FUNDAMENTALS OF TREATMENT PLANNING · 2020-04-20 · bibliographical references and index. |...
27
FUNDAMENTALS OF TREATMENT PLANNING
Transcript of FUNDAMENTALS OF TREATMENT PLANNING · 2020-04-20 · bibliographical references and index. |...

FUNDAMENTALS OF TREATMENT PLANNING
Calvani_Frontmatter.indd 1 3/10/20 9:28 AM

III
FUNDAMENTALS OF TREATMENT PLANNINGGuidelines on how to develop,
plan, write and deliver a prosthodontic care project
Lino CalvaniLino Calvani, MD, DDS, CDT, MSc, PhD
Adjunct Associate Professor Department of Prosthodontics and Operative Dentistry
Faculty of ProsthodonticsTufts University School of Dental Medicine
Boston, Massachusetts, USA
Fellow of the:American College of Prosthodontists
Academy of ProsthodontistsGreater New York Academy of Prosthodontists
International College of ProsthodontistsInternational College of Dentists
Calvani_Frontmatter.indd 3 3/10/20 9:28 AM

Library of Congress Cataloging-in-Publication Data
Names: Calvani, Lino, author. Title: Fundamentals of treatment planning : guidelines on how to develop, plan, write and deliver a prosthodontics care project / Lino Calvani. Description: Chicago : Quintessence Publishing Co, Inc, 2020. | Includes bibliographical references and index. | Summary: “This book helps dentists, prosthodontists, and students form and organize their thinking and formulate correct diagnoses and therapies that start with appropriate treatment planning”-- Provided by publisher. Identifiers: LCCN 2020010451 (print) | LCCN 2020010452 (ebook) | ISBN 9780867157925 (hardcover) | ISBN 9781647240332 (ebook) Subjects: MESH: Dental Prosthesis | Patient Care Planning | Prosthodontics--methodsClassification: LCC RK651 (print) | LCC RK651 (ebook) | NLM WU 500 | DDC 617.6/92--dc23LC record available at https://lccn.loc.gov/2020010451LC ebook record available at https://lccn.loc.gov/2020010452
©2020 Quintessence Publishing Co, Inc
Quintessence Publishing Co, Inc411 N Raddant RoadBatavia, IL 60510www.quintpub.com
5 4 3 2 1
All rights reserved. This book or any part thereof may not be reproduced, stored in a retrieval system, or transmitted in any form or by any means, electronic, mechanical, photocopying, or otherwise, without prior written permission of the publisher.
Editing: Quintessence Publishing Co Ltd, London, UKLayout and Production: Quintessenz Verlags-GmbH, Berlin, GermanyCover illustration: Lino Calvani
Printed in Korea
Calvani_Frontmatter.indd 4 3/10/20 9:28 AM

V
“Tristo Discipulo Qui Magister Non Superavit!”“Bad is the student who won’t do better than his teacher!”University La Sapienza, Rome, Italy (founded in 1303)
“Great spirits have always encountered violent opposition from mediocre minds. Imagination is more important than knowledge. Knowledge is limited; imagination encircles the world. Any fool can know, but the point is to understand.
I didn’t arrive at my understanding of the fun-damental laws of the universe through my rational mind. I have no special talent; I am only passion-ately curious.
Time is relative and its unique value is given by what we do as it passes.
Only a life lived for others is a life worthwhile.” Albert Einstein (1879–1955)
Calvani_Frontmatter.indd 5 3/10/20 9:28 AM

VI
As science teaches, the concepts expressed in this book were not written as a point of arrival of learning, but rather as a continuous progression of learning. This book is dedicated to all my beloved teachers who inspired me and who still enrich my life as I remind my students that knowledge always follows when you have passion and commitment.
Lino Calvani
Dedication
Calvani_Frontmatter.indd 6 3/10/20 9:28 AM

VII
Table of Contents
Foreword XIIIAcknowledgments XVOrganization of the book and how to use it XVI
Prosthodontists: Who we are and what we do XIXLiterature XX
Chapter one Past, present, and future of treatment planning ________________________________________ 1
The distant past 220th century to the present 3
‘Hyper-science’ and the future 4References 7
Chapter two Treatment planning management __________________________________________________________ 9
Some definitions and basic premises 10Professionalism: four human factors 11 | 1. Proper communication and dialogue with the patient 11
| 2. Motivating patients 11 | 3. Patient management 12 | 4. Positive professional characteristics 12Priorities 12The ideal treatment plan 12Compromise 13Prosthodontic economics and patient treatment costs 14 | Affordability of the treatment plan 14 | The patient’s occupation 14
| Costs in the face of disease 14 | Transparency and politeness 14Informed consent 15 | Consent 15 | Informed consent 15 | We are not obliged to treat all patients 15 | In case of emergency 16 | The use of the informed consent 16 | Essential aspects of the informed consent document 16
| Digital technology and informed consent documents 17
References 18
Chapter three Prosthodontic tools for treatment planning _____________________________________________ 21
How prosthodontists can help their patients 22Aims and requirements of all prostheses 22Current main prosthodontic tools 22Fixed restorations 22Removable partial dentures 23Complete dentures 23
Removable overdentures 24Full-arch implant-retained fixed prostheses 25Bioinformatics and the digital prosthodontics paradigm shift 25Computerized chairside and laboratory technologies 25
Calvani_Frontmatter.indd 7 3/10/20 9:28 AM

VIII
Table of Contents
| Digital software treatment revolution 25 | In the clinic 26 | Digital treatment planning 26 | Cloud dentistry 26 | Computer-guided implant-positioning software and hardware 26
| 3D virtual articulators 26 | Facially driven dentistry 26 | Computerized laboratory technologies 27Holographic prosthodontics 27The day after tomorrow 27References 28
Chapter four Data, findings, and dental semiotics _______________________________________________________ 33
Data 34Findings 34 | Symptoms 34 | Signs 36
| Simultaneous symptoms and signs 36 | Main symptoms and signs in dental medicine 37Semiotics and dental semiotics 43References 45
Chapter five The first visit – diagnostics __________________________________________________________________ 49
Approaching and meeting the patient 50 | Professionalism 51 | Attitude 51 | Kindness 51 | Empathy 52Where we meet our patients for the first visit 52How to communicate with patients during the first visit 52Professional office techniques to gather information 53
| Emergency examination 53 | Screening examination 53 | Comprehensive examination 54The first professional appraisal 54The important basic information 54Chief complaint 55 | The histories 56Clinical examinations 60 | Radiographic examinations 60References 64
Chapter six Diagnosis and prognosis _____________________________________________________________________ 69
Diagnosis 70 | Differential diagnosis 70Prognosis 71
| New predictive technologies 71 | Prosthodontic prognoses 71References 79
Chapter seven Physical examination – Part I: extraoral examination __________________________________ 85
Clinician qualities 86Steps of the physical examination 86
| Prepare the environment 87 | Make the patient feel at ease 87
Calvani_Frontmatter.indd 8 3/10/20 9:28 AM

