Gaylinn Daniel Media Assistance
131
MEDIA ASSISTANCE: EXPLORING THE EFFECTS OF THREE METHODS OF GUIDED RELAXATION ON STRESS WITH ADOLESCENTS by Daniel L. Gaylinn A dissertation submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy in Clinical Psychology Institute of Transpersonal Psychology Palo Alto, California May 22, 2009 I certify that I have read and approved the content and presentation of this dissertation: ________________________________________________ __________________ Patricia Campbell, Psy.D., Committee Chairperson Date ________________________________________________ __________________ Janice Holden, Ed.D., Committee Member Date ________________________________________________ __________________ Anees Sheikh, Ph.D., Committee Member Date
-
Upload
dan-gaylinn-phd -
Category
Documents
-
view
120 -
download
3
Transcript of Gaylinn Daniel Media Assistance

MEDIA ASSISTANCE:
EXPLORING THE EFFECTS OF THREE METHODS OF GUIDED RELAXATION ON
STRESS WITH ADOLESCENTS
by
Daniel L. Gaylinn
A dissertation submitted
in partial fulfillment of the requirements
for the degree of Doctor of Philosophy
in Clinical Psychology
Institute of Transpersonal Psychology
Palo Alto, California
May 22, 2009
I certify that I have read and approved the content and presentation of this dissertation: ________________________________________________ __________________ Patricia Campbell, Psy.D., Committee Chairperson Date ________________________________________________ __________________ Janice Holden, Ed.D., Committee Member Date ________________________________________________ __________________ Anees Sheikh, Ph.D., Committee Member Date

UMI Number: 3358661
Copyright 2009 by Gaylinn, Daniel L.
All rights reserved
INFORMATION TO USERS
The quality of this reproduction is dependent upon the quality of the copy
submitted. Broken or indistinct print, colored or poor quality illustrations and
photographs, print bleed-through, substandard margins, and improper
alignment can adversely affect reproduction.
In the unlikely event that the author did not send a complete manuscript
and there are missing pages, these will be noted. Also, if unauthorized
copyright material had to be removed, a note will indicate the deletion.
______________________________________________________________
UMI Microform 3358661 Copyright 2009 by ProQuest LLC
All rights reserved. This microform edition is protected against unauthorized copying under Title 17, United States Code.
_______________________________________________________________
ProQuest LLC 789 East Eisenhower Parkway
P.O. Box 1346 Ann Arbor, MI 48106-1346

Copyright
©
Daniel L. Gaylinn
2009
All Rights Reserved
ii

Abstract
Media Assistance:
Exploring the Effects of Three Methods of Guided Relaxation on Stress With Adolescents
by
Daniel L. Gaylinn
I explored the effects of 3 methods of delivering a brief 10-minute guided relaxation with an
ethnically diverse population of 77 adolescents with an average age of 15.2 years within a
Northern California high school classroom. Of the 77 participants recruited for the study, a total
of 21 appeared to disengage from the study as evidenced by the minimal variability of their
responses to the scale used for the study and were thus removed from the primary analyses.
Using a pre-post experimental research design, multiple repeated measures analyses of variance
revealed that, of the 3 delivery methods explored (audio-guided, video-guided, and live-guided),
all 3 produced statistically significant decreases in all 5 subscales of nonclinical psychological
stress as measured by the Smith Stress Symptoms Inventory—State scale (Autonomic
Arousal/Anxiety, Attention Deficit, Worry/Negative Emotion, Striated Muscle Tension, and
Interpersonal Conflict/Anger). No 1 method of delivery was significantly more effective in its
reduction of self-reported levels of psychological stress than any other. Preliminary correlations
showed that males with low grade point averages were more likely to disengage. Significant
decreases in the levels of Attention Deficit, Autonomic Arousal/Anxiety and Striated Muscle
Tension were reported by participants who also reported closing their eyes to some extent during
the audio or video conditions. Participants in the afternoon classes reported significantly higher
Interpersonal Conflict/Anger and Worry/Negative Emotion scores than participants in the
morning classes. Subjectively, many participants responded favorably to their exposure to the 3
iii

treatment conditions, and most participants reported an overall preference for the video condition
over the other 2. The results of this study has implications for the possible adjunctive therapeutic
role electronic media-assisted psychological treatments may play in the modern lives of
adolescents as well as to the relative convenience of providing media-assisted programs to
adolescents by teachers in a high school setting.
iv

Dedication
I dedicate this work to children feeling lost in the darkness.
Your light resides within; your spirit is larger than belief itself.
v

Acknowledgements
I would like to express my deepest gratitude to everyone whose support, encouragement,
and guidance helped make this work a reality. My thanks go to my committee chairperson, Dr.
Patricia Campbell, whose steadfast support served as a lifeline to me during periods that felt like
insurmountable setbacks. Without her guidance and assistance, this dissertation would not have
been possible.
I would like to thank my committee members, Dr. Janice Holden and Dr. Anees Sheikh,
whose patience, rigor, and positivity served and continues to serve as an inspiration to me in my
academic endeavors. Great thanks go to them for demonstrating by example the essence of
scientific scholarship.
In addition, a thank you goes to everyone whose advice and guidance helped to clarify for
me the many questions and concerns that arose over the course of this project. They tolerated my
pedantic nature with patience and positivity. In this group, I include the faculty and staff at the
Institute for Transpersonal Psychology, my statistics assistant, Dr. Jean Oggins, and all those I
count among my friends and esteemed colleagues in the field.
I wish to thank all of the teachers and students involved with the Focus on Success
program at Henry M. Gunn high school, especially Tarn Wilson, whose willingness to grant me
access to the students could not have come at a better time. Of course, special thanks go to all of
the students who participated in this study. May you continue to find benefit from your practice
of relaxation.
Last but not least, I wish to thank my family whose love, humor, and temerity is proof of
nothing short of a miracle. Thank you for believing in me. We have more than any other family I
have ever known.
vi

Table of Contents
Abstract .......................................................................................................................................... iii
Dedication ........................................................................................................................................v
Acknowledgements........................................................................................................................ vi
List of Tables ...................................................................................................................................x
Chapter 1: Introduction ....................................................................................................................1
Adolescents, Media, and Stress ...........................................................................................1
Psychotherapy and Visual Media.........................................................................................2
Visual Media Research ........................................................................................... 3
Visual Media Therapy............................................................................................. 4
The Present Study ................................................................................................................5
Chapter 2: Literature Review...........................................................................................................9
Psychological Stress.............................................................................................................9
Stress in Adolescence ........................................................................................... 11
Stress in Adolescent Development ....................................................................... 12
Stress Management ............................................................................................................15
Relaxation Response............................................................................................. 16
Guided Relaxation .............................................................................................................18
Audio-Guided Relaxation ..................................................................................... 19
Video-Guided Relaxation ..................................................................................... 21
Audio- and video-Guided Relaxation ................................................................... 24
Chapter 3: Method .........................................................................................................................26
Research Design.................................................................................................................26
Participants.........................................................................................................................28
vii

Instruments.........................................................................................................................31
Demographic Questionnaire ................................................................................. 34
Reactions to an Experiential Exercise Scale (REES) ........................................... 35
Smith Stress Symptoms Inventory-State (SSSI-S) ............................................... 37
Procedure ...........................................................................................................................42
Treatment Conditions............................................................................................ 46
Chapter 4: Results ..........................................................................................................................49
Treatment of Data ..............................................................................................................49
Data Analysis ........................................................................................................ 50
Analysis of Subjective Reports............................................................................. 52
Results of the Analyses......................................................................................................53
Additional Findings .............................................................................................. 65
Qualitative Findings.............................................................................................. 65
Chapter 5: Discussion ....................................................................................................................69
Summary and Interpretation of Findings ...........................................................................69
Limitations and Delimitations............................................................................................79
Directions for Future Research ..........................................................................................91
References......................................................................................................................................95
Appendix A: Informed Consent...................................................................................................107
Appendix B: Demographic Questionnaire...................................................................................109
Appendix C: Smith Stress Symptoms Inventory-State (SSSI-S).................................................110
Appendix D: Reactions to an Experiential Exercise Scale (REES).............................................111
Appendix E: Guided Relaxation Transcript.................................................................................112
Appendix F: Instructions for the Interventions............................................................................114
Appendix G: Permission to Screen Digital Video Disc...............................................................115
viii

Appendix H: Pretreatment Talk Transcript..................................................................................116
Appendix I: Reader / Transcriber Confidentiality Agreement ....................................................117
Appendix J: Relaxation Techniques Handout..............................................................................118
ix

List of Tables Tables 1 Demographic Variables .............................................................................32
2 Guided Relaxation Treatment Schedule for All Seven Classes.................45
3 Reported Media Preferences and Prior Experience With Relaxation Techniques .................................................................................................55 4 Descriptive Statistics for Baseline Subscales of the Smith Stress Symptoms Inventory-State.........................................................................56 5 Descriptive Statistics for the Conflict/Anger and Worry/Negative Emotion Subscales of the Smith Stress Symptoms Inventory-State for All Treatment Conditions and Baseline Scores With Time of Day as a Covariate ....................................................................................................58 6 Descriptive Statistics for the Muscle Tension, Attention Deficit, and Autonomic Arousal of the Smith Stress Symptoms Inventory-State for All Treatment Conditions and Baseline Scores With Eye
Closure as a Covariate ...............................................................................60
7 Summary of Significant Stress Reductions for All Three Treatment Methods......................................................................................................64 8 Summary of Common Themes and Method Preferences From Subjective Reports .....................................................................................67
x

1
Chapter 1: Introduction
Adolescents, Media, and Stress
Adolescents growing up in the 21st century live in a world saturated with all forms of
visual media, including television, videos, and videogames. Their pervasive exposure to such
media has steadily increased over the last decade (Comstock & Scharrer, 2006). Studies have
shown that adolescents tend to spend more time watching some form of visual media than they
do engaging in any other waking activity, including being in school (Roberts, Henriksen, &
Foehr, 2004). Such immersion in visual media makes modern adolescents unlike any preceding
generation of adolescents, leading one researcher to name this particular segment of the
population the “new media generation” which she described as
the first cohort to have grown up learning their ABCs on a keyboard in front of a computer screen, playing games in virtual environments rather than their backyards or neighborhood streets, making friends with people they have never and may never meet through Internet chat rooms, and creating custom CDs for themselves and their friends. (Brown, 2005, p. 279)
Some researchers have correlated adolescent exposure to visual media with the prevalence of
stress in this demographic, leading some researchers to suggest that adolescents may be using
media partly as a means of coping or at least as a means of temporarily escaping the
uncomfortable feelings associated with stress (Bickham et al., 2003; Lohaus et al., 2005).
In direct contrast with this postulation, some researchers suggested that visual media may
in fact be evoking the stress response. Laboratory studies exploring the attentional and
physiological effects of visual media have revealed that the simple formal features of visual
media, such as cuts, edits, zooms, pans, or sudden noises routinely activate the orienting reflex,
an instinctual and spontaneous reaction to any sudden or novel stimulus (Kubey &
Csikszentmihályi, 1990; La Ferle, Edwards, & Lee, 2000; Lang, Zhou, Schwartz, Bolls, &
2
Potter, 2000; Reeves & Thorson, 1986). As Halgren (1992, p. 205) originally discovered, this
orienting reflex is an autonomic reaction originating in the limbic region of the brain that gives
rise to the fight or flight—that is, stress—response.
These contrasting positions raise important questions as to the role of visual media in the
process of mediating a psychological condition such as stress. Whereas adolescents may be using
visual media partly as a means of coping with stress (Lohaus et al., 2005), the impact of this
media may be implicitly evoking the stress response (La Ferle et al., 2000). This contradiction
may be resolved by a theory put forth by a small number of media researchers that postulates that
the effect of visual media may be a dialectical one in that the viewer’s own unique experiences,
motivations, and expectations interact with the media to a greater degree than has been
previously assumed (Brown, 2006; Brown & Walsh-Childers, 2002; Levy & Windahl, 1985;
Rubin, 2002; Steele & Brown, 1995; Ward, Gorvine, & Cytron-Walker, 2002).
Theorists who adhere to this Media Practice Model hold that the influence of a particular
medium is a function of the user’s sense of identity, the user’s reason for selecting the media, the
context or situation in which one uses the medium, and the user’s interpretation of that medium
(Steele & Brown, 1995). This model supports the notion that a medium used for a therapeutic
purpose may influence measures associated with that purpose. Although the purpose of the
present study is not to examine this theory directly, the theory does describe how viewers’
expectations influence the medium’s effects inasmuch as these effects correspond with the
medium’s therapeutic purpose.
Psychotherapy and Visual Media
The association between psychotherapy and visual media began when they both emerged
at the same moment in history. In 1895, when Sigmund Freud, the pioneer of what has become

3
modern psychotherapy, published his seminal work, Studies in Hysteria (Freud, 1895/2004), he
initiated the commencement of the scientific analysis of purely mental conditions. Mere months
later, Auguste and Louis Lumière (as cited in Tarnas, 1995, p. 88) unveiled their cinematograph
invention, marking an event that most film historians consider to be the birth of cinema as a
commercially viable medium (Salazard, Casanova, Zuleta, Desouches, & Magalon, 2003). Since
that time, both psychotherapy and visual media have made great strides towards the realization
of what may be considered a shared impulse: to project the image of mind in a linguistically or
visually tangible form so as to illuminate and influence its inner workings. Although these
disciplines have dramatically different intentions, insofar as psychotherapy is to treat mental
illness and electronic media are to inform and entertain, they do seem to share this unique
purview on the mind.
Since their beginnings, both psychotherapy and visual media have made great strides in
their respective domains. On the one hand, visual media have integrated story, performance,
stylistic techniques, and compelling images to influence audiences’ moods and emotions,
evoking sadness, anger, curiosity, joy, and even fear. On the other hand, psychotherapy employs
scientific research and clinical practices that yield a vast range of instruments and methodologies
that influence the critical functioning of the human mind. Yet, it has been within only the past 2
decades that researchers and clinicians have begun to examine and explore the role that visual
media may play in the influence and treatment of the mind.
Visual media research. Although a study on the mental effects of a photo-play, which
was described as a series of projected images on a screen, can be found in the psychology
literature as early as 1916 (Münsterberg, 1916), serious and scientific inquiry into the effects of
visual media did not emerge until “the advent and market penetration of television in the 1950s

4
[was] coupled with concerns about unconscious influences of advertising, in all its forms and
venues” (Fischoff, 2005). As a result of the concern over potentially “subliminal effects” in
media, specifically in advertisements, Media Psychology emerged as a subdiscipline in
psychology, evidenced by the inauguration of the Journal of Media Psychology in 1996 and the
inception of Division 46 for media psychology in the American Psychological Association.
Similarly, the emergence of communication science and media research resulted in psychologists
publishing in nonpsychology journals such as the Journal of Communication, founded in 1951,
and the Journal of Broadcasting and Electronic Media, founded in 1956. Together, these journals
have offered a wide range of content pertaining to the changing faces and interactions between
media and psychology.
In these and other peer-reviewed journals, concern has been raised regarding the
influence of visual media on children and adolescents, particularly for three reasons: (a) Youth
spend more time with media than they do in school or with their parents, (b) The media
frequently depicts glamorous portrayals of risky adult behavior, and (c) Parents and other
socialization agents have been unable to direct youth towards less risky behaviors (Steele &
Brown, 1995). In one early example of such research, the investigation of the influence of media
on children issued a severe indictment of all motion pictures as being an inspiration for all bad
behavior among children (Thurstone, 1931).
Visual media therapy. In contrast to these concerns, some clinicians have begun to
employ various therapeutic uses of media in their practices, including (a) Cinematherapy,
combining bibliotherapy with film-viewing as a means of inducing a therapeutic effect or
catalyzing a therapeutic discussion (Berg-Cross, Jennings, & Baruch, 1990); (b) Instructional
Media, transmitting information regarding a treatment, procedure, or therapeutic process to

5
inform clients of their roles and any preparations or decisions they must make during the course
of treatment (Wilkins et al., 2006); (c) Media Recall, recording and later reviewing recordings of
clinical sessions (Trierweiler, Nagata, & Banks, 2000); (d) Creative Media, using the tools of
media production, such as audiorecording and videorecording equipment, as a form of art
therapy enabling clients to reflect on their experiences, express themselves, and increase their
self-awareness (Orr, 2006); (e) Biofeedback, using auditory or visual feedback to depict
physiological processes in real-time (e.g., heart rate or brainwave activity) and to facilitate a
greater awareness of them (Masterpasqua, 2005); (f) Virtual Reality, recreating an artificial
environment in which a client can experience known fears in relative safety (Riva, 2003); (g)
Media Assistance, a term herein coined by the author, defined as the use of sounds and images
from audio or video content, such as music, nature imagery, and verbal inductions, for the
purpose of guiding individuals through an internal psychological process. This method draws
upon research dating from 1970 to the present that has investigated the use of media programs as
a means of eliciting psychological processes, most notably for relaxation (Boersma & Gagnon,
1992; Byrnes, 1996; DeSchriver & Riddick, 1990; Putman, 2000; Robar, 1978; Smyth, Soefer,
Hurewitz, & Stone, 1999; Tsai, 2004; Ulett, Akpinar, & Itil, 1972; Wells, 2005; Wood, 1986).
The term Media Assistance is intended to unify these disparate studies into a single therapeutic
method and to initiate inquiry into the use of media as a guide for psychological processes.
The Present Study
Of the seven clinical methods of employing some form of visual media in the service of
psychotherapeutic treatment, Media Assistance serves as the intervention to be investigated in
the present study. The purpose of selecting Media Assistance is threefold.

6
First, many adolescents already use visual media as a way of managing or at least
temporarily escaping the stress they experience in their day-to-day lives (Bickham et al., 2003;
Lohaus et al., 2005).
Second, despite the many therapeutic claims made by the producers of commercially
available audio and video tapes, CDs, and DVDs that principally utilize Media Assistance as a
means of delivering relaxation, such as Direct Source Special Products (2006), surprisingly no
studies in the literature were found to support the efficacy of these claims. This finding alone
may serve to justify the rationale behind the present study, in which I aim to explore the validity
of these claims as to the efficacy of nature videos in the management of stress.
Third, numerous studies demonstrate the clinical efficacy of elements that may be
considered a form of Media Assistance, including listening to audiotapes of guided relaxation or
watching nature imagery on video, as a way of managing stress (Boersma & Gagnon, 1992;
Byrnes, 1996; DeSchriver & Riddick, 1990; Putman, 2000; Smyth et al., 1999; Tsai, 2004; Ulett
et al., 1972; Wells, 2005; Wood, 1986). These elements of Media Assistance have been shown to
trigger the relaxation response (RR; Jacobs, Benson, & Friedman, 1996), effectively reducing
symptoms of psychological stress (Tsai, 2004; Wells, 2005). Surprisingly, only one study within
the past 20 years was found to have been published comparing audio and video methods of
facilitating relaxation (Byrnes, 1996).
The present study was aimed in part to replicate and update these findings specifically
with regard to how in-person guided relaxation (Cropley, Ussher, & Charitou, 2007), audiotaped
relaxation (Smyth et al., 1999), video guided relaxation (DeSchriver & Riddick, 1990; Wells,
2005), or both audio and video guided relaxation (Byrnes, 1996) have each been shown to
facilitate the management of some indicators of psychological stress. Because the use of audio or

7
video tape is significantly cheaper and more readily available to the average person than is
working with a professional clinician, research on the use of media as a therapeutic adjunct, or
Media Assistance, may help to serve individuals in an efficacious manner.
To explore the clinical viability of Media Assistance, I employed a prepost experimental
research design to investigate the potential differences between three different methods of
delivering a guided relaxation to a population of adolescents. The purpose of this study was to
investigate the differences in effectiveness between a Video-Guided Relaxation Program, VGRP;
an Audio-Guided Relaxation Program, AGRP; and a Live, in vivo, Guided Relaxation Program,
LGRP, on the self-reported levels of stress among a sample of high school students. All three
treatment conditions lasted 10 minutes in duration and employed the same guided relaxation
transcript (Appendix E) that I prerecorded or read live.
Upon meeting the criteria for participation in the study, participants completed a
preassessment research packet made up of a demographic questionnaire (Appendix B) and a
brief assessment of frequently reported symptoms of stress (SSSI-S; Appendix C; Piiparinen &
Smith, 2003, 2004), which established a baseline stress state upon which to compare the effects
of the treatments. Next, I utilized the seven separate classes to serve as separate treatment groups
to receive the first of the three treatment conditions. Each group received the remaining two
treatment conditions over the course of the next 3 days. All participants received all three
treatment conditions by the end of the 4 days. After each exposure to treatment, participants
again completed the stress symptoms scale as well as a scale designed specifically for the present
study to measure the participants’ reactions to the experiential exercise (REES; see Appendix D).
This study was designed mainly to answer one specific research question: “Is there a
relationship between the means of delivering guided relaxation to adolescents and the amount of

8
stress that they report?” If a relationship was found, then a follow-up question explored in this
study was “What is the magnitude of the relationship between the method of delivering guided
relaxation to the amount of stress adolescents report?” Secondary research questions examined
the extent to which reactions to the treatments influenced their effects and what demographic
variables, if any, correlated with the influence of the treatment conditions on the reported levels
of stress.

9
Chapter 2: Literature Review
Psychological Stress
Psychological stress is defined as “a particular relationship between the person and the
environment that is appraised by the person as relevant to the individual’s well-being and in
which the person’s resources are taxed or exceeded” in a foundational study (Lazarus &
Folkman, 1984, p. 152). The term stress, first used in the psychological sense by Harvard
physiologist Walter B. Cannon, identifies the physiological fight or flight (i.e., stress) response
as evidenced by the biochemical changes that take place within the body during times of
difficulty by generating the quick bursts of energy needed to fight or flee the threat of danger
(1914).
The term stress was brought into prominent use in psychology by Hans Selye who found
that any threat of danger, be it real or imagined, can elicit a cascading physiological effect
throughout the individual’s entire body (Selye, 1950). His early research revealed a universal
reaction to stress, broken into three stages, termed the General Adaptation Syndrome (GAS;
Selye, 1956). Recent studies have supported and elaborated upon this paradigm (Lazarus, 2007;
Uchino, Smith, Holt-Lunstad, Campo, & Reblin, 2007). The GAS defines the first stage, termed
Alarm, as the body’s stress (i.e., fight or flight) response to the perceived presence of danger,
triggers the production of adrenaline and cortisol along the hypothalamic-pituitary-adrenal axis
of the autonomic nervous system (Tsigos & Chrousos, 2002). If the stressor persists, stage two,
termed Resistance, occurs when the body attempts to regain homeostasis in spite of the stressor.
Because the body cannot resist the stressor indefinitely, stage three, termed Exhaustion, occurs as
the body’s resources are gradually depleted and autonomic nervous system symptoms appear,
such as increased sweating, heart rate, respiration, muscle tension, metabolism, and blood

10
pressure (Segerstrom & Miller, 2004; Selye, 1950). Additional physiological symptoms
associated with stress include a contracted anus, dilated pupils, sharpened vision and hearing, a
feeling of butterflies in the stomach, or cold hands and feet resulting from the redirection of
blood flowing away from the digestive system and extremities and into the larger muscles of
body facilitating motility (Selye, 1950; Taché & Selye, 1985).
Whereas the biochemical changes associated with stress at one time provided ancestral
humans with the quick bursts of energy that they needed to fight or flee a threat of danger
(Cannon, 1914), modern humans must learn how to manage stress in a manner that is more
appropriate to societal customs. Failure to appropriately manage the symptoms of psychological
stress and its consequent biochemical and physiological changes has been shown to lead to a
wide array of social and health problems. Some short-term effects of unmanaged stress include
the exhibition of aggression (Hampel & Petermann, 2005), anxiety, depression (Segrin, 1999),
suicidal ideation, and hopelessness (Dixon, Rumford, Heppner, & Lips, 1992). Some long-term
effects include substance abuse (Macleod et al., 2004; Sadava & Pak, 1993) and various
behavioral problems (Compas, Connor-Smith, Saltzman, Thomsen, & Wadsworth., 2001;
Compas, Orosan, & Grant, 1993; McNamara, 2000).
Although the direct association between unmanaged stress and physical illness has
remained somewhat modest in strength (Barr, Boyce, & Zeltzer, 1996), the excessive presence of
stress hormones has been shown to be coincident with various maladies of the vital systems of
the body. The autonomic nervous system may be affected causing headaches (Wittrock &
Forkaer, 2001), sleep disturbances (Farnill & Robertson, 1990), irritable bowel syndrome
(Blanchard & Turner, 2000), and high blood pressure (Schwartz, Pickering, & Landsbergis,
1996). The endocrine and immune systems can be affected causing chronic fatigue (Chalder,

