808 Stool Frequency / 808 Fecal Incontinence / 809 Metabolic Function / 810 Patient Satisfaction with Ileal PouchAnal Anastomosis / 811 References / 811 & 27: Crohns Disease / 819 Santhat Nivatvongs and Philip H. Gordon Introduction / 820 Epidemiology / 820 Etiology and Pathogenesis / 821 Pathology / 825 Clinical Manifestations / 826 Diagnosis / 826 Endoscopy / 827 Contrast Studies / 827 Nuclear Scans / 828 ASCA Test / 828 Ultrasonography / 828 Computed Tomography / 829 Magnetic Resonance Imaging / 829 Capsule Endoscopy / 829 Virtual Colonoscopy / 829 New Diagnostic Criteria / 830 Differential Diagnosis / 830 Natural History / 830 Classication / 833 Medical Management / 834 Sulfasalazine and 5-aminosalicylic Acid / 835 Antibiotics / 835 Corticosteroids / 835 Immunosuppressive Agents / 836 Biologic Modiers / 838 Analgesics / 841 Nutrition / 842 Smoking Cessation / 842 Probiotics / 843 Summary / 843 Indications for Operation / 844 Intractability to Medical Treatment / 845 Bowel Obstruction / 845 Intra-abdominal Abscess / 845 Internal Fistula / 846 Colocutaneous and Enterocutaneous Fistula / 847 Fulminant Colitis / 847 Toxic Megacolon / 848 Free Perforation / 848 Massive Bleeding / 849 Carcinoma Prevention / 849 Carcinoma / 850 Extracolonic Manifestations / 850 Growth Retardation / 850 Overview / 850 Interventional Options and Their Results / 850 Ileocecal Resection / 850 Total Proctocolectomy and Ileostomy / 851 Subtotal Colectomy with Closure of Rectal or Sigmoid Stump or Mucous Fistula and Ileostomy / 851 Fate of Rectal Stump / 852 Colectomy with Ileorectal Anastomosis / 852 Ileostomy / 853 Segmental Colon Resection / 853 Operations for Intestinal Fistula / 854 Bypass Operation / 855 Small Bowel Resection / 855 Strictureplasty / 856 Percutaneous Drainage of Intra-Abdominal Abscess / 860 Stricture Dilatation / 861 Likelihood of Stoma Necessity / 862 Fate of Ileal Pouch-Anal Anastomosis in Unsuspected Crohns Disease / 862 How Much Bowel to Resect / 864 Overview of Results / 864 Challenging Anatomic Locations of Crohns Disease / 867 Oropharynx / 867 Esophagus / 867 Gastroduodenum / 868 Diffuse Jejunoileitis / 870 Appendix / 871 Perianal and Anal Canal Crohns Disease / 871 Special Considerations / 880 Extracolonic Manifestations / 880 Hepatobiliary Manifestations / 881 Risk of Carcinoma / 882 Chemoprevention of Colorectal Carcinoma / 887 Crohns Disease and Pregnancy / 888 Recurrence / 890 Factors Inuencing Recurrence / 890 Maintaining Remission in Crohns Disease / 893 Summary / 896 References / 899 & 28: Diverticular Disease of the Colon / 909 Philip H. Gordon Introduction / 910 Pathologic Anatomy / 910 Incidence / 910 Etiology / 912 Pathogenesis / 913 Pathology / 916 Patterns of Disease / 917 Natural History / 918 Clinical Manifestations / 920 Diagnosis / 920 Treatment / 922 Complications / 928 Results and Prognosis / 957 Right-Sided Diverticula / 958 Giant Colonic Diverticulum / 962 Coexisting Disorders / 962 Special Problems / 964 References / 965 & 29: Volvulus of the Colon / 971 Santhat Nivatvongs Introduction / 971 Sigmoid Volvulus / 971 xx & CONTENTS
- 16. Ileosigmoid Knotting / 979 Sigmoid Volvulus in Pregnancy / 981 Cecal Volvulus / 981 Volvulus of Transverse Colon / 983 Splenic Flexure Volvulus / 984 References / 984 & 30: Mesenteric Vascular Diseases / 987 Philip H. Gordon Vascular Anatomy / 987 Pathophysiology of Intestinal Ischemia / 988 Diagnostic Studies / 990 Clinical Syndromes / 991 Superior Mesenteric Artery Embolism / 991 Superior Mesenteric Artery Thrombosis / 993 Nonocclusive Mesenteric Ischemia and Infarction / 994 Mesenteric Venous Thrombosis / 995 Chronic Mesenteric Vascular Disease / 996 Ischemic Colitis / 999 Ischemic Colitis and Aortoiliac Surgery / 1007 Total Colonic Ischemia / 1010 Ischemic Proctitis / 1010 References / 1011 & 31: Radiation Injuries to the Small and Large Intestine / 1015 Santhat Nivatvongs Introduction / 1015 Incidence and Clinical Manifestations / 1015 Mechanisms of Radiation Injury / 1016 Pathology / 1016 Pathogenesis / 1017 Predisposing Factors / 1018 Small Intestine Injuries / 1018 Colon and Rectal Injuries / 1020 Radiation Proctitis / 1024 Increased Risk of Rectal Carcinoma after Prostate Radiation / 1025 Prevention / 1026 References / 1028 & 32: Intestinal Stomas / 1031 Philip H. Gordon, Jean MacDonald, and Peter A. Cataldo Introduction / 1032 Ileostomy / 1032 Colostomy / 1039 Outcomes of Stomal Construction and Closure / 1060 Enterostomal Care and Rehabilitation / 1061 References / 1077 & 33: Constipation / 1081 W. Rudolf Schouten and Philip H. Gordon Introduction / 1082 Denition / 1082 Etiology / 1083 Investigation / 1084 Why Treat Constipation? / 1094 Treatment / 1095 Special Considerations / 1114 References / 1117 Part IV: Problem-Oriented Approach to Colorectal Disease & 34: Traumatic Injuries / 1125 Lee E. Smith Etiology / 1125 Penetrating Trauma / 1125 Blunt Trauma / 1126 Iatrogenic Injury / 1126 Ingested Foreign Bodies / 1130 Foreign Bodies and Sexual Trauma / 1130 Sexual Assault / 1131 Child Abuse / 1131 Unusual Perforations / 1132 Management / 1132 Diagnosis of Trauma (Secondary Survey Phase) / 1132 Laparoscopy / 1134 Surgical Treatment (Denitive Care Phase) / 1134 References / 1143 & 35: Complications of Colonic Disease and Their Management / 1147 Santhat Nivatvongs Acute Colonic Obstruction / 1148 Free Perforation / 1150 Neutropenic Enterocolitis / 1151 Massive Bleeding / 1152 Fistula / 1158 References / 1162 & 36: Complications of Anorectal and Colorectal Operations / 1165 Santhat Nivatvongs Introduction / 1166 Early Complications of Anorectal Operations / 1166 Delayed Complications of Anorectal Operations / 1167 Complications of Colorectal Operations / 1169 References / 1187 & 37: Unexpected Intraoperative Findings / 1191 Philip H. Gordon, Santhat Nivatvongs, and Lee E. Smith Introduction / 1191 Case 1: Carcinoma of Rectum and Unexpected Synchronous Carcinoma of Hepatic Flexure / 1191 Case 2: Carcinoma of Right Colon and Unexpected Major Single Hepatic Metastasis / 1192 Case 3: Sigmoid Mass that Proves to Be Endometrioma Instead of Carcinoma / 1192 Case 4: Exploration for Appendicitis that Proves to Be Carcinoma of Cecum / 1193 Case 5: Pelvic Laparotomy for Gynecologic Mass that Proves to Be Carcinoma of Sigmoid / 1193 CONTENTS & xxi