IX
Table of Contents
| Check the evaluation questionnaire with the patient 88
Physical examination checklist 88Physical inspection of the body, auscultation, and odor examination 89 | General appearance 89 | Body posture 89 | Movements and muscle coordination 89 | Nails, skin, and hair 89 | Breathing patterns 90 | Odors 90 | Speaking ability 90 | Speech peculiarities 91 | Understanding ability 92 | Vital statistics 92Head and neck inspection – examination 92 | Face 92 | Eyes 92 | Ears 95 | Nose 95 | Mouth 95Head and neck inspection – palpation examination 96 | Static and dynamic possibilities 96 | Palpation techniques 96
Nerves 97 | Neurologic examination 97 | Trigeminal nerve (sensory component of the nerve) 98
| Facial nerve (sensory and motor components of the nerve) 99
Muscles 100 | Masticatory muscles 102 | Muscles of facial expression 103Temporomandibular joints 104 | Neurological examination 104Lymphatic system 106 | The lymph nodes and their importance 106Salivary glands 114 | How to palpate the salivary glands 114Thyroid gland 116 | Shape 116 | Inspection 116 | Palpation 117 | Health status 118 | Function 118 | Clinical relevance 118 | Absence 118References 119
Chapter eight Physical examination – Part II: intraoral examination __________________________________ 121
Intraoral examination procedure 122Intraoral examination checklist 122Vestibular area 123 | Lips 123Vestibules 126 | Cheeks 126 | Parotid (salivary) glands 126 | Floor of the vestibules 128Oral cavity 128 | Palate 128Oropharynx and isthmus of fauces 129 | Pharyngeal tonsils 131Tongue 132
| Anatomy 132 | Examination of the tongue 133Floor of the mouth 135Salivary glands 137 | Submandibular salivary glands 137 | Sublingual salivary glands 137 | Minor mucous salivary glands 138 | Von Ebner’s glands 139 | Clinical conditions of salivary glands 139Alveolar arches and teeth 140Occlusion 140 | Radiographic examination 141References 149
Calvani_Frontmatter.indd 9 3/10/20 9:28 AM

X
Table of Contents
Chapter nine Main clinical examination assessment questions _______________________________________ 153
Clinical extraoral examination 154Clinical intraoral examination 156 | Oral mucosa evaluation 156
| Case assessment occlusal evaluation 158 | Clinical oral and tooth assessment questions 159References 161
Chapter ten The type and structure of prosthodontic treatments ___________________________________ 163
Prosthodontic treatment algorithms 164Treatment planning and predictable results 164 | Clinical priorities 164 | Presence of an infectious disease and its healing time 165
| Need for additional clinical collaborators 165 | Consequentiality of procedures 165Treatment planning of complex cases 165 | Concept of the ‘initial phase’ 166 | Concept of customization 166 | Expectations: a danger zone 166 | ‘Not enough time’ 167 | Balance of time commitment 167 | Posttreatment care commitment 167 | The clinical result should not be equal to or worse than the problem itself 167
Classification of prosthodontic treatments 168 | Class I: Prosthodontic treatments – full reconstructive rehabilitations 168
| Class II: Prosthodontic treatments – interdisciplinary improving rehabilitations 169
| Class III: Prosthodontic treatments – interdisciplinary healing rehabilitations 169
Prosthodontic treatment phases and their algorithms 169Predictability, sequence of work, and consent 171 | Predictability 171 | ‘Red line’ concept 171 | Emergencies and priorities 172References 172
Chapter eleven Treatment planning analysis of complex rehabilitations Phase I: Diagnostics, consultations, and emergencies __________________________________ 173
Some preliminary remarks 174 | Treatment variations and alterations 174 | Time for communication and explanations 174
Diagnostics 175 | Initial diagnostic screening questionnaire 175 | Second updating questionnaire 175 | Initial interview and first visit 176Consultations with other specialists 178 | Dental specialties and other areas of consultation 179
| Diagnostic digital dental technology 180Emergencies 181 | Preprosthetic emergencies, priority treatments, and initial disease control 181
| Preferential route medical priorities 181 | Oral cancer control 182 | Maxillofacial emergencies 183 | Periodontal emergencies 183 | Endodontic emergencies 184 | Tooth extraction emergencies 184 | Caries emergencies 184
Calvani_Frontmatter.indd 10 3/10/20 9:28 AM

XI
Table of Contents
| Professional oral hygiene emergencies 184 | Relining and rebasing of complete and partial dentures 185
References 185
Chapter twelve Treatment planning analysis of complex rehabilitations Phase II: Prosthetic and restorative treatment __________________________________________ 189
Some preliminary remarks 190 | General factors that may affect the planned treatment sequence 190
| Complications that may affect the planned treatment sequence 191
Orthodontic therapy 191Periodontal and oral surgery therapies 192Endodontic therapies 192Mutilated roots and teeth 193Post and cores 193Provisional restorations 194 | Planning the lifespan of provisionals 194
| Long-term fixed provisionals 195 | Analog or digital provisionals? 195Implant placement 195 | Implants are a sensitive rehabilitation to plan 197 | Implant postsurgery instructions for patients 198Maxillomandibular registration 199Final impressions 199Final prosthesis try-in and delivery 200 | Relining and rebasing of RPDs and CDs 200Bite guards 201References 206
Chapter thirteen Treatment planning analysis of complex rehabilitations Phase III: Posttreatment care and recalls _________________________________________________ 211
Planning for Phase III 212 | Periodic recalls for maintenance 213 | Patient compliance and special maintenance holding programs 213
Basic prosthodontic maintenance checklists 214 | Fixed prosthesis maintenance checklist 214 | Removable partial denture (RPD) maintenance checklist 214
| Complete denture (CD) maintenance checklist 215Reinforcing oral hygiene at recall visits 216
| Educating patients about personal oral hygiene 216
Treatment planning fluoride 219Treatment planning prophylactic therapies 220Treatment planning the improvement of the patient’s diet 221Making patients more aware of dangerous habits 222References 223
Chapter fourteen Treatment planning for the elderly and those with challenging health conditions ______________________________________________________________________________________ 227
Some medical statistics 228Patient awareness and communication 229
Prosthodontic treatment planning for elderly and geriatric patients 230
Calvani_Frontmatter.indd 11 3/10/20 9:28 AM

XII
Table of Contents
| Some basic statistics 230 | Treating elderly people 231Prosthodontic treatment planning for patients who are addicted to drugs 232Signs and symptoms of the most common drugs 235 | Prescription analgesics 235
| Sedatives, anxiolytics, and antidepressants 235 | Marijuana 236 | Cocaine 236 | MDMA and ecstasy 236 | Methamphetamines 236 | Heroin 237References 237
Chapter fifteen How to write a prosthodontic treatment plan ___________________________________________ 241
I. How to write a prosthodontic treatment plan for your patient 242II. How to write a prosthodontic treatment plan for a professional case presentation 243III. Main text and writing guidelines 243IV. Prosthodontic case presentation narratives 247 | Examples and scenarios 247Case 1 Perioprosthetic treatment 248 | Phase I diagnostics – case narrative 248Case 2 Perioprosthetic treatment 252 | Phase I diagnostics – case narrative 252Case 3 Perioprosthetic treatment 255
| Phase I diagnostics – case narrative 255Case 4 Perioprosthetic treatment 259 | Phase I diagnostics – case narrative 259Case 5 Perioprosthetic treatment 263 | Phase I diagnostics – case narrative 263Case 6 Maxillary complete dentures and mandibular fixed/removable partial denture 266 | Completed case narrative 1 266Case 7 Rehabilitation of complete dentures 277 | Completed case narrative 277Case 8 Fixed and removable combined rehabilitation 282 | Completed case narrative 282
Calvani_Frontmatter.indd 12 3/10/20 9:28 AM

