Gastritis final
57
-
Upload
aamir-sharif -
Category
Education
-
view
25 -
download
12
description
I m a student of BEMS 4th Professional at University of Poonch. Sir Asif teach us Pathology.
Transcript of Gastritis final


Gastritis
Aamir Sharif,
BEMS 4th ProfessionalDepartment of Eastern Medicine & Surgery
Presented By:

3
Stomach
3 muscle layers Oblique Circular Longitudinal
Regions Cardiac sphincter Fundus Antrum (pylorus) Pyloric sphincter
Vascular Inner surface thrown into folds – Rugae Contains enzymes that work best at pH 1-2

Normal Stomach Anatomy

Stomach - Normal

Stomach - Normal

7
Stomach
Functions Mix food Reservoir Start digestion of
Protein Nucleic acids Fats
Activates some enzymes Destroy some bacteria Makes intrinsic factor – B 12 absorption Destroys some bacteria
AbsorbsAlcoholWaterLipophilic acidB 12

InflammatoryDisease of Stomach
GASTRITIS

Definition The term gastritis is used to denote
inflammation associated with mucosal injury.
Gastritis is mostly a histological term that needs biopsy to be confirmed.
Gastritis is usually due to infectious agents (such as Helicobacter pylori) and autoimmune and hypersensitivity reactions.

Definition
Epithelial cell damage and regeneration without associated inflammation is properly referred to as "gastropathy.“
Gastropathy may be referred without histological evidence and just according to gross appearance in endoscopy or radiology
Gastropathy is usually caused by irritants such as drugs (e.g., nonsteroidal anti-inflammatory agents and alcohol), bile reflux, hypovolemia, and chronic congestion.

Sex:
Male-to-female ratio of gastritis is approximately1:1
Male-to-female ratio of PUD is approximately 2:1

Pathophysiology The mechanisms of mucosal injury in gastritis is thought
to be an imbalance of aggressive factors
acid production or pepsin
and defensive factors
mucus production bicarbonate and blood flow

Protective factors vs. hostile factors

Gastritis
Acute Chronic

Acute & Chronic Difference
Acute refers to short term inflammation Acute refering to neurophilic infiltrate
Chronic referring to long standing forms Chronic referring to mononuclear cell
infiltrate especially lymphocyte and macrophages

Acute Gastritis
Definition An acute mucosal inflammatory
process, with neutrophilic infiltrate, that is usually transient.
There may be hemorrhage into the mucosa or sloughing of the mucosa.
Severe erosive form is an important cause of severe GI bleeding

Etiology Frequently associated with, among others:
heavy use of NSAIDS, especially aspirinexcessive alcohol consumptionheavy smokingsevere stress e.g. trauma, burns,
surgeryIschemiaSystemic infection
Often, idiopathic

NSAIDs
NSAIDs and aspirin also interfere with the protective mucus layer by inhibiting mucosal cyclooxygenase activity, reducing levels of mucosal prostaglandins

Smoking
Promotes gastritis & ulcer occurrence Increases the likelihood of
ulcer complications
Mechanisms Stimulate gastric acid secretion Stimulate bile salt reflux Causes alteration in mucosal blood flow Decrease mucus secretion Reduces prostaglandin synthesis Decrease pancreatic bicarbonate secretion

Effects of Diet and Stress
Diet and Stress Action
Diet Dyspepsia, may pain - not believed to cause ulcer or assist healing
Physiologic stress
↓ mucosal blood flow, tissue hypoxia, mucosal lining degradation; e.g. ICU, sepsis, burn, trauma. Associated with multiple erosions & significant bleeding

Etiology of GastritisA) NormalB) Increased Attack *Hcl*Pepsin.*NSAIDs.
C) Weak defense *Helicobacter pylori
*Stress, drugs, smoking

Acute Gastritis - Pathogenesis
All above Factor Acid secretion+ back diffusion
+ Bicarbonatebuffer
+
Blood flow
Disruptionof
Mucus layer +
DirectMucosal
Injury
Acute Gastritis

