Bethesda Hospitals’ Emergency Preparedness Collaborative: A Regional Model for

s
December 2016
Neurology A new approach for London
Hyper acute neurology services
For district general hospitals and regional neuroscience centres

2
Hyper acute neurology servicesFor district general hospitals and regional neuroscience centres
Acknowledgements
The London Neuroscience Clinical Network is grateful to all who have contributed to this publication, with special thanks to:
» Dr Niranjanan Nirmalananthan, Consultant Neurologist, St George’s University Hospitals NHS Foundation Trust
» Dr Arani Nitkunan, Consultant Neurologist, Croydon University Hospital NHS Trust » Dr Kuven Moodley, Locum Consultant Neurologist, St George’s University Hospitals NHS Foundation
Trust » Michael Oates, Quality Improvement Manager, London Neuroscience Clinical Network » Hyper Acute Neurology Unit (HANU) Working Group

Hyper acute neurology servicesFor district general hospitals and regional neuroscience centres
3
Foreword 4Introduction 5Targeted outcomes 5Current landscape 5Case for change 6Summary of experience of a HANU 6Summary of experience of DGH model 7Model A | DGH: Model for a hyper acute neurology service (HANS) 8Model B | Regional centre: Model for a HANS 9How the model worksDGH (Model A) 10Regional tertiary neuroscience centre (Model B) 11Neurology acute short stay admissions unit (NASSAU) 12Liaison with EDs and AMUs 14Service structure 14Potential financial benefits 15Potential risks 15Recommendations 15Appendix 1 | RCP and the ABN 16Appendix 2 | CCG / STP breakdown of hospital admissions 17Appendix 3 |Common conditions admissions 19Appendix 4 | Data sources 21Appendix 5 | Glossary 22
Contents

4
Hyper acute neurology servicesFor district general hospitals and regional neuroscience centres
More than four million people in England are living with a neurological condition.
In 2012/13 the NHS invested £3.3 billion in neurological services, yet substantial inconsistencies remain in the services patients receive. Reports indicate 64 percent of neurological admissions to a hospital are on an emergency basis -- with more than half of the neurological programme budget spent on unplanned admissions. London has the highest rate of referrals to adult neurology outpatients in the country, yet despite this, the rates of unplanned admissions remain high.
The London Neurology Clinical Network’s Quality and Safety Organisational Audit1 found no hospital where patients with a primary neurological diagnosis were systematically admitted under a neurological specialist from emergency departments. Additionally, integrated care systems for patients with neurologic conditions are poorly developed.
The London Neuroscience Clinical Network proposes a new commissioning approach to address these issues and raise the quality and efficiency of services for people with neurologic conditions.
This paper describes one of three interlocking models examining new approaches to:
» The management of common conditions in the community by a provider network, using a tiered approach.
» Improved acute neurology services at a secondary care level led by neurologists.
» The adoption of patients with neurologic conditions into integrated care systems by providing the tools necessary to make this successful.
Most importantly, we wish to raise the profile of this very important group of patients with commissioners, challenging the status quo of services that are outdated for current needs.
Nick LosseffLondon Clinical DirectorLondon Neuroscience Clinical Network
Foreword
1. London Neuroscience Clinical Network, London organisational audit of secondary and tertiary neurological care providers (2014) Link: http://www.londonscn.nhs.uk/publication/london-neuro-quality-and-safety-organisational-audit/

Hyper acute neurology servicesFor district general hospitals and regional neuroscience centres
5
Introduction
This paper recommends the commissioning of a new approach to address issues of quality, efficiency and responsiveness in the care of people with an acute neurological presentation at an emergency department.
The approach offers two models: one for acute general hospitals and one for regional centres. Both models are based on extensive research and the evaluation and learning from the hyper acute neurology unit pilot run by the Network in 2015/16.
Most patients with an acute neurologic illness are not primarily managed by neurological specialists, and there is significant variation in access to neurological input into clinical decision making.
We believe a change to early neurological opinion at investigation and treatment will provide efficiency savings and improved patient outcomes and experience.
The primary focus of a hyper acute neurology service is to direct efficient and appropriate care of patients with neurological disorders presenting to emergency medicine and acute medicine departments, particularly those considered for admission. However, the service also aims to work across the whole pathway, in parallel with other work streams being developed by the network, to:
» Manage referrals from general practioners (GPs) – diagnosing, treating and directing self care where appropriate; setting strict and implementable referral management pathways.
» Review and manage appropriate patients through a tiered model.
» Triage patients (for example, those with migraine) to prevent them from being admitted unnecessarily to hospital.
» Work with providers to ensure that where emergency treatment is needed patients are directly assessed by neurologic experts, improving quality, preventing unneeded diagnostics and admissions.
» Support community integrated care with expert advice.
Targeted outcomes
» Reduce A&E admissions of patients managed by the service through admission prevention. Use of urgent care clinics or appropriate referral to other services.
» Early diagnosis and appropriate use of diagnostics. » Reduce readmissions of patients managed by the
service. » Reduce inpatient transfers to tertiary neuroscience
centres. » Achieve consistent outcomes and standards.
See Appendix 2 for Sustainability and Transformation Plan (STP) and Clinical Commissioning Group (CCG) data on outpatients, admissions and costs.
Current landscape
There are 252,000 people living with a neurological condition in London (not including migraine, stroke or dementia, which constitutes an additional 1.9 million). This is more than the number of people living with cancer, coronary heart disease, chronic kidney disease or cardiovascular disease. Neurological symptoms account for one in 10 GP consultations, 10 per cent of all hospital admissions and 17 per cent of all emergency admissions in London.
Sixty-four per cent of neurological admissions to a hospital are on an emergency basis, and more than half of the neurological programme budget is spent on unplanned admissions. There are more emergency admissions for neurological conditions than for other disease groups including cancer, musculoskeletal problems and stroke. However, many patients with neurological conditions suffer unpredictable changes in their condition or a related comorbidity and require access to urgent or emergency care.
Throughout this document, the term “acute neurology” is used for the neurological care a patient receives on entering the health system via emergency or urgent care routes, whether as an undiagnosed patient or as an existing patient where the condition has suddenly deteriorated or a comorbidity has initiated the need for emergency attendance.