- 17. Case 6: Exploration for Acute Appendicitis that Proves to Be Sigmoid Phlegmon / 1194 Case 7: Carcinoma of Rectum with Incidental Cholelithiasis / 1194 Case 8: Carcinoma of Rectum with Invasion of Urinary Bladder / 1195 Case 9: Concomitant Carcinoma of Rectum and Abdominal Aortic Aneurysm / 1196 Case 10: Propriety of Incidental Appendectomy / 1197 Case 11: Propriety of Incidental Meckels Diverticulectomy / 1198 Case 12: Rectal Prolapse and Unexpected Ovarian Mass / 1199 Case 13: Vaginal Hysterectomy and Intraoperative Perforation of Rectum / 1199 Case 14: Exploration for Appendicitis with Unexpected Pseudomyxoma Peritonei / 1200 Conclusion / 1200 References / 1200 Part V: Minimally Invasive Surgery & 38: Laparoscopic Colon and Rectal Surgery / 1203 Lee E. Smith and Philip H. Gordon Background and Rationale / 1204 Indications / 1205 Equipment and Instrumentation / 1207 Operative Procedure / 1211 Specic Colorectal Procedures / 1214 Robotics / 1227 Postoperative Care / 1228 Results / 1228 Laparoscopic Complications and Their Prevention / 1257 References / 1261 Part VI: Et Cetera & 39: Miscellaneous Entities / 1267 Philip H. Gordon Coccygodynia / 1268 Endometriosis / 1271 Proctalgia Fugax and Levator Syndrome / 1274 Oleogranuloma / 1276 Melanosis Coli / 1277 Colitis Cystica Profunda / 1278 Descending Perineum Syndrome / 1279 Pneumatosis Coli / 1281 Hidradenitis Suppurativa / 1284 Anal Leukoplakia / 1288 Diversion Colitis / 1288 Segmental or Diverticula-Associated Colitis / 1289 Aortoenteric Fistula / 1290 Colon Interposition / 1291 References / 1295 Index / 1299 xxii & CONTENTS
- 18. Surgical Anatomy Santhat Nivatvongs and Philip H. Gordon & Colon, 2 General Conguration, 2 Course and Relations, 2 Peritoneal Coverings, 3 Ileocecal Valve, 4 & Rectum, 4 Peritoneal Relations, 4 Fascial Attachments, 4 Fascia Propria (Investing Fascia), 4 Waldeyers Fascia, 5 Denonvilliers Fascia, 5 Lateral Ligament, 6 & Mesorectum, 7 & Histology, 7 & Anal Canal, 7 Lining of Canal, 8 Anal Transitional Zone, 9 Anal Glands, 9 & Muscles of the Anorectal Region, 10 Internal Sphincter Muscle, 10 Conjoined Longitudinal Muscle, 10 External Sphincter Muscle, 10 Perineal Body, 11 Pelvic Floor Muscles, 11 Puborectalis Muscle, 11 Iliococcygeus Muscle, 11 Pubococcygeus Muscle, 11 Anorectal Ring, 11 & Anorectal Spaces, 11 Perianal Space, 13 Ischioanal Space, 13 Intersphincteric Space, 14 Supralevator Space, 14 Submucous Space, 14 Supercial Postanal Space, 15 Deep Postanal Space, 15 Retrorectal Space, 15 & Arterial Supply, 15 Ileocolic Artery, 15 Right Colic Artery, 15 Middle Colic Artery, 17 Inferior Mesenteric Artery, 17 Superior Rectal Artery, 17 Middle Rectal Arteries, 17 Inferior Rectal Arteries, 17 Median Sacral Artery, 19 Collateral Circulation, 19 & Venous Drainage, 20 Superior Mesenteric Vein, 20 Inferior Mesenteric Vein, 20 & Lymphatic Drainage, 21 Colon, 22 Epicolic Glands, 22 Paracolic Glands, 22 Intermediate Glands, 22 Main Glands, 22 Rectum and Anal Canal, 22 & Innervation, 23 Colon, 23 Sympathetic Innervation, 23 Parasympathetic Innervation, 24 Rectum, 24 Sympathetic Innervation, 24 Parasympathetic Innervation, 25 Pudendal Nerve, 26 Anal Canal, 26 Motor Innervation, 26 Sensory Innervation, 27 & References, 27 & Colon, 2 General Conguration, 2 Course and Relations, 2 Peritoneal Coverings, 3 Ileocecal Valve, 4 & Rectum, 4 Peritoneal Relations, 4 Fascial Attachments, 4 Fascia Propria (Investing Fascia), 4 Waldeyers Fascia, 5 Denonvilliers Fascia, 5 Lateral Ligament, 6 & Mesorectum, 7 & Histology, 7 & Anal Canal, 7 Lining of Canal, 8 Anal Transitional Zone, 9 Anal Glands, 9 & Muscles of the Anorectal Region, 10 Internal Sphincter Muscle, 10 Conjoined Longitudinal Muscle, 10 External Sphincter Muscle, 10 Perineal Body, 11 Pelvic Floor Muscles, 11 Puborectalis Muscle, 11 Iliococcygeus Muscle, 11 Pubococcygeus Muscle, 11 Anorectal Ring, 11 & Anorectal Spaces, 11 Perianal Space, 13 Ischioanal Space, 13 Intersphincteric Space, 14 Supralevator Space, 14 Submucous Space, 14 Supercial Postanal Space, 15 Deep Postanal Space, 15 Retrorectal Space, 15 & Arterial Supply, 15 Ileocolic Artery, 15 Right Colic Artery, 15 Middle Colic Artery, 17 Inferior Mesenteric Artery, 17 Superior Rectal Artery, 17 Middle Rectal Arteries, 17 Inferior Rectal Arteries, 17 Median Sacral Artery, 19 Collateral Circulation, 19 & Venous Drainage, 20 Superior Mesenteric Vein, 20 Inferior Mesenteric Vein, 20 & Lymphatic Drainage, 21 Colon, 22 Epicolic Glands, 22 Paracolic Glands, 22 Intermediate Glands, 22 Main Glands, 22 Rectum and Anal Canal, 22 & Innervation, 23 Colon, 23 Sympathetic Innervation, 23 Parasympathetic Innervation, 24 Rectum, 24 Sympathetic Innervation, 24 Parasympathetic Innervation, 25 Pudendal Nerve, 26 Anal Canal, 26 Motor Innervation, 26 Sensory Innervation, 27 & References, 27 1 I: Essential Considerations 1
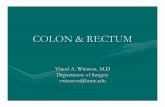
- 19. Although seemingly a single organ, the colon is embryo- logically divisible into two parts. The transverse colon and portions proximal to it are derived from the midgut and are supplied by the superior mesenteric artery, while the distal half of the colon is derived from the hindgut and receives blood from the inferior mesenteric artery. The large bowel begins in the right lower quadrant of the abdomen as a blind pouch known as the cecum. The ileum empties into the medial and posterior aspect of the intestine, a point known as the ileocecal junction. The colon proceeds upward and in its course is designated according to location as: ascending colon, hepatic exure, transverse colon, splenic exure, descending colon, sigmoid colon, rec- tum, and anal canal. The colon is approximately 150 cm long, and its diameter gradually diminishes from the cecum to the rectosigmoid junction, where it widens as the rectal ampulla, only to narrow again as the anal canal. & COLON & GENERAL CONFIGURATION The colon differs from the small bowel in that it is character- ized by a saccular or haustral appearance, it contains three taenia bands, and it has appendices epiploicae, a series of fatty appendages located on the antimesenteric surface of the colon. The taenia bands are longitudinal muscle run- ning along the colon from the base of the appendix. They merge in the distal sigmoid colon, where the longitudinal bers continue through the entire length of the rectum. A study by Fraser et al. (1) has shown that the longitudinal muscle forms a complete coat around the colon but is much thicker at the taeniae. The three taenia bands are named according to their relation to the transverse colon: taenia mesocolica, which is attached to the mesocolon; taenia omen- talis, which is attached to the greater omentum; and taenia libera, which has no attachment. These bands are about one sixth shorter than the intestine and are believed to be responsible for the sacculations (2). The transition from the sigmoid colon to the rectum is a gradual one. It is characterized