11
Cleare, & Wessely, 2000), rheumatoid arthritis (Zautra & Smith, 2001), lupus (Peralta-Ramírez,
Jiménez-Alonso, Godoy-García, & Perez-García, & the Group Lupus Virgen de las Nieves,
2004), and asthma (Rietveld, Beest, & Everaerd, 1999), as well as a susceptibility to infection (S.
Cohen, 2002), illness (J. Cohen, Tyrrell, & Smith, 1991), and the common cold (Stone,
Bovbjerg, Neale, & Napoli, 1992).
Stress in adolescence. Although stress is a condition that one must learn to manage
throughout one’s lifespan, it may not emerge as a critical condition until one reaches adolescence
(Wagner, Abela, & Brozina, 2006). This is partly due to the physical and hormonal changes that
occur in a maturing body between ages of 10 and 20, but it may also pertain to the many
cognitive, social, and emotional changes that emerge during this period as well. In this unique
phase of life, as the individual is transformed from a child into an adult, a great many
possibilities for learning and maturation emerge, but it can also be a period in which personal
resources and social limits are routinely tested and frequently exceeded.
Consequently, psychological stress is considered to be a natural part of adolescent
development by many researchers (Hutchinson, Baldwin, & Oh, 2006; Kraag, Zeegers, Kok,
Hosman, & Abu-Saad, 2006; Washburn-Ormachea, Hillman, & Sawilowsky, 2004). Whereas
studies demonstrate that adolescents are most particularly affected by those stressors that arise
out of ongoing and daily routines over which they perceive they have little or no control, such as
school assignments, quarrels within peer relationships, family responsibilities, and other stressors
(Frydenberg & Lewis, 2004; Hurrelmann & Raithel, 2005; Hutchinson et al., 2006), such
challenges may be exacerbated by the incidence of traumatic life events, such as accidents,
illnesses, parental divorce, child abuse, or the loss of a loved one (Nastasi et al., 2007).
Teenagers whose present living environment is chaotic, whose upbringing taxes their resources,
12
or who presently suffer from a serious emotional or behavioral problem, are more likely to have
difficulty coping with stress during adolescence and later in life (J. Compas, 1987; Hampel &
Petermann, 2006; Windle, 1992).
It is important to note that stress has emerged as a significant issue within the adolescent
population in recent years. The literature reveals that the rate of adolescent suicides (Gibbons,
Hur, Bhaumik, & Mann, 2006) as well as adolescents’ need for antipsychotic and antidepressant
medications (dosReis et al., 2005) have both increased markedly in the last decade. Although it
would be erroneous to posit a correlation between these findings and the increased rate of
adolescent use of visual media as noted in Chapter 1 (Comstock & Scharrer, 2006), such findings
suggest the need for a close investigation into how stress is impacting this particular segment of
the population.
Stress in adolescent development. As adolescents develop and explore new roles and
behaviors, they must learn new ways of managing the stress they face lest they fall prone to
dangerous or risky behaviors as an escape from the discomfort engendered by stressful
encounters (i.e., use of drugs or promiscuous sex; Compas et al., 2001; Macleod et al., 2004).
Stress in adolescence may be considered closely tied with adolescent development. Two
developmental changes are undergone in adolescence according to prominent psychological
theory: (a) the cognitive developmental stage of formal operations is achieved (Piaget, 1972),
and (b) the psychosocial developmental stage of self-identity is forged (Erikson, 1950, 1968).
Both of these theories of adolescent development are discussed below regarding their relevance
to the present study, followed by some discussion of identity development particularly and how
media may influence it.
13
According to cognitive developmental theorist, Jean Piaget, adolescence is the phase of
life when abstract reasoning, or what he called formal operational thinking, begins to appear
(Piaget, 1972). The stage of formal operations enables individuals to extend their thoughts
beyond the here-and-now and to begin to make predictions and create plausible ideals based on
hypotheses using logic and reason. While this stage enables individuals to engage thoughtfully
and meaningfully in the larger social issues of society (e.g., pollution or racism), this capacity
also makes the individual susceptible to the anxiety, worries, and stressors that such awareness
may bring and the existential threats they potentially impose (Piaget, 1972). Thus, the ability to
recognize and manage the uncomfortable feelings and emotions that such cognitions may bring
helps to lay the cognitive foundation that the adolescent will need to establish the appropriate
thinking and stress management habits the individual will need to draw upon later as an adult.
With regard to the present study, formal operations may predispose teens to the stress that
accompanies exposure to certain forms of media, but it may also help teens to learn how to
recognize and manage stress before it becomes detrimental (Harrison, 2006).
According to psychosocial developmental theorist, Erik Erikson, adolescence can be
conceptualized as the period of life in which the emerging self, or ego, must establish an identity
as separate from but interconnected with the wider social context or consequently suffer from
role confusion (Erikson, 1950, 1968). In Erikson’s view, psychosocial development may be seen
from the point of view of the conflicts, inner and outer, which the vital personality weathers, re-emerging from each crisis with an increased sense of inner unity, with an increase in the capacity “to do well” according to his [sic] own standards and the standards of those who are significant to him. (Erikson, 1968, pp. 91-92)
Thus, the adolescent self is psychologically characterized as a tester of social limits, an explorer
of roles and behaviors, and a pursuant of existential quandaries such as “Who am I?” and “Why
am I here?” Adolescence can be viewed as a period of moratorium, as a temporary postponement

14
of societal commitments, such that a differentiated self-identity can be established (Erikson,
1968).
In the past 20 years, researchers have expanded on Erikson’s fifth (i.e., adolescent) stage
of development. Among them, James Marcia has examined the role of identity formation from
the two aspects of crisis and commitment (Marcia, 1966, 1980). According to Marcia’s
perspective, adolescent identity can be conceptualized as being one of four identity statuses that
he describes according to the presence or absence of crisis (i.e., defined as making one’s own
decisions) and commitment (i.e., defined as investing personally in an ideology). These four
identity statuses are (a) identity diffusion (i.e., the absence of both crisis and commitment), (b)
identity foreclosure (i.e., the presence of commitment in the absence of crisis), (c) moratorium
(i.e., the presence of crisis in the absence of commitment), and (d) identity achieved (i.e., the
presence of both crisis and commitment; Marcia, 1980). According to this theory, these identity
statuses can be ordered into two subcategories such that identity diffused and identity foreclosed
can be considered to be lower and less sophisticated, whereas moratorium and identity achieved
can be considered to be higher and more sophisticated (Marcia, 1980).
This theory supports the assertion that stress can be considered an integral part of
adolescent development insofar as adolescents must forge a new identity by differentiating
themselves from the beliefs, values, and goals that are passed on to them by their parents and
society and committing to an identity based upon their own existential exploration. This
exploration can become a stressful period of confusion and doubt, but the avoidance of this vital
piece of development may result in psychological stagnation and a proneness to pathology
(Marcia, 1980). The establishment of a stable adult identity, then, may be considered a

15
consequence of the adolescent’s capacity to recognize and manage the stress generated in the
course of existential exploration (Johnson, Buboltz, & Seeman, 2003; Makros & McCabe, 2001).
It is worth noting that adolescent exploration may occasionally be sought through the use
of visual media (Bickham et al., 2003; Lohaus et al., 2005). However, studies have suggested
that the content of the media to which many adolescents gravitate tends to portray messages and
behaviors that promote unattainable standards and expectations (Csikszentmihályi & Schneider,
2000; Signorielli & Kahlenberg, 2001). Such portrayals may contribute to the stress they feel,
rather than offering some relief from it. Some research of commercial television suggests that
market researchers aim to influence and monetize the moods and behaviors of the adolescent
demographic specifically (Comstock & Scharrer, 2006; Desmond & Carveth, 2007; Nelson &
McLeod, 2005). This type of directive influence may not be conducive to their general health
and well-being, but may instead encourage maladaptive behaviors such as aggressiveness
(Anderson et al., 2003; Darwish, 2002), disordered eating (e.g., Alperin, 2005; Tiggemann,
2005), sexual promiscuity (L’Engle, Brown, & Kenneavy, 2006; Tolman, Kim, Schooler, &
Sarsoli, 2007), substance abuse (e.g., Primack, Gold, Land & Fine, 2006; Stacy, Zogg, Unger, &
Dent, 2004), and other risky behaviors (e.g., Buwalda, 2004). It is for this reason that alternative
forms of media content, such as those associated with Media Assistance, are explored in the
present study, and serve as the basis for investigation.
Stress Management
Traditionally, at least four different kinds of approaches have been clinically employed as
a form of stress management: (a) guided relaxation training, (b) social problem solving, (c) social
adjustment and emotional self-control, and (d) a combination of each of these approaches (Kraag
et al., 2006). Given the one-way (i.e., prerecorded) communication that is implicit in the Media
16
Assistance method of treatment, guided relaxation served as the best approach to stress
management for exploration in the present study. Before discussing guided relaxation as an
approach to stress management, the way in which relaxation itself influences the mind and body
and impacts stress warrants further discussion.
Relaxation response. As noted above, cardiologist Herbert Benson (1977) demonstrated
that an individual can use one’s mind to change physiology for the better, thus improving one’s
health and emotional outlook on life. In a seminal paper published by Benson and his colleagues
(Benson, Beary, & Carol, 1974), the relaxation response (RR) was demonstrated to initiate an
integrated set of physiological changes that directly counteract the fight or flight (i.e., stress)
response thereby triggering the body’s natural restorative process. According to Benson, a person
can shut off or tune out the physiological danger signals associated with stress by initiating the
RR (e.g., by taking deep diaphragmatic breaths, actively relaxing their muscles, slowly repeating
calming words or phrases, or passively ignoring distracting thoughts or feelings). After 3
minutes, the stress response burns out as the cerebral cortex stops sending emergency signals to
the hypothalamus, which in turn ceases to send panic messages to the nervous system such that
heart and breathing rate, muscle tension, metabolism, and blood pressure all return to their
normal levels (Benson, Beary & Carol, 1974). Whereas the stress response is characterized by
sympathetic activation stimulating the body to react to potential threats, the RR is characterized
by parasympathetic activation that enables the body to maintain a generalized state of
homeostasis (Jacobs et al., 1996).
Additional studies from the 1970s showed that triggering the RR decreases oxygen
consumption, and lowers heart rate, arterial blood pressure, and the rate of respiration (Wallace
& Benson, 1972). In the 1980s, the regular and extensive elicitation of the RR for 4-6 weeks of

17
daily practice was associated with more enduring physiological changes such as a generally
reduced responsiveness to the stress hormone, norepinephrine, an increased resiliency to stress,
and the reduced need for medication (Benson, Arns, & Hoffman, 1981; Lehmann, Goodale, &
Benson, 1986).
In more recent studies, the regular triggering of the relaxation response has been shown
to help individuals manage many of the symptoms associated with anxiety, addiction, and stress,
and generally improve their mental and physical functioning (Deckro et al., 2002; Scheufele,
2000). Among middle school populations, students whose classes were taught by teachers trained
in the relaxation response curriculum exhibited higher academic performance, as measured by
GPA (p = .0001), better work habits (p = .0001), and a greater degree of cooperativeness (p =
.0001) than those students whose teachers were not trained in the RR curriculum (Benson,
Wilcher et al., 2000). Another recent study showed that daily practice of the RR has been linked
with significant improvements in symptoms associated with irritable bowel syndrome (Keefer &
Blanchard, 2001).
Popular techniques for triggering the relaxation response (RR) include massage,
progressive muscle relaxation (PMR), yoga stretching, diaphragmatic breathing, imagery,
meditation, or some combination of these (Smith, Amutio, Anderson, & Aria, 1996). Benson
(1977) proposed four underlying elements that should be present during the relaxation,
regardless of the technique being used, in order to effectively elicit the RR: (a) the presence of an
object on which to focus, such as a candle, a mantra, one’s breath, a television; (b) a quiet
environment; (c) a comfortable position; and (d) a positive attitude. These elements, coupled
with three cognitive skills proposed by Smith (1990), will ensure the influence of the technique
on cognitive and somatic arousal. These cognitive skills are (a) focusing, described as the ability

18
to identify, differentiate, maintain attention on, and return attention to simple stimuli for an
extended period; (b) passivity, described as the ability to stop unnecessary goal-directed and
analytic activity; and (c) receptivity, described as the ability to tolerate and accept experiences
that may be uncertain, unfamiliar, or paradoxical. These underlying elements and cognitive skills
are implicitly beneficial, but aid the efficacy of the particular relaxation technique when
practiced over time (Smith, 1990, p. 65).
Guided Relaxation
While the skills associated with triggering the relaxation response (RR) are accessible to
almost everyone, guided and deliberate practice relaxing is usually needed for the individual to
learn to recognize and manage the indicators of psychological stress (Jacobson, 1925, 1934,
1970). Even a single exposure to the guided practice of relaxation has been demonstrated in early
studies to have ameliorative effects on mental and physical conditions (Benson, Beary et al.,
1974; Benson, 1977; Benson, Arns, & Hoffman, 1981; Benson, 1983).
In a systematic review of the literature exploring various relaxation techniques in the
treatment of pain from 1996 to 2005 (Kwekkeboom & Gretarsdottir, 2006), the randomized trials
of relaxation interventions were analyzed in an effort to draw conclusions as to the efficacy of
various relaxation interventions (e.g., progressive muscle relaxation, jaw relaxation, rhythmic
breathing, and other relaxation exercises). The authors concluded that most of the 15 studies that
were reviewed demonstrated weaknesses in methodology, limiting the ability to draw
conclusions as to the efficacy of the interventions. Among these weaknesses, the authors noted
that many of the studies failed to address individual differences among participants as to their
responsiveness to particular relaxation techniques. The present investigation addresses one such
19
weakness by examining how the method by which guided relaxation is delivered influences its
potential efficacy with stress.
Audio-guided relaxation. The research cited above demonstrates the relative efficacy of
live or in-person guided relaxation programs. Yet, it is not always feasible, practically or
financially, for individuals to employ the services of trained professionals in order to make use of
a relaxation program, particularly if one intends to gain the more enduring and lasting benefits
that come from a daily practice routine. As such, audio tapes may be used to guide individuals
into the RR in lieu of in-person instruction. When practicing with a tape rather than with a live
trainer, some disadvantages arise, such as the inability to tailor the program to the individual’s
own unique style or challenges. The benefit of having ready access to a tape that can be used at
any time may outweigh some of these potential drawbacks.
Most of the early research into the use of audio tapes for guided relaxation met with an
underwhelming response in the literature. In a systematic meta-analysis of the early research
exploring audiotaped relaxation, Paul and Trimble (1970) stated, “None of the available
literature provides evidence that recorded relaxation instructions . . . produce effects comparable
with those obtained by ‘live’ treatment procedures,” (pp. 299-300). When these early studies of
audiotaped relaxation programs were shown to be at all beneficial, it tended to be when the audio
programs were used in combination with live training (Zeisset, 1968). As such, Paul and Trimble
(1970) concluded that the lack of efficiency of audiotaped procedures was due to the “lack of
response contingent feedback in the recorded mode,” (p. 300). In other words, the responsiveness
of a live trainer to the individual differences of individual participants was lost in the
employment of recorded training.

20
Given the datedness of Paul and Trimble’s (1970) meta-analysis of the literature, it is the
position of the researcher that responsiveness to audiotaped instructions has possibly increased
since that time, as demonstrated by Smyth et al. (1999). In this research, the effects of the use of
an audiotaped guided relaxation on the symptoms associated with asthma (i.e., self-report and
expiratory flow), stress, and general well-being were examined with a group of middle-aged
asthmatics (n = 20). Their results showed that listening to the relaxation tape generated responses
in the direction of the hypothesis and achieved statistical significance in the measures of reported
asthma symptoms (p < 0.1) and expiratory flow (p < 0.05). [This p-value is reported in the
primary source article by Smyth et al. (1999). Because the social sciences report statistical
significance at p < 0.05 or lower, it is presumed that the authors’ reporting of significance with a
p < 0.1 does not broaden the definition of what constitutes a significant finding, but is more
likely the result of a misprint of “p < 0.01” in the original article. At the time of this writing, the
authors of the study did not respond to e-mailed requests for confirmation of this assumption.]
Listening to the relaxation tape did appear to decrease negative mood (p < 0.05) and stressor
reports (p < 0.01) in the treatment group, but the effects were unrelated to positive mood (p =
0.001). Although the researchers maintained some reservations regarding the small sample size
and the potential threats to internal validity posed by the Hawthorne, or placebo, effect or the
tendency for scores to regress towards the mean, these findings remain suggestive that guided
relaxation audio tapes can serve as a brief, low-risk, and relatively inexpensive form of
supplemental treatment for stress.
In another recent study published in 2007, Cropley et al. examined the effects of a 10-
minute guided relaxation tape on the desire to smoke and several symptoms associated with
tobacco withdrawal, such as tension, irritability, and restlessness, with a group of smokers of at

21
least 10 daily cigarettes for at least 3 years (n = 30). Participants were asked to rate the strength
of their desire to smoke and to rate the intensity of their withdrawal symptoms before a guided
relaxation, immediately following the relaxation tape, and at three 5-minute intervals following
the intervention. The research tentatively demonstrated that the desire to smoke decreased
immediately following the relaxation and for at least 5 minutes following the relaxation as
compared to the control group that did not receive guided relaxation (p = 0.05). Although the
authors recognized that the effects of the intervention were “modest and requires [sic]
replication” (p. 992), the effects that were measured were in the predicted direction of the present
hypothesis, namely that even a brief 10-minute guided relaxation audiotape can impact
participants’ scores on self-reported measures.
Video-guided relaxation. As mentioned in the previous chapter, psychological research
into the effects of visual media has been in the literature for as long as the medium has been in
existence. Since its inception, many studies have been published suggesting that visual media
(specifically, video) can influence behavior, either as the result of social modeling (Bandura,
Ross, & Ross, 1963) or as a result of how it influences the various neurological processes in the
brain (Kelly, Grinband, & Hirsch, 2007) or both.
The majority of studies that examine the effects of visual media, such as television,
movies, and videogames, on adolescents tend to focus primarily on how violent content tends to
lead to the exhibition of violent or aggressive behaviors (Anderson & Dill, 2000; Ferguson,
2007; Palys, 1986). While it is difficult to refute the direct effects of media on adolescents
revealed in these laboratory studies, the view that violent media invariably leads to violent
behaviors has been challenged by a small group of researchers who have posited a theory that the
effect of visual media is not necessarily as direct as is presumed by these studies. These

22
researchers posit the Media Practice Model that holds that the effect of visual media is more
dialectical and interactive with the viewer’s own unique experiences, motivations, and
expectations and may relate to the user’s sense of identity, the user’s reason for selecting the
media, the context or situation in which that media is viewed, and the viewer’s interpretation of
that media (Brown, 2006; Brown & Walsh-Childers, 2002; Levy & Windahl, 1985; Rubin, 2002;
Steele & Brown, 1995).
Given this theoretical basis, the effect that a particular piece of visual media has with an
adolescent may have more to do with the purpose or intention behind watching the video than is
usually presumed by the direct effects model. This interactive quality of the Media Practice
Model serves as a theoretical support for the therapeutic use of video herein proposed. Previous
exploration into the use of video with a therapeutic intention has demonstrated some promising
results. In one study in particular, a process of using video imagery called photic stimulation—
flashes of light from a video screen—was shown to induce relaxation in individuals who watched
it as the frequency of the flashes was progressively slowed over time (Landeck, 2004). Landeck
suggested that photic stimulation could be used as an alternative approach to inducing relaxation
in a clinical setting with reluctant or anxious clients.
Only a few studies were found in the literature to explore the potential therapeutic value
of video. Among them, the earliest known study was published nearly 20 years ago and
examined how videos of quiescent animals could be used to moderate the stress response in an
elderly population (DeSchriver & Riddick, 1990). DeSchriver and Riddick investigated whether
the stress-ameliorating effects of animal companionship (Allen, Blascovich, & Mendes, 2002;
Friedmann, Thomas, & Eddy, 2000) are comparable to watching videos of animals, which could
avert the potential allergies or phobias that could be triggered by the use of live animals in a

23
clinical setting. To this end, the researchers evaluated the muscle tension and cardiovascular
responses using pulse rate and skin temperature in a relatively small sample (n = 27) of elders
(with a mean age of 75 years) who were randomly assigned to two experimental conditions (e.g.,
viewing an aquarium or a video tape of an aquarium with the sound of water trickling over
rocks) and a control condition (a placebo video tape of television color bars and static). Members
of all three groups perceived their treatments as relaxing, and results appeared to move in the
expected direction, but the results did not achieve statistical significance overall. However,
qualitative evaluations elicited the overall sentiment from the participants that gazing at the fish
was an enjoyable and beneficial activity. Almost universally, participants stated that the videos
allowed them to feel “totally relaxed” and helped them to temporarily “forget about [their]
problems while watching” the videos (DeSchriver & Riddick, 1990, p. 47). Subjective reports
such as these, which are suggestive of results in the direction of the present study’s hypothesis,
raise the possibility that the lack of empirical support offered by this study is not a matter of the
videos being ineffectual, but rather the failure of the instrumentation utilized to measure the
effect.
In another more recent and compelling study of the therapeutic use of video, Wells
(2005) extended the findings of DeSchriver’s and Riddick’s work (1990) beyond videos of fish
to also include videos of other animals as well. In this study, Wells evaluated the heart rate and
blood pressure of a larger sample (n = 100) of younger university students (with a mean age of
19.71), who were randomly assigned to three experimental conditions (i.e., videos of fish, birds,
or primates) and two controls (videos of humans or a blank screen). She found that the videos
universally encouraged relaxation, with participants in all three experimental conditions
exhibiting significantly (p < 0.001) lower levels of heart rate and blood pressure than those
24
individuals exposed to the control videos. She concluded that “videotapes of certain animals can
reduce cardiovascular responses to psychological stress and may help to buffer viewers from
anxiety, at least in the short term” (in abstract). Overall, the results from Wells’ (2005) study
suggest that the presence of animals in video form can have a stress-ameliorating effect on
cardiovascular dynamics similar to that of live animals. However, this study investigated the
effects of the video only in the short-term, and thus, long-term implications cannot be drawn. It
is possible that participants may become habituated by repeated viewings of the video such that
its stress-reducing impact may be weakened.
It may be noted that Wells’ (2005) study is the first study of its kind to present
videotapes of animals without any type of auditory stimulation (p. 213). While certain types of
auditory cues (e.g., classical or new age music) have been demonstrated to reduce stress (Chafin,
Roy, Gerin, & Christenfeld, 2004; Krout, 2007; Pelletier, 2004; Smith & Joyce, 2004), the
results from Wells’ study show that visual stimulation by itself can buffer people against some of
the symptoms of stress. This finding gives support to the lack of auditory stimulation, in the
treatment conditions explored by the present study.
Audio- and video-guided relaxation. As noted in the previous chapter, only one study was
found to have been published in the last 2 decades exploring the comparative efficacy of audio
and video methods of facilitating relaxation (Byrnes, 1996). In this study, Byrnes measured the
ongoing levels of stress experienced by 33 adult subjects and 21 college students (n = 54) as they
were subjected to one of three experimental conditions. Subjects were randomly assigned to
either listen to a piece of classical music, view an underwater film of tropical sea life, or listen to
the same piece of classical music while viewing the same underwater film of tropical sea life.
Participants were also asked to complete a brief questionnaire pertaining to profession and

25
relaxation preferences, and they were asked to rate their current level of stress on a 7-point Likert
scale both before and after the intervention. Then, during the intervention itself, participants
utilized a device designed to assess their overall tension on a continuum in real time (known as
the Continuous Response Digital Interface or CRDI) by which participants turned a dial to
denote their current level of tension during the exposure to the intervention. The data gathered by
the CRDI was subjected to a post hoc t test analysis against the perceived stress levels as
reported by the pretreatment and posttreatment questionnaires.
Byrnes’ (1996) results demonstrated that there was a significant difference between the
pretreatment and posttreatment stress responses for the combined audio-video condition (p =
0.002), but not for the audio or video conditions separately (p = 0.154). Although the results for
all three conditions did not achieve statistical significance, Byrnes stated that participants in all
three conditions reported an overall decrease of tension and stress over the course of the
intervention and, upon completion, reported that they enjoyed their participation. Such positive
results offer promise to the employment of VGRP in the reduction of stress and facilitation of
relaxation, albeit they are inconclusive at this time. Byrnes’ treatment lasted approximately 2
minutes and 50 seconds, which is a relatively brief intervention that would not be expected to
generate as robust an effect as it seemed to based on the participants’ subjective experience of
stress. Moreover, one cannot discount the possible placebo effect of the use of the CRDI
instrumentation as well as of the video tape itself. However, Byrnes’ study suggests the
possibility of eliciting a similarly effective result from Media Assistance programs as was found
by the present study.

26
Chapter 3: Method
Research Design
At the end of Chapter 1, the basic research design of this study was briefly discussed. In
this chapter, I explore this subject more deeply. Given that live (in vivo) guided relaxation has
already been shown to help individuals manage stress (Cropley et al., 2007), as discussed
previously in Chapter 2, the primary aim of this study was to explore whether Media Assistance
might be a comparable adjunct to the clinical treatment of stress. The investigation of Media-
Assisted forms of treatment provided useful findings in terms of determining their potential role
in the range of clinical treatments.
In this research, I explored how three different methods of delivering guided relaxation—
video, audio, and live—influence various symptoms associated with stress. As is described in
more detail below, the video-guided relaxation program, or VGRP, is composed of nature
imagery that was used with permission from a commercially available DVD (see Appendix G).
The visual imagery is accompanied by a prerecorded audio track of the guided relaxation
transcript recited in a calm and soothing intonation (see Appendix E). The audio-guided
relaxation program, or AGRP, was composed of the same audio track used in the VGRP in the
absence of the visual nature imagery. The live, or in vivo, guided relaxation program, or LGRP,
was composed of the researcher reciting the guided relaxation transcript (see Appendix E) in a
calm and soothing intonation, in person with the participants. No music was employed with any
of these methods as this could potentially confound the primary focus of whether visual imagery
helps or hinders the stress-ameliorating efficacy of guided relaxation.