6
Hyper acute neurology servicesFor district general hospitals and regional neuroscience centres
Most patients with an acute neurologic illness are not primarily managed by neurological specialists but by emergency physicians, general and acute physicians, geriatricians, or intensive therapy unit (ITU) staff, with or without advice through consultative visits or by telephone support from regional centres. The long standing neurological service structure and peripatetic organisation of neurologists’ job plans explain the low numbers of neurologists, particularly at district general hospital level. This is compounded by difficult access to vital diagnostic tests (eg MRI, EEG, EMG). Most neurological resources are centred at regional centres which provide both a local neurology service and specialist services for complex or rare neurological conditions.
Case for change
The rationale behind the need to improve the service for a patient with a neurological symptom when using emergency services was described in the Network’s London acute neurology services: A case for change. Evidence from other emergency models in the UK indicates that admissions, length of stay and diagnostic error can be reduced with early specialist opinion. London has excellent stroke services that have transformed experience, outcome and reduced costs, and which has many synergies with other neurological conditions. The organisation of acute secondary care neurological services in London does not promote ownership of patients with neurological problems by neurologists. Most patient facing neurological input is obtained through outpatient appointments which do not meet the urgent needs of neurological patients.
This case for change proposes that patients with a primary neurological diagnosis are systematically reviewed and managed by neurology specialists in acute settings through the development of acute neurology standards and models.
There is an opportunity to develop services that provide patients with acute neurological conditions with timely access to neurological opinion, investigation, and treatment. The London Neuroscience Clinical Network co-ordinated a series of pilots in London that introduced acute neurology services, which we called hyper acute neurology units (HANUs).
Summary of experience of a HANU
Pilot hyper acute neurology services were evaluated during 2015, including local hospital audit and outcome data from St George’s Hospital and King’s College Hospital plus UCLPartners’ evaluation of the HANU project.
Key findings
» Improved patient experience - Feedback from staff suggested the HANU models resulted in positive outcomes for patients, due to an increased and early neurological input providing timely diagnosis and a more clear management plan.
» Improved clinical outcomes and processes - Post HANU, those with common conditions such as headache and epilepsy showed a clear benefit from early neurological involvement. At King’s, there was a 100 per cent increase in epilepsy patients referred to neurology outpatients. Patients with a first suspected seizure or with ongoing seizures need to be referred into specialist National Institute for Health and Care Excellence (NICE) approved pathways; this study suggests that dedicated neurological input can facilitate this.
» Improved diagnosis - Early neurology input showed the benefit of identifying less common or complex disorders frequently not recognised by non-neurological specialists. During the HANU pilot, King’s recorded 106 different primary neurological diagnoses, suggesting early input at acute presentation could significantly reduce the need for unnecessary tests to establish a diagnosis.
» Reduced readmissions - Comparative data pre and post HANU showed a reduction in the number of patients who re-attended the emergency department (ED) within 30 days for the same condition, specifically those with common conditions relating to headaches (13.9% versus 3.8%) and epilepsy (6.1% versus 0%) post HANU at UCLH. It is suggested a clear management plan offered by specialist in the HANU is linked to this reduction in readmission.