by the taeniae coli spread- ing out from three distinct bands to a uniformly distributed layer of longitudinal smooth muscle that is thicker on the front and back than on each side. & COURSE AND RELATIONS The general topography of the colon varies from person to person, and such differences should be taken into account while reading the following discussion (Fig. 1). The vermiform appendix projects from the lowermost part of the cecum. From the ileocecal junction the colon ascends on the right in front of the quadratus lumborum and transversus abdominis muscles to a level overlying the lower pole of the right kidney, a distance of about 20 cm. It is invested by peritoneum on its anterior, lateral, and medial surfaces. Superior to the colon is the undersur- face of the right lobe of the liver, lateral to the gallbladder, and here the colon angulates acutely medially, downward, and forward, forming the hepatic exure. Occasionally there is a lmy web of adhesions extending from the right abdominal wall to the anterior taenia of the ascending colon, and this has been referred to as Jacksons membrane. FIGURE 1 & General topography of the large bowel. (A) Colon. (B) Peritoneum and adjacent structures. 2 & PART I: ESSENTIAL CONSIDERATIONS
- 20. The transverse colon is the longest (4050 cm) segment of colon, extending from the hepatic to the splenic exure. It is usually mobile and may descend to the level of the iliac crests or even dip into the pelvis. The transverse colon is enveloped between layers of the transverse mesocolon, the root of which overlies the right kidney, the second por- tion of the duodenum, the pancreas, and the left kidney. It contains the middle colic artery, branches of the right and left colic arteries, and accompanying veins, lymphatic structures, and autonomic nerve plexuses. This posterior relationship is of paramount importance because these structures are subject to injury during a right hemi-colect- omy if proper care is not exercised. In the left upper quadrant of the abdomen, the colon is attached to the undersurface of the diaphragm at the level of the 10th and 11th ribs by the phrenocolic ligament. The distal trans- verse colon lies in front of the proximal descending colon. The stomach is immediately above and the spleen is to the left. The greater omentum descends from the greater curva- ture of the stomach in front of the transverse colon and ascends to the upper surface of the transverse colon. The splenic exure describes an acute angle, is high in the left upper quadrant, and therefore is less accessible to operative approach. It lies anterior to the midportion of the left kidney. The descending colon passes along the posterior abdominal wall over the lateral border of the left kidney, turns somewhat medially, and descends in the groove between the psoas and the quadratus lumborum muscles to its junction with the sigmoid at the level of the pelvic brim and the transversus abdominis muscle (3). Its length averages 30 cm. The anterior, medial, and lateral portions of its circumference are covered by peritoneum. The distal por- tion of the descending colon is usually attached by adhesions to the posterior abdominal wall, and these adhesions require division during mobilization of this portion of the colon. The sigmoid colon extends from the pelvic brim to the sacral promontory, where it continues as the rectum. Its length varies dramatically from 15 to 50 cm, and it may follow an extremely tortuous and variable course. It often loops to the left but may follow a straight oblique course, loop to the right, or ascend high into the abdomen. It has a generous mesentery and is extremely mobile. The serosal surface has numerous appendices epiploicae. The base of the mesocolon extends from the iliac fossa, along the pelvic brim, and across the sacroiliac joint to the second or third sacral segment; in so doing, it forms an inverted V. Con- tained within the mesosigmoid are the sigmoidal and superior rectal arteries and accompanying veins, lymphat- ics, and autonomic nerve plexuses. At the base of the mesosigmoid is a recess, the intersigmoid fossa, which serves as a valuable guide to the left ureter, lying just deep to it. The upper limb runs medially and upward, crossing the left ureter and iliac vessels; this is an extremely impor- tant relationship during resection of this part of the colon. The lower limb extends in front of the sacrum and also may be alongside loops of small bowel, the urinary bladder, and the uterus and its adnexa. Saunders et al. (4) conducted a novel study in which they investigated possible differences in colonic anatomy and mesenteric attachmentsbetween Western(Caucasian)and Ori- ental patients. Measurements of colonic length and mesenteric attachments were taken according to a set protocol from 115 Western and 114 Oriental patients at laparotomy. Sig- moid adhesions were found more frequently in Western patients (17%) compared to Oriental patients (8%) (p 0.047). A descending mesocolon of !10 cm occurred in 10 (8%) Western patients but only one (0.9%) Oriental patient (p 0.01). The splenic exure was more frequently mobile in Western (20%) compared to Oriental patients (9%) (p 0.016). In 29% of Western patients, the midtrans- verse colon reached the symphysis pubis, or lower when pulled downward, in contrast to that nding in 10% of Oriental patients (p < 0.001). There was no signicant dif- ference in total colonic length when Western patients (median, 114 cm; range, 68159 cm) were compared with Oriental patients (median, 111 cm; range, 78161 cm). Western patients have a higher incidence of sigmoid colon adhesions and increased colonic mobility when compared with Orientals. These ndings support the observation that colonoscopy is a more difcult procedure to perform on Western patients. & PERITONEAL COVERINGS The antimesenteric border of the distal ileum may be attached to the parietal peritoneum by a membrane (Lanes membrane) (5). The cecum usually is entirely enveloped by peritoneum. The ascending colon is attached to the poste- rior body wall and is devoid of peritoneum in its posterior surface; thus, it does not have a mesentery. The transverse colon is invested with peritoneum. Its posterosuperior sur- face, along the taenia band, is attached by the transverse mesocolon to the lower border of the pancreas. The poste- rior and inferior layers of the greater omentum are fused on the anterosuperior aspect of the transverse colon. To mobi- lize the greater omentum or to enter the lesser sac, the fusion of the omentum to the transverse colon must be dis- sected. Because