27
The purpose of this research was to answer the following questions:
1. “Is there a relationship between the method used to deliver guided relaxation to
adolescents and the amount of stress they report after receiving the treatment?” and
2. “What is the magnitude of the relationship between the method of delivering guided
relaxation and the amount and subtypes of stress levels that are reported?” Secondary research
questions were:
1. “Which demographic variables, if any, correlate with the influence of the guided
relaxation programs on reported levels of stress?” and
2. “To what extents do the participants’ reactions to the treatment conditions correlate
with reported levels of stress after exposure to treatment?”
In an effort to answer these questions, I utilized quantitative methods that had been
employed to view data objectively and to understand the relationship between variables in a
uniform fashion (Braud & Anderson, 1998). To establish and maintain a high quality of
standards, quantitative measures, such as questionnaires and surveys that have a high degree of
reliability and validity, were used. Quantitative methods are one of the most accepted forms of
data collection in the field of psychology today and are presumed to be the most congruent with
the scientific method (Creswell, 1994).
In this study, I employed a prepost experimental research design to serve an exploratory
function as to how three methods of delivering guided relaxation influence reports on a
psychological measure of stress. Specifically, I compared the effects that a Video-Guided
Relaxation Program (VGRP), an Audio-Guided Relaxation Program (AGRP), and a Live (in
vivo) Guided Relaxation Program (LGRP) had on the self-reported levels of stress among a
group of 77 Northern California high school students.
28
Upon acceptance into the study, all participants completed a pretreatment research packet
composed of a Demographic Questionnaire (Appendix B) and an assessment of frequently
reported stress symptoms, as measured by the Smith Stress Symptoms Inventory-State version
(SSSI-S, see Appendix C; Piiparinen & Smith, 2003, 2004) to establish demographics and the
baseline measures of participants’ present state of stress prior to the treatment. The third
instrument utilized in the present study, the Reactions to an Experiential Exercise Scale (REES,
see Appendix D), was employed after each treatment condition. A more detailed discussion of
these instruments is provided later in this chapter.
Upon completion of the pretreatment research packet, participants received the first of the
three treatment conditions (e.g., VGRP, AGRP, or LGRP), depending on the class to which they
were assigned. Each class received a different treatment condition for each of the 4 days of data
gathering. In other words, all seven classes received all three treatment conditions during the 4-
day period, albeit in a different order. This counterbalancing design was used to maintain the
distinction between the effects of order with that of the treatment itself. Participants completed
the two psychological assessments, the REES and the SSSI-S, after each exposure to a treatment
condition.
Participants
A convenience sample of 91 adolescents was recruited from a local high school in
Northern California to participate in the study in order to obtain sufficient statistical data that
could be made generalizable to the population at large and to account for the possibility of
attrition. Participation was solicited through contact with the school’s teachers with the
understanding that students’ participation throughout the study was entirely voluntary, although
teachers were encouraged to offer class participation credit for involvement in the study. All

29
participants and at least one of each participant’s parents were required to sign an informed
consent form (Appendix A) and were told about the nature of the study prior to filling out the
pretreatment questionnaires. Participants and at least one parent were informed that participation
in the study was entirely voluntary and that participants might choose at any time to discontinue
participation for any reason.
The required criteria for inclusion in the study were as follows: (a) willingness to
participate, (b) ability to speak and read English fluently as attested by their teacher, (c) signed
and parentally cosigned informed consent forms, and (d) full-time enrollment in mainstream,
rather than special-education, classes at a local high school. Students from special education
classes were excluded so as to ensure that all participants in this study had the appropriate level
of intelligence and the minimal fluency in English that was required to maintain the scientific
validity of the assessments.
Participants were selected from a diverse sampling across all grade levels from within a
“Focus on Success” class, the purpose of which was to offer students skills and techniques that
fostered good study habits. Although a diverse sample was difficult to achieve within a single
high school, diversity of participants was sought within the confines of the above-stated criteria.
Out of the 91 participants recruited, 77 returned the parentally cosigned informed consent forms
and were thus given the Demographic Questionnaire (Appendix B) and the Smith Stress
Symptoms Inventory-States version (Appendix C; Piiparinen & Smith, 2003, 2004) to establish
the baseline measures of stress.
After all of the data were collected, 21 of the 77 participants needed to be eliminated for
the reason that invalid data was suspected. These 21 participants’ responses to both the baseline
measures and to the three repeated measures of SSSI-S reflected the overall impression that none
30
of the items on the stress scale applied to them at all. (A thorough discussion of the rigorous
manner by which the participants’ “disengagement” from the study was conceptualized will be
provided later in this chapter.)
A preliminary correlational analysis between this disengaged segment of the sample and
the rest of the participants showed that this group of disengaged participants was more likely to
be male (r = .32, p < .004) and to report lower grades (e.g., Ds and Fs; r = -.23, p < .05) than the
group whose scores were included in the primary analysis. Although suggesting that males with
low grades would typically disengage from studies such as this one, this study did not have
enough individuals in the sample to allow this finding to serve a predictive function. The other
participants’ inclusion in the study was not related to any of the other demographic variables
including ethnicity, socioeconomic status, grade, primary language, or media preferences.
Although a moderate amount of selection bias—or a distortion of data arising from the
way in which the data is collected—is to be expected in any self-reported measure, this amount
of disengagement within the study was higher than expected. It is possible that doing research in
a classroom setting created a conflation between participation in the study with other in-class
assignments. Those students who disengaged from the study might have been disposed to tuning
out in-class assignments, in an effort to be “cool,” hostile, or otherwise resistant to in-class
authority. If so, their responses would not have accurately reflected the effects of the
interventions on how people perceived their emotional responses—which was the primary focus
of the study—and so therefore a decision was made to remove these participants’ scores from the
primary sample in order to maintain the validity of the study.
This scenario raises some interesting questions pertaining to the way in which
interventions such as the ones explored in this research might be brought into the classroom

31
setting and used with individuals who fit this particular demographic profile. The interventions
themselves might have, in fact, been quite effective with such participants, but their general
disengagement from participation in the study might have evoked what could be considered to be
due to the study’s methodology or due to a problem of instrumentation for this particular
subgroup of the population. A more thorough exploration of these methodological findings and
the limitations they imposed on the present research are discussed in more detail in Chapter 5.
The demographics for the remaining 56 participants are shown in Table 1. This sample of
participants was evenly split between the two genders, with an average age of 15 years (M =
15.2, SD = 1.1), primarily English-speaking, in 9th and 10th grade, and who reported getting
mostly Bs or Cs academically. They reported being mainly Caucasian or Latino/Hispanic,
followed by Bimultiracial, Asian, African American or another unlisted ethnicity. A majority of
the students reported that they did not know their socioeconomic status, but those that did know
predominantly reported a high SES (e.g., more than $100 thousand per year), with some lower-
income exceptions.
Instruments
In this study, participants completed three questionnaires. The first questionnaire was
designed to gather general demographic information from the participants and to gather specific
information pertinent to the present topic of inquiry (Appendix B). The second questionnaire, the
Smith Stress Symptoms Inventory-States version (SSSI-S, see Appendix C; Piiparinen & Smith,
2003, 2004) was designed to measure frequently reported stress symptoms, such as
Worry/Negative Emotions, Striated Muscle Tension, Attention Deficit, Autonomic
Arousal/Anxiety, Depression, and Interpersonal Conflict/Anger. The third questionnaire, the
Reactions to an Experiential Exercises Scale (REES, see Appendix D), was an instrument
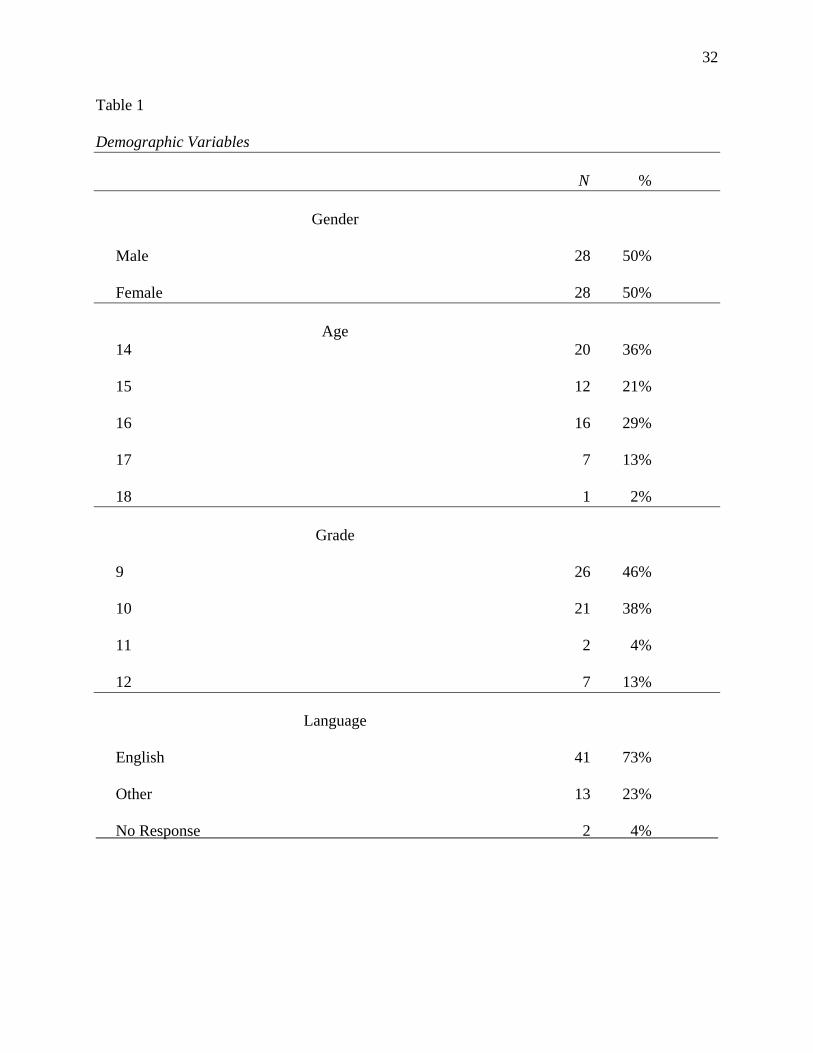
32
Table 1
Demographic Variables N %
Gender
Male 28 50%
Female 28 50%
Age 14 20 36%
15 12 21%
16 16 29%
17 7 13%
18 1 2%
Grade
9 26 46%
10 21 38%
11 2 4%
12 7 13%
Language
English 41 73%
Other 13 23%
No Response 2 4%

33
Table 1 (continued) N %
Ethnicity
Caucasian 23 41%
Latin / Hispanic 13 23%
Bimultiracial 7 13%
Asian 6 11%
African American 4 7%
Other 3 5%
No Response 1 2%
Grade Point Average
As 4 7%
Bs 34 61%
Cs 16 29%
Ds 1 2%
Fs 0 0%
No Response 1 2%

34
Table 1 (continued) N %
Socioeconomic Status
More Than $100 Thousand 10 18%
Between $75 & $100 Thousand 3 5%
Between $50 & $75 Thousand 7 13%
Between $25 & $50 Thousand 3 5%
Less Than $25 Thousand 2 4%
Don’t Know 30 54%
No Response 1 2%
designed especially for the purposes of this study and measured participants’ reactions (in terms
of their Enjoyment, Engagement, and Interest in Repeating the exercise) to each of the three
treatment conditions. All of these instruments will be discussed in greater detail below.
Demographic questionnaire. All participants completed a demographic questionnaire.
This questionnaire (see Appendix B) consisted of 10 multiple choice items that elicited
participants’ demographic information, such as their age, grade, sex, ethnicity, academic
performance, and socioeconomic status. Additional questionnaire items were included in an
attempt to explore participants’ media preferences in general, while relaxing, average time spent
daily using said media, and the extent of any prior experience with relaxation techniques that the
participants may have had. It was hoped that the data generated by these items would enable me
to explore whether a participant’s predilections toward and uses of media would influence the
participant’s compliance to the Media Assistance methods being studied as well as the
participant’s response to them. Although follow-up research would be needed to focus on this

35
relationship more directly, such exploratory data could help to provide the basis for such studies
examining how elements of the Media Practice Model (discussed in Chapter 1) might relate to
the potential efficacy of Media Assistance as an adjunctive form of clinical treatment. Items
about media preference were coded as binary variables for each type of media listed with type of
media reported = 1 and not reported = 0.
Reactions to an Experiential Exercise Scale (REES). The Reactions to an Experiential
Exercise Scale (REES; Appendix D) is an 18-item, 6-point Likert-type scale designed expressly
for the purposes of the present study. I developed it to measure the extent to which individuals
felt Engagement during, Enjoyment of, and an Interest in Repeating the given experiential
exercise. Respondents to this questionnaire were asked to indicate the extent to which a
statement fit with how the respondent felt “in reaction to the exercise” along a 6-point Likert
scale (with 1 indicating “Strongly Disagree” and 6 indicating “Strongly Agree”). The statements
used in the REES were used to assess three subscale reaction categories: engagement,
enjoyment, and interest in repeating the exercise. The REES is written at a junior high school
reading level, is easy to administer with groups or individuals, and takes about 5 to 7 minutes to
complete.
For the purposes of the present study, a 19th item was added to the REES to elicit the
extent to which participants elected to close their eyes during the exercise, as measured across a
6-point Likert-type scale, with 1 indicating “Strongly Disagree” and 6 indicating “Strongly
Agree.” The purpose of including this additional item was to evaluate the potential confound
imposed by the possibility of participants closing their eyes during the exercise. As some
research has shown (Craig et al., 2000; Putman, 2000), closed eyes increases alpha brainwaves,
which are 8-12 cycles per second, and which in turn increase relaxation, reduce stress, and

36
reduce the beta brainwaves, which are 13-25 cycles per second, and thus reducing wakefulness.
Moreover, this item may have helped to elicit data concerning the relative efficacy of the
imagery used in the VGRP on the reported levels of stress among participants in this condition
who reported that they kept their eyes open during the treatment. For this study, the measure of
whether participants closed their eyes during the treatment conditions was reverse-coded and
then recoded as a dichotomous variable with closed eyes reported as 1 and eyes opened to any
extent reported as 2.
For the final implementation of the REES after the third treatment condition was
completed, an open-ended question was added to elicit participants’ preference and experience
with each of the three conditions. Participants were asked to describe the treatment that they
liked the best and why, in as much detail as they wanted. This item was intended to elicit
subjective information about which aspects of the three conditions aided or hindered the
participants’ relaxation and overall reaction. It was hoped that this qualitative information would
help to deepen the interpretation offered by the quantitative data of the questionnaires and
possibly guide the direction of future studies.
To determine the reliability of the REES, the instrument was piloted in a total of seven
separate graduate-level psychology classes in Northern California in which students underwent
brief experiential exercises lasting approximately 10 minutes in duration (n = 75, M age = 29.3
years old, SD = 6.4 years) with 48 females, 15 males, and 13 participants with undisclosed age
and gender. The specific classes to pilot the REES participated in various creative expression
exercises that related to their personal goals for the academic semester. The Cronbach’s alpha
coefficient for internal reliability was calculated for the entirety of the REES at .92 (for
subscales, Enjoyment = .83, Engagement = .85, and Interest in Repeating = .86). For females,

37
alpha was .92 for the REES overall, with Enjoyment = .84, Engagement = .85, and Interest in
Repeating = .86. For males, alpha was .85 for the REES overall, with Enjoyment = .72,
Engagement = .83, and Interest in Repeating = .88.
For the present study, the Cronbach’s alpha coefficient for internal reliability for the
REES was calculated for each of the three treatment conditions. The participants of the present
study (n = 56) were all treated to the three treatment conditions in seven separate classes in
varying orders over the course of 4 consecutive days. Cronbach’s alpha for each of the three
subscales for each of the three treatment conditions ranged from .71 to .93, meeting the minimal
criterion of alpha = .50 (J. Cohen, 1987).
The overall reactions to each of the interventions tended to be correlated with one another
so that participants who enjoyed the live condition also tended to enjoy the audio and video
conditions, with similar findings revealed for their feeling of engagement with the interventions
and their interest in repeating the interventions. Cronbach’s alpha for Enjoyment for the
combined live, audio, and video conditions was .81, for Engagement was .71, and for Interest in
Repeating was .84. As a result, a decision was made to average ratings of Enjoyment,
Engagement, and Interest in Repeating across conditions, to give one score each for each
respondent in each of the three subscales.
Smith Stress Symptoms Inventory-State (SSSI-S). The Smith Stress Symptoms Inventory-
State version (SSSI-S) is a 34-item 4-point Likert-type scale measuring the degree to which
individuals currently feel a range of frequently reported stress symptoms (see Appendix C;
Piiparinen & Smith, 2003, 2004). Respondents to this questionnaire were asked to indicate the
extent to which a statement described how they felt “right now” along a 4-point Likert scale,
with a 1 indicating “Doesn’t fit me at all” and a 4 indicating “Fits me very well.” The SSSI-S

38
was based on the Smith Stress Symptoms Scale (1990) and the Stress Costs Inventory (Smith,
1993) and was designed to reflect content areas typically measured by cognitive anxiety
inventories. It measures five symptom categories identified through a thorough factor analysis of
stress (Smith, Rausch, & Kettmann, 2004): (a) Worry/Negative Emotion, (b) Attention Deficit,
(c) Striated Muscle Tension, (d) Autonomic Arousal/Anxiety, and (e) Interpersonal
Conflict/Anger. Each of these symptom categories is well established in the stress literature as
reflecting part of naturally-occurring stress responses. The SSSI-S is not a measure of
psychopathology inasmuch as its items and categories were obtained from and tested on
nondiagnosed college students and no clinical samples were used in its development. As a result,
the symptoms assessed by the SSSI-S are to be considered normal mood states, or naturally-
occurring stress symptoms, and not comprehensive enough to suggest a psychopathological
diagnosis. The SSSI-S is written at a junior high school reading level and is easy to administer
with individuals or groups in about 5 to 7 minutes.
Each subscale of the SSSI-S is made up of a sample of questionnaire items, the scores of
which are averaged together to calculate the reported level for that particular symptom’s
subscale. For example, the Striated Muscle Tension subscale is made up of item number 17 (“My
shoulders, neck, or back are tense.”), item number 20 (“My muscles feel tight, tense, or clenched
up.”), item number 23 (“I have backaches”), and item number 32 (“I have headaches.”). Taken
together, these items can offer a good picture of the participant’s current level of muscle tension;
however, this score may be distorted by the incidence of a passing headache or temporary injury.
Similarly, the other symptom subscales are based on items that may be prone to transient
changes. So, overall, the SSSI-S should not be used to serve a diagnostic function. Rather, the

39
scale offers an assessment of the participant’s moment-to-moment incidence of naturally-
occurring stress symptoms to serve as an area requiring further evaluation.
Although Smith created the SSSI-S with a subscale for Depression, I decided to remove
this subscale from the analyses for this study because the two items associated with this subscale
(item number 11, “I feel distressed,” and item number 13, “I am depressed”) were both included
among the items comprising the Worry/Negative Emotion subscale making it somewhat
redundant. Additionally, the Depression items subscale might have been somewhat
underreported by adolescents who might report depressive mood states in a more active language
such as those associated with the Interpersonal Conflict/Anger subscale (e.g., item number 16, “I
feel cynical or hostile,” and item number 35, “I feel irritated or angry,”), as opposed to the
passive language associated with the Depression subscale.
In terms of psychometrics, the SSSI-S has a Cronbach’s alpha coefficient ranging from
0.86 to 0.79 (Smith, 1990, p. 199), suggesting that it has high internal reliability. However, no
studies have yet been performed to evaluate its concurrent validity—that is, its validity as
compared with other similar scales of stress or anxiety. Nevertheless, the results of many studies
have demonstrated that the SSSI-S has substantial construct validity. An instrument’s construct
validity refers to the extent to which it measures all of the unobservable facets of the social
construct that it purports to measure. In the case of the SSSI-S, the scale’s construct validity is
evaluated by its measurement of the six stress symptom categories noted above as a function of
recognized patterns of response to a stressful situation.
An example of the SSSI-S’s construct validity is evident in two complementary studies
performed by Piiparinen and Smith (2003, 2004) who investigated the influence of the terrorist
attacks in New York City on September 11, 2001 (9/11). Archival data of the SSSI-S

40
administered to a sample of Chicago-area college students 5 months prior to 9/11 (n = 320, M
age = 25.7, SD = 8.6) was compared with data gathered 1 to 5 weeks after 9/11 with a similar,
albeit a separate, group of Chicago-area college students (n = 149, M age = 22.0, SD = 6.1). The
two groups did not differ by gender distribution, but the pre-9/11 group was slightly older.
Analyses of variance showed that men and women displayed the same pattern of stress
symptoms.
Multiple analyses of variance, with age included as a covariate, indicated that the post-
9/11 respondents scored higher than pre-9/11 respondents on the attention deficit scale (F[1, 467]
= 7.6, p = 0.006), indicating that college students displayed higher scores on stress-related
attention deficit after the attacks of 9/11 than a comparable group of college students did before
the attacks. The attention deficit scale, as implemented by the SSSI-S, measures cognitive
responses to stress, including memory loss, loss of concentration, feeling disorganized, feeling
confused, and becoming easily distracted. Interestingly, no other significant differences were
found between the two groups in any of the other six categories of stress symptoms. Moderately
strong correlations between attention deficit, autonomic arousal/anxiety (r = .66, p < .0005),
worry (r = .69, p < .0005), and anger (r = .60, p < .0005) and moderate correlations with muscle
tension (r = .45, p < .0005) and depression (r = .57, p < .0005) were found, supporting the
suggestion that the attention deficit measured was related to stress.
In other words, the pattern of these college students’ stress-related attention deficit
resembled the kind of dissociative symptoms and denial that are associated with the initial phases
of posttraumatic stress disorder (Piiparinen & Smith, 2003). As Lazarus and Folkman (1984)
suggested, dissociation and denial serve as ways of distancing oneself from the disruptive and
negative feelings following a traumatic event in response to which nothing concrete can be

41
accomplished. As Piiparinen and Smith (2003) pointed out, this pattern of distancing oneself
from negative affect is consistent with the findings shown in studies of posttraumatic stress
reactions of persons living in terrorized communities. The comparability of these findings
demonstrates the SSSI-S’s adequate construct validity as a stress scale and presents the SSSI-S
as an effective measure of the social construct of stress, including its cognitive, physical, and
emotional ancillaries as delineated by the instrument’s six categorical subscales.
This scale was selected because it is the only available nonpathological self-report
measure that elicits the participant’s moment-to-moment transient state symptoms of stress
across a variant of cognitive, physical, and emotional subscales. Short of using
psychophysiological measures, such as electroencephalograms, electrocardiograms, or galvanic
skin response measures (which can be difficult to employ for the purposes of a brief intervention
in a classroom setting), a state-based self-report questionnaire served as the best and most
feasible method for eliciting individuals’ moment-to-moment awareness of their present states of
mind. Further, all of the other self-report measures of stress I found were either assessments for
clinical pathology, such as the State-Trait Anxiety Inventory, or served as measures of the static
disposition or trait of stress rather than the momentary state of stress, such as the Perceived
Stress Scale. These measures were deemed inappropriate because the intention of the study was
to examine the immediate impact of a brief intervention on participants’ transient stress states in
a nonclinical setting. Although the SSSI-S assesses state of mind, which is, by definition,
transient and subject to low test-retest reliabilities, the SSSI-S serves as a one-of-a-kind self-
report measure inasmuch as it enables the individual to evaluate the individual’s own present
experience of stress in the present moment. This moment-to-moment awareness is critical for the
development of meditative attention (Smith, 2005). As such, a measure like the SSSI-S requires

42
respondents to attend to their current state of mind, thereby enhancing the meditative attention
that is indicative of the present study’s approach to relaxation (Smith, 2001).
For the present study, the Cronbach’s alpha coefficient for internal reliability for the
SSSI-S was calculated for each of the three treatment conditions. The participants of the present
study were all treated to the three treatment conditions in seven separate classes in varying orders
over the course of 4 consecutive days. Cronbach’s alpha for each of the six subscales for the
baseline scores and each of the three treatment conditions range from .56 to .92, meeting the
minimum criterion of .50.
Procedure
Teachers in a Northern California high school were contacted through a mutual associate,
and permission to conduct research in their seven “Focus on Success” study-habits classes was
requested. A written description of the study was provided to introduce the study in greater
depth. Upon receipt of permission to conduct research at the high school, I visited each of the
classes designated for prospective participation in order to introduce myself and the study to the
students and the teachers, to answer any questions that the students or teachers might have had,
as well as to provide information pertinent to the topic of the study and informed consent forms
to all interested persons. The study was introduced by informing potential participants that
research had determined that most people find relaxation exercises to be beneficial and
enjoyable. Although it is understood that such information may have biased participants’
responses and generated placebo effects, such information was given to all participants so that
any placebo effects were distributed uniformly across all treatment conditions and made
irrelevant to the focus of the present study, specifically, the comparative efficacy of the three
treatments, not whether the treatments themselves were effective at reducing reported levels of