XIII
Foreword
What we know and do today creates the premises of our tomorrow.
A scientific book is like a mosaic, a complex of many chapters or tiles, each one with its color and meaning and specific position in the whole. How-ever, when you look at a single tile you only see that particular color, whereas if you look at all the tiles you see the overall final composition. This book it-self is a humble tile that is part of a much larger mosaic – medical care.
The specialty of prosthodontics was born almost two centuries ago in the United States of America, where it still evolves at a pace and level of complex-ity that is unknown anywhere else. Prosthodon-tic science is not an easy matter to deal with. It is probably the field of dental medicine that deals with the largest amount of medical, dental, clinical, and laboratory data. But even though it is complex, it is beautiful and requires humble passion and commit-ment to know it well. Recent discoveries and tech-nological advances have increased the amount and quality of new treatment modalities. This may some-times be misinterpreted as ‘heavier’ procedures, but in fact it is not. While the increasing wealth of in-formation may appear to be overwhelming or very complex, it is really only a matter of putting in the constant effort of learning how to handle it. For-tunately, there are many new digital technologies available today that are helping us to achieve this. The entire preliminary before-treatment assessment that professionals in all fields of medicine and den-tal medicine have to commit to before they begin to care for a patient can be summarized in two simple words: treatment planning.
I wrote this book because while lecturing on the topic of prosthodontic treatment planning over the years I was asked to organize my notes and make them easily access ible to all students. The complex-ity of the topic and the enormous body of existing literature engaged me in a great effort of synthesis
to rationalize and select the fundamentals. It was a challenge to avoid dipping too deeply into the var ious more philosophical ideas and notions that comprise this complex field, although some of these are touched upon in the text when necessary. How-ever, analysis and description are the backbones of the book, and treatment planning is the basic scaf-folding on which I have constructed the text. Treat-ment planning is the investigative and diagnostic phase where the clinician plans a well-structured, rational sequence of care steps in order to best treat each individual patient. And this aspect naturally expands in the book into defining and discussing many other aspects of prosthodontic work as well as possible collaboration with other related dental medical specialties that contribute to the rehabil-itation of patients such as periodontics, orthodon-tics, endodontics, maxillofacial surgery, and other specialties.
Although the book primarily addresses pros-thodontic specialists, it also explains basic mat-ters relevant to all medical fields. Therefore, grad-uate and postgraduate students as well as general practitioners and specialists in other fields besides prosthodontics will hopefully find useful explana-tions and outlines that will make them aware of the various aspects and possibilities of medical and prosthetic treatment planning as it exists today. Af-ter all, medical and dental medical treatment plans have the same basic origin and structure.
I strongly believe that treatment planning should be elevated to the same level as other scientific medical fields such as anatomy and physiology and afforded the same respect and dignity. It should be taught and evaluated as a subject in its own right. Furthermore, in the study, discussion, and formulation of a treat-ment plan, practitioners should never place their own professional pride or economic interest be-fore the best interests of the patient, whose health should always be the paramount issue. The needs of
Calvani_Frontmatter.indd 13 3/10/20 9:28 AM

XIV
Foreword
every patient should be treated with respect. Every case deserves to be rehabilitated in full agreement with the patient.
Winston Churchill is credited with saying: “He who fails to plan is planning to fail.” This refers to the logical premise that planning is essential in order to achieve success in human endeavor. Knowledge and organization are the main keys to success and make all the difference between professionalism and in-competence. For this reason, success in prosthodon-tics (as in most other human activity) depends on the amount and quality of our knowledge and how we plan to carry out the work we face – the detail of the where, when, and how of it – in order to predict and then achieve the best possible results.
The topic of this book is deeply rooted in medical ethics. As a board-certified physician, dentist, dental technician, and prosthodontist, over time I have become convinced that our professional duties go way beyond the limits of the teeth and the oral cavity.
Who we are is expressed by what we know and what we do, which is largely a matter of conscious-ness and awareness. The physical health of our pa-tients is our primary goal; it is for this reason they seek our help. Apart from how patients take care of themselves, once they are in our offices their phys-ical health largely depends on how well we perform our examinations, and how attentive and clever
we are in detecting their condition/s and realizing how other physical ailments may be manifesting as dental problems. It is for this reason that we need to know our patients better from a broader med-ical perspective. A deeper understanding of how to conduct a physical examination of the head and neck area may be helpful and improve the way we work. The eyes, ears, nose, hands, and brain of the dental medical professional can not only help peo-ple to chew, speak, and look better, but also to live better, safer, and longer lives; in some cases, they may even save lives. As professionals we have to be conscious and aware of this because we work in the same medical field as physicians and surgeons, and we should all be able to perform a careful phys-ical examination of the head and neck. The more we know and practice, the better able we are to take care of our patients.
I respectfully bring this book to the attention of all my young colleagues, both national and inter-national, who may find the text helpful in order to form and organize their thinking and to formulate correct diagnoses and therapies that start with ap-propriate treatment planning. I will derive a little satisfaction if, with my effort, I am able to help cli-nicians and patients to improve their work and live better lives.
Lino Calvani, 2020
Calvani_Frontmatter.indd 14 3/10/20 9:28 AM

XV
Acknowledgments
Thank you to my parents, Mario and Jole, beloved knowledgeable pediatrician and dentist. Your superb example and loving memories are always with me. You taught me to commit my profession to the exclusive interest of the patient and of science.
Thank you to my daughter, Ludovica, ortho-dontist, for your invaluable contribution, and to my son, Gianluigi, actor and playwright, for your
helpful sensitivity and brainstorming capabilities. Thank you, dearest Francesca, for your love. I hope you will forgive me for all the private time I took from your lives. Thank you dear Avril, unique editor and friend, you are always able to teach me a lot.
Thank you to my endless list of teachers who have been beacons for me. I will always be your humble student.
Calvani_Frontmatter.indd 15 3/10/20 9:28 AM