the omental bursa becomes obliterated caudal to the transverse colon and toward the right side, the dissection should be started on the left side of the trans- verse colon. Topor et al. (6) studied 45 cadavers to elucidate surgical aspects of omental mobilization, lengthening, and transposition into the pelvic cavity. They identied that the most important anatomic variables for omental transpo- sition were three variants of arterial blood supply: (i) In 56% of patients, there is one right, one (or two) middle, and one left omental artery. (ii) In 26% of patients, the mid- dle omental artery is absent. (iii) In the remaining 18% of patients, the gastroepiploic artery is continued as a left omental artery but with various smaller connections to the right or middle omental artery. The rst stage of omen- tal lengthening is detachment of the omentum from the transverse colon mesentery. The second stage is the actual lengthening of the omentum. The third stage is placement of the omental ap into the pelvis. The left colonic exure is attached to the diaphragm by the phrenocolic ligament, which also forms a shelf for supporting the spleen. The des- cending colon is devoid of peritoneum posteriorly, where it is in contact with the posterior abdominal wall and thus has no mesentery. The sigmoid colon begins at about the level of the pelvic brim and is completely covered with peritoneum. The posterior surface is attached by a fan-shaped mesen- tery. The lateral surface of the sigmoid mesentery is fused to the parietal peritoneum of the lateral abdominal wall CHAPTER 1: SURGICAL ANATOMY & 3
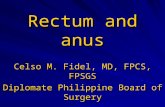
- 21. and is generally known as the white line of Toldt. Mobi- lization of the sigmoid colon requires cutting or incising the lateral peritoneal reection. The sigmoid colon varies greatly in length and conguration. & ILEOCECAL VALVE The superior and inferior ileocecal ligaments are brous tis- sue that helps maintain the angulation between the ileum and the cecum. Kumar and Phillips (7) found these struc- tures to be important in the maintenance of competence against reux at the ileocecal junction. In an autopsy evaluation, the ascending colon was lled with saline solution by retrograde ow, and in 12 of 14 cases the ileo- cecal junctions were competent to pressures up to 80 mmHg. Removal of mucosa at the ileocecal junction or a strip of circular muscle did not impair competence to pres- sures above 40 mmHg, but division of the superior and inferior ileocecal ligaments rendered the junction incompe- tent. Operative reconstruction of the ileocecal angle restored competence. It therefore appears that the angulation between the ileum and the cecum determines continence. & RECTUM Although anatomists traditionally assign the origin of the rectum to the level of the third sacral vertebra, surgeons generally consider the rectum to begin at the level of the sacral promontory. It descends along the curvature of the sacrum and coccyx and ends by passing through the levator ani muscles, at which level it abruptly turns down- ward and backward to become the anal canal. The rectum differs from the colon in that the outer layer is entirely longitudinal muscle, characterized by the merging of the three taenia bands. It measures 1215 cm in length and lacks a mesentery, sacculations, and appendices epiploicae. The rectum describes three lateral curves: the upper and lower curves are convex to the right, and the middle is convex to the left. On their inner aspect these infoldings into the lumen are known as the valves of Houston (8,9). About 46% of normal persons have three valves, 33% have two valves, 10% have four valves, 2% have none, and the rest have from ve to seven valves (9). The clinical signi- cance of the valves of Houston is that they must be negotiated during successful proctosigmoidoscopic exami- nation and, more importantly, that they are an excellent location for a rectal biopsy, because the inward protrusion makes an easy target. They do not contain all the layers of the bowel wall, and therefore biopsy in this location car- ries a minimal risk of perforation. The middle fold is the internal landmark corresponding to the anterior peritoneal reection. Consequently, extra caution must be exercised in removing polyps above this level. Because of its curves, the rectum can gain 5 cm in length when it is straightened (as in performing a low anterior resection); hence, a lesion that initially appears at 7 cm from the anal verge is often found 12 cm from that site after complete mobilization. In its course the rectum is related posteriorly to the sacrum, coccyx, levator ani muscles, coccygeal muscles, median sacral vessels, and roots of the sacral nerve plexus. Anteriorly in the male, the extraperitoneal rectum is related to the prostate, seminal vesicles, vasa deferentia, ureters, and urinary bladder; the intraperitoneal rectum may come in contact with loops of the small bowel and sigmoid colon. In the female, the extraperitoneal rectum lies behind the posterior vaginal wall; the intraperitoneal rectum may be related to the upper part of the vagina, uterus, fallopian tubes, ovaries, small bowel, and sigmoid colon. Laterally above the peritoneal reection, there may be loops of small bowel, adnexa, and sigmoid colon. Below the reection, the rectum is separated from the side wall of the pelvis by the ureter and iliac vessels. & PERITONEAL RELATIONS For descriptive purposes the rectum is divided into upper, middle, and lower thirds. The upper third is covered by peritoneum anteriorly and laterally, the middle third is cov- ered only anteriorly, and the lower third is devoid of peritoneum. The peritoneal reection shows considerable variation between individuals and between men and women. In men, it is usually 79 cm from the anal verge, while in women it is 57.5 cm above the anal verge. The middle valve of Houston roughly corresponds to the ante- rior peritoneal reection. The posterior peritoneal reection is usually 1215 cm from the anal verge (Fig. 2). The location of the peritoneal reection has not been extensively studied in living patients. Najarian et al. (10) investigated the location of the peritoneal reection in 50 patients undergoing laparotomy. The distance from the anal verge to the peritoneal reection was measured in each patient via simultaneous intraoperative proctoscopy and intra-abdominal visualization of the peritoneal reec- tion. The mean lengths of the peritoneal reection were 9 cm anteriorly, 12.2 cm laterally, and 14.8 cm posteriorly for females, and 9.7 cm anteriorly, 12.8 cm laterally, and 