43
stress (see Appendix H for a transcript of what was disclosed to participants just prior to each
treatment). Providing such information is considered to be part of the participants’ informed
consent and part of what is likely to occur when introducing similar relaxation exercises in actual
clinical practice. A brief explanation of stress, its causes, and its effects was offered, followed by
a brief description of relaxation, its causes, its effects, and the benefits of reducing stress. Lastly,
a general description of what was entailed in participation in the study was given.
All interested participants were asked to take an informed consent form, sign it, have it
signed by at least one parent, and then return it to a designated collection folder at the school
maintained by a teacher. Prior to distributing the informed consent forms, the forms were
verbally explained to the students in the classes with regard to the nature of the study and what
was required of them if they chose to participate. Additional copies of the informed consent
forms were provided to the teachers to distribute to prospective participants upon request. The
students had 4 weeks to contact the researcher with any questions and to return the signed and
cosigned informed consent forms. The teachers’ assistance was enlisted to remind the students of
the deadline and to distribute additional copies of the informed consent forms should they be
needed.
Once enough qualified participants submitted their informed consent forms, each
student’s name was written on a master list with a three-digit numeric code corresponding to the
random number assigned to each of the pretreatment research packets that were distributed to the
participants at the commencement of the study. This numeric code became the participant’s
identification number throughout the course of the study.
The instructions for both of the pretreatment questionnaires were explained to the
participants by the researcher with the reminder that all of the information provided by them

44
would be kept strictly confidential. The students were asked to answer all of the questions as
honestly and accurately as they could. The students had a total of 10 minutes to complete the
pretreatment research packet. The first questionnaire is the demographic questionnaire that
assesses basic information about the participant such as age, gender, academic performance,
socioeconomic status, preferred methods of relaxation, and electronic media preferences (see
Appendix B). The second questionnaire is the Smith Stress Symptoms Inventory-State version
(SSSI-S; Piiparinen & Smith, 2003, 2004), a 34-item 4-point Likert-type questionnaire designed
to measure the degree to which individuals feel that statements pertaining to stress symptoms fit
how they are feeling right now. The students were instructed to return the completed research
packets to the researcher upon completion. These were then placed in a locked file box and
stored in a secure location to which the researcher had sole access in order to maintain
participants’ confidentiality.
Each of the seven classes received each of the three treatment conditions—LGRP,
AGRP, or VGRP—once per day over the course of four days. The order in which the classes
received the treatments followed a counterbalancing method, also known as the Latin Squares
method, which helped to minimize the threats posed by the order of the treatment methods or
other outside influences that might have impacted the results of the study (e.g., natural disasters
or the death of a classmate), while increasing the statistical significance achieved by a within
groups analysis of the data. (For an illustration of the order in which the seven classes received
the three treatment methods over the course of the 4 days of the study, see Table 2.)
It would have been more convenient for the statistical rigor of the study if all seven
classes had rotated through the schedule uniformly, so that their respective treatment conditions
would not be influenced by the relative time of day over the course of the study; however, not all

45
Table 2
Guided Relaxation Treatment Schedule for All Seven Classes Period Day 1 Day 2 Day 3 Day 4
1 Class 5: Audio Class 4: Video Class 3: Live Class 2: Audio
2 Class 1: Video Class 5: Live Class 4: Audio Class 3: Video
3 Class 2: Live Class 1: Audio Class 5: Video Class 4: Audio
4 Class 3: Audio Class 2: Video Class 1: Live No Treatment
5 Class 6: Audio Class 7: Live Class 7: Audio Class 7: Audio
6 No Treatment Class 6: Video No Treatment Class 6: Audio of the classes rotated through the schedule. As Table 2 shows, periods 5 and 6 (i.e., the afternoon
periods) were split between Class 6 and Class 7. Such realities of the school’s class schedule
made the implementation of a uniform treatment schedule challenging within the school setting.
Preliminary statistical analyses comparing the morning classes and the afternoon classes
showed some significant differences between the two groups, which will be discussed in greater
detail in the following chapter. These differences may be accounted for by the fact that by the
afternoon students may have experienced increased stress as a function of classroom activities or
peer interactions throughout the day. However, these differences might also be accounted for by
reasons other than the time-of-day, including the relatively smaller sizes of the afternoon classes
(n = 11) as compared to the morning classes (n = 45), or bias as a function of class assignment.
A thorough discussion of the details for each of the three treatment conditions is
described in detail below. Upon completion of each treatment, participants were asked to
complete a posttreatment questionnaire, consisting of the SSSI-S and a version of the REES
which includes an open-ended question (see item 20 in Appendix D) to elicit the participants’

46
overall experience of the three treatment conditions. Participants’ written responses to this open-
ended question were treated with the same level of confidentiality as all of the data gathered over
the course of the study. This qualitative data did not receive the in-depth thematic analysis that
might have been warranted for the reason that such an in-depth analysis fell outside the scope of
the present study. Rather, these data were compared with the participants’ demographic
information to see if any demographic correlates emerged in comparison to the participants’
reception of the three methods of treatment. These data were also used to evaluate the possible
direction of future studies based on the participants’ open-ended feedback about their own
unique experiences of the three methods of guided relaxation. Although the need for a reader or a
transcriber for these open-ended answers was not planned, in the event that the need for a reader
or a transcriber arose as a necessity, the confidentiality of participant information was ensured by
the use of a Reader/Transcriber Confidentiality Agreement (see Appendix I).
Upon receipt of the participants’ completed final questionnaires, all participants received
a complimentary copy of a Relaxation Techniques Handout (see Appendix J) detailing various
ways of maintaining a relaxation practice throughout the day. All of the completed
questionnaires were hand-scored by the researcher according to the directions designated by the
assessment manual.
Treatment conditions. The treatment condition of most critical importance to the present
study was the VGRP. The other treatment conditions, AGRP and LGRP, served as comparisons
to evaluate the extent to which the video-delivered guided relaxation influenced the measures
being evaluated, as opposed to the audio or the live guided relaxation. To reiterate for the sake of
clarity, following their completion of the pretreatment assessment, each of the seven classes
received each of the three treatment conditions, once per day over the course of four days.
47
All three treatment conditions began with a memorized pretreatment talk (see Appendix
H), which was recited with a natural intonation to all seven classes. The purpose of this
pretreatment talk was threefold. First, it was intended to account for the placebo effect across all
three conditions, because expectancy effects are intended for most clinical uses of relaxation
programs. Second, it informed participants of their option to close their eyes during the treatment
or to keep them open in a soft, eyes-opened, unfocused gaze, so as to reduce the threat posed by
the likelihood of participants closing their eyes in the AGRP and LGRP, but not the VGRP,
respectively. Lastly, it was to remind participants that they ought to keep their personal thoughts
and feelings about the treatment they receive to themselves until after the study had been
completed on the 4th day. The purpose of this last procedure was to minimize the threats to the
study’s validity posed by participants comparing their reactions with others, thereby biasing or
influencing either their own or other participants’ reactions to the respective treatments.
For the VGRP, the video imagery was made up of a compilation of various scenes from
nature (i.e., ocean waves, trees, breaches, clouds, and a sunset) with each shot lasting roughly 10
seconds; there were brief dissolve edits between the scenes. This imagery is part of a DVD
entitled Mind Body Spirit: Simply Relax (2006) and was used for the purpose of this study with
the express permission from the producer (see Appendix G). The audio component of the DVD
was muted and replaced by a recording of the researcher’s voice, guiding participants through
the relaxation program. This procedure was to minimize the number of variables that might
influence the relative efficacy of each of the three conditions. The researcher recorded a guided
relaxation instruction in a calm intonation (see Appendix E). The guided relaxation lasted the
entire 10-minute duration of the treatment.

48
Detailed instructions for presenting the three treatments are available in Appendix F. All
three presentations followed a similar format. In the case of the VGRP, the video was played on
an available DVD player that was connected to an overhead projector onto a 36-inch screen at
the front of the classroom. The video was played inside the classroom provided by the school.
Participants were asked to clear their desks and to find a comfortable position in their seats such
that they had an unobstructed view of the screen. They were instructed to follow along with the
instructions offered by the guided relaxation program and to pay very close attention to how the
program made them feel. They had the option of closing their eyes if they so chose.
For the AGRP, the audio CD was identical to the audio content used for the VGRP. This
CD was played on an available stereo sound system at a reasonable volume so all participants
could comfortably hear the program clearly and easily. Participants were asked to find a place, to
clear their desks, and to find a comfortable position in their seats such that they were able to
follow along with the instructions provided by the guided relaxation program and to pay very
close attention to how the program made them feel. They had the option of closing their eyes if
they so chose.
For the LGRP, the intervention consisted of the researcher reading aloud the guided
relaxation instructions that had been used in both the VGRP and the AGRP in a calm and
soothing intonation similar to the way it was recorded for the VGRP and the LGRP (see
Appendix E for the transcript). Again, participants in this group were asked to clear their desks
and to find a comfortable position in their seats such that they were able to follow along with the
instructions given in the guided relaxation program and to pay very close attention to how it
made them feel. They had the option of closing their eyes if they so chose.

49
Chapter 4: Results
Treatment of Data
The Informed Consent Forms and the master lists containing the participants’ names and
their respective numeric codes were kept together in a locked file box that was placed in a locked
office to which the researcher had sole access. The completed pretreatment and posttreatment
research packets were also kept in a locked file box that was kept in a secure office space to
which, in maintenance of the participants’ confidentiality, the researcher had sole access. These
steps were taken in order to secure and maintain the participants’ anonymity and confidentiality
to the greatest extent possible and to ensure that the participants’ personal information was used
strictly for the purposes of the present research.
As stated above, in the course of reviewing the gathered data, evidence for invalid data
was suggested in that some of the participants did not seem to respond thoughtfully to the
questionnaires. This was achieved by tabulating all of the participants’ reports on the SSSI-S
over the course of the entire study, including baseline measures and all three conditions. These
scores were summed, showing that some participants had scores that were consistently low,
indicating that the given measures did not, in the verbiage of the scale, “fit [them] at all.”
Because any scientific instrument requires participants’ engagement with it in order for its
measurements to have value, it was necessary to exclude individuals who reported that none of
the items of the scale fit their present experience at baseline or after any of the three treatment
conditions. As such, a minimum cutoff score was used to remove those individuals with very
little or no variability in their scores. Subscale scores were averaged and then summed, with a
score of 7 or below used to remove students from the sample.

50
Data analysis. The data for the remaining 56 participants were scored through the
Statistical Package for the Social Sciences (SPSS) program, and a professional statistician was
consulted to assist the researcher in the scoring and analysis. All statistical analyses for this study
were performed using the SPSS default confidence level of 95%. Initially, descriptive statistics
were run in order to establish the means and standard deviations for the SSSI-S and the REES.
Preliminary analysis of the data using repeated measures analyses of variance for the stress
subscales (not including the baseline scores), and a p value set at .05 revealed no significant
differences between any of the five stress subscales or any of the three reactions subscales.
Further preliminary analyses of this type showed no significant decreases in the scores from the
first administration of the guided relaxation to the second or third. This finding showed that there
were no significant order effects that needed to be taken into account when analyzing the effects
of the three treatment conditions. Final preliminary repeated measures ANOVAs revealed that
there were no significant effects of any of the demographic variables or reports of prior
experience with relaxation techniques on reported levels of stress as they changed over the
course of the three treatments. This finding showed that neither the participants’ prior experience
with relaxation techniques, nor their unique demographic status significantly influenced the
efficacy of any of the three treatment conditions’ amelioration of stress.
Frequencies were run for participants’ reports of their preferred media for relaxation and
preferred media in general, daily exposure to media, and their prior experience with relaxation
techniques. Baseline measures of stress were also entered into a multivariate analysis of variance
(MANOVA) to obtain the means and standard deviations for these variables and were correlated
with each other using Pearson’s two-tailed correlations. Frequencies were also run for

51
participants’ reported levels of Engagement in, Enjoyment of, and Interest in Repeating the
intervention; correlations of these variables with each other were run as well.
Next, analyses were run to examine whether there was a relationship between the method
used to deliver the guided relaxation to adolescents and the amount of stress that they reported
after receiving the treatment. Repeated measures analyses of variance (ANOVAs) or covariance
(ANCOVAs) were run to examine changes that occurred in each dependent variable measuring
stress after the guided relaxation was delivered in the three treatment conditions. With p value set
at .05 and 95% confidence, if a relationship was found between the treatment condition and
reduced stress, then a post hoc test was employed to answer the follow-up question: For each
treatment condition, what is the magnitude of the effect size for the impact of the treatments? For
the present study, a small effect size was considered to fall between 0.1 and 0.3, a medium effect
size between 0.4 and 0.7, and a large effect size between 0.8 and 1.0 (J. Cohen, 1987).
Possible covariates (such as demographic variables, the time of day the treatment was
administered, whether participants had their eyes open or closed, and the level of Engagement,
Enjoyment, and Interest in Repeating the exercise that the participants reported) were also tested
in repeated measures ANCOVAs with p values of .05 to answer the secondary research
questions: “Which additional variables, if any, correlate with the influence of the guided
relaxation programs on reported levels of stress?” and “To what extents do participants’
reactions to the treatment conditions correlate with the reported levels of stress after exposure to
the treatment?” If no additional variables were significantly associated with treatment effects,
only repeated measures ANOVAs were run and the data for those insignificant variables were
not reported.

52
For the qualitative responses, an informal procedure was followed by which participants’
responses were coded into themes, and these results were tallied in an effort to offer a
preliminary report of the overall reactions expressed by the participants in their own words. This
treatment of the qualitative responses is not to be confused with rigorous qualitative analysis,
which subjects the data to a protocol of thematic analysis, a procedure that fell outside the scope
of the present research. Rather, these qualitative findings, as stated in the previous chapter,
served more as guides for the directions of future research than as primary results of the present
study.
Analysis of subjective reports. For the participants’ subjective responses to the open-
ended question at the end of the final implementation of the REES, an informal procedure was
followed to code the participants’ subjective responses to the open-ended question at the end of
the third use of the REES into a series of common themes. These results are intended to serve as
a cumulative summary of the participants’ overall reactions to the exercises as expressed in their
own words. This summary does not constitute the rigors and scope of a formalized qualitative
thematic analysis, however, and should be considered to be preliminary findings in need of
further study. These subjective reports may serve as guides for future research aimed at building
upon or deepening the findings reported by the present study.
Participants’ subjective responses to the open-ended question at the end of the last use of
the REES were transcribed and then coded into common themes to provide a sense of the most
common reactions or responses that participants offered in their own words. These themes were
then tallied in order to determine a range of responses from the least common to the most
common. Because all of the feedback and responses offered by the participants was potentially
useful for the ongoing development and improvement of these exercises, those provided by the

53
participants who had disengaged from the quantitative portion of the assessment and were
thereby dropped from the statistical analyses were included for this qualitative portion of the
study.
Results of the Analyses
In this section, I will report the results of the analyses described in the previous section.
However, before reporting these results, I would like to briefly discuss the statistical notations
that are associated with the ANOVA and are used in this section. The notation M refers to the
mean, or average, scores that were reported by participants of the given sample. For example, the
average stress scores for the Attention Deficit subscale that were calculated for all of the study’s
participants at baseline came out to be 2.24, or M = 2.24. This is to say that, on average, the
participants reported that the items associated with the Attention Deficit subscale “Fits me a
little” on the SSSI-S. These scores have a standard deviation, or SD, of .71, which is to say that
most of the participants’ scores (68% for a normal distribution) were spread within a range of .71
(or from 1.53 to 2.95) from the mean Attention Deficit score at baseline.
In order to approximate the size of the sample or group involved in a particular
experiment, one is subtracted from the number of participants in order to determine the degrees
of freedom, or df, for the particular experimental analysis. In the example above, the total
degrees of freedom for the analyses are 54 (or the number of participants involved in the
analysis, 55, minus 1). This statistic is presented as two separate values which indicate both the
between-groups estimate (which, in this case is 6, or 7 groups minus 1), and the within-groups
estimate (which in this case is 48, or the total number of participants, 55, minus the total number
of groups, 7).

54
Because the scores of this particular test are prone to variance, or distribution around the
mean, a statistical ratio has been devised to determine the overall variability of the scores divided
by the variability that may be due to random error of the scores. This is done by dividing the
mean sums of squares due to between-group differences by the mean sums of squares due to
within-group differences. The resulting value is known as the F statistic, or F ratio, which in the
example provided above can be presented as follows: F(6, 48) = 8.65, p < .0001. This final
notation, p < .0001, indicates that the probability is less than .01% on any one test of the null
hypothesis that the average scores of each group’s Attention Deficit scores was due to random
chance rather than as a result of the intervention. Because the p-value for this experiment was set
at .05, the conclusion is that the research hypothesis (that guided relaxation facilitates the
amelioration of stress) is more likely than the null hypothesis that guided relaxation does not
facilitate the amelioration of stress.
Reports of the participants’ media preferences in general and for relaxation, along with
duration of daily exposure to electronic media, are presented in Table 3. A majority of the
participants selected music as their primary medium for relaxing, followed by videogames and
the internet, then movies, television, and other media. A relatively large portion of respondents
reported using the internet daily, but not as a means of relaxing. Participants reported that music
was the second most preferred medium in general. Many of the participants reported spending
between 3 and 5 hours daily with some form of electronic media, followed by many that reported
using media less than 3 hours a day, and a few that reported using it more than 5 hours per day.
All participants reported spending some time with electronic media on a daily basis. Also
included in this table are the participants’ reports of any previous experience they may have had
with various types of relaxation techniques, such as progressive muscle relaxation, breathing

55
Table 3
Reported Media Preferences and Prior Experience With Relaxation Techniques
For relaxation1 In general1
N % N %
Media preference
Music 33 59% 23 41%
Videogames 12 21% 9 16%
Internet 11 20% 24 43%
Movies 10 18% 6 11%
Television 9 16% 11 20%
Other 9 16% 2 4%
Daily exposure to electronic media
None at all 0 0%
Less than 3 hours 19 34%
Between 3 and 5 hours 24 43%
More than 5 hours 13 23%
Prior experience with relaxation techniques
None at all 31 55%
Less Than 3 months 12 21%
Between 3 and 5 months 7 13% More than 5 months 6 11%
1Respondents could select more than one choice, so percentages exceed 100%.

56
techniques, or meditation. Most of the respondents reported having no prior experience with
relaxation techniques, although some reported having a moderate-to-extensive amount of prior
experience. As reported at the end of the previous chapter, covariate analysis of the participants’
prior experience revealed no significant difference as it pertains to the efficacy of the three
interventions at decreasing the levels of reported stress.
The means and standard deviations from a multivariate analysis of variance (MANOVA),
in which the baseline measures of stress of each of the five subscales (Worry/Negative Emotion,
Attention Deficit, Striated Muscle Tension, Autonomic Arousal/Anxiety, and Interpersonal
Conflict/Anger) were entered as a dependent variable, is presented in Table 4. The table shows
that the means for these items differed significantly from each other, with students reporting that
their present experience was more likely to involve Attention Deficit and Muscle Tension and
less likely to involve Negative Emotions, such as Worry, Anxiety, Depression, and Anger. All
subscale variables correlated with one another from .29 to .77 at p < .05, except for the Attention
Deficit subscale, which did not correlate significantly with the other subscales at all. Additional
correlations showed that media preferences did not correlate significantly with baseline stress
scores with one exception: Participants who reported using movies as their preferred relaxation
medium tended to have high Attention Deficit scores at baseline (r = .36, p < .01).
With respect to the participants’ reactions to the interventions, students tended to report
that they slightly enjoyed the intervention (M = 4.16, SD = .94) and were slightly interested in
repeating it (M = 3.88, SD = .97). They tended to give neutral reports of feeling engaged with the
intervention (M = 3.39, SD = .79). Reports of Engagement, Enjoyment, and Interest in Repeating
the exercise correlated with each other between .78 to .84, p < .0001.

57
Table 4
Descriptive Statistics for Baseline Subscales of Smith Stress Symptoms Inventory-State Subscale M SD df F Attention Deficit 2.24 .71 6, 48 8.65*
Striated Muscle Tension 2.03 .73
Worry/Negative Emotion 1.84 .63
Autonomic Arousal/Anxiety 1.78 .51
Interpersonal Conflict/Anger 1.62 .56 Note. N = 55. *p < .0001. Items coded from 1, “Does not fit me at all,” to 4, “Fits me very well.”
Although participants seemed to show somewhat neutral responses to the treatment,
findings showed that all of the participants did seem to experience some reduced stress as a result
of the treatments. None of the stress scores increased as a result of the treatments. Table 5 shows
the means and standard deviations for the Interpersonal Conflict/Anger and Worry/Negative
Emotion subscales from baseline and across the three treatment conditions. For both subscales,
there was a significant decrease in negative affect after all of the treatment conditions as
compared to the baseline condition. Because the class schedule did not allow for the different
classes to rotate between the morning and the afternoon periods (see Table 2), I measured the
impact that the time of day had on the decreased stress levels reported by the participants. Out of
all five stress symptoms assessed by the SSSI-S, only the Worry/Negative Emotion subscale was
found to be significantly impacted by the time of day, so this covariate was included in the
presentation in Table 5. There was also a significant interaction of condition x time of day.
Participants who underwent the interventions in the afternoon were found to have a higher
Worry/Negative Emotion score at baseline as compared to those who received the interventions

58
in the morning; however, this difference between morning and afternoon baseline scores was
found to be too small to be considered statistically significant (p < .07). For the afternoon group,
the magnitude of the effect for the treatment was greater [η2 = .48] than for the morning group
[η2 = .22]. This finding showed that students tended to be slightly more keyed up in the
afternoon classes; however, because the classes did not rotate between morning and afternoon
periods, the extent to which this difference was a function of the students who made up these
classes as opposed to the time in which they undertook the exercise is unclear.
To reiterate for the sake of clarity, as stated in the instruments section in the previous
chapter, the stress symptoms assessed by the SSSI-S are based on nonclinical, nonpathological
questionnaire items. Therefore, the appearance of certain stress symptoms for a participant’s
score does not fulfill a diagnostic criterion but, rather, a signpost that indicates areas of the
participant’s naturally-occurring stress-states that were affected by the given treatment
conditions. In this case, a significant score suggests that these mood states were significantly
influenced by the treatment conditions rather than being the result of random chance.
Table 6 shows the means and standard deviations for the Autonomic Arousal/Anxiety,
Striated Muscle Tension, and Attention Deficit subscales from baseline and across the three
treatment conditions. For all three measures, there was a significant decrease in negative affect
after all of the treatment conditions as compared to the baseline condition. For these three
subscales, whether or not participants reported having their eyes open or closed was related to
the magnitude of the change in reported stress. Because most participants reported closing their
eyes to some extent at some point during at least one of the relaxation conditions, I measured the
impact that eye closure had on the decreased stress levels reported by the participants. Out of all

59
Table 5
Descriptive Statistics for the Conflict/Anger and Worry/Negative Emotion Subscales of the Smith Stress Symptoms Inventory-State for All Treatment Conditions and Baseline Scores With Time of Day as a Covariate
M (SD)
Subscale Baseline Live Audio Video Source df F η2
Conflict/Anger 1.62a (.56) 1.22b (.29) 1.26b (.31) 1.36b (.56) Condition 3 17.68* .24
Worry/Neg. Emotion 1.84a (.63) 1.36b (.42) 1.41b (.45) 1.42b (.58) Condition 3 22.27* .29
Morning 1.77a (.61) 1.36b (.42) 1.42b (.47) 1.45b (.61) Time of Day (TOD) 1 .06 .00
Afternoon 2.13a (.64) 1.33b (.42) 1.37b (.32) 1.30b (.45) Condition x TOD 3 3.31* .06
___________________________________________________________________________________________________________
Note. N (for analyses) = 56. Means marked a are significantly higher (p < .05) than means marked b. *p < .05.

60
Table 6
Descriptive Statistics for the Muscle Tension, Attention Deficit, and Autonomic Arousal Subscales of the Smith Stress Symptoms Inventory-State for All Treatment Conditions and Baseline Scores With Eye Closure as a Covariate
M (SD)
Live (L) Audio (A) Video (V)
Eyes Open Closed Open Closed Open Closed Source df F η2
Muscle Tension Condition (C) 3 4.04** .08
Baseline 1.97 (.72) 2.45 (.69) 1.98 (.69) 2.31 (.95) 1.92 (.70)bd 2.69ac (.59) C x Eyes (A) 3 .11 .00
Posttest 1.43 (.45) 1.68 (.64) 1.48 (.53) 1.69 (.50) 1.47 (.60)d 1.42c (.73) C x Eyes (V) 3 3.38* .07
C x Eyes (L) 3 .52 .01
Note. N (for all analyses) = 50. Means marked a are significantly higher (p < .05) than means marked b. Change in means marked c are
greater than changes in means marked d. **p < .01 and *p < .05.