XVI
Organization of the book and how to use it
The book is divided into 15 chapters that describe different aspects of prosthodontic treatment plan-ning, from the first meeting with the patient to the delivery of the final prosthodontic treatment plan.
As you will see, each chapter describes a specific topic. Due to the complexity of the subject mat-ter, many topics appear in more than one chapter. The reader is therefore provided with an index at the back of the book as well as cross-referencing throughout in order to reinforce the understanding of treatment planning.
Progressive explanations lead the reader to the last chapter, which contains a number of examples of how to write and describe a treatment plan.
The structure of the book is learner-friendly and will hopefully help readers to understand and memo-rize both the concepts and their functional rationale.
The following paragraphs present a short de-scription of what you can expect from each chapter.
Chapter one: Past, present, and future of treatment planningThis introductory chapter, born from a curiosity to better understand how medical treatment planning came to be conceived, highlights the scientific as-pects related to the development of treatment plan-ning. Only the information that seems to have an obvious connection to the topic is discussed. The data show the clear growth trend of treatment plan-ning in the western world. Possible future perspec-tives to date and in the foreseeable future are also touched upon. Due to the obvious restraints of the size and nature of this publication, much informa-tion has had to be omitted.
Chapter two: Treatment planning managementThe purpose and aims of any treatment plan are ex-plained and discussed in this chapter. Also discussed are the basis of respect for all patients; the priorities
to be considered; the importance of clearly under-standing the chief complaint/s that lead to patients seeking help; patients’ understanding of their actual condition/s; the possibility of achieving an ideal treatment plan; the sometimes inevitable compro-mises that need to be clearly explained to patients to gain their understanding, awareness, and final approval; and the importance and possible limita-tions of the informed consent, which is the neces-sary final step before treatment begins.
Chapter three: Prosthodontic tools for treatment planningThis chapter describes the main restorative treatment options that exist in prosthodontics, which can be used as care tools to plan any type of rehabilitation. The chapter also includes a discussion of the rapid development of digital technologies and the impact of this on the field of prosthodontics, including the way in which our work has to be continually updated.
Chapter four: Data, findings, and dental semioticsThe topic of data and findings is discussed in the next chapter, including how, when, and why to col-lect and interpret their meaning. Signs and symp-toms such as pain, fever, and hyperthermia are also defined and their diagnostic importance described. The semiotic clinical analysis is explained with re-gard to investigating the clinical signs that lead to a more complete diagnosis.
Chapter five: The first visit – diagnosticsThe aims and significance of the first visit are elab-orated upon in this chapter. A description is given of the different types of practical techniques that are used to gather information about patients. Also delineated is the diagnostic information that needs to be gathered and assessed during the first visit such as the patient’s chief complaint/s; personal,
Calvani_Frontmatter.indd 16 3/10/20 9:28 AM

XVII
Organization of the book
medical, dental, and prosthodontic history; and psy-chologic profile. The development of the initial part of the treatment plan, the management of emergen-cies, and the restorative planning are also described.
Chapter six: Diagnosis and prognosisThe meaning of the diagnosis, the differential diag-nosis, and the prognosis are detailed in this chapter as well as their importance to the positive outcome of the prosthodontic treatment. The pretreatment and posttreatment prognoses are analyzed, and the periodontal, prosthodontic, and orthodontic eti-ology and risk factors that may impact the timing of the prognoses are also described.
Chapters seven and eight: Physical examinationsThese two chapters on the medical examination present a step-by-step description of the basic pro-cedures and methods that need to be applied when examining patients, starting from the first moment of engagement with the patient and following with the chairside examination at the first visit. Useful descriptions of all the most important extraoral and intraoral anatomical features are provided, together with their clinical and prosthodontic relevance and importance. The semiotic possibilities of these ex-aminations are also evaluated.
Chapter nine: Main clinical examination assessment questionsThis chapter continues the topic of examinations. It details the clinical intraoral and extraoral examina-tions and their importance in evaluating and assess-ing patients’ health status and possible past and ongo-ing conditions. This can be considered an important juncture in the clinician–patient relationship, which can decide whether we gain patients’ trust or lose them as patients; the procedures and suggestions in this chapter are therefore crucial.
Chapter ten: The type and structure of prosthodontic treatmentsThis chapter describes, analyzes, and proposes a new and original classification for prosthodontic
treatment types according to the three main possi-ble clinical variables: pure prosthodontic rehabilita-tions, those in collaboration with other specialists, and the presence of disease.
Chapters eleven, twelve, and thirteen: Treatment planning analysis of complex rehabilitationsThe timing and organization of the different phases comprising a prosthodontic treatment plan are described and analyzed in these three chapters. Each of the three phases is explained with a view to understanding the priorities and to better organize the sequence of the phases in order to simplify the analysis and narrative de-scription of a treatment plan. Also explained is the importance of integrating the radiographic and cone beam computed tomography (CBCT) diagnostic examinations to better define the final diagnosis.
Chapter fourteen: Treatment planning for the elderly and those with challenging health conditionsThis chapter deals with the topic of treatment plan-ning for elderly patients and those with drug addic-tions. Included are observations on how the body and oral cavity age, and how medicines and drugs influence and affect patients and, in turn, the effect this has on medical or dental treatment plans. Also shown is how the changes of aging can significantly affect a prosthodontic treatment, so that alternative solutions need to be planned according to the pa-tient’s needs. Discussed too is how transitory or chronic major conditions may modify a patient’s capability to withstand an oral rehabilitation. A description and analysis are given of the most im-portant drugs and how they may cause addiction as well as how they affect and influence oral treatment choices.
Chapter fifteen: How to write a prosthodontic treatment planThe final chapter describes why and how treatment plans can be presented for in-office purposes or for
Calvani_Frontmatter.indd 17 3/10/20 9:28 AM

XVIII
Organization of the book
PowerPoint or Keynote presentations. A number of useful clinical case narratives are presented as practical treatment planning examples that could be used for the purposes of university case pres-entations and examinations, meetings, congress presentations or lectures. The ‘narrative frame-works’ of all the narrative reports explain the ra-tionale behind why certain decisions have been made while other choices have been avoided, and how this rationale can be explained to patients, to other professionals or to students during seminars.
Calvani_Frontmatter.indd 18 3/10/20 9:28 AM

XIX
Prosthodontists: Who we are and what we do
“The world moves in front of them who know where to go and what to do.”Lino Calvani
I approached this profession and specialty with in-finite humbleness, respect, curiosity, and commit-ment, and this is what still pushes me forward with passion. Prosthodontics is a beautiful, complex, and very demanding specialty in terms of knowledge and commitment. I have been moved to see in the literature how many have dedicated so much of their lives to its development and success. The list of lit-erature that follows (in alphabetical order) is a small but highly representative sample of the significant writings dedicated to the growth and development of prosthodontics. The amazing professionals who have written these articles, papers, and books, and the many others who are not included in this list for reasons of space, have set a standard of passion and professionalism that is difficult to match.
The specialty of prosthodontics was originally recognized in 1948 by the Commission of Dental Accreditation (CODA), an independent agency of the American Dental Association (ADA), which is an independent organization recognized by the United States Department of Education.
The ADA defines prosthodontics as: “the den-tal specialty pertaining to the diagnosis, treatment planning, rehabilitation, and maintenance of oral function, comfort, appearance, and health of patients with clinical conditions associated with missing or deficient teeth and/or oral and maxillofacial tissues using biocompatible substitutes.”
During the three years of training in all United States postgraduate prosthodontics specialty pro-grams, students must become knowledgeable in the
comprehensive treatment of clinical cases for miss-ing or deficient teeth and oral and maxillofacial tis-sue in order to competently find solutions and cures using biocompatible substitutes. The focus is on the following areas:
1. Patient assessment (both medical and dental history).
2. Extraoral and intraoral examination.3. Radiologic assessment and occlusal analysis.4. Temporomandibular joint (TMJ) assessment. 5. Systemic, infectious, and neoplastic disease
screening (education for prevention).6. Diagnosis.7. Risk assessment and prognosis.8. Treatment planning.9. Comprehensive treatment.10. Outcomes assessment and delivery.11. Follow-up and maintenance.
As professionals, we ‘profess’ to believe in who we are and what we do. As the Mission Statement of the American College of Prosthodontics states: “Prost-hodontists are specialists in the restoration and re-placement of missing teeth and oral/facial structures with natural, esthetic, and functional replacements. This includes surgical implant placement, the simple to most complex implant-supported restorations, lab-oratory and clinical training in esthetics/cosmetics, crowns, bridges, veneers, inlays, removable complete and partial dentures, dental implants, TMD-jaw joint issues, traumatic injuries to the mouth’s structures, congenital or birth anomalies and/or teeth, snoring and sleep disorders, as well as oral cancer, prosthetic reconstruction, and continuing care. Prosthodontists are experts in treatment planning.”
Calvani_Frontmatter.indd 19 3/10/20 9:28 AM