15.5 cm posteriorly for males. The lengths of the anterior, lateral, and posterior peritoneal measurements were statistically different from one another, regardless of gen- der. Theirs (10) data indicated that the peritoneal reection is located higher on the rectum than reported in autopsy studies, and that there is no difference between males and females. Knowledge of the location and position of a rectal carcinoma in relationship to the peritoneal reec- tion will help the surgeon optimize the use of peranal techniques of resection. & FASCIAL ATTACHMENTS Fascia Propria (Investing Fascia) The posterior part of the rectum, the distal lateral two thirds, and the anterior one third, are devoid of peritoneum, but they are covered with a thin layer of pelvic fascia, called fascia propria or the investing fascia. At the level of the rec- tal hiatus, the levator ani is covered by an expansion of the pelvic fascia, which on reaching the rectal wall divides into an ascending component, which fuses with the fascia pro- pria of the rectum, and a descending component, which interposes itself between the muscular coats forming the conjoint longitudinal coat (11). These broelastic bers run downward to reach the dermis of the perianal skin and split the subcutaneous striated sphincter into 812 discrete muscle bundles. 4 & PART I: ESSENTIAL CONSIDERATIONS
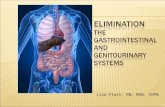
- 22. Waldeyers Fascia The sacrum and coccyx are covered with a strong fascia that is part of the parietal pelvic fascia. Known as Waldeyers fascia, this presacral fascia covers the median sacral vessels. The rectosacral fascia is the Waldeyers fascia from the peri- osteum of the fourth sacral segment to the posterior wall of the rectum (12,13). It is found in 97% of cadaver dissections (13). Waldeyers fascia contains branches of sacral splanch- nic nerves that arise directly from the sacral sympathetic ganglion and may contain branches of the lateral and medi- an sacral vessels. This fascia should be sharply divided with scissors or electrocautery for full mobilization of the rectum (Fig. 3). The posterior space below the rectosacral fascia is the supralevator or retrorectal space (see Fig. 12). Denonvilliers Fascia Anteriorly, the extraperitoneal portion of the rectum is covered with a visceral pelvic fascia, the fascia propria, or investing fascia. Anterior to the fascia propria, or is a lmy delicate layer of connective tissue known as Denonvilliers fascia (14). It separates the rectum from the seminal vesicles and the prostate or vagina (Fig. 4). Denonvilliers fascia has no macroscopically discernible layers. Histologically, it is composed of dense collagen, smooth muscle bers, and coarse elastic bers (15,16). Its attachments have been surrounded by confusion and debates. Some authors believe it is adherent to the rectum (1619), others note that it is applied to the seminal vesicles and the prostate (15,2022). FIGURE 2 & Peritoneal relations of the rectum. FIGURE 3 & (A) Rectosacral fascia. (B) Sharp division of rectosacral fascia for full mobilization of the rectum. CHAPTER 1: SURGICAL ANATOMY & 5
- 23. Lindsey et al. (23) designed a study to evaluate the anatomic relation of Denonvilliers fascia: whether it is attached on the anterior fascia propria of the rectum, or on the seminal vesicles and prostate. They prospectively col- lected 30 specimens from males undergoing total mesorectal excision for mid and low rectal carcinoma, with a deep dissection of the anterior extraperitoneal rectum to the pelvic oor. The anterior aspects of the extraperitoneal rectal sections were examined microscopically for the presence or absence of Denonvilliers fascia. In 20/30 patients that the carcinoma involved anteriorly, 55% vs. 45% of the specimens had Denonvilliers fascia present. On the other hand, when the anterior rectum was not involved with carcinoma (10 patients), 90% of the specimens con- tained no Denonvilliers fascia. The authors concluded, when rectal dissection is conducted on fascia propria in the anatomic plane, Denonvilliers fascia remains on the posterior aspect of the prostate and seminal vesicles. Denonvilliers fascia lies anterior to the anatomic fascia propria plane of anterior rectal dissection in total mesorectal excision (TME) and is more closely applied to the prostate than the rectum. This study has put the debates to rest; Denonvilliers fascia is more closely applied to the seminal vesicles and the prostate than the rectum. Lateral Ligament The distal rectum, which is extraperitoneal, is attached to the pelvic side wall on each side by the pelvic plexus, connective tissues, and middle rectal artery (if present) (24). Histologically it consists of nerve structures, fatty tissue, and small blood vessels (25). Recently, the anatomi- cal term of lateral ligament has been a subject of debate. In dissection of 27 fresh cadavers and ve embalmed pelves, Nano et al. (26) found that lateral ligaments were extension of the mesorectum to the lateral endopelvic fascia. From their experience with anatomic dissection applied to surgery, several conclusion were drawn: & Lateral ligaments are extensions of the mesorectum and must be cut at their attachment at the endopelvic fascia for TME to take place. & Lateral ligaments contain fatty tissue in communication with mesorectal fat and possibly some vessels and nerve laments that are of little importance. & Insertion of lateral ligaments at the endopelvic fascia is placed under the urogenital bundle. & The middle rectal artery courses anteriorly and infer- iorly in respect to the lateral ligament. & Lateral ligaments can be cut at their insertion on the endopelvic fascia without injuring the urogenital ner- vous bundle, which, however, should be kept in view during this procedure, because it crosses the middle rec- tal artery and fans out behind the seminal vesicles. & The lateral aspect of the rectum receives the lateral pedi- cle, which consists of the nervi recti and the middle rectal artery. A study by Rutegard et al. (25) on 10 patients who underwent total mesorectal excision for rectal carcinoma revealed, the often thin structures, usually referred to as FIGURE 4 & Denonvilliers fascia. 6 & PART I: ESSENTIAL CONSIDERATIONS