61
Table 6 (continued)
M (SD)
Live (L) Audio (A) Video (V)
Eyes Open Closed Open Closed Open Closed Source df F η2
Attention Deficit Condition (C) 3 18.18** .28
Baseline 2.21 (.72) 2.43 (.68) 2.20 (.71) d 2.47 c (.76) 2.18 (.75) 2.53 (.52) C x Eyes (A) 3 2.79* .06
Posttest 1.51 (.51) 1.53 (.41) 1.65 (.53)ad 1.31bc (.30) 1.50 (.57) 1.67 (.64) C x Eyes (V) 3 .74 .02
C x Eyes (L) 3 .39 .01
Autonomic Arousal Condition (C) 3 18.61** .29
Baseline 1.73 (.46) 2.00 (.59) 1.74 (.47)d 2.03c (.67) 1.71bd(.48) 2.22ac (.49) C x Eyes (A) 3 3.86* .08
Posttest 1.39 (.32) 1.45 (.51) 1.41 (.34)d 1.42c (.32) 1.41d (.47) 1.57 c (.58) C x Eyes (V) 3 2.80* .06
C x Eyes (L) 3 .24 .01

62
five stress symptoms assessed by the SSSI-S, only the Autonomic Arousal/Anxiety and Muscle
Tension subscales were found to be significantly impacted by eye closure, so this covariate was
included in the presentation in Table 6. As this table shows, participants who reported having
their eyes closed during the video condition reported higher levels of Autonomic
Arousal/Anxiety and Muscle Tension at baseline than their counterparts who kept their eyes
open during this condition. As a result, eyes-closed participants showed steeper decreases in
arousal and tension as a result of the intervention.
Participants who closed their eyes during the Audio condition also showed steeper
decreases in Autonomic Arousal than their counterparts who kept their eyes open during this
condition. These participants also had especially low scores for Attention Deficit at posttest, and
their change in scores for Attention Deficit from baseline to posttest was steeper than for their
counterparts who kept their eyes open. Correlations also showed that people who kept their eyes
closed in the Video condition had higher scores of Engagement with the task (r = .25, p < .04),
with the same being true for people who kept their eyes closed during the Live condition (r = .27,
p < .03), but not for the audio condition. Stated more simply, participants who reported closing
their eyes during the relaxation tended to report having less Autonomic Arousal after the Audio
condition than those who preferred to keep their eyes open during the Audio condition. In
addition, participants who closed their eyes during the Video and Live condition tended to report
being more engaged by these conditions than those who kept their eyes open. Because no
significant between-subjects effects for whether or not participants had their eyes open or closed
during any of the three treatment conditions were found for these three stress symptoms, the F
statistic for these particular effects were not presented in Table 6.

63
Across all six variables, medium effect sizes for the intervention were found for
Autonomic Arousal/Anxiety (η2 = .44), Attention Deficit (η2 = .37), and Worry/Negative
Emotion (η2 = .35). Small effect sizes were found for Interpersonal Conflict/Anger (η2 = .24)
and for Muscle Tension (η2 = .16). Considering the brevity of the interventions used in this
research, a medium effect size can be considered to suggest a robust effect, worthy of closer
examination. In these findings, the relationship between the interventions and certain symptoms
of stress, such as Autonomic Arousal/Anxiety and Attention Deficit, were stronger than the
relationship between the interventions and the symptoms of Interpersonal Conflict/Anger and
Striated Muscle Tension.
Broken down even further, there was a small effect size found for the effects of the
treatment conditions on the Worry/Negative Emotion subscale for the afternoon classes,
suggesting that the intervention influenced this subscale more strongly in the afternoon than in
the morning. Similarly, small effect sizes were found on the basis of whether participants closed
their eyes during a particular treatment condition on various symptoms of stress. For example, a
small η2 of .08 was found on the Autonomic Arousal/Anxiety subscale for those participants
who closed their eyes during the Audio condition, as compared to an even smaller η2 of .06 for
those who closed their eyes during the Video condition or η2 of .01 for the Live condition. This
finding suggests that the Audio condition was more effective at reducing reports of Autonomic
Arousal/Anxiety than the Video or Live conditions for those participants who reported closing
their eyes to some extent during the treatment. The same was true for the Attention Deficit
subscale, but, in contrast, the Video condition seemed to have more of an impact on the Muscle
Tension subscale than either of the other two conditions combined. A more thorough and
detailed interpretation of these findings will be provided in the following chapter.
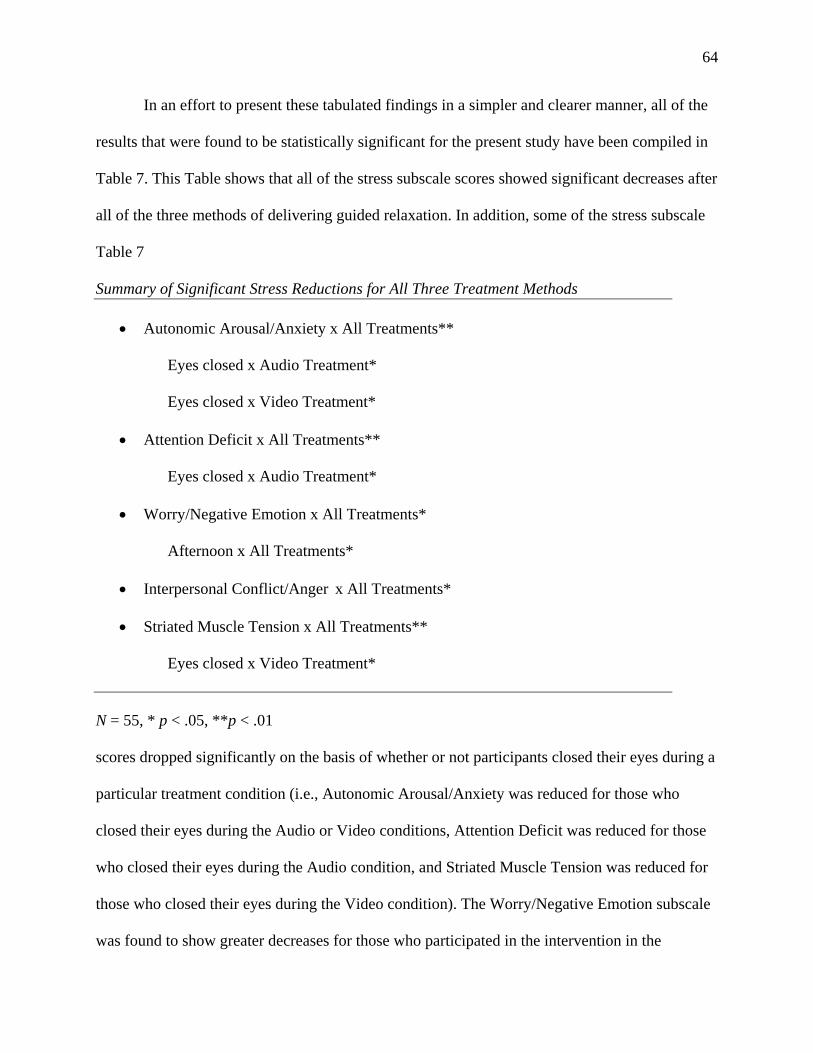
64
In an effort to present these tabulated findings in a simpler and clearer manner, all of the
results that were found to be statistically significant for the present study have been compiled in
Table 7. This Table shows that all of the stress subscale scores showed significant decreases after
all of the three methods of delivering guided relaxation. In addition, some of the stress subscale
Table 7
Summary of Significant Stress Reductions for All Three Treatment Methods
• Autonomic Arousal/Anxiety x All Treatments**
Eyes closed x Audio Treatment*
Eyes closed x Video Treatment*
• Attention Deficit x All Treatments**
Eyes closed x Audio Treatment*
• Worry/Negative Emotion x All Treatments*
Afternoon x All Treatments*
• Interpersonal Conflict/Anger x All Treatments*
• Striated Muscle Tension x All Treatments**
Eyes closed x Video Treatment*
N = 55, * p < .05, **p < .01
scores dropped significantly on the basis of whether or not participants closed their eyes during a
particular treatment condition (i.e., Autonomic Arousal/Anxiety was reduced for those who
closed their eyes during the Audio or Video conditions, Attention Deficit was reduced for those
who closed their eyes during the Audio condition, and Striated Muscle Tension was reduced for
those who closed their eyes during the Video condition). The Worry/Negative Emotion subscale
was found to show greater decreases for those who participated in the intervention in the

65
afternoon rather than in the morning, partly due to the fact that the afternoon classes started
higher on this subscale. Overall, none of the three treatment conditions stood out as being more
or less effective at ameliorating participants’ reports of stress symptoms.
Additional findings. Some additional results were found that bordered on significance that
may require further inquiry to discover the robustness of these findings. Among these findings
were significant correlations between certain baseline levels of stress and certain items reported
on the demographic questionnaires. These findings include a strong positive correlation for
participants who reported using movies as a preferred method for relaxing and the level of
Attention Deficit they reported at baseline (r = .36, p < .01). For participants who reported using
media between 3 and 5 hours per day, baseline levels of Autonomic Arousal/Anxiety were also
significantly higher (r = .35, p < .01). Slightly weaker, but still significant correlations were
found for participants reporting use of electronic media between 3 and 5 hours per day with the
baseline levels of Worry/Negative Emotion (r = .28, p < .05) and Interpersonal Conflict/Anger (r
= .33, p < .05) that they reported. High baseline levels of Interpersonal Conflict/Anger were also
positively correlated with a general preference for music (r = .30, p < .05) but were negatively
correlated with the use of media for more than 5 hours per day (r = -.27, p < .05).
Qualitative findings. A total of 75 of 77 students responded to the subjective open-ended
question at the end of the final implementation of the REES that asked participants to “take as
much space as you need to describe your experience with each of the three exercises and be sure
to state which exercise(s) you enjoy the most and least, and why?” Of these, only 42 participants
reported which of the three delivery methods they liked the most, least, or both. As stated above,
subjective reports for all of the participants who provided answers were included in this

66
preliminary qualitative inquiry, including those who had been selected out of the quantitative
analysis for the reason of their apparent disengagement.
Overall, the students offered a positive response to the three exercises as a whole,
although some reported negative or neutral reactions to their involvement in the program. These
qualitative findings have been tallied and presented in Table 8. This table shows that most of the
students reported that the exercises helped them to feel relaxed overall. Some participants
reported feeling distracted during the program, although some stated that the feelings of
distraction may have aided their relaxation. Some participants reported feeling sleepy or sedated
during the program, with one participant reporting that the exercises “helped me understand how
sleep deprived I am.” Just as many participants reported feeling bored or restless during the
exercises. A few more than 10% of the participants reported their enjoyment of the exercise and
a few less than 10% reported feeling calmed or soothed by the exercise. A few participants
reported experiencing “no change” as a result of the exercise, revealing that they were already
calm or without stress prior to their involvement in the study. A few participants reported feeling
more stressed or tensed by the exercises with one participant stating “sitting still” created stress.
A few participants expressed difficulty relaxing, stating that the “voices were too sharp” or
“annoying,” that the “room was too cold,” or that the exercises themselves were “repetitive,”
“tedious,” “irritating,” and “not fun.” Finally, a couple of participants reported feeling focused
and engaged by the exercises, with one noting that discipline helped to “clear her mind.”
Exactly half of the participants who reported having a preference of one delivery method
over another reported enjoying the video method the most, with many making specific comments
about their enjoyment of the nature imagery itself, or just having something to look at during the
program. Fewer than half as many participants reported enjoying the live method the most, with

67
Table 8
Summary of Common Themes and Method Preferences From Subjective Reports
Preferred method (N = 42) Theme (N = 75)
Most Least
N % N % N %
Method
Video 21 50% 5 12%
Live 8 19% 6 14%
Audio 7 17% 5 12%
Theme
Relaxation 21 28%
Distraction 12 16%
Sleepiness/Sedation 11 15%
Boredom/Restlessness 11 15%
Enjoyment 8 11%
Calmness 7 9%
No change 6 8%
Stress/Tension 5 7%
Difficulty/Irritation 5 7%
Focus/Engagement 2 3% about as many reporting the audio method as most preferred. In terms of the least
preferred method, almost equal numbers of participants reported enjoying each method
the least, with the live method being the least preferred method overall.

68
Anecdotally, a teaching assistant, who was the only other individual besides the
researcher who was in the classroom for all 21 performances of the treatment exercises
(and who had participated actively in many of them), expressed his preference at the
completion of the 4 days of treatment. After sitting through all three methods multiple
times, he stated that the video method seemed to shed too much light into the room and
was too distracting for relaxation. Between the audio method and the live method, he
reported feeling “safer” and more able to “trust” the audio method more than the live
method, due to its predictability and what he described as a sort of acoustic depth that
was lacking in the live version. He had not met me prior to the study and did not know
how well he could trust me during the live method, but felt that he could relax in the trust
he felt with the audio method, despite his knowledge that the voice in the audio method
was mine as well. This subjective report seemed genuine enough to include in this
section, if only to provide information for similar research intended for older participants.

69
Chapter 5: Discussion
Summary and Interpretation of Findings
Overall, the research appeared to be successful inasmuch as the results showed that a
brief 10-minute guided relaxation produced statistically significant reductions in self-reported
stress levels for all participants in the study. These findings make a strong argument for the
inclusion of similar exercises in school curricula to aid students’ general composure and well-
being. Some of the findings uncovered by this study are consistent with the existing research that
was outlined in Chapter 2. However, some findings are anomalous. In this section I will present
the major findings of the present study and provide some interpretation for the results in light of
the research already cited or with the help of studies that have not yet been cited. In all cases, I
will offer some interpretations of these results and suggestions for the direction that might be
taken for follow-up research.
The present study found that all three methods of delivering guided relaxation were
equally and significantly effective in the amelioration of all five subscales of stress. These
findings were consistent with the kinds of research cited in Chapter 2, which suggested that
various types of guided relaxation will reduce most kinds of psychological stress (Smith et al.,
1996). However, the fact that there was no increase in any of the stress reports, or any
differences between the three methods in terms of their efficacy in the amelioration of stress
reports, was somewhat surprising and inconsistent with earlier research. For example, previous
studies comparing recorded and live methods of guided relaxation suggested that the recorded
methods were less effective in their reduction of stress than the live methods due to their lack of
contingent feedback with the participants (Paul & Trimble, 1970). Given the datedness of that
research, the present study may have served to update these findings, suggesting that either an

70
older mean age of the participants, or a more contemporary population may be more predisposed
to the use of recorded media than those studied in earlier research. The absence of significant
differences between the three methods explored by the present study provides useful information
as to the utility of Media Assistance as an adjunct to more traditional forms of intervention.
The absence of statistically significant differences between the efficacies of the three
methods also suggests that some forms of visual media may not increase stress as has been
previously posited in the literature (Kubey & Csikszentmihályi, 1990; La Ferle et al., 2000; Lang
et al., 2000; Reeves & Thorson, 1986). Although these studies suggest that some of the stress
induced by visual media is due to its graphic or provocative content, many of the studies point to
the basic features of visual media (such as cuts, zooms, pans, and edits) that were present in the
video used for the present study. According to these studies, these basic features of visual media
may be responsible, at least in part, for the stress-inducing functions of the format. To be sure,
the kinds of dissolve transition edits used in the visual media that was explored by the present
study is of a very different type than the kinds of abrupt and rapid-style edits used in the kinds of
media that examined by these studies. However, the findings of this study call for a closer
examination of the potentially positive role visual media may play in the lives of adolescents,
and stand in contrast to an indictment of the medium as a whole.
The results of the present study suggest that the basic features of visual media, alone, are
insufficient to significantly influence participants’ self-reports of stress. Although the lack of
stress-inducing impact of the video condition may have been due to the limited amount of time in
which the participants were exposed to it, follow-up research would be needed to conclusively
confirm this speculation. Indeed, no one method of delivering guided relaxation was found to be
more efficacious in its reduction of stress than any other method explored in the present study.

71
Some significant differences were found between the different subscales of stress that
were measured, however. Participants who underwent the three conditions in the afternoon
periods as compared those who participated in the morning periods had marginally higher (p <
.07) baseline scores for the Worry/Negative Emotion subscale than their counterparts in the
morning periods. However, these scores dropped to equally low levels for both the morning and
afternoon participants at the time of the posttest. Such a finding suggests that students in the
afternoon periods may have been more “keyed up” than their morning counterparts. It remains
unclear whether this difference was a result of the time of day (as, for example, the accumulated
stress associated with mounting academic and social pressures that built up over the course of the
school day), or if it was merely the result of a biased sample in which a predominance of
distressed or worried students were assigned to the afternoon sections of this course as compared
to the morning sections. This finding seems relevant for education, particularly as it pertains to
classroom assignment or the scheduling of certain curriculum during the school schedule. Yet, in
order to determine whether the time of day was in fact responsible for the higher levels of worry
and negative emotion after midday or if it was a function of classroom assignment, a similar
study would need to be run with classes whose schedule changed between morning and
afternoon periods. In the absence of the definitive data that such a study would yield, the impact
that the time of day had on the students’ reports of worry and negative emotion remains partially
in an area of speculation.
Differences between the various subscales were also found to be associated with
participants’ reports of closing their eyes to some extent during one or more of the conditions. In
fact, participants’ level of relaxation appeared to be a function of closing one’s eyes, especially
during the video condition. For those participants who reported closing their eyes to some extent

72
during the video condition, significantly greater decreases on both the Striated Muscle Tension
subscale and on the Autonomic Arousal/Anxiety subscale were found when compared to those
participants who elected to keep their eyes open. Similarly, participants who reported closing
their eyes to some extent during the audio condition reported significantly lower Autonomic
Arousal/Anxiety and Attention Deficit levels after the relaxation than those participants who kept
their eyes open. Such differences could be expected given the research associating closing one’s
eyes with the process of relaxing, as cited in Chapter 2 (Benson, 1977; Craig et al., 2000;
Putman, 2000), but the absence of significant differences on the other three stress symptoms
between those participants who closed their eyes and those participants who did not is not well
understood.
This finding might have been due to the predisposition of participants who reported
closing their eyes. The results of the present study showed that the baseline scores for Muscle
Tension and Autonomic Arousal were significantly higher for those participants who reported
closing their eyes during the Video condition than for those who reported keeping their eyes
open. This finding suggests that individuals with high levels of tension or arousal may be more
predisposed to closing their eyes during all or part of the video condition than those with lower
tension or arousal. Students with high anxiety, arousal, or tension may be seeking a refuge from
the discomfort of muscle tension and anxiety by closing their eyes during the Video condition as
indicated by the fact that closed-eyed stress levels drop to equally low levels as open-eyed stress
levels. It is conceivable that, by closing their eyes, students with high tension or arousal
successfully established the kind of “quiet environment” that Benson (1977) posited as one of the
four underlying elements that should be present to effectively elicit the Relaxation Response
(RR). This interpretation also helps to explain why Attention Deficit levels would dropped

73
significantly lower for those students who closed their eyes during the audio condition than those
students who kept their eyes open. These results indicate that, in presenting these types of
exercises, some individuals may feel more comfortable closing their eyes than others, due to the
individual’s own history, comfort, or present level of trust in the presenter. Given that, it may be
noted that individuals who wish to close their eyes during the program may even be encouraged
to follow their inclination to do so, providing that they remain awake, given that the research
suggests that those who close their eyes seem to benefit from doing so across certain subscales of
stress.
Other baseline measures of stress were found to be significantly correlated with
participants’ use of various media. Such correlations are indicative of certain associations
between adolescents’ use of media and stress levels but require further inquiry to suggest a
definitive link. The presence of Attention Deficits at baseline for those individuals who reported
using movies as a preferred method of relaxation (r = .36, p < .01) is one such finding that
warrants follow-up research. This finding may be interpreted along the lines of compensatory
behavior inasmuch as movies elicit the greatest demand on sustained exterior attention than any
of the media choices presented on the demographic questionnaire. In comparison with music,
television, or the internet, movies tend to elicit prolonged attention to external stimuli, which
may help those with attention deficits to establish a relaxed (or homeostatic) state of mind.
Whether one causes or facilitates the other would require follow-up research.
Another correlation warranting follow-up research pertains to the presence of high levels
of Anxiety, Worry, and Anger at baseline for those participants who reported a daily exposure to
electronic media for 3 to 5 hours. Reports of this level of daily media exposure were claimed by
nearly half of the entire population that was studied, suggesting the prevalence of electronic

74
media in these adolescents’ lives. Whether the significant correlation of Anxiety (r = .35, p <
.01), Worry (r = .28, p < .05), and Anger (r = .33, p < .05) with 3 to 5 hours of daily media is
indicative of teens seeking escape from stress through various forms of media—as some
researchers (Bickham et al., 2003; Lohaus et al., 2005) have suggested—or the result of
electronic media inducing stress—as other researchers (La Ferle et al., 2000) have suggested—
the association between extended use of media with certain emotional states in teens has been
confirmed by this study and warrants further research. Interestingly, reports of Anger were
significantly lower for those participants reporting daily exposure to electronic media of 5 hours
or more (r = -.27, p < .05), suggesting that extended periods with electronic media is associated
with decreased levels of anger.
Aside from these correlations, no additional demographic variables were associated with
the stress-ameliorating efficacy of any of the guided relaxation methods. In other words, gender,
age, ethnicity, grade point average, socioeconomic status, and media preferences were in no way
significantly related to the efficacy of one guided relaxation condition over any other. This result
is in slight contrast with the Media Practice Model theory (Steele & Brown, 1995), which
suggests that an individual’s sense of identity (that is, the individual’s unique experiences,
motivations, and expectations) may influence the impact that certain media has on that
individual. Whereas this may be the case for certain narrative forms of media as some
researchers have suggested (Brown, 2006; Brown & Walsh-Childers, 2002; Levy & Windahl,
1985; Rubin, 2002; Ward et al., 2002), this theory was not borne out by the data gathered in the
present study, which may have been limited in terms of the content employed in the media used,
limited demographic diversity represented by the sample studied, or the unique sensitivity of the
instrumentation that was employed. The different forms of imagery used in the video, for

75
example, or the greater cultural diversity participating in the study, or the more qualitative
measures used for assessment may have each yielded differences within the efficacy of the three
methods explored in this study. Further exploration would be needed along these lines in order to
determine the role a dialectic interaction between various forms of media and its users could
have, especially with regard to Media Assistance methods of treatment as outlined in Chapter 2
(Byrnes, 1996; DeSchriver & Riddick, 1990; Smyth et al., 1999; Wells, 2005).
In terms of the participants’ subjective reactions to the three exercises, it was remarkable
to find such a robust preference for the video method over the other two methods of delivery.
Exactly half of the participants who reported a preference at all reported the video method as
their most preferred method of the three conditions. The audio and live methods split the
remainder almost equally, suggesting that the video method was the most subjectively enjoyable.
Although this finding was not expected, the ubiquity of visual media in the lives of modern
adolescents as discussed in Chapter 1 may help explain a preference for visual media over the
other two methods of delivery. This interpretation is underscored by the fact that the live method
was reported as the least favorite method among those who reported a least preferred method,
albeit by a small amount more than the other two. Whether the participants’ reported preferences
of one method over another was associated with their reports of their daily exposure to media or
preferred form of media is an inquiry warranting further attention. Given the fact that one
participant’s preferred method of delivery may be another participant’s least preferred method, in
addition to the fact that no one method was found to be significantly more effective in its
reduction of stress than any other, presenters of these exercises may be well-served to offer their
participants the choice of which method—if any—the adolescent would like to use once they

76
have had the opportunity to experience both the Audio and the Video formats, which tend to be
the more convenient and less expensive formats in comparison to the Live format.
In terms of the participants’ more descriptive reactions, there seemed to be a majority of
students reporting feeling relaxed by the exercises overall. This may have been due to the
demand characteristics of participants reporting what they believe the researcher wants or
expects to receive. The same may be said for those participants who reported enjoying the
exercises, or feeling “calm[ed]” or “soothe[d]” by them. To the as-yet-unknown extent that these
reports were authentic, participants were positively impacted by their involvement in this study,
supporting its continued use with students in the classroom setting.
Yet, the participants’ reports of less positive reactions warrant discussion, as such
reactions may be associated with individuals’ stress levels or other forms of well-being. For
example, participants’ reports of feeling sleepy or sedated may be attributable to the relative
novelty of these types of exercises with regard to the participants’ overall lack of prior
experience (as indicated in the demographic questionnaires). An exercise whose purpose is
relaxation that is not sleep, may evoke a certain amount of dissonance for those participants with
little or no prior experience relaxing. The familiar subjective interpretation of such dissonance
may be in terms of sleepiness, which is an appropriate reaction to relaxation if someone is
unfamiliar with its practice. Similarly, participants who reported feeling bored or restless during
the conditions may have also been unaccustomed to involvement with exercises whose chief aim
is not to impart information or some overt behavior, but rather whose purpose is aimed at
becoming more reposed and restful. The process of relaxation, for students whose entire day may
be filled with demands on their external attention, may seem rather “boring” or “tedious.”
Follow-up research would be valuable along the lines of the extent to which previous exposure to

77
relaxation techniques correlates with subjective reports of sleepiness, boredom, or restlessness as
a result of the exercise. Similarly, students may be filling their days with activities to distract
themselves, in part, from the discomfort associated with the stress they are carrying. Practicing
relaxation could, in effect, allow the stress to become apparent, which the student experiences as
“boredom,” “irritation,” “annoyance,” and other negative feelings.
For those participants who subjectively reported “no change” in their stress levels after
the exercises, distinctions at baseline were not apparent between them and the rest of the sample.
Similarly, those participants who reported feeling “annoy[ed]” or “irritate[d]” by the exercises
were not significantly higher on the Anger subscale than the rest of the sample at baseline.
Unfortunately, such comparisons were not entirely reliable due to the small sample sizes among
the groups that constituted the themes elicited by the qualitative analysis. Yet, in the absence of
statistical comparison, such negative reactions might be interpreted in a number of ways. One
interpretation may be that participants’ negative reactions to the exercise might have been due to
a feeling of dislike or distrust of the researcher. If, for example, the exercise was taught and
employed by a student peer, a familiar teacher, or a professional trainer, the students’ reactions
may have been more positive. Another interpretation may be that these participants were deterred
by the specific content of the exercise and that different content, such as one that employed
music or directions for yogic stretching, might have been more conducive to these participants’
overall enjoyment. Yet another interpretation may be that the participants were positively
impacted by their involvement in the exercise, that they felt genuinely relaxed by it, and that
these participants felt disarmed or disoriented by such an impact and therefore reacted with
feelings of negativity. Further exploration along these lines, with larger sample sizes, would be
warranted and valuable for the exploration of such connections.

