Gas Gangrene: Need for Aggressive Management in Delayed Presentation
2
Gas Gangrene: Need for Aggressive Management in Delayed Presentation Murugavaithianathan Pragatheeswarane, Nitesh Naga Balaji, Shyam Duvuru, and Sreenath Gubbi Shamanna G as gangrene is an anaerobic infection of skin and soft tissue characterized by the presence of gas under the skin produced by Clostridium spp. It is a potentially lethal condition that spreads quickly in soft tissues of the body. Tissue necrosis occurs because of the exotoxins produced by spore-forming bacteria that in turn produce gas in an envi- ronment of low oxygen [1]. Delay of surgery for more than 12 h is associated with higher overall morbidity [2]. Early amputation and prosthetic fitting is associated with decreased morbidity, fewer operations, shorter hospital course, de- creased hospital costs, and shorter rehabilitation time in cases of traumatic limb injury [3]. A 75-year-old farmer presented to our emergency depart- ment with a history of painful swelling in the right upper limb following impalement by an animal horn 4 d prior. On ex- amination, the patient had an altered sensorium and was unable to move his right forearm. His edematous right forearm revealed a 4 · 2cm ulcer in the posteromedial aspect near the elbow and crepitus on palpation. Neither the radial nor ulnar pulses were palpable and the brachial pulse was feeble. Radiography showed gas in the subcutaneous tissue and in the muscular planes (Fig. 1). The patient underwent an emergency fasciotomy to manage compartment syndrome, and a gram stain revealed gram-positive bacilli with subterminal spores (Fig. 2). The patient was given tetanus immune globulin 250 IU and tetanus toxoid 0.5 intramuscular stat, and started on intravenous (IV) penicillin G and clindamycin mL. The next day, infection had ascended to compartments of the arm. The patient underwent an emergency guillotine above-elbow am- putation to control spreading infection. Anaerobic culture showed growth of C. perfringens sensitive to cloxacillin, cef- triaxone, and meropenem. Escherichia coli and Proteus mir- abilis were also isolated. Blood culture was sterile. Patient received 5 d of IV antibiotics followed by oral cloxacillin 500 mg for 7 d. Post-operatively, the patient improved and the wound healed (Fig. 4). The patient was discharged after a 14-d hospital stay. Gas gangrene of the limbs is rare. Usually, amputation is necessary to control infection and preserve life, whereas functional limb preservation is rare [1]. Incubation time is brief, usually less than 24 h, and the physical finding of cre- pitus is characteristic but a relatively late finding in the set- ting of soft tissue infection [4,5]. Plain radiographs identify gas in deep tissues. Bacteremia occurs in approximately 15% of patients and typically develops several hours before skin manifestations [1]. Despite heroic efforts, amputation may be necessary; a salvaged limb may be chronically painful or functionless. The worst case scenario occurs when a limb FIG. 1. Radiograph of the forearm. FIG. 2. Gram-positive bacilli with subterminal spores. Department of Surgery, Jawaharlal Institute of Postgraduate Medical Education and Research, Puducherry, India. SURGICAL INFECTIONS Volume 15, Number 3, 2014 ª Mary Ann Liebert, Inc. DOI: 10.1089/sur.2013.071 361
Transcript of Gas Gangrene: Need for Aggressive Management in Delayed Presentation

Gas Gangrene:Need for Aggressive Management in Delayed Presentation
Murugavaithianathan Pragatheeswarane, Nitesh Naga Balaji, Shyam Duvuru, and Sreenath Gubbi Shamanna
Gas gangrene is an anaerobic infection of skin and softtissue characterized by the presence of gas under the
skin produced by Clostridium spp. It is a potentially lethalcondition that spreads quickly in soft tissues of the body.Tissue necrosis occurs because of the exotoxins produced byspore-forming bacteria that in turn produce gas in an envi-ronment of low oxygen [1]. Delay of surgery for more than12 h is associated with higher overall morbidity [2]. Earlyamputation and prosthetic fitting is associated with decreasedmorbidity, fewer operations, shorter hospital course, de-creased hospital costs, and shorter rehabilitation time in casesof traumatic limb injury [3].