XX
Literature
1. American Board of Prosthodontics. History, information, and examination requirements of the American Board of Prosthodontics. J Prosthet Dent 1984;52:281–287.
2. American College of Prosthodontists. Reframing the Future of Prosthodontics: An Invitational Leadership Summit, 2006:11–12.
3. American College of Prosthodontic. Mission Statement, 2018.
4. American Dental Association. Report of the ADA-Rec-ognized Dental Specialty Certifying Boards, 2012;2.
5. Atwood DA. Practice of prosthodontics: past, present, and future. J Prosthet Dent 1969;21:393–401.
6. Boucher CO. Trends in the practice and philosophy of prosthodontics in the United States. J Prosthet Dent 1966;16:873–879.
7. Boucher LJ. The role of research in prosthodontics. J Prosthet Dent 1965:15;962–966.
8. Boucher LJ, Wood GH. Workshop on advanced prostho-dontic education: a preliminary report. J Prosthet Dent 1969;21:433–442.
9. Boucher LJ. Advanced prosthodontic education. J Pros-thet Dent 1976;35:29–30.
10. Carlsson GE, Omar R. Trends in prosthodontics. Med Princ Pract 2006;15:167–179.
11. Chalian VA, Dykema RW. Minimal clinical require-ments for advanced education in prosthodontics. J Prosthet Dent 1976;35:39–42.
12. Garfunkel E. The consumer speaks: how patients select and how much they know about dental health care per-sonnel. J Prosthet Dent 1980;43:380–384.
13. Hardy IR. History of the specialty of prosthodontics. J Prosthet Dent 1965;15:946–948.
14. Johnson WW. The history of prosthetic dentistry. J Prosthet Dent 1959;9;841–846.
15. Jones PM. Advanced education in prosthodontics – cur-riculum content. J Prosthet Dent 1976;31:31–33.
16. Kelsey CC. Survey of income of prosthodontists as assessed by the American College of Prosthodontists. J Prosthet Dent 1975;34:120–124.
17. Knutson JW. Research and the future of prosthodontics. J Prosthet Dent 1961;11:375–381.
18. Koper A. Minimal clinical requirements for advanced prosthodontics education. J Prosthet Dent 1976;35: 34–36.
19. Koper A. Advanced prosthodontic education: a ra-tionale for a curriculum which integrates fixed and
removable prosthodontic education. J Prosthet Dent 1979;41:576 –578.
20. Laney WR. History of the American Board of Prostho-dontics. J Prosthet Dent 1972;28:655–656.
21. Laney WR. American Board of Prosthodontics. J Pros-thet Dent 1975;34:675–693.
22. Laney WR. Limitation of clinical practice to prostho-dontics. J Prosthet Dent 1976;35:57–61.
23. Love WB. Prosthodontics – Past, present and future. J Prosthet Dent 1976;36:261–264.
24. Lytle RB. Criteria for evaluating candidates or the American Board of Prosthodontics. J Prosthet Dent 1969;21:417–422.
25. Mann WR. What dentistry expect of the prosthodontist. J Prosthet Dent 1965;15:949–955.
26. Morse PK, Boucher LJ. How 274 prosthodontists ranked four methods of advanced education in prosthodontics. J Prosthet Dent 1969;21:431–432.
27. Morse PK, Boucher LJ. What a prosthodontist does. J Prosthet Dent 1969;21:409–416.
28. Nagle RJ. The role of the specialty of prosthodontics in service to the public and to the profession. J Prosthet Dent 1965;15:956–961.
29. Ortman HR. Meeting the challenges facing prosthodon-tics. J Prosthet Dent 1980;43:586–589.
30. Payne SH. Knowledge and skills necessary in the prac-tice of prosthodontics. J Prosthet Dent 1968;20:255–257.
31. Payne SH. The future of prosthodontics. J Prosthet Dent 1976;35:3–5.
32. Taylor TD, Bergen SF, Conrad H, Goodacre CJ, Piermatti J. What is a Prosthodontist and the Dental Specialty of Prosthodontics? American College of Prosthodontics, Position Statement, 2014.
33. The Academy of Denture Prosthetics. Principles, con-cepts and practices in prosthodontics. J Prosthet Dent 1968;19:180–198.
34. Travaglini EA. Prosthodontics and the single-concept film. J Prosthet Dent 1973;30(4 Pt 2):640–641.
35. Wiens JP. Leadership, stewardship, and prosthodontic’s future. Int J Prosthodont 2007;20:456–458.
36. Wiens JP, Koka S, Graser G, et al. Academy of Prost-hodontics centennial: The emergence and develop-ment of prosthodontics as a specialty. J Prosthet Dent 2017;118:569–572.
37. Young JM. Prosthodontics in general practice residency. J Prosthet Dent 1974;31:615–627.
Calvani_Frontmatter.indd 20 3/10/20 9:28 AM

1
CHAPTER ONE
Past, present, and future of treatment planning
Calvani_Ch_1.indd 1Calvani_Ch_1.indd 1 12.02.20 12:0412.02.20 12:04