78
With regard to the portion of the population who had apparently disengaged from
participation in the study as evidenced by their minimal reports of stress on the SSSI-S, it would
be worth exploring the extent to which these students differed from their more engaged
counterparts, aside from the demographic distinctions noted in Chapter 4. It may be interesting to
examine, for example, how participants who failed to engage with in-class activities such as the
one employed in the present study compare with those that did engage in terms of the
psychosocial development. That is, do the disengage participants predominate within any one of
Marcia’s four identity statuses, as outlined in Chapter 2? Do they tend to present a more diffused
or foreclosed identity than those who are more engaged? Do the engaged participants tend to
present a more achieved identity than those who have disengaged? If such a distinction could be
established, students’ participation (or lack thereof) in relaxation exercises such as the ones
presented by this study might not only serve as a useful means of teaching and practicing a
stress-reduction technique, but might also help the assessment of the students’ level of
development, which, in turn might facilitate a more individualized and tailored approach.
Moreover, the fact that there was a subgroup of students who had seemed to disengage
from the exercises raises the issue of some students’ capacity to self-determine their needs and to
self-regulate their personal level of involvement in such programs. According to the self-report
measures of stress, some students did not appear to find any personal relevance of the exercise
for them in their relaxation, indicating a sort of self-regulated disengagement from the program.
From this, I interpret that making an exercise such as this one a requirement for all students
would be contraindicated, given that it would, at best, produce little or no benefit or, at worst, an
increase rather than a reduction in stress levels due to the student’s resistance. These findings
suggest that students may have the ability to determine for themselves what they need. As such,

79
they may be given the option as to whether or not they wish to participate. Overall, students
seem to know whether or not they needed or would benefit from engaging in a relaxation
exercise, whether or not they would benefit from keeping their eyes opened or closed, and which
medium they subjectively enjoyed the most. As a result, future indications of relaxation exercises
such as these would be well-served to offer participants options across each of these dimensions.
Limitations and Delimitations
The shape and scope of the present research posed many limitations and delimitations on
the utility of its results. This section will discuss this study’s many limitations and delimitations,
some of the ways I attempted to curb their influence on the results, and suggestions as to how
such limitations might be addressed in future research. The first limitation in this study is that it
is primarily an exploratory study that aimed to explore the role of electronic media in the
treatment of stress with adolescents as well as the role of relaxation in the classroom
environment. Given the current dearth of research on these topics, particularly as they pertain to
adolescents, this study aimed to explore this population in terms of its relationship with
electronic media and relaxation techniques in the service of stress reduction. As mentioned in
Chapter 2, Media Assistance is a generally emergent area of research and has yet to be
thoroughly defined or researched.
One significant limitation is that the population sampled by this study is representative
only of self-selected Northern California high school students in the “Focus on Success”
program and thus posed a threat to the study’s external validity. The study’s results are not
generalizable to the wider population of adolescents because the sample was localized and
participants’ involvement was voluntary. It is hoped that the findings, however ungeneralizable,
might still provide a preliminary indication as to whether segments of the adolescent population

80
are influenced by different ways of delivering guided relaxation. Larger, school-wide
participation in future studies would yield far more generalizeable results in terms of the
usefulness of Media Assisted guided relaxation programs in the classroom.
Another limitation of the present study has to do with the fact that the first day of the
data-collection portion of this study took place on a historical day. The classes’ routine was
modified slightly so that students were allowed to view the inauguration of a new President of
the United States of America. The extent to which any excitement about such an event could
have influenced the stress-ameliorating impact of a guided relaxation program is unclear, but the
fact of this event coinciding with the implementation of a relaxation program should not be
overlooked as a potential limitation of the study’s results, keeping in mind that all of the students
viewed this historic event at the same time, thereby presumably influencing all of the participants
uniformly.
In terms of the interventions themselves, the quality of the equipment being used did not
generate the most immersive experience to participants and might therefore have limited the
robustness of its effects. For the AGRP, a medium-sized stereo system was used to play the
recorded program on CD at a medium volume. This same stereo was used to provide the audio
component for the VGRP while the video of nature imagery was played on DVD and projected
onto a 36-inch screen at the front of the classroom. It should be noted that the projected image
occasionally flickered during the treatment condition, which may or may not have influenced the
amount of relaxation (or concomitant stress) that was achieved. A careful record of which trials
of the video-guided program might have been impacted by the flickering image was not
recorded. Such occurrences have implications for future research studies that explore this method
of delivering guided relaxation. A research assistant might be employed to monitor and record

81
such instances to explore whether or not they influence the efficacy of the program or
intervention. However, it may be noted that, although the equipment used for this condition was
prone to some dysfunction, this limitation did not seem to interfere with the significant benefits
that many students managed to glean from its employment. In fact, most students still expressed
an overall preference for this condition over the other two.
Whereas a high quality video image might have positively influenced the impact of the
visual imagery being depicted, such equipment was outside the financial and logistical scope of
the present study and would not be entirely representative of the ways in which VGRP would be
most readily implemented as an adjunct to clinical treatment (Persky & Blascovich, 2007).
Similarly, whereas multiple speakers surrounding the listener would be more likely to generate a
more immersive and therefore robust and significant effect, such equipment is not yet a feasible
expectation for how Media Assistance may be implemented, although it is hoped that, with
further research, such equipment might be explored for its potential viability for Media
Assistance. Again, as the benefits reported by the participants in spite of the slight technical
difficulties with the equipment seemed to indicate, such perfectly functional equipment does not
seem to be necessary to evoke a positive effect.
Another threat to this study’s internal validity was due to the potential for contamination
that might have occurred between the seven treatment groups. It is possible that the participants
in the seven groups could have discussed their experiences with one another during the interim
periods between the treatment conditions, thereby influencing the responsiveness or expectations
of the participants during subsequent meetings. Moreover, nonclinical group exposures to the
three treatment conditions created the likelihood of individuals’ responsiveness to the treatments
regressing towards the overall mean for the seven groups. Given the traditional high school

82
setting, with students intermingling throughout the day, the potential for contamination as a
threat to the study’s internal validity cannot be entirely controlled. However, I aimed to minimize
this threat of contamination by encouraging the participants to keep their thoughts and feelings
about the treatments to themselves until after their participation had been completed (see
Appendix H). Moreover, it is believed that, for the influence of the treatment conditions to be
viable, their effects would need to maintain a magnitude that outweighed any possible influence
that such contamination between the groups might have had.
Another limitation that posed a threat to the present study’s external validity was that the
use of questionnaires to quantify the symptoms of stress could be somewhat superficial in terms
of eliciting more meaningful or in-depth information about the experience or the phenomenon of
stress. Although questionnaires can be helpful in the collection of large amounts of information
on specific conditions, some of the more meaningful or compelling nuances and intricacies of
those conditions are not adequately captured by the statistical analysis of pencil-and-paper
surveys. However, objective assessment aside, the subjective self-report measures serve as
perhaps the greatest determinants of whether or not participants are likely to continue with a
given exercise (as the strong correlations of the three subscales of the REES between Enjoyment,
Engagement, and Interest in Repeating seemed to indicate). Thus, if a person is to benefit from
an activity, the person will need to practice in an ongoing manner. Ongoing practice, according
to this correlational finding, is best sustained if the activity is subjectively experienced as
positive and beneficial, as seemed the case for many of the participants in the present study.
In addition, the self-report measures of stress might have been prone to a certain amount
of floor effects whereby the participants’ reports hovered proximal to the lowest possible value,
failing to adequately depict the variable extent of stress states the participants were experiencing

83
at the moment of reporting. Even after selecting out a sizeable portion of the population whose
reporting variability ranged minimally if at all, the majority of the remaining participants’ mean
scores ranged between 1 (“doesn’t fit me at all”) and 2 (“fits me a little”), with only a few
exceptions. Expanding the levels of possible responses from 4 to 6 might help to limit the impact
such floor effects might have had on the reliability of the data analyzed by the present study.
Furthermore, reverse-coding some of the items (that is, phrasing an item in terms of its opposite)
might also help to limit the students’ tendencies to respond to the questionnaire by rote, as
opposed to a more thoughtful report of their self-assessment.
In addition, all of the participants’ measures were self-reported. Although self-assessment
can be a way to solicit information about certain psychological experiences or conditions, they
may be subject to some degree of participant biases. Participant bias occurs when research
participants make an intentional effort to influence the outcome of their responses. Such bias
may be magnified among an adolescent population whose tendency may be to respond in ways
that suggest “normalcy” as opposed to accuracy or honesty. Because many of the questions on
the SSSI-S (see Appendix C) and the REES (see Appendix D) can be seen by the participants as
having a “correct”—that is, more socially desirable—answer, it is difficult to discern the degree
to which participants selected answers that best represented their feelings as opposed to those
that portrayed them in a more positive (or negative) way. Therefore, another threat to the present
study’s external validity and a limitation in its design is that the measures did not necessarily
evaluate the presence or absence of stress directly but, rather, the participants’ tendencies to
respond to the questionnaires as such; thus, their responses may have been biased.
Because a certain amount of inaccuracy is expected in the use of self-report measures that
are not automatically responsive, self-report measures such as the specific instruments used in

84
this study were designed to overcome the potential for bias by including multiple statements
referencing a single category or state (Piiparinen & Smith, 2003, 2004). It may be added that the
SSSI-S is a measure of a state of mind that is, by definition, transient and subject to change
(Smith, 2005). As a result, the timing in which the measure is administered might have
influenced the data that were produced. It is important, for example, that these measures evaluate
the participants’ stress as a function of the particular treatment condition and not as a function of
the instrument itself. In an attempt to minimize this threat, the SSSI-S was administered
immediately upon completion of the treatment, and was then followed by the REES. Also, the
same instruments were used in all of the treatment conditions so that any effects measured by the
instruments themselves remained uniform.
However, modifications to the self-report instruments could not control for those students
who appeared to resist participation in the study altogether. As reported above, a total of 21 of
the 77 participants appeared to disengage from the study and were thus eliminated from the
sample pool prior to the primary analysis of the data. Preliminary results confirmed that this
disengaged segment of the sample were more likely to be males who reported a low grade point
average. Although the specific reasons for this segment’s disengagement remain unclear, it may
be speculated that their disengagement might have been related to their perception of the study as
being a formal “class assignment” and therefore subject to the poor academic performance that
they reported to exhibit throughout their academic career. It is possible that the students,
primarily males, who tended to disengage from the study may be opposed to participation in
sedentary activities in general—hence the poor grades on assignments which tend to reward
mental over physical performance—and relaxation exercises specifically. Academic incentives

85
such as extra credit may have paradoxically deterred some participants who are generally
opposed to academic rewards for curricular performance.
Their disengagement might also have been related to their perception of the researcher as
a teacher, rather than as a peer, who would be grading their performance as a teacher would
examine a classroom assignment. In this manner, the level of disengagement might have been
due to the study’s methodology rather than the result of the students’ lack of stress at the outset
of the study and throughout the duration of the interventions. This segment’s lack of candor on
the given assessments might have been related to an overall resistance to perceived authorities—
as the researcher may have appeared to them—although this speculation could not be confirmed
without additional research or examination. Whatever the reasons for this segment’s minimal
participation in the study, the efficacy of the given treatments with this group remains unknown,
as the lack of valid data neither confirms nor rejects the given treatments’ effectiveness Had I
more time, charisma, or resources available to connect with all of the students more closely or
had the classes been more accustomed to my presence in the classroom with them over time, the
number of resistant or disengaged participants might have been reduced or eliminated. In
addition, had the treatments themselves been presented by someone other than myself, either a
teacher with whom the students had come to form a relationship or perhaps even another peer,
the number of resistant or disengaged students might have been reduced or eliminated. These
issues raised by the unexpectedly high number of disengaged students might offer some
suggested guidelines for future studies along these lines, which might help to implement
alternate settings to control for such a problem or alternate measures to aid in capturing its
effects.

86
Participants whose responses to both the baseline measures and to the three repeated
measures of SSSI-S reflected the overall sense that the scale did not apply to them at all were
removed from the data sample prior to analysis. Although it is possible that these students were
extremely relaxed from the outset, it is unlikely that no statement on the SSSI-S seemed to fit
their present experience at any time throughout the three employments of the instrument. As
such, these participants’ scores were removed because it is believed that this data would have
skewed the data in such a way that suggested that the treatment conditions were having little or
no effect when, in fact, they were having an effect which was going under-reported. With this in
mind, it was determined that, due to the appearance that the instrumentation was inadequate to
capture the students’ experience of stress, whatever effects that the treatments might have been
having among these 21 participants, the self-report instruments that were being used to assess
such effects were inadequate tools of measurement for this portion of the sample. Follow-up
studies with more adequate measures of stress would be needed to further confirm the efficacy of
these types of interventions for this portion of the population. However, at the same time these
self-report measures proved invaluable for picking up this subset of the population that
disengaged from the study in a similar manner as the false-positive or false negative scales
embedded within the Minnesota Multiphasic Personality Inventory (MMPI) would do.
One variable has been identified as having a likelihood of confounding the results of the
present study and limiting the conclusions that may be drawn from it. The variable of individuals
tending to close their eyes during the AGRP and the LGRP, but not during the VGRP, might
have potentially influenced the extent of relaxation and, by extension, stress reduction that was
achieved and reported. Such a discrepancy between eyes-open and eyes-closed relaxation
techniques has been borne out by several recent studies that have shown how closing one’s eyes

87
can increase the appearance of the alpha brainwaves (8-12 cycles per second) associated with
relaxation in the place of beta brainwaves (13-25 cycles per second) associated with the state of
being awake and alert (Craig et al., 2000; Putman, 2000).
Another limitation has to do with the limited time constraints of the participants’
availability at the high school. Whereas some research has shown that multiple 30-minute
sessions practicing relaxation techniques are sometimes necessary in order for the participant to
become proficient enough to demonstrate the technique’s specific effects (Smith et al., 1996),
participants in this study practiced the technique for a total of only three 10-minute sessions. This
restriction limits the potential efficacy of the treatment and of the effects reported in this study to
differences that could become more robust given a more prolonged exposure to and practice with
the various treatment conditions being explored. If the students had more time with me and with
the techniques, they might have felt more comfortable and been better able to follow along with
the guided relaxation instructions. Having a mere 10 to 15 minutes per class to complete the
exercise and to fill out the questionnaires may have created a feeling of being rushed that
counteracts the establishment of deep levels of relaxation. An attempt to overcome this limitation
was made in the increased sensitivity of the statistical methods used to analyze the data gathered
during the course of the interventions. Moreover, given that the results of the present study
indicated the general utility of the three relaxation methods, a more extended exposure to the
treatment conditions should be considered for follow-up studies.
Similarly, the fact that the conditions themselves were only practiced for a total of three
times for each class served as a limitation on the potential impact that these exercises could have
had on the students’ levels of stress. Although it is possible that some of the effects of the
exercise were due to its relative novelty for the participants—a novelty that would quickly
88
diminish over prolonged use of the exercise—it is also possible that the exercise could have had
more robust and long-lasting effects, serving not only to reduce the participants’ moment-to-
moment stress states, but also to enhance some of the additional benefits associated with guided
relaxation that were discussed in Chapter 2 (Deckro et al., 2002; Scheufele, 2000). It is
encouraging to note that teachers with limited time and resources can still feel justified in
presenting a brief relaxation exercise a few times with imperfect equipment, as even the brief
exercises with imperfect equipment did seem to evoke beneficial effect.
Along these lines, another limitation had to do with the limited knowledge that I had of
the living, social, and school environments to which the students were accustomed. As noted in
Chapter 2, stress tends to be a combination of normal adolescent development (Hutchinson et al.,
2006; Kraag et al., 2006; Washburn-Ormachea et al., 2004), the presence of certain situations
over which individuals perceive themselves to have little or no control (Frydenberg & Lewis,
2004; Hurrelmann & Raithel, 2005; Hutchinson et al., 2006), and the challenges posed by
traumatic life events, such as accidents, illnesses, or divorces (Nastasi et al., 2007). The limited
familiarity that I had with the relative presence or absence of these contributing factors in the
lives of my participants might have limited my ability to connect with the students during the
exercises and to understand them during my analysis and interpretation of the results. This is
particularly the case for the portion of the students who had disengaged from the study, as well
as for those students who presented greater anxiety during the afternoon classes. The ability to
spend more time in getting to know the students and their unique living, social, and school
environments might increase the depth that might be gleaned from this research.
In addition, because almost every element of this study was considered to be innocuous if
not intentionally beneficial, it is impossible to anticipate or know how all of the participants

89
might have interpreted, responded, or reacted to every aspect of their involvement in this study.
Although relaxation techniques tend to be beneficial for most people, a paradoxical relaxation-
induced anxiety reaction remains a distinct possibility (Smith et al., 1996) as evidenced by some
of the students more negative subjective responses (e.g., irritation or tension). As a result, I took
all of the known precautions, including providing my contact information to the all of the
participants, should concerns arise or a list of clinical referrals for counseling services be
requested. Although no such contact or requests were made during the course of the study, it
remains unclear whether the informed consent forms, which delineated to all the participants
their right to deny their consent or to discontinue their participation in the study at any time
during the research process and for any reason without discrimination, served as an adequate
informant to the participants’ liberties throughout the study. Although such relaxation-induced
anxiety was not evidenced by the quantitative measures of stress provided by the SSSI-S, this
response did seem to appear in the participants’ more negative subjective responses, such as
feeling irritated or tensed by the exercises.
Several possible demand characteristics in this study may have influenced its results and
thus represented another limitation. One demand characteristic was that the participants received
the intervention and were given the surveys in a classroom setting. As a result, the participants’
experiences of the interventions and their responses on the questionnaires might have both been
influenced by their presence in this particular environment, treating the interventions as an
academic, rather than therapeutic, activity and treating the questionnaires as an academic, rather
than psychological, assessment. This might have limited the therapeutic potential of the
treatments and the reflective candor elicited by the questionnaires. As such, the extent to which
the context and setting of the treatments influenced their respective impact as compared to, for

90
example, if the study had been performed during a study hall, or after school, or outside of the
school setting altogether remains unclear. Furthermore, some students may have completed the
questionnaires according to their willingness to go along with what they perceived to be the
researcher’s expectations of them, as opposed to being an authentic response to the given
exercise. Such a demand characteristic might have been further exacerbated by the teachers’
routine provision of in-class participation credit after each employment of a daily exercise, of
which this study was a part. Another demand characteristic pertains to the sort of motivations
with which the participants entered the study. These may have ranged from being influenced by
the presence of their peers, their desire to receive approval from their teacher, escape class work
or to get class credit, or their curiosity about being involved in a psychological study.
In terms of experimenter bias, my involvement in the study has undoubtedly impacted the
effects found in the research, although the exact impact of my involvement remains unclear. For
example, the fact that I recorded and performed the guided relaxation programs for all three
treatment conditions might have influenced some participants to respond to me as a certain type
of person, rather than to the treatment condition itself. Suffice it to say that the extent to which
the participants’ reactions to the treatments would have been different had I been older or
younger than I am, an employee of the school or a classmate, a woman of a different ethnicity or
background, and so on remains unknown. The fact that it was clear to the participants that I was
both serving in the role of the researcher of the study as well as being the provider of the various
treatment conditions could have influenced the demand characteristics of the study in one
direction or the other. Again, this bias was held by the researcher throughout the study for all of
the participants and so whatever influence this bias may have had would have been uniform
across all participants.

91
In addition, as the researcher I firmly believe that stress in adolescence is an important
area of research and that guided relaxation tends to be a viable means of managing it. Although I
remained mindful of this bias during the distribution of the consent forms and research packets
during the interventions themselves and during the analysis and interpretation of the data, it is
certainly difficult to omit this bias completely given my own positive experiences with the
processes that were presented. Although the lack of available resources made it impossible to
double-blind this study, I did enlist unbiased assistance during the scoring of the instruments and
the analysis of the data, even though objective and statistical measures were selected specifically
in order to curb the potential for interpretative bias and increase the validity of the results
produced.
Directions for Future Research
The present study offers many fruitful directions for follow-up studies and future
research. It is quite heartening to find that such a brief intervention, lasting only 10-minutes in
duration, which is economical in terms of its required time, equipment needs, and overall effort,
produces significant drops in self-reported levels of psychological stress. As such, follow-up
studies along these lines would be warranted and encouraged. Among these include research that
explores some of the educational and clinical implications posed by the present results. The fact
that none of the methods, be it audio, video, or live, was found to be more effective in its
amelioration of stress reports than any other provides encouraging support to the use of audio- or
video-recorded relaxation exercises in the absence of a live trainer. In fact, the live method
appeared to be the least preferred method among the participants studied here, suggesting that
the cheaper, more convenient methods of audio- or video-guided relaxation programs are just as
effective and also more preferable. As such, audio CDs or video DVDs might be made available

92
to adolescent clients or to students as a means of learning, practicing, or supplementing a stress-
reduction protocol. Such easily accessible exercises might help to facilitate classroom
management or other clinical interventions that are otherwise difficult to achieve when needed.
The exploration of these exercises in the classroom or clinical setting could yield invaluable data
with regard to its usefulness for students’ academic performance or in terms of its utility for
clients’ psychological or emotional wellbeing. Such follow-up inquiries seem warranted by the
results gleaned by the present study.
As noted in the previous section, a closer examination of the role that time of day had on
participants’ baseline measures of stress would provide useful information in terms of how to
schedule these types of exercises during the school day. In addition, a more controlled
examination of the role that eye closure had on the impact of the exercises may be useful in
terms of understanding how it may directly impact one subscale over another. The fact that such
findings emerged during the analysis of the data suggests that research on this factor, as a central
focus of future studies, is warranted by the results found here.
Another avenue for future research could entail its implementation by a teacher or
someone with whom the students have established an existing relationship. This may help to
reduce some of the bias that could have been generated by the demand characteristics of the
study inasmuch as the students are able to honestly present their current level of stress, rather
than compose their responses to a particular expectation.
Additional replication of the present study would be needed to address some of the
subtler findings noted above. For example, the use of more rigorous psychophysiological
measures (such as EEG, EKG, GSR, and others) could serve to illustrate, in a more finely-tuned
manner, the neurological, psychological, and physiological impact that guided relaxation can

93
have on adolescents. Short of the enormous resources needed to implement instrumentation of
that type with a large population, the present study might be replicated with the use of a stress
scale that limited the potential for floor effects and that reverse coded some of the items to
discourage disengagement. In this way, a more finely-tuned picture of the stress levels reported
by the participant could emerge.
Furthermore, it would be worth offering a program like this one over the course of
several weeks, perhaps providing students with the freedom to choose among the three
conditions, to explore the extent to which the stress-ameliorating effects of the exercises persist
over time and to examine if significant distinctions between the effects of the three conditions
emerge over the course of time. It is possible that one condition is more conducive to repeated
practice than another, but further research would be needed to elaborate upon this speculation.
Such follow-up research or longitudinal replication would also help to elucidate the extent to
which the effects of these types of interventions tend to last and how quickly such effects tend to
diminish.
Another way to follow-up on the present study would be to replicate it with the use of
different measures, aimed to explore the psychosocial impact that such exercises might have with
this population. As noted above, a better sense of the psychological distinctions that existed
between those participants who seemingly disengaged from the study and those who did not
would be most useful in terms of guiding the focus of future interventions of this kind. For
example, such follow-up research may help in the determination of the extent to which those
who seemed to disengage from the program are action-oriented or generally opposed to
sedentary activities. Equipped with such information, it might be possible to tailor these

94
exercises in such a way that no participants disengage. However, without such research, a certain
amount of disengagement from the study might need to be expected.
Future studies may recruit larger samples so as to increase the likelihood of a wider
demographic diversity and add statistical significance to those correlative findings linking certain
baseline stress scores, for example, with media preferences or demographic differences. Such
information might help to guide educational or clinical interventions aimed at addressing the
impact of a given type of media or at targeting particular portions of the adolescent population.
This type of information might also guide further iterations of Media Assisted forms of
clinical treatment that might be used to address specific psychological or emotional conditions or
certain deficits associated with a particular group. In this manner, Media Assisted forms of
treatment might be designed to exploit the Media Practice Model directly, by uncovering what
unique experiences, motivations, or expectations played into the clinical efficacy of a particular
form of media (Steele & Brown, 1995).
Lastly, the present study serves as a touchstone for studies aimed at introducing
transpersonal techniques, such as yoga, mindfulness, and group meditation, into the school
curriculum. With the prevalence of stress in the lives of contemporary adolescents, the need to
implement exercises like those explored in the present research continues to increase. Future
research exploring the benefits of relaxation in the school setting may serve as precursors for
transpersonally oriented practices. While the initial steps may be small and tentative at first, the
hope is that, with the accumulation of studies examining the benefits of relaxation among
teenagers, there will be a wider acceptance of such practices and a deeper appreciation for the
benefits of living with moderated levels of stress.