Hyper acute neurology servicesFor district general hospitals and regional neuroscience centres
7
» Reduction of ED visits and unplanned hospital admissions - The findings from the study also suggested that the model may have additional benefits arising from rapid follow up in outpatient clinics, which might further reduce ED visits and unplanned hospital admissions.
» Discharge - During the pilot at King’s, 43 patients were discharged who, prior to the HANU model, would have been admitted to the medical admissions unit. This accounts for 19 per cent of admissions avoided from the total number of patients reviewed (n=231). Similarly, St George’s saw a significant change in the increase of patients discharged following a neurological review. According to two audits at St George’s discharges increased from 23 per cent in 2012 to 72 per cent in 2015 from the short stay unit during which saw a number of changes being implemented linked to earlier consultant input.
» Models of care – The greatest benefits were observed secondary to more specialised input at the acute medical unit (AMU) / ED level rather than by the “ownership” of inpatients, as admissions were in any case substantially reduced. The resulting need for secondary care level inpatients was small, but itself prevented referral to tertiary beds for common problems.
Summary of experience of DGH model
The pilot at Croydon University Hospital involved an acute neurology clinical coordinator (a stroke nurse by background). Evaluation of this pilot included a review of the number of referrals for neurological opinion, how quickly they were seen and the rate of readmission, length of stay and satisfaction. It concluded that:
» Referrals for neurological opinion increased 28 per cent as a result of the coordinator reviewing all referrals. Admissions seen within 48 hours increased from 89 to 97 per cent, due to improved co-ordination by the nurse, with 76 per cent of all referrals seen on the day of the referral.
» Although the average length of stay during the evaluation period did not change, the model had a significant impact on the shorter length of stay group. In this group, length of stay reduced from 3.6 to 3.1 days (p=0.04), yielding an estimated savings of £57,750. The model for the acute neurology coordinator would therefore be cost neutral.
» The evaluation did not identify any change in readmission rates, but the satisfaction with the service from the acute medical unit staff was greater than for all other major medical specialities.
» Due to the faster discharge of the shorter stay patients, nurse led telephone clinics and “hot clinic” (defined as urgent clinics with a short wait, eg three days) appointments were established; a minimum of three slots each week were needed in the Croydon pilot.

8
Hyper acute neurology servicesFor district general hospitals and regional neuroscience centres
Model A | District general hospital: Model for a hyper acute neurology service (HANS)

Hyper acute neurology servicesFor district general hospitals and regional neuroscience centres
9
Model B | Regional centre: Model for a hyper acute neurology service (HANS)

10
Hyper acute neurology servicesFor district general hospitals and regional neuroscience centres
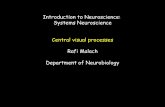
How the model works
District general hospitalModel for a HANS | Model A
The hyper acute neurology service (HANS) model for the district general hospital (page 8) is based on a consultant-delivered, specialist nurse supported model, currently delivered at Croydon University Hospital.
The HANS model is suitable for a hospital with an ED that serves a local population of 350,000 with 3 to 5 whole time equivalent (WTE) consultant neurologists based at or visiting the hospital. The model is not contingent on neurology beds or neurology juniors, although these may be available at some DGHs. There will be access to clinical neurophysiology and a general radiology service providing EEGs, EMGs, CTs and MRIs within a five day service.
The Association of British Neurologists (ABN) recommended consultant ratio for local adult neurology services is 1 neurologist per 70,000 population. Commissioning of HANS services should account for this. Current typical job plans entail four outpatient clinics for DGH neurology consultants. If the model was to be delivered by three neurologists, this would necessitate a move in job plans away from scheduled care to more acute facing time. This may lead to a reduction in the number of clinics if there is insufficient consultant numbers, and therefore should be supported by changes in commissioning arrangements. The focus for a DGH model is improved management of patients with a neurological condition after admission through an acute medical unit. Due to staffing pressures, consistent in-reach into ED (with its four hour target) is not viable in DGH settings. The neurologists will provide a five day acute ward referral service. This service would include AMU, but also AMU ambulatory care and
ED clinical decisions units (ie ED patients outside the four hour ED target) where these are present. With sufficient staffing, cover will be consistent even when consultants are away.
To support this model, an acute neurology specialist nurse provides an AMU in-reach service to improve quality of care, length of stay and rates of readmission. Disease specific nurse specialists (eg epilepsy, multiple sclerosis, Parkinson’s disease) may or may not already be present in some DGHs and could also integrate within the HANS, primarily by focusing on admission avoidance for patients with long-term neurological conditions.
All patients are seen within 24 working hours of admission.
Staffing for Model A
The role of acute neurology clinical coordinator could be performed by a nurse, extended scope therapist or physician associate (all band 7): » Twice daily review for new referrals (preferably
through an electronic ward referral system). » In-reach to AMU to pick up new referrals at
9am Monday to Friday (flagged for review at admission).
» Contact via bleep for urgent queries. » Collation of data regarding the clinical query by
admitting team. » Clinically assessing the patient using an
impairment-based approach. » Obtaining information on the history (including
collateral history from witnesses if needed) prior to consultant review.
» Summarising the investigations performed. » Expediting investigations if clinically appropriate. » Documenting referral details for consultant review
and directly liaising with neurology consultants to facilitate appropriate prioritisation; all patients to be reviewed by a neurologist.
» Identification of frequent attenders. » Nurse led telephone clinics to support follow up
of early discharge and management of frequent attenders.