1 Past, present, and future of treatment planning
2
“Those who do not learn from history are doomed to repeat it.”George Santayana (1863–1952) “The past should be read with the eyes of present time.”Charles Darwin (1809–1882)
“The past is never dead. It’s not even past.”William Faulkner (1897–1962)
The distant pastThe author believes it is important to understand history not so much as a chronicle of events but in terms of the value we attach to and derive from these events. In this way, we arrive at the signifi-cance of the events. When we look back, we under-stand that for long millennia our civilization was not able to conceive or understand much about sci-ence, as we know it today. Certainly, in the distant past, people had absolutely no idea what they were doing when treating physical disease and illness.1-4
But once in a while, a gifted individual with a ‘beau-tiful mind’ sensed something new, and in this way our knowledge was carried a step or two forward. Slowly there developed the understanding and ac-knowledgment that the causes of illness and disease were not so much ‘divine’ as they were natural or human-made, and this understanding was the route to healing them. Of course, the first medical treat-ments were simple natural herbal remedies, primi-tive bandages and cream prototypes, coupled with attempts of a philosophical or religious nature to explain and justify all incomprehensible events by relating them to the will of a moody God.5-7
In more recent history, after the ‘static’ middle ages (from a medical point of view), an increasing awareness of scientific evidence over the past five centuries has allowed for a better understanding of the mechanics of our nature and of the ‘innate con-sciousness’ and ‘self-awareness’ that distinguishes us as a species.8-10 However, compared with other sciences, the development of medicine, including
dental medicine, was more difficult because those bright-minded individuals who became involved had to face not only the extreme complexity and difficulty of the subject matter of the human body and mind, but also the limitations imposed by the endless short-sighted and ignorant doctrines of the time.11-13 The intelligent nature of humans means that we need to trust in order to understand; trusting in science means that in time science will explain everything, whereas trusting in a religious sense (having faith) means believing that God will take care of everything. Historically, the development of medical treatment planning has been strongly in-fluenced by this.14,15 Nevertheless, over the last two centuries, science finally gained its autonomy from religion, and today the two areas of human endeavor are separate, to the obvious advantage of medicine.
An important aspect of the renaissance of med-ical science was the contribution scientists made to laying the anatomical foundations for the under-standing of the cause-and-effect relationship that exists in the human body, and how the various parts of the body function and malfunction in relation to each other. This had profound implications for the development of clinical and surgical therapies. This cause-and-effect relationship can be seen as the initial basis for the current treatment planning ra-tionale. Nevertheless, despite all efforts, ignorance about medicine among the general public was rife because society was disconnected and disorganized, and it was difficult and often impossible to teach and impart new medical knowledge and trends. At that time, medical treatment planning was largely unknown, and to the extent that it did exist, it was very primitive and poorly understood. Therefore, due to almost no true medical understanding, epi-demics, traumas, infections, and cancers indiscrim-inately killed hundreds of millions of people. It took other two centuries before anatomy, physio-logy, and pathology became actual sciences, and the word ‘treatment’ became a medical term.
So, regardless of all the clever minds, poor trans-port and communication meant that people were isolated and led an insular way of life. Medicine it-self was still largely based on old, inaccurate, and
Calvani_Ch_1.indd 2Calvani_Ch_1.indd 2 12.02.20 12:0412.02.20 12:04

20th century to the present
3
often imaginary notions. Medical practitioners were on the whole pompously dressed, incapable igno-ramuses, trying to describe nonexistent diseases with useless Latin words. Original paintings of this medical class show images of fantastic methods and therapies full of enemas, leeches, ointments, and draught potions that were invented and concocted to ‘cure’ all ailments and diseases.4,16
Only during the 17th and 18th centuries did physicists and chemists boost the curiosity of many people, so that people started to believe that they could follow in the footsteps of these scientists in all scientific matters, driven by their then brand-new practice of scientific research methods and the pur-suit of evidence of reality theories. This indirectly contributed to the speeding up of the understand-ing of medical science and treatment planning. In-deed, probably without realizing it, physicists and chemists at that time were changing the way people thought about medical science.
It can therefore be said that medical treatment planning has its origins in scientists attempting to prove that formulas could explain all scientific elements and, indeed, the world. Over time, it be-came clear that signs and symptoms were useful and necessary to make a correct diagnosis of illness and disease. In fact, medical treatment planning is entirely based on scientific methodology and evi-dence. However, while physics, astronomy, math-ematics, and biology were progressing at a rapid pace, scarce technologies and immature methods limited people’s knowledge of the human body, no matter how curious they were. Also, the slow pace of life and very limited social contact meant that it was difficult to spread news, which created many problems.4,16,17
During the 19th century, medical scientists looking for scientific evidence and using the new scientific instruments of the time discovered more ways to heal and cure, which were perfected with time and passion, although many essential notions were lacking, and there was still no precise under-standing of treatment planning.13,18 Universities and medical and dental medical schools began to open and flourish in the USA and in other parts of
the developed world, for example, the Baltimore College of Dental Surgery was founded in 1840, the Philadelphia College of Dental Surgery in 1842, Tufts Dental School in 1852, Harvard Dental School in 1867, and the University of Michigan in 1875. Passionate researchers and clinicians started to cre-ate the basis of actual medical and dental medical scientific treatments.19 So, by the turn of the 20th century, official medical and dental medical sci-ence was starting to be oriented toward what we know today as ‘assessed methodology.’ The study of anatomy was acknow ledged as the basis for un-derstanding medicine, and investigations into the body’s functions and malfunctions started to drive more organized and critical laboratory research and clinical practice.18,20 Scientists’ curiosity and eager-ness for clarification drove them to begin to look for ‘evidence’ as the starting point. The worst of the religious influence on medicine was part of the past.
20th century to the presentWhile the 20th century gifted us with geniuses such as Albert Einstein (1879–1955), it also plagued us with two devastating world wars, which had a sig-nificant influence on the development of treatment planning in the west. About 20 million lives were lost in the First World War (1914 –1918), and about 68 million in the Second World War (1939–1945). Apart from the death toll, war means all kinds of terrible injuries, physical and psychologic, created by all types of weapons. It means traumas, wounds, burns, disfigurements, and epidemics.
The world wars profoundly changed the lives of our grandparents and parents, and forced medical science to find surgical, clinical, and pharmacologi-cal solutions to address the sudden, terrible, and ur-gent traumas they caused. The wide range of inju-ries and infections, many of them never seen before, meant that the understanding about how to plan the treatment of patients accelerated, both during emergencies on the battlefields and in the clinic.
In addition, the 1918 influenza epidemic (known as the Spanish Flu), largely brought on by the un-
Calvani_Ch_1.indd 3Calvani_Ch_1.indd 3 12.02.20 12:0412.02.20 12:04

1 Past, present, and future of treatment planning
4
hygienic conditions of the First World War, left roughly 50 million dead worldwide. Therefore, the total death toll in the almost 50-year period span-ning both world wars was about 125 million peo-ple, not to mention the millions more who were seriously injured in these wars and who died pre-maturely later on. On top of this, other local wars and epidemics followed, bringing the death toll to some 13% to 14% of the entire world population at that time.21,22-24
Due to these events, and thanks to the increased number of dedicated medical scientists and facili-ties, improved communication and media, and the growing body of scientific and medical knowledge that had been slowly accumulating over centuries, medical science made a great leap forward in the first part of the 20th century. The level of aware-ness and consciousness regarding medical treat-ment and its planning increased rapidly during that time, bringing a deeper understanding of the importance of knowledge about medical proce-dures and being well organized in the planning of treatment (this includes dental medicine and pros-thodontic treatment planning, even though the lat-ter is not always that well defined).25-27
Population growth is another important factor in the development of treatment planning. Over the last three millennia, the human population has increased from about 50 million to 7.5 billion peo-ple. Parallel to this is the increase in the number of scientists and thinkers who have dedicated their lives to solving medical problems, which has esca-lated the number of possibilities for furthering med-ical and dental medical science.28,29 Inventions and discoveries that make possible the forward move-ment of science and medicine are not made so much by specific individuals as by the collective know-ledge and awareness that accumulates over time.30-
34 This is known as ‘collective intelligence,’ which expands exponentially all the time, thereby increas-ing the possibility of more and more discoveries that lead to better medical understanding. For instance, about a century ago there would have been few, if any, physicists who properly understood Einstein’s theories. Today, hundreds of thousands of students
easily do, and thanks largely to the internet, their contributions to science are easily and quickly spread throughout the world. Just a century ago, only a few physicians knew what an antibiotic was, and thousands of people died of bacterial infections. Today, most people know about antibiotics and mil-lions of people take them, often autonomously and without careful prescription (which has unfortu-nately also resulted in an alarming and increasing physiologic resistance to them).
This ties in with another important factor in the understanding of the development of treatment planning, which is communication and the media, particularly the internet and smart phones.17,35-37 Since the two world wars (and therefore in less than a century), information about medical sci-ence has rapidly increased, and has been shared among millions of medical and dental profession-als. This means that the panorama of clinical plan-ning and treatment is continually changing and evolving.
‘Hyper-science’ and the future When the famous physicist Niels Bohr (1885–1962) was asked to make predictions about the future, he said humorously: “Predictions are very difficult, es-pecially about the future.” Every small scientific step forward changes our understanding of how to plan and treat medical conditions. However, despite how technology today allows for easy online access for most people to medical research, data, literature, and information, human endeavor remains crucial and necessary.
Currently, data acquisition and processing speeds seem to depend on a number of disruptive ‘innovation platforms’ that cut across sectors and markets and converge on each other on the medical stage, such as:1. 5G and 6G internet connections.2. Micro and macro energy storage for industry,
farming, transportation, cities, etc. 3. Plasma and quantum computers; liquid, nano-
magnetic, and graphene transistors.
Calvani_Ch_1.indd 4Calvani_Ch_1.indd 4 12.02.20 12:0412.02.20 12:04