Stages of Acute Gastritis
Acute superficial gastritis
Inflammation of superficial gastric
mucosa.
Acute erosive gastritis
Destruction of multiple small zones of
superficial mucosa.
Acute Gastric Ulceration
Destruction of full thickness of mucosa

Mucosal congestion ,edema inflammation & ulceration
ACUTE GASTRITIS - MORPHOLOGY

Acute Gastritis - MorphologyRanges from edema with neutrophil infiltration, vascular congestion,& an intact epithelium, to erosion (mucosal defect that does not cross the muscularis mucosa) and hemorrhage.

Acute Gastritis
Gastric mucosa demonstrates infiltration by Neutrophils

Acute Gastritis
diffusely hyperemic gastric mucosa
causes for acute gastritis alcoholism drugs infections, etc.

Acute Gastritis Clinical Features
broad range of signs and symptoms that depend on the severity of the condition
AsymptomaticEpigastric pain, nausea & vomitingHemorrhage, massive hematemesis, melena, or
fatal blood loss One of the major causes of massive
hematemesis, particularly in alcoholics. ~25% patients taking aspirin for rheumatoid
arthritis will develop acute gastritis, and some will bleed

Complications:
Malignancy
Hemorrhage
Perforation
Obstruction

Chronic Gastritis
Definition
Chronic mucosal inflammatory changes leading to atrophy and metaplasia (usually without erosions)
Dysplasia and ultimate neoplasia are complications.

Chronic Gastritis
Type B
Antral Gastritis
Type A
Autoimmune gastritis

Type B (Antral Gastritis)
90% of patients with antral chronic gastritis: Helicobacter pylori infected
Motile, gram negative curvilinear rods that elaborate urease (buffers gastric acid) & toxins and have adhesins to bind to the epithelium.
Pathogenesis H. pylori (urease NH4
+ + toxins) + Host (acid + peptic enzymes) Chronic Inflammation
Antibodies Gland destruction + Mucosal atrophy acid intrinsic factor (which can lead to pernicious anemia)

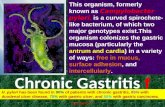
Helicobacter gastritis
2 patterns of infection Diffuse involvement of body and antrum (“pan
gastritis” associated with diminishing acid output)
Infection confined to antrum (antral gastritis, associate with increased acid output)

Helicobacter pylori
Adapted to live in association with surface epithelium beneath mucus barrier
Causes cell damage and inflammatory cell infiltration
In most countries the majority of adults are infected

H. pylori Gastritis - Morphology
Web Path
H. pylori organisms along superficial mucus layer of antral biopsy

Bile reflux gastropathy Bile reflux gastropathy typically results from the
regurgitation of bile into the stomach because of an operative stomach, an incompetent pyloric sphincter, or abnormal duodenal motility.
The effect of bile salts on gastric mucosa is comparable to that seen after chronic NSAID use

Chemical gastritis
Commonly seen with bile reflux (toxic to cells)
Prominent hyperplastic response (inflammatory cells scanty)
With time – intestinal metaplasia

Clinical Features
Usually only a few symptoms:
nausea, vomiting, upper abdominal discomfort
Most infected person have gastritis, but are asymptomatic
Hypochlorhydria, but NOT achlorhydria and pernicious anemia (parietal cells never completely destroyed)
Gastrin normal to slightly elevatedAntibiotics are treatment of choice

Clinical Complications
H. pyloriH. pylori predisposes to peptic ulcers
in duodenum and stomach—Most patients with a peptic ulcer are infected.
Risk of gastric carcinoma and lymphoma

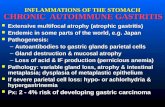
Type A (Auto immune)Etiology
Autoimmune - antibodies to parietal cells, gastrin receptor, intrinsic factor, and H+,K+ ATPase<10% of cases of chronic gastritisPossible autosomal dominant
inheritance

Morphology of chronic gastritis
Chronic inflammatory cell infiltration
Mucosal atrophy Intestinal (goblet cell)
metaplasia
Seen in Helicobacter and autoimmune gastritis (not chemical)

Autoimmune gastritis
Autoimmune gastritis - pernicious anemia
Chronic atrophic gastritis is associated with Ab’s
- intrinsic factor
- patietal cell bright green IF- in the
parietal cells of the gastric mucosa.