Hyper acute neurology servicesFor district general hospitals and regional neuroscience centres
11
Role of neurologist
» Admitted ward referral service – patients admitted 9am to 5pm reviewed same day.
» Availability for telephone advice to ED / AMU consultants.
» Liaison with acute neurology nurse. » Ensure sufficient training, support and continuing
professional development (CPD) for acute neurology nurse.
» Review of all specialist neurology nurse documented referrals.
» Provide definitive diagnosis. » Management plan, including explicit escalation
plans for frequent attenders to avoid re-presentation to emergency / acute services.
» “Hot clinics” – depending on service size this is most likely to be delivered by “acute” slots delivered daily within existing general neurology clinics.
» Urgent referral management for admission avoidance (see Model B, page 9): » GP telephone calls. » CCGs may wish to access online referral
management via the regional neuroscience centre who will be better resourced to provide such a service. Doing so will significantly reduce the burden on the DGH neurologists, improve access to advice and reduce costs for CCGs.
» With sufficient staffing, cross cover to provide consistent weekday service even accounting for leave.
There will also be access to: » General radiology service for CT and MRI (five
day service): » Local liaison to ensure responsiveness for
rapid access to CT / MRI where request has been made by a consultant neurologist.
» Escalation processes for specialist neuroradiology review where required.
» Clinical neurophysiology service providing EEGs, EMGs – where not present this should be commissioned to enable timely decision-making and discharge.
Out of hours cover
» Acute neurological care at 5pm to 9am Monday to Friday and on weekends will be led by the acute medical team, with appropriate advice / escalation to 24/7 services based at the regional neurosciences centre. In the longer term a solution to provide a seven day service in all DGHs is desirable. At present, as this involves significant additional resource and logistical hurdles with cross-trust working / telemedicine, this is outside the scope of this model.
» Patients who are discharged from ED / AMU overnight by emergency or acute physicians but felt to require early but not inpatient neurological review are referred through a simple written / electronic process for triage by neurology consultants in the morning to either a hot clinic or routine outpatient neurology as required.
Regional tertiary neuroscience centreModel for a HANS | Model B The major difference to the acute general hospital model is the greater availability of consultant neurologists, the availability of neurology trainees and 24/7 service. This allows review of patients prior to admission and in-reach into ED where appropriate.
The centre will have its local population and a secondary catchment area for tertiary services of over one million, with all specialities on site.
Patient with suspected neurological diagnosis for admission (9am to 5pm)
A patient entering the ED is assessed and, if an admission for neurological diagnosis is warranted, the patient is referred to the AMU. At this stage, where time allows, patients in whom an admission decision has already been made will be reviewed in the ED by the neurology team, as this may identify patients who would benefit from earlier discharge. If it is not possible to assess within ED itself, the patient will be seen by a neurologist (consultant or Specialty Trainees with consultant review) within four hours of admission.

12
Hyper acute neurology servicesFor district general hospitals and regional neuroscience centres
This model can work without an inpatient secondary care neurology unit. Evidence from pilots suggests the majority of the benefit arises from early acute liaison resulting in admission avoidance or rapid discharge (“zero length of stay patients”). However, for those patients who do require admission, the pilot data (from King’s and St George’s) suggest neurological ownership of care at secondary care level within an AMU leads to improved outcomes.
Neurology acute short stay admission units (NASSAU)
The NASSAU has either virtual beds or dedicated neurology beds based within the AMU. (The St George’s hospital pilot allocated six beds, for example, but this would depend upon local processes and throughput). This requires a full team in addition to the acute neurology consultant and specialist registrar (SpR). In addition an ST1/2 / + F1/2 or Physician Associate support are required although this can be drawn from the existing AMU team and does not require additional investment. Clear nursing protocols on shared care are required. Patients are reviewed by an acute neurology consultant daily. As the purpose of the unit is to enable rapid discharge home and direct access to specialist care, the length of stay on the short stay admissions unit should not exceed three days (as is the case of AMU admissions in general). If the neurological problem requires investigation or treatment for longer than this and there is no medical contra-indication, patients are transferred to the regional neurology unit. If patients need more time in hospital for treatment of ongoing non-neurological medical problems, or are awaiting a care package or placement they would transfer to a medical ward. This is essential if a NASSAU is to work well without compromising the flow of patients though the tertiary neurology unit.
Where patients with acute neurological problems are referred by GPs directly to the AMU this should be following neurology consultant advice and the acute neurology team will pick them up for onward admission within working hours.
Pre-existing local acute pathways are likely to apply for management of certain neurological conditions in
individual centres. Stroke patients will follow existing hyper acute stroke pathways. Others, for example, patients with traumatic brain injury, potential subarachnoid haemorrhage, or acute brain infection may follow alternative pathways depending on the site.
In general, patients with the following conditions would not ordinarily be admitted to a NASSAU. » Elderly patients with delirium / confusional state. » Elderly patients with reduced mobility and falls
unless a clear primary neurological cause is identified.
» Patients with known neurological disease (eg Parkinson’s disease, Alzheimer’s disease, multiple sclerosis) where the condition is a complicating factor but not the primary reason for admission. However, these patients would nonetheless have access to early neurological advice if needed.
» Suspected neurosurgical emergencies.
Patient with suspected neurological diagnosis – not requiring admission – 9am to 5pm
The role includes a review of all patients rejected by the acute stroke pathway (ie “stroke mimics”). These patients will, in any case, have been reviewed by a neurology / stroke physician at point of entry. The change in practice will be to identify alternative neurological diagnoses and clear plans of management (which may not currently be possible in stroke pathways due to time pressures) and facilitate early discharge and avoid readmission.
The pathway does not envisage routine reviews of non-admitted patients due to the numbers of patients involved -- that is, 17 per cent of all ED attendances in London. However, patients who attend more than one ED attendance for the same issue within a two week period – repeat attenders – and who are not admitted are reviewed in the ED by the neurology consultant or senior SpR. This service does depend on other work commitments. The aim here is to rationalise future investigation, to consider early treatments, and most importantly, to avoid re-attendance to the ED. If an ED review has not been possible due to service pressures, then these patients are referred to neurology “hot clinics” for early review.