- 24. the lateral ligaments, seem to arise from the pelvic plexuses and bridge over into the mesorectum, . . . they can be iden- tied in almost every patient. The authors contend that the lateral ligaments are real anatomical ndings. This nd- ing was supported by Sato and Sato (13) in the dissection of 45 cadavers. On the other hand, Jones et al. (24) meticulously dissected 28 cadaveric pelves; they found insubstantial thin strands of connective tissues traversing the space between the mesorectum and the pelvic side wall. These strands of connective tissues were no different from those one would expect to nd in any areolar plane. They were often absent altogether. The pelvic plexuses were distinct from the middle rectal artery (if present) and had no association with the connective tissues. Jones et al. (24) believed that the lateral ligament was nothing more than a surgical arti- fact that results from injudicious dissection. When the rectum is pulled medially, the complex of middle rectal artery and vein, the splanchnic nerves, and their accompanying connective tissues form a band-like structure extending from the lateral pelvic wall to the rec- tum (27). This structure was most likely mistaken as the lateral ligament in the past. Whatever one would call the lateral attachment of the low rectum, the tissues need to be divided in full mobilization of the rectum. & MESORECTUM The posterior rectum is devoid of peritoneum and has no mesorectum. The term mesorectum is a misnomer and does not appear in the Normina Anatomica although it is listed in the Normina Embryologica (28). The word mesorectum was possibly rst used by Maunsell in 1892 and later popu- larized by Heald of the United Kingdom (28). In answering the critique of using this word, Heald answered, . . . it was a surgical word used by the foremost of my surgical teachers when I was a young registrar. Mr. Rex Lawrice of Guys Hospital used to describe the process of dividing the mesorectum as was well described in Rob and Smiths text book of surgery at that time. . . . no other word seems readily available to describe it (29). Total mesorectal excision implies the complete exci- sion of all fat enclosed within the fascia propria, which Heald calls the mesorectum. This dissection is performed in a circumferential manner down to the levator muscles (28). Bisset et al. (30) preferred the term extra fascial exci- sion of the rectum. The term mesorectum has now been used worldwide and appears well entrenched. Canessa et al. (31) studied the lymph nodes in 20 ca- devers using conventional manual dissection. The starting point was at the bifurcation of the superior rectal artery and ending at the anorectal ring. They found an average of 8.4 lymph nodes per rectum; 71% of the lymph nodes were above the peritoneal reection and 29% were below it. Dissection of seven fresh cadavers on the mesorectum by Toper et al. (32) yielded 174 lymph nodes; over 80% of the lymph nodes were smaller than 3 mm. Fifty-six percent of the nodes were located in the posterior mesentery, and most were located in the upper two thirds of posterior rectal mesentery. & HISTOLOGY Knowledge of the microscopic anatomy of the large intes- tine is of paramount importance in understanding the various disease processes. This is especially true in the case of neoplasia, where the depth of penetration will dic- tate the treatment recommendation. Therefore it is essential to examine histologic features. The innermost layer is the mucosa, which is com- posed of three divisions. The rst is a layer of columnar epithelial cells with a series of crevices or crypts character- ized by straight tubules that lie parallel and close to one another and do not branch (glands of Lieberkuhn). The sur- face epithelium around the openings of the crypts consists of simple columnar cells with occasional goblet cells. The tubules are lined predominantly by goblet cells, except at the base of the crypts where undifferentiated cells as well as enterochromafn and amine precursor uptake and decarboxylation (APUD) cells are found. The epithelial layer is separated from the underlying connective tissue by an extracellular membrane composed of glycopolysac- charides and seen as the lamina densa of the basement membrane when viewed by electron microscopy (33). Abnormalities classied as defects, multilayering, or other structural abnormalities have been reported in many types of neoplasms, including those of the colon and rectum. These abnormalities are more common in malignant than in benign neoplasms. The second division of the mucosa is the lamina propria, composed of a stroma of connective tissue containing capillaries, inammatory cells, and lymphoid follicles that are more prominent in young per- sons. The third division is the muscularis mucosa, a ne sheet of smooth muscle bers that serves as a critical demarcation in the diagnosis of invasive carcinoma and includes a network of lymphatics (34). Beneath the muscularis mucosa is the submucosa, a layer of connective tissue and collagen that contains ves- sels, lymphatics, and Meissners plexus. It is the strongest layer of the bowel. The next layer is the circular muscle, which is a contin- uous sheath around the bowel, including both the colon and the rectum. On the external surface of the circular muscle are clusters of ganglion cells and their ramications; these make up the myenteric plexus of Auerbach. Unmyelinated postganglionic bers penetrate the muscle to communicate with the submucosal plexus. The outer or longitudinal muscle bers of the colon are characteristically collected into three bundles, called the taeniae coli; however, in the rectum these bers are spread out and form a continuous layer. The muscularis propria is pierced at regular intervals by the main arterial blood supply and venous drainage of the mucosa. The outermost layer, which is absent in the lower por- tions of the rectum, is the serosa or visceral peritoneum. This layer contains blood vessels and lymphatics. & ANAL CANAL The anal canal is the terminal portion of the intestinal tract. It begins at the anorectal junction (the point passing CHAPTER 1: SURGICAL ANATOMY & 7