95
References
Allen, K., Blascovich, J., & Mendes, W. B. (2002). Cardiovascular reactivity in the presence of pets, friends, and spouses: The truth about cats and dogs. Psychosomatic Medicine, 64(5), 727-739.
Alperin, R. J. (2005). Young children and disturbed eating attitudes and behaviors: Relationships
with parents, peers, media, and body image. Dissertation Abstracts International, 65, 7- B. (UMI No. AAI3141034)
Anderson, C. A., Berkowitz, L., Donnerstein, E., Huesmann, L. R., Johnson, J. D., Linz, D. et al. (2003). The influence of media violence on youth. Psychological Science in the Public Interest, 4(3), 81-110.
Anderson, C. A., & Dill, K. E. (2000). Video games and aggressive thoughts, feelings, and behavior in the laboratory and in life. Journal of Personality and Social Psychology, 78(4), 772-790. Bandura, A., Ross, D., & Ross, S. A. (1963). Imitation of film-mediated aggressive models. The Journal of Abnormal and Social Psychology, 66(1), 3-11. Barr, R. G., Boyce, W. T., & Zeltzer, L. K. (1996). The stress-illness association in children: A perspective from the biobehavioral interface. New York: Cambridge University Press. Benson, H. (1977). Systemic hypertension and the relaxation response. New England Journal of Medicine, 296(20), 1152-1156. Benson, H. (1983). The relaxation response: Its subjective and objective historical precedents and physiology. Trends in Neurosciences, 6(7), 281-284. Benson, H., Arns, P. A., & Hoffman, J. W. (1981). The relaxation response and hypnosis.
International Journal of Clinical and Experimental Hypnosis, 29(3), 259-270. Benson, H., Beary, J. F., & Carol, M. P. (1974). The relaxation response. Psychiatry: Journal for the Study of Interpersonal Processes, 37(1), 37-46. Benson, H., Wilcher, M., Greenberg, B., Huggins, E., Ennis, M., Zuttermeister, P. C. et al. (2000). Academic performance among middle-school students after exposure to a relaxation response curriculum. Journal of Research & Development in Education, 33(3), 156-165.
Berg-Cross, L., Jennings, P., & Baruch, R. (1990). Cinematherapy: Theory and application. Psychotherapy in Private Practice, 8(1), 135-156.
96
Bickham, D. S., Vandewater, E. A., Huston, A. C., Lee, J. H., Caplovitz, A. G., & Wright, J. C. (2003). Predictors of children’s electronic media use: An examination of three ethnic groups. Media Psychology, 5(2), 107-137.
Blanchard, E. B., & Turner, S. M. (2000). Anxiety and its management in irritable bowel syndrome. Needham Heights, MA: Allyn & Bacon. Boersma, F. J., & Gagnon, C. (1992). The use of repetitive audiovisual entrainment in the
management of chronic pain. Medical Hypnoanalysis Journal, 7(3), 80-97. Braud, W., & Anderson, R. (1998). Transpersonal research methods for the social sciences: Honoring human experience. Thousand Oaks, CA: Sage. Brown, J. D. (2005). Emerging adults in a media-saturated world. Washington, DC: American Psychological Association. Brown, J. D. (2006). Media literacy has potential to improve adolescents’ health. Journal of Adolescent Health, 39(4), 459-460. Brown, J. D., & Walsh-Childers, K. (2002). Effects of media on personal and public health. Mahwah, NJ: Lawrence Erlbaum. Buwalda, K. L. (2004). An exploratory case study examining the effects of watching an
aggressive video on displayed levels of imitated and unique aggression in two contexts. Dissertation Abstracts International, 64, 10-B. (UMI No. AAI3107819)
Byrnes, S. R. (1996). The effect of audio, video, and paired audio-video stimuli on the
experience of stress. Journal of Music Therapy, 33(4), 248-260. Cannon, W. B. (1914). The interrelations of emotions as suggested by recent physiological researches. American Journal of Psychology, 25(2), 256-282. Chafin, S., Roy, M., Gerin, W., & Christenfeld, N. (2004). Music can facilitate blood pressure recovery from stress. British Journal of Health Psychology, 9(3), 393-403. Chalder, T., Cleare, A., & Wessely, S. (2000). The management of stress and anxiety in chronic fatigue syndrome. Needham Heights, MA: Allyn & Bacon. Cohen, J. (1987). Statistical power analysis for the behavioral sciences (Rev. ed.). Hillsdale, NJ: Lawrence Erlbaum. Cohen, S. (2002). Psychosocial stress, social networks, and susceptibility to infection. New York: Oxford University Press. Cohen, S., Tyrrell, D. A., & Smith, A. P. (1991). Psychological stress and susceptibility to the common cold. New England Journal of Medicine, 325(9), 606-612.

97
Compas, B. E. (1987). Coping with stress during childhood and adolescence. Psychological Bulletin, 101(3), 393-403. Compas, B. E., Connor-Smith, J. K., Saltzman, H., Thomsen, A. H., & Wadsworth, M. E.
(2001). Coping with stress during childhood and adolescence: Problems, progress, and potential in theory and research. Psychological Bulletin, 127(1), 87-127.
Compas, B. E., Orosan, P. G., & Grant, K. E. (1993). Adolescent stress and coping: Implications for psychopathology during adolescence. Journal of Adolescence. Special Issue: Stress and coping in adolescence, 16(3), 331-349. Comstock, G., & Scharrer, E. (2006). Media and popular culture. Hoboken, NJ: John Wiley & Sons. Copeland, M. E. (2001). Wellness recovery action plan: A system for monitoring, reducing and
eliminating uncomfortable or dangerous physical symptoms and emotional feelings. New York: Haworth Press.
Craig, A., Tran, Y., McIsaac, P., Moses, P., Kirkup, L., & Searle, A. (2000). The effectiveness of activating electrical devices using alpha wave synchronization contingent with eye closure. Applied Ergonomics, 31(4), 377-382. Creswell, J. W. (1994). Research design: Qualitative & quantitative approaches. Thousand Oaks, CA: Sage. Cropley, M., Ussher, M., & Charitou, E. (2007). Acute effects of a guided relaxation routine
(body scan) on tobacco withdrawal symptoms and cravings in abstinent smokers. Addiction, 102(6), 989-993.
Csikszentmihályi, M., & Schneider, B. (2000). Becoming adult: How teenagers prepare for the world of work. New York: Basic Books. Darwish, A. M. (2002). The effects of viewing media violence on aggressive behavior: A theoretical perspective. Dissertation Abstracts International, 62, 11-B. (UMI No. AAI3034533) Deckro, G. R., Ballinger, K. M., Hoyt, M., Wilcher, M., Dusek, J., Myers, P. et al. (2002). The evaluation of a mind/body intervention to reduce psychological distress and perceived stress in college students. Journal of American College Health, 50(6), 281-287. DeSchriver, M., & Riddick, C. (1990). Effects of watching aquariums on elders’ stress. Anthrozoös, 4(1), 44-48. Desmond, R., & Carveth, R. (2007). The effects of advertising on children and adolescents: A meta-analysis. Mahwah, NJ: Lawrence Erlbaum.

98
Direct Source (Producer). (2006). Mind, body, spirit: Simply relax [Motion picture]. (Available from Direct Source Special Products, 2695 Dollard Street, LaSalle, QC, Canada, H8N 2J8) Dixon, W. A., Rumford, K. G., Heppner, P. P., & Lips, B. J. (1992). Use of different sources of stress to predict hopelessness and suicide ideation in a college population. Journal of Counseling Psychology, 39(3), 342-349. dosReis, S., Zito, J. M., Safer, D. J., Gardner, J. F., Puccia, K. B., & Owens, P. L. (2005).
Multiple psychotropic medication use for youths: A two-state comparison. Journal of Child and Adolescent Psychopharmacology. Special Issue on Psychopharmacoepidemiology, 15(1), 68-77.
Erikson, E. H. (1950). Childhood and society. Oxford, England: Norton. Erikson, E. H. (1968). Identity: Youth and crisis. Oxford, England: Norton. Farnill, D., & Robertson, M. F. (1990). Sleep disturbance, tertiary-transition stress, and
psychological symptoms among young first-year Australian college students. Australian Psychologist, 25(2), 178-188.
Ferguson, C. J. (2007). Evidence for publication bias in video game violence effects literature: A meta-analytic review. Aggression and Violent Behavior, 12(4), 470-482. Fischoff, S. (2005). Media psychology: A personal essay in definition and purview. Journal of
Media Psychology, 10(1). Retrieved March 10, 2007, from http://www.calstatela.edu/faculty/sfischo/MEDIADEF-2.html
Freud, S. (2004). Studies in hysteria. New York: Penguin Press. (Original work published 1895) Friedmann, E., Thomas, S. A., & Eddy, T. J. (2000). Companion animals and human health: Physical and cardiovascular influences. New York: Cambridge University Press. Frydenberg, E., & Lewis, R. (2004). Adolescents least able to cope: How do they respond to their stresses? British Journal of Guidance & Counseling, 32(1), 25-37. Gibbons, R. D., Hur, K., Bhaumik, D. K., & Mann, J. J. (2006). The relationship between
antidepressant prescription rates and rate of early adolescent suicide. American Journal of Psychiatry, 163(11), 1898-1904.
Halgren, E. (1992). Emotional neurophysiology of the amygdala within the context of human cognition. In J. P. Aggleton (Ed.), The amygdala: Neurobiological aspects of emotion, memory, and mental dysfunction (pp. 191-229). New York: Wiley-Liss. Hampel, P., & Petermann, F. (2005). Age and gender effects on coping in children and
adolescents. Journal of Youth and Adolescence, 34(2), 73-83.
99
Hampel, P., & Petermann, F. (2006). Perceived stress, coping, and adjustment in adolescents. Journal of Adolescent Health, 38(4), 409-415. Harrison, K. (2006). Scope of self: Toward a model of television’s effects on self-complexity in adolescence. Communication Theory, 16(2), 251-279. Hurrelmann, K., & Raithel, J. (2005). Risk behavior in adolescence: The relationship between developmental and health problems. International Journal of Adolescence and Youth, 12(4), 281-299. Hutchinson, S. L., Baldwin, C. K., & Oh, S. (2006). Adolescent coping: Exploring adolescents’ leisure-based responses to stress. Leisure Sciences, 28(2), 115-131. Jacobs, G. D., Benson, H., & Friedman, R. (1996). Topographic EEG mapping of the relaxation response. Biofeedback & Self Regulation, 21(2), 121-129. Jacobson, E. (1925). Progressive relaxation. American Journal of Psychology, 36, 73-87. Jacobson, E. (1934). You must relax. Oxford, England: Whittlesey House. Jacobson, E. (1970). Psychology and the integrative action of the nervous system. Acta
Symbolica, 1(2), 31-35. Jarvis, M. (2002). Smoking and stress. Williston, VT: BMJ Books. Johnson, P., Buboltz, W. C., Jr., & Seemann, E. (2003). Ego identity status: A step in the
differentiation process. Journal of Counseling & Development, 81(2), 191-195. Keefer, L., & Blanchard, E. B. (2001). The effects of relaxation response meditation on the symptoms of irritable bowel syndrome: Results of a controlled treatment study.
Behaviour Research and Therapy, 39(7), 801-811. Kelly, C. R., Grinband, J., & Hirsch, J. (2007). Repeated exposure to media violence is
associated with diminished response in an inhibitory frontolimbic network. Retrieved January 10, 2008, from http://www.plosone.org/article/
Klein-Hessling, J., & Lohaus, A. (2002). Benefits and interindividual differences in children’s responses to extended and intensified relaxation training. Anxiety, Stress, & Coping: An International Journal, 15(3), 275-288. Kraag, G., Zeegers, M. P., Kok, G., Hosman, C., & Abu-Saad, H. H. (2006). School programs targeting stress management in children and adolescents: A meta-analysis. Journal of School Psychology, 44(6), 449-472.

100
Krout, R. E. (2007). Music listening to facilitate relaxation and promote wellness: Integrated aspects of our neurophysiological responses to music. The Arts in Psychotherapy, 34(2), 134-141. Kubey, R., & Csikszentmihályi, M. (1990). Television and the quality of life: How viewing shapes everyday experience. Hillsdale, NJ: Lawrence Erlbaum. Kwekkeboom, K. L., & Gretarsdottir, E. (2006). Systematic review of relaxation interventions for pain. Journal of Nursing Scholarship, 38(3), 269-277. La Ferle, C., Edwards, S. M., & Lee, W. (2000). Teens’ use of traditional media and the internet. Journal of Advertising Research, 40(3), 55-65. Landeck, K. (2004). Lernförderung durch photostimulation.[promotion of learning through photic stimulation]. Psychologie in Erziehung und Unterricht, 51(3), 221-233. Lang, A., Zhou, S., Schwartz, N., Bolls, P. D., & Potter, R. F. (2000). The effects of edits on arousal, attention, and memory for television messages: When an edit is an edit can an edit be too much? Journal of Broadcasting and Electronic Media, 44(1), 94-109. Lazarus, R. S. (2007). Stress and emotion: A new synthesis. Westport, CT: Praeger/Greenwood. Lazarus, R. S., & Folkman, S. (1984). Stress, appraisal, and coping. New York: Springer. Lehmann, J. W., Goodale, I. L., & Benson, H. (1986). Reduced papillary sensitivity to topical phenylephrine associated with the relaxation response. Journal of Human Stress, 12(3), 101-104. L’Engle, K. L., Brown, J. D., & Kenneavy, K. (2006). The mass media are an important context for adolescents’ sexual behavior. Journal of Adolescent Health, 38(3), 186-192. Levy, M., & Windahl, S. (1985). The concept of audience activity. In K. E. Rosengren, P.
Palmgreen, & L. Wenner (Eds.), Media gratification research: Current Perspectives (109-122). Beverly Hills, CA: Sage.
Lohaus, A., Ball, J., Klein-Hessling, J., & Wild, M. (2005). Relations between media use and self-reported symptomatology in young adolescents. Anxiety, Stress & Coping: An International Journal, 18(4), 333-341. Lohaus, A., & Klein-Hessling, J. (2003). Relaxation in children: Effects of extended and
intensified training. Psychology & Health, 18(2), 237-249. Lohaus, A., Klein-Hessling, J., & Shebar, S. (1997). Stress management for elementary school children: A comparative evaluation of different approaches. European Review of Applied Psychology, 47(2), 157-162.

101
Macleod, J., Oakes, R., Oppenkowski, T., Stokes-Lampard, H., Copello, A., Crome, I. et al. (2004). How strong is the evidence that illicit drug use by young people is an important cause of psychological or social harm? Methodological and policy implications of a systematic review of longitudinal, general population studies. Drugs: Education, Prevention & Policy, 11(4), 281-297. Makros, J., & McCabe, M. P. (2001). Relationships between identity and self-representations during adolescence. Journal of Youth and Adolescence, 30(5), 623-639. Marcia, J. E. (1966). Development and validation of ego-identity status. Journal of Personality and Social Psychology, 3(5), 551-558. Marcia, J. E. (1980). Identity in adolescence. In J. Adelson (Ed.), Handbook of adolescent psychology (pp. 159-187). New York: John Wiley & Sons. Masterpasqua, F. (2005). Changing brainwaves in psychological practice. Washington, DC: American Psychological Association. McCraty, R., Atkinson, M., Tomasino, D., Goelitz, J., & Mayrovitz, H. N. (1999). The impact of an emotional self-management skills course on psychosocial functioning and autonomic recovery to stress in middle school children. Integrative Physiological & Behavioral Science, 34(4), 246-268. McNamara, S. (2000). Stress in young people: What’s new and what can we do? New York: Continuum. Münsterberg, H. (1916). The photo-play: A psychological study. Oxford, England: Appleton. Nastasi, B. K., Hitchcock, J. H., Burkholder, G., Varjas, K., Sarkar, S., & Jayasena, A. (2007). Assessing adolescents’ understanding of and reactions to stress in different cultures: Results of a mixed-methods approach. School Psychology International, 28(2), 163- 178. Nelson, M. R., & McLeod, L. E. (2005). Adolescent brand consciousness and product
placements: Awareness, liking and perceived effects on self and others. International Journal of Consumer Studies, 29(6), 515-528.
Orr, P. P. (2006). A documentary film project with first-year art therapy students. The Arts in Psychotherapy, 33(4), 281-287. Palys, T. S. (1986). Testing the common wisdom: The social content of video pornography. Canadian Psychology/Psychologie Canadienne, 27(1), 22-35. Paul, G. L., & Trimble, R.W. (1970). Recorded vs. “live” relaxation training and hypnotic suggestion: Comparative effectiveness for reducing physiological arousal and inhibiting stress response. Behavior Therapy, 1(3), 285-302.

102
Pelletier, C. L. (2004). The effect of music on decreasing arousal due to stress: A meta-analysis. Journal of Music Therapy, 41(3), 192-214. Peralta-Ramírez, M. I., Jiménez-Alonso, J., Godoy-García, J. F., Perez-García, M., & The Group Lupus Virgen De Las Nieves. (2004). The effects of daily stress and stressful life events on the clinical symptomatology of patients with lupus erythematosus. Psychosomatic Medicine, 66(5), 788-794. Persky, S., & Blascovich, J. (2007). Immersive virtual environments versus traditional platforms: Effects of violent and nonviolent video game play. Media Psychology, 10(1), 135-156. Piaget, J. (1972). Intellectual evolution from adolescence to adulthood. Human Development, 15(1), 1-12. Piiparinen, R. A., & Smith, J. C. (2003). Stress symptoms of two groups before and after the terrorist attacks of 9/11/01. Perceptual and Motor Skills, 97(2), 360-364. Piiparinen, R. A., & Smith, J. C. (2004). Stress symptoms one year after 9/11/01: A follow- up. Perceptual and Motor Skills, 99(2), 577-580. Primack, B. A., Gold, M. A., Land, S. R., & Fine, M. J. (2006). Association of cigarette smoking and media literacy about smoking among adolescents. Journal of Adolescent Health, 39(4), 465-472. Putman, J. (2000). The effects of brief, eyes-open alpha brain wave training with audio and video relaxation induction on the EEG of 77 army reservists. Journal of Neurotherapy, 4(1), 17-28. Reeves, B., & Thorson, E. (1986). Watching television: Experiments on the viewing process. Communication Research, 13(3), 343-361. Rietveld, S., Beest, I. V., & Everaerd, W. (1999). Stress-induced breathlessness in asthma. Psychological Medicine, 29(6), 1359-1366. Riva, G. (2003). Virtual environments in clinical psychology. Psychotherapy: Theory, Research, Practice, & Training, 40(1), 68-76. Robar, D. E. (1978). The comparative effectiveness of live, videotaped and audiotaped group relaxation training on the ability to reduce physiological arousal and self-report measures of anxiety. Dissertation Abstracts International, 39, 5B. Robb, S. L. (2000). Music assisted progressive muscle relaxation, music listening, and silence: A comparison of relaxation techniques. Journal of Music Therapy, 37(1), 2-21. Roberts, D. F., Henriksen, L., & Foehr, U. G. (2004). Adolescents and media. Hoboken, NJ: John Wiley & Sons.

103
Rubin, A. M. (2002). The uses-and-gratifications perspective of media effects. Mahwah, NJ: Lawrence Erlbaum. Sadava, S. W., & Pak, A. W. (1993). Stress-related problem drinking and alcohol problems: A longitudinal study and extension of Marlatt’s model. Canadian Journal of Behavioral Science, 25(3), 446-464. Salazard, B., Casanova, D., Zuleta, J., Desouches, C., & Magalon, G. (2003) Auguste Lumière, pioneer of the modern civilization. Annales de Chirurgie Plastique et Esthetique, 48(3), 194-199. Salkind, N. J. (2000). Statistics for people who think they hate statistics. Thousand Oaks, CA: Sage. Scheufele, P. M. (2000). Effects of progressive relaxation and classical music on measurements of attention, relaxation, and stress responses. Journal of Behavioral Medicine, 23(2), 207- 228. Schwartz, J. E., Pickering, T. G., & Landsbergis, P. A. (1996). Work-related stress and blood
pressure: Current theoretical models and considerations from a behavioral medicine perspective. Journal of Occupational Health Psychology, 1(3), 287-310.
Segerstrom, S. C., & Miller, G. E. (2004). Psychological stress and the human immune system: A meta-analytic study of 30 years of inquiry. Psychological Bulletin, 130(4), 601-630. Segrin, C. (1999). Social skills, stressful life events, and the development of psychosocial
problems. Journal of Social & Clinical Psychology, 18(1), 14-34. Selye, H. (1950). The physiology and pathology of exposure to stress. Oxford, England: Acta. Selye, H. (1956). Stress and psychobiology. Journal of Clinical & Experimental
Psychopathology, 17, 370-375. Signorielli, N., & Kahlenberg, S. (2001). Television’s world of work in the nineties. Journal of Broadcasting & Electronic Media, 45(1), 4-22. Smith, J. C. (1990). Cognitive-behavioral relaxation training: A new system of strategies for treatment and assessment. New York: Springer. Smith, J. C. (1993). Creative stress management. Hoboken, NJ: Prentice-Hall. Smith, J. C. (Ed.). (2001). Advances in ABC relaxation: Applications and inventories. New York: Springer. Smith, J. C. (2005). Smith inventories and inventory packets. Retrieved March 10, 2008, from http://faculty.roosevelt.edu/jsmith/

104
Smith, J. C., Amutio, A., Anderson, J. P., & Aria, L. A. (1996). Relaxation: Mapping an uncharted world. Biofeedback & Self Regulation, 21(1), 63-90.
Smith, J. C., & Joyce, C. A. (2004). Mozart versus new age music: Relaxation states, stress, and
ABC relaxation theory. Journal of Music Therapy, 41(3), 215-224. Smith, J. C., Rausch, S. M., & Kettmann, J. D. J. (2004). Factor structure of the Smith Irrational Beliefs Inventory: Results of analysis on six independent samples. PsychologicalReports, 95(2), 696-704. Smith, J. C., Wedell, A. B., Kolotylo, C. J., Lewis, J., Byers, K. Y., & Segin, C. M. (2000). ABC relaxation theory and the factor structure of relaxation states recalled relaxation activities, dispositions, and motivations. Psychological Reports, 86(3, Pt2), 1201-1208. Smyth, J. M., Soefer, M. H., Hurewitz, A., & Stone, A. A. (1999). The effect of tape-recorded relaxation training on well-being, symptoms, and peak expiratory flow rate in adult asthmatics: A pilot study. Psychology & Health, 14(3), 487-501. Stacy, A. W., Zogg, J. B., Unger, J. B., & Dent, C. W. (2004). Exposure to televised alcohol ads and subsequent adolescent alcohol use. American Journal of Health Behavior, 28(6), 498-509. Steele, J. R., & Brown, J. D. (1995). Adolescent room culture: Studying media in the context of everyday life. Journal of Youth and Adolescence Special Issue: Adolescents’ uses of the media, 24(5), 551-576. Stone, A. A., Bovbjerg, D. H., Neale, J. M., & Napoli, A. (1992). Development of common cold symptoms following experimental rhinovirus infection is related to prior stressful life events. Behavioral Medicine, 18(3), 115-120. Taché, J., & Selye, H. (1985). On stress and coping mechanisms. Issues in Mental Health
Nursing. Special Issue: Stress and Anxiety, 7(1-4), 3-24. Tarnas, R. (1995) Prometheus the awakener: An essay on the archetypal meaning of the planet Uranus. Woodstock, CT: Spring. Thurstone, L. L. (1931). Influence of motion pictures on children’s attitudes. Journal of Social Psychology, 2, 291-305. Tiggemann, M. (2005). Television and adolescent body image: The role of program content and viewing motivation. Journal of Social & Clinical Psychology, 24(3), 361-381. Tolman, D. L., Kim, J. L., Schooler, D., & Sorsoli, C. L. (2007). Rethinking the associations between television viewing and adolescent sexuality development: Bringing gender into focus. Journal of Adolescent Health, 40(1), e9-e16.

105
Trierweiler, S. J., Nagata, D. K., & Banks, J. V. (2000). The structure of interpretations in family therapy: A video-enhanced exploration. Family Process, 39(2), 189-205. Tsai, S. (2004). Audio-visual relaxation training for anxiety, sleep, and relaxation among
Chinese adults with cardiac disease. Research in Nursing & Health, 27(6), 458-468. Tsigos, C., & Chrousos, G. P. (2002). Hypothalamus-pituitary axis, neuroendocrine factors and stress. Journal of Psychosomatic Research: Special Issue: Depression and Mental Disorders and Diabetes, Renal Disease, and Obesity and Nutritional Disorders, 53(4), 865-871. Uchino, B. N., Smith, T. W., Holt-Lunstad, J., Campo, R., & Reblin, M. (2007). Stress and illness. New York: Cambridge University Press. Ulett, G. A., Akpinar, S., & Itil, T. M. (1972). Hypnosis by video tape. International Journal of Clinical and Experimental Hypnosis, 20(1), 46-51. Wagner, C., Abela, J. R. Z., & Brozina, K. (2006). A comparison of stress measures in children and adolescents: A self-report checklist versus an objectively rated interview. Journal of Psychopathology and Behavioral Assessment, 28(4), 251-261. Wallace, R. K., & Benson, H. (1972). The physiology of meditation. Scientific American, 226(2), 84-90. Ward, L. M., Gorvine, B., & Cytron-Walker, A. (2002). Would that really happen? Adolescents’ perceptions of sexual relationships according to prime-time television. Mahwah, NJ: Lawrence Erlbaum. Washburn-Ormachea, J. M., Hillman, S. B., & Sawilowsky, S. S. (2004). Gender and gender- role orientation differences on adolescents’ coping with peer stressors. Journal of Youth and Adolescence, 33(1), 31-40. Wells, D. L. (2005). The effect of videotapes of animals on cardiovascular responses to stress. Stress and Health: Journal of the International Society for the Investigation of Stress, 21(3), 209-213. Wilkins, E. G., Lowery, J. C., Copeland, L. A., Goldfarb, S. L., Wren, P. A., & Janz, N. K. (2006). Impact of an educational video on patient decision making in early breast cancer treatment. Medical Decision Making, 26(6), 589-598. Windle, M. (1992). A longitudinal study of stress buffering for adolescent problem behaviors. Developmental Psychology, 28(3), 522-530. Wittrock, D. A., & Foraker, S. L. (2001). Tension-type headache and stressful events: The role of selective memory in the reporting of stressors. Headache, 41(5), 482-493.