Hyper acute neurology servicesFor district general hospitals and regional neuroscience centres
13
Patient with suspected neurological diagnosis for admission – 5pm to 9am and weekends
The patient is referred to medicine and remains under their care. The patient is reviewed by an on-call neurology SpR for early advice on management out of hours where possible. The patient is then picked up by acute neurology day teams on AMU/clinical decisions unit (CDU) the next day. Patients with new neurological symptoms with no prior diagnosis and do not meet the criteria for admission are referred to most appropriate outpatient facing service or back to the GP for symptom surveillance or may be referred on to a “hot clinic”. Staffing for Model B
Role of the SPR
» Identified neurology SpR within hours » 9am to 5pm acute neurology registrar, holding
bleep. » Ideally two registrars should be identified to
cover this role to allow inclusion of hot clinics within the pathway and cover for leave.
» 5pm to 9am and weekends: » Shared cover with acute stroke in most
centres. » Stroke care will necessarily be a priority out
of hours. » Contact via bleep for urgent queries. » ED in-reach and advice 24 hours a day
(consultant led, SpR supported 9am to 5pm). » AMU in-reach with consultant, including am AMU
ward round. » Review patients referred by ED for admission. » Clerking secondary care neurological referrals
requiring admission (within 9am to 5pm). » Obtaining information on the history (including
collateral history from witnesses if needed) prior to consultant review and summarising the investigations performed.
» Expediting investigations if clinically appropriate. » “Hot clinics” (consultant supported).
Role of the neurologist
» Consultant of week model used. » Daily ward round on AMU and review of admitted
patients (early am). » Weekend ward round by on-call neurology
consultant. » Liaison meeting with acute medicine – to facilitate
discharge planning (am). » Handover meeting for on-call teams (pm). » Review of referrals once clerked by SPR. » “Hot clinics”:
» Hot clinics would facilitate discharge from ED or early discharge from AMU.
» Triage to hot clinics would be via neurology consultant in hours, or neurology SpR out of hours (with consultant advice if needed).
» Overnight discharges by ED / AMU referred. for urgent OP review picked up for triage as a routine process in the morning (see below).
» Patients to be seen within 1-3 days (urgency to be determined by consultant).
» GP access via telephone referral for urgent cases to facilitate admission avoidance.
» Electronical urgent referral management: » GP advice via instant messaging within 24
hours (eg through the Kinesis system currently in use in a number of trusts in London).
» The Kinesis system allows mobile phone notification to consultants and so could be used, if appropriately resourced, to provide 9 am to 5pm advice to GPs within much tighter time frames (eg within 2 to 4 hours).
Role of acute medical teams
Royal College of Physicians (RCP) guidelines for acute medical care recommend a 12 hour a day, 7 day a week, “shop floor” consultant presence in acute medical units. Due to staffing pressures and low ratios of neurologists to population relative to that recommended by the ABN, it is not possible nor likely to be possible to provide neurology consultant presence 12 hours a day, 7 days a week. Furthermore, numbers of patients are unlikely to ever justify such a presence. Pressures on acute stroke services in London preclude neurology registrars (responsible for acute stroke rotas) taking a lead in ED / AMU in-reach out of hours.

14
Hyper acute neurology servicesFor district general hospitals and regional neuroscience centres
Most AMUs in London have an acute medical consultant on site 12 hours a day with additional out of hours cover. Therefore after 5pm to 9am and on weekends acute medical consultants would remain responsible for new admissions, with support and advice from the neurology registrar / consultant.
Patients who are discharged from ED / AMU overnight by emergency or acute physicians but felt to require early (but not inpatient) neurological review are referred through a simple written / electronic process to the day acute neurology team. These referrals are picked up as routine process early morning and triaged by consultant as appropriate to hot clinics or routine neurology outpatient clinics. The neurology SpR out of hours will have access to booking these clinic slots to facilitate early discharge overnight. Liaison with EDs and AMUs
In both model A and model B a key issue will be effective liaison with AMUs and EDs. Due to staffing pressures at acute hospitals, out of hours cover in both models will largely be delivered by emergency medicine and acute medicine, with neurological support.
To facilitate this, a designated consultant should be identified within emergency medicine and acute medicine to act as neurology / stroke liaison. This role would entail: » Acting as a single point of contact for feedback. » Working with neurology to develop, coordinate
and implement local hyper acute neurology pathways (eg for thunderclap headache, status epilepticus).
» Responsibility for coordinating regular CPD for acute neurology with ED / AMU: » This is particularly important given high
proportion of acute presentations with a neurological flavour and high rates of junior staff turnover in ED / AMU.
» Acting as a focus of enhanced neurology expertise within the ED or AMU team for internal discussions.
Moving to these models, particularly in regional neuroscience centres (model B), will lead to
acute medical trainees losing exposure to acute neurological conditions. They will, however, be required to manage acute neurological conditions in both DGHs and in their future consultant roles. Therefore from a training perspective, it is desirable for acute medical ST3+ trainees to rotate through acute neurology services (in addition to providing additional staffing support).
Service structure for models
Acute hospital
» Acute neurology clinical coordinator (1 / 350,000 population, based on Croydon model).
» Consultant neurologists, 1/70,000 population. » Neurophysiology services where not already
commissioned. » Radiology services will need some
reconfiguration. Increased neurological input will reduce the proportion of patients receiving imaging. » Need for responsive radiology to ensure timely
scans in patients requiring input. » AMU link consultant. » ED link consultant.
Regional centre
» Consultant neurologists (2 options): » 2-3 WTE acute neurology consultants OR » Rota – consultant of the week (likely need
a minimum of 7 to allow 7-8 weeks a year to minimise impact on outpatient neurology services).
» Neurology SpR: » Minimum two ST3+ to cover acute neurology
(or an alternative mechanism to allow cross cover for leave for one ST3+ with cover for OPD clinics and other training requirements).
» Out of hours: » SpR – linked to stroke.
» AMU link consultant. » ED link consultant. » Optional - Acute medicine SpR (see Liaison with
AMUs, left). » Senior house officer or physician associate -
Only required if a NASSAU with neurological ownership of patients.