- 25. through the levator ani muscles), is about 4 cm long, and terminates at the anal verge (35,36). This denition differs from that of the anatomist, who designates the anal canal as the part of the intestinal tract that extends from the den- tate line to the anal verge. The anal canal is surrounded by strong muscles, and because of tonic contraction of these muscles, it is com- pletely collapsed and represents an anteroposterior slit. The musculature of the anorectal region may be regarded as two tubes, one surrounding the other (Fig. 5) (37). The inner tube, being visceral, is smooth muscle and is inner- vated by the autonomic nervous system, while the outer funnel-shaped tube is skeletal muscle and has somatic innervation. This short segment of the intestinal tract is of paramount importance because it is essential to the mechanism of fecal continence and also because it is prone to many diseases. The anatomy of the anal canal and perianal structures has been imaged using endoluminal magnetic resonance imaging (38). Investigators found that the lateral canal was signicantly longer than its anterior and posterior part. The anterior external anal sphincter was shorter in women than in men and occupied, respectively, 30% and 38% of the anal canal length. The median length and thickness of the female anterior external anal sphincter were 11 and 13 mm, respectively. These small dimensions explain why a relatively small obstetrical tear may have a devastating effect on fecal continence and why it may be difcult to iden- tify the muscle while performing a sphincter repair after an obstetrical injury. The caudal ends of the external anal sphinc- ter formed a double layer. The perineal body was thicker in women than in men and easier to dene. The supercial transverse muscles had a lateral and caudal extension to the ischiopubic bones. The bulbospongiosus was thicker in men than in women. The ischiocavernosus and anococcygeal body had the same dimensions in both sexes. Posteriorly the anal canal is related to its surrounding muscle and the coccyx. Laterally is the ischioanal fossa with its inferior rectal vessels and nerves. Anteriorly in the male is the urethra, a very important relationship to know during abdominoperineal resection of the rectum. Anteriorly in the female are the perineal body and the lowest part of the pos- terior vaginal wall. & LINING OF CANAL The lining of the anal canal consists of epithelium of dif- ferent types at different levels (Fig. 6). At approximately the midpoint of the anal canal there is an undulating demarcation referred to as the dentate line. This line is approximately 2 cm from the anal verge. Because the rec- tum narrows into the anal canal, the tissue above the dentate line takes on a pleated appearance. These longitu- dinal folds, of which there are 6 to 14, are known as the columns of Morgagni. There is a small pocket or crypt at the lower end of and between adjacent columns of the folds. These crypts are of surgical signicance because for- eign material may become lodged in them, obstructing the ducts of the anal glands and possibly resulting in sepsis. The mucosa of the upper anal canal is lined by colum- nar epithelium. Below the dentate line the anal canal is lined with a squamous epithelium. The change, however, is not abrupt. For a distance of 612 mm above the dentate line there is a gradual transition where columnar, transi- tional, or squamous epithelium may be found. This area, referred to as the anal transitional or cloacogenic zone, has extremely variable histology. A color change in the epithelium is also noted. The rectal mucosa is pink, whereas the area just above the FIGURE 5 & Anal canal. 8 & PART I: ESSENTIAL CONSIDERATIONS
- 26. dentate line is deep purple or plum color due to the under- lying internal hemorrhoidal plexus. Subepithelial tissue is loosely attached to and radially distensible from the inter- nal hemorrhoidal plexus. Subepithelial tissue at the anal margin, which contains the external hemorrhoidal plexus, forms a lining that adheres rmly to the underlying tissue. At the level of the dentate line, the lining is anchored by what Parks (39) called the mucosal suspensory ligament. The perianal space is limited above by this ligament and below by the attachment of the longitudinal muscle to the skin of the anal verge. The area below the dentate line is not true skin because it is devoid of accessory skin struc- tures (e.g., hair, sebaceous glands, and sweat glands). This pale, delicate, smooth, thin, and shiny stretched tissue is referred to as anoderm and runs for approximately 1.5 cm below the dentate line. At the anal verge the lining becomes thicker and pigmented and acquires hair follicles, glands, and other histologic features of normal skin (2). In this circumanal area there is also a well-marked ring of apocrine glands, which may be the source of the clinical condition called hidradenitis suppurativa. Proximal to the dentate line the epithelium is supplied by the autonomic nervous system, while distally the lining is richly inner- vated by the somatic nervous system (40). & ANAL TRANSITIONAL ZONE The anal transitional zone (ATZ) is interposed between uninterrupted colorectal type mucosa (columnar) above and uninterrupted squamous epithelium (anoderm) below, irrespective of the type of epithelium present in the zone itself (41). The ATZ usually commences just above the dentate line. Using computer maps of histology, Thompson- Fawcett et al. (42) found that the dentate line was situated at a median of 1.05 cm above the lower border of the inter- nal sphincter. This is much smaller than the study by Fenger (41), which portrayed the ATZ extending 0.9 cm above the dentate line. Fenger used the traditional Alcian blue stain. This results in overestimation of the length of the ATZ because the pale blue staining is due to staining of supercial nuclei of both squamous anoderm and transi- tional epithelium rather than staining of mucin-producing cells in the transitional epithelium (42). The ATZ is much smaller than commonly thought. The histology of the ATZ is extremely variable. Most of the zone is covered by ATZ epithelium, which appears to be composed of four to nine cell layersthe basal cells, columnar, cuboidal, unkeratinized squamous epithelium, and anal glands. The ATZ epithelium contains a mixture of sulphomucin and sialomucin. The mucin pattern in the columnar variant of the ATZ epithelium and in the anal canal is of the same type and differs from that of colorec- tal-type epithelium. The ndings of a similar mucin pattern in mucoepidermoid carcinoma and in some cases of carci- noma arising in anal stulas as well as in carcinoma suspected of arising in anal glands might indicate a com- mon origin of the neoplasm in the ATZ epithelium. Histochemical study shows that endocrine cells have been demonstrated in 87% of specimens. Their function is unknown. Melanin is found in the basal layer of the ATZ epithelium in 14% of specimens. Melanin cannot be demon- strated in the anal gland but is a constant nding in the squamous epithelium below the dentate line, increasing in amount as the perianal skin is approached. The melanin- containing cells in the ATZ seem a reasonable point of origin for melanoma, as do the ndings of junctional activ- ity and atypical melanocyte hyperplasia in the ATZ. The ATZ epithelium has a dominating diploid popu- lation, although there was a small hyperdiploid peak representing nuclei with a scattered volume considerably higher than that of the main diploid population. This was present regardless of the histologic variant (columnar or cuboid) of the ATZ epithelium. Tetraploid or octoploid populations are not found (41). & ANAL GLANDS The average number of glands in a normal anal canal is six (range, 310) (43). Each gland is lined by stratied columnar epithelium with mucus-secreting or goblet cells interspersed within the glandular epithelial lining and has a direct opening into an anal crypt at the dentate line. Occasionally, two glands open into the same crypt, while half the crypts have no communication with the glands. FIGURE 6 & Lining of the anal canal. CHAPTER 1: SURGICAL ANATOMY & 9