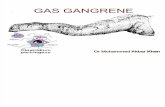
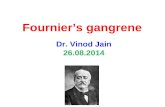
A 75-year-old farmer presented to our emergency depart-ment with a history of painful swelling in the right upper limbfollowing impalement by an animal horn 4 d prior. On ex-amination, the patient had an altered sensorium and wasunable to move his right forearm. His edematous right forearmrevealed a 4 · 2 cm ulcer in the posteromedial aspect near theelbow and crepitus on palpation. Neither the radial nor ulnarpulses were palpable and the brachial pulse was feeble.Radiography showed gas in the subcutaneous tissue and in themuscular planes (Fig. 1). The patient underwent an emergencyfasciotomy to manage compartment syndrome, and a gramstain revealed gram-positive bacilli with subterminal spores(Fig. 2). The patient was given tetanus immune globulin250 IU and tetanus toxoid 0.5 intramuscular stat, and started onintravenous (IV) penicillin G and clindamycin mL. The nextday, infection had ascended to compartments of the arm. Thepatient underwent an emergency guillotine above-elbow am-putation to control spreading infection. Anaerobic cultureshowed growth of C. perfringens sensitive to cloxacillin, cef-triaxone, and meropenem. Escherichia coli and Proteus mir-abilis were also isolated. Blood culture was sterile. Patientreceived 5 d of IV antibiotics followed by oral cloxacillin500 mg for 7 d. Post-operatively, the patient improved and thewound healed (Fig. 4). The patient was discharged after a 14-dhospital stay.
Gas gangrene of the limbs is rare. Usually, amputation isnecessary to control infection and preserve life, whereasfunctional limb preservation is rare [1]. Incubation time isbrief, usually less than 24 h, and the physical finding of cre-pitus is characteristic but a relatively late finding in the set-ting of soft tissue infection [4,5]. Plain radiographs identify
gas in deep tissues. Bacteremia occurs in approximately 15%of patients and typically develops several hours before skinmanifestations [1]. Despite heroic efforts, amputation maybe necessary; a salvaged limb may be chronically painful orfunctionless. The worst case scenario occurs when a limb
FIG. 1. Radiograph of the forearm.
FIG. 2. Gram-positive bacilli with subterminal spores.
Department of Surgery, Jawaharlal Institute of Postgraduate Medical Education and Research, Puducherry, India.
SURGICAL INFECTIONSVolume 15, Number 3, 2014ª Mary Ann Liebert, Inc.DOI: 10.1089/sur.2013.071
361

must be amputated after the patient has endured multipleattempts at salvage or after years of pain following a ‘‘suc-cessful’’ salvage. On the other hand, early amputation andprosthetic fitting is associated with decreased morbidity,fewer operations, a shorter hospital course, decreased hos-pital cost, and shorter duration of rehabilitation in cases oftraumatic limb injury [3].
The subjective importance of body image, the possibilityof prolonged hospitalization, financial burden, and possiblesocial isolation should be discussed with patients in order tohelp them make informed decisions [3]. Aggressive man-agement in those presenting late may result in better out-come.
References
1. Bryant AE, Stevens DL. Clostridial myonecrosis: New in-sights in pathogenesis and management. Curr Infect Dis Rep2010;12:383–391.
2. Sudarsky LA, Laschinger JC, Coppa GF, Spencer FC.Improved results from a standardized approach in treating
patients with necrotizing fasciitis. Ann Surg 1987;206:661–665.
3. Heck R. General Principles of Amputations. In: Canale ST,Beaty JH, eds. Campbell’s Operative Orthopedics, Volume 1,11th ed. Philadelphia: Mosby, Elsevier 2008:562–566.
4. Lanting B, Athwal GS, Naudie DD. Spontaneous Clos-tridium perfringens myonecrosis of the shoulder: A casereport. Clin Orthop Relat Res 2007;461:20–24.
5. Hoffman S, Katz JF, Jacobson JH. Salvage of a lower limbafter gas gangrene. Bull N Y Acad Med 1971;47:40–49.
Address correspondence to:Dr. Murugavaithianathan Pragatheeswarane
Department of SurgeryJawaharlal Institute of Postgraduate
Medical Education and ResearchDhanvanthri Nagar
Puducherry, India 605001
E-mail: [email protected]
362 PRAGATHEESWARANE ET AL.