Hyper acute neurology servicesFor district general hospitals and regional neuroscience centres
15
Potential financial benefitsCost of current neurological admissions in LondonSee Appendix 2 for further details.
Elective admissions Non elective admissions Total
Elective admissions
Elective admissions
spend
Non elective admissions
Non elective admissions
spend
Total admissions Total admissions
spend149,925 £32,425,991 79,430 £75,482,853 229,355 £107,914,077
The benefits of this is model are multifactorial, reflecting improvements in admission avoidance, proactive management of frequent emergency attenders, early specialist care and rapid discharge of admitted patients and direct primary care access to urgent specialist input. It is difficult to model all of the benefits.
As an illustration, the HANU pilots at King’s and St George’s identified that 19 per cent and 23 per cent of patients respectively were prevented from admission with early neurological input. Previously many patients had been admitted to the AMU for tests, and or a neurological review, and diagnosis. The main impact of the model will be on the 0-3 day stay patients. Approximately half of admissions during the HANU pilots were for headache or seizures (King’s epilepsy/seizures - 26% and headaches - 24%; UCLH seizures - 21.8% and headaches - 25.8%).
An example of the current cost of target group using only migraine and epilepsy, extracted from London-wide secondary uses service (SUS) data, and assuming a 20 per cent prevention of admissions (as at St George’s and King’s) would predict 3,141 fewer admissions for these two conditions with a reduction in admission costs of £3,055,791.
Number of patients
prevented from being admitted (20% of total)
Spend per admission5
Admission Cost
Epilepsy 1,348 1,371 £1,848,562Migraine 1,792 674 £1,207,230Total 3,141 2,044 £3,055,791
Cost of proposed modelThe cost of the model will depend on current resourcing and the impact of reassigning staff to the HANS.
The main cost elements of the model:
» Consultant costs – depends on current local numbers at regional centre and DGH reassigned to support the service
» Costs for ST3+ trainees (funded by Health Education England [HEE] in regional centres) – reassigned to support service
» Costs for acute neurology clinical coordinator (recruit, band 7/8a physician associate, specialist nurse or expanded scope therapy practitioner, approximately £50,000)
» Recruitment costs » Diagnostic tests: Investment in neurophysiology
services where not already present in DGHs. » Administration support
Potential risks » Not able to recruit suitable candidates to acute
neurology consultant and acute neurology clinical coordinator roles.
» Initially only open during working hours at DGH sites.
» Single handed coordinator – cover arrangements – could consider other specialist nurses who are currently employed by trust.
» Increase in demand for outpatients – “just in case” reasons/patient pressure or fear of complaint.
» Behaviour change (eg neurologists – rota for acute, ED/general medicine – removing work).
» Service is overwhelmed due to stimulated demand – impact on response time and care management time. Protocols and audit.
Recommendations » Discussion with interested parties from December
2016. » Pilot 2017. » Evaluation of pilot 2018.
5. Total spend (SUS SEM Commissioning for Value 2014/15) divided by admissions (NIN)

16
Hyper acute neurology servicesFor district general hospitals and regional neuroscience centres
Appendix 1 | RCP and the ABN
The Royal College of Physicians (RCP) and the Association of British Neurologists (ABN) published a 2011 paper, Local adult neurology services for the next decade, which made six recommendations for acute neurology ser¬vices (unscheduled care):
1. Patients should ideally be admitted to hospitals providing an acute neurology service led by consultant neurologists.
2. There should be a change in emphasis from scheduled to unscheduled care, to allow the development of acute neurology services in the AGHs that provide inpatient services.
3. The hospital should have an acute neurology ward area, led by a consultant neurologist with specialist staff, next to the acute stroke unit.
4. The operational policy should include: » Daily consultant ward rounds » Local neuroradiology linked to the regional
neurosciences centre » Local access to clinical neurophysiology » Access to local ITU and neurorehabilitation » Close operational links to the regional centre
for rapid transfer and repatriation of appropriate patients
» Development of on-call rotas
5. Consultant neurologist management of emergency cases could be achieved by modification of job plans to include ward liaison work, emergency outpatient clinics and daily ward rounds in admitting areas to prevent and shorten admissions.
6. This may require an expansion in the hospital neurology workforce, appointing neurologists solely to provide emergency care.