106
Wood, A. V. (1986). Hypnosis and audio tapes as a treatment for agoraphobia. Australian Journal of Clinical Hypnotherapy and Hypnosis, 7(2), 100-104.
Zautra, A. J., & Smith, B. W. (2001). Depression and reactivity to stress in older women with rheumatoid arthritis and osteoarthritis. Psychosomatic Medicine, 63(4), 687-696. Zeisset, R. M. (1968). Desensitization and relaxation in the modification of psychiatric patients’ interview behavior. Journal of Abnormal Psychology, 73(1), 18-24.

107
Appendix A: Informed Consent
To the Research Participant and the Parents or Guardians of Research Participants: You have been invited to participate in a study to explore the effects of guided relaxation. For this study, you will meet for a total of three separate 15-minute sessions at the high school. During each of these meetings, you will be asked to fill out a brief questionnaire about who you are and how much stress you are under. You will then receive a brief 10-minute guided relaxation exercise. The school administration and your teachers have all been notified of this study and are in support of your participation given your and your parent’s consent. The school has made accommodations with regard to scheduling and class assignments.
For the preservation of privacy, all information provided by you will be kept completely confidential as to its source and identity. To this end, you will be given a confidential numeric code so as to protect your identity. The master list of names and corresponding numeric codes will be kept in a locked file box. The completed questionnaires will be kept in a separate locked file box. These locked file boxes will only be accessed by the researcher and will be kept in the researcher’s secure office. In the event that any information is used in published material, please know that information that may identify you will be altered so as to ensure all parties’ complete anonymity. Guided relaxation has been repeatedly shown to be generally pleasant and beneficial for most people who make use of it. The program used in this study has served as an effective way of regulating and managing most minor forms of stress, such as the kind that arises from academic or performance-related issues or from minor conflicts with family or friends. It has also been demonstrated to be an effective way of managing the discomfort associated with tension and pain. Although few studies of this program have been performed with teenagers to date, existing research suggests that those children who choose to participate in this study and who continue its practice upon its completion will receive many of the same benefits with which it has been associated. Overall, the program is generally pleasant and provides a valuable skill that, with repeated use, can offer you many lasting and positive benefits. While I have expressly designed this study to minimize any potential risks that may arise from this program, all of the many possible reactions can not be fully addressed. For example, some individuals may be sensitive to test-taking, so the completion of any pencil-and-paper questionnaire in a classroom-type setting may potentially evoke some feelings of uneasiness. Be advised that the completion of this questionnaire will not influence your academic grades. Secondly, in some rare instances, participants in a guided relaxation program may experience feelings of stress or discomfort rather than the expected feelings of well-being. Please be assured that, as the researcher of this study with specialized clinical training with teens, I will be in the room with you at all times during the program and if, at any point, I observe any distress or discomfort, I pledge to call a halt to the session immediately and take all of the appropriate steps to ensure all participant’s well-being. If, in the rare instance, any aspect of this program is deemed to be too upsetting to you during or following your involvement, referrals for counseling are available for ongoing support.
If, at any time, you have any questions or concerns, I will make every effort to discuss them with you and inform you of the options available to you for resolving your concerns. You are encouraged call me collect at (xxx) xxx-xxxx, or my Dissertation Chairperson, Patricia Campbell, PsyD., at (xxx) xxx-xxxx, or the head of the Ethics Committee at the Institute for
108
Transpersonal Psychology, Frederic Luskin, Ph.D., at (xxx) xxx-xxxx, ext. xxx. If you decide to participate in this research, you may withdraw your consent and discontinue participation at any time during the conduct of this study and for any reason without penalty or prejudice. A brief statement of the conclusions of the study will be made available for all interested parties. The statement will include the conclusions found from the information collected during the course of the study. You may request a summary of the findings of this research by providing your mailing address in the designated area below your signature.
By signing below, you are acknowledging that you have read and understood this consent form and have had the study explained to you and have had any questions about this research answered to your satisfaction. You are also acknowledging that your participation in this research is entirely voluntary and that no coercion has been applied to encourage such participation. Your signature below indicates your willingness to participate in this research. Thank you kindly for your attention. _____________________________________________ __________________ Participant’s Name (please print clearly) Date _____________________________________________ __________________ Participant’s Signature Date _____________________________________________ __________________ Parent’s Signature Date _____________________________________________ __________________ Researcher’s Signature Date Mailing Address (if you wish a summary of the research findings mailed to you): ______________________________________________________________________________________ Name of Participant and/or Participant’s Parent or Guardian ______________________________________________________________________________________ Street Address City ______________________________________________________________________________________ State Zip Code Country
_____________________________________________ __________________ Researcher’s Signature Date Daniel L. Gaylinn, MA Mailing Address: Mailing address E-mail: E-mail address

109
Appendix B: Demographic Questionnaire
INSTRUCTIONS: Your honest answer to EACH item is very important. Please CIRCLE the response which is most true for you. 1. Age: (a) 14 (b) 15 2. Grade: (a) 9th (b) 10th
(c) 16 (d) 17 (c) 11th (d) 12th
(e) 18 3. Gender: (a) Male 4. Primary Language: (a) English (b) Female (b) Other: ______________
(please indicate) 5. Ethnicity: (a) Caucasian (b) Latin/Hispanic (c) African American (d) Asian (e) Bimultiracial (f) Other: ____________________
(please indicate) 6. What is your level of academic performance (on average)?:
(a) A’s: Better than 90% (b) B’s: 80-90% (c) C’s: 70-80% (d) D’s: 60-70% (e) F’s: Worse than 60%
7. What is your best estimate of your family’s annual income (on average)?:
(a) More than $100 Thousand (b) Between $75 and $100 Thousand (c) Between $50 and $75 Thousand (d) Between $25 and $50 Thousand (e) Less than $25 Thousand (f) Don’t Know
8. How much experience would you say you have with relaxation techniques (e.g., progressive muscle relaxation, breathing techniques, meditation, etc.)?: (a) More Than 5 Months (b) Between 3 and 5 Months (c) Less Than 3 Months (d) None At All 9. When you want to relax, what do you frequently tend to do?
(a) Music (b) Videos/Movies (c) Books (d) Friends (e) Videogames (f) Other: ______________
(please describe on reverse side of page)
10. How much time do you generally spend with various forms of electronic media (e.g., television, movies, videogames, radio, music) each day? (a) More Than 5 Hours (b) Between 3 and 5 Hours (c) Less Than 3 Hours (d) None At All 11. When you do use electronic media, what do you use most often? (a) Music (b) Television (c) Movies (d) Internet (e) Videogames (f) Other: ____________________
(please describe on reverse side of page)

110
Appendix C: Smith Stress Symptoms Inventory-State (SSSI-S)
The statements in this scale are about how you feel right now at the present moment. Although some of the statements are similar to one another, there are differences between them and you should treat each one separately. For each statement, please indicate the extent to which it fits how you are feeling right now at the present moment by circling one of the numbers corresponding with one of the following options: 1 = Doesn’t fit me at all; 2 = Fits me a little; 3 = Fits me moderately well; 4 = Fits me very well 1. I have a nervous stomach. 1 2 3 4 2. I am easily distracted. 1 2 3 4 3. I feel like I am losing my memory and forgetting things. 1 2 3 4 4. I feel like I am losing sleep. 1 2 3 4 5. I worry too much about things that do not really matter. 1 2 3 4 6. My breathing is hurried, shallow, or uneven. 1 2 3 4 7. I have conflicts with others. 1 2 3 4 8. I find myself thinking in narrow, rigid ways. 1 2 3 4 9. My heart is beating fast, hard, or irregularly. 1 2 3 4 10. I have difficulty controlling negative thoughts. 1 2 3 4 11. I feel distressed (discouraged or sad). 1 2 3 4 12. I have lost my appetite. 1 2 3 4 13. I am depressed. 1 2 3 4 14. I am anxious. 1 2 3 4 15. I feel distaste or disgust. 1 2 3 4 16. I feel cynical or hostile. 1 2 3 4 17. My shoulders, neck, or back are tense. 1 2 3 4 18. I have difficulty keeping troublesome thoughts out of mind. 1 2 3 4 19. I feel confused. 1 2 3 4 20. My muscles feel tight, tense, or clenched up (furrowed brow, tightened fist, clenched jaw). 1 2 3 4 21. I feel less sensitive or caring to others. 1 2 3 4 22. I feel fatigued. 1 2 3 4 23. I have a backache. 1 2 3 4 24. I feel like I am losing my concentration. 1 2 3 4 25. I am afraid. 1 2 3 4 26. My mouth feels dry. 1 2 3 4 27. I feel like I might make mistakes. 1 2 3 4 28. I perspire or feel too warm. 1 2 3 4 29. I feel disorganized. 1 2 3 4 30. I feel the need to go to the rest room unnecessarily. 1 2 3 4 31. I find myself thinking unimportant, bothersome thoughts. 1 2 3 4 32. I have a headache. 1 2 3 4 33. I feel less cooperative with others. 1 2 3 4 34. I feel restless and fidgety. 1 2 3 4 35. I feel irritated or angry. 1 2 3 4

111
Appendix D: Reactions to an Experiential Exercise Scale (REES)
Your feedback on this exercise is kindly requested. Your responses will remain anonymous and are kept completely confidential and will only be used in the service of improving this program. Your honesty is greatly appreciated. The items in this scale measure a variety of states of mind associated with your reactions to the guided relaxation program you just experienced. For each statement, please circle the number that indicates the extent to which you agree with the statement describing your experience of the program. 1 = Strongly Disagree 2 = Disagree 3 = Slightly Disagree 4 = Slightly Agree 5 = Agree 6 = Strongly Agree 1. For me the exercise was not enjoyable. 1 2 3 4 5 6 2. I have no real desire to repeat this program. 1 2 3 4 5 6 3. The idea of doing this exercise regularly does not appeal to me. 1 2 3 4 5 6 4. During the exercise, I felt bored or restless. 1 2 3 4 5 6 5. I would rather not do this exercise again. 1 2 3 4 5 6 6. I enjoyed the exercise overall. 1 2 3 4 5 6 7. During the exercise, I felt focused or engaged. 1 2 3 4 5 6 8. I found the exercise enjoyable. 1 2 3 4 5 6 9. I would do this exercise again. 1 2 3 4 5 6 10. I felt the exercise was pleasant. 1 2 3 4 5 6 11. During the exercise, I had trouble staying focused. 1 2 3 4 5 6 12. I disliked the exercise overall. 1 2 3 4 5 6 13. I feel I would benefit from repeated use of the exercise. 1 2 3 4 5 6 14. During the exercise I felt absorbed or engrossed. 1 2 3 4 5 6 15. I found the program unpleasant. 1 2 3 4 5 6 16. During the exercise, I felt involved and interested. 1 2 3 4 5 6 17. During the exercise, I felt my mind wandering. 1 2 3 4 5 6 18. If I could do this exercise on a regular basis, I would. 1 2 3 4 5 6 19. During the exercise, my eyes were closed. 1 2 3 4 5 6 *20. You have now completed all three exercises. Please take as much space as you need to describe your experience with each of the three exercises and be sure to state which exercise(s) you enjoyed the most and least, and why?

112
Appendix E: Guided Relaxation Transcript
As you settle into a comfortable and relaxing position, allow the weight of your body to
relax into the support of the chair. Notice how your body makes contact with the chair. Relax the
back of your legs in your seat. . . . Relax the back of your hips. . . . Relax the back of your arms. .
. . Relax the back of your neck. . . . Relax the back of your head. Make any adjustments that you
may need to make, in order to relax your body into your chair more fully. Relax yourself into the
support of the chair, completely.
Relax the muscles of your face. Relax your eyes and your forehead. Relax your temples
and cheeks. Relax your mouth and your jaw. Relax your entire face. Place your hands on your
belly. Feel the rise and fall of your belly as you breathe. Notice each inhalation as it enters your
body, and each exhalation as it exits your body. Allow your breathing to become soft, full, and
easy. Without effort or strain. Simply allow the body to be breathed as you relax. As you inhale,
listen to the word “Let,” and as you exhale, listen to the word “Go.” Inhale, Let. Exhale, Go.
Continue to observe the natural rhythm of your breath, allowing your body to sink deeper
and deeper into relaxation. Allow your arms to rest comfortably by your side or in your lap. As
you exhale, feel any tension and strain leaving through your hands. As you inhale, feel any
tension, and as you exhale, let it go, soft and relaxed. Allow your body to sink deeper and deeper
into the support of the chair.
Now, bring your awareness to your feet. Feel the soles of your feet, and all ten of your
toes. Imagine that you could inhale and exhale through the soles of your feet. Imagine the breath
entering your body through the soles of your feet, and exiting your body through the soles of
your feet. Inhale, Let. Exhale, Go.

113
Now, bring your awareness back to your hands. Feel the back of your hands and the
palms of your hands and all ten fingers. Imagine you could inhale and exhale through the palms
of your hands. Imagine the breath entering the body through the palms of your hands, and exiting
the body through the palms of your hands. Inhale, Let. Exhale, Go.
Now, bring your awareness to your belly. Feel your belly rise and fall as you breathe.
Imagine that you could inhale and exhale through your navel, through your belly button. Imagine
your breath entering your body through your navel, and filling your belly with calm and relaxing
air. Imagine the breath exiting your body through your navel, taking with it any stress or strain
you may be holding. Inhale, Let. Exhale, Go.
Now, allow your mind to relax deeper, below the awareness of your breath. Allow your
mind to relax below the level of concentration on anything at all, including your breath. Allow
your body and mind to let go. Let go completely. [pause for several minutes to allow
participants to relax.]
Now bring your attention back to your breathing. Notice each inhalation as it enters your
body, and each exhalation as it exits your body. Bring your attention back to your belly and feel
the belly rise and fall with each and every breath. Allow your breathing to be soft, full, and easy.
Notice your entire body. Notice your entire body supported by the chair. Notice how easy it is to
be in your body, in this moment. Feeling calm, relaxed, and supported. When you are ready to
begin moving out of this relaxation process, you can begin by gently moving your fingers and
your toes. Allow some sensation to spread into your hands and feet. Stretch or move in any way
that feels good. Take your time, remain relaxed. Breathe easily. Take the best feeling of
relaxation with you.

114
Appendix F: Instructions for the Interventions
For the Video-Guided Relaxation Program (VGRP), the video of nature imagery will be
played on a DVD player connected to a television with a 36-inch screen or larger. Participants
will be asked to seat themselves in their assigned seats or in a place where they feel most
comfortable and have an unobstructed view of the screen. They will be instructed to follow along
with the guided relaxation program and to pay close attention to how the program makes them
feel. They will have the option of closing their eyes if they so choose, or leave them open in a
soft, unfocused gaze a few feet in front of them.
For the Audio-Guided Relaxation Program (AGRP), the audio tape will be identical to
the audio used for the VGRP. This tape will be played on an available stereo sound system so all
participants will comfortably hear the program clearly and easily. Participants will be asked to
seat themselves in their assigned seats or in a place where they feel most comfortable. They will
be instructed to follow along with the guided relaxation program and to pay close attention to
how the program makes them feel. They will have the option of closing their eyes if they so
choose, or leave them open in a soft, unfocused gaze a few feet in front of them.
For the Live-Guided Relaxation Program, the intervention will consist of the researcher
reading the same guided relaxation instructions used in both the VGRP and the AGRP in person
with a calm and soothing intonation. Participants will be asked to seat themselves in their
assigned seats or in a place where they feel most comfortable. They will be instructed to follow
along with the guided relaxation program and to pay close attention to how it makes them feel.
They will be given the option of closing their eyes or leaving them open in a soft, unfocused
gaze a few feet in front of them.

115
Appendix G: Permission to Screen Digital Video Disc
Dear Daniel L. Gaylinn, MA It gives us pleasures (sic) to allow you the use of the Mind Body and Spirit DVD titled Simply Relax for your research study. Sincerely, Tony Lacroix Manager, Home Video Product Development Direct Source Special Products Inc. Street Address City, Province Country, Zip Code tel xxx-xxx-xxxx ext. xxx fax xxx-xxx-xxxx e-mail address
Please consider the environment before printing this e-mailVeuillez considérer l’environnement avant d’imprimer ce courriel.

116
Appendix H: Pretreatment Talk Transcript
Thank you for your participation in today’s program. Please be sure that you are seated
comfortably, with your arms and legs uncrossed, and completely unobstructed by anything in
your immediate area. In a moment, I will ask you to follow along with a brief guided relaxation
exercise. Although you have the option of keeping your eyes open or closed throughout the
session, I invite you to keep your eyes open using a soft, unfocused gaze without attending to
anything in particular. This is to ensure that, while your body is relaxing, you will remain awake
throughout the session. As you allow your body to become relaxed, I invite you to follow along
with the instructions provided by the program, paying very close attention to how you feel in
your own body. Most people find relaxation exercises to be very beneficial and enjoyable,
especially when practiced over the course of several days. However, your experience is unique
and you are permitted to respond in any way that feels right and natural for you. If, during the
session, you experience any noises or distractions, I would like you to see if you can allow
anything short of a real emergency to simply help you to relax more deeply. During your
involvement with this program, you may feel the desire to share your experiences with others. I
would like to request that you please keep all of your thoughts and feelings of what you
experience here to yourself, making note of them in the questionnaires that you complete after
each session. On the final day of the study, you will be given the opportunity to share all of your
thoughts and feelings about your involvement in the study with me. You will then be free to
share your experiences here with others. Thank you again for your cooperation and for your
participation in today’s program. I would like to now invite you to follow along with this guided
relaxation exercise.
117
Appendix I: Reader / Transcriber Confidentiality Agreement
I, __________________________________________________, the Reader / Transcriber agree to:
• Keep all of the research information shared with me confidential by not discussing or sharing the research information in any form or format (e.g., disks, tapes, transcripts) with anyone other than the Researcher.
• Keep all research information in any form or format (e.g., disks, tapes, transcripts) secure
while it is in my possession.
• Return all research information in any form or format (e.g., disks, tapes, transcripts) to the Researcher when I have completed the research tasks.
• After consulting with the Researcher, erase or destroy all research information in any
form or format regarding this research project that is not returnable to the Researcher (e.g., disks, tapes, transcripts, information stored on a computer hard drive).
• Refrain from duplicating in part or in full any of the digital or written materials regarding
this research project (e.g., disks, tapes, transcripts). Reader / Transcriber __________________________ __________________________ _________ (print name) (signature) (date) Researcher __________________________ __________________________ _________ (print name) (signature) (date)

118
Appendix J: Relaxation Techniques Handout
1. Everyday Quick Techniques. a. Walk in nature; watch clouds in the sky, observe the wind. b. Put head down and close eyes for a few minutes. c. Rub hands together until warm; cup them over closed eyes. d. Vigorously shake your hands and arms for 10 seconds.
2. Six-Second Minirelaxation: The Quieting Reflex relieves muscle tightening, jaw
clenching, breath holding, and activation of sympathetic nervous system. For best results, practice Quieting Reflex frequently throughout the day, at the moment a stressful situation arises. With several months’ practice, this Quieting Reflex can become an automatic skill. It can be done with eyes opened or closed.
a. Become aware of what is annoying you (a sound, a comment, an urge, a thought, etc.). This becomes the cue to start the Quieting Reflex.
b. Repeat the phrase “Alert mind, calm body,” to yourself. c. Smile inwardly with eyes and mouth to prevent facial muscles from
displaying angry or fearful expressions. This is more a feeling than any observable expression.
d. Inhale slowly to the count of three, imagining that the breath comes in through the bottom of your feet. Then exhale slowly, feeling your breath move back down your legs and out through your feet. Allow your jaw, tongue, neck, and shoulder muscles to loosen.
3. Breathing: Changing your breathing can shift attention and mood. Breathing
patterns can reflect and redirect emotions a. Relax with belly breathing. All babies, some children, and some pets use
abdominal (belly or diaphragmatic) breathing. This is when your belly distends as you inhale and contracts as you exhale. As we grow up, many replace belly breathing with chest breathing—shallow, rapid breathing associated with tension and anxiety. Many take on the puffed chest, flat belly posture to impress, but this is not healthy.
i. Lay down on back on a comfortable surface. Knees may be bent, feet slightly apart. Loosen belt or constrictive clothing. Place hands just below navel. Close eyes, imagine a balloon inside your abdomen.
ii. As you inhale, imagine balloon is filling up with air, feel hands gently rise. As you exhale, imagine balloon deflating and feel hands gently fall.
iii. Focus on the sound and sensation of breathing as you relax. b. Quick tension relief
i. Reach for the sky or the ceiling as you inhale deeply and fully. Then exhale forcefully as you bend forward at the waist. Inhale deeply as you straighten up and reach. Repeat several times.
ii. Stand with arms straight in front of you. As you inhale, make several large backward circles with arms like a windmill. Then exhale, reverse

119
the direction of the circles. You can also alternately swing your arms, as if you were doing the backstroke.
c. Breathing with imagery: You can use mental images like warmth, coolness, vitality, peacefulness as you breathe. Imagine that your breath is charged with that particular quality. As you exhale, allow breath to carry that quality throughout your body as though you were exhaling through the entire surface of your skin. Below are some suggestions, but you can experiment with your own images.
i. Imagine inhaling warm, soothing air as you inhale, sending this soothing sensation throughout your body as you exhale.
ii. Imagine taking cool blue breaths if you feel warm. iii. See how it feels to inhale sparkling and energizing breaths. iv. Inhale heaviness to help settle and relax you. v. Direct the energy of your breath to certain areas of your body that feel
tense or pain to relax or heal that area.
4. Muscle Relaxation: People carry unnecessary tension in their muscles even though it may feel “normal” or “relaxed” to them. Learning to relax each muscle individually helps you to learn the difference between how it feels when your muscles are tense and when they are relaxed. It is based on the idea that whatever relaxes your body will also relax your mind. You can guide your friend through this process, you can have your friend guide you, or you can read the instructions into a tape recorder and play it for yourself. Daily practice will help to learn how to scan your body and pinpoint areas of tension that you can tense and then relax.
a. Find comfortable chair, supportive of head and neck or, lay down on a soft surface. Tense and relax muscle groups one at a time.
b. Tense each muscle group for about 5 seconds, concentrate on what tension feels like. The individual groups can be as follows:
i. Hands and Arms ii. Legs and Feet
iii. Abdomen and Buttocks iv. Chest, Back, and Shoulders v. Neck and Throat
vi. Head and Face vii. Your Entire Body
c. Breathe deeply. As you exhale, let go of all the tension as though an electrical current was suddenly turned off, so that all of your muscles go completely limp.
d. For 10 to 20 seconds, observe how it feels to have muscles that are tense as compared to ones that are relaxed.
e. Go through your body tensing and relaxing each muscle group twice. f. Leave time to notice the difference during the relaxation phase.
5. Mindfulness: Most people live on “automatic pilot,” either thinking about the past or
anticipating the future, while the present moment slips by barely noticed. Mindfulness involves keeping attention in the present moment, without judging it as
120
happy or sad, good or bad. It encourages living each moment—even painful ones—as fully and mindfully as possible. Mindfulness is an attitude toward living by calmly, consciously observing and accepting whatever happens, moment to moment. This may sound simple, but restless, judging minds make it surprisingly difficult. As a monkey jumps from branch to branch, our mind jumps from thought to thought. In mindfulness, you focus your mind on the present moment. The only moment we have is the present one and living it as fully aware as possible is what mindfulness is about, nurturing an inner balance of mind that enables you to respond to life situations with composure, clarity, and compassion. It reduces our tendency to react automatically. For example, the sound of someone’s voice (e.g., your mother’s, your teacher’s, your classmate’s) might trigger tension, anger, or fear. You can learn to mindfully observe this reaction to the voice without reacting or judging it. The “goal” is simply to observe—with no intention of changing or improving anything. People are positively changed by the practice of observing and accepting life as it is, with all its pleasures, pains, frustrations, disappointments, and insecurities. As you develop your capacity of mindfulness, you will become calmer, more confident, and better able to cope with whatever comes along:
a. Single-focused mindfulness: Sit comfortably on floor or in a chair, with back, neck, and head straight, but not stiff.
i. Concentrate on a single object, such as breathing. Focus attention on the feeling of the air as it passes in and out of nostrils with each breath. Do not attempt to control your breath, speeding it or slowing it. Simply observe it as it is.
ii. Even with attention focused solely on breath, your mind may wander to thoughts of other topics. As this occurs, observe that your mind has strayed, gently return attention to breathing.
iii. Each time a thought or feeling arises, acknowledge that breath has wandered, without analysis or judgment. Again, gently observe it, return attention to breath.
iv. Abandon thoughts of achieving some goal or having any special occurrence. Simply string moments of mindfulness together, breath by breath.
v. Practice this for 5 minutes at a time; gradually extend this period to 10, 20, or 30 minutes
Your thoughts are like waves on the surface of an ocean. Do not attempt to stop them to make the water flat, peaceful, or still. As you observe these waves, you begin to find relief from the turbulence and no longer get swept away easily.
Copeland, M.E. (2001). Wellness recovery action plan. New York: Haworth Press.