- 27. These glands were rst described by Chiari in 1878 (44). The importance of their role in the pathogenesis of stulous abscess was presented by Parks in 1961 (37). Seow-Choen and Ho (43) nd that 80% of the anal glands are submucosal in extent, 8% extend to the internal sphincter, 8% to the conjoined longitudinal muscle, 2% to intersphincteric space, and 1% penetrate the external sphincter. The anal glands are fairly evenly distributed around the anal canal, although the greatest number are found at the anterior quadrant. Mild to moderate lympho- cytic inltration is noted around the anal glands and ducts; this is sometimes referred to as anal tonsil. In an autopsy study of 62 specimens, Klosterhalfen et al. (45) found that nearly 90% of specimens contained anal sinuses. In fetuses and children, more than half the anal sinuses were accompanied by anal intramuscular glands penetrating the internal anal sphincter, whereas in adult specimens, anal intramuscular glands were rare. & MUSCLES OF THE ANORECTAL REGION & INTERNAL SPHINCTER MUSCLE The downward continuation of the circular, smooth muscle of the rectum becomes thickened and rounded at its lower end and is called the internal sphincter. Its lowest portion is just above the lowest part of the external sphincter and is 11.5 cm below the dentate line (Fig. 5). & CONJOINED LONGITUDINAL MUSCLE At the level of the anorectal ring, the longitudinal muscle coat of the rectum is joined by bers of the levator ani and puborectalis muscles. Another contributing source is the pelvic fascia (11). The conjoined longitudinal muscle so formed descends between the internal and external anal sphincters (Fig. 5) (46). Many of these bers traverse the lower portion of the external sphincter to gain insertion in the perianal skin and are referred to as the corrugator cutis ani (47). Fine and Lawes (48) described a longitudinal layer of muscle lying on the inner aspect of the internal sphincter and named it the muscularis submucosae ani. These bers may arise from the conjoined longitudinal muscle. Some bers that traverse the internal sphincter muscle and become inserted just below the anal valves have been referred to as the mucosal suspensory ligament (37). Some bers may traverse the external sphincter to form a transverse septum of the ischioanal fossa (Fig. 5). In a review of the anatomy and function of the anal longi- tudinal muscle, Lunnis and Phillips (49) speculated that this muscle plays a role as a skeleton supporting and bind- ing the internal and external sphincter complex together, as an aid during defecation by everting the anus, as a support to the hemorrhoidal cushions, and as a determining factor in the ramication of sepsis. & EXTERNAL SPHINCTER MUSCLE This elliptical cylinder of skeletal muscle that surrounds the anal canal was originally described as consisting of three distinct divisions: the subcutaneous, supercial, and deep portions (36). This account was shown to be invalid by Goligher (50), who demonstrated that a sheet of muscle runs continuously upward with the puborectalis and leva- tor ani muscles. The lowest portion of the external sphincter occupies a position below and slightly lateral to the internal sphincter. A palpable groove at this level has been referred to as the intersphincteric groove. The lowest part (subcutaneous bers) is traversed by the conjoined longitudinal muscle, with some bers gaining attachment to the skin. The next portion (supercial) is attached to the coccyx by a posterior extension of muscle bers that combine with connective tissue, forming the anococcygeal ligament. Above this level, the deep portion of the external sphincter is devoid of posterior attachment and proximally becomes continuous with the puborectalis muscle. Ante- riorly, the high bers of the external sphincter are inserted into the perineal body, where some merge and are continu- ous with the transverse perineal muscles. The female sphincter has a variable natural defect occurring along its anterior length (51). This makes interpretation of the isolated endoanal ultrasound difcult and explains overre- porting of obstetric sphincter defects. The external sphincter is supplied by the inferior rectal nerve and a perineal branch of the fourth sacral nerve. From their embryolic study, Levi et al. (52) demonstrated that the external sphincter is subdi- vided into two parts, one supercial and one deep without any connection with the puborectalis. Shak (46) has suggested that the anal sphincter mechanism consists of three U-shaped loops and that each loop is a separate sphincter and complements the others to help maintain continence (Fig. 7). This concept has not been generally accepted. In fact, more recently Ayoub (56) found that the external sphincter is one muscle mass, not divided into layers or laminae, and that all bers of the external sphincter muscles retain their skeletal attachment by the anococcygeal ligament to the coccyx. Clinical experience supports Ayoubs concept; we have not been able to identify Shaks three-part scheme. Indeed, during posta- nal repairs for anal incontinence, the external sphincter, puborectalis, and levator ani muscles present as one contin- uous funnel-shaped sheet of skeletal muscle. The currently accepted perception of the arrangement of the external FIGURE 7 & Shak loops. Source: From Ref. 46. 10 & PART I: ESSENTIAL CONSIDERATIONS
- 28. sphincter is that it is one continuous circumferential mass, a concept in accordance with a study in which anal endoso- nography was used (53). & PERINEAL BODY The perineal body is the anatomic location in the central portion of the perineum where the external sphincter, bulbocavernosus, and supercial and deep transverse peri- neal muscles meet (Fig. 8). This tends to be a tendinous intersection and is believed to give support to the perineum