Hyper acute neurology servicesFor district general hospitals and regional neuroscience centres
17
Elective Non elective TotalCCG Total elective
admissionsElective admissions - spend £
Non elective admissions
Non elective admissions - spend £
Total admissions
Total admissions - spend £
North Central London STP
NHS Barnet CCG 7,071 1,295,555 3,706 3,680,627 10,777 4,976,183 NHS Camden CCG 4,291 801,548 2,288 1,568,479 6,579 2,373,491 NHS Enfield CCG 6,318 1,085,722 3,063 3,010,530 9,381 4,096,252 NHS Haringey CCG 4,412 1,203,933 2,260 2,295,406 6,672 3,499,339 NHS Islington CCG 4,898 943,045 2,327 1,821,197 7,225 2,764,242 NC London STP 26,990 5,329,803 13,644 12,376,239 40,634 17,709,507
North East London STP
NHS Barking and Dagenham CCG
3,406 590,710 1,856 1,427,256 5,262 2,019,007
NHS City and Hackney CCG
4,003 847,139 2,348 2,182,615 6,351 3,029,754
NHS Havering CCG 5,011 956,039 2,478 2,762,927 7,489 3,718,966 NHS Newham CCG 4,432 877,079 2,728 2,527,564 7,160 3,404,643 NHS Redbridge CCG
5,011 862,338 2,671 2,356,205 7,682 3,218,543
NHS Tower Hamlets CCG
3,661 750,237 1,969 2,501,303 5,630 3,252,266
NHS Waltham Forest CCG
4,632 947,606 2,685 2,572,195 7,317 3,519,801
NE London STP 30,156 5,831,148 16,735 16,330,065 46,891 22,162,980
North West London STP
NHS Brent CCG 6,156 1,088,683 3,178 2,774,612 9,334 3,863,295 NHS Central London (Westminster) CCG
2,647 588,529 1,416 1,441,832 4,063 2,030,362
NHS Ealing CCG 7,138 1,685,421 3,997 3,255,170 11,135 4,940,591 NHS Hammersmith and Fulham CCG
3,475 687,959 2,009 1,806,536 5,484 2,494,495
NHS Harrow CCG 4,715 947,098 2,304 2,096,721 7,019 3,043,818 NHS Hillingdon CCG 6,423 1,203,994 3,196 2,944,868 9,619 4,148,862 NHS Hounslow CCG 4,788 1,129,167 2,783 3,053,162 7,571 4,182,329 NHS West London CCG
3,625 880,964 1,912 1,882,785 5,537 2,763,749
NW London STP 38,967 8,211,815 20,795 19,255,686 59,762 27,467,501
London total 149,925 32,425,991 79,430 75,482,853 229,355 107,914,077
Appendix 2 | CCG / STP breakdown of hospital admissions (HES, 2014/15)

18
Hyper acute neurology servicesFor district general hospitals and regional neuroscience centres
Elective Non elective TotalCCG Total elective
admissionsElective admissions - spend £
Non elective admissions
Non elective admissions - spend £
Total admissions
Total admissions - spend £
South East London STP
NHS Bexley CCG 4,110 934,825 2,126 2,640,020 6,236 3,574,845 NHS Bromley CCG 6,405 1,593,217 3,354 2,804,907 9,759 4,398,123 NHS Greenwich CCG
4,177 1,062,075 2,027 2,489,405 6,204 3,551,480
NHS Lambeth CCG 5,317 1,389,751 2,960 2,409,430 8,277 3,799,181 NHS Lewisham CCG 4,632 1,226,721 2,454 2,299,187 7,086 3,525,909 NHS Southwark CCG
4,769 1,008,235 2,702 2,176,736 7,471 3,184,971
South East London STP
29,410 7,214,824 15,623 14,819,685 45,033 22,034,509
South West London STPNHS Croydon CCG 5,598 1,445,240 2,918 3,792,562 8,516 5,237,803 NHS Kingston CCG 2,943 656,473 1,345 1,241,008 4,288 1,897,482 NHS Merton CCG 3,715 745,518 1,981 1,532,625 5,696 2,278,143 NHS Richmond CCG 3,132 777,647 1,561 1,648,337 4,693 2,425,984 NHS Sutton CCG 4,056 817,621 2,092 2,323,579 6,148 3,141,200 NHS Wandsworth CCG
4,958 1,395,902 2,736 2,163,067 7,694 3,558,968
South West London STP
24,402 5,838,401 12,633 12,701,178 37,035 18,539,580
London total 149,925 32,425,991 79,430 75,482,853 229,355 107,914,077
Appendix 2 | CCG / STP breakdown of hospital admissions (HES, 2014/15)