Autoimmune Gastritis -Morphology
PJ Goldblatt, MD
Diffuse mucosal damage of the body and fundic mucosa. Antrum less involved.

Clinical Features Usually only a few symptoms: nausea,
vomiting, upper abdominal discomfort
AutoimmuneHypo to achlorhydria (severe loss of
parietal glands)Hypergastrinemia10% have pernicious anemia
Chronic Gastritis

Clinical Complications
Autoimmune:Often seen in association with other
autoimmune disorders (Hashimoto thyroiditis, Addison disease, and type I diabetes)
Significant risk for the development of gastric carcinoma (2-4%) and endocrine tumors (carcinoid tumor)

Chronic GastritisMorphology
Varying degrees of mucosal damage possible
Mucosal lesions are reddened, with thickened rugae
Atrophied rugae in long-standing cases Lymphocytes and plasma cell infiltrate;
neutrophils indicate “active” inflammation (may or may not be present)

Regeneration - constant feature Metaplasia - mucosa of antral and
body-fundic regions converts to columnar absorptive cells and goblet cells (intestinal metaplasia)
Atrophy - marked loss of glands Dysplasia – precursor lesion to
gastric cancer in atrophic gastritis

Hypertrophic gastritis
Three variants are recognized
Menetrier’s disease
Hypersecretory gastropathy
Gastric gland hyperplasia
[the Zollinger-Ellison syndrome]

Hyperplastic gastropathies
proliferative, inflammatory, and infiltrative conditions are associated with large folds due to excessive number of mucosal epithelial cells

Ménétrier's disease Epithelial hyperplasia
involving the surface and foveolar mucous cells (i.e., foveolar hyperplasia); the oxyntic glands can be normal or atrophic.

Zollinger-Ellison syndrome
Increased numbers of parietal cells with no change in surface and foveolar mucous cells.

Hyperplastic gastropathies
mixed-type in which both mucous and oxyntic glandular cells show hyperplasia, may be seen in as lymphocytic and H. pylori gastritis.

Stomach Acute Gastritis= inflammation of gastric mucosa
acute – presence of neutrophils Chronic –lymphocytes and plasma cells
Caused by ingestion of strong acids or alkalies, NSAIDs, cancer chemotherapy, irradiation, alcohol, uremia, severe stress & shock states
Proposed mechanisms: ↑ acid production with ↓ surface bicarbonate buffer
Morphology: Mucosal edema, hyperemia, PML infiltration, erosions (not deeper than muscularis mucosa) & hemorrhages

Stomach Chronic Gastritis = Chronic mucosal inflammation Leading to mucosal atrophy, intestinal metaplasia &
dysplasia. Pathogenesis: Chronic infection by Helicobacter pylori (90%): MCC of
chronic gastritis, Elaboration of urease produces ammonia that buffers gastric acid, protecting organism from acid
Other diseases associated with H. pylori Infection Peptic ulcer disease Gastric carcinoma Gastric lymphoma
Autoimmunity (>10%): Antibodies to parietal cells cause parietal cell destruction (HCl & intrinsic factor)

Stomach Chronic Gastritis Morphology:
Autoimmune diffuse mucosal damage of the body-fundic mucosa H. pylori affect antral mucosa
Histology: Lymphocytic & plasma cell infiltrate of the lamina propria atrophy, regeneration, metaplasia (to intestinal type mucosa) &
dysplasia. H. pylori detected on the mucosal surface
Clinically: Mild abdominal discomfort, nausea, vomiting; hypochlorhydria,
hypergastrinemia & rarely Overt pernicious anemia (in autoimmune) gastritis).
Long-term risk of cancer is 2-4%