‘Hyper-science’ and the future
5
4. Artificial intelligence (AI), artificial narrow intelligence (ANI), artificial general intelli-gence (AGI), deep-learning software (DLS), and self-learning software (SLS).
5. Collaborative robotics and humanoids.6. Computer-aided design/computer-aided manu-
facturing (CAD/CAM) and 3D printing.7. DNA sequencing and CRISPR therapeutic
genome editing. 8. Nanotechnologies.
‘Hyper-science’ (author’s own word) seems an ap-propriate composite word for these revolutionary technologies and the current rapid growth of sci-entific knowledge. As never before, the progress of science is accelerating, and capabilities and possibil-ities are increasingly opening up. Which is why the medical progress indicators predict that medical and dental schools will structurally change in the near future under the pressure of digital innovations.38-44
A clear example of the above is the new, cheaper DNA sequencing and CRISPR genome editing that is enabling scientists to develop new types of diag-nostic screens, tests, and therapies. Computational techniques are changing our schools and educa-tional programs constantly, with the three-dimen-sional resources of virtual reality (VR) and aug-mented reality (AR) changing the way students and faculty interact, including the interaction with robots.45-54 Nanotechnology is increasingly being used to treat patients. Predictions made on solid sci-entific bases foresee that, two or three decades from now, well-programmed super-intelligent ANI, and well-instructed human-dependent or independent AGI machines as well as AGI humanoid robotized digital doctors and caregivers will clinically treat patients suffering from an increasing variety of dis-eases and will also feature in the laboratory. These machines will be able to handle programmable and
injectable chemotherapeutical nanorobots and na-nocarriers. They will be much faster and, in many ways, more capable than humans to do the job of medical care providers.25,41,55-58 We will refer to them with trust when we are ill or wounded.
Knowledge, consciousness, and indeed our entire way of living and working are being revolutionized. One only has to attend medical and dental medical meetings, conferences, and expos all over the world to see where the market is now and where it is heading, and how much money is involved. Human history has always demonstrated that whatever we are capable of imagining, we are capable of achiev-ing. Digital science has come a long way, being completely free today of any religious constraints that might prevent it from progressing.
Currently, there is much hyper-scientific intel-ligent curiosity and imagination at work.59 An ex-citing example is the newest IBM Watson Machine Learning, which harnesses machine learning and deep learning in a way that enables the manage-ment of an infinite amount of data. It gives flexible answers, insights, and possible solutions in many different fields of human endeavor, and is already useful to medical professionals in various fields of health care. For treatment planning, for instance, it can be used for collecting and reading scientific lit-erature published in many languages. When asked about a specific disease or illness, it can promptly give one or more answers, propose a fitting diag-nosis, and suggest various treatment options ac-cording to clinical facts, scientific evidence, and sta-tistics. It can also design program interventions.60
However, despite all future AI digital capabilities and skills, the logic of treatment planning, with its basic and complex algorithms, will always consti-tute the common scientific foundation of medical, dental medical, and prosthodontic treatment and its planning.
Calvani_Ch_1.indd 5Calvani_Ch_1.indd 5 12.02.20 12:0412.02.20 12:04

1 Past, present, and future of treatment planning
6
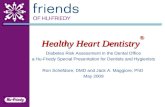
Fig 1-1 The birth and growth of medical examination, diagnosis, and treatment planning in western civilization. The first real scientific impulse occurred in 1500, with curiosity for the unknown and for medicine following until the end of 1700, when scientific evidence changed the schools and universities and gave birth to empirical knowledge and scientific research.
2000–presentAI, ANI, AGI, and beyond ...
ANCIENT AGE of GODS MIDDLE AGE of GOD MODERN AGE SCIENCE AGE DIGITAL AGE
3600–1000 BC AD
129–216 Galen of Pergamon
354–430 Saint Augustine
b. 1300–1600Chauliac, Da Vigo,
Da Vinci, Paracelsus, Paré, Vesalius, Harvey
1163 – Edict of Tours 1225–1274 Saint Thomas
Aquinas
460–359 Hippocratic Corpus428–347 Plato
384–322 Aristotleb. 1700–1800
Auenbrugger, Pinel, Pfaff, Bichat, Corvisart, Laennec,
Andral, Welsley
b. 1600–1700Sydenham, Locke, Lancisi,
Boerhaave, Fauchard, Morgagni, Bounon
b. 1800–2000Skoda, von Hebra, von
Helmholtz, Pasteur, Osler, Bourdet, Kemperer, Muller,
Frugoni, Müller, Valdoni
Calvani_Ch_1.indd 6Calvani_Ch_1.indd 6 12.02.20 12:0412.02.20 12:04