Hyper acute neurology servicesFor district general hospitals and regional neuroscience centres
19
Appendix 3 Common conditions admissions Epilepsy, headache and migraine CCG Epilepsy -
non-elective admissions
Epilepsy - non-elective spend
Migraine and Headache - non-elective admissions
Migraine and headache - non-elective spend
% of total neurology admissions
% of total neurology spend
North Central London
NHS Barnet CCG 265 442,474 305 220,587 12% 17%NHS Camden CCG 200 248,775 212 138,463 14% 22%NHS Enfield CCG 224 323,852 297 209,224 12% 18%NHS Haringey CCG 221 306,168 253 173,966 16% 19%NHS Islington CCG 267 350,900 292 177,276 18% 25%
NC London STP 1,177 1,672,169 1,359 919,516 14% 19%
North East London
NHS Barking and Dagenham CCG
163 254,204 224 187,157 16% 28%
NHS City and Hackney CCG 201 295,704 208 136,546 14% 19%NHS Havering CCG 203 303,704 222 168,212 13% 17%NHS Newham CCG 207 354,493 361 267,866 17% 22%NHS Redbridge CCG 179 246,094 290 215,058 13% 18%NHS Tower Hamlets CCG 189 314,442 224 142,917 16% 19%NHS Waltham Forest CCG 225 313,956 360 261,923 17% 22%NE London STP 1,367 2,082,597 1,889 1,379,679 15% 20%
North West London
NHS Brent CCG 259 382,019 322 207,915 14% 20%NHS Central London (Westminster) CCG
113 178,521 183 129,708 17% 21%
NHS Ealing CCG 292 453,491 454 369,774 15% 20%NHS Hammersmith and Fulham CCG
148 170,487 296 195,354 18% 20%
NHS Harrow CCG 198 287,027 223 163,700 14% 20%NHS Hillingdon CCG 255 353,531 387 272,434 15% 20%NHS Hounslow CCG 224 317,617 436 301,806 19% 19%NHS West London CCG 161 221,999 259 187,118 17% 20%NW London STP 1,650 2,364,692 2,560 1,827,809 16% 20%
London Total 6,742 9,242,808 8,962 6,036,149 15% 19%
`

20
Hyper acute neurology servicesFor district general hospitals and regional neuroscience centres
Appendix 3 Common conditions admissions Epilepsy, headache and migraine CCG Epilepsy -
non-elective admissions
Epilepsy - non-elective spend
Migraine and Headache - non-elective admissions
Migraine and headache - non-elective spend
% of total neurology admissions
% of total neurology spend
South East London
NHS Bexley CCG 144 171,993 244 123,841 14% 14%NHS Bromley CCG 274 230,269 321 135,597 14% 14%NHS Greenwich CCG 172 242,686 216 144,301 15% 18%NHS Lambeth CCG 303 293,768 342 150,532 18% 20%NHS Lewisham CCG 210 268,541 273 183,358 16% 24%NHS Southwark CCG 250 218,211 320 128,022 18% 19%South East London STP 1,353 1,425,468 1,716 865,651 16% 18%
South West London
NHS Croydon CCG 374 560,851 466 331,067 21% 21%NHS Kingston CCG 81 115,433 97 69,824 10% 15%NHS Merton CCG 185 245,734 217 137,702 17% 22%NHS Richmond CCG 123 164,705 152 107,796 13% 15%NHS Sutton CCG 192 286,564 226 193,141 15% 20%NHS Wandsworth CCG 240 324,595 280 203,964 16% 21%SW London STP 1,195 1,697,882 1,438 1,043,494 16% 19%
London Total 6,742 9,242,808 8,962 6,036,149 15% 19%

Hyper acute neurology servicesFor district general hospitals and regional neuroscience centres
21
Appendix 4 | Data sources
Hospital activity data Definition Hospital admissions over the age of 20 with a mention of a neurological condition (as defined by ICD-10 codescategories by the NIN to fall under neurology); common condition data is based on primary diagnosis categorySource Neurology Intelligence Network (NIN), Public Health EnglandData source Hospital Episode Statistics (HES), Admitted Patient Care datasetTime period 2014/15Published October 2016Link www.yhpho.org.uk//resource/view.aspx?RID=242946 Spend data Definition Spend on neurology conditions (as defined by the neurology programme budget)Source Commissioning for Value - Neurology focus packData source SUS SEM (Secondary User Services Extract Mart), Admitted Patient Care datasetTime period 2014/15Published October 2016Link www.england.nhs.uk/rightcare/intel/cfv/data-packs/

22
Hyper acute neurology servicesFor district general hospitals and regional neuroscience centres
Appendix 5 | Glossary
A&E Accident and EmergencyABN Association of British Neurologists AMU Acute medical unitCCG Clinical Commissioning GroupCDU Clinical decisions unitCPD Continuing professional developmentCT Computed tomographyED Emergency departmentEEG ElectroencephalogramEMG ElectromyographyGP General practionerHANU Hyper acute neurology unitHEE Health Education EnglandITU Intensive therapy unitMRI Magnetic resonance imagingNASSAU Neurology acute short stay admission unitsNICE National Institute for Health and Care ExcellenceRCP Royal College of PhysiciansSpR Specialist registrarSTP Sustainability and transformation planSUS Secondary uses serviceWTE Whole time equivalent