References
7
References1. Garrison FH. An Introduction to the History of Medi-
cine. Philadelphia: W.B. Saunders, 1921:508. 2. Heidel WA. Hippocratic Medicine: Its Spirit and
Method. New York: Columbia University Press, 1941.3. Crone HD. Paracelsus: the man who defied medicine:
his real contribution to medicine and science. Mel-bourne: Albarello Press, 2004.
4. Major RH. A History of Medicine. Springfield: Charles C Thomas, 1954.
5. Nutton V. Ancient Medicine. Taylor & Francis, 2004.6. Phillips ED. Greek Medicine. London: Thames and
Hudson, 1973.7. Temkin O. Galenism. Ithaca: Cornell University Press,
1973.8. Klein R. Anatomy, Behavior, and Modern Human Ori-
gins. Journal of World Prehistory 1995;9: 167–198. 9. Kording KP, Tenenbaum JB, Shadmehr R. The dynamics
of memory as a consequence of optimal adaptation to a changing body. Nat Neurosci 2007;10: 779–786.
10. O’Neal JC. Auenbrugger, Corvisart, and the perception of disease. Eighteenth Century Stud 1998;31: 473–489.
11. Durant W. The Age of Faith: A History of Medieval Civ-ilization – Christian, Islamic, and Judaic – From Con-stantine to Dante, A.D. 325–1300. MJF Books, 1993.
12. French R. Medicine before Science: The Business of Medicine from the Middle Ages to the Enlightenment. Cambridge University Press, 2003.
13. Grant E. A Source Book in Medieval Science. Harvard University Press, 1974:807.
14. Buck AH. The Growth of Medicine from the Earliest Times to about 1800. Yale University Press, 1917.
15. Prioreschi P. A History of Medicine, Volume 5: Medie-val Medicine, ed 2. Lewiston, NY, USA: Edwin Mellen Press, 1996.
16. Johnson DA, Schaffer D. Learning from the Past – The History of Planning: Introduction. Journal of the Amer-ican Planning Association 1985;51: 131–135.
17. Loudon I. Western Medicine: An Illustrated History. Oxford University Press, 2001.
18. Adams FD. Physical Diagnosis, ed 14. Baltimore: Wil-liams & Wilkins, 1958.
19. Gillis J. The history of the patient history since 1850. Bull Hist Med 2006;80: 490–512.
20. DeGowin EL, DeGowin RL. Bedside Diagnostic Exam-ination. New York: Macmillan, 1965.
21. McCallum JE. Military Medicine: From Ancient Times to the 21st Century. ABC-CLIO, 2008.
22. Porter R. The Cambridge Illustrated History of Medi-cine. Cambridge University Press, 2001.
23. Tallett F. War and Society in Early Modern Europe 1495–1715. Routledge, 1997.
24. Rutkow IM. History of Surgery in the United States, 1775–1900: Periodical and Pamphlet Literature. Nor-man Publishing, 1992:98.
25. Byrne D. Complexity theory and planning theory; a ne-cessary encounter. Planning Theory 2003;2: 171–178.
26. Walker HK. The origins of the history and physical examination. In: Walker HK, Hall WD, Hurst JW (eds). Clinical Methods: The History, Physical, and Labora-tory Examinations, ed 3. Boston: Butterworths, 1990.
27. Ellis H. A History of Surgery. Cambridge University Press, 2001.
28. Rosling H. Why the world population won’t exceed 11 billion. TGS.ORG, 2016. YouTube lecture.
29. Haub C. How Many People Have Ever Lived on Earth? Population Reference Bureau (PRB), 2011.
30. Goodman ND, Tenenbaum JB, Feldman J, Griffiths TL. A rational analysis of a rule-based concept learning. Cogn Sci 2008;32: 108–154.
31. Gopnik A, Tenenbaum JB. Bayesian Networks, Bayesian learning and cognitive development. Dev Sci 2007;10: 281–287.
32. Jaynes J. The Origin of Consciousness in the Breakdown of the Bicameral Mind. Toronto: University of Toronto Press, 1976.
33. Tenenbaum JB. Griffiths TL, Kemp C. Theory-based Bayesian models of inductive learning and reasoning. Trends Cogn Sci 2006;10: 309–318.
34. Zimmerman LM, Veith I. Great Ideas in the History of Surgery. Norman Publishing, 1993.
35. Heisenberg W. The Physical Principles of the Quantum Theory. New York: Dover, 1949.
36. Selin H (ed). Encyclopaedia of the History of Science, Technology, and Medicine in Non-Western Cultures. Springer, 2016.
37. Rosa H. Social acceleration: ethical and political conse-quences of a desynchronized high-speed society. Con-stellations, 2003;10: 3–33.
38. Albuha AI-Mussawi RM, Farid F. Computer-based tech-nologies in dentistry: types and applications. J Dent (Tehran) 2016;13: 215–222.
39. Al-Thobity AM, Farooq I, Khan SQ. Effect of software facilitated teaching on final grades of dental students in a dental morphology course. Saud Med J 2017;38: 192–195.
40. Lake BM, Salakhutdinov R, Tenenbaum JB. Human-level concept learning through probabilistic program induc-tion. Science 2015;350: 1332–1338.
41. Chang AC. How artificial intelligence will transform medicine. Lecture on: History of Artificial Intelligence, 2017.
Calvani_Ch_1.indd 7Calvani_Ch_1.indd 7 12.02.20 12:0412.02.20 12:04

1 Past, present, and future of treatment planning
8
42. Connell DJ. Planning and its Orientation to the Future.International Planning Studies 2009;14: 85–98.
43. Goodacre CJ. Digital Learning Resources for Prost-hodontic Education: The Perspectives of a Long-TermDental Educator Regarding 4 Key Factors. J Prostho-dont 2018;27: 791–797.
44. Greene CC. How to educate millennials. J Calif DentAssoc 2018;46: 359–362.
45. Aerbersold M, Voepel-Lewis T, Cherara L, et al. Interac-tive Anatomy-Augmented Virtual Simulation Training.Clin Simul Nurs 2018;15: 34–41.
46. Bacca J, Baldiris S, Fabregat R, Graf S, Kinshuk. Aug-mented reality trends in education: a systematic review ofresearch and applications. Educ Tech Soc 2014;17: 133–149.
47. Garg AX, Norman G, Sperotable L. How medical stu-dents learn spatial anatomy. Lancat 2001;357: 363–364.
48. Hu J, Yu H, Shao J, Li Z, Wang J, Wang Y. Effects ofDental 3D Multimedia System on the performance ofjunior dental students in preclinical practice: a reportfrom China. Adv Health Sci Educ Theory Pract 2009;14:123–133.
49. Huang TK, Yang CH, Hsieh YH, Wang JC, Hung CC.Augmented reality (AR) and virtual reality (VR) applied in dentistry. Kaohsiung J Med Sci 2018;34: 243–248.
50. Kell HJ, Lubinsky D, Benbow CP, Steiger JH. Creativityand technical innovation: spatial ability’s unique role.Psychol Sci 2013;24: 1831–1836.
51. Piromchai P, Avery A, Laopaiboon M, Kennedy G,O’Leary S. Virtual reality training for improving the
skills needed for performing surgery of the ear, nose or throat. Cochrane Database Syst Rev 2015;(9):CD010198.
52. Radu I. Augmented reality in education; a meta-reviewand cross-media analysis. Pers Ubiquit Comput 2014;18:1533–1543.
53. Walsh CM, Sherlock ME, Ling SC, Carnahan H. Virtualreality simulation training for health professions train-ees in gastrointestinal endoscopy. Cochrane DatabaseSyst Rev 2012;6:CD008237.
54. Wright EF, Hendricson WD. Evaluation of a 3-D inter-active tooth atlas by dental students in dental anatomyand endodontics courses. J Dent Educ 2010;74: 110–122.
55. Allmendinger P. Planning Theory. New York: Palgrave,2002.
56. Bergdaà M. Temporal Frameworks and Individual Cul-tural Activities: Four typical profiles. Time & Society,Sage, 2007;16: 387–407.
57. EmTech Next. AI and robotics are changing the futureof work. Are you ready? MIT Technology Review. On-line publication, 2018. https://events.technologyreview.com/emtech/next/19/.
58. Reiser SJ. Medicine and the Reign of Technology. Cam-bridge, New York: Cambridge University Press, 1978.
59. Alexander ER. Approaches to Planning: IntroducingCurrent Planning Theories, Concepts and Issues. Lux-embourg: Gordon and Breach Science Publishers SA,1992.
60. IBM – Watson Machine Learning. https://www.ibm.com/cloud/machine-learning. Accessed 29 June 2019.
Calvani_Ch_1.indd 8Calvani_Ch_1.indd 8 12.02.20 12:0412.02.20 12:04